 Xiao Zhang1,2,3
Xiao Zhang1,2,3 Zhao Huangfu4*
Zhao Huangfu4*- 1Department of Gynecology and Obstetrics, Beijing Hospital, National Center of Gerontology, Beijing, China
- 2Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, China
- 3Peking Union Medical College, Graduate School of Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, China
- 4Department of Urology, Changhai Hospital, Naval Medical University, Shanghai, China
Pregnant individuals with pulmonary arterial hypertension (PAH) have significantly high risks of maternal and perinatal mortality. Profound changes in plasma volume, cardiac output and systemic vascular resistance can all increase the strain being placed on the right ventricle, leading to heart failure and cardiovascular collapse. Given the complex network of opposing physiological changes, strict contraception and reduction of hemodynamic fluctuations during pregnancy are important methods of minimizing the risk of maternal mortality and improving the outcomes following pregnancy. In this review, we discuss the recent research progress into pre-conception management and the various therapeutic strategies for pregnant individuals with PAH.
Introduction
Pulmonary arterial hypertension (PAH) is characterized by increased pulmonary artery pressure and vascular resistance, leading to increased right ventricular afterload, dysfunction or even failure which can be fatal (1). In 2016, it was estimated that a PAH prevalence of ~1% of the global population (2). Additionally, PAH prevalence in the United Kingdom has doubled in the last decade and is currently 125 cases/million person1. PAH among pregnant women confers high risks of mortality for both the mother and fetus. The adverse outcomes of PAH are exacerbated by the physiologic changes of pregnancy, which contribute to a high maternal mortality reaching 30–56% and a high neonatal mortality reaching 13% (3). With the improved treatment of PAH, maternal mortality has declined but remains high, ranging 11–25% (4–8). Given the high risk following pregnancy, appropriate contraception and reduction of hemodynamic fluctuations during pregnancy is key to reducing this risk of maternal mortality and improving pregnancy outcomes. In this review, we summarized the classification systems of PAH, strategies devised for preconception counseling and treatment strategies developed that are or will soon become available for pregnant women with PAH.
Definition and classification
PAH is a heterogeneous disease that is characterized by an elevated mean pulmonary artery pressure of ≥20 mmHg at rest as per the 2022 European Society of Cardiology/European Respiratory Society (ESC/ERS) guidelines (1, 9). When echocardiographic tricuspid regurgitation velocity exceeds the threshold (>2.8 m/s), PAH should also be highly suspected according to the updated hemodynamic definition (10). It can be classified into the following five main groups based on the 2022 ESC/ERS guidelines: (i) Group 1, PAH; (ii) Group 2, PAH associated with left heart disease; (iii) Group 3, PAH associated with lung disease and/or hypoxia; (iv) Group 4, PAH associated with pulmonary artery obstructions; and (v) Group 5, PAH with unclear and/or multifactorial mechanisms (11) (Table 1).
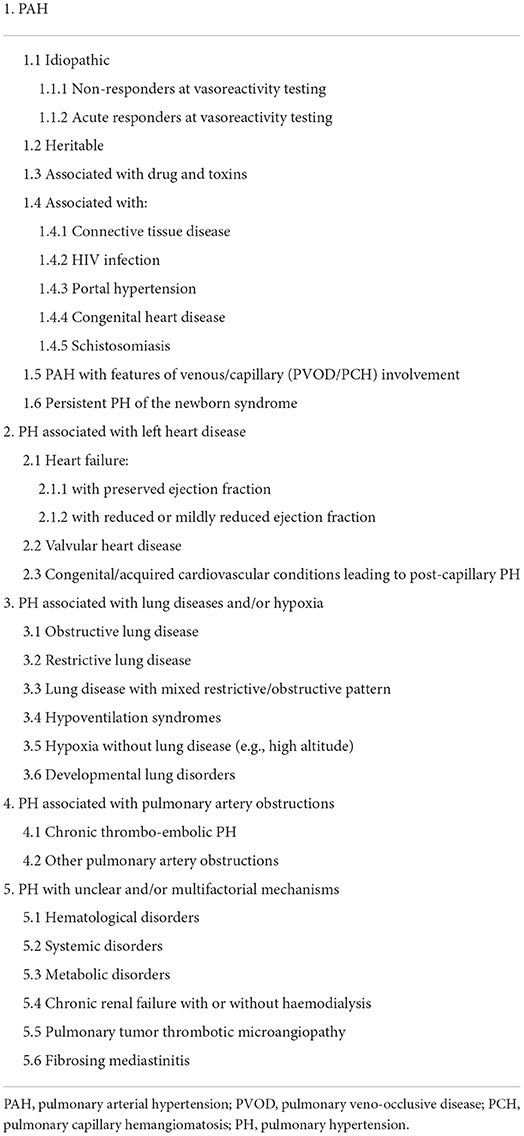
Table 1. Updated classification from the 2022 ESC/ERS guidelines.
Preconception management
Contraceptives
The 2022 ESC/ERS guidelines recommended that all patients with PAH should be treated with contraception using a strict regimen (9). Although pregnancy may be feasible in some PAH patients with well-controlled disease, a low-risk profile, and normal or near-normal resting hemodynamics, for women with poorly controlled disease or women without fertility requirements, effective contraception is essential in view of the possible harm caused by contraceptive failure (12). The use of progesterone-only oral contraceptives, condoms, intrauterine contraceptive devices, or emergency post-coital contraception after intercourse is effective for PAH patients (9, 13). However, considering the obstacles of drug-drug interactions, potential contraindications to hormonal interventions (e.g., thromboembolism) and unreliability of contraceptive tools, a number of reports previously proposed that a combination of two or more contraceptive methods should be used, especially for patients with PAH treated with endothelin receptor antagonists (14–16). Tubal ligation is also an effective way to achieve permanent contraception, but patients have to face some risks of anesthesia accidents and complications since it is an invasive procedure. Therefore, tubal ligation can be performed at the same time when a woman is undergoing another surgery, such as cesarean section, reducing the risk of multiple surgeries. In addition, micro-insertion hysteroscopic sterilization is one of the effective contraceptive methods for patients with PAH due to its apparently lower surgical risk (17, 18).
Preconception counseling
Because of high risk of adverse pregnancy outcomes and inherited heart defects (19, 20), the 2022 ESC/ERS guidelines recommended that women with PAH who are considering pregnancy or having already been pregnant should receive genetic counseling and shared decision-making at experienced medical centers (9). Fetal genetic testing should also be performed in pregnant women with known PAH-associated genetic mutations (21). Even though genetic testing is not performed, family members should be made aware of early signs and symptoms, to ensure that a timely and appropriate diagnosis is made (22). In fact, in addition to counseling on the risks associated with maternal mortality, patients at high risk should be informed about the option of avoiding pregnancy and therapeutic abortion. In such cases, alternatives such as adoption and surrogacy (if legal) may also be explored (9).
Treatment
Although PAH patients have been required to take strict contraception, there are still some patients who do not take it because PAH has not been diagnosed before pregnancy, or still insist on pregnancy despite being aware of the higher pregnancy risks (23). Therefore, early drug intervention, comprehensive multidisciplinary assessment and co-management could become key factors in improving maternal and fetus outcomes (13, 16, 24). The principles of treatment for pregnant women with PAH are relieving clinical symptoms, enhancing exercise tolerance and improving pulmonary circulation hemodynamics. A summary of the Food and Drug Administration Pharmaceutical Categories in pregnancy and relevant PAH-associated therapeutic drugs are shown in Tables 2, 3, respectively.
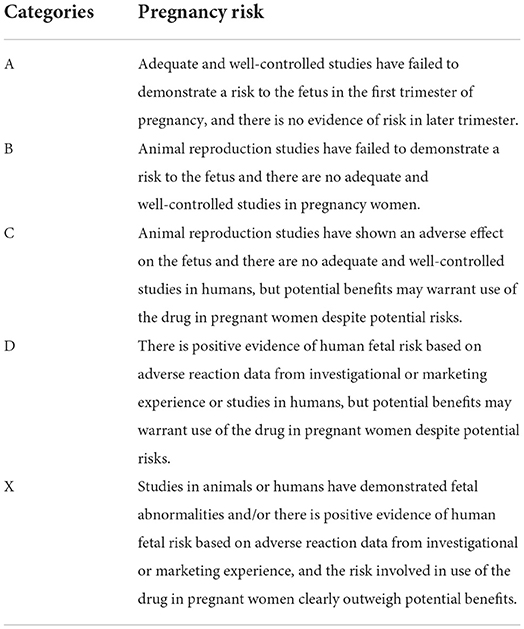
Table 2. United States of America food and drug administration (FDA) pharmaceutical categories in pregnancy.
