
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 01 December 2022
Sec. Cardio-Oncology
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.1062858
This article is part of the Research TopicCardiovascular Sequelae of Chemotherapy and Radiotherapy in Cancer Survivors: Current evidence and perspectivesView all 10 articles
 María Torrente1,2*†
María Torrente1,2*† Mariola Blanco1†
Mariola Blanco1† Fabio Franco1
Fabio Franco1 Yago Garitaonaindia1
Yago Garitaonaindia1 Virginia Calvo1Ana Collazo-Lorduy1Lourdes Gutiérrez1Juan Cristóbal Sánchez1Aranzazu González-del-Alba1Roberto Hernández1Miriam Méndez1
Virginia Calvo1Ana Collazo-Lorduy1Lourdes Gutiérrez1Juan Cristóbal Sánchez1Aranzazu González-del-Alba1Roberto Hernández1Miriam Méndez1 Blanca Cantos1Beatriz Núñez1Pedro A. C. Sousa3Mariano Provencio1
Blanca Cantos1Beatriz Núñez1Pedro A. C. Sousa3Mariano Provencio1Background: Immune checkpoint inhibitors (ICIs) have revolutionized cancer treatment. However, despite their excellent therapeutic effect, these medications typically result in a broad spectrum of toxicity reactions. Immune-related cardiotoxicity is uncommon but can be potentially fatal, and its true incidence is underestimated in clinical trials. The aim of this study is to assess the incidence and identify risk factors for developing a cardiac event in patients treated with ICIs.
Methods: We conducted a single-institution retrospective study, including patients treated with ICIs in our center. The main outcomes were cardiac events (CE) and cardiovascular death.
Results: A total of 378 patients were analyzed. The incidence of CE was 16.7%, during a median follow-up of 50.5 months. The multivariable analysis showed that age, a history of arrhythmia or ischemic heart disease, and prior immune-related adverse events were significantly associated with CE.
Conclusion: CE during ICI treatment are more common than currently appreciated. A complete initial cardiovascular evaluation is recommended, especially in high-risk patients, being necessary a multidisciplinary approach of a specialized cardio-oncology team.
The hallmark of many cancers is their ability to avoid the host immune response, allowing cell proliferation and metastasis (1). Cytotoxic T lymphocyte-associated antigen-4 (CTLA-4) and programmed cell death protein (PD-1) are co-inhibitory T-cell surface molecules, which downregulate the immune response by attenuating T-cell activation, proliferation, and cytokine production (2, 3). The immune system employs these inhibitory pathways to maintain T-cell tolerance and prevent autoimmunity (4). Numerous cancer cells overexpress the programmed cell death ligand 1 (PD-L1) on their surface, which contributes to their immune evasion by enhancing their immune escape ability, resulting in a poor prognosis for the patient (5). Based on these inhibitory molecules, several monoclonal antibodies targeting these immune checkpoint pathways have been developed in the last decade.
Immune checkpoint inhibitors (ICIs) have revolutionized the therapeutic landscape of many hematological and solid tumors. Since the introduction of the first ICI, ipilimumab (human IgG1 k anti-CTLA-4 monoclonal antibody) in 2011, six additional ICIs have been approved for cancer therapy by regulatory agencies (6), becoming a mainstay in the treatment of several neoplasms, including non-small cell lung cancer (NSCLC) and malignant melanoma. ICIs have shown high and durable response rates, either alone or in combination with other therapies, improving the survival of patients with advanced-stage malignancies, historically endowed with a poor prognosis (7, 8).
However, these agents also produce a wide spectrum of immune-related adverse events (irAEs), mainly due to aberrant autoreactive T-cell activation (9). These immune-mediated toxicities may affect any organ or tissue, with the most frequently reported being the skin, gastrointestinal system, and endocrine system (10). The incidence of irAEs varies between CTLA-4 inhibitors and PD-1 inhibitors, being high-grade adverse events more common with the combination ICI therapy (11).
Immune-related cardiotoxicity is a potentially fatal irAE. Since the first specific case of ICI-associated cardiotoxicity was reported in 2014 (12), cardiotoxicity during ICI treatment has been increasingly reported (13–15). The current evidence available arises from pharmacovigilance databases, case reports, and retrospective series (16), but no randomized controlled trials have assessed the potential cardiotoxic role of ICIs. Among the various forms of ICI cardiotoxicities, myocarditis is the most frequently reported due to its high morbidity and mortality. Retrospective evaluation literature has estimated that the incidence of ICI-related myocarditis ranges from 0.09 to 1.14% (17, 18). Nevertheless, the true incidence of other cardiovascular effects of immunotherapy is uncertain. Immune-related cardiotoxicity involves almost all parts of the heart, being the myocardium the most sensitive to ICIs toxicity. The potential mechanism of ICI-mediated cardiac toxicity is not fully understood, but histological analysis has revealed that the infiltration of CD4+/CD8+ T-cells and macrophages in the heart tissue may play a key role in the pathogenesis (19). ICI-related cardiotoxicity can be inflammatory, including conditions such as pericarditis, myocarditis, and perimyocarditis, or non-inflammatory, including left ventricular dysfunction without myocarditis, Takotsubo-like syndrome, coronary vasospasm, arrhythmias, and myocardial infarction (20). Various reports have revealed that immune-related cardiotoxicity may occur early after exposure to an ICI, suggesting a potential predisposition to cardiotoxicity that is possibly associated with pre-existing cardiovascular risk factors (CVRF) (21). Likewise, as reported with other irAEs, a combined ICI therapy with anti-CTLA4 and anti-PD-1/PD-L1, significantly increases the risk of developing an immune-related CE (22), as well as previous administration of other cardiotoxic cancer therapies, such as anthracyclines, trastuzumab, thoracic radiotherapy, or antiangiogenic therapy.
In order to gain a more robust understanding of immune-related cardiotoxicity, we reviewed the incidence of CE developed during ICI treatment in our institution. In addition, we tried to assess the role of CVRF and other cancer therapies in the development of cardiac toxicity.
We conducted a single-institution retrospective study at the Puerta de Hierro-Majadahonda University Hospital in Madrid, Spain. Oncologic patients treated in our center with immune checkpoint inhibitors, either in monotherapy or in combination with chemotherapy or other therapies, were included from March 2014 to November 2020.
Clinical history from electronic health records was retrieved, and specific data were collected regarding demographics, previous CVRF, and oncological features such as specific tumor, histology, AJCC/UICC stage, treatments received (including type of chemotherapy and targeted therapies, with an emphasis on those with cardiotoxic effects), treatment-related toxicity, and outcomes (overall survival).
Cardiac events identified during or after immune checkpoint inhibition were electrocardiographic alterations (such as long QT syndrome, any grade bundle branch or atrioventricular blockades or atrial fibrillation), congestive heart failure, pulmonary embolism, acute coronary syndrome, pericarditis, and myocarditis. Treatment interruptions, hospitalizations due to cardiologic issues, and cardiac-related deaths were also identified.
The aim of the study was to determine the incidence of cardiac events in patients exposed to immune checkpoint inhibitors and to identify clinical factors for predicting the onset of these events.
