
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 08 November 2022
Sec. Cardiovascular Surgery
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.1026445
This article is part of the Research Topic Emerging Opportunities in Congenital Cardiac Surgery View all 11 articles
 Paul Philipp Heinisch1,2†
Paul Philipp Heinisch1,2† Paul Metz1,2†
Paul Metz1,2† Helena Staehler1,2
Helena Staehler1,2 Benedikt Mayr3Janez Vodiskar1,2Martina Strbad1,2Bettina Ruf4
Benedikt Mayr3Janez Vodiskar1,2Martina Strbad1,2Bettina Ruf4 Peter Ewert4Alfred Hager4Jürgen Hörer1,2Masamichi Ono1,2*
Peter Ewert4Alfred Hager4Jürgen Hörer1,2Masamichi Ono1,2*Background: This study investigated the volume and duration of pleural and mediastinal effusions following extracardiac total cavopulmonary connection, as well as preoperative risk factors and their impact on outcome.
Materials and methods: A total of 210 patients who underwent extracardiac total cavopulmonary connection at our center between 2012 and 2020 were included in this study. Postoperative daily amount of pleural and mediastinal drainage were collected and factors influencing duration and amount of effusions were analyzed. The impact of effusions on adverse events was analyzed.
Results: Median age at extracardiac total cavopulmonary connection was 2.2 (interquartile range, 1.8–2.7) years with median weight of 11.6 (10.7–13.0) kg. Overall duration of drainage after extracardiac total cavopulmonary connection was 9 (6–17) days. The total volume of mediastinal, right pleural, and left pleural drainage was 18.8 (11.9–36.7), 64.4 (27.4–125.9), and 13.6 (0.0–53.5) mL/kg, respectively. Hypoplastic left heart syndrome (p = 0.004) and end-diastolic pressure (p = 0.044) were associated with high volume of drainages, and hypoplastic left heart syndrome (p = 0.007), presence of aortopulmonary collaterals (p = 0.002), and high end-diastolic pressure (p = 0.023) were associated with long duration of drainages. Dextrocardia was associated with higher volume (p < 0.001) and longer duration (p = 0.006) of left pleural drainage. Duration of drainage was associated with adverse events following extracardiac total cavopulmonary connection (p = 0.015).
Conclusion: Volume and duration of pleural and mediastinal effusions following extracardiac total cavopulmonary connection were related with hypoplastic left heart syndrome, aortopulmonary collaterals, and end-diastolic pressure. The duration of drainage for effusions was a risk factor for adverse events after total cavopulmonary connection.
As patient selection, surgical procedures, and postoperative management have been refined over time, today’s early staged Fontan surgery for patients with univentricular heart is linked to excellent early survival (1–4). Nevertheless, in the absence of a sub-pulmonary ventricle, redirection of the inferior vena cava to the pulmonary circulation inevitably exposes the systemic venous and lymphatic system to significantly higher pressure, which is associated with the majority of the acute and late postoperative complications following the Fontan procedure (5–8). The increase in hydrostatic capillary pressure, which results in excessive filtration in the interstitial space and overwhelming outflow into the lymphatic system, is one of the postulated mechanisms of pleural effusion and chylothorax in Fontan physiology (9).
Our institution has been performing an extracardiac conduit total cavopulmonary connection (EC-TCPC) as the standard procedure (10, 11). Various short-term morbidities may occur following EC-TCPC, including prolonged pleural effusion, arrhythmias, and acute kidney injury, all of which are associated with adverse in-hospital and long-term outcomes (11–14).
In general, studies have consistently found that pleural effusions are associated with morbidity and prolonged hospitalization in EC-TCPC patients (15, 16). Kim et al. were unable to replicate these findings, and prolonged pleural effusions had no effect on late adverse events (17). All possible causes of pleural effusions have been accounted for. A 2019 study conducted at a single center found that prolonged mechanical ventilation can lengthen the time spent in the intensive care unit and the entire hospital stay. A shorter duration of ventilation was also associated with a decreased risk of pleural effusion (18). However, the incidence of postoperative pleural effusions continues to be high and is a significant determinant of postoperative hospital length of stay.
In an effort to close the current knowledge gap, we sought to identify risk factors for pleural effusion and evaluate the effects of pleural and mediastinal effusions following EC-TCPC.
The Institutional Review Board of the Technical University of Munich approved the study (approved number of 305/20 S-KH on 2nd June, 2020). Due to the retrospective nature of the study, the need for individual patient consent was waived.
The retrospective review of medical records including in-hospital and out-patient notes, laboratory data, cardiac catheterization and other non-invasive images was performed for patients who underwent EC-TCPC at the German Heart Center Munich between 2012 and 2020. Patients who underwent TCPC conversion from classic Fontan procedure were excluded. The preoperative variables were measured at the closest time before surgery and postoperative variables were the first measurements when admitted to the ICU. Postoperative daily amounts of right pleural, left pleural and mediastinal effusions from the ICU charts were collected.
Following EC-TCPC surgery, all patients were admitted to the intensive care unit (ICU). Extubation was performed several hours after ICU submission. If the drainage of pleural effusion was less than 2 mL/kg/day/tube, the chest/mediastinal tube was removed. The diagnosis of chylothorax was established by fluid analysis through puncture, including the presence of chylomicrons, triglyceride content of ≥110 mg/dl, or a total cell count of 1,000 cells/mm3 and lymphocyte fraction ≥80%.
Extracardiac conduit total cavopulmonary connection was performed through a median sternotomy on cardiopulmonary bypass with aortic and bicaval cannulation (10, 11). Connection between inferior vena cava and pulmonary artery was performed using a non-ringed Gore-Tex tube graft. A graft diameter of 18 mm was most frequently used. Aortic cross-clamping with subsequent cardioplegic arrest of the heart was done only in patients who received a concomitant intra-cardiac procedure. Fenestration was only created in patients with a high preoperative risk of a poor outcome after TCPC: elevated mean pulmonary artery pressure (>15 mm Hg), elevated pulmonary vascular resistance (>2 mm Hg/L per min/m2), pulmonary artery distortion, and elevated ventricular filling pressure (12 mm Hg).
The patients underwent outpatient follow-up with pediatric cardiologists, and follow-up periods were defined as the time between the EC-TCPC and the time of the final appointment for each individual patient in the study. Adverse events were defined as death, heart transplantation, TCPC take down, symptomatic protein-losing enteropathy, symptomatic plastic bronchitis, thromboembolic events, sustained episode of supraventricular tachycardia, and requirement of permanent pacemaker implantation after EC-TCPC.
Categorical variables are presented as absolute numbers and percentages. Continuous variables are expressed as medians with interquartile ranges (IQR). Associated factors for excessive volume of drainage after EC-TCPC were identified using a logistic regression analysis. A cut-off value of 75 IQR was used in this analysis. Odds ratio (OR) with 95% confidence interval (CI) were estimated. Cox proportional hazard models was used to identify the variables that are associated with the duration of drainages. Hazard ratio (HR) with 95% CI were estimated. Impact of the duration as well as the amount of effusions on late adverse events after EC-TCPC were analyzed through Cox regression model. Risk factor analysis was tested by a univariable regression model and later as a multivariable model. For the multivariate model, those variables with a P-value < 0.1 in the univariable analysis were entered into the multivatiable model, with no subsequent removal of variables. Both forward inclusion and backward elimination process was used to generate the final multivariate model. It was confirmed that the risk factors resulting from forward inclusion and backward elimination was identical. P-values < 0.05 were considered significant. Data analysis and graphing were performed with the Statistical Package for the Social Sciences (SPSS) version 28.0 for Windows (IBM, Ehningen, Germany).