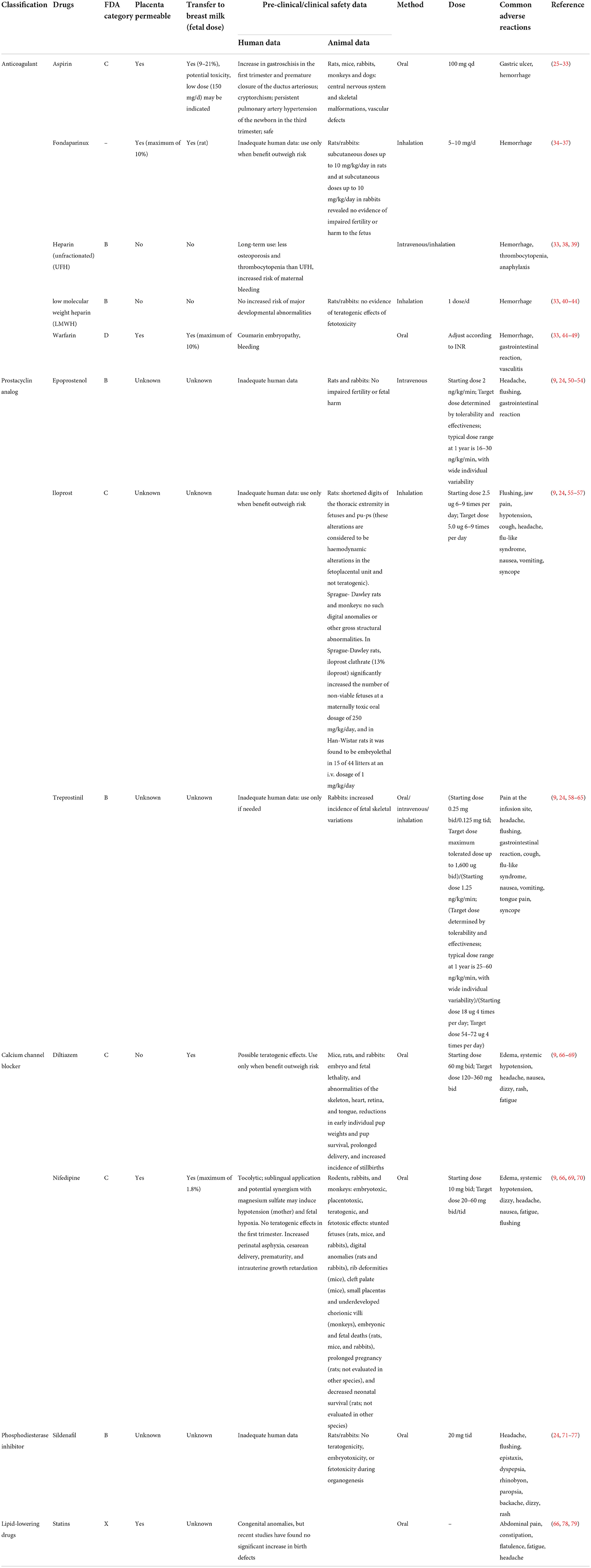
Table 3. Drugs and safety data.
General management
Pregnant women with PAH should avoid excessive activity but should still be encouraged to be active within symptom limits (16, 80). Whenever possible, lateral position should always be taken to minimize the compression of the inferior vena cava in the third trimester. Elastic support stockings can also be used whilst walking to avoid drastic changes in blood volume. In addition, appropriate supplementation of iron and folic acid should be encouraged to prevent anemia, whereas vaccination at least against influenza, Streptococcus pneumoniae and SARS-CoV-2 before pregnancy is recommended to enhance immunity (9, 81, 82).
For patients with PAH who decide to continue pregnancy, a standardized, individualized and realistic diagnosis and treatment plan should be formulated. They should receive regular and stringent evaluation and examination by clinicians from multiple disciplinary backgrounds during the pregnancy period (83). Prenatal check-ups should be performed every 2 weeks before 20 weeks and then once a week after 20 weeks of gestation. In addition to the routine obstetric examination, classification of the primary disease causing PAH, primary symptoms of PAH, cardiac function, echocardiography, 6-min walk test and biochemical indicators, including platelet count, hemoglobin, brain natriuretic peptide levels and arterial blood gas analysis, should also be focused upon (23). Since fetuses of pregnant women with PAH typically exhibit different degrees of growth restriction, ultrasound should be performed to examine the status of fetal growth at each obstetric examination (7, 13, 23). Hospitalization would be required if the condition worsens. Management by a multidisciplinary team is necessary for pregnant women with moderate to severe PAH (mWHO II-IV). This expert team should at least include a cardiologist, an ophthalmologist and an anesthesiologist with expertise in managing high-risk pregnant women with cardiac diseases. Furthermore, according to the unique scenarios posed by each patient, to produce a detailed delivery and emergency plan that includes the possibility of extracorporeal membrane oxygenation (ECMO) or transplantation, other specialists, including those who with extensive knowledge in pharmacy, cardiothoracic surgery, fetal medicine, neonatology, hematology, nursing and respiratory medicine, should be involved (1, 84). In fact, considering the high prevalence of symptoms of depression, anxiety and adjustment disorders in patients with PAH, empathic and hopeful communication is also crucial for physicians caring for pregnant women with PAH (9).
Supportive therapy
Oxygen therapy
Oxygen inhalation is recommended when the peripheral oxygen saturation is < 90% or arterial oxygen partial pressure is < 60 mmHg. Maintaining the arterial partial pressure of oxygen at >70 mmHg and the oxygen saturation at >92% can reduce pulmonary vascular resistance, right-to-left shunt and the incidence of low-birth-weight infants (85). Nocturnal oxygen therapy should be considered in case of sleep-related desaturation (86). Oxygen inhalation should also be considered when pregnant patients with PAH travel by air, especially those with New York Heart Association (NYHA) class III-IV PAH or with the arterial partial pressure of oxygen < 8 kPa (87, 88). Although oxygen administration reduces pulmonary vascular resistance and improves exercise toleration in patients with PAH, there are no data to suggest that long-term oxygen therapy has sustained benefits on the course of the disease (9).
Diuretics, cardiotonics and antiarrhythmics
Diuretics can relieve the symptoms of decompensation following right heart failure. Torasemide or furosemide are options of loop diuretics during pregnancy. However, spironolactone should be avoided during the first trimester because due to its antiandrogenic effects (13, 66, 89, 90). During the use of diuretics, regular monitoring of kidney function and serum electrolytes is necessary to avoid intravascular volume depletion and further decline in cardiac output and systemic blood pressure.
Cardiac agents, including digoxin or milrinone, can improve cardiac output in patients with PAH, although their long-term efficacy remains unclear. In addition, maintenance of sinus rhythm is important, because atrial fibrillation and supraventricular tachycardia are associated with the occurrence of right heart failure and subsequent mortality (91). Intravenous adenosine is the priority treatment method for acute episodes of paroxysmal supraventricular tachycardia (PSVT). By contrast, β-adrenergic receptor blockers, with the exception of atenolol, are first-line drugs for PSVT prevention. Electrical cardioversion is also recommended when patients with atrial fibrillation become hemodynamically unstable or if they are considered to be at great risk of mortality (92). Ibutilide or flecainide injections may be considered to eliminate atrial fluttering and atrial fibrillation in PAH patients with structurally normal hearts (93). By the same token, since patients with congenital heart disease do not typically tolerate atrial flutter effectively, electrical cardioversion should be performed to restore sinus rhythm (94). Idiopathic right ventricular outflow tract tachycardia is the most common type of ventricular tachycardia, which requires β-adrenergic receptor blockers, verapamil or other antiarrhythmic prophylactics. If drug treatment fails, catheter ablation would then be needed. If possible, catheter ablation should be delayed until the second trimester and performed at a well-equipped medical center containing experts with extensive experience (95, 96). In addition, occasional sinus bradycardia may be associated with the supine hypotensive syndrome. Symptomatic bradycardia should be treated with changes in maternal position, following which temporary pacemaker should be installed if clinical symptoms persist (97, 98). Temporary pacemakers are usually not required in hemodynamically stable patients but are recommended during labor in women at risk of bradycardia or those with a history of syncope (97). Implantable cardioverter defibrillators should also be considered before pregnancy in patients at high risk of sudden cardiac death (80, 99).
