 Wei Li
Wei Li Xiaojun Liu1
Xiaojun Liu1 Lei Zhang
Lei Zhang Tianfang Li
Tianfang Li
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 25 April 2022
Sec. Atherosclerosis and Vascular Medicine
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.824561
This article is part of the Research Topic Insights in Atherosclerosis and Vascular Medicine: 2021 View all 22 articles
Objective: This study aimed to investigate the association of serum bone turnover markers (BTMs) with metabolic syndrome components and carotid atherosclerosis in patients with type 2 diabetes mellitus (T2DM).
Methods: We performed a cross-sectional based study in T2DM populations. Serum BTMs including N-terminal osteocalcin (N-MID), β-cross-linked C-telopeptide of type I collagen (β-CTX), and procollagen type I N-terminal propeptide (PINP) were measured by immunoassay method. Carotid artery intima-media thickness and carotid artery plaque (CAP) were measured by B-mode ultrasound.
Results: The serum N-MID, PINP, and β-CTX levels significantly lower in the CAP group compared with the non-CAP group. N-MID and PINP levels were inversely associated with fasting blood glucose, HOMA-IR, CRP, eGFR, and triglycerides (all P < 0.05), whereas β-CTX levels were negatively associated with triglycerides (P < 0.05). After multiple adjustment, the odds ratios (ORs) were substantially higher for CAP with decreased N-MID level (OR = 0.958; 95% CI = 0.926–0.991; P = 0.013). However, serum levels of PINP and β-CTX were not associated with the presence of CAP. Multivariate logistic regression analysis further revealed that serum N-MID, PINP, and β-CTX levels were significantly associated with hypertriglyceridemia, whereas serum N-MID and β-CTX levels were associated with overweight/obesity risk.
Conclusions: These findings indicated that serum N-MID level was an independent risk factor for carotid atherosclerosis, whereas BTM levels were associated with other metabolic syndrome components in a T2DM population.
Bone turnover is a dynamic process that comprises the formation of new bone by osteoblasts and the resorption of old bone by osteoclasts. This process generates many bone turnover markers (BTMs) from bone cells and the bone matrix, which provide a noninvasive evaluation of bone remodeling status (1, 2). BTMs comprises bone formation markers, namely, N-terminal osteocalcin (N-MID), procollagen type I N-terminal propeptide (PINP), and bone resorption markers, such as β-cross-linked C-telopeptide of type I collagen (β-CTX). All these molecules are key markers of bone metabolism (3, 4). In addition to the use of BTMs as indicators of bone formation and resorption, as well as markers for the assessment, diagnosis, and treatment of osteoporosis, BTMs have been shown to be associated with energy metabolism in recent studies (5, 6).
Previous studies have shown that bone metabolism is affected by the risk factors of atherosclerosis, such as obesity, hypertension, dyslipidemia, and diabetes (7–9). Patients with diabetes are at two-to fourfold increased risk of cardiovascular disease (CVD), which is reflected by atherosclerosis (10). BTMs are highly associated with diabetes, insulin sensitivity, and beta cell function, and serum osteocalcin plays an important role in the association of bone metabolism with glucose metabolism (11, 12). A cross-sectional based study has demonstrated that serum osteocalcin level is an independent risk factor for carotid atherosclerosis in patients with T2DM (13). In addition, previous observational and indirect interventional studies suggested a relationship between serum osteocalcin level with metabolic homeostasis and CVD (14). However, the relationship of other BTMs with metabolic syndrome and carotid atherosclerosis risk is substantially unknown. Recently, a case-control study has shown that higher osteopontin concentrations are associated with increased CVD risk in T2DM patients, but no association is found for the osteocalcin level and risk of CVD (15). Furthermore, a longitudinal follow-up study demonstrated that the serum total osteocalcin level was not associated with the development of CVD after adjusting for other risk factors (16).
Clinical studies have revealed that the association between different BTMs and cardiometabolic risk is controversial, and most studies have focused on osteocalcin (15, 16). Accordingly, the present study aimed to determine whether serum N-MID levels and other BTMs were independently associated with carotid atherosclerosis and other cardiometabolic risk factors, such as obesity, hypertension, dyslipidemia, and metabolic syndrome (MetS) in patients with T2DM.