A total of 210 Patients were identified who underwent EC-TCPC at our center during the study period. Patient’s characteristics are shown in Table 1. The median follow-up following EC-TCPC was 1.7 (IQR = 0.2–3.8, maximum 8.6) years. Median age at EC-TCPC was 2.2 [Interquartile range (IQR) = 1.8–2.7] years with a body weight of 11.6 (IQR = 10.7–13.0) kg. Most frequent diagnosis was hypoplastic left heart syndrome (n = 79, 38%) and dominant right ventricle (RV) was observed in 127 (61%) patients. Dextrocardia was present in 19 patients (9%), and heterotaxy syndrome in 17 (8%). All patients had previous BCPS at the median age of 0.3 (IQR = 0.3–0.5) years and median interval between BCPS and EC-TCPC was 1.8 (IQR = 1.4–2.2) years. Pre-TCPC catheter data is shown in Supplementary Table 1. Operative and perioperative data are depicted in Table 2. An 18 mm extra-cardiac conduit was used in 194 patients (92%).
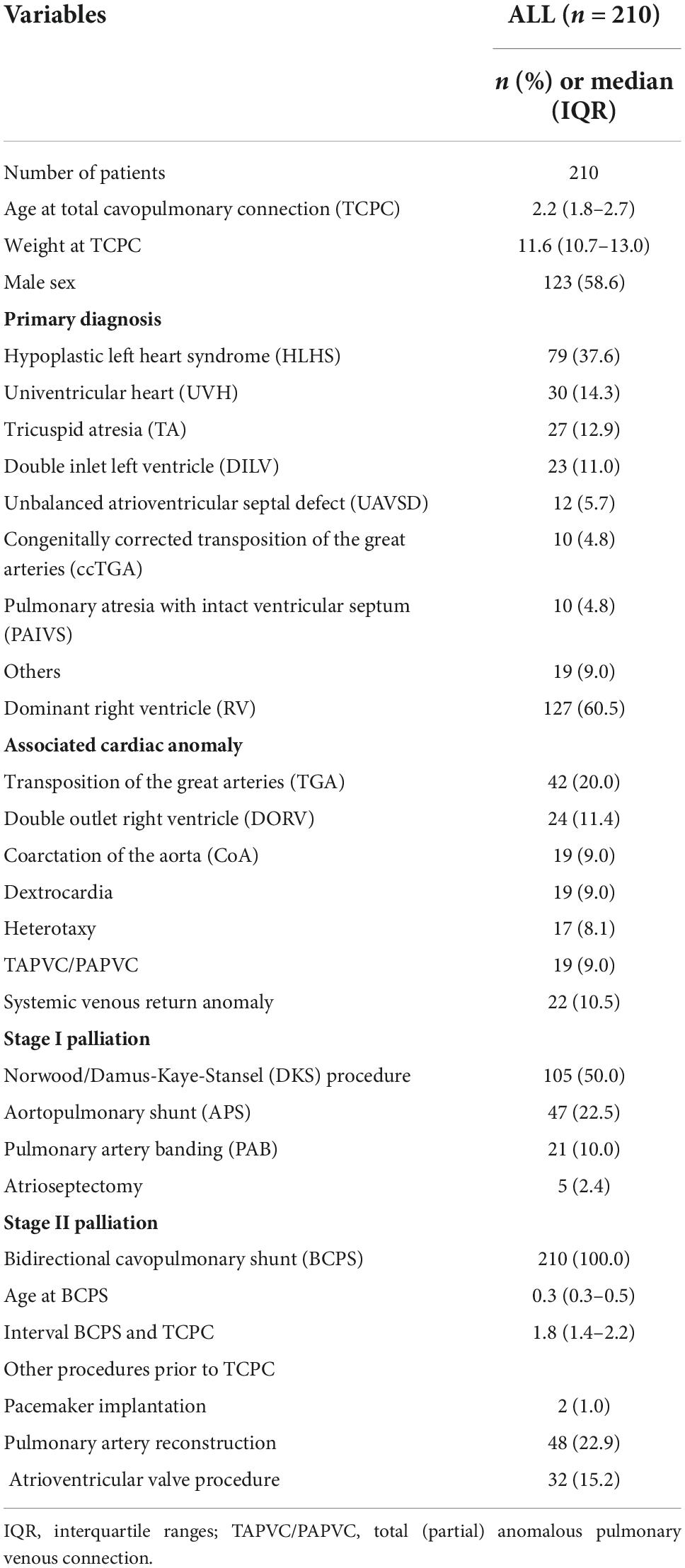
Table 1. Patient characteristics.
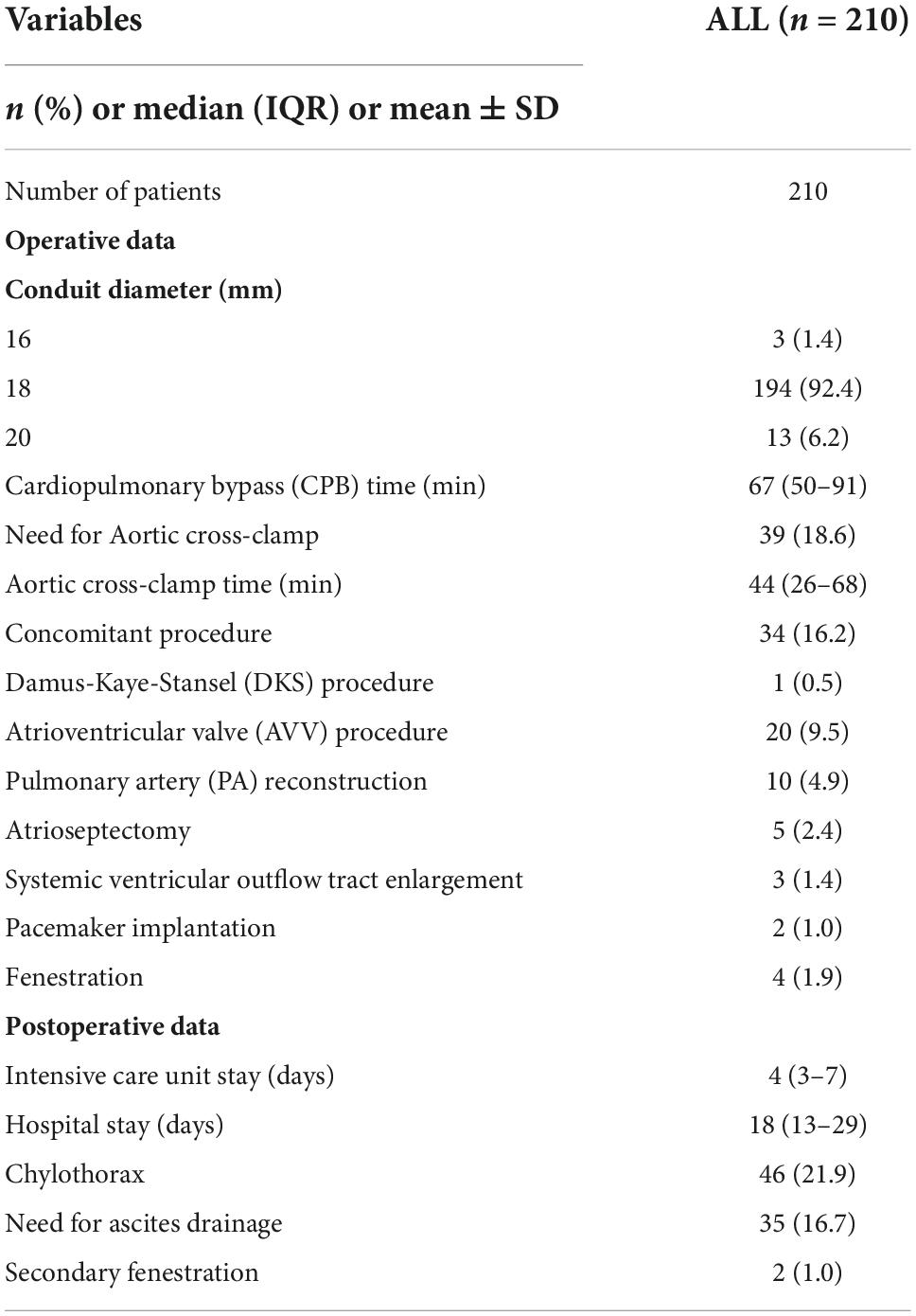
Table 2. Perioperative variables.
