 Guigao Guo
Guigao Guo Shucheng Liang
Shucheng Liang Zeyu Guan2*
Zeyu Guan2*
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Cardiovasc. Med., 16 November 2022
Sec. Thrombosis and Haemostasis
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.1070806
This article is part of the Research TopicEffects of Oral Anticoagulant Therapy in Atrial Fibrillation Patients with ComorbiditiesView all 15 articles
Background: Several studies have summarized the clinical performance of direct oral anticoagulants (DOACs) in atrial fibrillation (AF) patients with mitral stenosis or aortic stenosis. The significance of this review was to provide clinicians the latest update of the clinical application of DOACs in managing this specific population.
Methods: Literatures from the PubMed database up to July 2022 were screened for inclusion. Studies on the effect of DOACs in patients suffering from AF with mitral or aortic stenosis were assessed for further selection.
Results: Results from four studies were gathered: the RISE MS trial, the DAVID-MS study, and two observational studies. In the Korean observational study with a 27-month follow-up duration and a sample population consisted of patients with mitral stenosis and AF, the thromboembolic events happened at a rate of 2.22%/ year in the DOAC group and 4.19%/year in the warfarin group (adjusted hazard ratio: 0.28; 95% CI: 0.18–0.45). Intracranial hemorrhage occurred at rates of 0.49% and 0.93% in the DOAC and the warfarin groups, respectively (adjusted hazard ratio: 0.53; 95% CI: 0.22–1.26). In the Danish observational study, which had a sample pool with AF patients with aortic stenosis, reported that the adjusted hazard ratios for thromboembolism and major bleeding were 1.62 (95% CI, 1.08–2.45) and 0.73 (95% CI, 0.59–0.91) for DOACs compared with warfarin during 3 years of follow-up. In the RISE-MS trial involving AF patients with mitral stenosis, there were no differences in ischemic stroke, systemic embolic events, or major bleeding between the rivaroxaban vs. warfarin groups during a 1-year follow-up as well as equal rate of increased thrombogenicity in the left atrial appendage at 6 months. The rate of silent cerebral ischemia at 12 months was higher in the warfarin group (17.6%) than that in the rivaroxaban group (13.3%).
Conclusions: Current published studies supported DOACs' effectiveness in preventing thromboembolism in patients of AF with mitral or aortic stenosis. Further clinical trials could confirm these findings.
Valvular heart disease (VHD) has a rising prevalence in the elderly population over 75 years old (1). Among the moderate-to-severe VHDs, mitral or aortic stenosis happen with rates of 11 and 9%, respectively. Mitral stenosis (MS) is the most common valve stenosis, characterized by the narrowing of the mitral valve, which is crucial to prevent backflow from the left ventricle, followed by the occurrence of life-threatening complications such as atrial fibrillation (AF) and heart failure (2). Aortic stenosis (AS) is featured by the narrowing of the aortic valve which subsequently restricts the ejection of blood from the left ventricle, leading to high ventricular pressure and serious complications like AF (3). It has been shown that patients develop AF associated with MS and AS in a rate of 66.6% (4) and >9% (5) respectively, of which 3–7.5% of the patients are complicated by thromboembolic stroke.
Current guidelines of anticoagulation for AF in patients with non-valvular heart disease recommend that warfarin, a vitamin-K-dependent anticoagulant (VKA), is the drug of choice (6–8). However, such guidelines do not include AF combined with VHDs like mitral or aortic stenosis, which leaves patients developing both VHDs and AF with less therapeutic options beyond traditional warfarin administration. There is an urgent need for the establishment of a more inclusive guideline that provides alternative anticoagulation involving the usage of direct oral anticoagulants (DOACs) for patients with both VHD and AF (9). More recent studies have shown that DOACs are superior to warfarin for the prevention of systemic embolism in patients with AF (10–14), and even have a significant reduction in intracranial hemorrhage (12, 15–19). The better effect of DOACs compared with warfarin is also found in the AF specific population (20–24) and is well supported by cohort studies (25–28). However, only a few have specifically studied the efficacy and safety outcomes of DOACs compared with warfarin in AF patients with MS or AS (29–33). In this review, we discussed all the relevant studies regarding the effect of DOACs in AF patients with MS or AS.
