
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med., 24 November 2022
Sec. Cardiovascular Epidemiology and Prevention
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.1012531
 Le Duc Huy1
Le Duc Huy1 Nguyen L. T. Truong2,3
Nguyen L. T. Truong2,3 Nhi Y. Hoang4
Nhi Y. Hoang4 Nhi Thi Hong Nguyen1,5
Nhi Thi Hong Nguyen1,5 Thao T. P. Nguyen6
Thao T. P. Nguyen6 Loan T. Dang7,8Yi-Hsin Elsa Hsu5,9,10
Loan T. Dang7,8Yi-Hsin Elsa Hsu5,9,10 Chung-Chien Huang5,10,11,12
Chung-Chien Huang5,10,11,12 Yao-Mao Chang5,13Chung-Liang Shih14Elena T. Carbone15
Yao-Mao Chang5,13Chung-Liang Shih14Elena T. Carbone15 Shwu-Huey Yang4,16,17*
Shwu-Huey Yang4,16,17* Tuyen V. Duong4,18*
Tuyen V. Duong4,18*Background: Health literacy (HL) has shown its important role on reducing the burden of heart diseases. However, no study has provided a comprehensive worldwide view of the data regarding HL and heart diseases. The study aimed to provide insight into: (1) the intellectual structure, (2) research trends, and (3) research gaps on HL and heart diseases; and (4) to explore HL scales commonly utilized in heart studies.
Materials and methods: Studies related to HL and heart diseases were retrieved from Web of Science, Scopus, and PubMed. All publications published between 2000 and 2021 were included after conducting keyword searches on “heart diseases” in general or on specific types of heart diseases (e.g., “heart failure”) and “health literacy”. Bibliometric analyses were carried out using the Bibliometrix R package and VOSviewer 1.6.14.
Findings: A total of 388 original research articles and reviews on HL and heart diseases were included in our study. The studies were primarily conducted in the United States and developed countries. A total of 337 studies (86.9%) focused on heart failure (200 studies, 51.5%) and ischemic heart diseases (137 studies, 35.3%). Sixty-two studies (16.0%) focused on other heart diseases (e.g., valvular diseases and rheumatic heart diseases). The number of interventional studies was limited (52 studies, 13.4%) and fluctuated from 2000 to 2021. The most common questionnaires measuring health literacy among patients with heart diseases were the Test of Functional Health Literacy in Adults (TOFHLA), Short Test of Functional Health Literacy in Adults (STOFHLA), and Brief Health Literacy Screen (BHLS). Use of the eHealth Literacy Scale (eHEALS) has become the latest trend among patients with heart diseases.
Conclusion: Health literacy and heart diseases were most often studied in the United States and developed countries. Several HL tools were used; eHEALS has been lately used in this field. These findings suggest the need to conduct more empirical studies on HL and heart diseases in different settings (e.g., developing or poor countries) and with different types of heart diseases (e.g., valvular and rheumatic disorders). Additionally, it is necessary to develop heart disease-specified HL scales for research and practice.
According to the Global Burden of Disease (GBD) Study 2019, cardiac diseases remain the most common cause of mortality globally, with over 9.1 million deaths. Of these, deaths due to ischemic heart disease made up the highest proportion (49.2%) in 2019 (1). Although cardiac risk factor management guidelines emphasize promoting healthy lifestyles, cardiac rehabilitation, and medication use (2, 3), it would be challenging for patients with inadequate health literacy (HL) to adopt and enhance healthy practices (4).
Health literacy indicates the different levels of knowledge and skills to understand, apply and critically analyze health information. Hence, people with adequate HL are able to foster self-management, decision making and many determinants of health (5–7). However, insufficient HL remains a major concern, resulting in restricted access to health services, poor physician-patient communication, unhealthy lifestyle behaviors, and increasing risks of hospital readmission and mortality (8, 9). Therefore, improvement of HL is of utmost importance to enhance patients’ capacity for self-management of their diseases and prevention of prospective cardiac events (10).
As a result of scientometric and big data advancements, bibliometric analysis is gaining more interest to deal with the large amount of data from scientific publications. Bibliometric research focuses on exploring new trends, deciphering potential areas in a particular research discipline, and investigating the contribution of journals, authorship networks, institutes, and countries based on constructing the intellectual structure over the time (11, 12). Bibliometric data are often extracted from large scientific databases including Scopus, Web of Science, PubMed, or Google Scholar. A recent bibliometric study on HL instruments shows that there were 90 health condition-specific HL instruments with a major focus on chronic diseases (13). In addition, to our knowledge, there has been a wealth of systematic reviews and meta-analyses to examine the role of HL in cardiovascular diseases. Yet, no recent bibliometric study has investigated the overall evidence on HL in cardiac disease care and management.
Therefore, we conducted a bibliometric analysis using data from three well-known large databases (Scopus, Web of Science, and PubMed) to systematically investigate all available evidence to create a global view of HL research in patients with heart diseases. We also explored the most common HL instruments used in these patients over time. We expect that our study will support researchers, health policymakers and practitioners in developing strategic interventions to enhance HL and improve the health outcomes of patients with heart diseases.