Qualitative variables are expressed as an absolute value and percentage. Quantitative variables are expressed as the median and interquartile range (IQR). To test for clinical data categorical associations with cardiac event development, we performed a Chi-square test in variables such as sex, known CVRF (hypertension, diabetes, valve disease, chronic kidney disease, ischemic heart disease, previous history of arrhythmia, smoking habit, tumor location, previous potentially cardiotoxic drug exposure, previous chest radiotherapy, and tumor objective response). T-student test was used for age. To identify risk factors increasing the probability of CE, Cox models were constructed. Risk factors with a P-value lower than 0.05 in the univariable analysis were developed into multivariable models. Odds ratios (ORs) and 95% confidence intervals (CIs) were provided for the multivariable model. In line with recommendations, the cumulative incidence was designed up to the 95 percentile of follow-up duration.
Based on the results obtained in the multivariable analysis, as well as clinically important variables, we developed a predictive score for the risk of developing a cardiac event after immunotherapy exposure. The score calibration was assessed using the Hosmer–Lemeshow goodness-of-fit test as well as the discrimination through the area under the receiver operating characteristic curve.
All statistical analyses were performed using Stata version 23 software.
Ethical approval was granted by the Puerta de Hierro-Majadahonda University Hospital Clinical Research Ethics Committee. The study was carried out in accordance with the requirements expressed in the Declaration of Helsinki, as well as with the current legislation in Spain on conducting observational studies (Ministerial Order SAS/3470/2009).
Between March 2014 and November 2020, a total of 378 patients receiving ICIs treatment in our institution were analyzed. Of those, 134 were females (35.5%) and 244 were males (64.6%). The median age was 61 years old (p25–p75: 55–68).
Table 1 lists the main baseline characteristics of our cohort of patients. The most frequent comorbidities were hypertension (40.7%), dyslipidemia (30.4%), and type 2 diabetes (13.2%); 29.9% of patients were current smokers at the time of the analysis, and 51.3% were former smokers. Regarding other more specific CVRF, the most prevalent was peripheral vascular disease (17.2%), followed by history of coronary heart disease (5.0%), heart valve disease (5.0%), chronic renal failure (4.5%), and congestive HF (0.5%); 24 patients (6.4%) had history of arrhythmia being the most frequent atrial fibrillation (83.4%). In addition, 10.9% of the patients were receiving anticoagulants and 11.9% antiplatelet treatment. Only 41 (10.8%) patients had a family history of cardiovascular disease. In the cardiologic evaluation prior to the start of ICI treatment, 20 patients (5.3%) presented with alterations in cardiac contractility, and 25 (6.6%) had left ventricular hypertrophy in the echocardiographic assessment. Only 2 patients had evaluable cardiomegaly in chest X-ray.
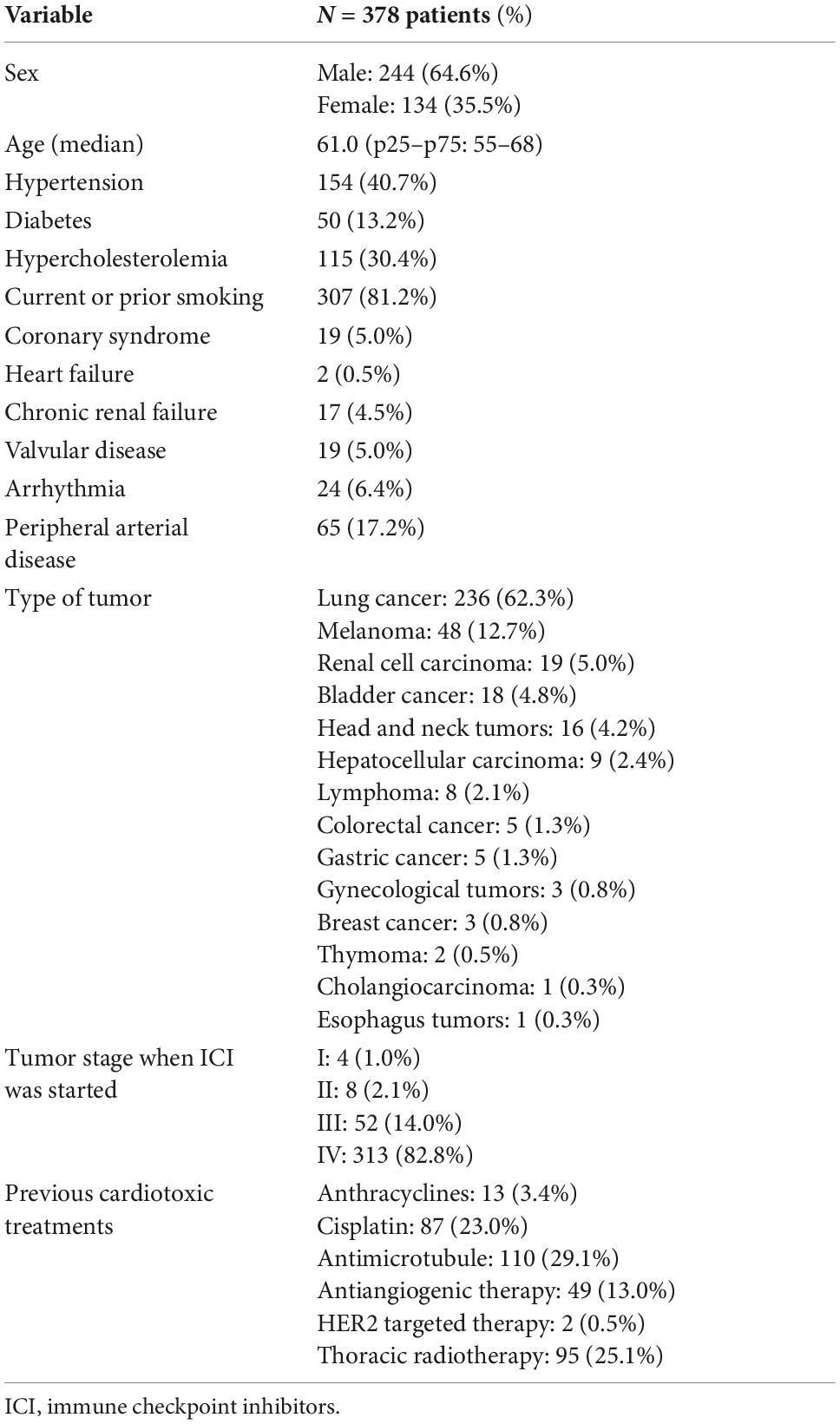
Table 1. Baseline characteristics of patients at the time of initial administration of immune checkpoint inhibitors.