Cross-sectional study populations were recruited from the First Affiliated Hospital of Zhengzhou University between 2018 and 2020. Diabetes was defined as fasting blood glucose ≥7.0 mmol/l, HbA1c≥ 6.5% or the use of any antidiabetic medication or self-reported history of diabetes based on the American Diabetes Association. Subjects were excluded if they had any known infection, malignant tumors, or were taking medicine that may influence the level of serum BTMs. Finally, a total of 1520 patients with T2DM were enrolled. Questionnaires were used to identify history of medical conditions, family history of disease, current medication use, and other lifestyle factors. Body weight and height were measured at baseline, and body mass index (BMI) was calculated by body weight (kg) divided by height square (m2). Blood pressure was measured using an automatic blood-pressure meter after seating for at least 10 min. The average of three measurements was recorded for further analysis. This study was approved by the Institutional Review Broad of the First Affiliated Hospital of Zhengzhou University.
Venous blood samples were collected in the morning followed by overnight fasting. An auto-biochemical analyzer was used to determine the fasting blood glucose (FBG), serum concentrations of total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), uric acid (UA), fasting plasma insulin, creatinine, and C-reactive protein (CRP) as previously described. Glycated hemoglobin (HbA1c) concentrations were quantified using high-performance liquid chromatography. The estimated glomerular filtration rate (eGFR) was calculated according to the CKD-EPI equation. Insulin resistance was estimated using homeostasis model assessment index-insulin resistance (HOMA-IR). BTMs associated with bone metabolism including N-MID, PINP, and β-CTX were measured by electrical chemiluminescent immunoassay.
Trained technicians performed B mode ultrasonography using an Acuson Sequoia. A lateral view of bilateral images of common carotid arteries (1 cm proximal to the dilatation of the carotid bulb), carotid bulb, and internal carotid artery was obtained. Carotid artery intima-media thickness (CIMT) was defined as the mean of the maximum thickness in both right and left sides of the common carotid artery, and IMT is the distance between the lumen-intima interface and the media adventitia interface. The carotid artery plaque (CAP) was defined as either a focal structure that encroaches into the arterial lumen by at least 50% of the surrounding IMT value or a thickness of > 1.5 mm. CAP presence was defined as ≥1 plaque in any of the carotid arteries.
We used the definition of MetS according to the NCEPATP III criteria (17). Subjects were classified as having MetS when ≥3 of the following criteria were present: FBG level ≥5.6 mmol/L, blood pressure ≥130/85 mmHg, TG ≥1.7 mmol/L, HDL-C < 1.03 mmol/L for men and < 1.29 mmol/L for women, and waist circumference >102 cm for men and >88 cm for women.
Normally distributed data were expressed as the mean ±SD, whereas variables with a skewed distribution were reported as median (interquartile range). Categorical variables were represented by percentage. Mann–Whitney U-test was used to compare the mean ranks between the CAP and non-CAP groups. Correlation coefficients between BTMs and metabolic features were calculated by partial correlation analysis. Multivariate logistic regression models were used to estimate the association of CAP with BTMs. Potential confounding variables including age, gender, smoking, alcohol drinking, self-reported CVD, hypertension, CRP, BMI, FBG, HbA1c, HOMA-IR, TG, TC, HDL-C, and LDL-C were controlled in the regression models. Statistical analyses were performed using SPSS version 26.0 (Chicago, IL, USA). Results were considered statistically significant at P < 0.05.
The baseline clinical characteristics of the participants are shown in Table 1. A total of 1520 subjects were enrolled in the present study, among which 695 (45.7%) had CAP. Participants were classified according to the presence of carotid plaques as CAP and non-CAP groups. The CAP group had significantly lower systolic blood pressure (SBP), diastolic blood pressure (DBP), BMI, TC, TG, and UA levels, as well as eGFR, HOMA-IR, this group also had a higher frequency of hypertension and self-reported CVD (all P < 0.05). The CAP group had higher HDL-C levels and longer diabetes duration. Furthermore, serum N-MID, PINP, and β-CTX levels significantly lower in the CAP group compared with the non-CAP group (all P < 0.05).
