 Yongjian Zhu
Yongjian Zhu Mingjing Liu2
Mingjing Liu2 Yacong Bo
Yacong Bo
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 07 March 2022
Sec. Hypertension
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.813244
Background: Exposure to ambient pollutants and chemicals were found to be associated with increased risk of hypertension. However, the relationship between the increased aldehyde exposure and hypertension are still unclear. This study aimed to investigate the potential associations of serum aldehydes levels with prevalent hypertension.
Methods: A total of 1,733 U.S. adults with data on hypertension outcome and serum aldehydes measurement from the National Health and Nutrition Examination Survey 2013–2014 were included. The serum levels of aldehydes were measured via an automated analytical method using solid phase microextraction gas chromatography and high-resolution mass spectrometry. Multivariate logistic regression models were adopted to assess the associations between six selected aldehydes exposure (benzaldehyde, butyraldehyde, heptanaldehyde, hexanaldehyde, isopentanaldehyde, and propanaldehyde) and prevalence of hypertension.
Results: The mean age was 48.0 ± 16.7 years and an approximately equivalent of sex distribution was observed (female 49.9%). There seems to be a numerically higher level of hexanaldehyde in participants with hypertension when compared to participants without hypertension (2.6 ± 3.9 ng/mL vs. 2.3 ± 1.1 ng/mL). After adjusting for potential confounders, the odds ratio (OR) for hypertension was 2.15 [95% confidence interval (CI): 1.33–3.51] in participants from the highest quartile of serum hexanaldehyde concentration in comparison to those from the lowest quartile. Subgroup analyses and sensitivity analyses showed generally similar results.
Conclusion: In summary, current evidence suggested that increased serum hexanaldehyde level was positively associated with prevalent hypertension in U.S. adults.
Hypertension is known to affect approximately one third of the world's adult population (1). As one of the most important risk factors for cardiovascular diseases and all-cause mortality (2), an estimated more than 7 million annual deaths are attributed to hypertension (3, 4). Epidemiological studies suggested that both genetic and environmental factors contribute to the development of this disorder. Cumulative evidences demonstrated that lifestyle interventions on modifiable risk factors of hypertension including obesity, dietary intakes, smoking, alcohol drinking, and physical activity, have been recognized as effective methods to reduce the morbidity and mortality (5–10). In recent years, exposure to certain ambient pollutants and chemicals were also found to be associated with increased risk of hypertension (11, 12).
Aldehydes are electrophilic organic compounds which include a number of particular components (13). The natural sources of aldehydes are various. Apart from aldehydes derived from environmental or occupational exposure, aldehydes are also generated by food heating and endogenous enzyme-dependent oxidation (14). In human, biogenic aldehydes are mainly from the peroxidation of sugars and lipids. In the past, the adverse health effects of aldehydes exposure and established diseases have been preliminarily investigated. Accumulation of aldehydes in the body aggregates the oxidative stress and covalent modification of protein, and were involved in the pathophysiology of aging related conditions including tumors, chronic liver and kidney diseases, and Alzheimer's disease (14–16). Under high levels of lipid and glucose oxidation, the cardiovascular systems are susceptible to the effects of endogenous aldehydes (17). Acrolein exposure has been shown to promote the development of systemic dyslipidemia, atherosclerosis and thrombosis (18). Serum acrolein and isopentanaldehyde levels were also demostrated to be positively associated with increased risk of cardiovascular diseases (19–21). However, the relationship between the serum levels of aldehydes and risk of hypertension is still unclear.
Therefore, based on data from the National Health and Nutrition Examination Survey (NHANES), this study was conducted to investigate the potential associations of serum aldehydes levels with prevalent hypertension in the U.S. adults.
NHANES has been conducted continuously since 1999 by the National Center for Health Statistics (NCHS) at the Centers for Disease Control and Prevention (CDC), which originated from the National Health Survey Act of 1956. This program aims to provide statistical information on the health and nutritional status of representative population in the U.S. by the means of a multistage, probability sampling survey1. Data collecting was performed using household interviews, self-reported questionnaire, physical examinations, and laboratory test. The NHANES data could be publicly accessed from the internet (https://www.cdc.gov/nchs/nhanes/index.htm). In this study, we initially included participants enrolled in 2013–2014 when aldehydes measurements were available (n = 10,175). Among them, 4,406 individuals aged <20 years old and 795 individuals with pregnant or unmeasured blood pressure were excluded. We further excluded 3,241 individuals because the levels of serum aldehydes were not analyzed. As a result, a total of 1,733 individuals were included in the final analysis. The flowchart of participants selection was shown in Figure 1. The NHANES protocol was approved by the NCHS Institutional Review Committee. All the participants provided written informed consent to authorize the use of data.