Two investigators conducted independent searches on online database. Combinations of the following keywords were used to generate a search for relevant articles on the PubMed database up to July 2022: dabigatran, rivaroxaban, apixaban, edoxaban, direct oral anticoagulants, novel anticoagulants, DOAC, NOAC, warfarin, atrial fibrillation, mitral stenosis, aortic stenosis, and valvular heart disease. Observational studies or randomized controlled trials (RCTs) were selected if they satisfied the following criteria: AF patients with mitral or aortic stenosis treated with DOACs compared with warfarin.
A total of 698 articles were identified from the database for initial screening, 30 of which met the inclusion criteria and were retrieved for full-text article reading. Upon assessment for eligibility, 19 articles were excluded for not being either a RCT or observational study, seven articles were removed due to irrelevance. Only four articles eventually out of 30 matched the criteria and were included in this review. Among the four articles reviewed, two are observational in design, both are multicenter retrospective cohort studies, one using 1 to 1 propensity score matching, the other one using target trial emulation. The rest two studies are RCTs, one of which is still a protocol, with results not yet available. The whole search and selection process is summarized in Figure 1. The study design and baseline information of the studies are demonstrated in Table 1.

Table 1. The baseline data of the included studies in this review.
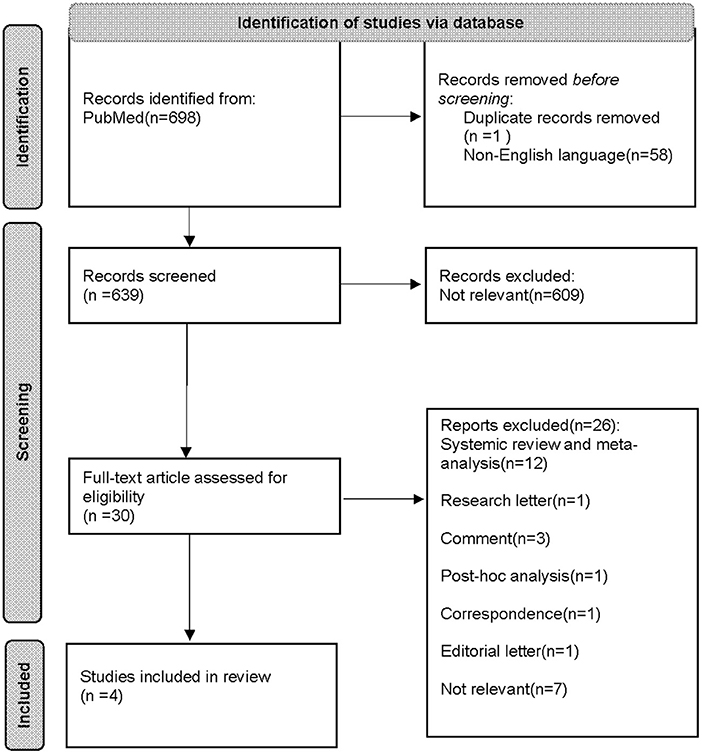
Figure 1. PRISMA flow diagram that summarizes the literature search process.
Among four studies included in this review (29–31, 33), the primary outcomes and safety outcomes are summarized in Table 1. The Korean observational study by Kim et al. (33) included 2,230 AF patients with MS, of which 30.6% were males. It was reported that thromboembolic events occurred at a rate of 2.22%/year in the DOAC group and 4.19%/year in the warfarin group (adjusted hazard ratio for DOACs vs. warfarin: 0.28; 95% CI: 0.18–0.45), while intracranial hemorrhage occurred in 0.49% in DOACs group and 0.93% in warfarin group (adjusted hazard ratio for DOACs vs. warfarin: 0.53; 95% CI: 0.22–1.26). The incidence rates of all-cause death were 3.45%/year in the DOAC arm and 8.08%/year in the warfarin arm. The overall survival curve showed a lower all-cause death in the DOAC group compared with the warfarin group. The estimated 3-year major bleeding-free survival was 87.6% for DOACs and 83.6% for warfarin. In the RISE-MS pilot RCT (29), 37 patients with AF and MS were recruited and randomized into either rivaroxaban (n = 18) or warfarin (n = 19) groups. This study reported no symptomatic ischemic stroke or systemic embolic events during the 1-year follow-up. For the safety outcomes, there was no major bleeding in neither group, but 1 clinically relevant nonmajor bleeding in the rivaroxaban group which was explained by increased menstrual bleeding. For exploratory outcomes, the rates of increased thrombogenicity in the left atrial appendage (LAA) assessed by transesophageal echocardiography (TEE) at 6 months and silent cerebral ischemia at 12 months assessed by brain magnetic resonance imaging (MRI) were explored. There were 11 patients in each group agreed to undergo the TEE assessment. There were 15 patients in the rivaroxaban group and 17 patients in the warfarin group accepted the MRI assessment. As results, both groups reported 27.2% rates of increased LAA thrombogenicity, whereas the rates of silent cerebral ischemia were 13.3 and 17.6% in the rivaroxaban and warfarin groups, respectively. Zhou et al. (31) published the protocol of the DAVID-MS trial on the effect of dabigatran vs. warfarin in patients with AF and MS.
