
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 11 March 2022
Sec. Coronary Artery Disease
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.793067
This article is part of the Research TopicInsights in Coronary Artery Disease: 2021View all 15 articles
 Farzin Beygui1*
Farzin Beygui1* Vincent Roule1
Vincent Roule1 Fabrice Ivanes2Thierry Dechery3Olivier Bizeau4Laurent Roussel5Philippe Dequenne6Marc-Antoine Arnould7Nicolas Combaret8Jean Philippe Collet9
Fabrice Ivanes2Thierry Dechery3Olivier Bizeau4Laurent Roussel5Philippe Dequenne6Marc-Antoine Arnould7Nicolas Combaret8Jean Philippe Collet9 Philippe Commeau10Guillaume Cayla11Gilles Montalescot9Hakim Benamer12Pascal Motreff8
Philippe Commeau10Guillaume Cayla11Gilles Montalescot9Hakim Benamer12Pascal Motreff8 Denis Angoulvant2Pierre Marcollet3Stephan Chassaing7Katrien Blanchart1
Denis Angoulvant2Pierre Marcollet3Stephan Chassaing7Katrien Blanchart1 René Koning13Grégoire Rangé5
René Koning13Grégoire Rangé5Background: First medical contact (FMC)-to-balloon time is associated with outcome of ST-elevation myocardial infarction (STEMI). We assessed the impact on mortality and the determinants of indirect vs. direct transfer to the cardiac catheterization laboratory (CCL).
Methods: We analyzed data from 2,206 STEMI patients consecutively included in a prospective multiregional percutaneous coronary intervention (PCI) registry. The primary endpoint was 1-year mortality. The impact of indirect admission to CCL on mortality was assessed using Cox models adjusted on FMC-to-balloon time and covariables unequally distributed between groups. A multivariable logistic regression model assessed determinants of indirect transfer.
Results: A total of 359 (16.3%) and 1847 (83.7%) were indirectly and directly admitted for PCI. Indirect admission was associated with higher risk features, different FMCs and suboptimal pre-PCI antithrombotic therapy.
At 1-year follow-up, 51 (14.6%) and 137 (7.7%) were dead in the indirect and direct admission groups, respectively (adjusted-HR 1.73; 95% CI 1.22–2.45). The association of indirect admission with mortality was independent of pre-FMC and FMC characteristics. Older age, paramedics- and private physician-FMCs were independent determinants of indirect admission (adjusted-HRs 1.02 per year, 95% CI 1.003–1.03; 5.94, 95% CI 5.94 3.89–9.01; 3.41; 95% CI 1.86–6.2, respectively).
Conclusions: Our study showed that, indirect admission to PCI for STEMI is associated with 1-year mortality independent of FMC to balloon time and should be considered as an indicator of quality of care. Indirect admission is associated with higher-risk features and suboptimal antithrombotic therapy. Older age, paramedics-FMC and self-presentation to a private physician were independently associated with indirect admission. Our study, supports population education especially targeting elderly, more adequately dispatched FMC and improved pre-CCL management.
Primary percutaneous coronary intervention (PCI) is the first-line treatment for ST-elevation myocardial infarction (STEMI) (1). System delays from the first medical contact (FMC) to cardiac catheterization laboratory (CCL) are associated with poor outcome (2–4) and should be reduced to the minimum (1). However, despite improved door to balloon times, within the past decades, rates of mortality seem to be unchanged in the setting of STEMI (5) and further investigations are needed to identify other pre-CCL correlates of outcome and to develop new strategies to improve outcome.
A direct admission to CCL by Pre-hospital emergency medical services (EMS) is recommended in order to reduce system delays (1, 6). Indirect admission to the CCL and the number of contacts, after the FMC, are associated with longer system delays and total ischemic time but their impact on mortality, independent of system delays remains controversial (7, 8).
The objective of our study was to investigate whether indirect admission to CCL impacted mortality independent of FMC to balloon time and other identified co-variables in patients enrolled in a STEMI networks within 24 h following symptom onset and admitted to CCL for primary PCI. We also aimed to assess the determinants of indirect admission.
The France PCI registry is an open, ongoing prospective multicenter registry (clinicaltrials.gov#NCT02778724) including consecutive patients admitted to CCLs for coronary interventions in different French regions as described previously (9, 10). In the setting of STEMI, pre-CCL management, timelines, reperfusion strategies, antithrombotic therapy and intervention characteristics are recorded in patients' medical files and electronically transferred to the registry. In-hospital and 1-year outcomes, derived from source files and/or physical or phone contacts are recorded. The quality of the registry is guaranteed by systematic audits by study coordinators independent of each center.
The current retrospective analysis focused on STEMI patients included within 24 h after symptom onset, undergoing primary PCI between January 1st 2014 and December 31st 2016, excluding patients with out-of-hospital cardiac arrest prior to STEMI, lytic therapy, and no attempt to PCI.
FMC was defined by the first person competent to obtain and interpret the ECG and, to provide initial intervention (1). The standard of care for the management of suspected STEMI in France is the physician-on board ambulance sent to the scene. However, paramedics-on board ambulances and self-presentation to an emergency department (ED) or to a private medical doctor (MD) are other potential pathways. “Door” was defined by the time of admission in the PCI-capable hospital and “balloon” was the time of coronary lesion crossing by the first PCI guidewire or balloon. Successful PCI was defined by a visually assessed coronary diameter stenosis <30% and a thrombolysis in myocardial infarction coronary flow 3. For the purpose of the current study we defined two groups based on the pathway from FMC to CCL: direct admission (guideline-recommended pathway without admission in any other medical facility prior to CCL; e.g., transfer from scene or an ED or ward to CCL) and indirect admission (admission to another medical facility prior to CCL; e.g., private MD or EMS to non-PCI facility then to CCL).
The primary outcome was mortality of any cause at 1-year follow-up. Secondary outcomes included hospital discharge and 1-year mortality, cardiovascular mortality (death related to cardiovascular causes or sudden death), major bleeding defined by the bleeding academic research consortium (BARC) classification ≥ 3, Non-fatal myocardial infarction, defined by types 1, 4 and 5 based on the universal definition (11), stroke, definite/probable stent thrombosis based on the academic research consortium criteria (12) and unplanned coronary revascularization.
