
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 04 January 2023
Sec. Cardiovascular Epidemiology and Prevention
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.1049036
This article is part of the Research Topic Prevention and Treatment of Cardiovascular Disease with Integrated Traditional Chinese and Western Medicine View all 21 articles
 Xiankun Chen1,2,3†
Xiankun Chen1,2,3† Wei Jiang1,4†
Wei Jiang1,4† Mariano Salazar5Huiying Zhu4
Mariano Salazar5Huiying Zhu4 Zehuai Wen1,2,6*Xixi Chen7*Cecilia Stålsby Lundborg3
Zehuai Wen1,2,6*Xixi Chen7*Cecilia Stålsby Lundborg3Objective: Baduanjin (eight silken movements) is a traditional Chinese exercise that can be used as cardiac rehabilitation therapy for patients with chronic heart failure (CHF) especially when other forms of rehabilitation are scarce or unaffordable. This study explores the experiences of Chinese patients with CHF who undertook Baduanjin exercise at home as part of a pilot trial in Guangzhou, China.
Methods: We conducted seven qualitative interviews with participants who had participated in the intervention arm of a pilot randomized controlled trial (RCT) (n = 8). For data collection, we used a semi-structured interview guide with both open-ended, and follow-up questions. We audio recorded the interviews, transcribed them verbatim, and then analyzed them with content analysis.
Results: Participants’ experiences of doing Baduanjin were classified into three categories: (1) improving practice (2) factors facilitating good exercise adherence, and (3) feeling good. Participants reported that the exercises were easy but that the correct Baduanjin execution and coordination between the mind, movements, and breathing were only achievable through practice. In addition, the training benefits which they perceived were the predominant motivation for patients to keep practicing. Finally, trust in Baduanjin, personal attitudes toward health, flexibility in practice times, as well as social support helped the participants to achieve good adherence to home-based training.
Conclusion: This study’s findings indicate that Baduanjin could be a cardiac rehabilitation exercise modality for patients with CHF in China, especially in a home-based setting.
Research findings have predicted that the prevalence of chronic heart failure (CHF) will continue to increase in the future on account of the aging population, risk factors’ increasing prevalence, and improvements in post-myocardial infarction survival. In China, heart failure mortality remains a significant public health concern, as the China Heart Failure Registry Study has reported an in-hospital mortality rate of 5.3% (1). CHF mortality rates are high, even for those patients who are compliant with the best available treatments (2). Studies have shown that exercise-based cardiac rehabilitation (EBCR) improves CHF patients’ exercise capacity and their quality of life (3, 4).
Despite its benefits, EBCR uptake remains sub-optimal around the world today (5). A key driver of this poor uptake is low availability due to insufficient resources such as rehabilitation facilities and trained professionals (6). A recent national survey in China has shown that only 24% of its tertiary hospitals have EBCR services (7). In addition, patient-related barriers have limited eligible patients’ participation in EBCR programs and/or regular exercise (8). The most common barrier is affordability (8), because EBCR services rely on out-of-pocket payment systems in China. There are other barriers to exercise as well, which are often related to practical issues such as timing, the convenience of travel to a rehabilitation center, or inclement weather (9).
A traditional form of exercise called Baduanjin can potentially contribute toward a solution to unmet demand for EBCR programs caused by their scarcity and unaffordability in China (7). Baduanjin, or “Eight Silken Movements” is a martial art that originated in ancient China, and has been practiced for over 1,000 years (10). It is characterized by interplay between flowing circular physical postures and movements, mindfulness, and breathing exercise which are conducted in synchronization (11). From a cultural perspective, it has been accepted as being beneficial to one’s health, and in modern times, it remains a popular exercise throughout Mainland China. Nowadays, with the proliferation of social media, Baduanjin exercise videos can easily be found online (12, 13).
The hallmark symptoms of CHF, such as fatigue and dyspnea, frequently cause decreases in physical activity, and erode the confidence necessary to initiate/maintain a regular exercise regimen (14). Baduanjin, however, has minimal physical or cognitive demands because it consists of only eight simple movements (10). Patients are also encouraged to do Baduanjin at home, reducing barriers such as weather, transportation, or cost (9). This equipment-free exercise might also be preferred by Chinese hospitals, especially those with limited resources in rural area (15).
Baduanjin has shown promise in cardiac rehabilitation in recent years (11, 16), especially among Chinese CHF patients (17–22). It has been shown to be a moderate-intensity aerobic exercise which is both an effective and a safe exercise modality for home-based cardiac rehabilitation for CHF patients (23). Results from a multi-center randomized controlled trial (RCT) have shown that 12 weeks of Baduanjin training can produce improvements in fatigue and quality of life (21). In addition, a growing body of evidence suggests that Baduanjin might be helpful to various CHF-related cardiac medical issues, including hyperlipidemia (24), fatigue (25, 26), hypertension (27), cardiorespiratory endurance (28), and that it also facilitates improvements in psychological health (29, 30).
Previous studies on Baduanjin efficacy have provided key quantitative data to assess its effectiveness (31); however, none of these studies have used qualitative methods to explore how patients experienced using Baduanjin in the context of cardiac rehabilitation and what are the factors facilitating or hindering its use. In addition, as a complex holistic “mind-body exercise” with influence from traditional Chinese medicine, Baduanjin may have additional health potential. Thus, information regarding the connection between Baduanjin and an individual’s subjective experiences may present new clinical outcomes.
With growing appreciation for patient-centered outcomes, it has been recognized that patient experience is equally as crucial as physiological tests and measurements for the successful implementation of intervention programs. Qualitative research, in which data is collected on participants’ personal experiences, is the ideal tool for exploring these complex experiences. This method may entail detailing experiences that are difficult to capture through quantitative research, and expanding our scientific understandings beyond what can be learned through quantitative analysis (32). Therefore, this study’s aim was to explore the experiences of Chinese CHF patients who use Baduanjin at home.
This study was conducted in Guangzhou, China. Guangzhou is the capital of Guangdong province in Southeast China, and China’s third largest city. It has a permanent population of 13.5 million, and over 7 million permanent residents in its urban districts (33). Cardiac rehabilitation remains insufficiently implemented in current clinical practice in Guangzhou’s urban districts. Firstly, there is a low availability of cardiac rehabilitation services, especially in the outpatient clinics (7). Secondly, the practice patterns of cardiac rehabilitation are still very simple and poorly standardized (7). In most cases, cardiac rehabilitation comes in the form of verbal information supplemented by leaflets and booklets which emphasize early mobilization and identifying and controlling risk factors (34).
In addition, most existing programs are coordinated by a nurse, but relatively few used other healthcare professionals such as exercise physiologists, dieticians or physical therapists which is recommended in current guideline (34). Thirdly, there is no cardiac rehabilitation referral system after hospital discharge. Hence, there remain few cardiologists who regularly add cardiac rehabilitation to their daily clinical practice for their patients (7). Low physician referral may be compounded by the lack of hospital staff with training in cardiac rehabilitation resulting in inadequate knowledge about its benefits and inadequate assessment of a patient’s (in)ability to participate (7).
