
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 25 January 2022
Sec. Lipids in Cardiovascular Disease
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.822626
 Huanqiang Li1,2†
Huanqiang Li1,2† Bo Wang1,2†
Bo Wang1,2† Ziling Mai1,2,3†
Ziling Mai1,2,3† Sijia Yu1,2,4†
Sijia Yu1,2,4† Ziyou Zhou1,2,5†
Ziyou Zhou1,2,5† Hongyu Lu1,2
Hongyu Lu1,2 Wenguang Lai1,2,3
Wenguang Lai1,2,3 Qiang Li1,2
Qiang Li1,2 Yongquan Yang1,2Jingru Deng1,2Ning Tan1,2,3,4,5Jiyan Chen1,2,3,4,5
Yongquan Yang1,2Jingru Deng1,2Ning Tan1,2,3,4,5Jiyan Chen1,2,3,4,5 Jin Liu1,2,3,4,5*
Jin Liu1,2,3,4,5* Yong Liu1,2,3,4,5*
Yong Liu1,2,3,4,5* Shiqun Chen1,2,3,4,5*
Shiqun Chen1,2,3,4,5*Background: Apolipoprotein B (ApoB) and low-density lipoprotein cholesterol (LDL-C) were identified targets for blood lipid management among coronary artery disease (CAD) patients. However, previous studies reported an inverse correlation between baseline LDL-C concentration and clinical outcomes. This study aims to explore the definite association between baseline ApoB and long-term prognosis.
Methods: A total of 36,460 CAD patients admitted to Guangdong Provincial People's Hospital were enrolled and categorized into two groups: high ApoB (≥65 mg/dL) group and low ApoB (<65 mg/dL) group. The association between baseline ApoB and long-term all-cause mortality was evaluated by the Kaplan-Meier method, Cox regression analyses and restricted cubic splines.
Results: The overall mortality was 12.49% (n = 4,554) over a median follow-up period of 5.01 years. Patients with low baseline ApoB levels were paradoxically more likely to get a worse prognosis. There was no obvious difference in risk of long-term all-cause mortality when only adjusted for age, gender, and comorbidity (aHR: 1.07, 95% CI: 0.99–1.16). When CONUT and total bilirubin were adjusted, the risk of long-term all-cause mortality would reduce in the low-ApoB (<65 mg/dL) group (aHR: 0.86, 95% CI: 0.78–0.96). In the fully covariable-adjusted model, patients in the ApoB <65 mg/d group had a 10.00% lower risk of long-term all-cause mortality comparing to patients with ApoB ≥65 mg/dL (aHR: 0.90; 95% CI:0.81–0.99).
Conclusion: This study found a paradoxical association between baseline ApoB and long-term all-cause mortality. Malnutrition and bilirubin mainly mediate the ApoB paradox. Increased ApoB concentration remained linearly associated with an increased risk of long-term all-cause mortality.
It is a well-established association between dyslipidaemias with the occurrence of coronary artery disease (CAD) (1–3) and increased risk of adverse outcomes in CAD patients (4). Additionally, lipid lowing therapy has been proved to benefit CAD patients' prognosis (5–7). For dyslipidemia management, the ESC guideline recommended apolipoprotein B (ApoB) and low-density lipoprotein cholesterol (LDL-C) as the secondary and the primary target, respectively (8, 9). However, several previous studies repeatedly reported that hypercholesterolemia on admission with elevated baseline concentration of LDL-C was paradoxically associated with decreased risk of poor outcomes among CAD patients (10–15).
Moreover, ApoB is the major apolipoprotein and a resonable estimate of the atherogenic lipoprotein families including LDL-C. Usually, patients with higher plasma ApoB will accumulate lipids more and faster, leading to worse prognosis (8). Elevated ApoB can also increase the risk of CAD, even if LDL-C is at an average level (16). Furthermore, a previous study demonstrated that ApoB could better reflect risk of mortality than LDL-C level in patients treated with statin (17). However, few studies reported the association between baseline ApoB level on admission and long-term all-cause mortality.
Therefore, this study aims to elucidate the definite association between baseline ApoB level and risk of long-term all-cause death in patients complicated with CAD.
Our study cohort stemmed from a previous retrospective cohort of 88,938 patients with coronary angiography (CAG) and percutaneous coronary intervention (PCI) treatment at Guangdong Provincial People's Hospital from January 2007 to December 2018. (Clinicaltrials.gov NCT04407936). The diagnosis of CAD was the basic condition of the patients enrolled (N = 59,667) in the current study. Patients who met the following criteria were excluded:under 18 years of age (n = 19), previous myocardial infarction (n = 3922), pervious underwent percutaneous coronary intervention (n = 4,996), previous underwent coronary artery bypass grafting (n= 328), cancer (n = 659), missing the data of ApoB (n = 7,322), and lacking follow-up data about mortality (n = 5,961). Finally, 36,460 CAD patients without the conditions above were enrolled in the study (Figure 1). Guangdong Provincial People's Hospital approved the study proposal [No. GDREC2019555H(R1)]. The study was implemented following the Declaration of Helsinki.
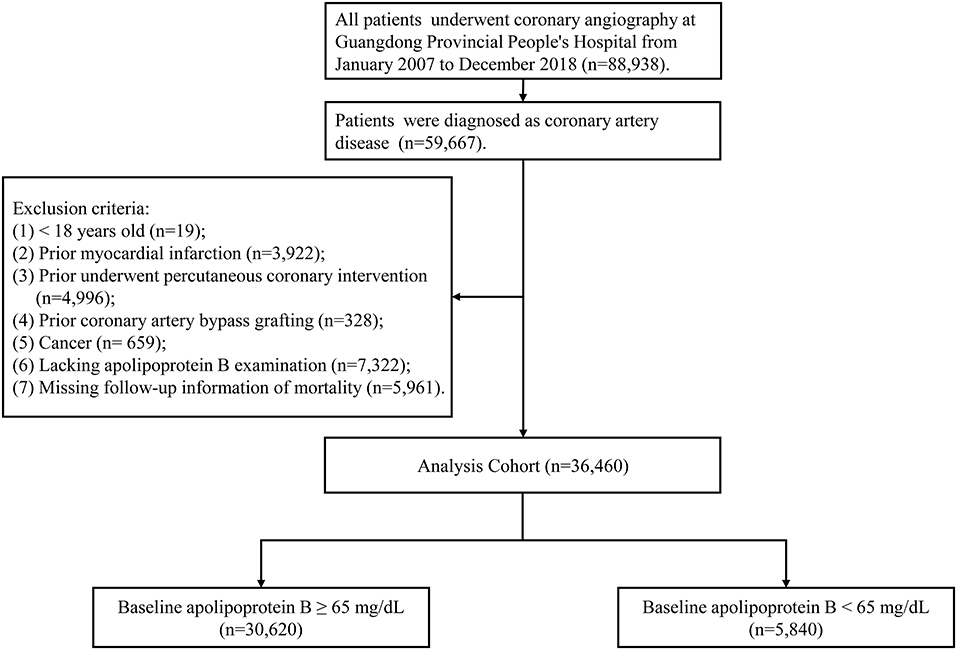
Figure 1. Study flow chart.