Baseline data are shown as n (%) and mean ± standard deviation and compared between groups using the χ2 test and the Student's t test for categorical and continuous variables, respectively. The primary outcome and 1-year cardiovascular mortality were compared between the two groups using Kaplan-Meier curves and the log-rank test. The association between the group and the latter outcomes was assessed using un-adjusted and adjusted on FMC to balloon time (primary analysis) cox regression models with calculation of Hazard ratios (HR) and 95% Confidence intervals (CI). Other 1-year outcomes were assessed by the unadjusted Cox analyses.
Supplementary analyses were performed by adjusting the Cox models on covariables unequally distributed between the two groups with a p value < 0.1 in order to assess: 1. the impact of patient characteristics at the time of FMC; 2. The impact of pre-CCL management; 3. The concomitant impact of all latter variables 4. The impact of all latter variables and in-hospital variables.
Sensitivity analyses were conducted using the number of pre-CCL contacts as a continuous variable (1, 2, ≥3) instead of direct vs. indirect admission and total ischemic (symptom-to-balloon) time in replacement of FMC to balloon time in the latter models.
The associations between the groups and in-hospital outcomes were assessed by unadjusted and, in case of significant associations, by adjusted on FMC-to-balloon time logistic regression models with calculation of odds ratios (OR) and 95% CI.
The determinants of indirect admission to CCL were explored using a multivariable logistic regression model including all patient characteristics at the time of FMC unequally distributed between groups (p < 0.1) as well as EMS number call, type of FMC and FMC-to-balloon time. Finally, in a final exploratory analysis, we compared data between FMC groups with the MD-EMS group considered as the reference group.
All tests were two sided and a p value < 0.05 was considered as statistically significant.
A total of 2,760 consecutive patients were admitted during the analysis period among whom 2,206 fulfilled the inclusion criteria.
Figure 1 depicts the flow chart and pathways from the FMC to CCL. The FMC was an EMS team in 1,310 (59.4%), an ED in 601 (27.2%), a private MD in 200 (9.1%) and a physician in a hospital where patients were already admitted at the time of STEMI in 95 (4.3%) cases. A total of 359 (16.3%) and 1,847 (83.7%) were indirectly and directly admitted to CCL, respectively. The national EMS number was called directly by 1,245 (56%) patients for whom MD- or paramedics-EMS team were sent on scene in 1,090 (88%) and 110 (9%), respectively while others were directed to their MD (0.5%) or an ED (2.5%). Among the 961 (44%) patients who did not call directly the national EMS number, 95 (10%) were already hospitalized for another condition, 601 (62.5%) self-presented to an ED, 200 (20.8%) self-presented to their MD and 65 (6.7%) were referred to the EMS by their MD after a phone call.
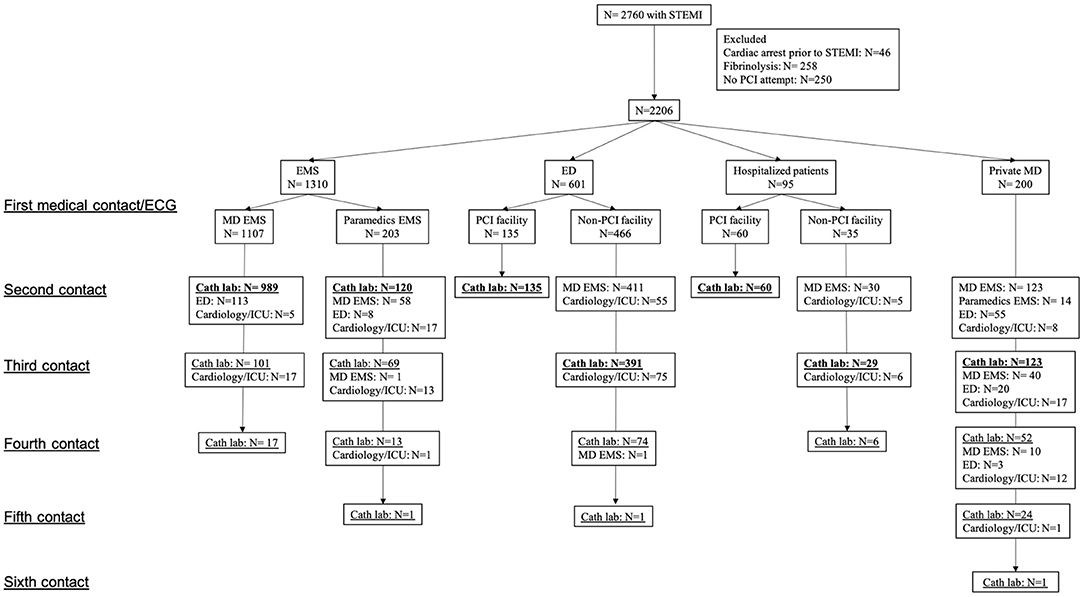
Figure 1. Flow chart and details of first medical contact to cardiac catheterization laboratory pathways. Direct admission to catheterization laboratory appears in bold text. STEMI, ST elevation myocardial infarction; PCI, percutaneous coronary intervention; EMS, emergency medical services; ED, emergency department; MD, medical doctor; ICU, intensive care unit; Cath lab, catheterization laboratory.
Table 1 depicts patient characteristics based on direct vs. indirect admission to CCL. Compared to directly admitted patients, those indirectly transferred were significantly older (p = 0.0006) with higher rates of female gender (p = 0.01), Killip class ≥1 (p = 0.008), diabetes (p = 0.01), hypertension (p = 0.02) and, lower rates of past history of MI (p = 0.002) and PCI (p = 0.0009). FMC was less often an MD-EMS (p < 0.0001), an ED (p = 0.003) or a ward MD (p = 0.007) and more often a paramedics-EMS (p < 0.0001) or a private MD (p < 0.0001) in those indirectly transferred.