Anticoagulant therapy
Pregnant women frequently present with hypercoagulability, which can increase the risk of thrombosis. Anticoagulants are recommended for reducing the risk of thrombosis if cardiopulmonary dysfunction was detected in the pregnant individual with PAH. The choice of anticoagulant drugs should be comprehensively considered based on the individual involved, gestational stage, risk of maternal bleeding and teratogenic effects (15, 100). Due to low molecular weight heparin (LMWH) having lower reported levels of impact on the fetus and lower risks in terms of osteoporosis, it is considered to be the priority drug for preventing and treating venous thromboembolism during pregnancy and puerperium. However, the preventive effect of valve thrombosis conferred by LMWH is weak (38). If LMWH or unfractionated heparin (UFH) is used during pregnancy, then it is recommended to calculate the initial dose according to the maternal weight in the first trimester (8–10 gestational weeks). The dose should be subsequently adjusted by monitoring the anti-factor Xa levels or partial thromboplastin time weekly until the 4- to 6-h peak anti-Xa levels reached 0.6–1.2 IU/ml (1, 101). Fondaparinux may even be considered for PAH patients if they are allergic to LMWH. Warfarin can pass through the placenta and may exert dose-dependent teratogenic effects, which can lead to “Fetal Warfarin Syndrome” (102). Therefore, warfarin should be used at limited dosages or be replaced with LMWH during the first trimester. The dosage of warfarin needs to be limited to < 5 mg/d and the international normalized ratio (INR) should be adjusted to 1.5–2.0 during the second and third trimesters. However, the safety profile of warfarin in pregnant women remains controversial and should therefore be avoided where possible during pregnancy (40, 45, 103–106). In addition, high-quality evidence supporting the safety and efficacy of novel oral anticoagulants, such as dabigatran, rivaroxaban and apixaban, in pregnant women with remain elusive obstructing their recommendation for use (107, 108). A meta-analysis of 339 pregnant women on new direct oral anticoagulants previously revealed that 22.2% suffered from miscarriages, whilst 3.6% had fetuses with skeletal and facial deformities (109). In particular, all patients had to terminate oral anticoagulation during the first 2 months of pregnancy, suggesting that the novel oral anticoagulation regimens used during pregnancy may be associated with higher risks of miscarriage and birth defects (110).
Oral anticoagulants should be replaced with LMWH or UFH 3–5 days before delivery, which would render it safer for cesarean sections. However, LMWH should be stopped 12–24 h before delivery, whereas UFH should be stopped >4–7 days before delivery. Protamine antagonism can be carefully applied for pregnant women requiring the emergency termination of pregnancy but did not stop heparin treatment. By contrast, warfarin can be antagonized by vitamin K1 antagonism (15, 111–113). If there is no obvious bleeding for 24 h after delivery, anticoagulation therapy can be resumed. It should however be noted that patients who were treated with warfarin prior should instead be administered with LMWH and have the INR monitored for several days after delivery. LMWH can then be stopped after warfarin comes into effect.
PAH-specific therapy
Currently available drugs targeting the pathological pathways underlying PAH did not result in the complete reversal of the condition but have been found to reduce pulmonary artery pressure and alleviate clinical symptoms. For patients with stable hemodynamics, routine use of vasodilators and other drugs that can interfere with hemodynamics is not recommended. However, for patients with unstable hemodynamics, addition of pulmonary vasodilators on cumulatively on the existing general treatment regimens can significantly reduce the risk of maternal mortality and adverse pregnancy outcomes (14, 114). These vasodilators include calcium channel blockers (CCB) (4, 6, 115), prostaglandins and associated analogs (7, 50, 51, 55, 116) and phosphodiesterase inhibitors (PDE-I) (117), but no endothelin receptor antagonists due to the teratogenic potential (118, 119). Pieper et al. suggested that pharmacological treatment of PAH should be started at ≥3 months before delivery, because the optimal effects did not appear until 3 months later (14). However, since the use of pulmonary vasodilators in pregnant women may endanger the safety of the fetus, their application must be evaluated with their standard formulations and usage requiring additional support by high-quality evidence-based research.
Prostaglandins and analogs
Prostacyclin can inhibit smooth muscle proliferation, reverse vascular remodeling, expand pulmonary and systemic circulation, enhance right ventricular function and exert anti-platelet effects (120). However, thrombocytopenia and bleeding-related complications may occur after the patients are treated with anticoagulants and prostacyclin at the same time. Therefore, blood routine and coagulation function parameters should be monitored closely (45). Indications of initiation use of prostaglandins are typically patients with WHO FC class III-IV PAH or impaired right ventricular function (88, 121–123).
At present, epoprostenol is the most widely used targeted drug in pregnant women with PAH (62%), which is also the first-line drug for the treatment of pregnancy with PAH or Eisenmenger syndrome (52, 124–126). Epoprostenol can improve exercise capacity, quality of life and survival rate (120). Due to its slow onset time and short half-life, it is recommended to commence treatment with this drug ≥8 weeks prior to delivery through the central venous catheter (120). It can also be used postpartum for preventing pulmonary hypertension crisis and right heart failure (127, 128). There is a lack of data and experience on the safety of this drug on the fetus, but several studies showed that it did not cause fetal malformation or intrauterine growth restriction in the third trimester (55, 116). Adverse reactions associated with the long-term use of epoprostenol may include facial flushing, headache, diarrhea, abdominal pain, uterine contractions, and postpartum hemorrhage. However, dosage reduction is only required when the adverse reactions become severe.
Iloprost is an inhaled prostacyclin analog that is frequently used to relieve dyspnea during surgery. The onset time is generally 15–20 min and the duration of drug effects is 1–2 h (125, 127, 129). Compared with intravenous administration, short-term application of aerosol iloprost inhalation tend to be more effective in reducing pulmonary arterial pressure (6, 7, 55). At present, there is no evidence indicating that inhaled iloprost can cause maternal mortality or congenital fetal anomalies. However, it was indicated that inhalation of iloprost within 24 weeks of gestation and perinatal period can significantly reduce the risk of fetal malformations and mortality (55, 114, 130). It is noteworthy that intravenous epoprostenol should be applied if the disease worsens after inhaling iloprost (52, 114). Inhaled prostaglandins are generally used for patients with less severe symptoms of PAH due to the short half-time caused by intermittent nebulized administration, which may lead to rebounds in pulmonary artery pressure (13, 55). However, it is a sign of serious condition if patients with PAH take iloprost before conception.
Treprostinil can be administered through various means, including subcutaneous infusion, intravenous and oral administration (131). This drug can be used for patients with WHO cardiac function class II-IV or NYHA III-IV PAH. It has been reported to significantly improve the 6-min walking distance, peripheral blood oxygen saturation and cardiac function (132). However, some patients (about 8%) refused to use this drug due to the infusion-site pain (133).
CCBs
A number of pregnant women with PAH may benefit from CCBs. However, CCBs are only typically used in patients whose acute pulmonary vasodilation test results are positive (4, 6, 85, 115). Diltiazem is the first choice CCBs for patients with fast heart rhythm, whereas nifedipine is used for patients with slow heart rhythm. The minimum dose should be used at first with the dose increasing gradually according to blood pressure, cardiac rhythm, heart rate, electrocardiogram results and clinical symptoms until the maximum tolerated dose is reached. If the right heart structure and function remain at physiological levels and the pulmonary arterial pressure is normal or close to normal (mean pulmonary arterial pressure ≤30 mmHg and pulmonary vascular resistance < 4 WU) after receiving CCB therapy, it can be adjudged that the patient is continuously sensitive to CCBs, meaning that it can be applied chronically. If there is no satisfactory response, additional PAH therapy should be instituted. However, various studies showed that CCBs are not able to mediate long-term vasodilation effects on patients with PAH, where exposure to CCBs in the third trimester may increase the risk of neonatal seizures (Odd ratio = 3.6) (134, 135). Therefore, it is necessary to consider the gradual conversion from CCBs to prostaglandins or analogs or PDE-I if cardiac function and pulmonary artery pressure are not maintained at normal levels (127).
PDE-I
PDE-5 inhibitors are the priority drug for women with WHO cardiac function class I-II PAH or normal right ventricular function (5, 71, 136). The expression levels of PDE-5 in the right ventricular myocardium are frequently found to be increased in patients with PAH. PDE-5 inhibitors can reverse this change to relax vascular smooth muscles and reduce the pulmonary artery pressure (6). In addition, the use of PDE-5 inhibitors does not change lactate levels or pH levels in the fetus. Sildenafil is the most extensively applied PDE-5 inhibitor. It has been previously found that sildenafil can significantly improve the clinical symptoms, cardiac function, hemodynamic indices and pregnancy outcomes (111). It can also increase the rate of successful vaginal delivery and reduce the incidence of premature births or infants with low birth weights (130, 136, 137). If cardiac function continues to deteriorate and the pulmonary vascular resistance increases after oral sildenafil treatment, inhaled iloprost may be considered to relieve symptoms (136, 137). In addition, a previous study indicated that five pregnant women with PAH who received PDE-5 inhibitors and prostacyclin intravenously did not show significant maternal and infant complications during long-term follow-up at the breastfeeding stage (84).
Although sildenafil is widely used, its safety during requires further study. In 2021, a study focusing on 77 infants born to women who were treated with PDE-5 inhibitors during pregnancy found that nine infants were premature, six had small statures for their gestational age, five scored < 8 in their 5-min appearance, pulse, grimace, activity and respiration tests, 18 were admitted to the neonatal intensive care unit and eight were diagnosed with respiratory and cardiovascular diseases (138). Furthermore, there is no clinical evidence to support the efficacy of vardenafil and tadalafil in pregnant women with PAH at present.
Statins
In addition to hypolipidemic effects, statins also have reported anti-inflammatory, anti-proliferative and apoptotic effects. A large number of clinical and experimental studies revealed that statins can reduce the pulmonary artery pressure and improve pulmonary vascular remodeling by promoting apoptosis, inhibiting cell proliferation, anti-inflammatory effects, inhibiting Rho kinase signaling and endothelin-1 release (139–142). Although statins also did not increase the rate of birth defects or the rate of fetal teratogenicity, the sample size was relatively small (78). Although statins are generally not recommended during pregnancy and lactation at present, they may be used for the long-term treatment of postpartum PAH after lactation (66, 79).