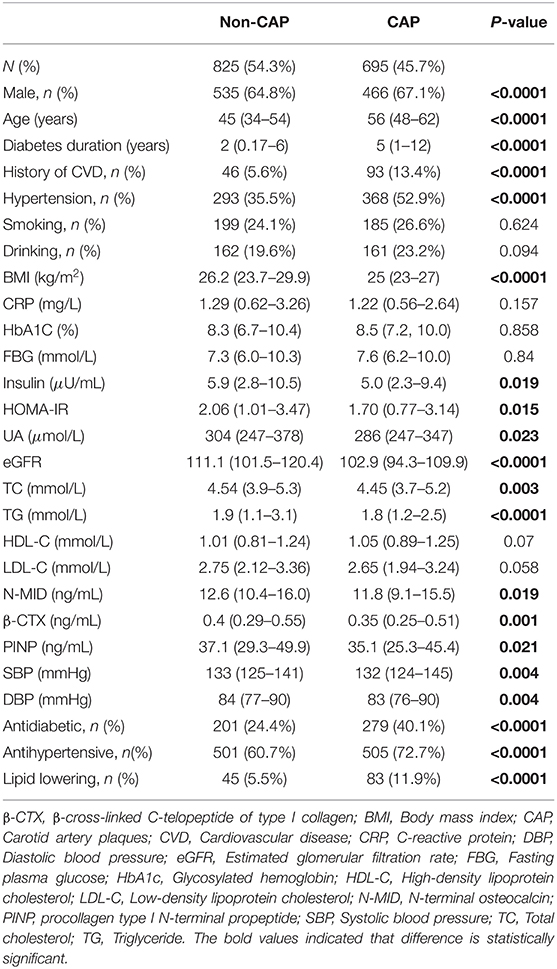
Table 1. Baseline characteristics for participants.
Spearman analysis showed that serum N-MID level was correlated with CRP (r = −0.127; P = 0.009), FBG (r = −0.235; P < 0.001), HbA1C (r = −0.224; P < 0.001), HDL-C (r = 0.105; P = 0.033), TG (r = −0.1; P = 0.041), eGFR (r = −0.19; P < 0.001), and SBP (r = 0.134; P = 0.006) after adjusting for age and sex. However, serum β-CTX was associated only with TG (r = −0.105; P = 0.032) and was not significantly associated with other parameters. Furthermore, serum PINP level was correlated with BMI (r = 0.149; P = 0.002), CRP (r = −0.103; P = 0.035), FBG (r = −0.233; P < 0.001), HbA1C (r = −0.187; P < 0.001), fasting plasma insulin (r = 0.193; P < 0.001), HOMA-IR (r = 0.098; P = 0.045), eGFR (r = −0.162; P = 0.001), and TG (r = −0.13; P = 0.007) after adjusting for age and sex (Table 2). However, the serum BTM levels was not independently associated with CIMT in all study populations.
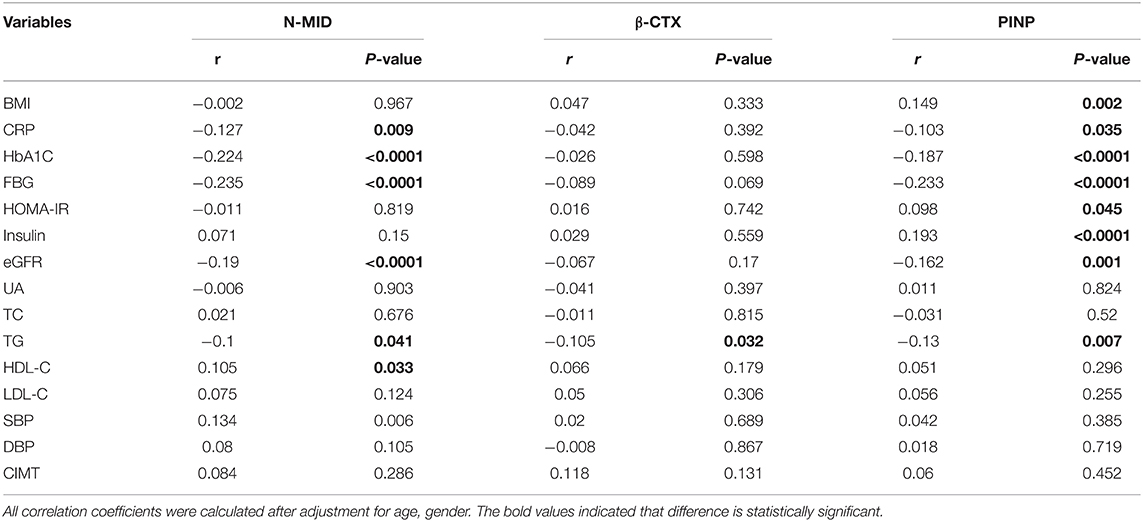
Table 2. Correlation between BTMs and other parameters in patients with T2DM.