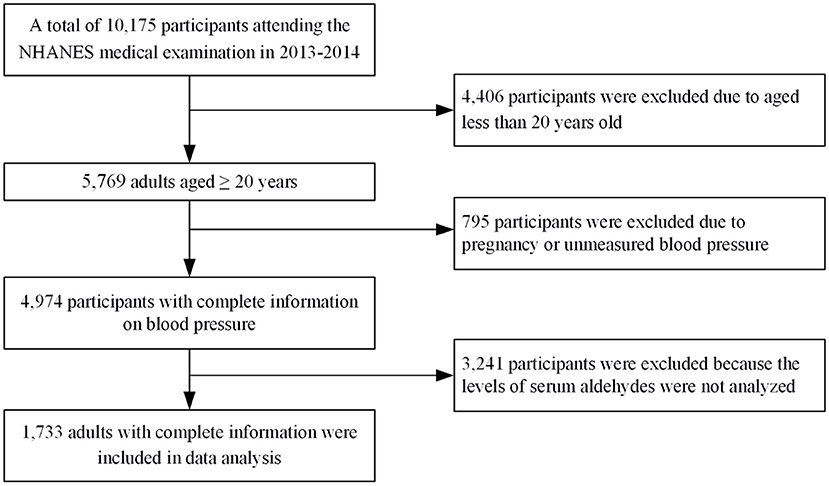
Figure 1. Flowchart of participant selection.
Blood pressure (BP) was measured by trained investigators using a standardized protocol. Before BP measurements in the mobile examination center, all participants were asked to rest quietly in a seated position for 5 min. Three consecutive blood pressure readings were obtained when the participants maximum inflation level had been determined. The mean values of the three readings was used to calculate the average BP. Participants were diagnosed as having hypertension if the average SBP was ≥ 140 mm Hg, or the average DBP ≥ 90 mm Hg, or their answer to the question “Are you now taking prescribed medicine for high blood pressure?” was “yes”.
Blood samples were collected in specially designed tubes and serum was separated using a microcentrifuge. Serum aldehydes were measured in a randomly selected one-third subsample of participants 12 years and older. Given that aldehydes tend to react with biological molecules to form various organic compounds including Schiff base protein adducts, free aldehydes that released into the headspace of biological samples from the Schiff base protein adducts at low pH (~3) were analyzed. The serum levels of aldehydes were measured via an automated analytical method using solid phase microextraction (SPME) gas chromatography (GC) and high-resolution mass spectrometry (HRMS). A detailed description regarding blood specimen sampling and detection procedures has been published elsewhere (22, 23). In human serum from NHANES, this analytical method quantitatively detects trace levels of 12 aldehydes (pentanaldehyde, propanaldehyde, octanaldehyde, o-toluenaldehyde, non-analdehyde, isopentanaldehyde, heptanaldehyde, hexanaldehyde, decanaldehyde, crotonaldehyde, benzaldehyde, and butyraldehyde). Among the group of 12 aldehydes, we selected 6 kinds of aldehydes which were detectable in more than 80% of NHANES participants, including benzaldehyde, butyraldehyde, heptanaldehyde, hexanaldehyde, isopentanaldehyde, and propanaldehyde. Values below the detection limit (LOD) of each aldehydes was replaced with the LOD divided by the square root of 2.
Covariates related to exposure or outcome were obtained and controlled in multivariate logistic regression. They were age, sex (male, female), race/ethnicity (non-Hispanic white, non-Hispanic black, Hispanic, non-Hispanic Asian, and other), body mass index (BMI), educational level (lower than high school, high school graduate or general equivalency diploma, some college or associate degree, and bachelor' s degree or above), self-reported history of cardiovascular diseases (congestive heart failure, coronary heart disease, angina/angina pectoris, heart attack, or stroke), diabetes status (self-reported diagnosis by a healthcare provider), smoking status (current, former, or never), alcohol use (yes or no), ratio of family income to poverty (≤1, 1–3, >3), and physical activity (inactive, insufficiently active, active). BMI was calculated as weight in kilograms divided by height in meters squared. Alcohol drinkers were defined as who consumed at least 12 drinks in the last 12 months. One drink was defined for NHANES participants as 12 ounces of beer, a 5-ounce glass of wine, or 1.5 ounces of liquor. Physical activity was classed to active group [defined as the product of the metabolic equivalent value (MET = 1 kcal/h per kilometer body weight) of 7.5 or more], insufficiently active group (defined as the product of the MET value ranging from 3.75 to 7.5), and inactive group (defined as the product of the MET value <3.75).
Continuous variables are summarized as the mean with standard deviation (SD), and categorical variables as the number with percentage. The serum levels of aldehydes were divided into quartiles using the lowest quartile as the reference group. Multivariate logistic regression models were adopted to evaluate the associations between aldehydes exposure and hypertension. Three models were developed to gradually adjust the confounders: model 1 was adjusted for age and sex; model 2 was further adjusted for education level, race, smoking, alcohol use, poverty income ratio, and physical activity; model 3 was further adjusted for BMI, diabetes, and cardiovascular disease. The shape of the concentration–response relationship between Aldehydes and hypertension were evaluated using generalized additive models through spline function.
Subgroup analyses were conducted to investigate whether these associations were modified by age, sex, education level, race, physical activity, alcohol use, smoking, diabetes, cardiovascular disease, and BMI. Additionally, two sensitivity analyses were conducted to further evaluate the robustness of study findings: (1) restricted to participants free of diabetes and cardiovascular disease; (2) used an alternative cut-off value of 130/80 mm Hg to define hypertension according to the 2017 AHA/ACA blood pressure guideline; (3) including participants aged 18–20 years old; (4) excluding participants reporting extreme total energy intakes (<850 or >4,000 kcal/day) (24) or currently breastfeeding a baby; (5) further adjusting for total energy intake and marital status. All statistical analyses were conducted using R version 4.0.2 (R Foundation for Statistical Computing, Vienna, Austria). A two-sided P-value of 0.05 or less was considered statistically significant.