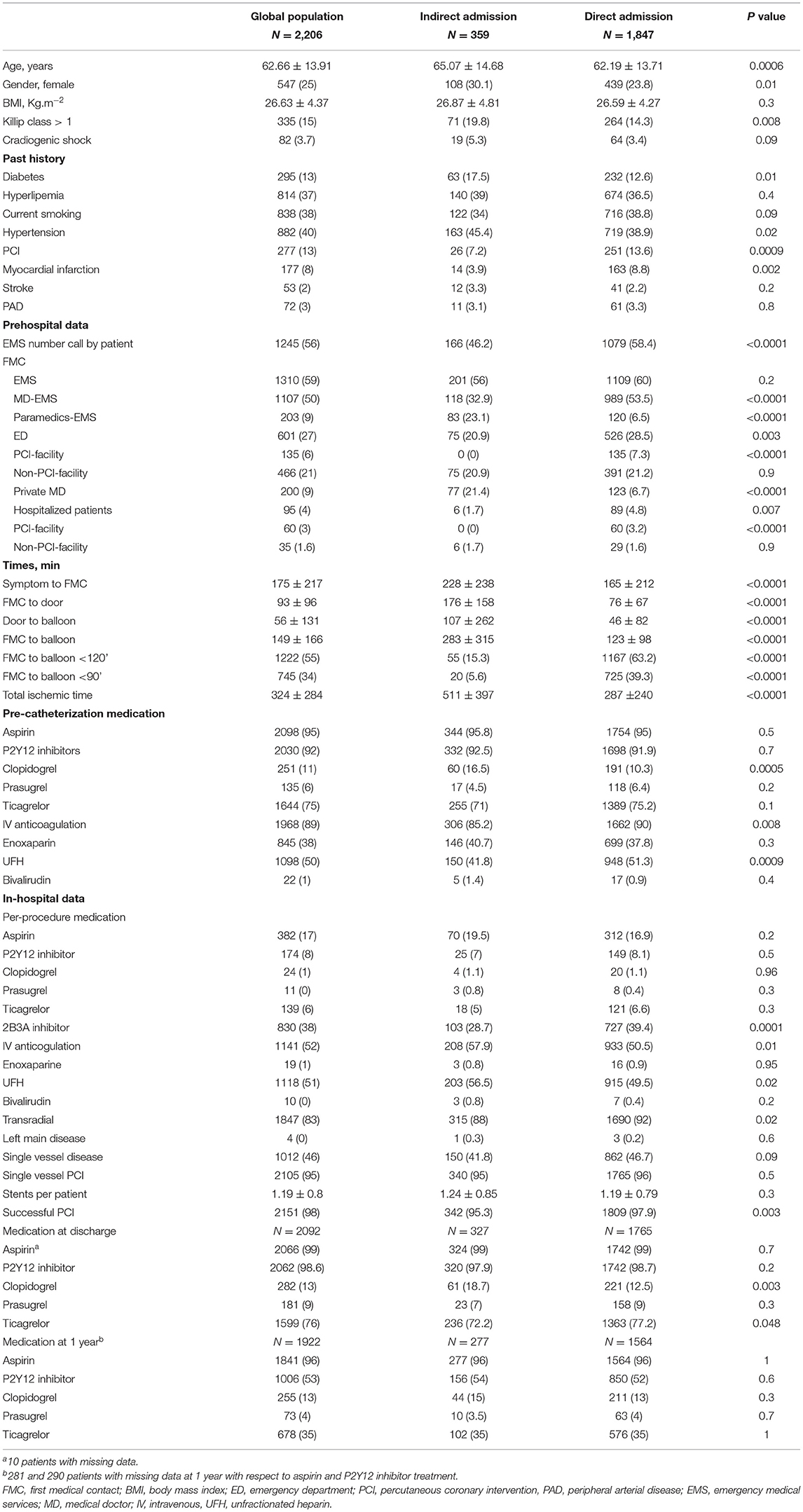
Table 1. Patient and procedure characteristics.
The rate of patients with a FMC to balloon time < 120 min was >3 times lower (p < 0.0001) and all delays were longer (p < 0.0001) in patients indirectly transferred.
Between FMC and CCL, patients indirectly transferred to the hospital were less likely to receive intravenous anticoagulation (p = 0.01) and received more frequently clopidogrel (p = 0.002) as compared to newer P2Y12 inhibitors.
During the procedure, 2B3A inhibitors and supplementary doses of intravenous anticoagulation were more frequently used in those indirectly transferred (p < 0.0001 and p = 0.01, respectively). Angiographic findings and PCI characteristics were similar between the groups but the rates of transradial approach and successful PCI were lower in those indirectly transferred (p = 0.02 and p = 0.003).
At hospital discharge, patients indirectly transferred were more frequently on clopidogrel (p = 0.003) and less frequently on ticagrelor (p < 0.05).
Outcome data (Table 2) were complete for all patients at hospital discharge and 2,124 (96.3%) patients at 1-year follow-up.
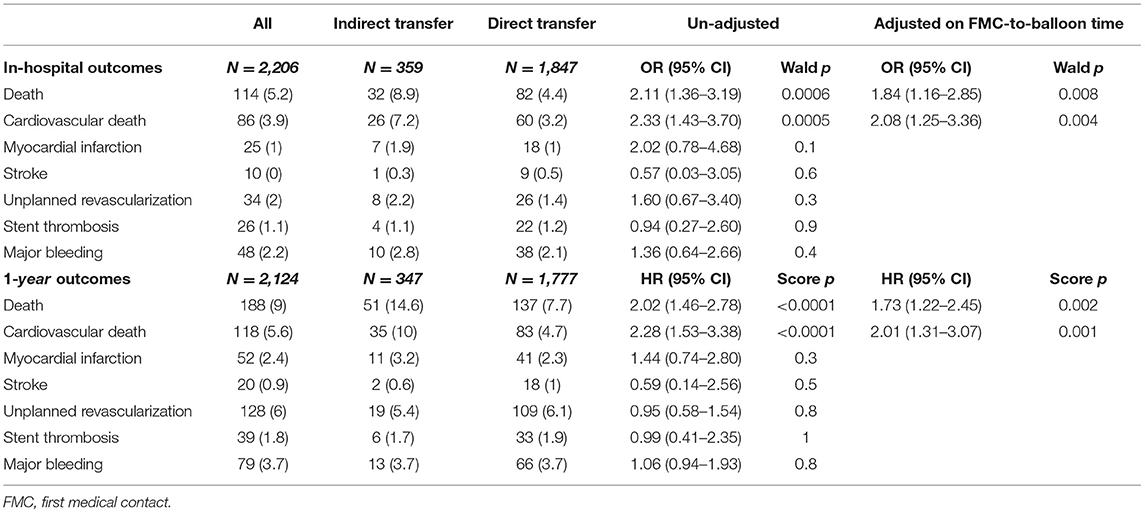
Table 2. Outcomes and their association with indirect vs. direct transfer.