Median total volume of mediastinal, right pleural, and left pleural drainage after EC-TCPC was 18.8 (IQR, 11.9–36.7), 64.4 (IQR, 27.4–125.9), and 13.6 (0.0–53.5) mL/kg, respectively (Figure 1). Median total volume from any drainage per patient was 120.3 (IQR = 61.0–202.7) mL/kg. Histogram of total volume from any drainage per weight is shown in Supplementary Figure 1.
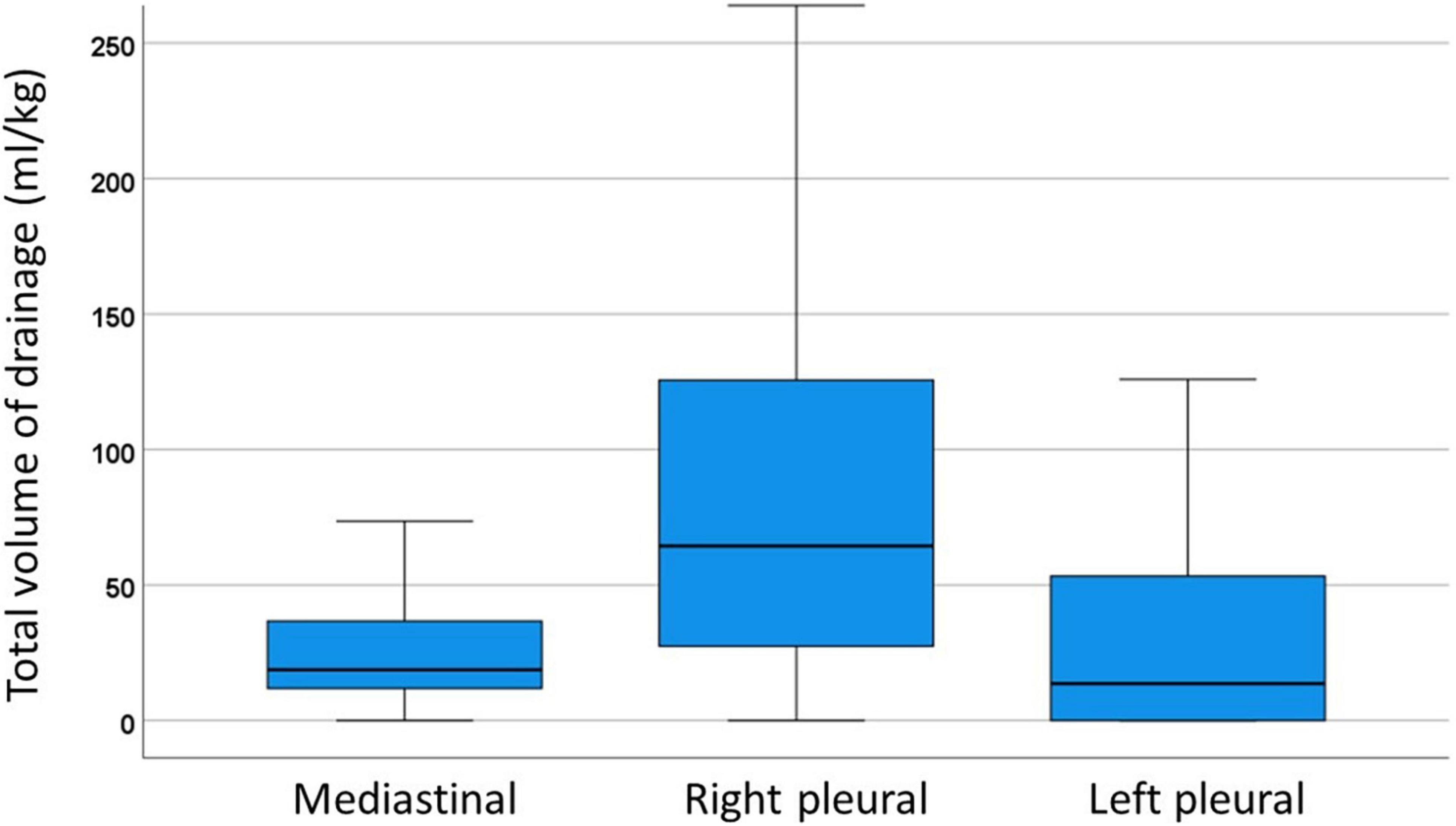
Figure 1. Box-and-whiskers dot plots showing total volume of drainage in right pleural, left pleural and mediastinal drainage. The upper and lower whiskers mark the minimum and maximum values, the upper and lower borders of the box represent the upper and lower quartiles, and the middle horizontal line represents the median.
Overall duration of any drainage was 9 (IQR 6–17) days, and the last drainage needed was right pleural drainage in 136 (64.8%), left pleural drainage in 33 (15.7%) patients, and both right and left pleural drainage in 41 (19.5%). Distribution of the duration of the drainage was shown in Figure 2. Median duration of right pleural and left pleural drainage after EC-TCPC was 7 (IQR = 4–13) days, and 6 (IQR = 1–6) days, respectively. Distribution of the duration of right pleural drainage and left pleural drainage is graphically shown in Supplementary Figure 2.