Regarding tumor characteristics, most of the patients receiving ICI treatment were lung cancer patients (62.3%), followed by melanoma (12.7%), renal cell carcinoma (5.0%), urothelial carcinoma (4.8%), and head-and-neck tumors (4.2%). The predominant histology was adenocarcinoma (42.9%) followed by squamous cell carcinoma (20.6%) and melanoma (12.7%). Most of the patients were at stage IV of the disease (82.2%). 34.4% of patients received ICI in the first-line setting, in monotherapy, or in combination with other therapies. Regarding the type of ICI treatment administered, most of the patients received anti-PD1 drugs (64.8%), followed by anti-PDL1 drugs (9%) and anti-CTLA4 drugs (1.6% in monotherapy and 9.5% in combination with anti-PD1), with a median of 6 cycles per patient. Details on ICI treatment are listed in Table 2. When we evaluated the best response to ICIs by radiologic assessment, 32.3% of patients had a partial response, 13% stable disease, and 9.2% complete response. Nevertheless, most of the patients had progressive disease at first evaluation (43.1%). At the time of the analysis, 335 patients (88.6%) had interrupted the ICI therapy, most of them due to disease progression (51.6%) or death (10.6%), end of treatment after 2 years completion (14.2%) and only 37 (9.8%) due to immune-related toxicity. The most frequent irAE was gastrointestinal (18.9%), followed by skin disorders (16.5%) and pneumonitis (16.5%). 45 patients experienced grade 3 adverse events (11.9%). Of note, only one patient interrupted ICI treatment due to SARS-CoV-2 infection.
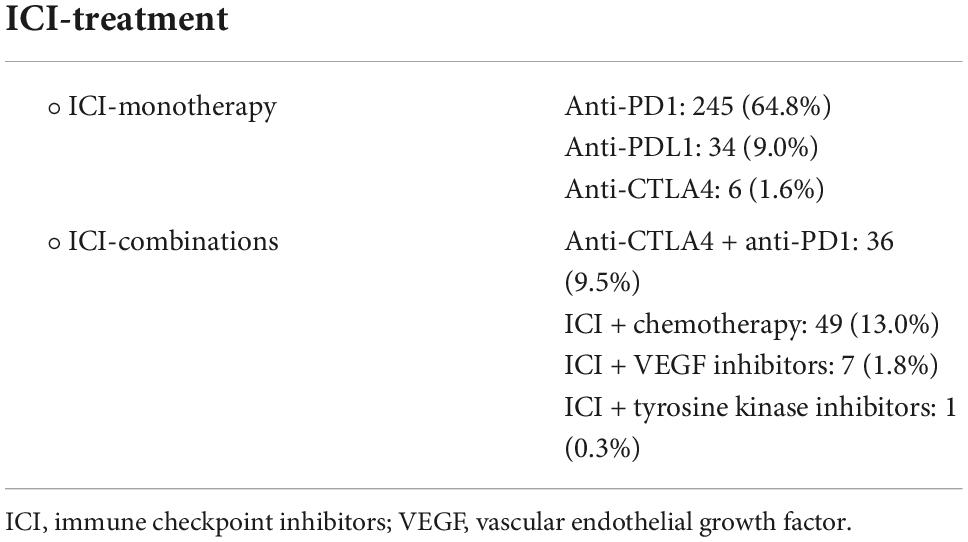
Table 2. Type of ICI treatment received.
As abovementioned, most patients presented advance stage of the disease upon ICIs initiation, and had progressed to several lines of treatment, including potentially cardiotoxic drugs. Specifically, 3.4% of patients had previously received anthracyclines, 23.0% cisplatin, 29.1% antimicrotubule agents, 13% antiangiogenic therapy, and only 0.5% (2 patients) anti-HER2 therapy. Regarding radiotherapy, 95 patients (25.1%) had received thoracic radiotherapy (including lung/mediastinum in 80%), most of them with radical/curative intention (median dose of 60 Gy). Only 54 patients received concomitant chemotherapy (55% platinum-based chemotherapy).
Focusing on the CE, 63 patients (16.7%) presented a CE during ICI treatment in our study (with some patients presenting more than one CE). The median time to CE onset from the initiation of ICI therapy was 4.3 months (p25: 1.5–p75: 11.1). Table 3 summarizes the incidence of each CE. Considering non-cardiac death as a competing event, the cumulative incidence rates for a CE were 10.2% at 6 months, 13.8% at 12 months, 16% at 18 months, 17.7% at 24 months, 18.8% at 6 months, and 19.8% at 48 months (Figure 1). The most prevalent event was an electrocardiographic alteration (69.8% of all CE), being atrial fibrillation the most frequently reported. Among the 44 patients who developed some type of arrhythmia during immunotherapy, 42 were newly onset and only 4 had history of atrial fibrillation. Congestive HF accounted for 19.0% of all CE; of important note, we found that all of these patients had previous CVRF, which could have predisposed to the subsequent HF event during ICIs. However, none of these patients had a history of HF or echocardiographic abnormalities prior to ICI therapy. Pulmonary embolism represented 10.8% of all CE, having all of them predisposing factors such as recent surgery, immobilization, or disease progression. None required fibrinolysis or ICU admission, and 3 patients (4.6% of all CE) developed an ACS, of whom, two had a previous history of coronary heart disease and were under cardiologic follow-up.
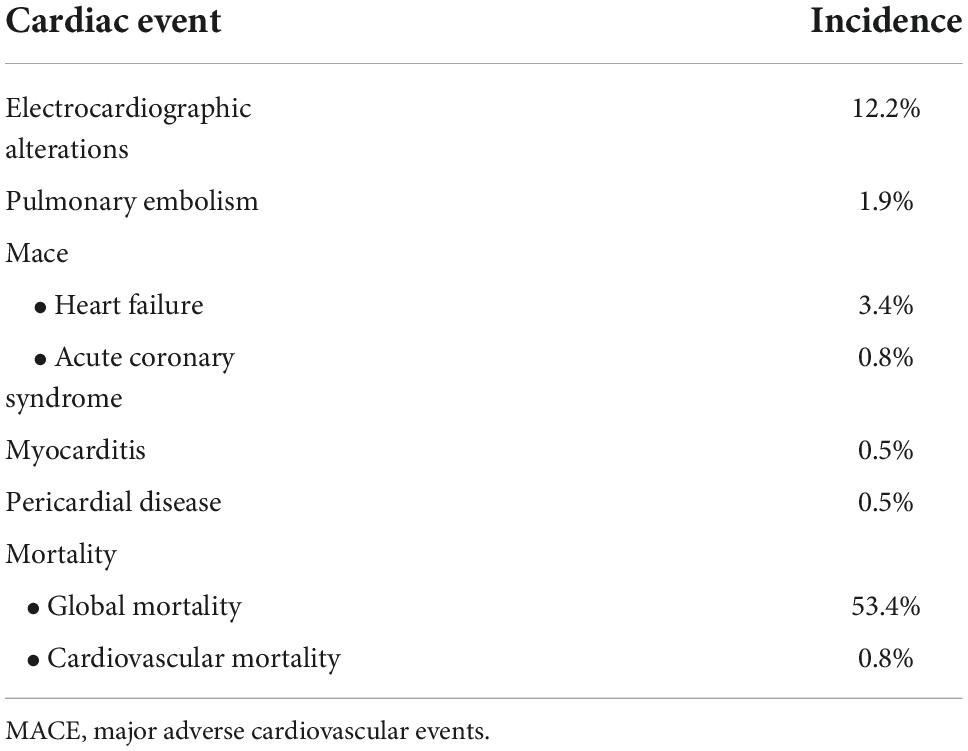
Table 3. Global incidence of cardiovascular events during ICI treatment.