The data of this study came from the electronic medical record system. Baseline nutritional status data, coexistence conditions, demographic characteristics, laboratory examination, and medicine at discharge were collected. Blood samples were taken on admission for hematology and chemistry or collected before PCI/CAG, which obeyed standard clinical practice guidelines (18–20). Follow-up data on patient mortality was obtained and recorded from the Public Security system of Guangdong Province.
In this study, all-cause mortality during the study period was considered as the primary outcome. CAD was confirmed by CAG (defined as >50% stenosis in at least one vessel) and differentiated in the 10th Revision Codes of the International Classification of Diseases. Additionally, comorbidities consist of several diseases. CHF was defined as Killip class ≥2 or New York Heart Association class ≥3 (21). eGFR <60 ml/min per 1.73 m2 was defined as CKD (CKD stage 3 or worse) (22–24). According to the World Health Organization, anemia was defined as hematocrit <39% in males and 36% in females (25). Nutritional status was evaluated using the Controlled nutritional status (CONUT) scoring system. CONUT score is a comprehensive evaluation of serum albumin concentration, the total number of peripheral blood lymphocytes, and total cholesterol concentration. Different scores correspond to different nutritional status (0–1 is normal; 2–4 represents mild malnutrition; >4 for severe malnutrition) (26).
Referring to the concentration of ApoB, patients were categorized into two groups: a group with a high concentration of ApoB (≥65 mg/dL) and a group with a low concentration of ApoB (<65 mg/dL), following the ApoB goal attainment of 2019 ESC guidelines for dyslipidemia management (8). The categorical variables of descriptive statistics are expressed as quantity (percentage), the continuous variables of the normal distribution are expressed as mean [standard deviation (SD)], and the continuous variables of abnormal distribution are expressed as median [quartile range (IQR)]. Continuous and normally distributed variables were analyzed by independent sample Student t-test and Pearson chi-square tests for categorical ones. Kaplan-Meier method and log-rank t-test were selected to analyze the difference in survival between two groups. We conducted adjusted and unadjusted Cox proportional risk models to evaluate the link between apolipoprotein cholesterol levels and long-term all-cause mortality. We build a multivariate Cox regression model which incorporates baseline variables clinically relevant. In our study, we selected variables cautiously based on the given number of available events for assurance of the simplicity in the final model. We have successively constructed four models in turn, each of which has or has not been adjusted for concomitant variable: (1) univariate model; (2) adjusted age, gender, and complications including AMI, CHF, hypertension, diabetes mellitus, CKD, anemia, atrial fibrillation, COPD, and stroke; (3) adjusted nutritional status (CONUT) and total bilirubin; (4) adjusted for all covariates. The correlation between ApoB, nutritional status and total bilirubin were analyzed by using spearman analysis. We also constructed the restricted cubic spline curve based on the models above to evaluate the potential non-linear association between baseline ApoB levels and all-cause mortality. Furthermore, we additionally adjusted the use of statin for sensitivity analysis based on model 3 and model 4, respectively. Statistical analyses have been performed by using R software, version 3.6.3. Data would be considered statistically significant with an adjusted P < 0.05.
The final analysis consists of 36,460 CAD patients who met the criteria. Enrolled patients' baseline characteristics have been reported in Table 1. The average ages of patients with ApoB <65 mg/dL and the group of patients with ApoB ≥ 65 mg/dL were 64.50 years and 62.65 years, respectively. Patients with ApoB <65 mg/dL were more likely to develop comorbidities, worse nutrition status, and higher total bilirubin than patients with ApoB ≥65 mg/dL.
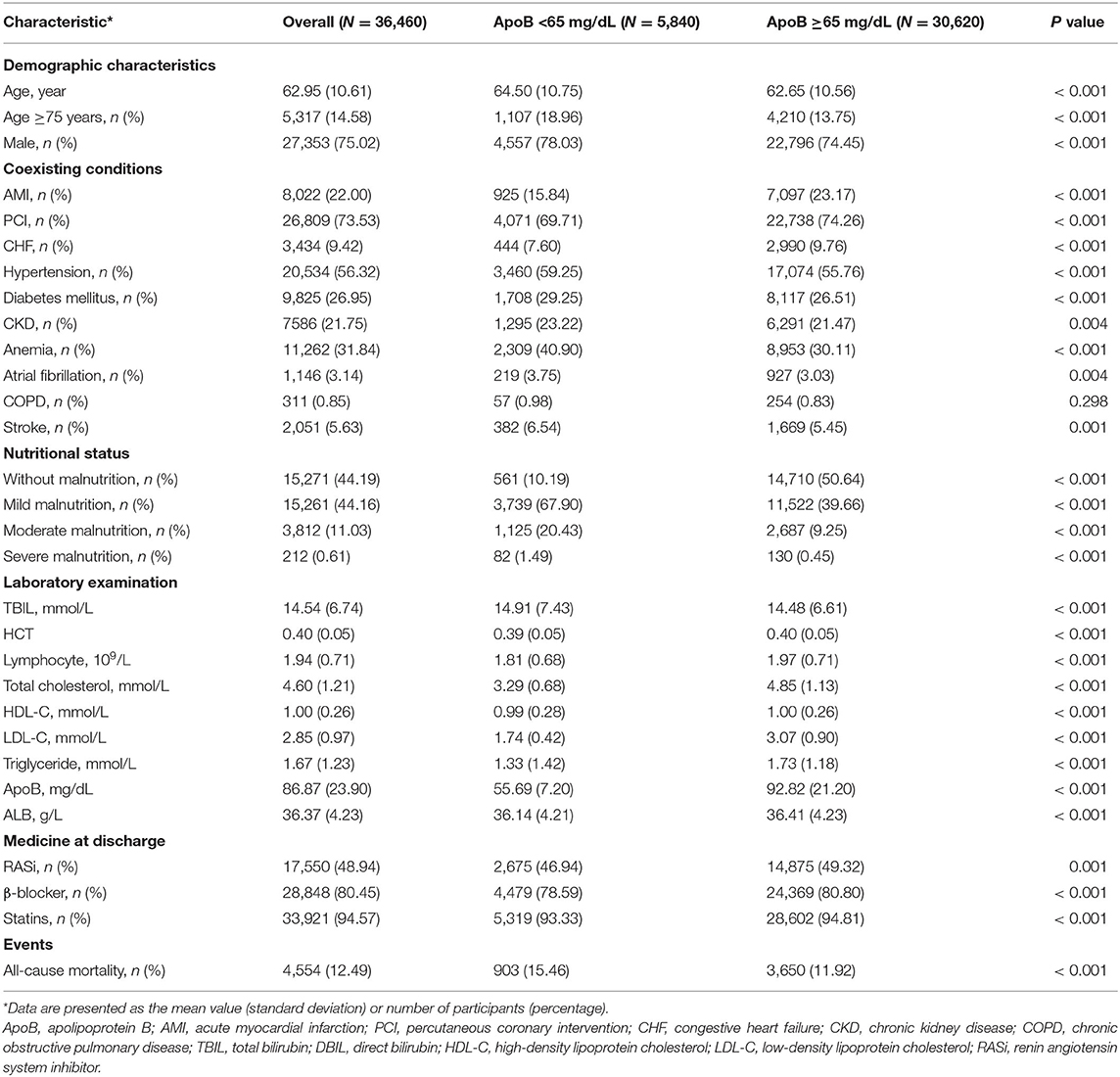
Table 1. Baseline characteristics.