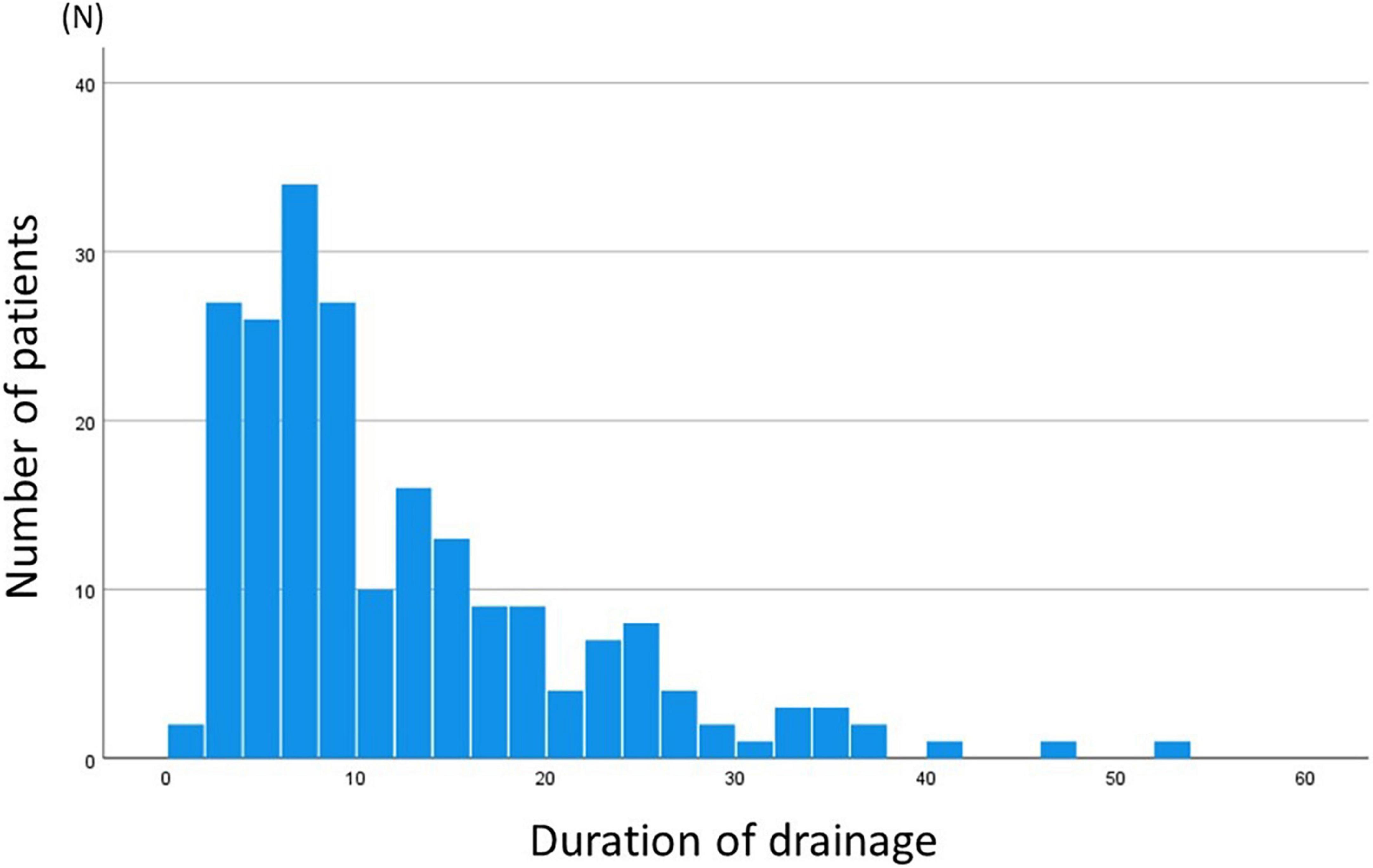
Figure 2. Histogram of duration of drainage. Median duration of drainage was at 9 (IQR = 5–17, minimum 1 and maximum 52) days.
As for the total volume of mediastinal and pleural drainage, HLHS (OR = 2.097, p = 0.022), presence of APCs (OR = 3.115, p = 0.008), PAP (OR = 1.199, p = 0.013), SVEDP (OR = 1.199, p = 0.011), and systolic arterial pressure (OR = 1.027, p = 0.037) were associated with volume from drainage with univariable analysis (Table 3). Multivariable analysis demonstrated HLHS (OR = 3.898, p = 0.004) and SVEDP (OR = 1.205, p = 0.044) were independent factors associated with high volume of drainages. Winter respiratory viral season of November through March was not identified as a factor influencing volume of mediastinal and pleural effusions (OR = 0.928, p = 0.822).
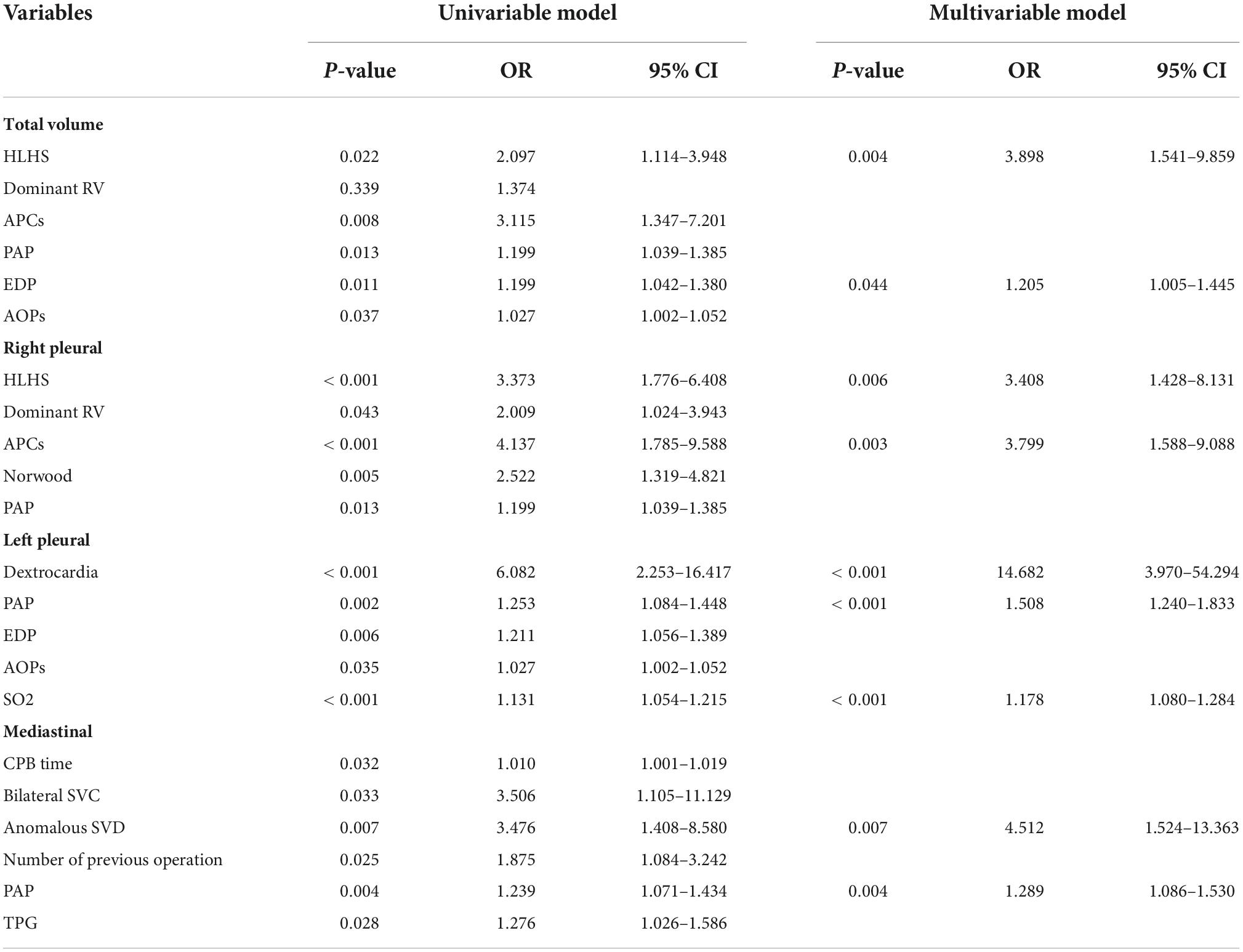
Table 3. Factors associated with excessive volume of drainage.