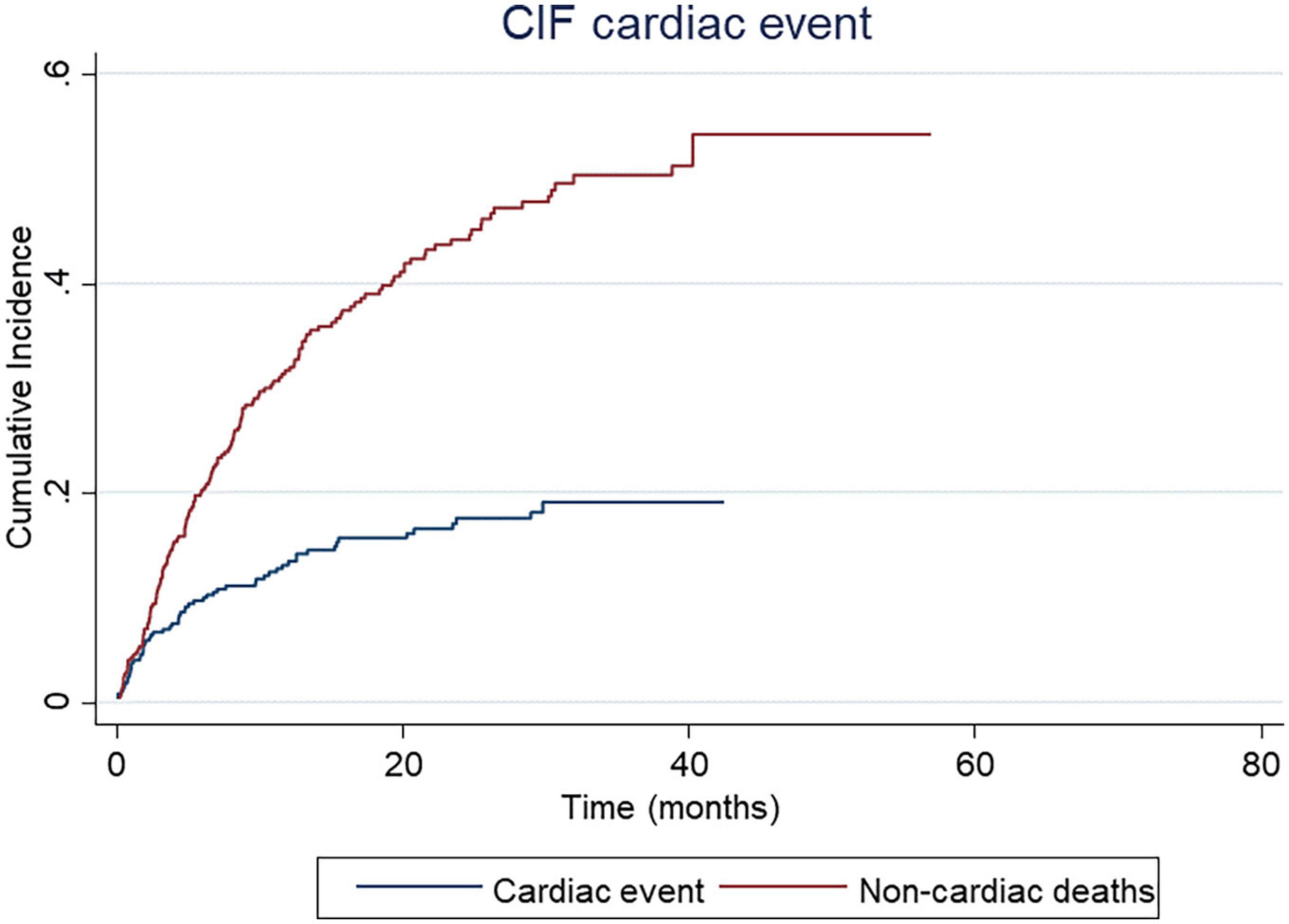
Figure 1. Cumulative Incidence Function (CIF) of cardiac events.
Regarding the “inflammatory” cardiotoxicity, two patients were diagnosed with pericarditis and two with myocarditis. These patients required hospital admission and close cardiologic monitoring, as well as high-dose corticosteroids, and, in the case of myocarditis, immunosuppressive treatment. Three of these four patients diagnosed with peri- or myocarditis presented other concomitant irAE, such as myasthenia gravis, polyarthritis, or Guillain–Barre syndrome. As previously stated, 37 patients (9.8%) had to interrupt treatment because of an irAE, but only 2 patients (0.5%) due to specific cardiac toxicity. During a median follow-up of 50.5 months (95% CI 45.5–57.7), 202 patients (53.4%) died, of whom 3 (0.8%) the cause of death was due to a CE: 2 fatal events associated to myocarditis and 1 to congestive HF.
The cumulative incidence function (CIF) represents the incidence rates of cardiac events in our cohort of patients, considering non-cardiac deaths as a competing event. Probably, the incidence of CE might be underestimated due to the high mortality rates observed in cancer patients.
Univariable and multivariable Cox regression analyses are presented in Table 4. Older patients and those with history of heart valve disease, ischemic heart disease, or arrhythmia were prone to develop a CE in the univariable analysis. However, only age (OR 1.03; 95% CI 0.99–1.06; p = 0.05), a history of ischemic heart disease (OR 3.25; 95% CI 1.16–9.14; p = 0.025), or arrhythmia (OR 4.11; 95% CI 1.66–10.22; p = 0.002), remained significantly associated with CE in the multivariable analysis. Likewise, those patients who had developed another irAE (31.7%) were also at increased risk (OR 2.08; 95% CI 1.11–3.94; p = 0.023). By contrast, other known CVRF such as hypertension, diabetes, dyslipidemia, chronic kidney failure, or smoking habit, did not increase the risk for cardiac toxicity in our study, nor did the type of tumor, stage, or response to treatment. Regarding ICI therapy, there were no differences between combination regimens (with other ICI, antiangiogenic therapy, or chemotherapy) and monotherapy (p = 0.87). Similarly, patients who had received other cardiotoxic therapies (anthracyclines, cisplatin, antimicrotubule agents, antiangiogenic therapy, anti-HER2 therapy, or thoracic radiotherapy), were not at increased risk for cardiac toxicity.