The participants of this study were taken from outpatient clinics at Guangdong Provincial Hospital of Chinese Medicine (GPHCM). GPHCM is a tertiary care public hospital with four campuses in different urban districts of Guangzhou. At GPHCM, cardiac rehabilitation is administered one-on-one by the cardiac nurses and rehabilitation physicians to individuals in a hospital outpatient clinic setting. It also includes exercise training. The most common exercise is cycle ergometer. However, this service is dependent on out-of-pocket payment systems. This creates financial stress for most patients, and in turn, results in low participation rates for cardiac rehabilitation.
To provide a way for heart failure patients to engage in a home-based EBCR program which is also equipment-free, low-cost, and easily implemented, we have developed a novel and contextually adapted EBCR program (BESMILE-HF) at GPHCM (35). BESMILE-HF is an acronym which stands for the Baduanjin Eight-Silken-Movement wIth SeLf-Efficacy building for Heart Failure. In this program, Baduanjin is applied as the core constituent in a multi-component EBCR which includes evaluation, consultancy, and education, in addition to a series of strategies for building self-efficacy. Our research group has conducted the pilot RCT to assess the feasibility and preliminary effects of Baduanjin in CHF patients. Pilot data suggested that Baduanjin may have a positive effect on clinical outcomes and may lead to increased long-term adherence to exercise through improved self-efficacy (36). As part of that project, this qualitative study was conducted.
This qualitative study has been nested within a pilot RCT (36, 37). In the pilot RCT, participants were recruited from GPHCM. We assessed potential study participants for eligibility via (1) on-site patient screening during clinic visits; (2) regular screening of potential participants via the use of electronic medical records; and (3) physician referrals. To be included, patients had to have clinically stable CHF with a New York Heart Association functional (NYHA) classification of either II or III, and no restriction on the left ventricular ejection fraction class.
In the intervention group, the intervention was delivered by a cardiac rehabilitation team consisting of one cardiologist, a cardiology nurse, a professional coach, and research assistants. Before starting the 6-week home-exercise period, participants would attend an exercise course at the hospital to learn the eight postures, with a professional coach confirming their technique. This was followed by a 6-week phase consisting of home exercise with guidance and instruction from a Baduanjin exercise video, a picture-brochure, as well as weekly follow-up.
Generally, participants were required to do 30 min of Baduanjin per day, 5 days a week, for a total of 150 min each week. This was tailored to individuals based on their evaluation results. We asked the participants in the intervention group to record their exercise performance in exercise logs every day throughout the study period. The logs included duration in minutes and frequency. After 6 weeks, we contacted the participants and asked them to return to the hospital. Finally, there were 18 participants in the pilot RCT. After they signed informed consent, we randomized eight participants into an intervention group which received the 6-week BESMILE-HF program plus the usual medications, and 10 others into a control group which received only the usual medications.
Upon the conclusion of the pilot RCT, the eight participants from the intervention groups were invited to partake in semi-structured interviews. Seven participants agreed to be interviewed over 2 weeks. The ages of the seven interviewed participants spanned from 61 to 72 (mean = 67 years). All were male and married. Two participants had finished only primary school, one had finished secondary school, and four of the participants had college or university degrees. Participant characteristics are shown in Table 1. At the time of the interviews, the pilot RCTs’ outcome measure results were unknown.
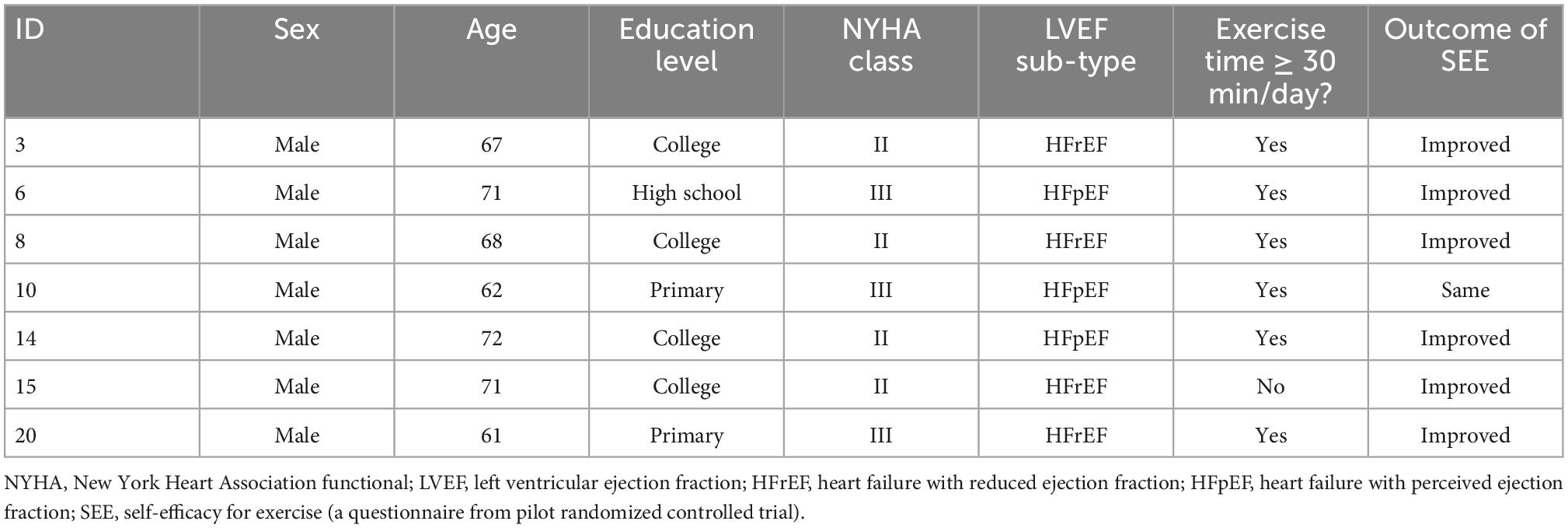
Table 1. Characteristics of the interviewed participants.
Each participant was interviewed once using a semi-structured interview guide. A female research assistant (HZ) who is an attending physician with a background in cardiology was trained to conduct the interviews. She was not a member of the BESMILE-HF research team. All interviews were conducted face-to-face using Mandarin or Cantonese in the cardiac rehabilitation room at the hospital. On average, the interviews lasted around 40 min. The interview guide is based on a review of relevant literature (9, 38). It contains open-ended questions designed to gain a deeper understanding of the Baduanjin experience. We pilot tested the guide for clarity, relevance, and pertinence to the study’s goals and then the research team finalized it. We began with an introduction question: “Tell me about your experiences practicing Baduanjin?” Subsequent questions covered various aspects of Baduanjin. In the follow-up questions, participants were asked to elaborate. For the complete interview guide, refer to Table 2. HZ conducted the interviews, recorded them, and transcribed them verbatim, The transcripts were checked by XC (first author) by comparing the recording and the transcribed texts line-by-line.