Given that the BTM levels were significantly in inverse association with CRP, we adjusted for CRP in the multivariable logistic regression analysis. Table 3 shows that after adjusting for age, sex, BMI, and CRP, only reduced serum N-MID level were revealed to be significantly associated with increased risk of CAP (odds ratios (OR) 0.957; 95% CI = 0.927–0.988; P = 0.006). We obtained similar associations when the multivariable logistic regression analysis was further adjusted for smoking, alcohol drinking, duration of diabetes, hypertension, and history of CVD (OR = 0.958; 95% CI = 0.928–0.989; P = 0.008). Low serum N-MID indicated a high risk for CAP (OR = 0.958; 95% CI = 0.926–0.991; P = 0.013) after further adjusting for FBG, HbA1C, serum TC, TG, HDL-C, and LDL-C. However, the PINP and β-CTX levels were not significantly associated with the risk of CAP in all multivariable logistic regression models.
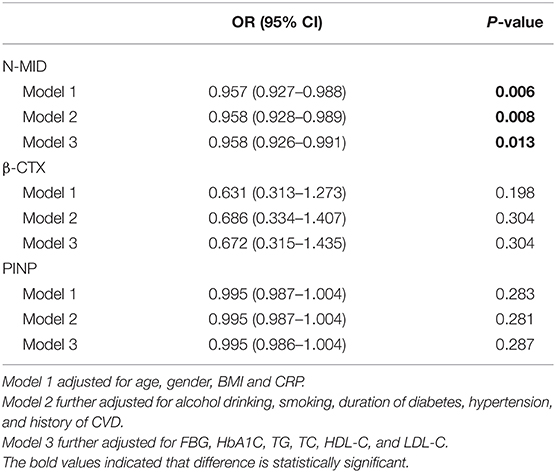
Table 3. Association of serum BTMs with CAP in T2DM populations.
Among MetS components, after adjusting for age, sex, BMI, CRP, smoking, alcohol drinking, duration of diabetes, hypertension, and history of CVD (model 2), overweight/obesity (BMI ≥ 25 kg/m2) were found to be negatively associated with N-MID (OR = 0.96; 95% CI = 0.94–0.99; P = 0.015) and β-CTX (OR = 0.446; 95% CI = 0.24–0.85; P = 0.014). Similarly, hypertriglyceridemia was negatively associated with N-MID (OR = 0.96; 95% CI = 0.93–0.99; P = 0.004) and β-CTX (OR = 0.34; 95% CI = 0.18–0.67; P = 0.002). Significant associations were also observed between the presence of hypertriglyceridemia and PINP after adjusting for potential confounders (OR = 0.99; 95% CI = 0.98–1.00; P = 0.003; model 2). However, no significant association was found between serum BTMs and the presence of MetS, hypertension, and HDL-C dyslipidemia in T2DM populations (Table 4).
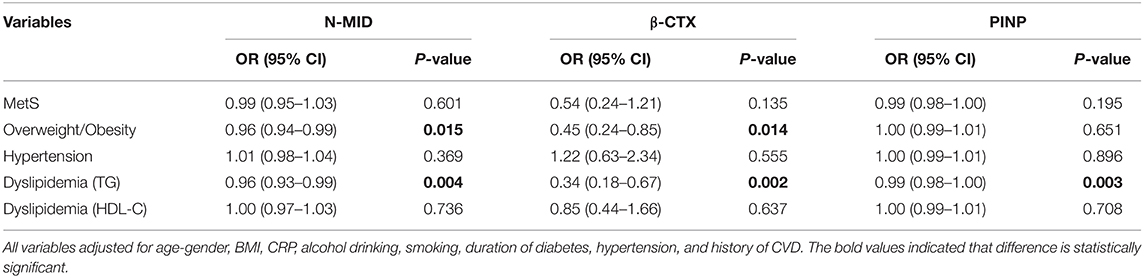
Table 4. Association of serum BTMs with metabolic syndrome components.
In the present study, we found an association between serum N-MID and the risk of carotid atherosclerosis in T2DM populations. These associations were independent of lifestyle factors, duration of diabetes, history of CVD, CRP, HbA1c, FBG, lipid parameters, and BMI. Multivariate logistic regression analysis revealed that serum N-MID, PINP, and β-CTX levels were significantly associated with hypertriglyceridemia, whereas serum N-MID and β-CTX levels were associated with overweight/obesity risk. These findings indicated the association between serum N-MID and metabolic syndrome components, as well as carotid atherosclerosis, independent of other known CVD risk factors in patients with T2DM, thus suggesting that BTMs (especially N-MID) were important for glucose and lipid metabolism, and atherosclerosis.