During the whole follow-up period with a median time of 5.01 years (IQR 2.96–7.65), The all-cause mortality rate of the patients surveyed was 12.49% (n = 4,553). Kaplan-Meier analysis indicated the phenomenon that patients with low ApoB (<65 mg/dL) had a worse prognosis (Figure 2).
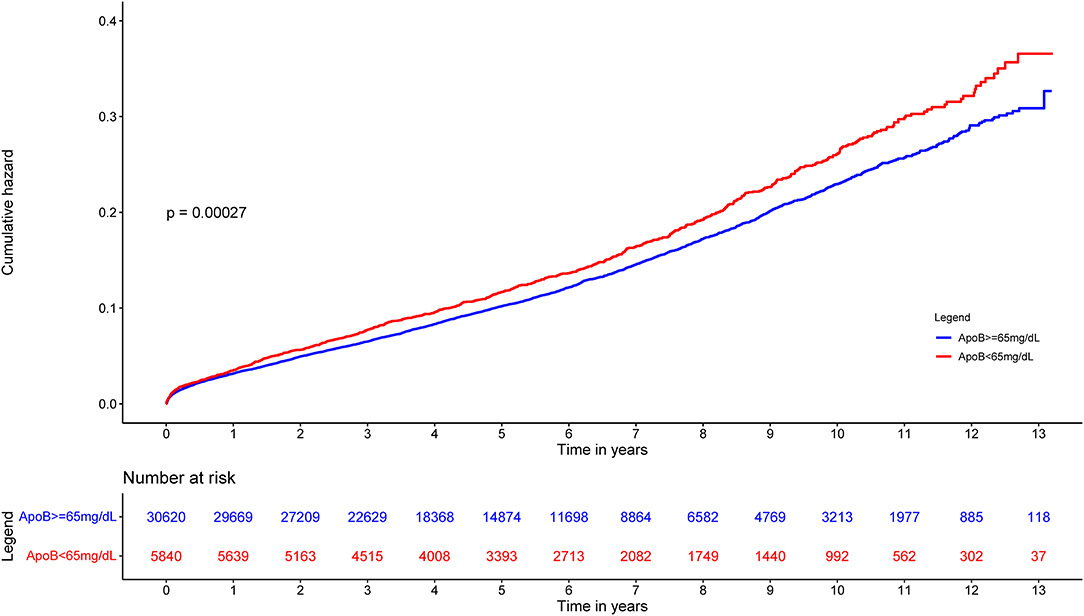
Figure 2. Cumulative incidence of all-cause death for ApoB <65 mg/dL group vs. ApoB ≥65 mg/dL group in CAD patients.
The correlations between ApoB and total bilirubin, nutritional status evaluated by CONUT score and components of CONUT score were shown in (Figure 3). ApoB did not show a significant correlation with total bilirubin (r = −0.023, p < 0.001) and no strong correlation between ApoB and nutritional status which was evaluated by CONUT score (r = −0.38, p < 0.001).
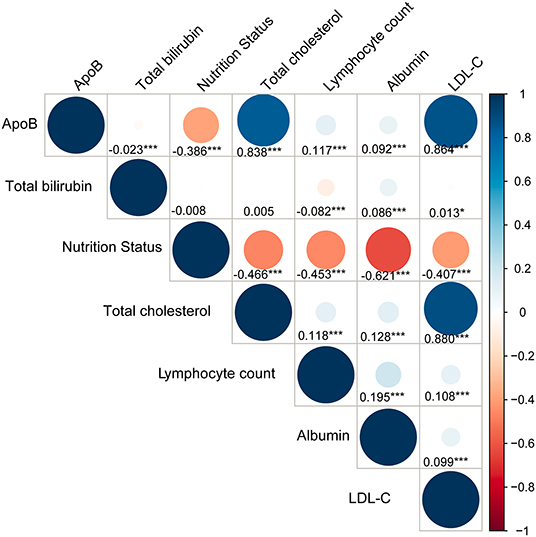
Figure 3. Correlations between ApoB, total bilirubin, nutritional status and its components. Nutritional status is assessed by Controlling Nutritional Status (CONUT) score. Total cholesterol, lymphocyte count and albumin are components of CONUT score. p < 0.05 *; p < 0.01**; p < 0.001***.