The Danish observational study by Melgaard et al. (30) included 3,726 patients with AF and AS who had been prescribed for either a DOAC (n = 2,357) or warfarin (n = 1,369). During a median follow-up 14 months, the adjusted hazard ratio for thromboembolism was 1.62 (95% CI, 1.08–2.45) for DOACs compared with warfarin. The estimated 3-year thromboembolic-free survival was 94% in the DOACs group and 96% for the warfarin group. For the safety outcomes, the adjusted hazard ratio for major bleeding was 0.73 (95% CI, 0.59–0.91) for DOACs compared with warfarin.
One of the earliest studies looking into the effect of DOACs in patients with MS was conducted by Kim et al. (33) in 2019. This study presented a retrospective analysis to validate the effectiveness and safety outcomes of DOACs vs. warfarin in patients with MS. Patients were selected using the Korean health insurance database between 2008 and 2017 that were identified with AF and MS. A total of 2,230 patients were enrolled with matching baseline characteristics and 1:1 propensity score matching, of which patients in the DOACs or warfarin group were divided evenly. The primary outcomes of interest were ischemic stroke and systemic embolism over a follow-up of 27 months, and the safety outcomes were intracranial hemorrhage and all-cause death over the same course of follow-up. Thromboembolic events happened in rates of 4.19% per year and 2.22% per year and intracranial bleeding occurred in rates of 0.93% per year and 0.49% per year in warfarin and DOACs groups, respectively. Although the results seemed to support that DOACs were more effective and safer than warfarin, since the use of DOACs was off-label administered, it was difficult to overcome the confounding factors given a narrow range of baseline characteristics. Moreover, comparing to RCTs, observational retrospective studies have less restrictions as well as less consistency in terms of experimental design due to the fact that the data gathered was collected from different healthcare providers. Such characteristics of all observational analysis make them prone to selection bias. Therefore, results from such observational study should be interpreted critically and the data should only be used for “hypothesis-generating”.
In another observational study conducted in 2021, Melgaard et al. (30) collected data from Danish nationwide registries between 2013 and 2018 with the intent to compare effectiveness and safety of DOACs with warfarin in patients with AF and AS. Similar to the situation regarding treatment for patients with both AF and MS, there is lack of information and update about the guidelines on the usage of DOACs for patients carrying AF and AS. Melgaard et al. has highlighted the necessity of exploring the efficacy of DOACs for such indication in the observational study. A total of 3,726 patients with AF and AS satisfied selection criteria, in which 2,357 patients initiated DOACs and 1,369 patients used warfarin. Throughout 3 years of follow-up, thromboembolism happened in a rate of 3.3% in the DOAC group and 2.6% in the warfarin group, indicating a higher risk of thromboembolism in treatment with DOACs, whereas major bleeding occurred in a rate of 13% and 7.8% in the DOACs and warfarin groups, respectively. A major drawback of this study is its non-randomized design, which is common in every observational study as discussed above, making confounding factors unavoidable. Another limitation is that even though the comparison is between DOACs and warfarin, the study did not specifically compare two single drugs. Instead, patients prescribed with apixaban, dabigatran, edoxaban, and rivaroxaban were all counted into analysis, which potentially increased heterogenicity. Inarguably, this study provided new information regarding the use of DOACs in patients with AF and complicated with AS. However, the lack of randomization renders it unpowerful to draw any definite conclusion.