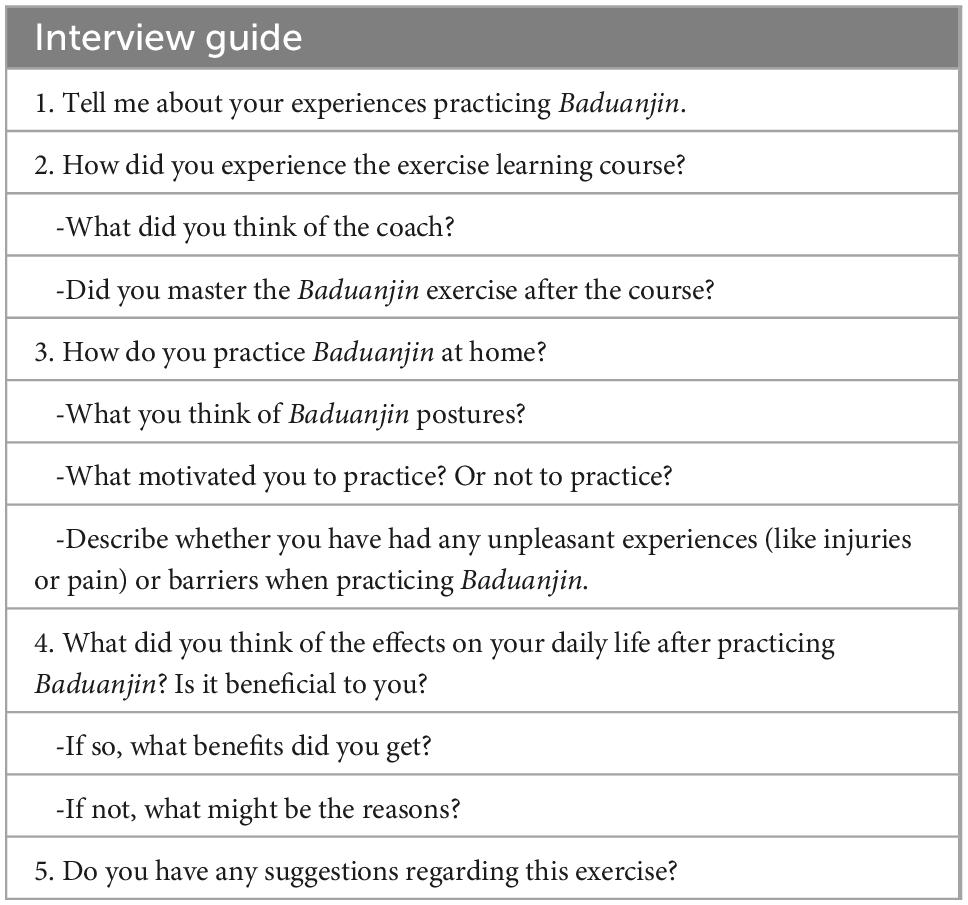
Table 2. Interview guide.
Two researchers (XC and HZ) performed qualitative content analysis based on an inductive approach utilizing the structure described by Elo and Kyngas (39) and assisted by NVivov11. Firstly, open coding was conducted. All transcribed texts were read several times with XC to make sense of the entire meaning, and then they were discussed for clarity with the interviewer (HZ). Then, the subjective experiences of donging Baduanjin were extracted. Next, we condensed the text into meaning units. Finally, the meaning units were coded. Examples of the resulting meaning units, condensed meaning units, and codes are shown in Table 3. Secondly, any codes with similar content were grouped into subcategories, and categories. Then, we sorted the subcategories and formulated them as categories. Co-author discussions were held throughout each step of the analysis until ultimately, there was consensus in terms of the structure of open coding and the structure of the sub-categories and categories. The analysis was initially conducted in Mandarin or Cantonese. Codes, sub-categories, and categories were then translated into English. The quotes presented are translated from Mandarin or Cantonese.
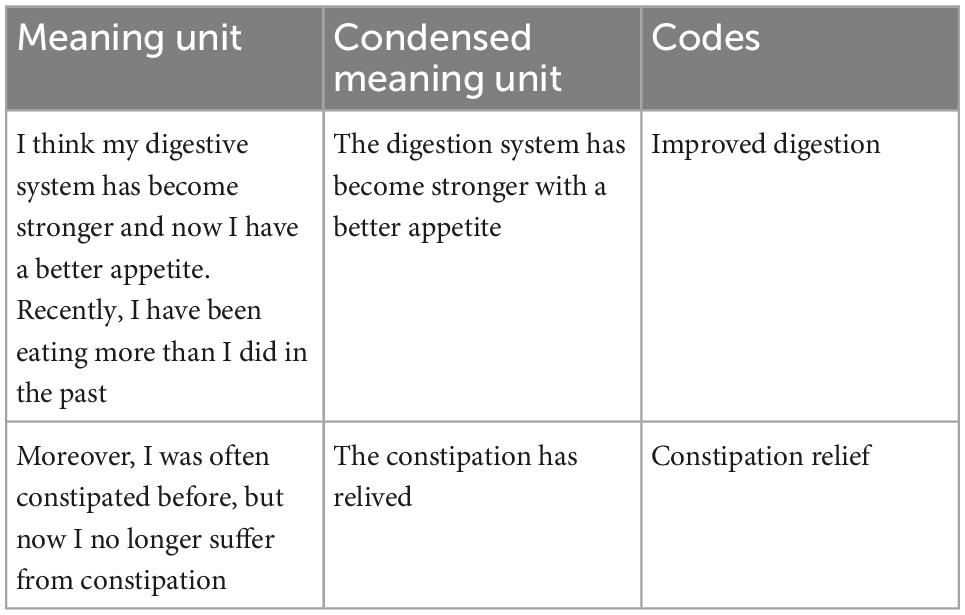
Table 3. An example of meaning units, condensed meaning units, and codes.
The BESMILE-HF trial has been approved by the Ethics Committee at the GPHCM (number: B2016-202-01) and also registered at ClinicalTrials.gov (NCT03180320). In addition, this qualitative study was also included in the trial protocol (35). Before each interview, we would ask the participant to read an information letter and provide both written and oral informed consent. We had an independent informed consent for the participants to take part in this qualitative study apart from the pilot study. Before giving consent, participants were allowed to ask questions and the personnel in the trial answered their questions carefully.
Participants’ experiences of doing Baduanjin were classified into three categories (1) improving practice; (2) factors facilitating good exercise adherence; and (3) feeling good. Details of the codes, subcategories and categories are listed in Table 4.