Several studies have shown that serum BTMs may be a predictor of CVD risk in patients with T2DM (15, 18). In a previous study, serum osteocalcin was negatively associated with parameters of atherosclerosis in T2DM patients (19). In another study, serum levels of osteocalcin were inversely associated with the metabolic syndrome and the severity of coronary artery disease in Chinese populations (20). Interestingly, consistent with previous studies, we observed that serum N-MID levels were an independent risk factor for carotid atherosclerosis in patients with T2DM. Endothelial dysfunction is considered as an early step in atherosclerosis development as it contributes to the initiation and early progression of atherosclerosis (21, 22). Some studies suggested that high serum osteocalcin level contributes to vascular calcification and atherosclerosis. However, different population lead to inconclusive results (23). Large longitudinal studies are needed to further explore the clinical relevance of serum osteocalcin in vascular calcification and atherosclerosis (24). In a mouse model of atherosclerosis, daily injections of osteocalcin reduced the risk of CVD, which showed an endothelial-protective effect because it improves glucose and lipid metabolism by activating the PI3K-Akt-eNOS signaling pathway (25). However, prospective studies are needed to clarify whether low osteocalcin level plays a causal role in atherosclerosis development.
The current study revealed that another bone formation marker, PINP level, was significantly associated with HOMA-IR, FBG, fasting insulin levels, CRP, and TG. These associations were reported in a previous study in which PINP was positively correlated with insulin sensitivity and negatively correlated with glucose and triglycerides (26). Significant associations were also observed between BTM levels and the presence of hypertriglyceridemia after adjustment for potential confounders. However, we did not find an association of serum PINP and β-CTX levels with CAP risk in T2DM populations. In view of the high correlation between PINP, β-CTX, and N-MID, the effects of PINP and β-CTX on carotid atherosclerosis were most likely to be attributable to the function of N-MID (11). Thus, the interactions among different BTMs require further investigations.
Vascular endothelial inflammation was considered to play a vital role in the mechanism of CVD development (27, 28). CRP is an acute-phase reactant and a well-known serum marker of chronic low-grade inflammation. It is associated with diabetes, hypertension, obesity, and CVDs (29, 30). In the present study, serum N-MID and PINP levels were negatively correlated with CRP. Accordingly, the results of current study may be partially attributed to the mechanism of chronic low-grade inflammation. Furthermore, elevated serum TG was an independent risk factor for CVD development (31). Consistent with previous studies, serum N-MID and PINP levels were negatively correlated with TG in our study (32). Meanwhile, after adjustment for potential confounders, all BMTs (including N-MID, β-CTX, and PINP) were negatively associated with hypertriglyceridemia. Therefore, given that serum N-MID levels were significantly associated with CRP and TG levels and the strong relationship of serum N-MID with carotid atherosclerosis risk, N-MID can be considered as a promising candidate for risk assessment and a potential intervention target for CVD.
A previous study has shown no significant correlation between CIMT and serum osteocalcin (33). In accordance with these findings, the present study demonstrated that the three BTMs were not significantly associated with CIMT in T2DM patients. Furthermore, clinical studies investigating the association of serum osteocalcin and CVD risk are controversial, and the lack of consistency may be due to different study populations or different degrees of confounding factors associated with serum osteocalcin level, such as metabolic factors and chronic low-grade inflammation, and these metabolic dysfunctions are related to the progression of atherosclerosis (34–36). In humans, bone turnover rate varies obviously according to individual variables, age and sex are the most important variables determining bone remodeling. Given that the serum levels of osteocalcin differ between sexes and alter with age, the relationship of serum osteocalcin levels with CVD risk may also differ according to these variables (37). Studies have demonstrated that close correlations of serum osteocalcin level with glucose and lipid metabolic disorders, obesity, and MetS (8, 38). Herein, the serum N-MID level was correlated with CRP, FBG, HbA1C, HDL-C, and TG after adjusting for age and sex. Similar associations were found in PINP, indicating that serum BTMs may play a key role in glucose and lipid metabolism. Thus, given the strong association between metabolic risk and atherosclerosis, our findings suggested that the association of BTMs with atherosclerosis may be influenced by metabolic variables.