The RISE MS is a pilot RCT (29) initiated in Rajaie Cardiovascular Medical and Research Center, Tehran, Iran. From May 2019 to February 2020, researchers of the study recruited 37 patients 18 to 75 years old out of a pool of 237 and they were subsequently randomized to receive either rivaroxaban 20 mg daily or warfarin (with a target international normalized ratio [INR] of 2–3) in a 1:1 ratio. Based on the inclusion criteria, the recruited patients must be diagnosed with moderate-to-severe MS and AF within the prior 12 months. The exclusion criteria excluded all the patients with high risk of bleeding, left atrial thrombi, renal impairments, or allergies to DOACs or VKA. The dosages of drugs were tightly monitored. Patients who had never been administered with anticoagulants were monitored with shorter intervals until reaching a therapeutic INR level. The primary outcomes consisted of symptomatic ischemic strokes and systemic embolic events occurred during the 12-month follow-up. TEE and brain MRI were taken at the beginning of the study, the 6th and 12th month after randomization and the results were used to evaluate thrombogenicity in the LAA and silent cerebral ischemia, respectively. There are several limitations in the study. First, the small sample size made it difficult to report robust results for primary outcomes. Furthermore, the study was discontinued for two reasons. The first reason indicated that COVID-19 was associated with higher risk of thrombotic complications. The second reason was local COVID-19 restrictions rendered a rigorous and consistent follow-up impossible. The COVID-19 restrictions also limited the patient participation in imaging examinations due to the concerns of COVID-19 contamination in the imaging center. The authors also highlighted a concern in patient enrollment. Since almost all the patients were advised with their family practitioner, sever patients with moderate to severe MS refused to participate in the study, which could become a major selection bias and confront outcome analysis. Despite the limitations, the study has generated new clinical data for the application of DOACs. The primary outcome results supported that DOACs were at least as effective as VKAs for lowering thrombotic risks in AF patients with moderate to severe MS.
With the urgency of filling the knowledge gap regarding DOACs' efficacy in treating patients with AF and MS, Zhou et al. (31) has submitted a protocol of dabigatran for stroke prevention in AF patients with moderate or severe MS (the DAVID-MS trial). According to the protocol, this will be the first open-label, multicenter, randomized clinical trial to compare the efficacy and safety of dabigatran and warfarin therapy for stroke prevention in patients with AF and moderate or severe MS. The targeted patients are those with AF aged 18 or over with moderate to severe MS without schedule for valvular intervention in the coming 12 months. Patients will be randomized in a 1:1 ratio to receive either two-doses of dabigatran (110 mg or 150 mg two times per day) or warfarin with an INR of 2–3 along with a follow-up of 12 months. The primary outcomes compose of stroke and systemic embolism and the secondary outcomes include ischaemic stroke, intracranial hemorrhage, and major bleeding. The sample size is estimated to require 686 participants and the study will be conducted mainly in Hong Kong and Mainland China. It is worth mentioning that Zhou et al. decided to use dabigatran as a comparison to warfarin not only because dabigatran appears to be more effective in stroke prevention with less intracranial bleeding than warfarin but also because of the availability of its antidote idarucizumab, granting more protection for patients involved in the DAVID-MS trial.
In summary, the guidelines for DOACs regarding its administration in AF with mitral or aortic stenosis are lacking. On the other hand, only a handful of works are done to fill in the knowledge gap. As far, there are four studies completed to explore the efficacy of DOACs in treating patients with AF and MS or AS. The two observational studies, one conducted in Korean (33) and the other one in Denmark (30), looked at the effect of DOACs in reducing thromboembolic events in patients with AF and MS or AS, respectively. The RISE-MS is a pilot RCT (29) to compare rivaroxaban to warfarin about their ability to lower risk of thromboembolism in patients with both AF and MS. DAVID-MS is a registered RCT to compare dabigatran to warfarin for the same indication above. The DAVID-MS trial (31), however, has not yet been conducted. Both the observational study by Kim et al. and the pilot RCT have reported non-inferior efficacy of DOACs compared to warfarin. The observational study conducted by Melgaard et al. (30), however, reported that DOACs are associated with higher rate of thromboembolism than warfarin. The two observational studies were subject to a variety of bias due to their retrospective nature. Therefore, their results should merely be considered as hypothesis generating but not clinically significant. The pilot RCT supported that DOACs possessed higher efficacy than warfarin, yet the study was limited to small sample size. Although DOACs have already been used widely as alternatives to traditional blood thinners such as warfarin in treatments for patients with AF, its applications in other indications like AF complicated with MS or AS have only been lightly explored. Such knowledge gap awaits elucidation as it will potentially open new windows for patients suffering from both AF and MS or AS (32).