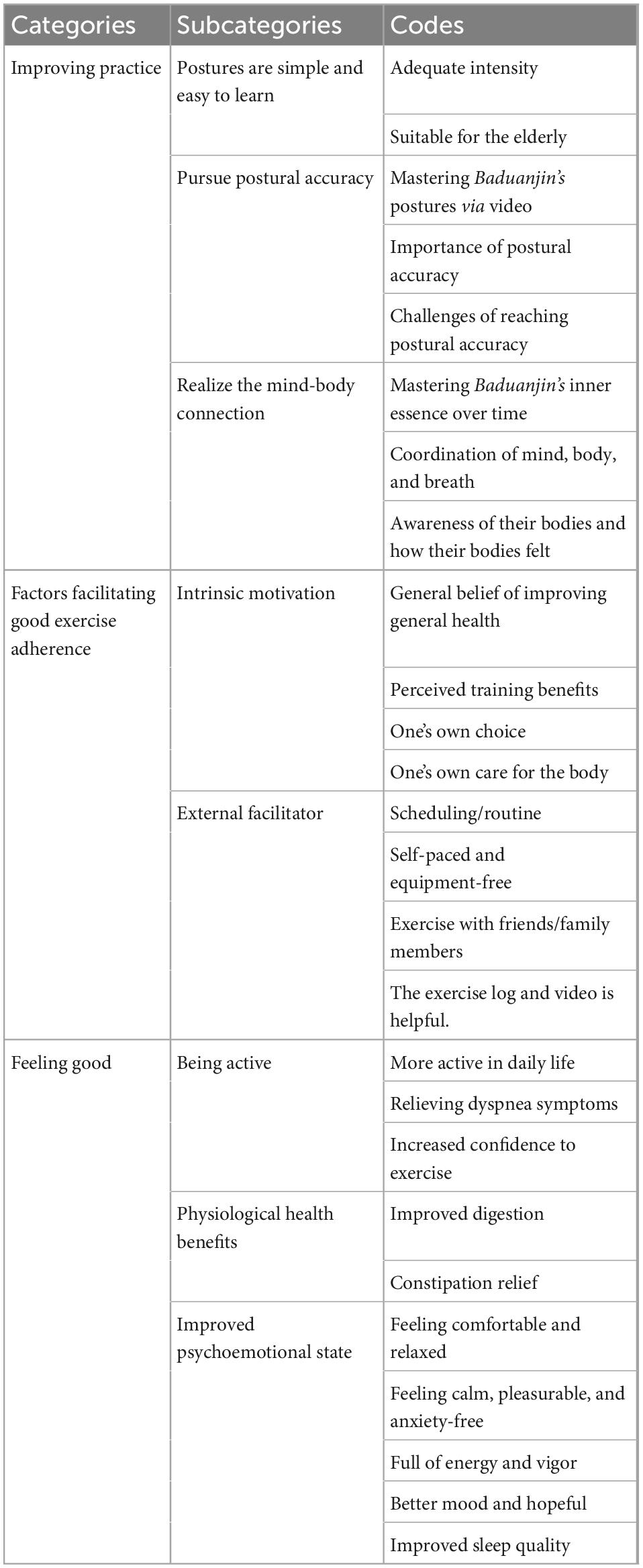
Table 4. Categories, subcategories, and codes describing experiences with Baduanjin among chronic heart failure patients.
The category “Improving practice” provided insight into participants learning process. At the beginning of learning, participants found that Baduanjin was easy to learn and required little skill. In addition, participants perceived that its gentle and slow movements provided a suitable intensity level for the elderly. However, challenges for postures requiring them to squat, bend their waist, or turn their head were also reported.
It only has eight movements! It is easy and I could master the postures after the course. You know, we have bad memories; it is hard for us to learn a new exercise. I think Baduanjin is simpler than other exercises. (ID: 6)
As participants familiarized with the postures, they experienced the importance of reaching postural accuracy. They described that the maximum training effects were difficult to achieve in cases where the exercises had been done incorrectly.
In the beginning, I had to follow the video to do the exercises. Slowly, I was able to remember it, but at the beginning, my movements were not very standard. Later, I found that I had to use force when doing the movements. This action has to be done in place, such as reaching the highest hand in the first posture and squatting in the fifth posture. Many people think that Baduanjin has no effect because they just do it casually without seriousness. Only when the movements are in place will they have an effect. (ID: 3)
With Baduanjin practice over time, participants said that they had gradually mastered its inner essence. They described that practicing requires coordination of the mind, the body, and their breath. Only by coordinating breathing, body, and mind through training to harmonize by practicing Baduanjin can a practitioner achieve its benefits. In addition, participants identified that it was essential to be aware of their bodies and how they felt during practice in order to achieve a good practice.
I have been doing it since 2004, and the effect of the previous years was not great, but the effect this time was much better. One reason was that I now coordinate my breathing. For example, in this movement, you must inhale when you stretch your arms backward, and exhale when you return them to the front, and breathe deeply. The other reason is the mind, that is to say, when you perform an action again, you have to know the purpose of the action. I used to just do exercises and not feel my body, so there was no effect. This time I learned that not only must I breathe well, but the idea of doing exercises is also very important. (ID: 3)
The category “Factors facilitating good exercise adherence” provide insight into the good adherence found in the pilot RCT. In the beginning, the reason they continued the exercises was the belief that Baduanjin can improve one’s general health. With the progression of Baduanjin training, participants emphasized that its perceived training benefits were the predominant motivation for them to adhere to it. Furthermore, participants reflected that “nobody can force me to exercise.” Whether or not to exercise was perceived as one’s own choice and this is determined primarily by the degree to which they cared for their own bodies.
I do benefit from Baduanjin, or else I would not have participated for so long. (ID: 8)
I stopped because I did not feel any improvement…(ID: 15, non-adhering participant)
In addition to those intrinsic motivations, several external facilitators were also reported to have supported participants’ sustained exercise. Participants told us that scheduling exercise or incorporating it into their routines promoted adherence. They also appreciated that the self-paced and equipment-free nature of the exercise allowed them to do it anytime and anywhere. They also reflected that they did not need a large training space or any other auxiliary apparatuses.
Practicing together with other friends or family members was found to facilitate practicing Baduanjin since it made it more enjoyable. Moreover, keeping exercise log was viewed as being helpful in keeping on track with their practice and reminding them to exercise daily. An exercise demonstration video was also a necessary tool to guide participants’ at-home exercise, especially at the outset when they were not so familiar with all eight postures.
It is convenient for me to practice Baduanjin. I even recommended it to my friends who also have heart disease. Sometimes I practice at the park with my friends and we all enjoy it. Since I retired, this has been a good opportunity to have something to do with them. This made me more willing to go and practice. (ID: 8)
The category “Feeling good” provided insight into participants’ perceived effects after practicing Baduanjin. Participants reported perceived improvements in their physical and mental health, and they become more active in their daily life.
In terms of physical health, after practicing Baduanjin for several weeks, participants described that they had become more active in their daily life as they experienced less shortness of breath. Participants also said that they gained confidence walking longer distances or at faster speeds, or even just had the confidence to get out of the house:
I used to keep a walking stick in my backpack, and I had to walk on the walking stick at all times. Now, I can walk without it. Sometimes I can walk more than 20,000 steps, and sometimes I will challenge myself to see how far I can go. (ID: 10)
In addition, participants experienced other improvements in their physiological health. Some participants mentioned gradual improvement in their digestion, and improved appetites following participation. Some participants had suffered intractable constipation for multiple years, but now reported regular bowel movements without constipation.