Table 1 showed the general characteristics of study population. The mean age was 48.0 ± 16.7 years and an approximately equivalent of sex distribution was noted (female 49.9%, male 50.1%). The Non-Hispanic White was the most common ethnic type (49.1%). The prevalence of hypertension in included participants was 18.3%. Compared to individuals without hypertension, those with hypertension seem to be older, more likely to be Hispanic, drinkers. Additionally, the trends of a higher proportion of cardiovascular disease, inactive exercise, higher level of BMI and hexanaldehyde were also observed in individuals with hypertension.
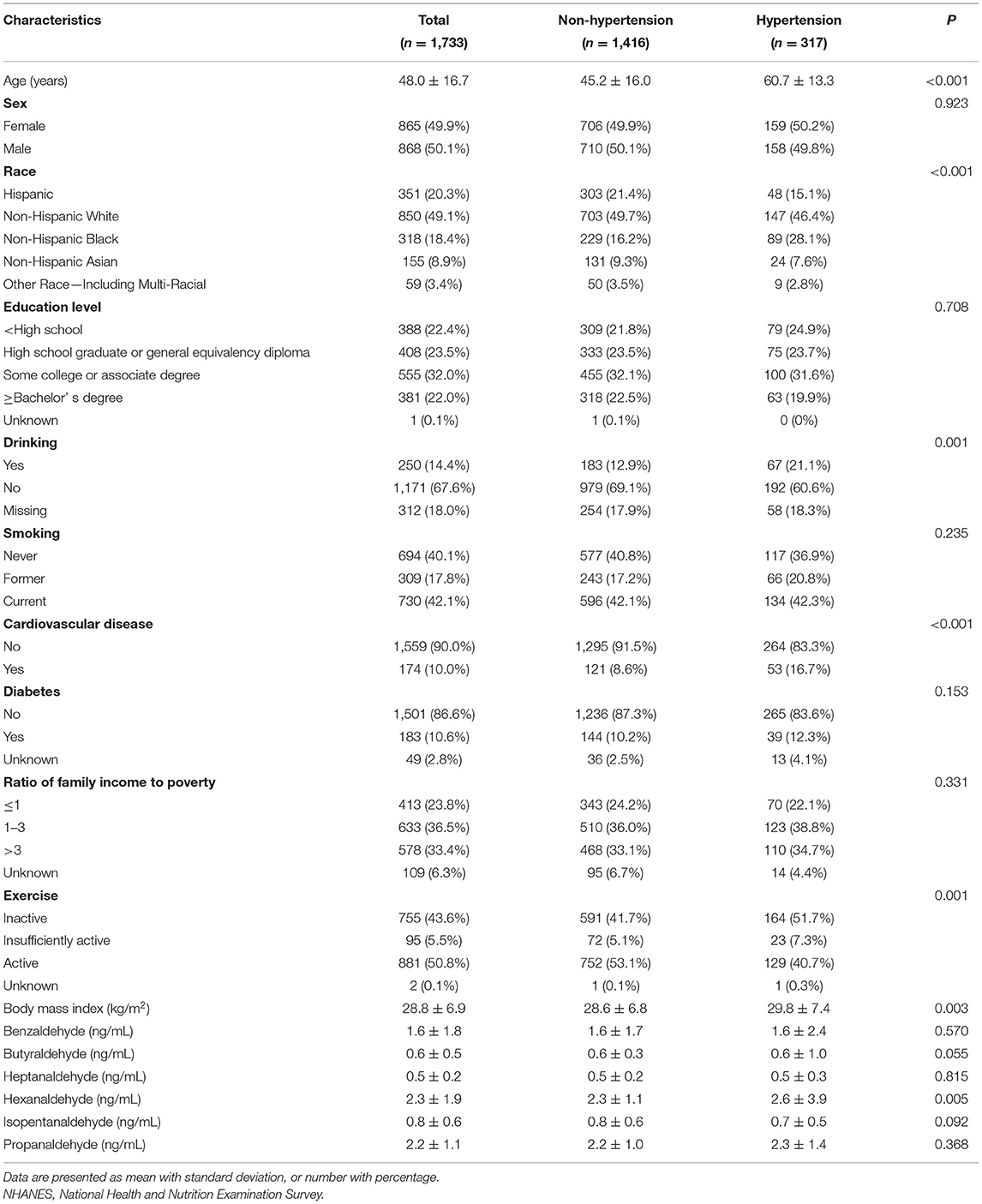
Table 1. Characteristics of participants in NHANES 2013–2014.