ECMO
ECMO is an advanced respiratory and circulatory support technology that has been proposed for patients with acute reversible respiratory failure (143). ECMO can maintain the oxygenation status of patients with PAH when cardiac function is decompensated (144, 145). Various case reports suggested that ECMO treatment in the majority of pregnant women with PAH conferred favorable pregnancy outcomes (146–148). However, it has also been reported that patients with PAH receiving ECMO did not survive beyond 3 months after delivery due to severe right heart failure (149). In addition, the continuous operation of ECMO requires systemic anticoagulation, where the continuous oozing of the surgical incision may lead to severe coagulation dysfunction (150, 151). Due to the small sample size reported thus far, further studies on larger sample sizes are warranted.
Operative therapy
PAH secondary to a known cardiopulmonary disease requires the aggressive treatment of primary disease, with procedures including biventricular pacing and cardiac operation (85). Cardiac surgery under cardiopulmonary bypass may be considered for patients who have responded to drug therapy but have opportunities for surgery. Surgery should be performed between 13 and 28 weeks of gestation. If the gestational week is >26 weeks, then cesarean section can be considered to terminate the pregnancy before performing the cardiopulmonary bypass operation. If the gestational week is >28 weeks, cardiac surgery can be considered after vaginal delivery. However, the risk of maternal and fetal mortality remains high during cardiopulmonary bypass operation. Cardiac surgery is recommended only when drug or other forms of interventional therapy fails and the pregnant individual is in mortal danger (1, 88, 152).
For patients with chronic thromboembolic PAH, pulmonary endarterectomy is a possible curative method, although not all patients are suitable for this form of surgical treatment. Chronic thromboembolic PAH may also require postpartum thrombectomy or lung transplantation (146). High-risk patients who decide to continue pregnancy should be promptly evaluated for lung transplantation (6).
Conclusions
PAH is considered to be an irreversible disease. Strict contraception or early termination of pregnancy is recommended for PAH of any severity. However, effective early management is important for improving the prognosis for pregnant women with PAH first discovered during pregnancy or strongly required to continue pregnancy. Strategies, such as anticoagulation therapy, PAH-specific therapy and operative therapy, should be considered. Since pregnancy with PAH is a rare condition, the majority of relevant studies are retrospective studies based on case reports and case series analysis, which have low levels of evidence-based medical evidence. Therefore, additional prospective multi-center studies should be conducted in the future to optimize the clinical management strategies for pregnant women with PAH.
Author contributions
XZ and ZH conducted the study conceptualization, writing, and review of the manuscript. Both authors contributed to the review and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
1. ^NHS Digital. National Audit of Pulmonary Hypertension 10th Annual Report, Great Britain, 2018-19. Available online at: https://digital.nhs.uk/data-and-information/publications/statistical/national-pulmonary-hypertension-audit/2019 (accessed October 19, 2022).
References
1. Regitz-Zagrosek V, Roos-Hesselink JW, Bauersachs J, Blomström-Lundqvist C, Cífková R, Bonis MD, et al. 2018 ESC guidelines for themanagement of cardiovascular diseases during pregnancy. Rev Esp Cardiol. (2019) 72:161. doi: 10.1016/j.rec.2018.12.003
2. Hoeper MM, Humbert M, Souza R, Idrees M, Kawut SM, Sliwa-Hahnle K, et al. A global view of pulmonary hypertension. Lancet Resp Med. (2016) 4:306–22. doi: 10.1016/s2213-2600(15)00543-3
3. Weiss BM, Zemp L, Seifert B, Hess OM. Outcome of pulmonary vascular disease in pregnancy: a systematic overview from 1978 through 1996. J Am Coll Cardiol. (1998) 31:1650–7. doi: 10.1016/s0735-1097(98)00162-4
4. Bédard E, Dimopoulos K, Gatzoulis MA. Has there been any progress made on pregnancy outcomes among women with pulmonary arterial hypertension? Eur Heart J. (2009) 30:256–65. doi: 10.1093/eurheartj/ehn597
5. Duarte AG, Thomas S, Safdar Z, Torres F, Pacheco LD, Feldman J, et al. Management of pulmonary arterial hypertension during pregnancy: a retrospective, multicenter experience. Chest. (2013) 143:1330–6. doi: 10.1378/chest.12-0528
6. Jaïs X, Olsson KM, Barbera JA, Blanco I, Torbicki A, Peacock A, et al. Pregnancy outcomes in pulmonary arterial hypertension in the modern management era. Eur Respir J. (2012) 40:881–5. doi: 10.1183/09031936.00141211
7. Kiely DG, Condliffe R, Webster V, Mills GH, Wrench I, Gandhi SV, et al. Improved survival in pregnancy and pulmonary hypertension using a multiprofessional approach. Bjog. (2010) 117:565–74. doi: 10.1111/j.1471-0528.2009.02492.x
8. Kamp JC, von Kaisenberg C, Greve S, Winter L, Park DH, Fuge J, et al. Pregnancy in pulmonary arterial hypertension: midterm outcomes of mothers and offspring. J Heart Lung Transplant. (2021) 40:229–33. doi: 10.1016/j.healun.2020.12.002
9. Humbert M, Kovacs G, Hoeper MM, Badagliacca R, Berger RMF, Brida M, et al. 2022 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Eur Heart J. (2022) 43:3618–731. doi: 10.1093/eurheartj/ehac237
10. D'Alto M, Di Maio M, Romeo E, Argiento P, Blasi E, Di Vilio A, et al. Echocardiographic probability of pulmonary hypertension: a validation study. Eur Respir J. (2022) 60:2102548. doi: 10.1183/13993003.02548-2021
11. Simonneau G, Montani D, Celermajer DS, Denton CP, Gatzoulis MA, Krowka M, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J. (2019) 53:1801913. doi: 10.1183/13993003.01913-2018
12. Corbach N, Berlier C, Lichtblau M, Schwarz EI, Gautschi F, Groth A, et al. Favorable pregnancy outcomes in women with well-controlled pulmonary arterial hypertension. Front Med. (2021) 8:689764. doi: 10.3389/fmed.2021.689764
13. Hemnes AR, Kiely DG, Cockrill BA, Safdar Z, Wilson VJ, Al Hazmi M, et al. Statement on pregnancy in pulmonary hypertension from the pulmonary vascular research institute. Pulm Circ. (2015) 5:435–65. doi: 10.1086/682230
14. Pieper PG, Lameijer H, Hoendermis ES. Pregnancy and pulmonary hypertension. Best Pract Res Clin Obstet Gynaecol. (2014) 28:579–91. doi: 10.1016/j.bpobgyn.2014.03.003
15. Olsson KM, Jais X. Birth control and pregnancy management in pulmonary hypertension. Semin Respir Crit Care Med. (2013) 34:681–8. doi: 10.1055/s-0033-1355438
16. Galiè N, Humbert M, Vachiery JL, Gibbs S, Lang I, Torbicki A, et al. 2015 ESC/ERS guidelines for the diagnosis and treatment of pulmonary hypertension. Rev Esp Cardiol. (2016) 69:177. doi: 10.1016/j.rec.2016.01.002
17. Famuyide AO, Hopkins MR, El-Nashar SA, Creedon DJ, Vasdev GM, Driscoll DJ, et al. Hysteroscopic sterilization in women with severe cardiac disease: experience at a tertiary center. Mayo Clin Proc. (2008) 83:431–8. doi: 10.4065/83.4.431
18. Običan SG, Cleary KL. Pulmonary arterial hypertension in pregnancy. Semin Perinatol. (2014) 38:289–94. doi: 10.1053/j.semperi.2014.04.018
19. van der Linde D, Konings EE, Slager MA, Witsenburg M, Helbing WA, Takkenberg JJ, et al. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol. (2011) 58:2241–7. doi: 10.1016/j.jacc.2011.08.025
20. Gill HK, Splitt M, Sharland GK, Simpson JM. Patterns of recurrence of congenital heart disease: an analysis of 6,640 consecutive pregnancies evaluated by detailed fetal echocardiography. J Am Coll Cardiol. (2003) 42:923–9. doi: 10.1016/s0735-1097(03)00853-2
21. Yucel E, DeFaria Yeh D. Pregnancy in women with congenital heart disease. Curr Treat Options Cardiovasc Med. (2017) 19:73. doi: 10.1007/s11936-017-0572-0
22. Morrell NW, Aldred MA, Chung WK, Elliott CG, Nichols WC, Soubrier F, et al. Genetics and genomics of pulmonary arterial hypertension. Eur Respir J. (2019) 53:1801899. doi: 10.1183/13993003.01899-2018
23. Martínez MV, Rutherford JD. Pulmonary hypertension in pregnancy. Cardiol Rev. (2013) 21:167–73. doi: 10.1097/CRD.0b013e318275cf01
24. Safdar Z. Pulmonary arterial hypertension in pregnant women. Ther Adv Respir Dis. (2013) 7:51–63. doi: 10.1177/1753465812461680
25. Kozer E, Nikfar S, Costei A, Boskovic R, Nulman I, Koren G. Aspirin consumption during the first trimester of pregnancy and congenital anomalies: a meta-analysis. Am J Obstet Gynecol. (2002) 187:1623–30. doi: 10.1067/mob.2002.127376
26. Werler MM, Sheehan JE, Mitchell AA. Maternal medication use and risks of gastroschisis and small intestinal atresia. Am J Epidemiol. (2002) 155:26–31. doi: 10.1093/aje/155.1.26
27. Perkin RM, Levin DL, Clark R. Serum salicylate levels and right-to-left ductus shunts in newborn infants with persistent pulmonary hypertension. J Pediatr. (1980) 96:721–6. doi: 10.1016/s0022-3476(80)80753-0
28. Alano MA, Ngougmna E, Ostrea Jr EM, Konduri GG. Analysis of nonsteroidal antiinflammatory drugs in meconium and its relation to persistent pulmonary hypertension of the newborn. Pediatrics. (2001) 107:519–23. doi: 10.1542/peds.107.3.519
29. James AH, Brancazio LR, Price T. Aspirin and reproductive outcomes. Obstet Gynecol Surv. (2008) 63:49–57. doi: 10.1097/OGX.0b013e31815e8731
30. Collins E. Maternal and fetal effects of acetaminophen and salicylates in pregnancy. Obstet Gynecol. (1981) 58:57s−62s.