As for right pleural drainage, HLHS (OR = 3.373, p < 0.001), presence of APCs (OR = 4.137, p < 0.001), and PAP (OR = 1.199, p = 0.013), were associated with volume from drainage with univariable analysis. Multivariable analysis identified HLHS (OR = 3.400, p = 0.006) and presence of APCs (OR = 3.799, p = 0.003) as independent factors associated with high volume of drainages.
As for left pleural drainage, dextrocardia (OR = 6.082, p < 0.001), PAP (OR = 1.253, p = 0.002), SVEDP (OR = 1.211, p = 0.006), systolic aortic pressure (OR = 1.027, p = 0.035), and arterial oxygen saturation (OR = 1.131, p < 0.001) were associated with a large volume from drainage in the univariable analysis. Multivariable analysis demonstrated dextrocardia (OR = 14.682, p < 0.001), PAP (OR = 1.508, p < 0.001), and arterial oxygen saturation (OR = 1.178, p < 0.001) were independent factors associated with high volume of drainages. Results of the analysis using all variables are shown in Supplementary Table 2. Results of risk factor analysis for total pleural effusions (right and left altogether) are shown in Supplementary Table 3.
As for total duration of mediastinal and pleural drainage, HLHS (HR = 1.776, p < 0.001), dominant RV (HR = 1.590, p = 0.001), presence of APCs (HR = 2.222, p < 0.001), previous Norwood procedure (HR = 1.541, p = 0.002), PAP (HR = 1.093, p = 0.004), and SVEDP (HR = 1.072, p = 0.020) were associated with total duration of drainage in univariable analysis (Table 4). Multivariable analysis demonstrated that HLHS (HR = 1.818, p = 0.007), presence of APCs (HR = 1.988, p = 0.002), and SVEDP (HR = 1.083, p = 0.023) were independent factors associated with total duration of drainages. Winter respiratory viral season of November through March was not identified as a factor influencing duration of pleural effusions (HR = 0.980, p = 0.890).
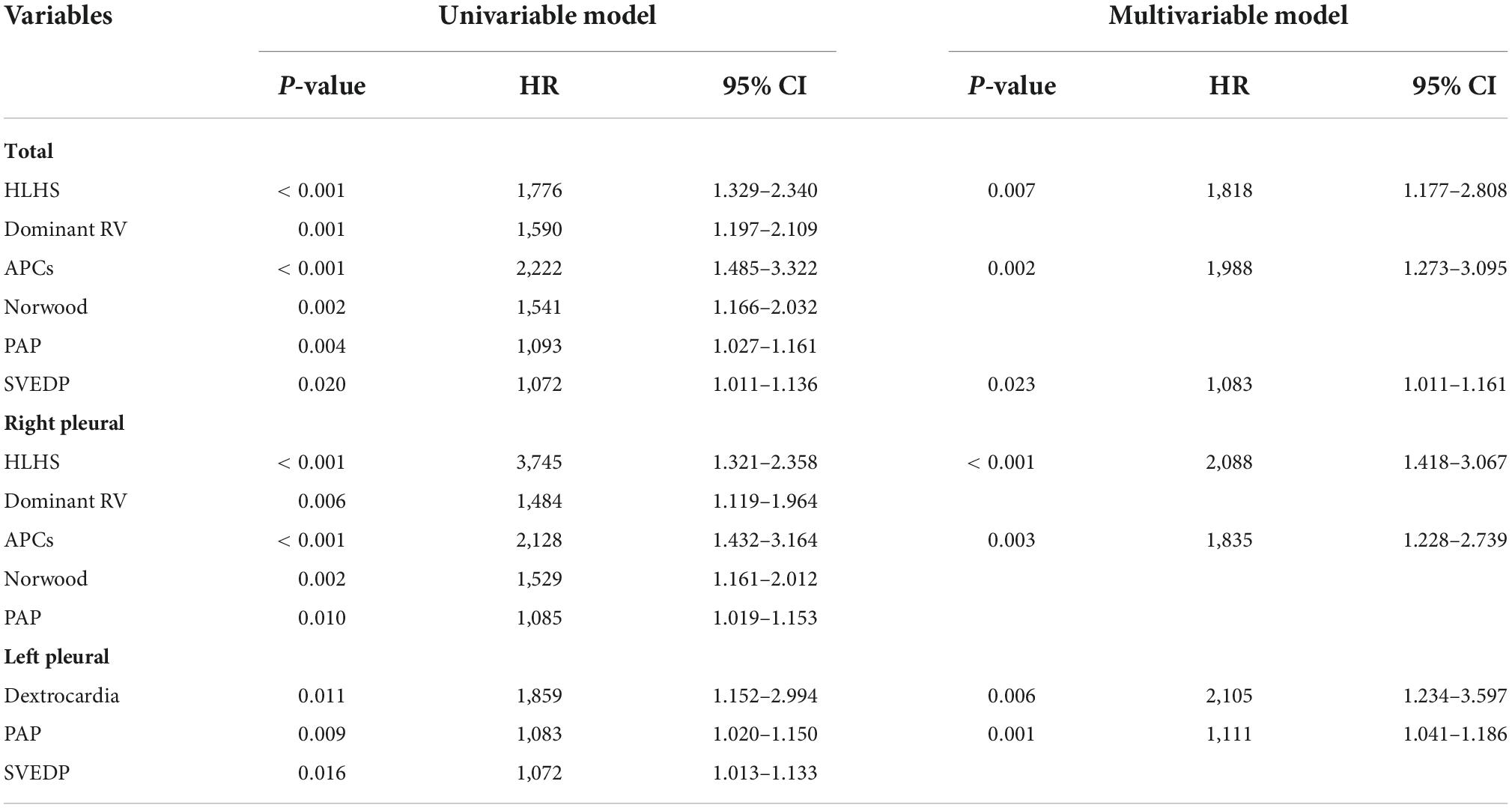
Table 4. Factors associated with duration of drainage.
As for duration of right pleural drainage, HLHS (HR = 3.745, p < 0.001), dominant RV (HR = 1.484, p = 0.006), presence of APCs (HR = 2.128, p < 0.001), previous Norwood procedure (HR = 1.529, p = 0.002), and PAP (HR = 1.085, p = 0.010) were associated with long duration of drainage in univariable analysis. Multivariable analysis showed that HLHS (HR = 2.088, p < 0.001) and presence of APCs (HR = 1.835, p = 0.003) were independent factors associated with long duration of drainages.
As for duration of left pleural drainage, dextrocardia (HR = 1.859, p = 0.011), PAP (HR = 1.083, p = 0.009), and SVEDP (HR = 1.072, p = 0.162), were associated with long duration of drainage in univariable analysis. Multivariable analysis demonstrated that dextrocardia (HR = 2.105, p = 0.006) and PAP (HR = 1.111, p = 0.001) were independent factors associated with long duration of drainages. The additional surgical procedures did not influence the analyzed outcomes. Results of the analysis using all variables are shown in Supplementary Table 4.