The serum concentrations of 6 selected aldehydes were shown in Table 1. There seems to be a numerically higher level of hexanaldehyde in participants with hypertension when compared to participants without hypertension (2.6 ± 3.9 vs. 2.3 ± 1.1 ng/mL). Table 2, Figure 2, and Supplementary Figure 1 summarized the associations of the quartiles of aldehydes with the odds of hypertension in three multivariate logistic regression models. After fully adjusting for demographic characteristics and other covariates (Model 3), the odds ratios (ORs) with 95% confidence intervals (CIs) for hypertension in participants from the highest quartile of serum aldehydes concentration were 0.77 (0.46–1.28), 1.35 (0.85–2.16), 1.07 (0.65–1.75), 2.15 (1.33–3.51), 1.09 (0.55–2.16), and 1.08 (0.65–1.79) for benzaldehyde, butyraldehyde, heptanaldehyde, hexanaldehyde, isopentanaldehyde, and propanaldehyde, respectively, in comparison to those with the lowest quartile. Among the 6 selected aldehydes, only serum hexanaldehyde was found to be significantly associated with hypertension in NHANES adults.
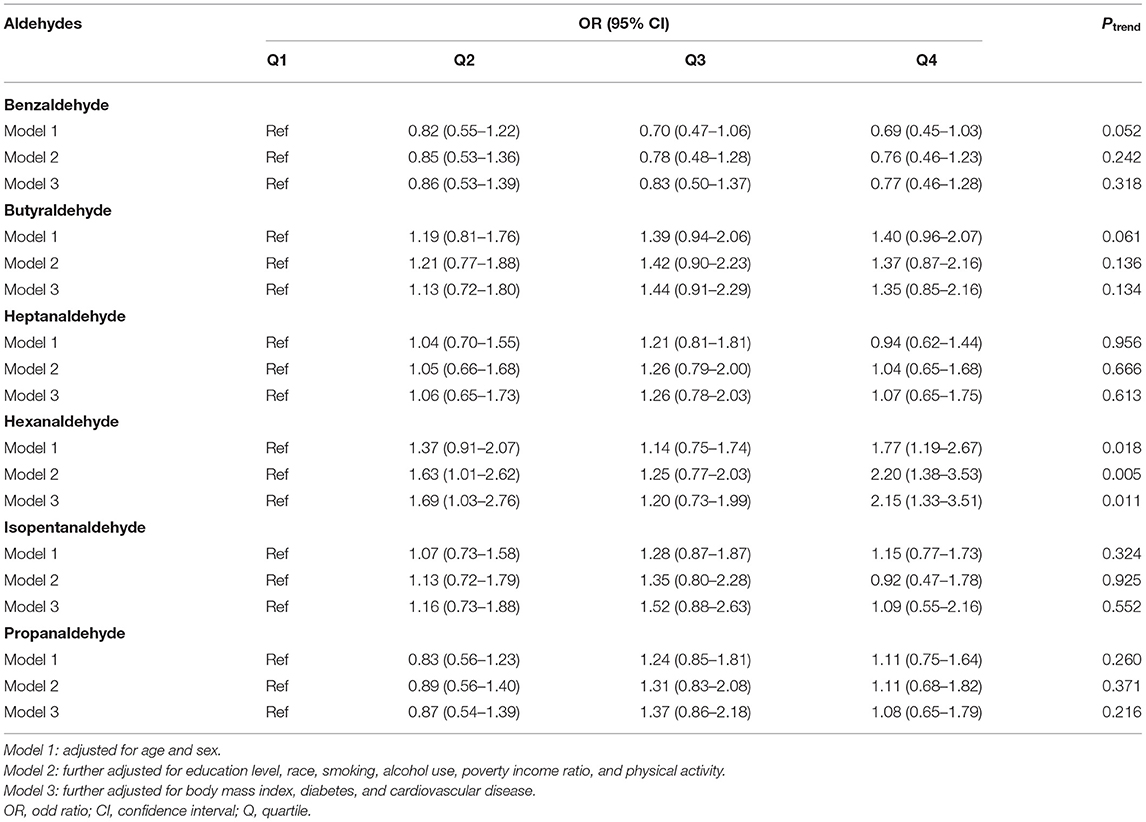
Table 2. Associations of selected aldehydes with odds of hypertension.
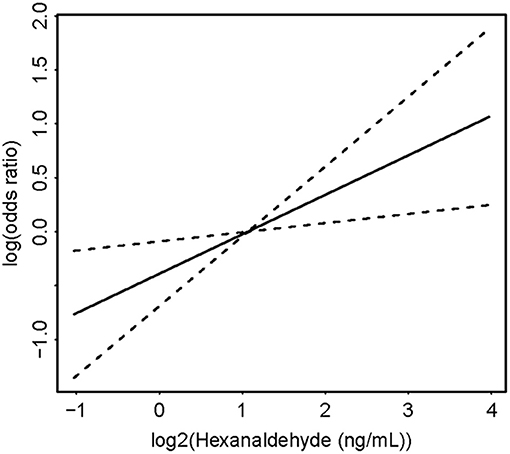
Figure 2. Concentration-response curve of association between hexanaldehyde and hypertension.
In subgroup analyses stratified by age, sex, education level, race, physical activity, alcohol use, smoking, diabetes, cardiovascular disease, and BMI, no significant interactions for the association between serum hexanaldehyde and the odds of hypertension were observed (Table 3). The subgroup analyses of the remaining 5 aldehydes were depicted in Supplementary Tables 1–5.