Univariate Cox regression model shows that low baseline concentration of ApoB (<65 mg/dL) is associated with a high risk of long-term all-cause mortality in CAD patients. (HR: 1.15, 95% CI: 1.06–1.23, Figure 4) Multivariate Cox regression analyses were then performed to adjust for confounding factors between patients with low ApoB (<65 mg/dL) and patients with high ApoB levels (≥65 mg/dL) (Figure 4). After adjusting for age, gender, and comorbidity (model 2), there was no obvious difference in long-term all-cause mortality between patients with low ApoB (<65 mg/dL) and patients with high ApoB levels (≥65 mg/dL) (aHR: 1.07, 95% CI: 0.99–1.16, Figure 4). Nevertheless, when CONUT and total bilirubin (model 3) were adjusted, the risk of long-term all-cause mortality would reduce for the patients with low-ApoB (<65 mg/dL) (aHR: 0.86, 95% CI: 0.78–0.96, Figure 4). In the fully covariable-adjusted model (model 4), patients with the baseline ApoB <65 mg/dL had a 10.00% lower risk of long-term all-cause death when comparing to patients with ApoB ≥65 mg/dL (aHR: 0.90; 95% CI:0.81–0.99, Figure 4).
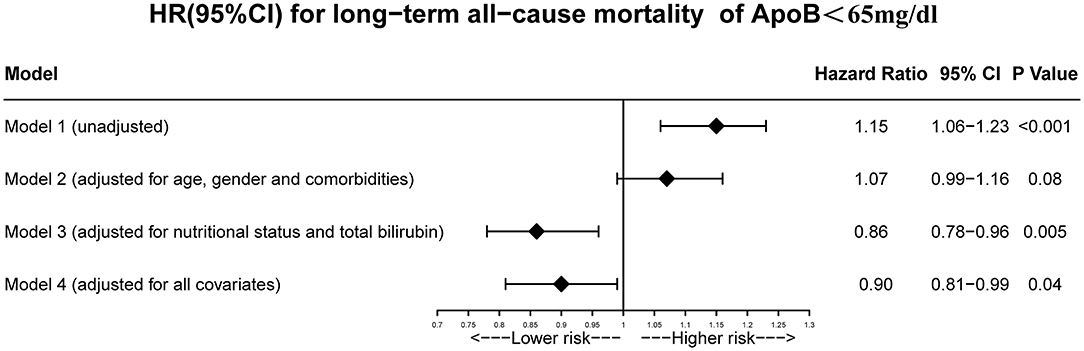
Figure 4. Unadjusted and adjusted HRs and 95% CIs for the primary end point (long-term all-cause mortality) of ApoB <65 mg/dL group vs. ApoB ≥65 mg/dL group in CAD patients. Model 1: Unadjusted model. Model 2: Adjusted for age ≥75 years, sex, PCI and comorbidities including AMI, CHF, hypertension, diabetes mellitus, CKD, anemia, atrial fibrillation, COPD and stroke. Model 3: Adjusted for malnutrition. Model 4: Adjusted for all covariates: age ≥75 years, sex, PCI and comorbidities including AMI, CHF, hypertension, diabetes mellitus, CKD, anemia, atrial fibrillation, COPD, stroke and malnutrition.
According to the results of restricted cubic splines, a J-shaped association existed in the univariable model (p for non-linearity = 0.006, Figure 5A) and a U-shaped association existed in the multivariable model adjusting age, gender and comorbidities (p for non-linearity = 0.009, Figure 5B). When CONUT and total bilirubin were adjusted, a linear association existed between baseline ApoB and the risk of long-term all-cause mortality (p for non-linearity = 0.62, Figure 5C; p for non-linearity = 0.80, Figure 5D).
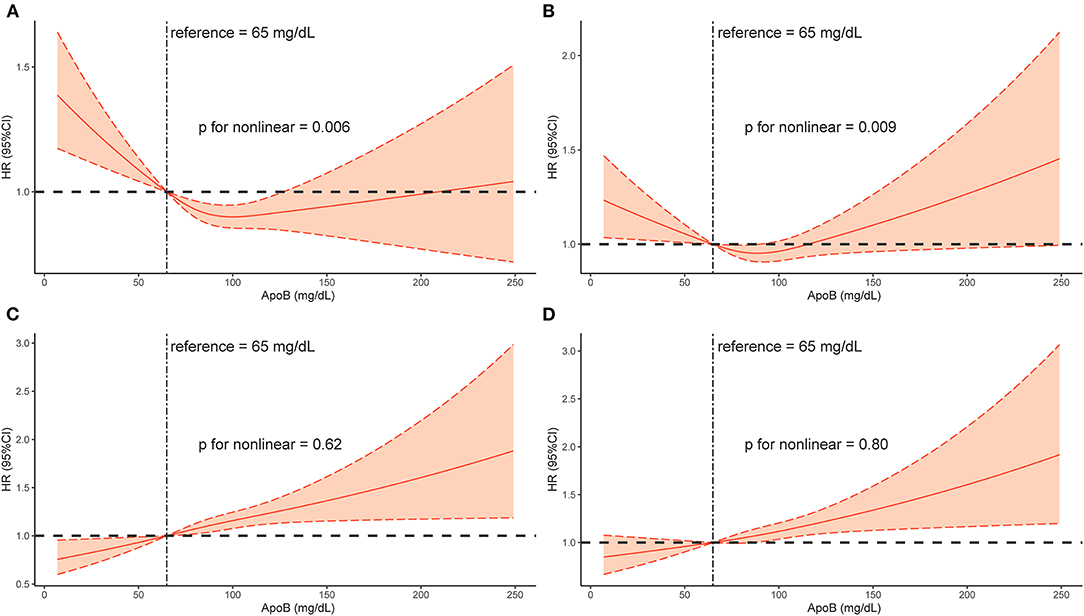
Figure 5. Restricted spline curve of the Baseline ApoB hazard ratio for mortality (long-term all-cause mortality) in CAD patients. (A): Model 1, Unadjusted model. (B): Model 2, Adjusted for age ≥75 years, sex, PCI and comorbidities including AMI, CHF, hypertension, diabetes mellitus, CKD, anemia, atrial fibrillation, COPD and stroke. (C): Model 3, Adjusted for malnutrition. (D): Model 4, Adjusted for all covariates: age ≥75 years, sex, PCI and comorbidities including AMI, CHF, hypertension, diabetes mellitus, CKD, anemia, atrial fibrillation, COPD, stroke and malnutrition.
After additional adjustment for the use of statin, the results of Cox regression and restricted cubic splines did not change significantly (Supplementary Figures 1, 2).