Our cross-section study suggested that serum N-MID levels were significantly associated with carotid atherosclerosis in patients with T2DM even after adjusting for potential confounders. Serum BTMs level were associated with other metabolic syndrome components, which may reflect the role of BTMs as a circulating endocrine markers regulating glucose and lipid metabolism, thereby posing a cardiovascular risk to T2DM patients.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Ethical Committee of the First Affiliated Hospital of Zhengzhou University. The Ethics Committee waived the requirement of written informed consent for participation.
WL, EC, XL, LZ, LL, TL, and SL contributed to the conception and design of the study. WL, SL, ML, and RL recruited the subjects and supervised the study. WL, EC, LZ, LL, and XL analyzed the data. WL, EC, and SL wrote the initial draft of the article. WL, EC, LZ, TL, XL, and SL contributed to the writing, reviewing, and revising of the manuscript. All authors contributed to the article and approved the submitted version.
WL is funded by the National Natural Science Foundation of China (82000831).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the participants in this study.
β-CTX, β-cross-linked C-telopeptide of type I collagen; BMI, Body mass index; BTM, bone turnover markers; CAP, Carotid artery plaque; CI, Confidence interval; CIMT, Carotid intima-media thickness; CVD, Cardiovascular disease; CRP, C-reactive protein; DBP, Diastolic blood pressure; eGFR, Estimated glomerular filtration rate; FBG, Fasting plasma glucose; HbA1c, Glycosylated hemoglobin; HDL-C, High-density lipoprotein cholesterol; LDL-C, Low-density lipoprotein cholesterol; MetS, metabolic syndrome; N-MID, N-terminal osteocalcin; OR, Odds ratio; PINP, procollagen type I N-terminal propeptide; SBP, Systolic blood pressure; TC, Total cholesterol; TG, Triglyceride; T2DM, Type 2 diabetes mellitus; SUA, Serum uric acid.
1. Eastell R, Szulc P. Use of bone turnover markers in postmenopausal osteoporosis. Lancet Diabetes Endocrinol. (2017) 5:908–23. doi: 10.1016/S2213-8587(17)30184-5
2. Fontalis A, Eastell R. The challenge of long-term adherence: The role of bone turnover markers in monitoring bisphosphonate treatment of osteoporosis. Bone. (2020) 136:115336. doi: 10.1016/j.bone.2020.115336
3. Greenblatt MB, Tsai JN, Wein MN. Bone turnover markers in the diagnosis and monitoring of metabolic bone disease. Clin Chem. (2017) 63:464–74. doi: 10.1373/clinchem.2016.259085
4. Naylor K, Eastell R. Bone turnover markers: use in osteoporosis. Nat Rev Rheumatol. (2012) 8:379–89. doi: 10.1038/nrrheum.2012.86
5. Hygum K, Starup-Linde J, Harslof T, Vestergaard P, Langdahl BL. Mechanisms In Endocrinology: diabetes mellitus, a state of low bone turnover - a systematic review and meta-analysis. Eur J Endocrinol. (2017) 176:R137–57. doi: 10.1530/EJE-16-0652
6. Bellissimo MP, Roberts JL, Jones KH, Liu KR, Taibl K, Uppal, et al. Metabolomic Associations with Serum Bone Turnover Markers. Nutrients. (2020) 12:3161. doi: 10.3390/nu12103161
7. Reiss AB, Miyawaki N, Moon J, Kasselman LJ, Voloshyna IRD'Avino Jr, J De Leon. CKD, arterial calcification, atherosclerosis and bone health: inter-relationships and controversies. Atherosclerosis. (2018) 278:49–59. doi: 10.1016/j.atherosclerosis.2018.08.046
8. Kanazawa I, Yamaguchi T, Sugimoto T. Relationship between bone biochemical markers versus glucose/lipid metabolism and atherosclerosis; a longitudinal study in type 2 diabetes mellitus. Diabetes Res Clin Pract. (2011) 92:393–9. doi: 10.1016/j.diabres.2011.03.015