Although DOACs have been branded and extensively used for more than a decade, there is always ongoing research regarding their safety efficacy. A recent study conducted in Italy found that the use of DOACs is associated with higher rate of recurrent thromboembolism than VKA in patients with antiphospholipid syndrome (34). In this review, no study has included antiphospholipid syndrome in their baseline characters. Recruiting patients with the syndrome would overestimate the bleeding risk and undermine the safety outcome. Therefore, in future observational studies, researchers must consider the syndrome in baseline characteristics to avoid bias.
Another baseline characteristic that can help to optimize baseline characteristic design is VKORC genotyping (35). Patients with the VKORC gene are more susceptible to warfarin overdose, as warfarin has a narrow therapeutic window. Genetic screening on these patients can help clinicians to estimate dosages more precisely and lower the effect of VKORC polymorphism on the time required to reach targeted INR and the time required to reach stable therapeutic plasma concentration for warfarin so to lower the risk of hemorrhage (36). In the mentioned studies of our review, no information was given regarding patients' VKORC polymorphism, which could be a potential confounding factor as some patients in the warfarin arm were more likely to bleeding upon warfarin treatment (37). This could overstate the bleeding risk of warfarin compared to DOACs. Hence, we suggested that in further studies, researchers need to normalize the results along with patients' VKORC screening results.
A retrospective review conducted in Denmark reported inclusively on all-cause mortality, stroke, and bleeding in patients with AF and valvular heart disease and treated with either rivaroxaban, apixaban, or VKA (38). The goal of the study was to compare the risk of the mentioned safety event in order to infer which drug is safer. The results showed that there was non-significant absolute 2-year risk difference between VKA and DOACs groups for all outcomes measured, suggesting that apixaban and rivaroxaban possess at least equal, if not better, safety profile as VKA. Nevertheless, the limitations in this study were obvious. For instance, there was a possible detection bias that patients treated with VKA were more often in contact with practitioners and professionals and were therefore more likely to be diagnosed with arisen problems, making the VKA arm more subject to false positive detection. The other problem was that populations in the study were not stratified according to their VHD degree. This proposed a major problem in data analysis since patients with more severe VHD are more susceptible to bleeding. Therefore, if patients with different VHD severity were mixed in the same group instead of being stratified, the total bleeding events could be exaggerated or understated as there were more moderate-severe VHD patients or mild-moderate VHD patients, respectively.
In the INVICTUS trial, which is the most recent RCT of DOACs, the efficacy and safety of rivaroxaban and warfarin for stroke prevention in patients who had AF due to rheumatic heart disease have been updated (39). Patients with AF and echocardiographically diagnosed rheumatic heart disease and satisfy the following criteria were enrolled: CHA2DS2VASc score of at least 2 (with higher scores suggesting a higher risk of stroke) and a mitral-valve area of no more than 2 cm2. In the end, there were over 80% of enrolled members in both arms with moderate-to-severe mitral stenosis. The patients were randomized in a 1:1 ratio to receive either 20 mg daily rivaroxaban or VKA. The efficacy outcomes included total stroke and systemic embolism and safety outcomes included myocardial infarction and death from vascular causes. The results showed that of 4,531 patients included in the on-treatment analysis, the occurrence rates of all stroke events of rivaroxaban and VKA groups were 1.39 and 0.87%, respectively. The rates of fatal bleeding, however, were 0.07 and 0.22 in rivaroxaban and VKA groups, respectively. In addition, VKA group also showed higher restricted mean survival time compared to rivaroxaban group, which was 1,686 days vs. 1,619 days (p = 0.002).
In connection to our review, since the INVICTUS enrolled mostly MS patients with rheumatic heart disease and AF, we can make inference accordingly. Compared to the observational studies in our review, the data from INVICTUS supported otherwise opposite conclusion as the INVICTUS have suggested that for preventing thromboembolic events in rheumatoid heart disease patients with AF, VKA is associated with better efficacy and lower mortality rate compared to rivaroxaban, although with higher bleeding rate. However, the authors of INVICTUS indicated that there was no relation between AF-related stroke prevention and reduced mortality rate. VKA also did not slow down the deterioration of heart-valve, which suggested that the better efficacy in preventing stroke and lower mortality in the VKA group was not related to MS progression. On the other hand, although the rivaroxaban group had higher mortality rate, there was no evidence to suggest rivaroxaban increased mortality among the patients, as it has been shown that rivaroxaban lowers mortality substantially in patients with atherosclerotic vascular disease (40). Hence, if VKA did not lower mortality through optimizing AF-related stroke prevention or slowing MS progression, it appeared more likely that VKA had a direct effect on the disease process of rheumatic heart disease. This information is important because if the efficacy of stroke prevention of VKA or DOACs is dependent on rheumatic heart disease progression, such condition should strictly be included as one of the exclusion criteria when studying the effectiveness of stroke prevention of DOACs vs. VKA in patients with AF and MS.