To the best of our knowledge, no previous study has demonstrated the relationship between long-term all-cause mortality and baseline serum ApoB concentration in CAD patients. According to the Kaplan-Meier curve, there is a paradoxical association between baseline ApoB concentration and long-term prognosis, in which low baseline ApoB was associated with a high risk of poor outcomes. After considering the baseline discrepancies including age, sex, and comorbidities, the association between low ApoB level and worse prognosis was insignificant. Taking nutrition status and total bilirubin level into consideration, high baseline serum concentration of ApoB was one of the factors which can affect long-term all-cause mortality independently. The apolipoprotein paradox has been observed in CAD patients, but it would no longer exist by taking the effects of malnutrition and bilirubin into account. The paradoxical association between ApoB and worse prognosis was mainly mediated by the effect of bilirubin and underlying malnutrition.
According to our findings, baseline plasma apolipoprotein B levels were negatively associated with long-term prognosis in unadjusted analysis. Although no previous studies have reported similar phenomena, previous studies have reported paradoxical relations between baseline LDLC level and long-term prognosis (10–14). Additionally, ApoB is highly correlated with LDLC (27). These previous studies illustrated that baseline confounders caused the cholesterol paradox of LDL-C. Cho et al. found AMI patients owing lower LDL-C levels (<1.8 mmol/L) on admission would be prone to have higher mortality in crude short-term (10). Meanwhile, patients in the lower LDL-C group were older and had a higher proportion of comorbidities. After adjusting for covariates, the level of LDL-C was not correlated strongly to short-term mortality. Another study conducted by Wang et al. showed that ACS patients' low baseline LDL-C concentration will increase the risk of mortality among hospitalized patients (10). Similarly, after adjustment for baseline confounders, the paradoxical association disappeared, and no apparent relationship between LDL-C levels and in-hospital mortality. The other three trials showed that the reduction of baseline LDL-C concentration was correlated to the increase of mortality in unadjusted and adjusted models (12–14).
All of these studies have found a paradoxical relationship between hyperlipidemia and well-prognosis, but these studies have not found causes for the phenomenon. A study conducted by Wallner et al. indicated that lipid profile would be altered in hyperbilirubinemia patients, characterized by a lower ApoB and LDL-C (28). Previous studies also demonstrated that the bilirubin concentration was negatively associated with LDL-C level (29, 30), and ApoB was the primary structural protein of low-density lipoprotein (LDL) (31). Moreover, increased bilirubin level was associated with an increased risk of poor prognosis (32–34). An observational study retrospectively recruited 3013 patients with AMI conducted by Huang et al. suggesting a positive correlation between serum total bilirubin concentration and short-term mortality among AMI patients (32). In another observational study including 1,167 patients with STEMI who underwent PCI, Baumann et al. found that high levels of total bilirubin (≥12 mg/L) were associated with a 128% increased risk of major adverse cardiac events (MACEs) during hospitalization (33). In addition, Wu et al. demonstrated that for patients with severe systolic heart failure, patients with higher bilirubin levels had conspicuously higher all-cause mortality (34). Since there was a tight connection between ApoB and total cholesterol, which is an evaluation index for nutritional status (26, 27), low ApoB may also indicate potential malnutrition. The CONUT score is an effective and objective tool to assess patients' nutritional status in hospital (26, 35). Roubín et al., Wada et al., and Chen et al. found that the nutritional status obtained by CONUT score can be considered one of the indicators to predict the long-term clinical outcomes of CAD patients (35–37).
Several reasons may explain the result of the present study. Firstly, according to the baseline, patients with low levels of ApoB (<65 mg/dL) were more elderly and complicated with more comorbidities. These confounders were highly associated with poor prognosis. Compared with patients having high levels of ApoB (≥65 mg/dL), patients with low ApoB (<65 mg/dL) had higher prevalence of elderly patients (18.96 vs. 13.75%), hypertension (59.25 vs. 55.76), CKD (23.22 vs. 21.47%), diabetes mellitus (29.25 vs. 26.51%) and anemia (40.90 vs. 30.11%). Thus, our study constructed model 2 in Cox regression which adjusted for age, male, and comorbidities. The results showed baseline ApoB concentration was not relevant to long-term all-cause mortality when taking age, male, and comorbidities into account. Secondly, patients with ApoB <65 mg/dL had higher bilirubin which was associated with worse prognosis. Bilirubin, the ultimate breakdown of hemoglobin, is an endogenous antioxidant with anti-inflammatory properties (38). On the one hand, as a strong antioxidant, bilirubin can inhibit the generation of atherogenic lipid such as oxidized-LDL. It may directly affect lipid metabolism through several pathways, including hepatic very-low-density lipoprotein (VLDL) assembly and cholesterol synthesis, bile cholesterol excretion, and intestinal cholesterol transport (39, 40). Meanwhile, ApoB is a direct measure of circulating numbers of atherogenic lipoproteins and is the main apolipoprotein of cholesterol within LDL, VLDL, and intermediate-density lipoprotein (IDL) particles (27, 41, 42). Thus, it is not surprising that bilirubin was negatively associated with ApoB. On the other hand, serum bilirubin concentration was a sign of heme oxygenase 1 (HO-1) enzyme activity which could be induced by stress, including as part of the acute phase response and complicated artery condition (43–45). Previous studies found that increased levels of serum bilirubin were associated with increased risk of adverse clinical outcomes among patients complicated with cardiovascular disease (46–48). Thirdly, patients with ApoB <65 mg/dL were at poorer nutritional status. In the present study, the prevalence of mild, moderate, severe malnutrition in the low ApoB group (<65 mg/dL) was 67.90, 20.43, and 1.49%, respectively. While, it was 39.66, 9.25, and 0.45% in high ApoB group (≥65 mg/dL), respectively. Evidence is emerging that malnutrition also often represents secondary immune dysfunction (49). Unrecognized malnutrition may cause susceptibility to infection and increase morbidity and mortality. Based on the above literatures, malnutrition and increased bilirubin level were highly associated with increased risk of poor long-term outcomes. The result of model 3 (adjusted for nutrition state, bilirubin) and model 4 (adjusted for all covariates including nutrition state, bilirubin) illustrated a normal association between baseline ApoB concentration and long-term all-cause death.
Lipid management is one of the critical points of secondary prevention in patients with CAD. Well-controlled lipid levels can significantly improve the long-term prognosis of CAD patients. ApoB as the secondary target should be paid attention to risk stratification. All these findings strongly support that physicians also need to incorporate malnutrition identification and bilirubin examination into their daily practice.