Table 3. Stratified analyses between hexanaldehyde and odds of hypertension.
After excluding participants with diabetes or cardiovascular disease (n = 304), the positive association between hexanaldehyde and the odds of hypertension was still significant (Table 4). A similar result was also found when using an updated 130/80 mm Hg to define hypertension in included participants. Likewise, the results from sensitivity analyses of the remaining five aldehydes did not significantly change when compared to main analyses.
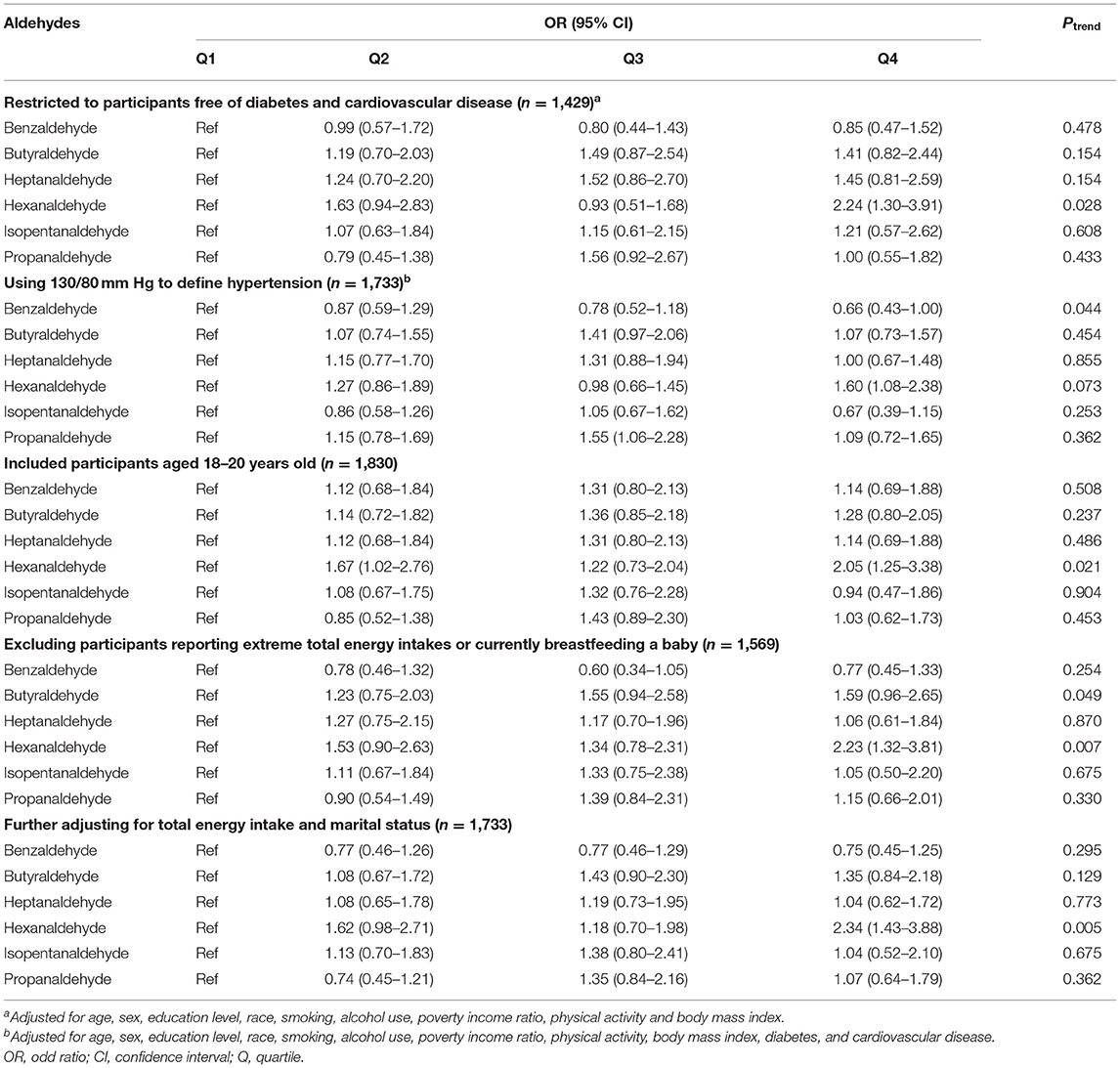
Table 4. Sensitivity analysis of associations between selected aldehydes and odds of hypertension.
To the best of our knowledge, this study is the first to investigate the associations between aldehyde exposure and the prevalence of hypertension in a selected, representative population. We found that increased serum hexanaldehyde level was positively associated with odds of hypertension in U.S. adults. We did not observe statistically significant associations between the other aldehydes (benzaldehyde, butyraldehyde, heptanaldehyde, isopentanaldehyde, and propanaldehyde,) and the prevalent hypertension.