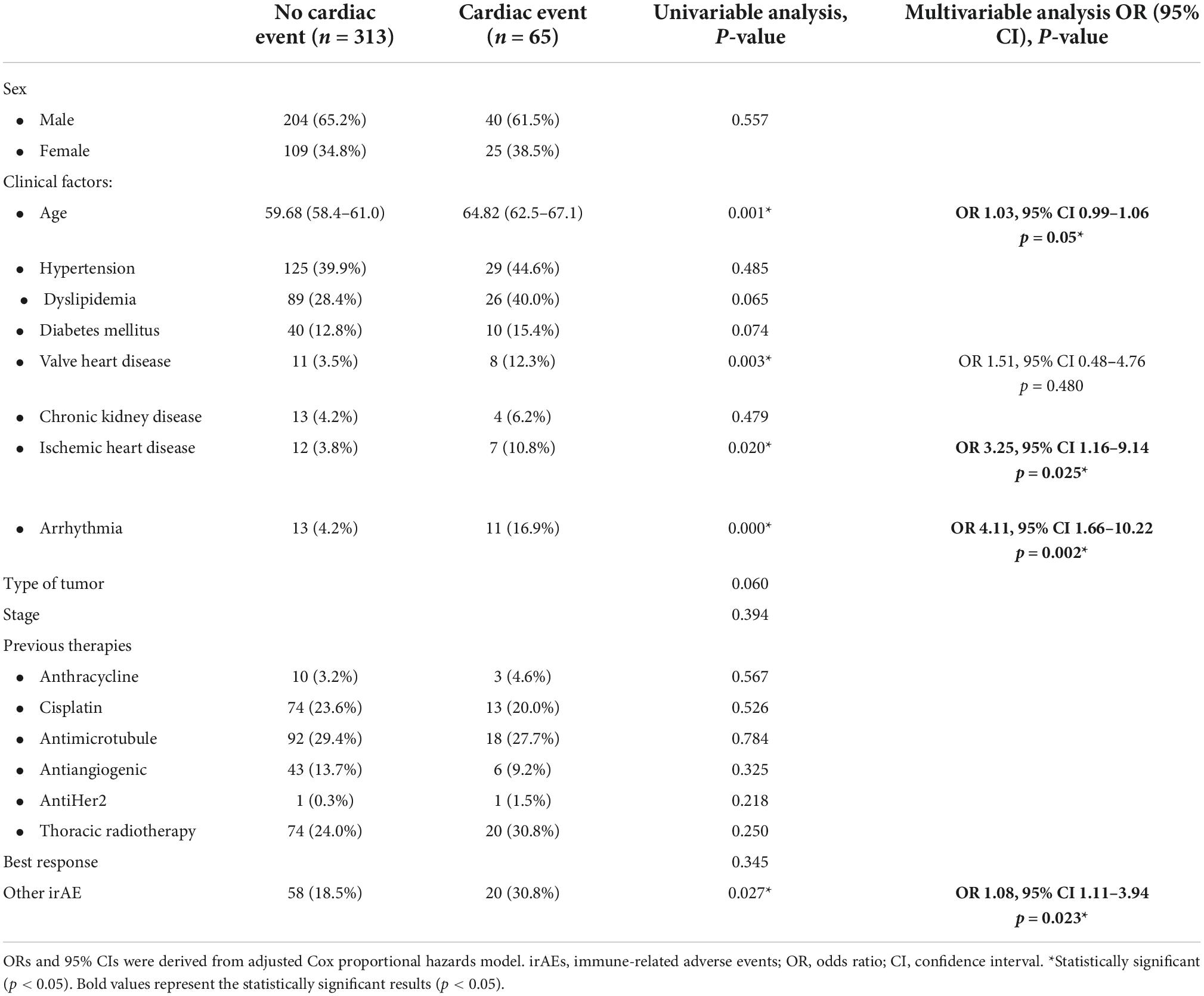
Table 4. Univariable and multivariable Cox regression analysis.
This study provides real-world observational data on the risk of CE associated with ICI treatment, which can extend beyond myocarditis. Their detection is currently challenging due to the lack of consistency of its clinical manifestation, and, consequently, their incidence is probably underestimated in clinical trials. Thus, prospective or retrospective studies with larger cohorts are essential for capturing the true incidence of CE in daily practice. A pharmacovigilance study using VigiBase, the WHO’s global database of individual case safety reports, reported significantly higher, but still very low incidences of myocarditis and pericarditis, with an incidence of 0.39 and 0.30%, respectively (23). A Danish nationwide study evaluated the risk of CE in ICI-treated patients, reporting an absolute risk at 1 year of 9.7% in 743 patients with lung cancer and 6.6% in 145 patients with melanoma. They concluded that the hazard rates of CE were higher in patients with vs. without ICI treatment (24).
The most prevalent CE reported in our study were arrhythmias, of which, atrial fibrillation was the most prevalent one. ICI-mediated arrhythmias and conduction diseases, in the absence of generalized myocarditis, are emerging as a more frequent and potentially serious cause of ICI-mediated sudden death (21). The mechanisms underlying the arrhythmias are unknown, but might include inflammation of the His–Purkinje conduction system, increased systemic inflammatory state, myocarditis with inflammation and fibrosis, and other causes of arrhythmias in cancer patients (QT-interval prolonging drugs, electrolyte imbalances, myocardial metastases) (20). Other relevant CE reported in our study were HF and ACS, which can be considered MACE. Although other well-known CVRF, such as hypertension, diabetes, or dyslipidemia, are major risk factors for developing a MACE, and immunotherapy seems to play an important role in the pathogenesis of these events. Preclinical models have shown that cardiomyocyte PD-L1 expression is upregulated in cardiac stress, including ischemia reperfusion and left ventricular hypertrophy, and might have cardioprotective actions by suppressing excessive myocardial inflammation (25). Likewise, it is known that atherosclerosis is characterized by low-grade chronic inflammation, and that acute or chronic inflammatory conditions can accelerate plaque rupture (26). Thus, ICIs could induce acceleration or decompensation of pre-existing HF and ACS in susceptible individuals. In line with this, in a matched cohort study of 5,684 patients, a threefold higher risk of atherosclerotic CE (myocardial infarction, coronary revascularization, and ischemic stroke) was observed after starting ICI therapy (27). Additionally, HF is not a marginal issue in this study and requires a better understanding of the systemic perturbation induced by immune checkpoints and its impact on cardiac function. Patients with dilated cardiomyopathy can have heterogeneous etiology such as genetic, viral, immunological, and environmental factors. Despite several animal studies that indicate that PD-1 may be an important factor contributing to the prevention of autoimmune diseases (28, 29), the involvement of an immune mechanism in patients with dilated cardiomyopathy is still controversial.
Regarding pulmonary embolisms, the evidence is scarce. Some reports suggest that these events may be associated with ICI therapy (30); however, this should be viewed as speculative and requires further investigation. In our cohort, the incidence of myocarditis and pericardial diseases was 0.5. Our rate is similar to that previously reported in other studies, although there has been a substantial increase in reporting incidence over time (31), probably due to an increased use of ICIs, along with heightened recognition of this new clinical entity. With a fatality rate of 27–46%, ICI- related myocarditis is the most lethal form of irAE (32), requiring high-dose corticosteroids and, in most cases, immunosuppressive treatment. The pathophysiology of ICI-induced myocarditis is incompletely understood. Post-mortem evaluations have observed inflammatory T-cell (CD4+ and CD8+) and macrophage infiltrate, as well as loss of cardiomyocytes, which, as mentioned before, might also employ the PD-1/PD-L1 pathway to prevent T-cell hyperactivation in the heart in physiological conditions (17). These findings are consistent with the mechanism of ICI action and can be considered an on-target toxicity.
The presence of pre-existent CVRF was common in our study population (46.6%), similar to that reported in the literature (33). Little is known about predisposing risk factors for ICI-related cardiotoxicity. Mahmood et al. reported that diabetes mellitus may predispose to immune-related myocarditis, but no such association has yet been found for other CVRF (18). In a recent retrospective match-cohort study of 672 patients treated with ICIs, only age, history of HF, and heart valve disease were independently associated with MACE (34). In our study, the multivariable analysis showed that older patients, those with history of ischemic heart disease or arrhythmias, and those who developed an irAE are at increased risk of developing a CE during ICI treatment. Other non-cardiac irAEs are frequent, occurring in approximately half of the patients with ICI-mediated myocarditis (18). Myositis is one of the most prevalent (23–25%) (21, 31), and this association might reflect a shared antigen profile and immune phenotype between cardiac and skeletal muscle.