Several limitations should be considered. Firstly, the data of the present study was a single-center observational study from China. However, the data of the present study was from a large real-world cohort. Secondly, the data of the included patients were limited, and information such as body weight, BMI, waist circumference, and obesity that might be helpful to evaluate the nutritional status of the patients was missing comprehensively. To compensate for this, we chose the CONUT score based on laboratory examination as a tool to assess nutritional status, which may also help us perform an objective appraisal on patients about their nutritional status. Thirdly, this study only enrolled the ApoB values collected from the patients on admission, making it tougher to evaluate the effect of changes in ApoB levels on clinical endpoints during follow-up. In summary, our study mainly focuses on the clinical importance of baseline ApoB level on prognosis among CAD patients.
Among CAD patients, there is a paradoxical association between baseline ApoB concentration on admission and the risk of all-cause mortality. Nutrition state and bilirubin levels mediate this abnormal association. Conversely, after considering these two factors, evaluated ApoB concentration remains associated with a worse prognosis.
The original contributions presented in the study are included in the article/Supplementary Materials, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by Research Ethics Committee of Guangdong Provincial People's Hospital, Guangdong Academy of Medical Sciences (No. GDREC2019555H[R1]). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
HLi, BW, and SC: substantial contributions to the conception and design of the study. ZM, SY, ZZ, WL, QL, and HLu: data collection. SC, YL, JC, YY, JD, JL, and NT: data analysis and/or interpretation of data for the work. HLi, BW, ZM, SY, SC, QL, YY, JD, JL, YL, and JC: drafting of the work or revising it critically for important intellectual content. All authors approved the final version to the manuscript published.
This study was supported by the National Natural Science Foundation of China (Grant Nos. 81670339 and 81970311), Beijing Lisheng Cardiovascular Health Foundation (LHJJ20141751), National Key Research and Development Program of China (Grant No. 2016YFC1301202), and Guangdong Provincial People's Hospital Dengfeng Project Fund (DFJH201919 and DFJH2020026).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.822626/full#supplementary-material
Supplementary Figure 1. Unadjusted and adjusted HRs and 95% CIs for the primary end point (long-term all-cause mortality) of ApoB <65 mg/dL group vs. ApoB ≥65 mg/dL group in CAD patients. Model 1: Unadjusted model. Model 2: Adjusted for age ≥75 years, sex, PCI and comorbidities including AMI, CHF, hypertension, diabetes mellitus, CKD, anemia, atrial fibrillation, COPD, stroke and the use of stain. Model 3: Adjusted for malnutrition. Model 4: Adjusted for all covariates: age ≥75 years, sex, PCI and comorbidities including AMI, CHF, hypertension, diabetes mellitus, CKD, anemia, atrial fibrillation, COPD, stroke, malnutrition and the use of stain.
Supplementary Figure 2. Restricted spline curve of the Baseline ApoB hazard ratio for mortality (long-term all-cause mortality) in CAD patients. (A): Model 1, Unadjusted model. (B): Model 2, Adjusted for age ≥75 years, sex, PCI and comorbidities including AMI, CHF, hypertension, diabetes mellitus, CKD, anemia, atrial fibrillation, COPD, stroke and the use of stain. (C): Model 3, Adjusted for malnutrition. (D): Model 4, Adjusted for all covariates: age ≥ 75 years, sex, PCI and comorbidities including AMI, CHF, hypertension, diabetes mellitus, CKD, anemia, atrial fibrillation, COPD, stroke, malnutrition and the use of stain.
1. Kastelein JJ, van der Steeg WA, Holme I, Gaffney M, Cater NB, Barter P, et al. Lipids, apolipoproteins, and their ratios in relation to cardiovascular events with statin treatment. Circulation. (2008) 11723:3002–9. doi: 10.1161/CIRCULATIONAHA.107.713438
2. Boekholdt SM, Arsenault BJ, Mora S, Pedersen TR, LaRosa JC, Nestel PJ, et al. Association of LDL cholesterol, non-HDL cholesterol, and apolipoprotein B levels with risk of cardiovascular events among patients treated with statins: a meta-analysis. JAMA. (2012) 30712:1302–9. doi: 10.1001/jama.2012.366
3. Thanassoulis G, Williams K, Ye K, Brook R, Couture P, Lawler PR, et al. Relations of change in plasma levels of LDL-C, non-HDL-C and apoB with risk reduction from statin therapy: a meta-analysis of randomized trials. J Am Heart Assoc. (2014) 32:e000759. doi: 10.1161/JAHA.113.000759
4. Reiner Z, Catapano AL, De Backer G, Graham I, Taskinen MR, Wiklund O, et al. ESC/EAS Guidelines for the management of dyslipidaemias: the task force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J. (2011) 3214:1769–818. doi: 10.1016/j.atherosclerosis.2011.06.011
5. Baigent C, Blackwell L, Emberson J, Holland LE, Reith C, Bhala N, et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. (2010) 3769753:1670–81. doi: 10.1016/S0140-6736(10)61350-5
6. Schwartz GG, Steg PG, Szarek M, Bhatt DL, Bittner VA, Diaz R, et al. Alirocumab and cardiovascular outcomes after acute coronary syndrome. N Engl J Med. (2018) 37922:2097–107. doi: 10.1056/NEJMoa1801174