9. Florez H, Hernandez-Rodriguez J, Carrasco JL, Filella X, Prieto-Gonzalez S, Monegal A, et al. Low serum osteocalcin levels are associated with diabetes mellitus in glucocorticoid treated patients. Osteoporos Int. (2021) 33:745–50. doi: 10.1007/s00198-021-06167-z
10. La Sala L, Prattichizzo F, Ceriello A. The link between diabetes and atherosclerosis. Eur J Prev Cardiol. (2019) 26:15–24. doi: 10.1177/2047487319878373
11. Wang J, Yan DD, Hou XH, Bao YQ, Hu C, Zhang ZL, et al. Association of bone turnover markers with glucose metabolism in Chinese population. Acta Pharmacol Sin. (2017) 38:1611–7. doi: 10.1038/aps.2017.23
12. Cipriani C, Colangelo L, Santori R, Renella M, Mastrantonio M, Minisola S, et al. The interplay between bone and glucose metabolism. Front Endocrinol (Lausanne). (2020) 11:122. doi: 10.3389/fendo.2020.00122
13. Sheng L, Cao W, Cha B, Chen Z, Wang F, Liu J. Serum osteocalcin level and its association with carotid atherosclerosis in patients with type 2 diabetes. Cardiovasc Diabetol. (2013) 12:22. doi: 10.1186/1475-2840-12-22
14. Levinger I, Brennan-Speranza TC, Zulli A, Parker L, Lin X, Lewis JR, et al. Multifaceted interaction of bone, muscle, lifestyle interventions and metabolic and cardiovascular disease: role of osteocalcin. Osteoporos Int. (2017) 28:2265–73. doi: 10.1007/s00198-017-3994-3
15. Zwakenberg SR, van der Schouw YT, Schalkwijk CG, Spijkerman AMW, Beulens JWJ. Bone markers and cardiovascular risk in type 2 diabetes patients. Cardiovasc Diabetol. (2018) 17:45. doi: 10.1186/s12933-018-0691-2
16. Hwang YC, Kang M, Cho IJ, Jeong IK, Ahn KJ, Chung HY, et al. Association between the circulating total osteocalcin level and the development of cardiovascular disease in middle-aged men: a mean 8.7-year longitudinal follow-up study. J Atheroscler Thromb. (2015) 22:136–43. doi: 10.5551/jat.25718
17. Grundy SM, Cleeman JI, Merz CN, Brewer HB Jr, Clark LT, Hunninghake DB, et al. American College of Cardiology, American Heart. Implications of recent clinical trials for the National Cholesterol Education Program Adult Treatment Panel III guidelines. Circulation. (2004) 110:227–39. doi: 10.1161/01.CIR.0000133317.49796.0E
18. Holvik K, van Schoor NM, Eekhoff EM, Heijer Mden, Deeg DJ, Lips P, et al. Plasma osteocalcin levels as a predictor of cardiovascular disease in older men and women: a population-based cohort study. Eur J Endocrinol. (2014) 171:161–70. doi: 10.1530/EJE-13-1044
19. Reyes-Garcia R, Rozas-Moreno P, Jimenez-Moleon JJ, Villoslada MJ, Garcia-Salcedo JA, Santana-Morales S, et al. Relationship between serum levels of osteocalcin and atherosclerotic disease in type 2 diabetes. Diabetes Metab. (2012) 38:76–81. doi: 10.1016/j.diabet.2011.07.008
20. Bao Y, Zhou M, Lu Z, Li H, Wang Y, Sun L, et al. Serum levels of osteocalcin are inversely associated with the metabolic syndrome and the severity of coronary artery disease in Chinese men. Clin Endocrinol. (2011) 75:196–201. doi: 10.1111/j.1365-2265.2011.04065.x
21. Gimbrone MA Jr, Garcia-Cardena G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ Res. (2016) 118:620–36. doi: 10.1161/CIRCRESAHA.115.306301
22. Xu S. Therapeutic potential of blood flow mimetic compounds in preventing endothelial dysfunction and atherosclerosis. Pharmacol Res. (2020) 155:104737. doi: 10.1016/j.phrs.2020.104737
23. Skenteris NT, Seime T, Witasp A, Karlof E, Wasilewski GB, Heuschkel MA, et al. Osteomodulin attenuates smooth muscle cell osteogenic transition in vascular calcification. Clin Transl Med. (2022) 12:e682. doi: 10.1002/ctm2.682
24. Millar SA, Patel H, Anderson SI, England TJ, O'Sullivan SE. Osteocalcin, vascular calcification, and atherosclerosis: a systematic review and meta-analysis. Front Endocrinol. (2017) 8:183. doi: 10.3389/fendo.2017.00183