At hospital discharge 114 (5.2%) patients were reported dead, 32 (8.9%) in the indirect admission and 82 (4.4%) in the direct admission groups, respectively (adjusted-OR 1.84, 95% CI 1.16–2.85, p = 0.008). In-hospital cardiovascular death occurred in 26 (7.2%) and 60 (3.2%) patients in the indirect and direct admission groups, respectively (adjusted OR 2.08, 95% CI 1.25–3.36, p = 0.004). Other end points were similarly distributed between the two groups.
At 1-year follow-up 188 (9%) were reported dead, 51 (14.6%) in the indirect and 137 (7.7%) in the direct admission groups, respectively (adjusted-HR 1.73, 95% CI 1.22–2.45, p = 0.002). Cardiovascular death was reported in 35 (10%) and 83 (4.7%) patients in the indirect and direct admission groups, respectively (adjusted-HR 2.01, 95% CI 1.31–3.07, p = 0.0003). Figure 2 depicts survival and cardiovascular survival Kaplan-Meier curves. Other 1-year end points were similarly distributed between the groups. At 1-year follow-up 96 and 53% of patients remained on aspirin and a P2Y12 inhibitor, respectively. Such rates as well as the distribution of different P2Y12 inhibitors were similar between the 2 groups suggesting comparable adherence to treatment.
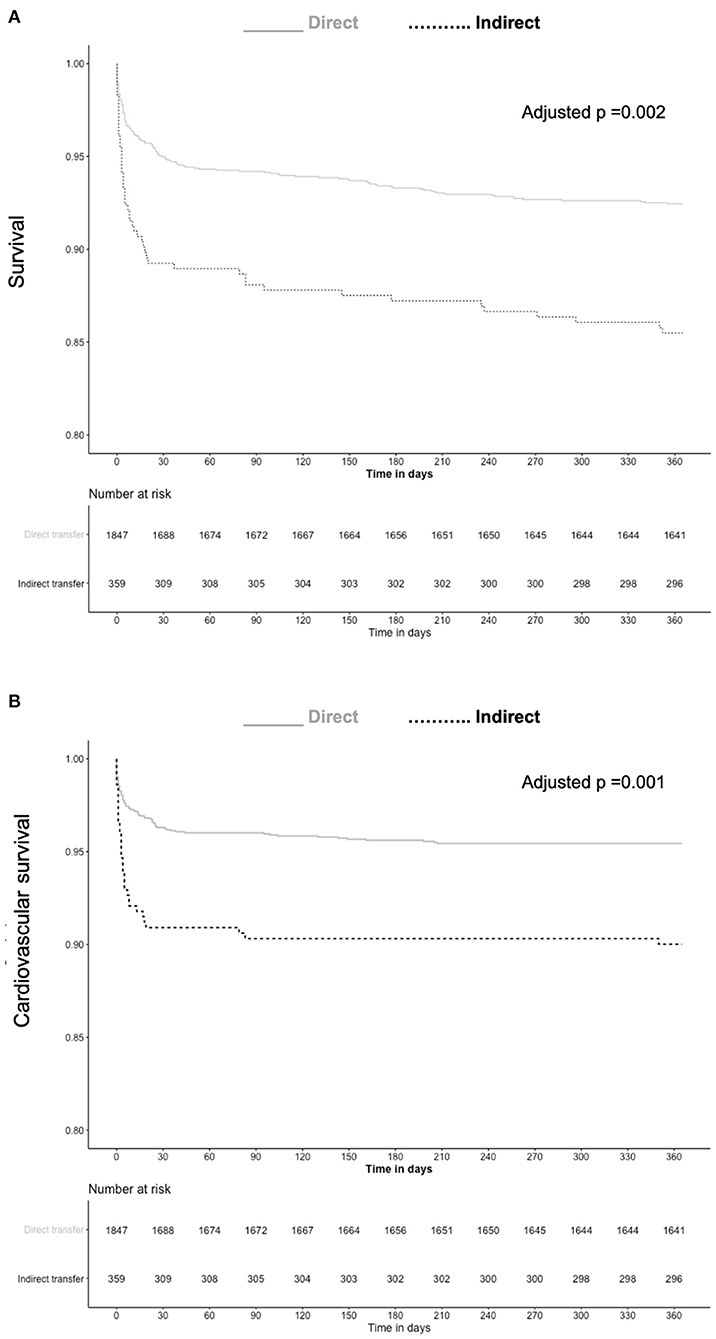
Figure 2. Kaplan-Meier curves for survival (A) and cardiovascular survival (B) based on direct or indirect admission to catheterization laboratory.
As shown in Table 3, the relationship between the group and, both 1-year mortality and cardiovascular mortality remained significant in models including separately pre-CCL patient (model 1) or intervention characteristics (model 2) both including FMC to balloon time. In model 3 gathering models 1 and 2, and model 4 including in-hospital variables on top of model 3, indirect admission was no more significantly associated with mortality. In the model 4, age, diabetes, Killip class ≥2, FMC to balloon time, pre-CCL P2Y12 inhibitor and anticoagulation, transradial access and successful PCI were independently associated with mortality. All such variables except diabetes, were also independently associated with cardiovascular mortality.