Among the reviewed studies (29–31, 33), two of them showed non-inferiority of DOACs to warfarin in treating patients with AF and mitral or aortic stenosis, and one observational study showed the opposite results. Due to their own limitations, the use of DOACs in AF patients with MS or AS is still controversial. A more adequately designed RCT with a larger sample size is needed to verify the results from the previous studies. Warfarin would remain the drug of choice for such patients as per the guideline, due to the lack of clinical data, until a more definitive trial showed otherwise.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rostagno C. Heart valve disease in elderly. World J Cardiol. (2019) 11:71–83. doi: 10.4330/wjc.v11.i2.71
2. Iung B, Leenhardt A, Extramiana F. Management of atrial fibrillation in patients with rheumatic mitral stenosis. Heart. (2018) 104:1062–8. doi: 10.1136/heartjnl-2017-311425
3. Burup K C, Jensen J S, Sogaard P, Carstensen HG, Mogelvang R. Atrial fibrillation in aortic stenosis–echocardiographic assessment and prognostic importance. Cardiovasc Ultrasound. (2012) 10:38. doi: 10.1186/1476-7120-10-38
4. Dhungana S P, Nepal R, Ghimire R. Prevalence and factors associated with atrial fibrillation among patients with rheumatic heart disease. J Atr Fibrillation. (2019) 12:2143. doi: 10.4022/jafib.2143
5. Dahl J S, Brandes A, Videbæk L, Kim K, Ehara N, Kobori A, et al. Atrial fibrillation in severe aortic valve stenosis — association with left ventricular left atrial remodeling. IJC Heart & Vessels. (2014) 4:102–7. doi: 10.1016/j.ijchv.2014.06.006
6. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. (2020). ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2021) 42:373–498. doi: 10.1093/eurheartj/ehaa612
7. Steffel J, Verhamme P, Potpara T S, Albaladejo N, Antz M, Desteghe L, et al. The 2018 European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. Eur Heart J. (2018) 39:1330–93. doi: 10.1093/europace/euab065
8. January C T, Wann L S, Calkins H, Chen LY, Cigarroa J, Cleveland J, et al. (2019). AHA/ACC/HRS focused update of the (2014). AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the heart rhythm society in collaboration with the society of thoracic surgeons. Circulation. (2019) 140:R665. doi: 10.1161/CIR.0000000000000665
9. Verhamme P, Alexander Yi B, Segers A, Salter J, Bloomfield D, BüllerHR, et al. Abelacimab for prevention of venous thromboembolism. N Engl J Med. (2021) 385:1821–3. doi: 10.1056/NEJMc2114895
10. Beyer-Westendorf J, Schellong SM, Gerlach H, Rabe E, Weitz JI, Jersemann K, et al. (2017). Prevention of thromboembolic complications in patients with superficial-vein thrombosis given rivaroxaban or fondaparinux: THE open-label, randomised, non-inferiority surprise phase 3B trial. Lancet Haematol. 4. doi: 10.1016/S2352-3026(17)30014-5
11. Fredenburgh JC, Weitz JI. New anticoagulants: moving beyond the direct oral anticoagulants. J Thromb Haemost. (2020) 19:20–9. doi: 10.1111/jth.15126
12. Giugliano RP, Ruff CT, Braunwald E, Murphy SA, Wiviott SD, Halperin JL, et al. Edoxaban vs. warfarin in patients with atrial fibrillation. N Engl J Med. (2013) 369:2093–104. doi: 10.1056/NEJMoa1310907
13. Raskob GE, van Es N, Verhamme P, Carrier M, Di Nisio M, Garcia D, et al. Edoxaban for the treatment of cancer-associated venous thromboembolism. N Engl J Med. (2018) 378:615–24. doi: 10.1056/NEJMoa1711948