As for the impact of effusion on late outcomes, the amount of effusion was not identified as an increased risk of adverse outcomes following EC-TCPC (Table 5). Whereas total duration of any drainages (HR = 1.074, p = 0.022) and duration of left pleural drainage (HR = 1.082, p = 0.043) were associated with an increased risk for late adverse outcomes. Need for ascites drainage was also associated with adverse events (HR = 6.768, p = 0.036). Variables which influenced the amount and duration of drainage were not associated with the following variables: HLHS (HR = 0.976, p = 0.979), presence of APCs (HR = 0.674, p = 0.732), previous Norwood procedure (HR = 1.251, p = 0.807), PAP (HR = 1.175, p = 0.385), SVEDP (HR = 1.248, p = 0.292), Dextrocardia (HR = 0.043, p = 0.657), systolic arterial pressure (HR = 0.980, p = 0.428), arterial oxygen saturation (HR = 0.969, p = 0.135), anomalous systemic venous drainage (HR = 0.043, p = 0.641), TPG (HR = 1.402, p = 0.313), dominant RV (HR = 0.932, p = 0.939), and heterotaxy (HR = 0.043, p = 0.657). The total duration of any drainage was an independent factor associated with adverse events following EC-TCPC (HR = 1.098, p = 0.015) as determined by multivariable analysis. The details of adverse events are shown in Supplementary Table 5.
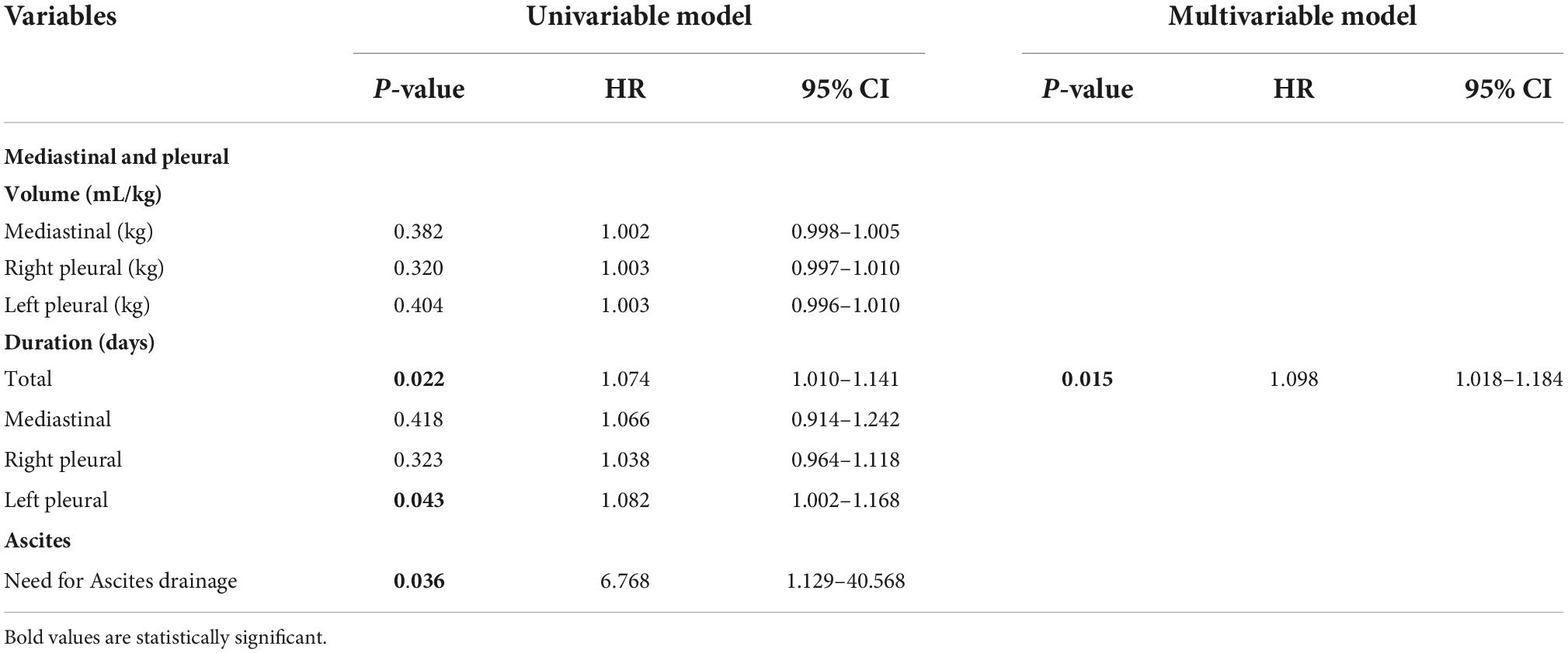
Table 5. Factors associated with adverse events after total cavopulmonary connection (TCPC).
Chylothorax was observed in 46 patients (21.9%). Patients with chylothorax had significantly longer duration of right pleural drainage (p < 0.001) and left pleural drainage (p < 0.001). Volume of drainage was higher in patients with chylothorax in the right pleural drainage (p < 0.001) and left pleural drainage (p < 0.001).
According to the findings of the current study, HLHS, dominant RV, APCs, PAP, and SVEDP were all associated with longer durations of pleural and mediastinal drainage after EC-TCPC. This was also the case for the volume of drainage that occurred after the procedure. Both the volume and the duration of left pleural drainage were found to be associated with dextrocardia. A risk factor for adverse events that occurred after EC-TCPC was not the amount of effusions themselves, but rather the length of time drainage was performed.
Previous studies demonstrated various factors which influenced postoperative pleural effusions after the Fontan procedure (5–8, 17–22): ventricular stiffness (5), pulmonary atresia (6), pre-Fontan PAP (6, 7, 17, 19, 20), chylothorax (7, 18), atrioventricular valve regurgitation (7), APCs (7, 21, 22), CPB time (7, 8), AXC time (7), oxygen saturation (8), HLHS (17, 23), absence of fenestration (17, 18, 20), younger age at Fontan (18), prolonged mechanical ventilation (18), and winter respiratory viral season of November through March (19). In our study, pre-Fontan PAP and APCs were significant determinants of pleural effusion volume and duration. Risk factors included HLHS, RV dominance, a previous Norwood procedure, APCs, and SVEDP. Dextrocardia was also found to affect the duration and volume of left pleural effusions. In patients with HLHS who had previously undergone the Norwood operation, the volume of right-sided pleural effusion increased significantly. On the contrary, patients with dextrocardia had a significant increase in the duration and volume of left-sided pleural effusion. Though, it is unclear why dextrocardia was linked to the volume and duration of left-sided pleural effusions. In patients with dextrocardia, we assume that the total volume of the left lung is greater than that of the right lung. As a result, the number of left-sided pleural effusions was greater than that of the right lung. However, we do not know why the duration of drainage was longer in the left lung. Further investigation of the pulmonary artery flow profile by cardiac magnetic resonance is required to explain this phenomenon.
The duration of pleural effusion may be affected by the timing of TCPC completion. Our clinical demographic criteria were an age of at least 2 years, a weight of at least ten kilograms, and the ability to walk. In another study, when the chest drainage criteria and age were examined, the factor older age was associated with significantly longer duration of chest drainage (24). According to a recent study, Fontan patients have a reduced carbon monoxide diffusing capacity, which is primarily due to low alveolar volume. Lung stiffness increases, affecting alveolar volume and capillary membrane function. These parameters have a negative correlation with Fontan completion age, implying that earlier Fontan completion may benefit lung function (25). We believe that early Fontan completion might preserve systemic ventricular function, prevent (or at least mitigate) the harmful consequences of the Fontan circulation, and provide better functional ability.
The duration of pleural effusions was found to be related with a higher risk of unfavorable outcomes following the Fontan procedure in several studies (1, 23, 26). Whereas another study did not show the association of adverse outcomes and prolonged pleural effusions (17). According to the findings of our study, the volume of pleural drainage was not a factor in determining whether or not there was an association between EC-TCPC and adverse events.