I think my digestive system has become stronger and now I have a better appetite. Recently, I have been eating more than I did in the past. Moreover, I was often constipated before, but now I no longer suffer from constipation. (ID: 3)
Moreover, participants also said that their mental wellbeing states had improved. Participants reported feeling comfortable every time they finished practicing Baduanjin. They also felt relaxed, as they said Baduanjin calmed them, gave them pleasure, and eased their anxiety. Participants also reported that they had obtained positive energy and vigor from Baduanjin. Other perceived benefits were an improvement on their moods (becoming more hopeful) and sleep patterns (bot in extended time and faster getting asleep).
Every time after I practice Baduanjin, I feel relaxed. I haven’t been so relaxed in a long time. To be honest, after getting this disease, I lost confidence in myself and there was no hope in life. But after a period of exercise, I felt that my mental state was much better and more energetic than before, and my thoughts were not so negative. (ID: 14)
I used to be afraid to sleep. Following several weeks of Baduanjin qigong training, I could get to sleep as soon as I lay down. (ID: 3)
This is the first study to explore CHF patients’ experiences’ using Baduanjin as a cardiac rehabilitation regimen. The results provide insight into participants’ learning and practice process, adherence, and perceived effects. While Baduanjin postures have a quick learning curve, their proper execution requires time and consistent practice. Coordinating the mind, the movements, and breathing in Baduanjin exercise is only possible progressively, through repeated practice. Participants experienced many benefits, for both mental and physical health, with regular high-quality Baduanjin practice. Moreover, the study showed that Baduanjin’s perceived training benefits were crucial to adherence to home-based training. In addition, internal facilitators such as trust in Baduanjin and attitudes toward health, as well as flexibility and external support, are also important for patients to keep practicing.
Baduanjin is an aerobic exercise in which the movements are simple, slow and relaxing. With varying skill levels, people may perform one style of Baduanjin in different ways. This may lead to variation in physiological responses. A previous study has shown that skill level may exert a sizable effect on metabolic and cardiorespiratory responses to Tai Chi practice (a traditional exercise similar to Baduanjin) (40). The authors found a higher mean heart rate and deeper breathing among the high-level practitioners. In our study, many participants experienced difficulty achieving maximum training effects if Baduanjin was practiced incorrectly. A high-level practitioner can perform Baduanjin with high quality, especially for the handful of movements which are particularly difficult. For example, high-level Baduanjin practitioners tend to perform those movements requiring participants to squat with lower positioned technique than the low-level practitioners, thus requiring increased muscle contraction from the lower extremities. Therefore, the improvements in their exercise capacity are expected to be more apparent. As most of the participants in this study were new to Baduanjin, several challenges to reaching postural accuracy were identified. These suggested that additional instructions should be added to the teaching course or demonstration videos in clinical practice.
Coordinating the mind, the movements and breathing in Baduanjin exercise is only achievable over time, with repeated practice. Unlike other types of exercise, Baduanjin involves both “internal” and “external” effort, and in this way, it trains both the body and the mind. Firstly, while practicing Baduanjin, the practitioner not only must move their body, but also circulate qi (vital energy) throughout the body via their breath. While practicing Baduanjin, a high-level practitioner should breathe in harmony with the movements in order to circulate qi throughout the body. However, a basic-level practitioner would not do it this way, because he or she would only have to concentrate on movement, maintaining natural breath. Secondly, with practice, a novice will gradually be able to concentrate their mind on each movement. However, only by achieving a certain level will they be able to coordinate the breathing and the movements with the guidance of conscious mental effort (10). The importance of the coordination between the mind, the movements and breathing has been reported in a previous qualitative study exploring the mind-body connection during Yoga (41). Hence, this implies the need for more guidance and explanation on the connection between mind, body, and breathing for Baduanjin practitioners in future.
With regular practice and rehearsing of the gentle movements, as well as the coordination of breath, Baduanjin practitioners may improve their strength, physical fitness, and function of multiple organs and systems. In addition to being accessible and learner-friendly, Baduanjin’s eight simple postures are also proven to be suitable in terms of their exercise intensity for CHF patients (23). Moreover, purported mind-body therapy mechanisms may be relevant for CHF pathophysiology, such as targeting various aspects of breathing and relaxation, mitigating sympathetic overdrive, modulating autonomic tone, and addressing the neurohormonal axis (42–44). This finding is consistent with existing literature which indicates that regular Baduanjin practice could promote the physical health of CHF patients. For example, Baduanjin practice can increase one’s capacity for physical activity and general physical fitness (45), enhance cardiopulmonary function (46), and improve sleep quality (21).
In terms of mental health, Baduanjin can relax, calm, and please practitioners’ minds, and therefore improve psychological and mental health. From the perspective of Chinese medicine, qi (vital energy) circulating throughout the body is intertwined with both psychological and mental health. Negative psychological states, for example anger, depression, irritability, and restless mood may stagnate qi. An underlying philosophy of the practice is that Baduanjin cultivates the balance and harmony of qi to maintain a healthy body (47). Baduanjin focuses on mobilizing functional potentialities, regularizing the breathing process, and unifying the mind and body through the regulation of breathing, thereby promoting normal qi circulation (48). Normal qi circulation can also regulate passive emotions. Regarding biological mechanisms, it has been reported that the activity and connectivity of key brain regions pertaining to depression, the autonomic nervous system, and neuroinflammatory sensitization are modulated via mind-body exercise (49, 50). Similarly, an interview study of 20 community elderly individuals who practiced Baduanjin for 40 min every day for 12 weeks reiterated that they felt psychologically relaxed, due to the self-tranquility, the pleasure, and the relief from emotional symptoms (51).
Our findings regarding intrinsic motivation to do Baduanjin exercise provide insight into the high adherence in this sample. “Intrinsic motivation” refers to the inherent satisfaction which individuals derive from physical activity. This includes feelings of enjoyment and accomplishment (52). Intrinsic motivation has been defined as the inherent satisfaction that drives one to undertake a particular activity (52). Motivation is a critical factor underlying sustained exercise. In turn, it is also associated with important health outcomes. In the interview, adherent participants often referenced their improvements as walking further, and improved their moods through participation in Baduanjin training. Therefore, it appears as if both actual and perceived improvements in health may serve as key mechanisms of long-term exercise adherence. This echoes the findings of a qualitative study regarding exercise adherence in patients with CHF (53) which reported that patients with CHF tended to be motivated by improved health and performance in their daily activities (53). Thus, when working with CHF patients starting an exercise program, highlighting improvements can support long-term adherence to exercise. Our findings also demonstrate the importance of autonomous regulation in fostering physical activity. Adherent participants mentioned that whether to exercise was one’s own choice, and that this was primarily decided by the degree to which they cared for their own bodies. This underscores the need to examine the goals and self-regulatory features associated with regular participation in exercise and other forms of physical activity.