7. Brugts JJ, Yetgin T, Hoeks SE, Gotto AM, Shepherd J, Westendorp RG, et al. The benefits of statins in people without established cardiovascular disease but with cardiovascular risk factors: meta-analysis of randomised controlled trials. BMJ. (2009) 338:b2376. doi: 10.1136/bmj.b2376
8. Mach F, Baigent C, Catapano AL, Koskinas KC, Casula M, Badimon L, et al. 2019 ESC/EAS guidelines for the management of dyslipidaemias: lipid modification to reduce cardiovascular risk. Eur Heart J. (2020) 411:111–88. doi: 10.1093/eurheartj/ehz455
9. Catapano AL, Graham I, De Backer G, Wiklund O, Chapman MJ, Drexel H, et al. 2016 ESC/EAS guidelines for the management of dyslipidaemias. Eur Heart J. (2016) 3739:2999–3058. doi: 10.1093/eurheartj/ehw272
10. Cho KH, Jeong MH, Ahn Y, Kim YJ, Chae SC, Hong TJ, et al. Low-density lipoprotein cholesterol level in patients with acute myocardial infarction having percutaneous coronary intervention (the cholesterol paradox). Am J Cardiol. (2010) 1068:1061–8. doi: 10.1016/j.amjcard.2010.06.009
11. Wang TY, Newby LK, Chen AY, Mulgund J, Roe MT, Sonel AF, et al. Hypercholesterolemia paradox in relation to mortality in acute coronary syndrome. Clin Cardiol. (2009) 329:E22–28. doi: 10.1002/clc.20518
12. Al-Mallah MH, Hatahet H, Cavalcante JL, Khanal S. Low admission LDL-cholesterol is associated with increased 3-year all-cause mortality in patients with non ST segment elevation myocardial infarction. Cardiol J. (2009) 163:227–33. Available online at: https://pubmed.ncbi.nlm.nih.gov/19437396/
13. Reddy VS, Bui QT, Jacobs JR, Begelman SM, Miller DP, French WJ. Relationship between serum low-density lipoprotein cholesterol and in-hospital mortality following acute myocardial infarction (the lipid paradox). Am J Cardiol. (2015) 1155:557–62. doi: 10.1016/j.amjcard.2014.12.006
14. Nakahashi T, Tada H, Sakata K, Yakuta Y, Tanaka Y, Nomura A, et al. Paradoxical impact of decreased low-density lipoprotein cholesterol level at baseline on the long-term prognosis in patients with acute coronary syndrome. Heart Vessels. (2018) 337:695–705. doi: 10.1007/s00380-017-1111-3
15. Wang B, Liu J, Chen S, Ying M, Chen G, Liu L, et al. Malnutrition affects cholesterol paradox in coronary artery disease: a 41,229 Chinese cohort study. Lipids Health Dis. (2021) 201:36. doi: 10.1186/s12944-021-01460-6
16. Williams K, Sniderman AD, Sattar N, D'Agostino R Jr, Wagenknecht LE, Haffner SM. Comparison of the associations of apolipoprotein B and low-density lipoprotein cholesterol with other cardiovascular risk factors in the Insulin Resistance Atherosclerosis Study (IRAS). Circulation. (2003) 10819:2312–6. doi: 10.1161/01.CIR.0000097113.11419.9E
17. Johannesen CDL, Mortensen MB, Langsted A, Nordestgaard BG. Apolipoprotein B. and Non-HDL cholesterol better reflect residual risk than LDL cholesterol in statin-treated patients. J Am Coll Cardiol. (2021) 7711:1439–50. doi: 10.1016/j.jacc.2021.01.027
18. Kushner FG, Hand M, Smith SC Jr, King SB 3rd, Anderson JL, Antman EM, et al. 2009 focused updates: ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction (updating the 2004 guideline and 2007 focused update) and ACC/AHA/SCAI guidelines on percutaneous coronary intervention (updating the 2005 guideline and 2007 focused update) a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. (2009) 5423:2205-41. doi: 10.1016/j.jacc.2009.10.015
19. Jneid H, Anderson JL, Wright RS, Adams CD, Bridges CR, Casey DE Jr, et al. 2012 ACCF/AHA focused update of the guideline for the management of patients with unstable angina/non-ST-elevation myocardial infarction (updating the 2007 guideline and replacing the 2011 focused update): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. (2012) 607:645–81. doi: 10.1016/j.jacc.2012.06.004
20. Levine GN, Bates ER, Blankenship JC, Bailey SR, Bittl JA, Cercek B, et al. 2015 ACC/AHA/SCAI focused update on primary percutaneous coronary intervention for patients with st-elevation myocardial infarction: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction. J Am Coll Cardiol. (2016) 6710:1235–50. doi: 10.1016/j.jacc.2015.10.005
21. Mehran R, Aymong ED, Nikolsky E, Lasic Z, Iakovou I, Fahy M, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. (2004) 447:1393–9. doi: 10.1016/S0735-1097(04)01445-7
22. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation. Modification of Diet in Renal Disease Study Group. Ann Intern Med. (1999) 1306:461–70. doi: 10.7326/0003-4819-130-6-199903160-00002
23. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis. (2002) 392(Suppl. 1):S1–266.
24. Manjunath G, Tighiouart H, Ibrahim H, MacLeod B, Salem DN, Griffith JL, et al. Level of kidney function as a risk factor for atherosclerotic cardiovascular outcomes in the community. J Am Coll Cardiol. (2003) 411:47–55. doi: 10.1016/S0735-1097(02)02663-3
25. Nutritional anaemias. Report of a WHO scientific group. World Health Organ Tech Rep Ser. (1968) 405:5–37.
26. Ignacio de Ulíbarri J, González-Madroño A, de Villar NG, González P, González B, Mancha A, et al. CONUT: a tool for controlling nutritional status first validation in a hospital population. Nutr Hosp. (2005) 201:38–45.