31. CLASP collaborative group. Low dose aspirin in pregnancy and early childhood development: follow up of the collaborative low dose aspirin study in pregnancy. Br J Obstet Gynaecol. (1995) 102:861–8. doi: 10.1111/j.1471-0528.1995.tb10872.x
32. Kristensen DM, Hass U, Lesné L, Lottrup G, Jacobsen PR, Desdoits-Lethimonier C, et al. Intrauterine exposure to mild analgesics is a risk factor for development of male reproductive disorders in human and rat. Hum Reprod. (2011) 26:235–44. doi: 10.1093/humrep/deq323
33. Yurdakök M. Fetal and neonatal effects of anticoagulants used in pregnancy: a review. Turk J Pediatr. (2012) 54:207–15.
34. Winger EE, Reed JL, A. retrospective analysis of fondaparinux versus enoxaparin treatment in women with infertility or pregnancy loss. Am J Reprod Immunol. (2009) 62:253–60. doi: 10.1111/j.1600-0897.2009.00733.x
35. Calzolari E, Barisic I, Loane M, Morris J, Wellesley D, Dolk H, et al. Epidemiology of multiple congenital anomalies in Europe: a EUROCAT population-based registry study. Birth Defects Res A Clin Mol Teratol. (2014) 100:270–6. doi: 10.1002/bdra.23240
36. Büller HR, Davidson BL, Decousus H, Gallus A, Gent M, Piovella F, et al. Fondaparinux or enoxaparin for the initial treatment of symptomatic deep venous thrombosis: a randomized trial. Ann Intern Med. (2004) 140:867–73. doi: 10.7326/0003-4819-140-11-200406010-00007
37. De Carolis S, di Pasquo E, Rossi E, Del Sordo G, Buonomo A, Schiavino D, et al. Fondaparinux in pregnancy: could it be a safe option? A review of the literature. Thromb Res. (2015) 135:1049–51. doi: 10.1016/j.thromres.2015.04.001
38. Greer IA, Nelson-Piercy C. Low-molecular-weight heparins for thromboprophylaxis and treatment of venous thromboembolism in pregnancy: a systematic review of safety and efficacy. Blood. (2005) 106:401–7. doi: 10.1182/blood-2005-02-0626
39. Casele HL. The use of unfractionated heparin and low molecular weight heparins in pregnancy. Clin Obstet Gynecol. (2006) 49:895–905. doi: 10.1097/01.grf.0000211958.45874.63
40. Hassouna A, Allam H. Limited dose warfarin throughout pregnancy in patients with mechanical heart valve prosthesis: a meta-analysis. Interact Cardiovasc Thorac Surg. (2014) 18:797–806. doi: 10.1093/icvts/ivu009
41. Deruelle P, Coulon C. The use of low-molecular-weight heparins in pregnancy–how safe are they? Curr Opin Obstet Gynecol. (2007) 19:573–7. doi: 10.1097/GCO.0b013e3282f10e33
42. Dimitrakakis C, Papageorgiou P, Papageorgiou I, Antzaklis A, Sakarelou N, Michalas S. Absence of transplacental passage of the low molecular weight heparin enoxaparin. Haemostasis. (2000) 30:243–8. doi: 10.1159/000054140
43. Omri A, Delaloye JF, Andersen H, Bachmann F. Low molecular weight heparin Novo (LHN-1) does not cross the placenta during the second trimester of pregnancy. Thromb Haemost. (1989) 61:55–6.
44. Xu Z, Fan J, Luo X, Zhang WB, Ma J, Lin YB, et al. Anticoagulation regimens during pregnancy in patients with mechanical heart valves: a systematic review and meta-analysis. Can J Cardiol. (2016) 32:1248.e1–9. doi: 10.1016/j.cjca.2015.11.005
45. D'Souza R, Ostro J, Shah PS, Silversides CK, Malinowski A, Murphy KE, et al. Anticoagulation for pregnant women with mechanical heart valves: a systematic review and meta-analysis. Eur Heart J. (2017) 38:1509–16. doi: 10.1093/eurheartj/ehx032
46. Sillesen M, Hjortdal V, Vejlstrup N, Sørensen K. Pregnancy with prosthetic heart valves - 30 years' nationwide experience in Denmark. Eur J Cardiothorac Surg. (2011) 40:448–54. doi: 10.1016/j.ejcts.2010.12.011
47. van Driel D, Wesseling J, Sauer PJ, Touwen BC, van der Veer E, Heymans HS. Teratogen update: fetal effects after in utero exposure to coumarins overview of cases, follow-up findings, and pathogenesis. Teratology. (2002) 66:127–40. doi: 10.1002/tera.10054
48. Wesseling J, Van Driel D, Heymans HS, Rosendaal FR, Geven-Boere LM, Smrkovsky M, et al. Coumarins during pregnancy: long-term effects on growth and development of school-age children. Thromb Haemost. (2001) 85:609–13.
49. van Driel D, Wesseling J, Sauer PJ, van Der Veer E, Touwen BC, Smrkovsky M. In utero exposure to coumarins and cognition at 8 to 14 years old. Pediatrics. (2001) 107:123–9. doi: 10.1542/peds.107.1.123
50. Bildirici I, Shumway JB. Intravenous and inhaled epoprostenol for primary pulmonary hypertension during pregnancy and delivery. Obstet Gynecol. (2004) 103:1102–5. doi: 10.1097/01.Aog.0000121826.75294.39
51. Stewart R, Tuazon D, Olson G, Duarte AG. Pregnancy and primary pulmonary hypertension : successful outcome with epoprostenol therapy. Chest. (2001) 119:973–5. doi: 10.1378/chest.119.3.973
52. Timofeev J, Ruiz G, Fries M, Driggers RW. Intravenous epoprostenol for management of pulmonary arterial hypertension during pregnancy. AJP Rep. (2013) 3:71–4. doi: 10.1055/s-0033-1338169
53. Galiè N, Corris PA, Frost A, Girgis RE, Granton J, Jing ZC, et al. Updated treatment algorithm of pulmonary arterial hypertension. J Am Coll Cardiol. (2013) 62:D60–72. doi: 10.1016/j.jacc.2013.10.031
54. Gomberg-Maitland M, Olschewski H. Prostacyclin therapies for the treatment of pulmonary arterial hypertension. Eur Respir J. (2008) 31:891–901. doi: 10.1183/09031936.00097107
55. Elliot CA, Stewart P, Webster VJ, Mills GH, Hutchinson SP, Howarth ES, et al. The use of iloprost in early pregnancy in patients with pulmonary arterial hypertension. Eur Respir J. (2005) 26:168–73. doi: 10.1183/09031936.05.00128504
56. Opitz CF, Wensel R, Winkler J, Halank M, Bruch L, Kleber FX, et al. Clinical efficacy and survival with first-line inhaled iloprost therapy in patients with idiopathic pulmonary arterial hypertension. Eur Heart J. (2005) 26:1895–902. doi: 10.1093/eurheartj/ehi283
57. Hoeper MM, Gall H, Seyfarth HJ, Halank M, Ghofrani HA, Winkler J, et al. Long-term outcome with intravenous iloprost in pulmonary arterial hypertension. Eur Respir J. (2009) 34:132–7. doi: 10.1183/09031936.00130408
58. Rosengarten D, Kramer R. Pregnancy in a woman with pulmonary hypertension: favorable outcome with intravenous treprostinil. Clin Exp Obstet Gynecol. (2015) 42:390–1.