Good adherence was also attributed to Baduanjin’s in-home setting. Home-based modalities might be more practical options for increasing patients’ accessibility to EBCR. This is because a third of Chinese CHF patients have been found to either rarely leave the home or are unable to do so due to their symptoms (54). Home-based exercises also empower patients to take personal responsibility and accountability for their disease management (55). Moreover, environmental constraints are mitigated, particularly the challenge of limited healthcare resources, including insufficient rehabilitation facilities, a paucity of medical insurance, and poor access to hospital services in many of China’s rural areas (56). According to a recent consensus statement on EBCR delivery in low-resource settings, safe, equipment-free, cheap, and easy-to-implement exercise modalities provide the most practical options for implementation in China (57).
This study has several strengths. We took several steps to enhance the findings’ credibility. To achieve dependability, we read the interviews several times to derive a general understanding, and there was also frequent comparison between the parts of the analysis and the complete interview texts. All interviews were conducted by one researcher (HZ), which also added to the results’ dependability and she could use experiences from earlier interviews in probing for more information. To achieve confirmability, several researchers with different backgrounds were involved in the analysis process and discussed the findings. This minimized the risk of inventing data or biased interpretation. As this qualitative study was nested in the pilot RCT, current qualitative study should help to explain, support, and complement the findings from the pilot RCT.
Regardless, there remain limitations to this study. Given that this qualitative study was nested in a pilot RCT with a small sample (n = 20), variation in patients’ characteristics were limited to a sub-set with heart failure. For example, all of the study population was male and relatively young; and no patients were included in the study with NYHA I or VI. Although we encouraged participants to elaborate on their perspectives on the research topic, it is possible that female, younger or elderly patients with HF could have different perceptions on Baduanjin. Yet, we still contend that the main findings described above are generally transferrable to other regions of China. This is because that the study participants’ demographic and clinical characteristics are similar to the those CHF patients who are undergoing a cross-sectional survey in Guangzhou (58), and in China in general (54). Moreover, Baduanjin is commonly accepted as being beneficial to one’s health and relatively easy to learn in a short time, it has been a community exercise throughout different regions of Mainland China (59), Taiwan, Macau, and Hong Kong (30, 60). Hence, similar experience of practicing Baduanjin are expected to be found. Moreover, future research should include more participants receiving Baduanjin intervention under the real world treatment environment.
Positive practicing experience and perceived training benefits from Baduanjin was reported among the participants, which indicates that Baduanjin has the potential to become a cardiac rehabilitation exercise modality for CHF patients in China, especially in a home-based setting.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee at the Guangdong Provincial Hospital of Chinese Medicine (number: B2016-202-01). The patients/participants provided their written informed consent to participate in this study.
XkC, WJ, ZW, XxC, and CL contributed to the conception and design of the research. ZW and XxC contributed to obtaining funding. XkC and HZ contributed to data collection and data analysis. XkC, WJ, HZ, and MS contributed to interpretation of the results. XkC and WJ drafted the first version of the manuscript and revised it based on other authors contribution. All authors contributed important intellectual content to the critical revision of the manuscript and read and approved the final manuscript.
This work was supported by the Overseas Experts Program from the Guangdong Science and Technology Commission (2020A1414010352), the General Research Fund of Traditional Chinese Medicine Science and Technology from the Guangdong Provincial Hospital of Chinese Medicine (YN2018ML02), and the Clinical Research Fund of the Traditional Chinese Medicine Science and Technology (Project 1010) from Guangdong Provincial Hospital of Chinese Medicine (YN10101910). This study was part of a Ph.D. thesis supported by the China Scholarships Council (201608440264).
We thank our professional coach (Haojian Yu) from the GPHCM for teaching the exercise, and our cardiology nurse (Yunxiang Fan) from the GPHCM for assistance with collecting data. Results of the upload manuscript were partially presented as an abstract at the 23rd Annual Scientific Meeting of the Heart-Failure-Society-of-America (HFSA) and the American Association of Cardiovascular and Pulmonary Rehabilitation 34th Annual Meeting. Some parts of the results in this manuscript were included the doctoral thesis of XkC and have been appeared online: https://openarchive.ki.se/xmlui/handle/10616/47582.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
BESMILE-HF, Baduanjin Eight-Silken-Movement wIth SeLf-Efficacy building for Heart Failure; CHF, chronic heart failure; EBCR, exercise-based cardiac rehabilitation; GPHCM, Guangdong Provincial Hospital of Chinese Medicine; NYHA, New York Heart Association functional; RCT, randomized controlled trial.
1. Zhang J, Zhang Y. Heart failure registry study a multicenter, prospective investigation for preliminary analysis on etiology, clinical features and treatment in heart failure patients. Chin Circ J. (2015) 30:413–6. doi: 10.1186/s13054-016-1208-6
2. Yancy CW, Jessup M, Bozkurt B, Butler J, Casey DE, Colvin MM, et al. 2016 ACC/AHA/HFSA focused update on new pharmacological therapy for heart failure: an update of the 2013 ACCF/AHA guideline for the management of heart failure: a report of the American college of cardiology/American heart association task force on clinical practice guidelines and the heart failure society of America. J Card Fail. (2016) 22:659–69. doi: 10.1016/j.cardfail.2016.07.001
3. Fleg JL, Cooper LS, Borlaug BA, Haykowsky MJ, Kraus WE, Levine BD, et al. Exercise training as therapy for heart failure: current status and future directions. Circ Heart Fail. (2015) 8:209–20. doi: 10.1161/circheartfailure.113.001420
4. Taylor RS, Sagar VA, Davies EJ, Briscoe S, Coats AJ, Dalal H, et al. Exercise-based rehabilitation for heart failure. Cochrane Database Syst Rev. (2014) 2014:Cd003331. doi: 10.1002/14651858.CD003331.pub4
5. Turk-Adawi K, Sarrafzadegan N, Grace SL. Global availability of cardiac rehabilitation. Nat Rev Cardiol. (2014) 11:586–96. doi: 10.1038/nrcardio.2014.98
6. Dalal HM, Wingham J, Palmer J, Taylor R, Petre C, Lewin R. Why do so few patients with heart failure participate in cardiac rehabilitation? A cross-sectional survey from England, Wales and Northern Ireland. BMJ Open. (2012) 2:e000787. doi: 10.1136/bmjopen-2011-000787
7. Zhang Z, Pack Q, Squires RW, Lopez-Jimenez F, Yu L, Thomas RJ. Availability and characteristics of cardiac rehabilitation programmes in China. Heart Asia. (2016) 8:9–12. doi: 10.1136/heartasia-2016-010758
8. Jin H, Wei Q, Chen L, Sun Q, Zhang Y, Wu J, et al. Obstacles and alternative options for cardiac rehabilitation in Nanjing, China: an exploratory study. BMC Cardiovasc Disord. (2014) 14:20. doi: 10.1186/1471-2261-14-20
9. Conraads VM, Deaton C, Piotrowicz E, Santaularia N, Tierney S, Piepoli MF, et al. Adherence of heart failure patients to exercise: barriers and possible solutions: a position statement of the study group on exercise training in heart failure of the heart failure association of the european society of cardiology. Eur J Heart Fail. (2012) 14:451–8. doi: 10.1093/eurjhf/hfs048
10. Koh TC. Baduanjin – an ancient Chinese exercise. Am J Chin Med. (1982) 10:14–21. doi: 10.1142/s0192415x8200004x
11. Wang N, Guo Y. Traditional Chinese practice, a promising integrative intervention for chronic non-infectious disease management. Chin J Integr Med. (2018) 24:886–90. doi: 10.1007/s11655-018-2572-7
12. Guangdong Provincial Health Publicity and Education Center, Guangdong Provincial Hospital of Chinese Medicine. Baduanjin Exercises [YouTube]. (2020). Available online at: https://www.youtube.com/watch?v=i2YY6t1JhCY&list=PLPCWVScVb76h (accessed June 29, 2020).