25. Dou J, Li H, Ma X, Zhang M, Fang Q, Nie M, et al. Osteocalcin attenuates high fat diet-induced impairment of endothelium-dependent relaxation through Akt/eNOS-dependent pathway. Cardiovasc Diabetol. (2014) 13:74. doi: 10.1186/1475-2840-13-74
26. Laurent MR, Cook MJ, Gielen E, Ward KA, Antonio L, Adams JE, et al. Lower bone turnover and relative bone deficits in men with metabolic syndrome: a matter of insulin sensitivity? The European male ageing study. Osteoporos Int. (2016) 27:3227–37. doi: 10.1007/s00198-016-3656-x
27. Serino A and Salazar G. Protective role of polyphenols against vascular inflammation, aging and cardiovascular disease. Nutrients. (2018) 11:53 doi: 10.3390/nu11010053
28. Marchio P, Guerra-Ojeda S, Vila JM, Aldasoro M, Victor VM, Mauricio MD. Targeting early atherosclerosis: a focus on oxidative stress and inflammation. Oxid Med Cell Longev. (2019) 2019:8563845. doi: 10.1155/2019/8563845
29. Zanoli L, Pino ADi, Terranova V, Marca SDi, Pisano M, Quattro RD, et al. Inflammation and ventricular-vascular coupling in hypertensive patients with metabolic syndrome. Nutr Metab Cardiovasc Dis. (2018) 28:1222–9. doi: 10.1016/j.numecd.2018.08.003
30. Yoon K, Ryu S, Lee J, Park JD. Higher and increased concentration of hs-CRP within normal range can predict the incidence of metabolic syndrome in healthy men. Diabetes Metab Syndr. (2018) 12:977–83. doi: 10.1016/j.dsx.2018.06.008
32. Liu XX, Jiang L, Liu Q, Zhang J, Niu W, Liu J, et al. Low bone turnover markers in young and middle-aged male patients with type 2 diabetes mellitus. J Diabetes Res. (2020) 2020:6191468. doi: 10.1155/2020/6191468
33. Luo Y, Ma X, Hao Y, Xiong Q, Xu Y, Pan X, et al. Relationship between serum osteocalcin level and carotid intima-media thickness in a metabolically healthy Chinese population. Cardiovasc Diabetol. (2015) 14:82. doi: 10.1186/s12933-015-0245-9
34. Poznyak A, Grechko AV, Poggio P, Myasoedova VA, Alfieri V, Orekhov AN. The diabetes mellitus-atherosclerosis connection: the role of lipid and glucose metabolism and chronic inflammation. Int J Mol Sci. (2020) 21:1835 doi: 10.3390/ijms21051835
35. Aboonabi A, Meyer RR, Singh I. The association between metabolic syndrome components and the development of atherosclerosis. J Hum Hypertens. (2019) 33:844–55. doi: 10.1038/s41371-019-0273-0
36. Mehu M, Narasimhulu CA, Singla DK. Inflammatory cells in atherosclerosis. Antioxidants (Basel). (2022) 11:233. doi: 10.3390/antiox11020233
37. Jung KY, Kim KM, Ku EJ, Kim YJ, Lee DH, Choi SH, et al. Age- and sex-specific association of circulating osteocalcin with dynamic measures of glucose homeostasis. Osteoporos Int. (2016) 27:1021–9. doi: 10.1007/s00198-015-3315-7
Keywords: bone turnover biomarkers, metabolic syndrome, carotid artery plaques, carotid atherosclerosis, type 2 diabetes mellitus
Citation: Li W, Liu X, Liu L, Zhang L, Li M, Liu R, Li T, Chen E and Liu S (2022) Relationships of Serum Bone Turnover Markers With Metabolic Syndrome Components and Carotid Atherosclerosis in Patients With Type 2 Diabetes Mellitus. Front. Cardiovasc. Med. 9:824561. doi: 10.3389/fcvm.2022.824561
Received: 07 December 2021; Accepted: 31 March 2022;
Published: 25 April 2022.
Edited by:
Michelangela Barbieri, University of Campania Luigi Vanvitelli, ItalyReviewed by:
Maaike Schilperoort, Columbia University Irving Medical Center, United StatesCopyright © 2022 Li, Liu, Liu, Zhang, Li, Liu, Li, Chen and Liu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: En Chen, Y2hlbmVuZzM4MjFAc2luYS5jb20=; Shengyun Liu, ZmNjbGl1c3kyQHp6dS5lZHUuY24=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.