A combination of ICI therapy seems to be a clear risk factor for developing a CE according to the literature. Johnson et al. reported a higher incidence (0.27 vs. 0.06%) and severity (60 vs. 10%) of myocarditis in patients receiving a combination of nivolumab and ipilimumab compared to nivolumab alone (17). Similarly, combined immunotherapy and other cardiotoxic cancer therapy (such as anti-VEGF-tyrosine kinase inhibitors, platinum-based chemotherapy, or radiotherapy) seem to increase the vulnerability for developing a CE (35). However, our study was unable to demonstrate those associations; possibly, a larger study sample might have exposed a statistical difference. On the other hand, many patients with metastatic disease have received multiple treatments before initiating ICIs treatment, some of which might have been cardiotoxic. By inducing myocardium damage, these treatments can lead to the exposure of cardiac antigens developing immune responses that can be amplified upon the initiation of ICIs (36). In our cohort, previous treatment with cardiotoxic therapy was common (58.9%), but no association was observed with the development of CE in the multivariable analysis.
Our real-world data support a baseline and protocoled cardio-oncology follow-up of high-risk patients, such as elderly patients and those with pre-existing cardiovascular comorbidities, especially history of ischemic heart disease and arrhythmias. In addition, patients who develop another irAE should be included in this high-risk group. Based on these results, we have designed a predictive risk-score, which could potentially assess the probability of developing a CE based on the presence or absence of these specific risk factors (Figure 2). This predictive risk score is based on four different variables associated with the development of a CE in our study. Depending on the presence or absence of each variable, the patient gets a score which might predict the probability of developing a cardiac event.
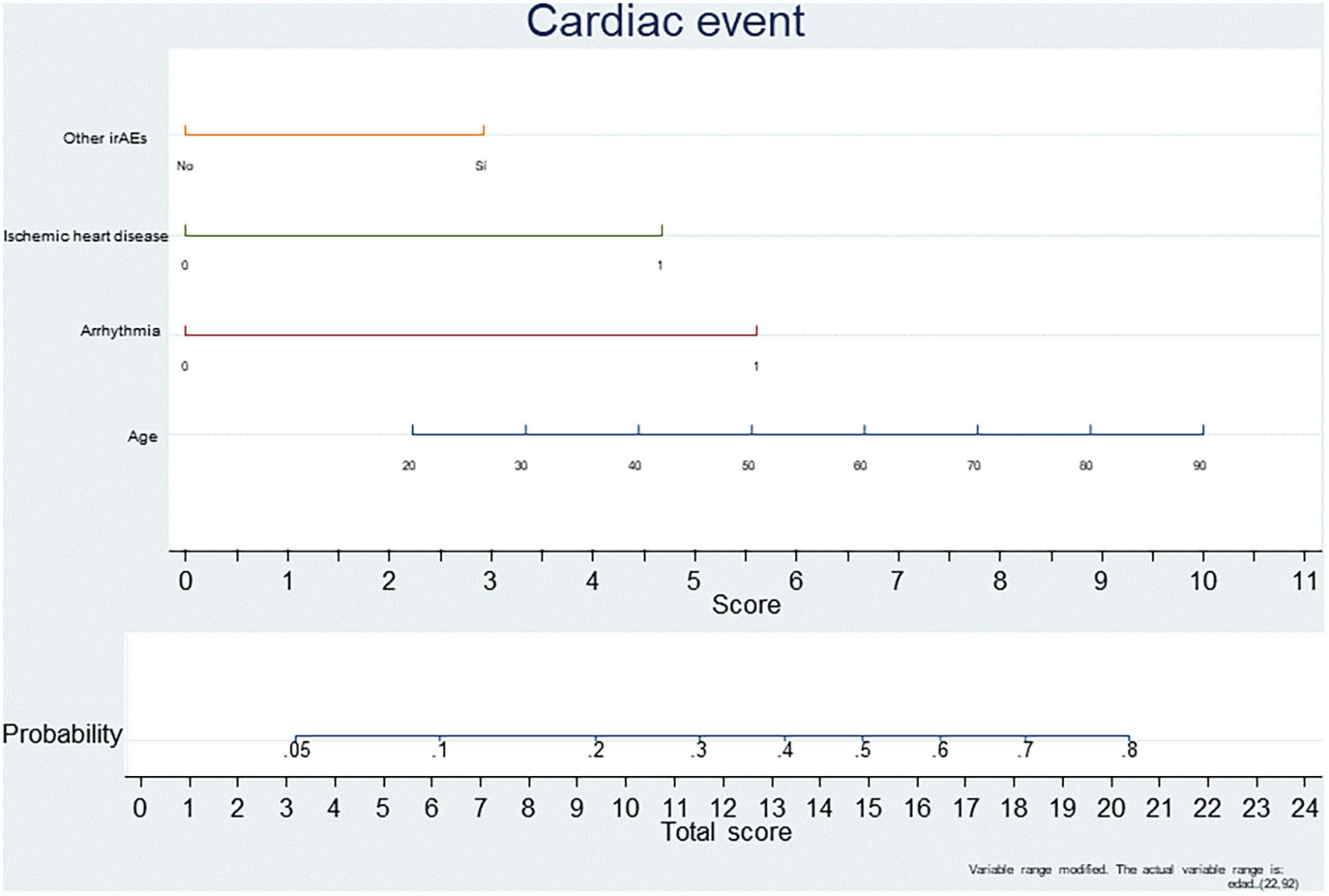
Figure 2. Predictive risk score for developing a cardiac event during ICI treatment.
No evidence-based algorithm yet exists for the management of these patients, mainly due to the absence of prospective trials. Two risk scores in the setting of breast cancer, specifically in early-stage HER2-positive breast cancer patients treated with trastuzumab have been reported. In 2012, Romond et al. used 7-year follow-up data from the National Surgical Adjuvant Breast and Bowel Project B-31 adjuvant trastuzumab study to derive a prediction tool for cardiotoxicity (37). A second prediction tool was derived by Ezaz et al., who used data from the U.S. Surveillance, Epidemiology, and End Results database in 1,664 women with previous exposure to trastuzumab (38). Moreover, the CHEMO−RADIAT study validated a predictive model for risk of major cardiovascular events after the diagnosis of breast cancer based on both conventional cardiovascular risk factors and breast cancer treatment−related cardiovascular risk factors, showing a good performance but only valid for breast cancer and again, based only on CVRF. The main limitation of these cardiotoxicity scores is that they focus on CVRF but do not incorporate damage cardiac biomarkers such as BNP or troponins, nor novel echocardiography parameters such as global longitudinal strain (GLS), used in clinical practice for early detection of changes in myocardial contractile function (39, 40).
In this sense, our score has two advantages: one, it is valid for any type of cancer, and two, that it includes cardiac biomarkers determination and echocardiography exams. Nevertheless, it needs to be validated in the different pathologies in a larger sample. Thus, a thorough cardiovascular evaluation is essential before starting ICI treatment, necessary for the multidisciplinary assessment of a cardio-oncology team.