As far as we know, there is no epidemiological study investigating the relationship between aldehyde exposure and risk of hypertension. Available evidences on this topic were based on few animal studies. Previous research reported that when aldehydes were administrated at low doses in spontaneously hypertensive rats, they could induce a dose-dependent pressor response by sympathomimetic effects though the release of norepinephrine from adrenergic neurons (25, 26). In addition, subsequent study also found that kidney aldehyde conjugates were significantly elevated in fructose induced hypertensive rats and spontaneously hypertensive rats (27, 28). More importantly, dietary supplement of methylglyoxal to Wistar-Kyoto rats has led to adverse renal vascular changes and hypertension (28). In the current study, we firstly observed that increased serum hexanaldehyde were significantly associated with higher odds of hypertension. As reported, hexanaldehyde is a kind of saturated aldehydes and a widespread exposure from tobacco smoke (29). Toxicology research suggested that hexanaldehyde exposure could cause nasal obstruction and headaches in humans (30). Moreover, elevated concentration of blood and exhaled hexanaldehyde has been noted in lung-cancer patients (31, 32). However, no mechanism research and population-based study have focused on the effects of hexanaldehyde exposure on cardiovascular diseases including hypertension. The health effect of hexanaldehyde and the reasons for differences of various aldehydes need further investigated.
There are limited studies investigating the health effect of aldehydes exposure, partly because the trait of volatile and high reactivity have resulted in difficulties in qualitative and quantitative determination of aldehydes in vivo. In recent years, some researchers have developed and validated a multistep procedure using SPME-GC-HRMS to detect the serum aldehydes concentrations (22). On the basis of above method, several cross-sectional studies have examined the potential relationship between serum aldehydes and cardiovascular diseases or obesity (20, 21, 33). Xu et al. showed that serum isopentanaldehyde concentrations were positively associated with the odds of cardiovascular disease (20). Given the differences in study outcomes, it is difficult to directly compare our results with the abovementioned findings. Even though, these insights collectively suggested that aldehyde exposure should be considered as an important environment contributor to cardiovascular diseases.
Although aldehydes have been suggested to have cytotoxic, mutagenic, genotoxic and carcinogenic effects (34), the possible mechanism underlying the association between serum aldehydes and hypertension were not well-defined. First, aldehyde-covalent modification of proteins and other biological macromolecules could be toxic and be mediators of inflammation and immune response which contributed to the pathogenesis of vascular diseases such as hypertension (35). Second, methylglyoxal has been reported to decrease serum nitric oxide levels in rats model (27). Excess reactive aldehydes may inhibit endogenous nitric oxide (NO) synthase via deactivation of endothelial proteins and impair NO-mediated endothelial function (36). Third, as aldehydes with the electrophilic nature prefer to react with the free amino and sulfhydryl groups of proteins, adducted aldehydes could bind to sufhydryl group of L-type Ca2+ channel proteins thus altering their functions. This may increase cytosolic free calcium levels and peripheral vascular resistance, and induce hypertension (37). Finally, oxidative stress has been confirmed to play a vital role in hypertension development by multiple animal models. Acrolein formed from lipid peroxidation or polyamine metabolism can induce and participate in oxidative stress which contributes to endothelial dysfunction (38). Increased methylglyoxal level has also been shown to cause oxidative stress in rat vascular smooth muscle cells (39).
Our study showed some advantages. First, the study was the first to report the association of aldehydes with hypertension using a nationally representative sample of U.S. adults, which facilitates the generalization of our findings. Second, the comprehensive data collection in the NHANES allowed us to adjust for a multitude of potential confounding factors. However, several limitations should also be acknowledged as well. First, due to the cross-sectional study design, causality relationship cannot be determined in this study. Second, the exposure of aldehydes can be endogenous and exogenous. Although we have observed a positive relationship between aldehydes and hypertension, it is difficult for us to evaluate whether the level of aldehydes in serum are exogenous or endogenous. Finally, the participants in the current study were adults from the U.S. Therefore, it should be cautious to generalize our results to other populations.
In summary, increased serum hexanaldehyde level was positively associated with odds of hypertension in U.S. adults. Future studies are warranted to verify the association between hexanaldehyde exposure and hypertension and the underlying mechanism.
Publicly available datasets were analyzed in this study. This data can be found at: https://www.cdc.gov/nchs/nhanes/index.htm.
The studies involving human participants were reviewed and approved by NCHS Institutional Review Committee. The patients/participants provided their written informed consent to participate in this study.
YB: conceptualization, methodology, and formal analysis. YZ: investigation, data curation, formal analysis, and writing—original draft. ML: data curation and writing—original draft. WF: investigation and writing—reviewing and editing. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.813244/full#supplementary-material
1. ^CDC National Health and Nutrition Examination Survey. 2013–2014.