59. Nadler ST, Edelman JD. Inhaled treprostinil and pulmonary arterial hypertension. Vasc Health Risk Manag. (2010) 6:1115–24. doi: 10.2147/vhrm.S14777
60. Feldman J, Habib N, Fann J, Radosevich JJ. Treprostinil in the treatment of pulmonary arterial hypertension. Future Cardiol. (2020) 16:547–58. doi: 10.2217/fca-2020-0021
61. Skoro-Sajer N, Lang I, Naeije R. Treprostinil for pulmonary hypertension. Vasc Health Risk Manag. (2008) 4:507–13. doi: 10.2147/vhrm.s2477
62. Lindegaard Pedersen M, Krüger M, Grimm D, Infanger M, Wehland M. The prostacyclin analogue treprostinil in the treatment of pulmonary arterial hypertension. Basic Clin Pharmacol Toxicol. (2019) 126:32–42. doi: 10.1111/bcpt.13305
63. Benza RL, Seeger W, McLaughlin VV, Channick RN, Voswinckel R, Tapson VF, et al. Long-term effects of inhaled treprostinil in patients with pulmonary arterial hypertension: the treprostinil sodium inhalation used in the management of pulmonary arterial hypertension (TRIUMPH) study open-label extension. J Heart Lung Transplant. (2011) 30:1327–33. doi: 10.1016/j.healun.2011.08.019
64. Jing ZC, Parikh K, Pulido T, Jerjes-Sanchez C, White RJ, Allen R, et al. Efficacy and safety of oral treprostinil monotherapy for the treatment of pulmonary arterial hypertension: a randomized, controlled trial. Circulation. (2013) 127:624–33. doi: 10.1161/circulationaha.112.124388
65. Tapson VF, Torres F, Kermeen F, Keogh AM, Allen RP, Frantz RP, et al. Oral treprostinil for the treatment of pulmonary arterial hypertension in patients on background endothelin receptor antagonist and/or phosphodiesterase type 5 inhibitor therapy (the FREEDOM-C study): a randomized controlled trial. Chest. (2012) 142:1383–90. doi: 10.1378/chest.11-2212
66. Pieper PG. Use of medication for cardiovascular disease during pregnancy. Nat Rev Cardiol. (2015) 12:718–29. doi: 10.1038/nrcardio.2015.172
67. Sandoval J, Aguirre JS, Pulido T, Martinez-Guerra ML, Santos E, Alvarado P, et al. Nocturnal oxygen therapy in patients with the eisenmenger syndrome. Am J Respir Crit Care Med. (2001) 164:1682–7. doi: 10.1164/ajrccm.164.9.2106076
68. Packer M. Therapeutic application of calcium-channel antagonists for pulmonary hypertension. Am J Cardiol. (1985) 55:196b−201b. doi: 10.1016/0002-9149(85)90631-9
69. Krikler DM, Rowland E. Clinical value of calcium antagonists in treatment of cardiovascular disorders. J Am Coll Cardiol. (1983) 1:355–64. doi: 10.1016/s0735-1097(83)80035-7
70. Davis RL, Eastman D, McPhillips H, Raebel MA, Andrade SE, Smith D, et al. Risks of congenital malformations and perinatal events among infants exposed to calcium channel and beta-blockers during pregnancy. Pharmacoepidemiol Drug Saf. (2011) 20:138–45. doi: 10.1002/pds.2068
71. Taçoy G, Ekim NN, Cengel A. Dramatic response of a patient with pregnancy induced idiopathic pulmonary arterial hypertension to sildenafil treatment. J Obstet Gynaecol Res. (2010) 36:414–7. doi: 10.1111/j.1447-0756.2009.01136.x
72. Goland S, Tsai F, Habib M, Janmohamed M, Goodwin TM, Elkayam U. Favorable outcome of pregnancy with an elective use of epoprostenol and sildenafil in women with severe pulmonary hypertension. Cardiology. (2010) 115:205–8. doi: 10.1159/000287638
73. Ala M, Mohammad Jafari R, Dehpour AR. Sildenafil beyond erectile dysfunction and pulmonary arterial hypertension: thinking about new indications. Fundam Clin Pharmacol. (2021) 35:235–59. doi: 10.1111/fcp.12633
74. Wright PJ. Comparison of phosphodiesterase type 5 (PDE5) inhibitors. Int J Clin Pract. (2006) 60:967–75. doi: 10.1111/j.1742-1241.2006.01049.x
75. Bhatia S, Frantz RP, Severson CJ, Durst LA, McGoon MD. Immediate and long-term hemodynamic and clinical effects of sildenafil in patients with pulmonary arterial hypertension receiving vasodilator therapy. Mayo Clin Proc. (2003) 78:1207–13. doi: 10.4065/78.10.1207
76. Dhillon R. The management of neonatal pulmonary hypertension. Arch Dis Child Fetal Neonatal Ed. (2012) 97:F223–8. doi: 10.1136/adc.2009.180091
77. Cross DM, Horsley E, Derzi M, Owen K, Stavros FL. An evaluation of reproductive and developmental toxicity of sitaxentan (thelin) in rats. Birth Defects Res B Dev Reprod Toxicol. (2012) 95:327–36. doi: 10.1002/bdrb.21021
78. Winterfeld U, Allignol A, Panchaud A, Rothuizen LE, Merlob P, Cuppers-Maarschalkerweerd B, et al. Pregnancy outcome following maternal exposure to statins: a multicentre prospective study. Bjog. (2013) 120:463–71. doi: 10.1111/1471-0528.12066
79. Godfrey LM, Erramouspe J, Cleveland KW. Teratogenic risk of statins in pregnancy. Ann Pharmacother. (2012) 46:1419–24. doi: 10.1345/aph.1R202
80. Priori SG, Blomström-Lundqvist C, Mazzanti A, Blom N, Borggrefe M, Camm J, et al. 2015 ESC guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death. Rev Esp Cardiol. (2016) 69:176. doi: 10.1016/j.rec.2016.01.001
81. Ruiter G, Manders E, Happé CM, Schalij I, Groepenhoff H, Howard LS, et al. Intravenous iron therapy in patients with idiopathic pulmonary arterial hypertension and iron deficiency. Pulm Circ. (2015) 5:466–72. doi: 10.1086/682217
82. Kramer T, Wissmüller M, Natsina K, Gerhardt F, Ten Freyhaus H, Dumitrescu D, et al. Ferric carboxymaltose in patients with pulmonary arterial hypertension and iron deficiency: a long-term study. J Cachexia Sarcopenia Muscle. (2021) 12:1501–12. doi: 10.1002/jcsm.12764
83. Rudiene V, Kapleriene L, Jančauskaite D, Meškene E, Palevičiute E, Laukyte-Sleniene M, et al. Pregnancy in congenital heart disease, complicated by pulmonary arterial hypertension-a challenging issue for the pregnant woman, the foetus, and healthcare professionals. Medicina. (2022) 58:476. doi: 10.3390/medicina58040476
84. Yang JZ, Fernandes TM, Kim NH, Poch DS, Kerr KM, Lombardi S, et al. Pregnancy and pulmonary arterial hypertension: a case series and literature review. Am J Obstet Gynecol MFM. (2021) 3:100358. doi: 10.1016/j.ajogmf.2021.100358
85. Madden BP. Pulmonary hypertension and pregnancy. Int J Obstet Anesth. (2009) 18:156–64. doi: 10.1016/j.ijoa.2008.10.006
86. Adir Y, Humbert M, Chaouat A. Sleep-related breathing disorders and pulmonary hypertension. Eur Respir J. (2021) 57:2002258. doi: 10.1183/13993003.02258-2020
87. López-Candales A, Cleary H, Edelman K. Constrictive-like physiology in severe pulmonary hypertension: the effect of the Valsalva maneuver. South Med J. (2011) 104:282–4. doi: 10.1097/SMJ.0b013e31820bf5d2
88. Galiè N, Hoeper MM, Humbert M, Torbicki A, Vachiery JL, Barbera JA, et al. Guidelines for the diagnosis and treatment of pulmonary hypertension: the task force for the diagnosis and treatment of pulmonary hypertension of the European society of cardiology (ESC) and the European respiratory society (ERS), endorsed by the international society of heart and lung transplantation (ISHLT). Eur Heart J. (2009) 30:2493–537. doi: 10.1093/eurheartj/ehp297
89. Olsson KM, Channick R. Pregnancy in pulmonary arterial hypertension. Eur Respir Rev. (2016) 25:431–7. doi: 10.1183/16000617.0079-2016
90. Taylor J. The first ESC Guidelines on the management of cardiovascular diseases during pregnancy. Eur Heart J. (2011) 32:3055–6. doi: 10.1093/eurheartj/ehr235
91. Tongers J, Schwerdtfeger B, Klein G, Kempf T, Schaefer A, Knapp JM, et al. Incidence and clinical relevance of supraventricular tachyarrhythmias in pulmonary hypertension. Am Heart J. (2007) 153:127–32. doi: 10.1016/j.ahj.2006.09.008
92. Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Europace. (2016) 18:1609–78. doi: 10.1093/europace/euw295
93. Kockova R, Kocka V, Kiernan T, Fahy GJ. Ibutilide-induced cardioversion of atrial fibrillation during pregnancy. J Cardiovasc Electrophysiol. (2007) 18:545–7. doi: 10.1111/j.1540-8167.2006.00752.x
94. Katritsis DG, Boriani G, Cosio FG, Hindricks G, Jaïs P, Josephson ME, et al. European heart rhythm association (EHRA) consensus document on the management of supraventricular arrhythmias, endorsed by heart rhythm society (HRS), Asia-pacific heart rhythm society (APHRS), and sociedad latinoamericana de estimulación cardiaca y electrofisiologia (SOLAECE). Europace. (2017) 19:465–511. doi: 10.1093/europace/euw301
95. Driver K, Chisholm CA, Darby AE, Malhotra R, Dimarco JP, Ferguson JD. Catheter ablation of arrhythmia during pregnancy. J Cardiovasc Electrophysiol. (2015) 26:698–702. doi: 10.1111/jce.12675
96. Chen G, Sun G, Xu R, Chen X, Yang L, Bai Y, et al. Zero-fluoroscopy catheter ablation of severe drug-resistant arrhythmia guided by Ensite NavX system during pregnancy: two case reports and literature review. Medicine. (2016) 95:e4487. doi: 10.1097/md.0000000000004487
97. Hidaka N, Chiba Y, Fukushima K, Wake N. Pregnant women with complete atrioventricular block: perinatal risks and review of management. Pacing Clin Electrophysiol. (2011) 34:1161–76. doi: 10.1111/j.1540-8159.2011.03177.x
98. Suri V, Keepanasseril A, Aggarwal N, Vijayvergiya R, Chopra S, Rohilla M. Maternal complete heart block in pregnancy: analysis of four cases and review of management. J Obstet Gynaecol Res. (2009) 35:434–7. doi: 10.1111/j.1447-0756.2008.00961.x
99. Natale A, Davidson T, Geiger MJ, Newby K. Implantable cardioverter-defibrillators and pregnancy: a safe combination? Circulation. (1997) 96:2808–12. doi: 10.1161/01.cir.96.9.2808
100. Ladouceur M, Benoit L, Radojevic J, Basquin A, Dauphin C, Hascoet S, et al. Pregnancy outcomes in patients with pulmonary arterial hypertension associated with congenital heart disease. Heart. (2017) 103:287–92. doi: 10.1136/heartjnl-2016-310003
101. Bates SM, Greer IA, Pabinger I, Sofaer S, Hirsh J. Venous thromboembolism, thrombophilia, antithrombotic therapy, and pregnancy: American college of chest physicians evidence-based clinical practice guidelines (8th Edition). Chest. (2008) 133:844s−86s. doi: 10.1378/chest.08-0761
102. A RS, Barreira R, Santos E. Low-dose warfarin maternal anticoagulation and fetal warfarin syndrome. BMJ Case Rep. (2018) 2018:223159. doi: 10.1136/bcr-2017-223159
103. Elkayam U, Goland S, Pieper PG, Silverside CK. High-risk cardiac disease in pregnancy: Part I. J Am Coll Cardiol. (2016) 68:396–410. doi: 10.1016/j.jacc.2016.05.048
104. Elkayam U, Goland S, Pieper PG, Silversides CK. High-risk cardiac disease in pregnancy: Part II. J Am Coll Cardiol. (2016) 68:502–16. doi: 10.1016/j.jacc.2016.05.050
105. van Hagen IM, Roos-Hesselink JW, Ruys TP, Merz WM, Goland S, Gabriel H, et al. Pregnancy in women with a mechanical heart valve: data of the European society of cardiology registry of pregnancy and cardiac disease (ROPAC). Circulation. (2015) 132:132–42. doi: 10.1161/circulationaha.115.015242
106. McLintock C. Thromboembolism in pregnancy: challenges and controversies in the prevention of pregnancy-associated venous thromboembolism and management of anticoagulation in women with mechanical prosthetic heart valves. Best Pract Res Clin Obstet Gynaecol. (2014) 28:519–36. doi: 10.1016/j.bpobgyn.2014.03.001
107. Khoo CW, Tay KH, Shantsila E, Lip GY. Novel oral anticoagulants. Int J Clin Pract. (2009) 63:630–41. doi: 10.1111/j.1742-1241.2009.02011.x
108. Hoeltzenbein M, Beck E, Meixner K, Schaefer C, Kreutz R. Pregnancy outcome after exposure to the novel oral anticoagulant rivaroxaban in women at suspected risk for thromboembolic events: a case series from the German embryotox pharmacovigilance centre. Clin Res Cardiol. (2016) 105:117–26. doi: 10.1007/s00392-015-0893-5
109. Areia AL, Mota-Pinto A. Experience with direct oral anticoagulants in pregnancy - a systematic review. J Perinat Med. (2022) 50:457–61. doi: 10.1515/jpm-2021-0457
110. Lameijer H, Aalberts JJJ, van Veldhuisen DJ, Meijer K, Pieper PG. Efficacy and safety of direct oral anticoagulants during pregnancy; a systematic literature review. Thromb Res. (2018) 169:123–7. doi: 10.1016/j.thromres.2018.07.022
111. Bassily-Marcus AM, Yuan C, Oropello J, Manasia A, Kohli-Seth R, Benjamin E. Pulmonary hypertension in pregnancy: critical care management. Pulm Med. (2012) 2012:709407. doi: 10.1155/2012/709407
112. Bian C, Wei Q, Liu X. Influence of heart-valve replacement of warfarin anticoagulant therapy on perinatal outcomes. Arch Gynecol Obstet. (2012) 285:347–51. doi: 10.1007/s00404-011-1962-2
113. Bates SM, Greer IA, Middeldorp S, Veenstra DL, Prabulos AM, Vandvik PO, et al. Thrombophilia, antithrombotic therapy, and pregnancy: antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. (2012) 141:e691S−736S. doi: 10.1378/chest.11-2300
114. Daimon A, Kamiya CA, Iwanaga N, Ikeda T, Nakanishi N, Yoshimatsu J. Management of pulmonary vasodilator therapy in three pregnancies with pulmonary arterial hypertension. J Obstet Gynaecol Res. (2017) 43:935–8. doi: 10.1111/jog.13279
115. Bonnin M, Mercier FJ, Sitbon O, Roger-Christoph S, Jaïs X, Humbert M, et al. Severe pulmonary hypertension during pregnancy: mode of delivery and anesthetic management of 15 consecutive cases. Anesthesiology. (2005) 102:1133–7; discussion 5A−6A. doi: 10.1097/00000542-200506000-00012
116. Avdalovic M, Sandrock C, Hoso A, Allen R, Albertson TE. Epoprostenol in pregnant patients with secondary pulmonary hypertension: two case reports and a review of the literature. Treat Respir Med. (2004) 3:29–34. doi: 10.2165/00151829-200403010-00004
117. Lacassie HJ, Germain AM, Valdés G, Fernández MS, Allamand F, López H. Management of eisenmenger syndrome in pregnancy with sildenafil and L-arginine. Obstet Gynecol. (2004) 103:1118–20. doi: 10.1097/01.Aog.0000125148.82698.65
118. de Raaf MA, Beekhuijzen M, Guignabert C, Vonk Noordegraaf A, Bogaard HJ. Endothelin-1 receptor antagonists in fetal development and pulmonary arterial hypertension. Rep Toxicol. (2015) 56:45–51. doi: 10.1016/j.reprotox.2015.06.048
119. Xing J, Cao Y, Yu Y, Li H, Song Z, Yu H. In Vitro micropatterned human pluripotent stem cell test (μP-hPST) for morphometric-based teratogen screening. Sci Rep. (2017) 7:8491. doi: 10.1038/s41598-017-09178-1
120. Barst RJ, Rubin LJ, Long WA, McGoon MD, Rich S, Badesch DB, et al. A comparison of continuous intravenous epoprostenol (prostacyclin) with conventional therapy for primary pulmonary hypertension. N Engl J Med. (1996) 334:296–301. doi: 10.1056/nejm199602013340504
121. McLaughlin VV, Archer SL, Badesch DB, Barst RJ, Farber HW, Lindner JR, et al. ACCF/AHA 2009 expert consensus document on pulmonary hypertension a report of the American college of cardiology foundation task force on expert consensus documents and the american heart association developed in collaboration with the American college of chest physicians; American thoracic society. Inc; and the pulmonary hypertension association. J Am Coll Cardiol. (2009) 53:1573–619. doi: 10.1016/j.jacc.2009.01.004
122. Brittain EL, Pugh ME, Wheeler LA, Robbins IM, Loyd JE, Newman JH, et al. Prostanoids but not oral therapies improve right ventricular function in pulmonary arterial hypertension. JACC Heart Fail. (2013) 1:300–7. doi: 10.1016/j.jchf.2013.05.004