Not performing fenestration for EC-TCPC was found to be a risk factor for adverse events including prolonged pleural effusion (6, 17, 18, 20, 27, 28). They demonstrated that fenestration is an effective procedure for lowering pulmonary artery pressure in patients with elevated pulmonary pressure. However, other institutions found no difference in need for chest drains between fenestrated and non-fenestrated Fontan procedure, and adopted selective fenestration strategy (1, 29–31). A propensity score–matched study with 1,443 patients, found no difference in long-term survival or freedom from Fontan failure between patients with and without fenestration (29). Patients with fenestration had a higher incidence of long-term thromboembolic events. It appears that fenestration in Fontan circulation has no long-term benefits. We agree that under usual circumstances a fenestration at the time of an EC-TCPC is not required. Only in patients who were considered to be high-risk, such as those who had an elevated pulmonary artery pressure or trans-pulmonary gradient, significant atrioventricular regurgitation, or single-lung physiology, we choose to perform fenestration (10, 11). In total, we have done EC-TCPC procedures in over 98% of our patients without fenestration.
It is important to recall that a shorter duration of mechanical ventilation is related to reduced pleural effusions. Previous research indicated that early extubation following EC-TCPC, including extubation in the operating room, is a safe and successful approach, resulted in clinical benefits (32–34).
Other therapies include diuretics, surgical and catheter intervention for pathway obstruction, coil embolization of APCs, and secondary fenestration. A defined management strategy might reduce the amount of effusion (35, 36). The use of modified ultrafiltration, which is a standard procedure at our center, helps to reduce postoperative effusions (37).
This study was limited by its retrospective, non-randomized, and single-center design. Surgical and medical management may have changed during the study period, probably influencing the long-term outcomes. As for adverse events, the pathophysiology leading to the endpoints may be very different, especially for death and rhythm disturbances. Hence, the impact of potential risk factors is difficult to interpret. These might be limitations for this risk analysis. A relatively short follow-up period might cause an unreliability for the analysis of impact of amount and duration of mediastinal and pleural drainage on adverse events.
According to the findings of our research with a relatively large cohort of non-fenestrated EC-TCPC performed at around 2 years old, pleural effusions following EC-TCPC were linked to a variety of factors, including but not limited to HLHS, RV dominance, Norwood surgery, a high PAP, and a high SVEDP. It was also found that the presence of similar risk factors is associated with greater volumes of pleural effusions. Dextrocardia was an independent factor for prolonged and higher volume of left pleural effusion, suggesting the importance of the dominant lung volume. However, the total amount of effusions was not associated with an increased risk of adverse outcomes, whereas the duration of pleural drainage affects the long-term prognosis following EC-TCPC. In the days following EC-TCPC, patients with persistent pleural effusions must be thoroughly observed.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Institutional Review Board of the Technical University of Munich approved the study (approved number of 305/20 S-KH on 2nd June, 2020). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
PH, PM, HS, BM, AH, JH, and MO: conceptualization. PH, PM, AH, JH, and MO: methodology. PH, PM, HS, AH, JH, and MO: validation and writing—review and editing. PH, PM, HS, BM, JV, MS, BR, PE, AH, JH, and MO: resources and writing—original draft. PH, PM, HS, JH, and MO: visualization. JH and MO: supervision and project administration. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.1026445/full#supplementary-material
Supplementary Figure 1 | Histogram of volume of drainage. Total volume from any drainage per patient was median 120.3 (IQR 61.0–202.7) mL/kg.
Supplementary Figure 2 | Histogram of duration of drainage. Median duration of right pleural and left pleural drainage after EC-TCPC was 7 (IQR 4–13, minimum 0 and maximum 51) days, and 2 (IQR 0–7, minimum 0 and maximum 40) days, respectively.
1. Mery CM, De León LE, Trujillo-Diaz D, Ocampo EC, Dickerson HA, Zhu H, et al. Contemporary outcomes of the fontan operation: a large single-institution cohort. Ann Thorac Surg. (2019) 108:1439–46.
2. Moon J, Shen L, Likosky DS, Sood V, Hobbs RD, Sassalos P, et al. Relationship of ventricular morphology and atrioventricular valve function to long-term outcomes following fontan procedures. J Am Coll Cardiol. (2020) 76:419–31. doi: 10.1016/j.jacc.2020.05.059
3. Cao JY, Marathe SP, Zannino D, Celermajer DS, Justo RN, Alphonso N, et al. Fontan operation at less than 3 years of age is not a risk factor for long-term failure. Eur J Cardiothorac Surg. (2022) 61:497–504.
4. Ono M, Burri M, Cleuziou J, Pabst von Ohain J, Beran E, Strbad M, et al. Impact of early fontan completion on postoperative outcomes in patients with a functional single ventricle. Eur J Cardiothorac Surg. (2017) 51:995–1002.
5. Garofalo CA, Cabreriza SE, Quinn TA, Weinberg AD, Printz BF, Hsu DT, et al. Ventricular diastolic stiffness predicts perioperative morbidity and duration of pleural effusions after the fontan operation. Circulation. (2006) 114:I56–61. doi: 10.1161/CIRCULATIONAHA.105.001396
6. Rito Lo M, Al-Radi OO, Saedi A, Kotani Y, Ben Sivarajan V, Russell JL, et al. Chylothorax and pleural effusion in contemporary extracardiac fenestrated fontan completion. J Thorac Cardiovasc Surg. (2018) 155:2069–77. doi: 10.1016/j.jtcvs.2017.11.046
7. Tran DD, Le TN, Dang VHT, Vo HL. Predictors of prolonged pleural effusion after the extracardiac fontan procedure: a 8-year single-center experience in resource-scare setting. Pediatr Cardiol. (2021) 42:89–99. doi: 10.1007/s00246-020-02457-1
8. Gupta A, Daggett C, Behera S, Ferraro M, Wells W, Starnes V. Risk factors for persistent pleural effusions after the extracardiac fontan procedure. J Thorac Cardiovasc Surg. (2004) 127:1664–9.
9. Buchhorn R, Bartmus D, Buhre W, Bürsch J. Pathogenetic mechanisms of venous congestion after the fontan procedure. Cardiol Young. (2001) 11:161–8. doi: 10.1017/s1047951101000051
10. Schreiber C, Hörer J, Vogt M, Cleuziou J, Prodan Z, Lange R. Nonfenestrated extracardiac total cavopulmonary connection in 132 consecutive patients. Ann Thorac Surg. (2007) 84:894–9. doi: 10.1016/j.athoracsur.2007.04.034
11. Ono M, Kasnar-Samprec J, Hager A, Cleuziou J, Burri M, Langenbach C, et al. Clinical outcome following total cavopulmonary connection: a 20-year single-centre experience. Eur J Cardiothorac Surg. (2016) 50:632–41. doi: 10.1093/ejcts/ezw091
12. Nakano T, Kado H, Tatewaki H, Hinokiyama K, Oda S, Ushinohama H, et al. Results of extracardiac conduit total cavopulmonary connection in 500 patients. Eur J Cardiothorac Surg. (2015) 48:825–32. doi: 10.1093/ejcts/ezv072
13. Kim SJ, Kim WH, Lim HG, Lee JY. Outcome of 200 patients after an extracardiac fontan procedure. J Thorac Cardiovasc Surg. (2008) 136:108–16.