13. Guangdong Provincial Health Publicity and Education Center, Guangdong Provincial Hospital of Chinese Medicine. Baduanjin Exercise (Tutorial) [YouTube]. (2020). Available online at: https://www.youtube.com/watch?v=UculAU8mWd8 (accessed June 29, 2020).
14. Pozehl B, Duncan K, Hertzog M, Norman JF. Heart failure exercise and training camp: effects of a multicomponent exercise training intervention in patients with heart failure. Heart Lung. (2010) 39(6 Suppl.):S1–13. doi: 10.1016/j.hrtlng.2010.04.008
15. Sun XG. Rehabilitation practice patterns for patients with heart failure: the Asian perspective. Heart Fail Clin. (2015) 11:95–104. doi: 10.1016/j.hfc.2014.09.001
16. Zou L, Sasaki JE, Wang H, Xiao Z, Fang Q, Zhang MA. Systematic review and meta-analysis of Baduanjin Qigong for health benefits: randomized controlled trials. Evid Based Complement Altern Med. (2017) 2017:4548706. doi: 10.1155/2017/4548706
17. Xiong X, Xu D. Therapeutic effect of Baduanjin on patients with coronary heart disease and chronic heart failure [in Chinese]. China Mod Med J. (2016) 18:55–6.
18. Yang X., Feixiang Huang, Yongchao Shi, Yanxia Wang, Ye L. Effect of Aerobics training on exercise tolerance in patients with chronic heart failure [in Chinese]. Chin J Nurs. (2015) 50:193–7.
19. Yan X. Effects of Liuzi and Ba Duan Jin training on exercise tolerance in patients with chronic heart failure [in Chinese]. Chin Trad Med Modern Distance Educ. (2016) 14:126–8.
20. Jing Y. Effect of TCM Aerobics on exercise endurance in patients with chronic heart failure [in Chinese]. Chin Trad Med Modern Distance Educ. (2015) 13:12–4.
21. Chen DM, Yu WC, Hung HF, Tsai JC, Wu HY, Chiou AF. The effects of Baduanjin exercise on fatigue and quality of life in patients with heart failure: a randomized controlled trial. Eur J Cardiovasc Nurs. (2017) 17:456–66. doi: 10.1177/1474515117744770
22. Li R. Observation on the improvement of cardiac function and quality of life in elderly patients with chronic heart failure by Ba Duan Jin [in Chinese]. Massage Rehabil Med. (2017) 8:23–5.
23. Chen X, Marrone G, Olson TP, Lundborg CS, Zhu H, Wen Z, et al. Intensity level and cardiorespiratory responses to Baduanjin exercise in patients with chronic heart failure. ESC Heart Fail. (2020) 7:3782–91. doi: 10.1002/ehf2.12959
24. Mei L, Chen Q, Ge L, Zheng G, Chen J. Systematic review of chinese traditional exercise baduanjin modulating the blood lipid metabolism. Evid Based Complement Altern Med. (2012) 2012:282131. doi: 10.1155/2012/282131
25. Chan JS, Ho RT, Chung KF, Wang CW, Yao TJ, Ng SM, et al. Qigong exercise alleviates fatigue, anxiety, and depressive symptoms, improves sleep quality, and shortens sleep latency in persons with chronic fatigue syndrome-like illness. Evid Based Complement Altern Med. (2014) 2014:106048. doi: 10.1155/2014/106048
26. Liao Y, Lin Y, Zhang C, Xue XL, Mao QX, Zhang Y, et al. Intervention effect of Baduanjin exercise on the fatigue state in people with fatigue-predominant subhealth: a cohort study. J Altern Complement Med. (2015) 21:554–62. doi: 10.1089/acm.2014.0395
27. Xiong X, Wang P, Li S, Zhang Y, Li X. Effect of Baduanjin exercise for hypertension: a systematic review and meta-analysis of randomized controlled trials. Maturitas. (2015) 80:370–8. doi: 10.1016/j.maturitas.2015.01.002
28. Li M, Fang Q, Li J, Zheng X, Tao J, Yan X, et al. The effect of Chinese traditional exercise-Baduanjin on physical and psychological well-being of college students: a randomized controlled trial. PLoS One. (2015) 10:e0130544. doi: 10.1371/journal.pone.0130544
29. Cheng FK. Effects of Baduanjin on mental health: a comprehensive review. J Bodyw Mov Ther. (2015) 19:138–49. doi: 10.1016/j.jbmt.2014.11.001
30. Chen MD, Yeh YC, Tsai YJ, Chang YC, Yu JW, Hsu CH. Efficacy of Baduanjin exercise and feasibility of mobile text reminders on follow-up participation in people with severe mental illness: an exploratory study. J Psychiatr Pract. (2016) 22:241–9. doi: 10.1097/pra.0000000000000158
31. Chen X, Savarese G, Cai Y, Ma L, Lundborg CS, Jiang W, et al. Tai Chi and Qigong practices for chronic heart failure: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Altern Med. (2020) 2020:2034625. doi: 10.1155/2020/2034625
32. Verhoef MJ, Lewith G, Ritenbaugh C, Boon H, Fleishman S, Leis A. Complementary and alternative medicine whole systems research: beyond identification of inadequacies of the RCT. Complement Ther Med. (2005) 13:206–12. doi: 10.1016/j.ctim.2005.05.001
33. Guangdong Government. 2015 Population Scope and Distribution in Guangzhou Population Department of Guangzhou Statistics Bureau. (2015). Available online at: https://www.ceicdata.com/en/china/population-prefecture-level-city-by-census/population-census-guangdong-guangzhou (accessed November 11, 2016).
34. Chief editor of Cardiovascular Committee of Chinese Rehabilitation Association. Chinese Guidelines for Cardiac Rehabilitation and Secondary Prevention 2018. 2nd ed. Beijing: Peking University Medical Press (2018).