27. Welsh C, Celis-Morales CA, Brown R, Mackay DF, Lewsey J, Mark PB, et al. Comparison of conventional lipoprotein tests and apolipoproteins in the prediction of cardiovascular disease. Circulation. (2019) 1407:542–52. doi: 10.1161/CIRCULATIONAHA.119.041149
28. Wallner M, Marculescu R, Doberer D, Wolzt M, Wagner O, Vitek L, et al. Protection from age-related increase in lipid biomarkers and inflammation contributes to cardiovascular protection in Gilbert's syndrome. Clin Sci. (2013) 1255:257–64. doi: 10.1042/CS20120661
29. Nascimento H, Alves AI, Coimbra S, Catarino C, Gomes D, Bronze-da-Rocha E, et al. Bilirubin is independently associated with oxidized LDL levels in young obese patients. Diabetol Metab Syndr. (2015) 7:4. doi: 10.1186/1758-5996-7-4
30. Dullaart RP, de Vries R, Lefrandt JD. Increased large VLDL and small LDL particles are related to lower bilirubin in Type 2 diabetes mellitus. Clin Biochem. (2014) 47:170–5. doi: 10.1016/j.clinbiochem.2014.08.008
31. Bell DA, Hooper AJ, Burnett JR. Mipomersen, an antisense apolipoprotein B synthesis inhibitor. Expert Opin Investig Drugs. (2011) 202:265–72. doi: 10.1517/13543784.2011.547471
32. Huang FY, Peng Y, Huang BT, Yang Y, Pu XB, Chen SJ, et al. The correlation between serum total bilirubin and outcomes in patients with different subtypes of coronary artery disease. Clin Chim Acta. (2017) 465:101–5. doi: 10.1016/j.cca.2016.12.020
33. Baumann S, Huseynov A, Koepp J, Jabbour C, Behnes M, Becher T, et al. Comparison of serum uric acid, bilirubin, and C-reactive protein as prognostic biomarkers of in-hospital MACE between women and men with ST-segment elevation myocardial infarction. Angiology. (2016) 673:272–80. doi: 10.1177/0003319715589246
34. Wu AH, Levy WC, Welch KB, Neuberg GW, O'Connor CM, Carson PE, et al. Association between bilirubin and mode of death in severe systolic heart failure. Am J Cardiol. (2013) 1118:1192–7. doi: 10.1016/j.amjcard.2012.12.048
35. Chen SC, Yang YL, Wu CH, Huang SS, Chan WL, Lin SJ, et al. Association between preoperative nutritional status and clinical outcomes of patients with coronary artery disease undergoing percutaneous coronary intervention. Nutrients. (2020) 12:1295. doi: 10.3390/nu12051295
36. Raposeiras Roubín S, Abu Assi E, Cespón Fernandez M, Barreiro Pardal C, Lizancos Castro A, Parada JA, et al. Prevalence and prognostic significance of malnutrition in patients with acute coronary syndrome. J Am Coll Cardiol. (2020) 767:828–40. doi: 10.1016/j.jacc.2020.06.058
37. Wada H, Dohi T, Miyauchi K, Doi S, Konishi H, Naito R, et al. Prognostic impact of nutritional status assessed by the controlling nutritional status score in patients with stable coronary artery disease undergoing percutaneous coronary intervention. Clin Res Cardiol. (2017) 10611:875–83. doi: 10.1007/s00392-017-1132-z
38. Li XH, Lin HY, Guan LY, Peng H, Wen MM, Cao YQ, et al. Direct bilirubin levels and risk of metabolic syndrome in healthy chinese men. Biomed Res Int. (2017) 2017:9621615. doi: 10.1155/2017/9621615
39. Jansen T, Hortmann M, Oelze M, Opitz B, Steven S, Schell R, et al. Conversion of biliverdin to bilirubin by biliverdin reductase contributes to endothelial cell protection by heme oxygenase-1-evidence for direct and indirect antioxidant actions of bilirubin. J Mol Cell Cardiol. (2010) 492:186–95. doi: 10.1016/j.yjmcc.2010.04.011
40. Bulmer AC, Verkade HJ, Wagner KH. Bilirubin and beyond: a review of lipid status in Gilbert's syndrome and its relevance to cardiovascular disease protection. Prog Lipid Res. (2013) 522:193–205. doi: 10.1016/j.plipres.2012.11.001
41. Wilkins JT, Li RC, Sniderman A, Chan C, Lloyd-Jones DM. Discordance between apolipoprotein B and LDL-cholesterol in young adults predicts coronary artery calcification: the CARDIA study. J Am Coll Cardiol. (2016) 672:193–201. doi: 10.1016/j.jacc.2015.10.055
42. Langlois MR, Sniderman AD. Non-HDL Cholesterol or apoB: which to prefer as a target for the prevention of atherosclerotic cardiovascular disease? Curr Cardiol Rep. (2020) 228:67. doi: 10.1007/s11886-020-01323-z
43. Breimer LH, Mikhailidis DP. Could carbon monoxide and bilirubin be friends as well as foes of the body? Scand J Clin Lab Invest. (2010) 701:1–5. doi: 10.3109/00365510903494252
44. Mito S, Ozono R, Oshima T, Yano Y, Watari Y, Yamamoto Y, et al. Myocardial protection against pressure overload in mice lacking Bach1, a transcriptional repressor of heme oxygenase-1. Hypertension. (2008) 516:1570–7. doi: 10.1161/HYPERTENSIONAHA.107.102566
45. Okuhara K, Kisaka T, Ozono R, Kurisu S, Inoue I, Soga J, et al. Change in bilirubin level following acute myocardial infarction is an index for heme oxygenase activation. South Med J. (2010) 1039:876–81. doi: 10.1097/SMJ.0b013e3181eac06a
46. Ambrosy AP, Vaduganathan M, Huffman MD, Khan S, Kwasny MJ, Fought AJ, et al. Clinical course and predictive value of liver function tests in patients hospitalized for worsening heart failure with reduced ejection fraction: an analysis of the EVEREST trial. Eur J Heart Fail. (2012) 143:302–11. doi: 10.1093/eurjhf/hfs007
47. Matthews JC, Koelling TM, Pagani FD, Aaronson KD. The right ventricular failure risk score a pre-operative tool for assessing the risk of right ventricular failure in left ventricular assist device candidates. J Am Coll Cardiol. (2008) 5122:2163–72. doi: 10.1016/j.jacc.2008.03.009
48. Matthews JC, Pagani FD, Haft JW, Koelling TM, Naftel DC, Aaronson KD. Model for end-stage liver disease score predicts left ventricular assist device operative transfusion requirements, morbidity, and mortality. Circulation. (2010) 1212:214–20. doi: 10.1161/CIRCULATIONAHA.108.838656
Keywords: apolipoprotein B, coronary artery disease, long-term prognosis, all-cause mortality, paradox
Citation: Li H, Wang B, Mai Z, Yu S, Zhou Z, Lu H, Lai W, Li Q, Yang Y, Deng J, Tan N, Chen J, Liu J, Liu Y and Chen S (2022) Paradoxical Association Between Baseline Apolipoprotein B and Prognosis in Coronary Artery Disease: A 36,460 Chinese Cohort Study. Front. Cardiovasc. Med. 9:822626. doi: 10.3389/fcvm.2022.822626
Received: 26 November 2021; Accepted: 03 January 2022;
Published: 25 January 2022.
Edited by:
Marat V. Ezhov, Ministry of Health of the Russian Federation, RussiaReviewed by:
Robert Kiss, McGill University, CanadaCopyright © 2022 Li, Wang, Mai, Yu, Zhou, Lu, Lai, Li, Yang, Deng, Tan, Chen, Liu, Liu and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shiqun Chen, c2hpcXVuY2hlbkAxMjYuY29t; Yong Liu, bGl1eW9uZ0BnZHBoLm9yZy5jbg==; Jin Liu, bGphdzM5NzAxNzU2OEAxNjMuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.