The American Society of Clinical Oncology (ASCO) recommends a baseline cardiac workup before initiating potential cardiotoxic therapy, and, in case of symptoms, an extended cardiology workup including echocardiography, chest x-ray, and cardiac biomarkers, such as cardiac troponin and brain natriuretic peptide (BNP) (41). On the other hand, other studies have also suggested a surveillance strategy for high-risk patients who are receiving ICI treatment (20). The baseline cardiac assessment pre-ICI should include a complete clinical history and risk factor assessment, electrocardiogram (ECG), cardiac troponin, BNP, and echocardiogram. In high-risk patients, a closer monitoring is recommended, with ECG and cardiac biomarkers determination before ICI initiation and dose-adjustment. These specific tests are proposed because ICI-related CE has been characterized consistently by BNP elevation or conduction disease. Measurement of cardiac troponin should also be considered because it is more specific for myocarditis, the most important ICI-triggered cardiotoxic effect. Given the heterogeneity in the risk of cardiotoxic effects, a personalized strategy based on the patient´s baseline risk assessment may be relevant. Upon cardiotoxicity suspicion, it is recommended to immediately interrupt ICI therapy, repeat all cardiovascular exams, and refer the patient to a cardio-oncology specialist (20). In case of major cardiovascular complications, management should be in accordance with the current European Society of Cardiology (ESC) and American Heart Association (AHA) guidelines.
The main limitation of this study is its retrospective, descriptive nature, based on the activity conducted in a single center, Puerta de Hierro-Majadahonda University Hospital. Consequently, the incidence of CE might have been underestimated due to the lack of information in the medical records.
The real incidence of immune-related cardiotoxicity in real-world practice is higher than that reported in clinical trials. Cardiovascular history, older age, and prior irAEs are potential risk-factors, making patients more susceptible to these events. A thorough cardiovascular evaluation is strongly recommended before ICI treatment and, in high-risk patients, a closer follow-up and prompt referral to a cardio-oncology specialist as soon as cardiotoxicity is suspected. Risk stratification using a risk scoring system may improve the cardiovascular outcomes of patients treated with ICIs by identifying the patients at risk for cardiovascular events. Incorporation of clinical biomarkers and imaging parameters should be incorporated into these scores in order to improve the accuracy of prediction. Future studies with larger samples are needed in order to validate risk scores and develop standardized follow-up strategies for these patients.
The raw data supporting the conclusions of this article will be made available by the authors upon reasonable request.
The studies involving human participants were reviewed and approved by the Comité de Ética de Investigación con Medicamentos del Hospital Universitario Puerta de Hierro Majadahonda. The patients/participants provided their written informed consent to participate in this study.
MT, MB, FF, and MP drafted and designed the study. MM, BC, LG, MB, RH, AC-L, VC, JS, AG-d-A, and BN performed patients’ inclusion. MT, MB, PS, and MP drafted the manuscript. All authors reviewed and approved the manuscript and read and agreed to the published version of the manuscript.
This article is part of the CLARIFY project, supported by the European Union Horizon 2020 Research and Innovation Program under grant agreement number 875160.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Zhou YW, Zhu YJ, Wang MN, Xie Y, Chen CY, Zhang T, et al. Immune checkpoint inhibitor-associated cardiotoxicity: current understanding on its mechanism, diagnosis and management. Front Pharmacol. (2019) 10:1350. doi: 10.3389/fphar.2019.01350
2. Swaika A, Hammond WA, Joseph RW. Current state of anti-PD-L1 and anti-PD-1 agents in cancer therapy. Mol Immunol. (2015) 67(2 Pt A):4–17.
3. Walker LS, Sansom DM. The emerging role of CTLA4 as a cell-extrinsic regulator of T cell responses. Nat Rev Immunol. (2011) 11:852–63. doi: 10.1038/nri3108
4. Boussiotis VA. Molecular and biochemical aspects of the PD-1 checkpoint pathway. N Engl J Med. (2016) 375:1767–78. doi: 10.1056/NEJMra1514296
5. Hino R, Kabashima K, Kato Y, Yagi H, Nakamura M, Honjo T, et al. Tumor cell expression of programmed cell death-1 ligand 1 is a prognostic factor for malignant melanoma. Cancer. (2010) 116:1757–66.
6. Vaddepally RK, Kharel P, Pandey R, Garje R, Chandra AB. Review of indications of FDA-approved immune checkpoint inhibitors per NCCN guidelines with the level of evidence. Cancers. (2020) 12:738. doi: 10.3390/cancers12030738
7. Reck M, Rodríguez-Abreu D, Robinson AG, Hui R, Csõszi T, Fülöp A, et al. Pembrolizumab versus chemotherapy for PD-L1-positive non-small-cell lung cancer. N Engl J Med. (2016) 375:1823–33.
8. Hodi FS, O’Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. (2010) 363:711–23.
9. Postow MA, Sidlow R, Hellmann MD. Immune-related adverse events associated with immune checkpoint blockade. N Engl J Med. (2018) 378:158–68.
10. Michot JM, Bigenwald C, Champiat S, Collins M, Carbonnel F, Postel-Vinay S, et al. Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur J Cancer. (2016) 54:139–48.
11. Wolchok JD, Chiarion-Sileni V, Gonzalez R, Rutkowski P, Grob JJ, Cowey CL, et al. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. (2017) 377:1345–56.
12. Heery CR, O’Sullivan Coyne GH, Madan RA, Schlom J, von Heydebreck A, Cuillerot JM, et al. Phase I, open-label, multi-ascending dose trial of avelumab (MSB0010718C), an anti-PD-L1 monoclonal antibody, in Japanese patients with advanced solid tumors. J Clin Oncol. (2015) 33(15_suppl.):3023–3023.
13. Geisler BP, Raad RA, Esaian D, Sharon E, Schwartz DR. Apical ballooning and cardiomyopathy in a melanoma patient treated with ipilimumab: a case of takotsubo-like syndrome. J Immunother Cancer. (2015) 3:4. doi: 10.1186/s40425-015-0048-2
14. Läubli H, Balmelli C, Bossard M, Pfister O, Glatz K, Zippelius A. Acute heart failure due to autoimmune myocarditis under pembrolizumab treatment for metastatic melanoma. J Immunother Cancer. (2015) 3:11. doi: 10.1186/s40425-015-0057-1
15. Norwood TG, Westbrook BC, Johnson DB, Litovsky SH, Terry NL, McKee SB, et al. Smoldering myocarditis following immune checkpoint blockade. J Immunother Cancer. (2017) 5:91.
16. Choueiri TK, Larkin J, Oya M, Thistlethwaite F, Martignoni M, Nathan P, et al. Preliminary results for avelumab plus axitinib as first-line therapy in patients with advanced clear-cell renal-cell carcinoma (JAVELIN Renal 100): an open-label, dose-finding and dose-expansion, phase 1b trial. Lancet Oncol. (2018) 19:451–60.
17. Johnson DB, Balko JM, Compton ML, Chalkias S, Gorham J, Xu Y, et al. Fulminant myocarditis with combination immune checkpoint blockade. N Engl J Med. (2016) 375:1749–55.