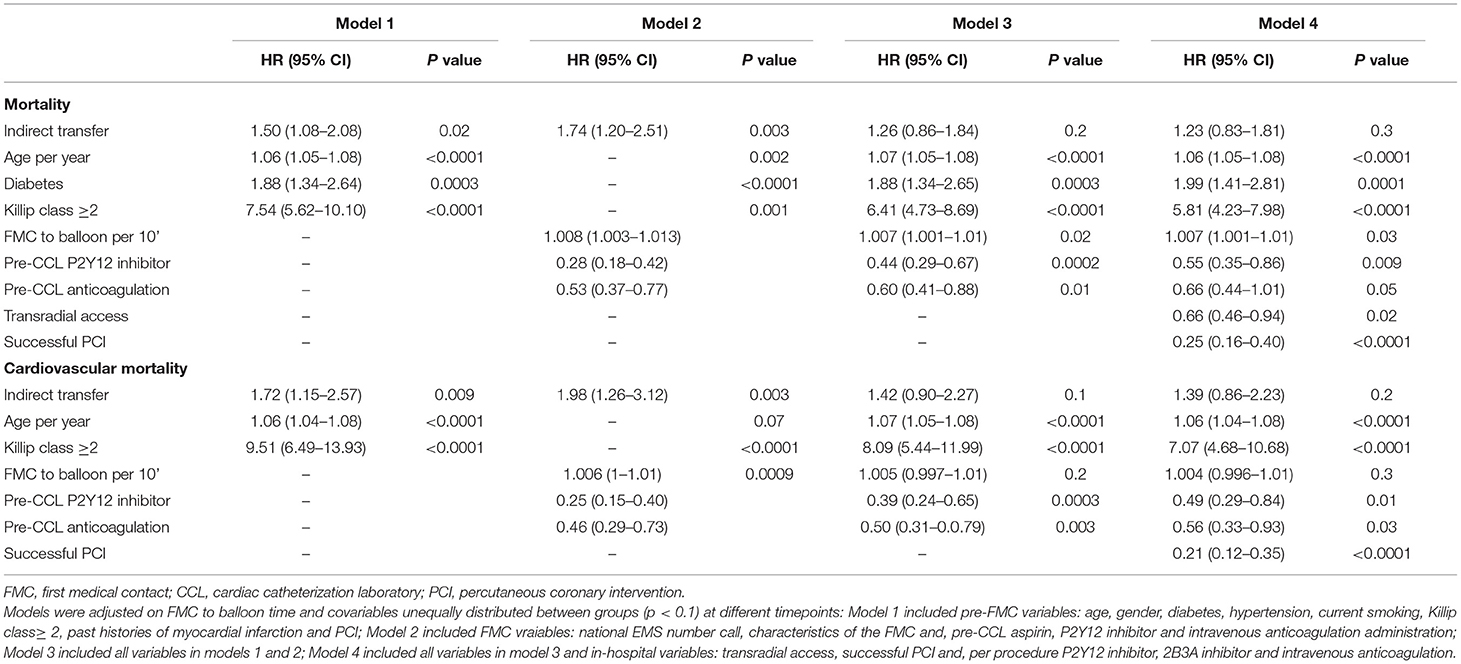
Table 3. Variables significantly associated with 1-year mortality and cardiovascular mortality.
Sensitivity analyses (Supplementary Table 1) showed consistent results.
As summerized in Table 4, age (OR 1.02 per year, 95% CI 1.003–1.03, p = 0.01), paramedics-EMS (OR 5.94 vs. MD-EMS, 95% CI 3.89–9.01, p < 0.0001) and private MD (OR 3.41 vs. MD-EMS, 95% CI 1.86–6.21, p < 0.0001) were determinants of indirect admission independent of FMC-to-balloon time and other co-variables.
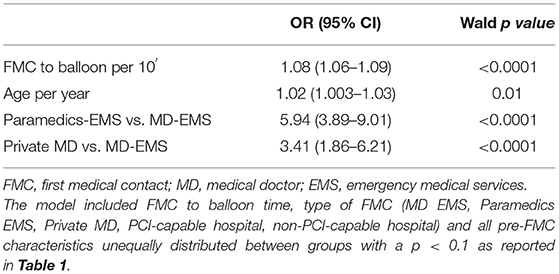
Table 4. Independent correlates of indirect admission to catheterization laboratory.
The Supplementary Table 2 and Figure 3 depict the analysis based on different pre-CCL pathways and their comparison to the MD-EMS group considered as the reference. The analysis adjusted on FMC to balloon time showed that compared to the MD-EMS group, there was an increased risk of in-hospital (adjusted-OR 1.94, 95% CI 1.10–3.31, p = 0.02) and 1 year mortality (adjusted-HR 1.62, 95% CI 1.05–2.48, p = 0.02) and cardiovascular mortality (adjusted OR 2.12, 95% CI 1.11–3.85, p = 0.02 and adjusted HR 1.85, 95% CI 1.08–3.15, p = 0.02) associated with the paramedic-EMS group.
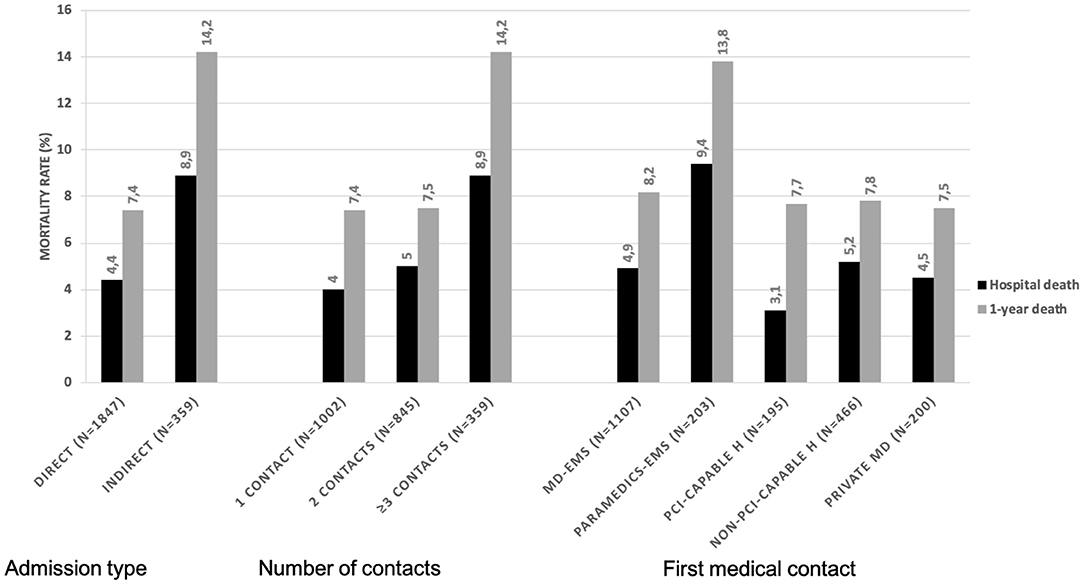
Figure 3. In-hospital and 1-year mortality rates based on different pathways to catheterization laboratory. PCI, percutaneous coronary intervention; EMS, emergency medical services; ED, emergency department; MD, medical doctor; H, hospital.