14. Weitz JI, Strony J, Ageno W, Gailani D, Hylek EM, Lassen MR, et al. Milvexian for the prevention of venous thromboembolism. N Engl J Med. (2021) 385:2161–72. doi: 10.1056/NEJMoa2113194
15. Goto S. Goto S. A patient-level meta-analysis: the end of the era of direct oral anticoagulant developmental trials in patients with atrial fibrillation? Circulation. (2022) 145:256–8. doi: 10.1161/CIRCULATIONAHA.121.058159
16. Granger CB, Alexander JH, McMurray JJV, Lopes RD, Hylek EM, Hanna M, et al. Apixaban vs. warfarin in patients with atrial fibrillation. N Engl J Med. (2011) 365:981–92. doi: 10.1056/NEJMoa1107039
17. Patel M R, Mahaffey K W, Garg J, Pan G, Singer D, Hacke W, et al. Rivaroxaban vs. warfarin in nonvalvular atrial fibrillation. N Engl J Med. (2011) 365:883–91. doi: 10.1056/NEJMoa1009638
18. Connolly S J, Ezekowitz M D, Yusuf S, Eikelboom J, Oldgren J, Parekh A, et al. Dabigatran vs. warfarin in patients with atrial fibrillation. N Engl J Med. (2009) 361:1139–51. doi: 10.1056/NEJMoa0905561
19. Liu F, Yang Y, Cheng W, Ma J, Zhu W. Reappraisal of non-vitamin k antagonist oral anticoagulants in atrial fibrillation patients: a systematic review and meta-analysis. Front Cardiovasc Med. (2021) 8:757188. doi: 10.3389/fcvm.2021.757188
20. Liu F, Xu Z, Luo J, Yu P, Ma J, Yuan P, et al. Effectiveness and safety of DOACs vs. VKAs in AF patients with cancer: evidence from randomized clinical trials and observational studies. Front Cardiovasc Med. (2021) 8:766377. doi: 10.3389/fcvm.2021.766377
21. Chen C, Cao Y, Zheng Y, Dong Y, Ma J, Zhu W, et al. Effect of rivaroxaban or apixaban in atrial fibrillation patients with stage 4–5 chronic kidney disease or on dialysis. Cardiovasc Drugs Ther. (2021) 35:273–81. doi: 10.1007/s10557-021-07144-8
22. Liao X, Fu Y, Ma J, Li X, Tan Y, Li J. Non-vitamin K antagonist oral anticoagulants vs. warfarin in patients with atrial fibrillation and peripheral artery disease: a systematic review and meta-analysis. Cardiovasc Drugs Ther. (2020) 34:391–9. doi: 10.1007/s10557-020-06962-6
23. Liu X, Xu Z, Yu P, Yuan P, Zhu W. Non-vitamin K antagonist oral anticoagulants in secondary stroke prevention in atrial fibrillation patients: an updated analysis by adding observational studies. Cardiovasc Drugs Ther. (2020) 34:569–78. doi: 10.1007/s10557-020-06961-7
24. Fu L, Zhu W, Huang L, Hu J, Ma J, Lip G, et al. Efficacy and safety of the use of non-vitamin k antagonist oral anticoagulants in patients with ischemic heart disease: a meta-analysis of phase III randomized trials. Am J Cardiovasc Drugs. (2019) 19:37–47. doi: 10.1007/s40256-018-0299-7
25. Briasoulis A, Inampudi C, Akintoye E, Alvarez P, Panaich S, VaughanSarrazin M. 2018 safety and efficacy of novel oral anticoagulants vs. warfarin in Medicare beneficiaries with Atrial Fibrillation and valvular heart disease. Am Heart J. 7:8. doi: 10.1161/JAHA.118.008773
26. Dawwas GK, Dietrich E, Cuker A, Barnes GD, Leonard CE, Lewis JD. Effectiveness and safety of direct oral anticoagulants vs. warfarin in patients with Valvular Atrial Fibrillation. Ann Intern Med. (2021) 174:910–9. doi: 10.7326/M20-6194
27. Li H-J, Lin S-Y, Lin F-J, Hung C-S, Wang C-C. Effectiveness and safety of non-vitamin K antagonist oral anticoagulants in Asian patients with atrial fibrillation and valvular heart disease. Curr Med Res Opin. (2021) 37:535–42. doi: 10.1080/03007995.2021.1885365
28. Moon I, Lee SR, Choi E, Lee E, Jung J, Han K, et al. Non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation and valvular heart disease. J Clin Med. (2019) 8:1624. doi: 10.3390/jcm8101624