1. Benjamin EJ, Virani SS, Callaway CW, Chamberlain AM, Chang AR, Cheng S, et al. Heart disease and stroke statistics-2018 update: a report from the American Heart Association. Circulation. (2018) 137:e67–492. doi: 10.1161/CIR.0000000000000558
2. Bundy JD, Li C, Stuchlik P, Bu X, Kelly TN, Mills KT, et al. Systolic blood pressure reduction and risk of cardiovascular disease and mortality: a systematic review and network meta-analysis. J Am Med Assoc Cardiol. (2017) 2:775–81. doi: 10.1001/jamacardio.2017.1421
3. Global Burden of Metabolic Risk Factors for Chronic Diseases Collaboration. Cardiovascular disease, chronic kidney disease, and diabetes mortality burden of cardiometabolic risk factors from 1980 to 2010: a comparative risk assessment. Lancet Diabet Endocrinol. (2014) 2:634–47. doi: 10.1016/S2213-8587(14)70102-0
4. GBD 2017 Risk Factor Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) 392:1923–94. doi: 10.1016/S0140-6736(18)32225-6
5. Du S, Batis C, Wang H, Zhang B, Zhang J, Popkin BM. Understanding the patterns and trends of sodium intake, potassium intake, and sodium to potassium ratio and their effect on hypertension in China. Am J Clin Nutr. (2014) 99:334–43. doi: 10.3945/ajcn.113.059121
6. Zhou B, Perel P, Mensah GA, Ezzati M. Global epidemiology, health burden and effective interventions for elevated blood pressure and hypertension. Nat Rev Cardiol. (2021) 2021:1–18. doi: 10.1038/s41569-021-00559-8
7. Sacks FM, Campos H. Dietary therapy in hypertension. N Engl J Med. (2010) 362:2102–12. doi: 10.1056/NEJMct0911013
8. Roerecke M, Kaczorowski J, Tobe SW, Gmel G, Hasan OSM, Rehm J. The effect of a reduction in alcohol consumption on blood pressure: a systematic review and meta-analysis. Lancet Public Health. (2017) 2:e108–20. doi: 10.1016/S2468-2667(17)30003-8
9. Virdis A, Giannarelli C, Neves MF, Taddei S, Ghiadoni L. Cigarette smoking and hypertension. Curr Pharm Des. (2010) 16:2518–25. doi: 10.2174/138161210792062920
10. Guo C, Zeng Y, Chang LY, Yu Z, Bo Y, Lin C, et al. Independent and opposing associations of habitual exercise and chronic PM(25) exposures on hypertension incidence. Circulation. (2020) 142:645–56. doi: 10.1161/CIRCULATIONAHA.120.045915
11. Bo Y, Guo C, Lin C, Chang LY, Chan TC, Huang B, et al. Dynamic changes in long-term exposure to ambient particulate matter and incidence of hypertension in adults. Hypertension. (2019) 74:669–77. doi: 10.1161/HYPERTENSIONAHA.119.13212
12. Lee TW, Kim DH Ryu JY. Association between urinary polycyclic aromatic hydrocarbons and hypertension in the Korean population: data from the Second Korean National Environmental Health Survey (2012-2014). Sci Rep. (2020) 10:17142. doi: 10.1038/s41598-020-74353-w
13. LoPachin RM, Gavin T. Molecular mechanisms of aldehyde toxicity: a chemical perspective. Chem Res Toxicol. (2014) 27:1081–91. doi: 10.1021/tx5001046
14. O'Brien PJ, Siraki AG, Shangari N. Aldehyde sources, metabolism, molecular toxicity mechanisms, and possible effects on human health. Crit Rev Toxicol. (2005) 35:609–62. doi: 10.1080/10408440591002183
15. Xue R, Dong L, Zhang S, Deng C, Liu T, Wang J, et al. Investigation of volatile biomarkers in liver cancer blood using solid-phase microextraction and gas chromatography/mass spectrometry. Rapid Commun Mass Spectrom. (2008) 22:1181–6. doi: 10.1002/rcm.3466
16. Butterfield DA, Castegna A, Lauderback CM, Drake J. Evidence that amyloid beta-peptide-induced lipid peroxidation and its sequelae in Alzheimer's disease brain contribute to neuronal death. Neurobiol Aging. (2002) 23:655–64. doi: 10.1016/S0197-4580(01)00340-2
17. Nelson MM, Baba SP, Anderson EJ. Biogenic aldehydes as therapeutic targets for cardiovascular disease. Curr Opin Pharmacol. (2017) 33:56–63. doi: 10.1016/j.coph.2017.04.004
18. Zirak MR, Mehri S, Karimani A, Zeinali M, Hayes AW, Karimi G. Mechanisms behind the atherothrombotic effects of acrolein, a review. Food Chem Toxicol. (2019) 129:38–53. doi: 10.1016/j.fct.2019.04.034
19. DeJarnett N, Conklin DJ, Riggs DW, Myers JA, O'Toole TE, Hamzeh I, et al. Acrolein exposure is associated with increased cardiovascular disease risk. J Am Heart Assoc. (2014) 3:934. doi: 10.1161/JAHA.114.000934
20. Xu C, Liang J, Xu S, Liu Q, Xu J, Gu A. Increased serum levels of aldehydes are associated with cardiovascular disease and cardiovascular risk factors in adults. J Hazard Mater. (2020) 400:123134. doi: 10.1016/j.jhazmat.2020.123134
21. Liao S, Zhang J, Shi S, Gong D, Lu X, Cheang I, et al. Association of aldehyde exposure with cardiovascular disease. Ecotoxicol Environ Saf. (2020) 206:111385. doi: 10.1016/j.ecoenv.2020.111385
22. Silva LK, Hile GA, Capella KM, Espenship MF, Smith MM, De Jesús VR, et al. Quantification of 19 aldehydes in human serum by headspace SPME/GC/high-resolution mass spectrometry. Environ Sci Technol. (2018) 52:10571–9. doi: 10.1021/acs.est.8b02745
23. Silva LK, Espenship MF, Newman CA, Zhang L, Zhu W, Blount BC, et al. Assessment of serum concentrations of 12 aldehydes in the U.S. Population from the 2013-2014 National Health and Nutrition Examination Survey. Environ Sci Technol. (2021) 55:5076–83. doi: 10.1021/acs.est.0c07294
24. Patriota P, Guessous I, Marques-Vidal P. No changes in dietary intake after quitting smoking; a prospective study in Switzerland. BMC Nutr. (2021) 7:34. doi: 10.1186/s40795-021-00440-4
25. Green MA, Egle JL Jr. Effects of intravenous acetaldehyde, acrolein, formaldehyde and propionaldehyde on arterial blood pressure following acute guanethidine treatment. Res Commun Chem Pathol Pharmacol. (1983) 40:337–40.