Our study shows that indirect admission of patients to CCL, as defined by guidelines, is associated with more than twice higher risks of both in-hospital and 1-year mortality and cardiovascular mortality. Although indirect admission was associated with increased system delays, its relationship with mortality remained independent of FMC to balloon and total ischemic times. Indirect admission is associated with higher risk features at the time of FMC (older age, female gender, Killip class ≥2, diabetes, hypertension, later presentation), different FMC characteristics (lower rates of national EMS number call, higher rates of paramedics-EMS and self-presentation to ED or to a private MD), pre-CCL medication (lower rates of newer P2Y12 inhibitors and anticoagulation) and in-hospital and procedure characteristics (higher rates of GP2B3A inhibitors and anticoagulation and, lower rates of transradial approach and successful PCI). We identified older age, paramedics-EMS and private MD-FMCs as independent determinants of indirect admission. Finally, paramedics-EMS pathway was associated with higher risks of in-hospital and 1 year mortality as compared to MD-EMS.
System delays are associated with increased mortality and heart failure in the setting of primary PCI for STEMI (2, 13, 14). Based on guidelines, STEMI patients should be transferred directly to the CCL bypassing ED and intensive care units in order to shorten the FMC to balloon times (1, 6). Our study shows that although indirect admission is associated with longer FMC to balloon times, the relationship between indirect admission and mortality remains independent of FMC to balloon time. Such impact of indirect admission on mortality may be explained by several findings in our study. Pre-FMC variables such as older age, female gender, diabetes, hypertension and clinical signs of heart failure (killip class ≥2 and cardiogenic shock), known correlates of mortality were more frequently encountered in the indirect admission group (15–17). Elderly, female and diabetic patients are also more often late presenters, have delayed management and longer total ischemic time and are more likely to have STEMI complicated by heart failure and subsequent mortality (16–18). Concordantly our study shows longer symptom to FMC and total ischemic times in the indirect admission group. However as shown on our multivariable analyses, patient characteristics and longer total ischemic times are not the single explanation to the impact of indirect admission on mortality.
Among FMC-related variables, the pre-CCL medication was different between the groups with higher rates of pretreatment with clopidogrel as compared to newer P2Y12 inhibitors and lower rates of intravenous anticoagulation in those indirectly admitted. Treatment by intravenous anticoagulants and more potent P2Y12 inhibitors rather than clopidogrel is recommended, in the setting of primary PCI based on strong evidence (1). Although the benefit of a pre-CCL administration of ticagrelor as compared to its administration in the CCL on clinical outcome-except in terms of stent thrombosis- or coronary artery flow was not demonstrated in a randomized controlled trial (19), several metanalyses show a benefit of more potent P2Y12 inhibitors over clopidogrel and the benefit of Pre-procedure over per-procedure P2Y12 inhibitors in the setting of STEMI both on clinical endpoints and the quality of coronary flow restoration (20–22). Such discrepancy may be related to the very short time separating the two groups in the latter randomized trial −30′-while in real life, system delays are much longer and allow the P2Y12 inhibitors to be effective at the time of PCI. As a matter of fact a sub-analysis of the above-mentioned trial showed that ticagrelor Pre-treatment was associated with improved reperfusion in those with long transfer delays (23). Pre-CCL anticoagulation has also been reported to be associated with improved coronary flow at the time of PCI (24) especially in those with long transfer delays (23) although an effect on clinical endpoints has not been demonstrated to date. In our study both pre-CCL P2Y12 inhibitor use and anticoagulation were associated with lower rates of mortality at 1 year independent of other covariables. The suboptimal pre-CCL antithrombotic management may expose to the risk of higher thrombus burden at the time of PCI, over-exposure to GP2B3A inhibitors in routine or bail-out situations and suboptimal myocardial reperfusion. The impact of pre-CCL administration of such drugs on coronary flow, a correlate of mortality (25), is supported by our findings of lower rates of GP2B3A inhibition and supplementary anticoagulation as well as the higher rates of successful PCI in those directly admitted to the CCL and may be another explanation of the relationship between the groups and mortality.
Another explanation to the differences in pre-CCL management is the diversity of FMCs and pathways. Unlike other FMCs, private MDs and paramedics-EMS, although capable of activating the CCL, did not administer such medication and systematically required another contact. The latter types of FMC, independently associated with indirect admission in our study, are also associated with longer FMC to balloon times and, no or delayed administration of P2Y12 inhibitors and/or intravenous anticoagulation. A poor impact of presentation to a private-MD vs. EMS on system delays and outcome has been previously reported (26).
Our analysis showed that age, paramedics-EMS and private-MD FMCs were associated with indirect admission independent of FMC to balloon time and other pre-FMC variables. The French EMS targeting STEMI patients are based on a dedicated national number and an MD on board organization. However, MD-EMS were the FMC in only half of patients. In almost 10% of patients the FMC was a paramedics-EMS, and mortality rates were almost twice higher in such patients compared to those managed by MD-EMS. Higher patient risk profile (female gender and Killip class >1) and the lack of medical expertise in the paramedics-EMS potentially leading to delayed diagnosis, patient misorientation and suboptimal management may explain such finding. It is likely that in an emergency care organization based on MD-EMS, paramedic-EMS, associated with indirect admission and increased risk of mortality should be avoided. Another 10% of patients self-presented to their private MD or a non-PCI facility ED. Interestingly, compared to MD-EMS, system delays were significantly higher in all such patients but mortality rates were not higher. Such finding may be due, to a selection bias, less severe status being more likely to lead to self-presentation than EMS call.
Direct admission to CCL was also associated with higher rates of transradial approach and successful PCI both known correlates of decreased mortality in the setting of STEMI (15, 27). Although a relationship between indirect admission and lower rates of transradial approach has previously been reported (8), in absence of a plausible mechanistic explanation such finding may be considered as random. Finally, as mentioned above, the relationship between indirect admission and PCI success may be related to more optimal upfront antithrombotic therapy.