14. Giannico S, Hammad F, Amodeo A, Michielon G, Drago F, Turchetta A, et al. Clinical outcome of 193 extracardiac fontan patients: the first 15 years. J Am Coll Cardiol. (2006) 47:2065–73. doi: 10.1016/j.jacc.2005.12.065
15. Ono M, Burri M, Balling G, Beran E, Cleuziou J, Pabst von Ohain J, et al. Predicted clinical factors associated with the intensive care unit length of stay after total cavopulmonary connection. J Thorac Cardiovasc Surg. (2019) 157:2005–13.
16. Allen KY, Downing TE, Glatz AC, Rogers LS, Ravishankar C, Rychik J, et al. Effect of fontan-associated morbidities on survival with intact fontan circulation. Am J Cardiol. (2017) 119:1866–71.
17. Kim G, Ko H, Byun J-H, Lee HD, Kim H, Sung SC, et al. Risk factors for prolonged pleural effusion after extracardiac fontan operation. Pediatr Cardiol. (2019) 40:1545–52.
18. Luo Q, Zhao W, Su Z, Liu Y, Jia Y, Zhang L, et al. Risk factors for prolonged pleural effusion following total cavopulmonary connection surgery: 9 years’ experience at Fuwai hospital. Front Pediatr. (2019) 7:456. doi: 10.3389/fped.2019.00456
19. Fedderly RT, Whitstone BN, Frisbee SJ, Tweddell JS, Litwin SB. Factors related to pleural effusions after fontan procedure in the era of fenestration. Circulation. (2001) 104:I148–51. doi: 10.1161/hc37t1.094817
20. Zou M, Wang Y, Cui H, Ma L, Yang S, Xia Y, et al. Outcomes of total cavopulmonary connection for single ventricle palliation. J Thorac Dis. (2016) 8:43–51.
21. Grosse-Wortmann L, Drolet C, Dragulescu A, Kotani Y, Chaturvedi R, Lee KJ, et al. Aortopulmonary collateral flow volume affects early postoperative outcome after fontan completion: a multimodality study. J Thorac Cardiovasc Surg. (2012) 144:1329–36. doi: 10.1016/j.jtcvs.2012.03.032
22. Odenwald T, Quail MA, Giardini A, Khambadkone S, Hughes M, Tann O, et al. Systemic to pulmonary collateral blood flow influences early outcomes following the total cavopulmonary connection. Heart. (2012) 98:934–40. doi: 10.1136/heartjnl-2011-301599
23. Iyengar AJ, Winlaw DS, Galati JC, Celermajer DS, Wheaton GR, Gentles TL, et al. Trends in fontan surgery and risk factors for early adverse outcomes after Fontan surgery: the Australia and New Zealand fontan registry experience. J Thorac Cardiovasc Surg. (2014) 148:566–75. doi: 10.1016/j.jtcvs.2013.09.074
24. Bezuska L, Lebetkevicius V, Lankutis K, Sudikiene R, Sirvydis VJ, Tarutis V. Fontan completion for younger than 3 years of age: outcome in patients with functional single ventricle. Pediatr Cardiol. (2015) 36:1680–4.
25. Laohachai K, Badal T, Thamrin C, Robinson PD, Kennedy B, Rice K, et al. Older age at fontan completion is associated with reduced lung volumes and increased lung reactance. Int J Cardiol. (2022) 364:38–43. doi: 10.1016/j.ijcard.2022.06.037
26. Poh CL, Cordina RL, Iyengar AJ, Zannino D, Grigg LE, Wheaton GR, et al. Pre- and post-operative determinants of transplantation-free survival after fontan. The Australia and New Zealand experience. Int J Cardiol Heart Vasc. (2021) 35:100825. doi: 10.1016/j.ijcha.2021.100825
27. Lemler MS, Scott WA, Leonard SR, Stromberg D, Ramaciotti C. Fenestration improves clinical outcome of the fontan procedure: a prospective, randomized study. Circulation. (2002) 105:207–12.
28. Atz AM, Travison TG, McCrindle BW, Mahony L, Quartermain M, Williams RV, et al. Late status of fontan patients with persistent surgical fenestration. J Am Coll Cardiol. (2011) 57:2437–43.
29. Daley M, Buratto E, King G, Grigg L, Iyengar A, Alphonso N, et al. Impact of fontan fenestration on long-term outcomes: a propensity score-matched analysis. J Am Heart Assoc. (2022) 11:e026087. doi: 10.1161/JAHA.122.026087
30. Salazar JD, Zafar F, Siddiqui K, Coleman RD, Morales DL, Heinle JS, et al. Fenestration during fontan palliation: now the exception instead of the rule. J Thorac Cardiovasc Surg. (2010) 140:129–36. doi: 10.1016/j.jtcvs.2010.03.013
31. Talwar S, Paidi A, Sreeniwas V, Dutt Upadhyay A, Das S, Choudhary SK. Comparison of pleural effusion between fenestrated and nonfenestrated extracardiac fontan: a prospective randomized study. J Card Surg. (2020) 35:2688–94. doi: 10.1111/jocs.14886
32. Morales DL, Carberry KE, Heinle JS, McKenzie ED, Fraser CD Jr., Diaz LK. Extubation in the operating room after fontan’s procedure: effect on practice and outcomes. Ann Thorac Surg. (2008) 86:576–81. doi: 10.1016/j.athoracsur.2008.02.010
33. Mutsuga M, Quiñonez LG, Mackie AS, Norris CM, Marchak BE, Rutledge JM, et al. Fast-track extubation after modified fontan procedure. J Thorac Cardiovasc Surg. (2012) 144:547–52. doi: 10.1016/j.jtcvs.2012.05.047
34. Ono M, Georgiev S, Burri M, Mayr B, Cleuziou J, Strbad M, et al. Early extubation improves outcome following extracardiac total cavopulmonary connection. Interact Cardiovasc Thorac Surg. (2019) 29:85–92.
35. Pike NA, Okuhara CA, Toyama J, Gross BP, Wells WJ, Starnes VA. Reduced pleural drainage, length of stay, and readmissions using a modified fontan management protocol. J Thorac Cardiovasc Surg. (2015) 150:481–7. doi: 10.1016/j.jtcvs.2015.06.042
36. Sunstrom RE, Muralidaran A, Gerrah R, Reed RD, Good MK, Armsby LR, et al. A defined management strategy improves early outcomes after the fontan procedure: the PORTLAND protocol. Ann Thorac Surg. (2015) 99:148–55. doi: 10.1016/j.athoracsur.2014.06.121
Keywords: pleural effusion, univentricular heart, total cavopulmonary connection (TCPC), congenital heart disease, outcome
Citation: Heinisch PP, Metz P, Staehler H, Mayr B, Vodiskar J, Strbad M, Ruf B, Ewert P, Hager A, Hörer J and Ono M (2022) Pleural and mediastinal effusions after the extracardiac total cavopulmonary connection: Risk factors and impact on outcome. Front. Cardiovasc. Med. 9:1026445. doi: 10.3389/fcvm.2022.1026445
Received: 23 August 2022; Accepted: 17 October 2022;
Published: 08 November 2022.
Edited by:
Bernhard Winkler, Vienna Health Association, AustriaReviewed by:
Arda Özyüksel, Biruni University, TurkeyCopyright © 2022 Heinisch, Metz, Staehler, Mayr, Vodiskar, Strbad, Ruf, Ewert, Hager, Hörer and Ono. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Masamichi Ono, b25vQGRobS5taG4uZGU=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.