26. Green MA, Egle JL Jr. The effects of acetaldehyde and acrolein on blood pressure in guanethidine-pretreated hypertensive rats. Toxicol Appl Pharmacol. (1983) 69:29–36. doi: 10.1016/0041-008X(83)90115-1
27. Vasdev S, Ford CA, Longerich L, Parai S, Gadag V, Wadhawan S. Aldehyde induced hypertension in rats: prevention by N-acetyl cysteine. Artery. (1998) 23:10–36.
28. Vasdev S, Mian T, Ford CA, Longerich L, Parai S. Role of endogenous aldehydes in spontaneously hypertensive and disulfiram-induced hypertensive rats. Nutr Metabol Cardiovasc Dis. (1996) 1996:130–40.
29. Csordas A, Bernhard D. The biology behind the atherothrombotic effects of cigarette smoke. Nat Rev Cardiol. (2013) 10:219–30. doi: 10.1038/nrcardio.2013.8
30. Ernstgård L, Iregren A, Sjögren B, Svedberg U, Johanson G. Acute effects of exposure to hexanal vapors in humans. J Occup Environ Med. (2006) 48:573–80. doi: 10.1097/01.jom.0000215235.42071.68
31. Deng C, Li N, Zhang X. Development of headspace solid-phase microextraction with on-fiber derivatization for determination of hexanal and heptanal in human blood. J Chromatogr B Anal Technol Biomed Life Sci. (2004) 813:47–52. doi: 10.1016/j.jchromb.2004.09.007
32. Fuchs P, Loeseken C, Schubert JK, Miekisch W. Breath gas aldehydes as biomarkers of lung cancer. Int J Cancer. (2010) 126:2663–70. doi: 10.1002/ijc.24970
33. Liao S, Wu N, Gong D, Tang X, Yin T, Zhang H, et al. Association of aldehydes exposure with obesity in adults. Ecotoxicol Environ Saf. (2020) 201:110785. doi: 10.1016/j.ecoenv.2020.110785
34. Ahmed Laskar A, Younus H. Aldehyde toxicity and metabolism: the role of aldehyde dehydrogenases in detoxification, drug resistance and carcinogenesis. Drug Metab Rev. (2019) 51:42–64. doi: 10.1080/03602532.2018.1555587
35. Antoniak DT, Duryee MJ, Mikuls TR, Thiele GM, Anderson DR. Aldehyde-modified proteins as mediators of early inflammation in atherosclerotic disease. Free Radic Biol Med. (2015) 89:409–18. doi: 10.1016/j.freeradbiomed.2015.09.003
36. Kuntic M, Oelze M, Steven S, Kröller-Schön S, Stamm P, Kalinovic S, et al. Short-term e-cigarette vapour exposure causes vascular oxidative stress and dysfunction: evidence for a close connection to brain damage and a key role of the phagocytic NADPH oxidase (NOX-2). Eur Heart J. (2020) 41:2472–83. doi: 10.1093/eurheartj/ehz772
37. Hatzitolios A, Iliadis F, Katsiki N, Baltatzi M. Is the anti-hypertensive effect of dietary supplements via aldehydes reduction evidence based? A systematic review. Clin Exp Hypertens. (2008) 30:628–39. doi: 10.1080/10641960802443274
38. Uchida K, Kanematsu M, Morimitsu Y, Osawa T, Noguchi N, Niki E. Acrolein is a product of lipid peroxidation reaction. Formation of free acrolein and its conjugate with lysine residues in oxidized low density lipoproteins. J Biol Chem. (1998) 273:16058–66. doi: 10.1074/jbc.273.26.16058
Keywords: aldehydes, hexanaldehyde, hypertension, adults, cross-sectional
Citation: Zhu Y, Liu M, Fu W and Bo Y (2022) Association Between Serum Aldehydes and Hypertension in Adults: A Cross-Sectional Analysis of the National Health and Nutrition Examination Survey. Front. Cardiovasc. Med. 9:813244. doi: 10.3389/fcvm.2022.813244
Received: 11 November 2021; Accepted: 01 February 2022;
Published: 07 March 2022.
Edited by:
Salvatore Pepe, Royal Children's Hospital, Melbourne, AustraliaReviewed by:
Dongfeng Zhang, Qingdao University, ChinaCopyright © 2022 Zhu, Liu, Fu and Bo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yongjian Zhu, emh1NDEyODI1QDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.