Our study is a retrospective analysis of a prospective registry and may have several limitations inherent to such design. The impact of several known or unknown variables may have been underestimated or unassessed. The registry focuses on the peri-CCL management and antithrombotic therapy; hence the impact of other evidence-based treatments could not be assessed. Furthermore, compliance to evidence-based medication impacting outcomes was not assessed in our study. However similar 1-year rates of antiplatelet therapy suggest comparable adherence to treatment between groups. The findings are specific to the STEMI networks based on MD-EMS as a reference in mixt rural/urban regions and may not apply to other types of organizations. However, none of the latter limitations is likely to impact the main finding of the study. Finally, the multiple analyses based on different FMCs and pathways, should be considered as only exploratory.
Our study shows that indirect admission to the CCL for primary PCI in the setting of STEMI is associated with in-hospital and 1-year mortality and cardiovascular mortality independent of system delays. Indirect admission to CCL is not only associated with longer FMC to balloon times but also, with higher rates of high-risk patients, suboptimal pre-CCL antithrombotic therapy and lower rates of successful PCI. Among all assessed variables, older age, Paramedics-EMS and self-presentation to a private MD as FMCs were independently associated with indirect admission to CCL. Such findings in a system based on MD-EMS for the management of STEMI, underscores the potential pitfalls of such organization. Our study, highlights the need for population education especially targeting elderly patients and EMS dispatching and staff training in order to improve pre-CCL management and promote direct admission to CCL. Direct admission and optimal pre-CCL management and not only reduced system delays should be considered as STEMI network quality of care measures.
The data analyzed in this study is subject to the following licenses/restrictions: The data underlying this article were provided by FRANCE-PCI registry. Data will be shared on request to the corresponding author with permission of the FRANCE-PCI registry steering committee. Requests to access these datasets should be directed to FB, beygui-f@chu-caen.r.
The studies involving human participants were reviewed and approved by Commission National Informatique et Libertés-CNIL-, 3 Place de Fontenoy-TSA 80715-75334 PARIS CEDEX 07. The Ethics Committee waived the requirement of written informed consent for participation.
FB, RK, and GR contributed to conception and design of the study. GR organized the database. FB performed the statistical analysis and wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
The France-PCI registry's management is funded by the French Regional Health Agencies.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.793067/full#supplementary-material
1. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. (2018) 39:119–77. doi: 10.1093/eurheartj/ehx393
2. de Luca G, Suryapranata H, Ottervanger JP, Antman EM. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation. (2004) 109:1223–5. doi: 10.1161/01.CIR.0000121424.76486.20
3. Jäger B, Farhan S, Rohla M, Christ G, Podczeck-Schweighofer A, Schreiber W, et al. Clinical predictors of patient related delay in the VIENNA ST-elevation myocardial infarction network and impact on long-term mortality. Eur Heart J Acute Cardiovasc Care. (2017) 6:254–61. doi: 10.1177/2048872616633882
4. Terkelsen CJ, Jensen LO, Tilsted H-H, Trautner S, Johnsen SP, Vach W, et al. Health care system delay and heart failure in patients with ST-segment elevation myocardial infarction treated with primary percutaneous coronary intervention: follow-up of population-based medical registry data. Ann Intern Med. (2011) 155:361–7. doi: 10.7326/0003-4819-155-6-201109200-00004
5. Menees DS, Peterson ED, Wang Y, Curtis JP, Messenger JC, Rumsfeld JS, et al. Door-to-balloon time and mortality among patients undergoing primary PCI. N Engl J Med. (2013) 369:901–9. doi: 10.1056/NEJMoa1208200
6. Beygui F, Castren M, Brunetti ND, Rosell-Ortiz F, Christ M, Zeymer U, et al. Pre-hospital management of patients with chest pain and/or dyspnoea of cardiac origin. A position paper of the Acute Cardiovascular Care Association (ACCA) of the ESC. Eur Heart J Acute Cardiovasc Care. (2020) 9:59–81. doi: 10.1177/2048872615604119
7. Ferreira AS, Costa J, Braga CG, Marques J. Impact on mortality of direct admission versus interhospital transfer in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention. Rev Port Cardiol. (2019) 38:621–31. doi: 10.1016/j.repce.2019.11.012
8. Rathod KS, Jain AK, Firoozi S, Lim P, Boyle R, Nevett J, et al. Outcome of inter-hospital transfer versus direct admission for primary percutaneous coronary intervention: an observational study of 25,315 patients with ST-elevation myocardial infarction from the London Heart Attack Group. Eur Heart J Acute Cardiovasc Care. (2020) 9:948–57.2048872619882340. doi: 10.1177/2048872619882340
9. Rangé G, Chassaing S, Marcollet P, Saint-Étienne C, Dequenne P, Goralski M, et al. The CRAC cohort model: a computerized low cost registry of interventional cardiology with daily update and long-term follow-up. Rev Epidemiol Sante Publique. (2018) 66:209–16. doi: 10.1016/j.respe.2018.01.135
10. Hakim R, Revue E, Saint Etienne C, Marcollet P, Chassaing S, Decomis MP, et al. Does helicopter transport delay prehospital transfer for STEMI patients in rural areas? Findings from the CRAC France PCI registry. Eur Heart J Acute Cardiovasc Care. (2019) 9:958–65. doi: 10.1177/2048872619848976
11. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth Universal Definition of Myocardial Infarction (2018). J Am Coll Cardiol. (2018) 72:2231–64. doi: 10.1161/CIR.0000000000000617
12. Cutlip DE, Windecker S, Mehran R, Boam A, Cohen DJ, van Es G-A, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. (2007) 115:2344–51. doi: 10.1161/CIRCULATIONAHA.106.685313