35. Chen X, Jiang W, Lin X, Lundborg CS, Wen Z, Lu W, et al. Effect of an exercise-based cardiac rehabilitation program “Baduanjin Eight-Silken-Movements with self-efficacy building” for heart failure (BESMILE-HF study): study protocol for a randomized controlled trial. Trials. (2018) 19:150. doi: 10.1186/s13063-018-2531-9
36. Chen X, Jiang W, Olson TP, Lundborg CS, Wen Z, Lu W, et al. Feasibility and preliminary effects of the BESMILE-HF program on chronic heart failure patients: a pilot randomized controlled trial. Front Cardiovasc Med. (2021) 8:715207. doi: 10.3389/fcvm.2021.715207
37. Xiankun C. Traditional Chinese Exercise in a Contextually Adapted Cardiac Rehabilitation Program for Chronic Heart Failure. Sweden: Karolinska Institutet (2020).
38. Tierney S, Mamas M, Skelton D, Woods S, Rutter MK, Gibson M, et al. What can we learn from patients with heart failure about exercise adherence? A systematic review of qualitative papers. Health Psychol. (2011) 30:401–10. doi: 10.1037/a0022848
39. Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs. (2008) 62:107–15. doi: 10.1111/j.1365-2648.2007.04569.x
40. Xiong KY, He H, Ni GX. Effect of skill level on cardiorespiratory and metabolic responses during Tai Chi training. Eur J Sport Sci. (2013) 13:386–91. doi: 10.1080/17461391.2011.635706
41. Guddeti RR, Dang G, Williams MA, Alla VM. Role of Yoga in cardiac disease and rehabilitation. J Cardiopulm Rehabil Prev. (2019) 39:146–52. doi: 10.1097/hcr.0000000000000372
42. Jindal V, Gupta S, Das R. Molecular mechanisms of meditation. Mol Neurobiol. (2013) 48:808–11. doi: 10.1007/s12035-013-8468-9
43. Taylor AG, Goehler LE, Galper DI, Innes KE, Bourguignon C. Top-down and bottom-up mechanisms in mind-body medicine: development of an integrative framework for psychophysiological research. Explore. (2010) 6:29–41. doi: 10.1016/j.explore.2009.10.004
44. Wayne PM, Kaptchuk TJ. Challenges inherent to t’ai chi research: part I–t’ai chi as a complex multicomponent intervention. J Altern Complement Med. (2008) 14:95–102. doi: 10.1089/acm.2007.7170a
45. Yu M. A Randomized Controlled Study on the Application of Baduanjin in Patients with Coronary Heart Disease and Chronic Heart Failure. [PhD Thesis in Chinese]. Beijing: Beijing University of Traditional Chinese Medicine (2018).
46. Shi Z. Clinical Study of Baduanjin on Rehabilitation Treatment of Patients with Chronic Heart Failure. [Master Thesis in Chinese]. Liaoning: Liaoning University of Traditional Chinese Medicine (2018).
47. Qu J, Wang X. Traditional Chinese Exercises. Newcastle-upon-Tyne: Cambridge Scholars Publishing (2015).
48. Hankey A, McCrum S. QIGONG: life energy and a new science of life. J Altern Complement Med. (2006) 12:841–2. doi: 10.1089/acm.2006.12.841
49. Cheng D, Wang B, Li Q, Guo Y, Wang L. Research on function and mechanism of tai chi on cardiac rehabilitation. Chin J Integr Med. (2020) 26:393–400. doi: 10.1007/s11655-020-3262-9
50. Kong J, Wilson G, Park J, Pereira K, Walpole C, Yeung A. Treating depression with Tai Chi: state of the art and future perspectives. Front Psychiatry. (2019) 10:237. doi: 10.3389/fpsyt.2019.00237
51. Zheng G, Fang Q, Chen B, Yi H, Lin Q, Chen L. Qualitative evaluation of Baduanjin (Traditional Chinese Qigong) on health promotion among an elderly community population at risk for ischemic stroke. Evid Based Complement Altern Med. (2015) 2015:893215. doi: 10.1155/2015/893215
52. Teixeira PJ, Carraça EV, Markland D, Silva MN, Ryan RM. Exercise, physical activity, and self-determination theory: a systematic review. Int J Behav Nutr Phys Activ. (2012) 9:78. doi: 10.1186/1479-5868-9-78
53. Warehime S, Dinkel D, Alonso W, Pozehl B. Long-term exercise adherence in patients with heart failure: a qualitative study. Heart Lung. (2020) 49:696–701.
54. Jackson JD, Cotton SE, Bruce Wirta S, Proenca CC, Zhang M, Lahoz R, et al. Burden of heart failure on patients from China: results from a cross-sectional survey. Drug Design Dev Ther. (2018) 12:1659–68. doi: 10.2147/DDDT.S148949
55. Zwisler AD, Norton RJ, Dean SG, Dalal H, Tang LH, Wingham J, et al. Home-based cardiac rehabilitation for people with heart failure: a systematic review and meta-analysis. Int J Cardiol. (2016) 221:963–9. doi: 10.1016/j.ijcard.2016.06.207
56. Thompson DR, Yu C-M. Cardiac rehabilitation: China. In: Perk J, Mathes P, Gohlke H, Monpere C, Hellemans I, McGee H, et al. editors. Cardiovascular Prevention and Rehabilitation. London: Springer (2007).
57. Grace SL, Turk-Adawi KI, Contractor A, Atrey A, Campbell N, Derman W, et al. Cardiac rehabilitation delivery model for low-resource settings. Heart. (2016) 102:1449–55. doi: 10.1136/heartjnl-2015-309209
58. Lai SW. The Investigation of the Current Status of the Use of Traditional Chinese Medicine (TCM) Exercise Regimen in Patients with Chronic Heart Failure. [PhD Thesis]. Sanyuanli: Guangzhou University of Traditional Chinese Medicine (2014).
59. Health Qigong Management Center of General Administration of Sport of China. Health Qigong-Baduanjin. Beijing: People’s Sports Publishing House of China (2003).
Keywords: Baduanjin, chronic heart failure, experience, qualitative study, cardiac rehabilitation
Citation: Chen X, Jiang W, Salazar M, Zhu H, Wen Z, Chen X and Lundborg CS (2023) Traditional Baduanjin exercise through the eyes of patients with chronic heart failure: A qualitative content analysis study. Front. Cardiovasc. Med. 9:1049036. doi: 10.3389/fcvm.2022.1049036
Received: 20 September 2022; Accepted: 08 December 2022;
Published: 04 January 2023.
Edited by:
Hongcai Shang, Beijing University of Chinese Medicine, ChinaReviewed by:
Chen Zhao, China Academy of Chinese Medical Sciences, ChinaCopyright © 2023 Chen, Jiang, Salazar, Zhu, Wen, Chen and Lundborg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zehuai Wen, ✉ d2VuemhAZ3p1Y20uZWR1LmNu; Xixi Chen, ✉ Y2hlbnhpeGlAZ3pjdW0uZWR1LmNu
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.