29. Sadeghipour P, Pouraliakbar H, Parsaee M, et al. RIvaroxaban in mitral stenosis (RISE MS): A pilot randomized clinical trial. Int J Cardiol. (2022) 356:83–6. doi: 10.1016/j.ijcard.2022.03.037
30. Melgaard L, Overvad TF, Jensen M, Christensen T, Lip G, Larsen T, et al. Effectiveness and safety of NOAC vs. warfarin in patients with atrial fibrillation and aortic stenosis. Am Heart J. (2021). 10:e022628. doi: 10.1161/JAHA.121.022628
31. Zhou M, Chan EW, Hai JJ, Wong C, Lau Y, Huang D, et al. Protocol, rationale and design of DAbigatran for Stroke PreVention In Atrial Fibrillation in MoDerate or Severe Mitral Stenosis (DAVID-MS): a randomised, open-label study. BMJ Open. (2020) 10:e38194. doi: 10.1136/bmjopen-2020-038194
32. Giugliano RP, O Gara PT. DOACs in patients with mitral stenosis and atrial fibrillation. J Am Coll Cardiol. (2019) 73:1132–4. doi: 10.1016/j.jacc.2018.12.048
33. Kim J Y, Kim S, Myong J, Kim Y, Kim T, Kim J, et al. Outcomes of direct oral anticoagulants in patients with mitral stenosis. J Am Coll Cardiol. (2019) 73:1123–31. doi: 10.1016/j.jacc.2018.12.047
34. Pastori D, Menichelli D, Cammisotto V, Pignatelli P. Use of direct oral anticoagulants in patients with antiphospholipid syndrome: a systematic review and comparison of the international guidelines. Front Cardiovasc Med. (2021) 8:715878. doi: 10.3389/fcvm.2021.715878
35. Al-Mahayri ZN, Al Jaibeji HS, Saab Y, Soliman K, Al-Gazali L, Patrinos GP, et al. VKORC1 variants as significant predictors of warfarin dose in Emiratis. Pharmacogenomics Res Pers Med. (2019) 12:47–57. doi: 10.2147/PGPM.S187350
36. Sridharan K, Sivaramakrishnan G. A network meta-analysis of CYP2C9, CYP2C9 with VKORC1 and CYP2C9 with VKORC1 and CYP4F2 genotype-based warfarin dosing strategies compared to traditional. J Clin Pharm Ther. (2020) 46:640–8. doi: 10.1111/jcpt.13334
37. Biswas M, Bendkhale SR, Deshpande SP, Thaker SJ, Kulkarni DV, Bhatia SJ, et al. Association between genetic polymorphisms of CYP2C9 and VKORC1 and safety and efficacy of warfarin: Results of a 5 years audit. Indian Heart J. (2018) 3:S13–S19. doi: 10.1016/j.ihj.2018.02.005
38. Strange JE, Sindet-Pedersen C, Staerk L, Grove EL, Gerds TA, Torp-Pedersen C, et al. All-cause mortality, stroke, and bleeding in patients with atrial fibrillation and valvular heart disease. Eur Heart J. (2020) 7:FI1. doi: 10.1093/ehjcvp/pvaa011
39. Connolly SJ, Karthikeyan G, Ntsekhe M, Haileamlak A, El Sayed A, El Ghamrawy A, et al. Rivaroxaban in rheumatic heart disease–associated atrial fibrillation. N Engl J Med. (2022) 387:978–88. doi: 10.1056/NEJMoa2209051
Keywords: direct oral anticoagulants, warfarin, atrial fibrillation, mitral stenosis, aortic stenosis
Citation: Guo G, Liang S, Guan Z and Zhu K (2022) Effect of direct oral anticoagulants in patients with atrial fibrillation with mitral or aortic stenosis: A review. Front. Cardiovasc. Med. 9:1070806. doi: 10.3389/fcvm.2022.1070806
Received: 15 October 2022; Accepted: 31 October 2022;
Published: 16 November 2022.
Edited by:
Wengen Zhu, First Affiliated Hospital of Sun Yat-Sen University, ChinaReviewed by:
Yalin Cao, Guizhou Provincial People's Hospital, ChinaCopyright © 2022 Guo, Liang, Guan and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shucheng Liang, bGlhbmdzaGNoMjAwMUBnbWFpbC5jb20=; Zeyu Guan, ZTM2MzAwNjkxMEBnbWFpbC5jb20=; Ke Zhu, MTMwNDQ2NTU4N0BxcS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.