18. Mahmood SS, Fradley MG, Cohen JV, Nohria A, Reynolds KL, Heinzerling LM, et al. Myocarditis in patients treated with immune checkpoint inhibitors. J Am Coll Cardiol. (2018) 71:1755–64.
19. Ji C, Roy MD, Golas J, Vitsky A, Ram S, Kumpf SW, et al. Myocarditis in cynomolgus monkeys following treatment with immune checkpoint inhibitors. Clin Cancer Res. (2019) 25:4735–48. doi: 10.1158/1078-0432.CCR-18-4083
20. Lyon AR, Yousaf N, Battisti NML, Moslehi J, Larkin J. Immune checkpoint inhibitors and cardiovascular toxicity. Lancet Oncol. (2018) 19:e447–58.
21. Escudier M, Cautela J, Malissen N, Ancedy Y, Orabona M, Pinto J, et al. Clinical features, management, and outcomes of immune checkpoint inhibitor-related cardiotoxicity. Circulation. (2017) 136:2085–7.
22. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, Lao CD, et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. (2015) 373:23–34.
23. Salem JE, Manouchehri A, Moey M, Lebrun-Vignes B, Bastarache L, Pariente A, et al. Cardiovascular toxicities associated with immune checkpoint inhibitors: an observational, retrospective, pharmacovigilance study. Lancet Oncol. (2018) 19:1579–89. doi: 10.1016/S1470-2045(18)30608-9
24. D’Souza M, Nielsen D, Svane IM, Iversen K, Rasmussen PV, Madelaire C, et al. The risk of cardiac events in patients receiving immune checkpoint inhibitors: a nationwide Danish study. Eur Heart J. (2021) 42:1621–31. doi: 10.1093/eurheartj/ehaa884
25. Baban B, Liu JY, Qin X, Weintraub NL, Mozaffari MS. Upregulation of programmed death-1 and its ligand in cardiac injury models: interaction with GADD153. PLoS One. (2015) 10:e0124059. doi: 10.1371/journal.pone.0124059
26. JBS3 Board. Joint British Societies’ consensus recommendations for the prevention of cardiovascular disease (JBS3). Heart. (2014) 100(Suppl 2.):ii1–67.
27. Drobni ZD, Alvi RM, Taron J, Zafar A, Murphy SP, Rambarat PK, et al. Association between immune checkpoint inhibitors with cardiovascular events and atherosclerotic plaque. Circulation. (2020) 142:2299–311.
28. Nishimura H, Okazaki T, Tanaka Y, Nakatani K, Hara M, Matsumori A, et al. Autoimmune dilated cardiomyopathy in PD-1 receptor-deficient mice. Science. (2001) 291:319–22. doi: 10.1126/science.291.5502.319
29. Okazaki T, Tanaka Y, Nishio R, Mitsuiye T, Mizoguchi A, Wang J, et al. Autoantibodies against cardiac troponin I are responsible for dilated cardiomyopathy in PD-1-deficient mice. Nat Med. (2003) 9:1477–83. doi: 10.1038/nm955
30. Bazaz R, Marriott HM, Francis SE, Dockrell DH. Mechanistic links between acute respiratory tract infections and acute coronary syndromes. J Infect. (2013) 66:1–17. doi: 10.1016/j.jinf.2012.09.009
31. Moslehi JJ, Salem JE, Sosman JA, Lebrun-Vignes B, Johnson DB. Increased reporting of fatal immune checkpoint inhibitor-associated myocarditis. Lancet. (2018) 391:933.
32. Wang DY, Salem JE, Cohen JV, Chandra S, Menzer C, Ye F, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol. (2018) 4:1721–8.
33. Rubio-Infante N, Ramírez-Flores YA, Castillo EC, Lozano O, García-Rivas G, Torre-Amione G. Cardiotoxicity associated with immune checkpoint inhibitor therapy: a meta-analysis. Eur J Heart Fail. (2021) 23:1739–47.
34. Laenens D, Yu Y, Santens B, Jacobs J, Beuselinck B, Bechter O, et al. Incidence of cardiovascular events in patients treated with immune checkpoint inhibitors. J Clin Oncol. (2022) 40:3430–8.
35. Du S, Zhou L, Alexander GS, Park K, Yang L, Wang N, et al. PD-1 modulates radiation-induced cardiac toxicity through cytotoxic T lymphocytes. J Thorac Oncol. (2018) 13:510–20. doi: 10.1016/j.jtho.2017.12.002
36. Cihakova D, Rose NR. Pathogenesis of myocarditis and dilated cardiomyopathy. Adv Immunol. (2008) 99:95–114.
37. Romond EH, Jeong JH, Rastogi P, Swain SM, Geyer CE Jr, Ewer MS, et al. Seven-year follow-up assessment of cardiac function in NSABP B-31, a randomized trial comparing doxorubicin and cyclophosphamide followed by paclitaxel (ACP) with ACP plus trastuzumab as adjuvant therapy for patients with node-positive, human epidermal growth factor receptor 2-positive breast cancer. J Clin Oncol. (2012) 30:3792–9. doi: 10.1200/JCO.2011.40.0010
38. Ezaz G, Long JB, Gross CP, Chen J. Risk prediction model for heart failure and cardiomyopathy after adjuvant trastuzumab therapy for breast cancer. J Am Heart Assoc. (2014) 3:e000472. doi: 10.1161/JAHA.113.000472
39. Kim DY, Park MS, Youn JC, Lee S, Choi JH, Jung MH, et al. Development and validation of a risk score model for predicting the cardiovascular outcomes after breast cancer therapy: the CHEMO-RADIAT score. J Am Heart Assoc. (2021) 10:e021931. doi: 10.1161/JAHA.121.021931
40. Oikonomou EK, Kokkinidis DG, Kampaktsis PN, Amir EA, Marwick TH, Gupta D, et al. Assessment of prognostic value of left ventricular global longitudinal strain for early prediction of chemotherapy-induced cardiotoxicity: a systematic review and meta-analysis. JAMA Cardiol. (2019) 4:1007–18. doi: 10.1001/jamacardio.2019.2952
Keywords: cardiovascular event, immune checkpoint inhibitors, myocarditis, cardiotoxicity, risk factors
Citation: Torrente M, Blanco M, Franco F, Garitaonaindia Y, Calvo V, Collazo-Lorduy A, Gutiérrez L, Sánchez JC, González-del-Alba A, Hernández R, Méndez M, Cantos B, Núñez B, Sousa PAC and Provencio M (2022) Assessing the risk of cardiovascular events in patients receiving immune checkpoint inhibitors. Front. Cardiovasc. Med. 9:1062858. doi: 10.3389/fcvm.2022.1062858
Received: 06 October 2022; Accepted: 08 November 2022;
Published: 01 December 2022.
Edited by:
Antonella Lombardo, Agostino Gemelli University Polyclinic (IRCCS), ItalyReviewed by:
Chiara Lestuzzi, Santa Maria degli Angeli Hospital, ItalyCopyright © 2022 Torrente, Blanco, Franco, Garitaonaindia, Calvo, Collazo-Lorduy, Gutiérrez, Sánchez, González-del-Alba, Hernández, Méndez, Cantos, Núñez, Sousa and Provencio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Torrente, bWFyaWEudG9ycmVudGVAc2FsdWQubWFkcmlkLm9yZw==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.