13. de Luca G, van't Hof AWJ, de Boer M-J, Ottervanger JP, Hoorntje JCA, Gosselink ATM, et al. Time-to-treatment significantly affects the extent of ST-segment resolution and myocardial blush in patients with acute myocardial infarction treated by primary angioplasty. Eur Heart J. (2004) 25:1009–13. doi: 10.1016/j.ehj.2004.03.021
14. Francone M, Bucciarelli-Ducci C, Carbone I, Canali E, Scardala R, Calabrese FA, et al. Impact of primary coronary angioplasty delay on myocardial salvage, infarct size, and microvascular damage in patients with ST-segment elevation myocardial infarction: insight from cardiovascular magnetic resonance. J Am Coll Cardiol. (2009) 54:2145–53. doi: 10.1016/j.jacc.2009.08.024
15. Eagle KA, Lim MJ, Dabbous OH, Pieper KS, Goldberg RJ, van de Werf F, et al. A validated prediction model for all forms of acute coronary syndrome: estimating the risk of 6-month postdischarge death in an international registry. JAMA. (2004) 291:2727–33. doi: 10.1001/jama.291.22.2727
16. Stehli J, Martin C, Brennan A, Dinh DT, Lefkovits J, Zaman S. Sex differences persist in time to presentation, revascularization, and mortality in myocardial infarction treated with percutaneous coronary intervention. J Am Heart Assoc. (2019) 8:e012161. doi: 10.1161/JAHA.119.012161
17. Norhammar A Lindbäck J Rydén L Wallentin L Stenestrand U Register Register of Information and Knowledge about Swedish Heart Intensive Care Admission (RIKS-HIA). Improved but still high short- and long-term mortality rates after myocardial infarction in patients with diabetes mellitus: a time-trend report from the Swedish Register of Information and Knowledge about Swedish Heart Intensive Care Admission. Heart. (2007) 93:1577–1583. doi: 10.1136/hrt.2006.097956
18. Margolis G, Letourneau-Shesaf S, Khoury S, Pereg D, Kofman N, Keren G, et al. Trends and predictors of prehospital delay in patients undergoing primary coronary intervention. Coron Artery Dis. (2018) 29:373–7. doi: 10.1097/MCA.0000000000000608
19. Montalescot G, van't Hof AW, Lapostolle F, Silvain J, Lassen JF, Bolognese L, et al. Prehospital ticagrelor in ST-segment elevation myocardial infarction. N Engl J Med. (2014) 371:1016–27. doi: 10.1056/NEJMoa1407024
20. Bellemain-Appaix A, O'Connor SA, Silvain J, Cucherat M, Beygui F, Barthélémy O, et al. Association of clopidogrel pretreatment with mortality, cardiovascular events, and major bleeding among patients undergoing percutaneous coronary intervention: a systematic review and meta-analysis. JAMA. (2012) 308:2507–16. doi: 10.1001/jama.2012.50788
21. Bellemain-Appaix A, Kerneis M, O'Connor SA, Silvain J, Cucherat M, Beygui F, et al. Reappraisal of thienopyridine pretreatment in patients with non-ST elevation acute coronary syndrome: a systematic review and meta-analysis. BMJ. (2014) 349:g6269. doi: 10.1136/bmj.g6269
22. Bellemain-Appaix A, Bégué C, Bhatt DL, Ducci K, Harrington RA, Roe M, et al. The efficacy of early versus delayed P2Y12 inhibition in percutaneous coronary intervention for ST-elevation myocardial infarction: a systematic review and meta-analysis. EuroIntervention. (2018) 14:78–85. doi: 10.4244/EIJ-D-17-00852
23. Fabris E, van't Hof A, Hamm CW, Lapostolle F, Lassen JF, Goodman SG, et al. Impact of presentation and transfer delays on complete ST-segment resolution before primary percutaneous coronary intervention: insights from the ATLANTIC trial. EuroIntervention. (2017) 13:69–77. doi: 10.4244/EIJ-D-16-00965
24. Zijlstra F, Ernst N, de Boer M-J, Nibbering E, Suryapranata H, Hoorntje JCA, et al. Influence of prehospital administration of aspirin and heparin on initial patency of the infarct-related artery in patients with acute ST elevation myocardial infarction. J Am Coll Cardiol. (2002) 39:1733–7. doi: 10.1016/S0735-1097(02)01856-9
25. de Luca G, van't Hof AWJ, de Boer M-J, Hoorntje JCA, Gosselink ATM, Dambrink J-HE, et al. Impaired myocardial perfusion is a major explanation of the poor outcome observed in patients undergoing primary angioplasty for ST-segment-elevation myocardial infarction and signs of heart failure. Circulation. (2004) 109:958–61. doi: 10.1161/01.CIR.0000120504.31457.28
26. Hafiz AM, Naidu SS, DeLeon J, Islam S, Alkhatib B, Lorenz M, et al. Impact of first contact on symptom onset-to-door time in patients presenting for primary percutaneous coronary intervention. Am J Emerg Med. (2013) 31:922–7. doi: 10.1016/j.ajem.2013.03.005
27. Valgimigli M, Frigoli E, Leonardi S, Vranckx P, Rothenbühler M, Tebaldi M, et al. Radial vs. femoral access and bivalirudin vs. unfractionated heparin in invasively managed patients with acute coronary syndrome (MATRIX): final 1-year results of a multicentre, randomised controlled trial. Lancet. (2018) 392:835–48. doi: 10.1016/S0140-6736(18)31714-8
Keywords: ST-elevation myocardial infarction, Pre-hospital, percutaneous coronary intervention, mortality, system delays
Citation: Beygui F, Roule V, Ivanes F, Dechery T, Bizeau O, Roussel L, Dequenne P, Arnould M-A, Combaret N, Collet JP, Commeau P, Cayla G, Montalescot G, Benamer H, Motreff P, Angoulvant D, Marcollet P, Chassaing S, Blanchart K, Koning R and Rangé G (2022) Indirect Transfer to Catheterization Laboratory for ST Elevation Myocardial Infarction Is Associated With Mortality Independent of System Delays: Insights From the France-PCI Registry. Front. Cardiovasc. Med. 9:793067. doi: 10.3389/fcvm.2022.793067
Received: 11 October 2021; Accepted: 09 February 2022;
Published: 11 March 2022.
Edited by:
Tommaso Gori, Johannes Gutenberg University Mainz, GermanyReviewed by:
Adel Aminian, Center Hospitalier Universitaire de Charleroi, BelgiumCopyright © 2022 Beygui, Roule, Ivanes, Dechery, Bizeau, Roussel, Dequenne, Arnould, Combaret, Collet, Commeau, Cayla, Montalescot, Benamer, Motreff, Angoulvant, Marcollet, Chassaing, Blanchart, Koning and Rangé. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Farzin Beygui, YmV5Z3VpLWZAY2h1LWNhZW4uZnI=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.