123. Waxman AB, Zamanian RT. Pulmonary arterial hypertension: new insights into the optimal role of current and emerging prostacyclin therapies. Am J Cardiol. (2013) 111:1A−16A; quiz 7A−9A. doi: 10.1016/j.amjcard.2012.12.002
124. Banerjee D, Ventetuolo CE. Pulmonary hypertension in pregnancy. Semin Respir Crit Care Med. (2017) 38:148–59. doi: 10.1055/s-0037-1602242
125. McLaughlin VV, Shillington A, Rich S. Survival in primary pulmonary hypertension: the impact of epoprostenol therapy. Circulation. (2002) 106:1477–82. doi: 10.1161/01.cir.0000029100.82385.58
126. Garabedian MJ, Hansen WF, Gianferrari EA, Lain KY, Fragneto RY, Campbell CL, et al. Epoprostenol treatment for idiopathic pulmonary arterial hypertension in pregnancy. J Perinatol. (2010) 30:628–31. doi: 10.1038/jp.2010.15
127. Sahni S, Palkar AV, Rochelson BL, Kepa W, Talwar A. Pregnancy and pulmonary arterial hypertension: a clinical conundrum. Preg Hypertens. (2015) 5:157–64. doi: 10.1016/j.preghy.2015.01.004
128. Goya M, Meseguer ML, Merced C, Suy A, Monforte V, Domingo E, et al. Successful pregnancy in a patient with pulmonary hypertension associated with mixed collagen vascular disease. J Obstet Gynaecol. (2014) 34:191. doi: 10.3109/01443615.2012.706663
129. Zhang J, Lu J, Zhou X, Xu X, Ye Q, Ou Q, et al. Perioperative management of pregnant women with idiopathic pulmonary arterial hypertension: an observational case series study from China. J Cardiothorac Vasc Anesth. (2018) 32:2547–59. doi: 10.1053/j.jvca.2018.01.043
130. Zhang ZN, Jiang X, Zhang R, Li XL, Wu BX, Zhao QH, et al. Oral sildenafil treatment for eisenmenger syndrome: a prospective, open-label, multicentre study. Heart. (2011) 97:1876–81. doi: 10.1136/heartjnl-2011-300344
131. Martin SR, Edwards A. Pulmonary hypertension and pregnancy. Obstet Gynecol. (2019) 134:974–87. doi: 10.1097/aog.0000000000003549
132. Kumar P, Thudium E, Laliberte K, Zaccardelli D, Nelsen A. A comprehensive review of treprostinil pharmacokinetics via four routes of administration. Clin Pharmacokinet. (2016) 55:1495–505. doi: 10.1007/s40262-016-0409-0
133. Simonneau G, Barst RJ, Galie N, Naeije R, Rich S, Bourge RC, et al. Continuous subcutaneous infusion of treprostinil, a prostacyclin analogue, in patients with pulmonary arterial hypertension: a double-blind, randomized, placebo-controlled trial. Am J Respir Crit Care Med. (2002) 165:800–4. doi: 10.1164/ajrccm.165.6.2106079
134. Curry RA, Fletcher C, Gelson E, Gatzoulis MA, Woolnough M, Richards N, et al. Pulmonary hypertension and pregnancy–a review of 12 pregnancies in nine women. Bjog. (2012) 119:752–61. doi: 10.1111/j.1471-0528.2012.03295.x
135. Galiè N, Ghofrani HA, Torbicki A, Barst RJ, Rubin LJ, Badesch D, et al. Sildenafil citrate therapy for pulmonary arterial hypertension. N Engl J Med. (2005) 353:2148–57. doi: 10.1056/NEJMoa050010
136. Wang RC, Jiang FM, Zheng QL Li CT, Peng XY, He CY, et al. Efficacy and safety of sildenafil treatment in pulmonary arterial hypertension: a systematic review. Respir Med. (2014) 108:531–7. doi: 10.1016/j.rmed.2014.01.003
137. Zhuang XD, Long M, Li F, Hu X, Liao XX, Du ZM. PDE5 inhibitor sildenafil in the treatment of heart failure: a meta-analysis of randomized controlled trials. Int J Cardiol. (2014) 172:581–7. doi: 10.1016/j.ijcard.2014.01.102
138. Cesta CE, Segovia Chacón S, Engeland A, Broe A, Damkier P, Furu K, et al. Use of sildenafil and other phosphodiesterase type 5 inhibitors among pregnant women in Scandinavia. Acta Obstet Gynecol Scand. (2021) 100:2111–8. doi: 10.1111/aogs.14251
139. Yao J, Xiong M, Tang B, Chen G, Liang M, Ma X, et al. Simvastatin attenuates pulmonary vascular remodelling by down-regulating matrix metalloproteinase-1 and−9 expression in a carotid artery-jugular vein shunt pulmonary hypertension model in rats. Eur J Cardiothorac Surg. (2012) 42:e121–7. doi: 10.1093/ejcts/ezs445
140. Chen D, Zhou D, Qian J, Chen F, Guan L, Dong L, et al. Atorvastatin prevents dehydromonocrotaline-induced pulmonary hypertension in beagles. Exp Lung Res. (2012) 38:333–43. doi: 10.3109/01902148.2012.702852
141. Wilkins MR, Ali O, Bradlow W, Wharton J, Taegtmeyer A, Rhodes CJ, et al. Simvastatin as a treatment for pulmonary hypertension trial. Am J Respir Crit Care Med. (2010) 181:1106–13. doi: 10.1164/rccm.2009111-699oc
142. Ali OF, Growcott EJ, Butrous GS, Wharton J. Pleiotropic effects of statins in distal human pulmonary artery smooth muscle cells. Respir Res. (2011) 12:137. doi: 10.1186/1465-9921-12-137
143. Cunningham JA, Devine PC, Jelic S. Extracorporeal membrane oxygenation in pregnancy. Obstet Gynecol. (2006) 108:792–5. doi: 10.1097/01.AOG.0000209184.33709.ec
144. Meng ML, Landau R, Viktorsdottir O, Banayan J, Grant T, Bateman B, et al. Pulmonary hypertension in pregnancy: a report of 49 cases at four tertiary north American sites. Obstet Gynecol. (2017) 129:511–20. doi: 10.1097/aog.0000000000001896
145. Abid Memon H, Safdar Z, Goodarzi A. Use of extracorporeal membrane oxygenation in postpartum management of a patient with pulmonary arterial hypertension. Case Rep Pulmonol. (2018) 2018:7031731. doi: 10.1155/2018/7031731
146. Ye J, Chen JY, Xu N, Wu B, Wang ZP, Xu HY, et al. Bilateral lung transplantation after caesarean section in pregnancy with severe pulmonary arterial hypertension: a case report. Medicine. (2019) 98:e18109. doi: 10.1097/md.0000000000018109
147. Hara R, Hara S, Ong CS, Schwartz G, Sciortino C, Hibino N. Cesarean section in the setting of severe pulmonary hypertension requiring extracorporeal life support. Gen Thorac Cardiovasc Surg. (2017) 65:532–4. doi: 10.1007/s11748-016-0729-x
148. Weinberg L, Kay C, Liskaser F, Jones D, Tay S, Jaffe S, et al. Successful treatment of peripartum massive pulmonary embolism with extracorporeal membrane oxygenation and catheter-directed pulmonary thrombolytic therapy. Anaesth Intensive Care. (2011) 39:486–91. doi: 10.1177/0310057x1103900323
149. Roldan T, Villamañán E, Rios JJ, Waxman AB. Assessment of the quality of anticoagulation management in patients with pulmonary arterial hypertension. Thromb Res. (2017) 160:83–90. doi: 10.1016/j.thromres.2017.10.024
150. Reyftmann L, Morau E, Dechaud H, Frapier JM, Hedon B. Extracorporeal membrane oxygenation therapy for circulatory arrest due to postpartum hemorrhage. Obstet Gynecol. (2006) 107:511–4. doi: 10.1097/01.Aog.0000173970.67736.92
151. Robertson LC, Allen SH, Konamme SP, Chestnut J, Wilson P. The successful use of extra-corporeal membrane oxygenation in the management of a pregnant woman with severe H1N1 2009 influenza complicated by pneumonitis and adult respiratory distress syndrome. Int J Obstet Anesth. (2010) 19:443–7. doi: 10.1016/j.ijoa.2010.04.010
Keywords: pregnancy, pulmonary arterial hypertension, management, therapy, preconception management
Citation: Zhang X and Huangfu Z (2022) Management of pregnant patients with pulmonary arterial hypertension. Front. Cardiovasc. Med. 9:1029057. doi: 10.3389/fcvm.2022.1029057
Received: 26 August 2022; Accepted: 27 October 2022;
Published: 10 November 2022.
Edited by:
Yuling Zhang, Sun Yat-sen Memorial Hospital, ChinaReviewed by:
Nilda Espinola-Zavaleta, Instituto Nacional de Cardiologia Ignacio Chavez, MexicoMai Jingting, Sun Yat-sen University, China
Copyright © 2022 Zhang and Huangfu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhao Huangfu, MTM0MDM0NTAzOTcmI3gwMDA0MDsxNjMuY29t