We retrieved scientific papers from three databases–Web of Science, Scopus, and PubMed. The search terms related to cardiac diseases were developed based on the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10) (14). The search terms focused on heart diseases in general and specific types of heart diseases, and HL. We searched and retrieved the relevant data on March 15 2022. Detailed steps of the search process are provided in Table 1.
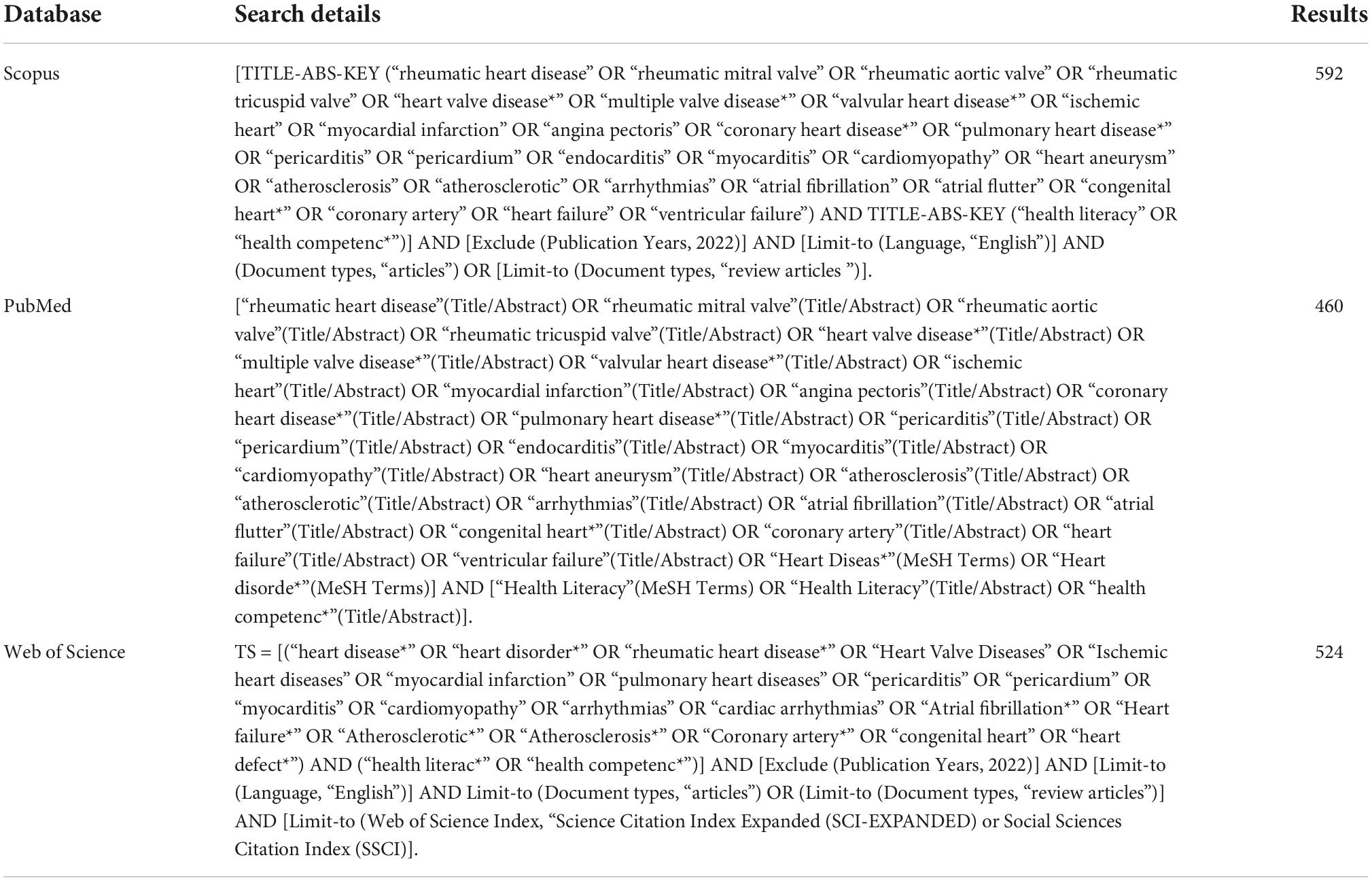
Table 1. Search strategies in PubMed, Scopus, and Web of Science.
We included original research articles and reviews written in English and published between 2000 and 2021 in the analysis. Grey literature, conference proceedings, books/book review, letters, case reports, congressional papers, editorials, comments, and news were excluded.
We used the Bibliometrix R package to combine data from various sources and remove duplication (15). Researchers screened article titles and abstracts to identify relevant papers and extract bibliometric parameters. During the extraction process, we focused on the following key bibliometric parameters: year of publication, citation, country, journal, study design, types of heart disease, and HL questionnaires. To identify the HL instruments, the researchers manually screened the full text in all the studies and created a comprehensive list of HL questionnaires. Then, we combined the uncommon HL instruments into groups with similar applications. After screening, 388 papers were included in the final analysis. We employed PRISMA for the extraction flow (16). The data extraction process is presented in Figure 1.
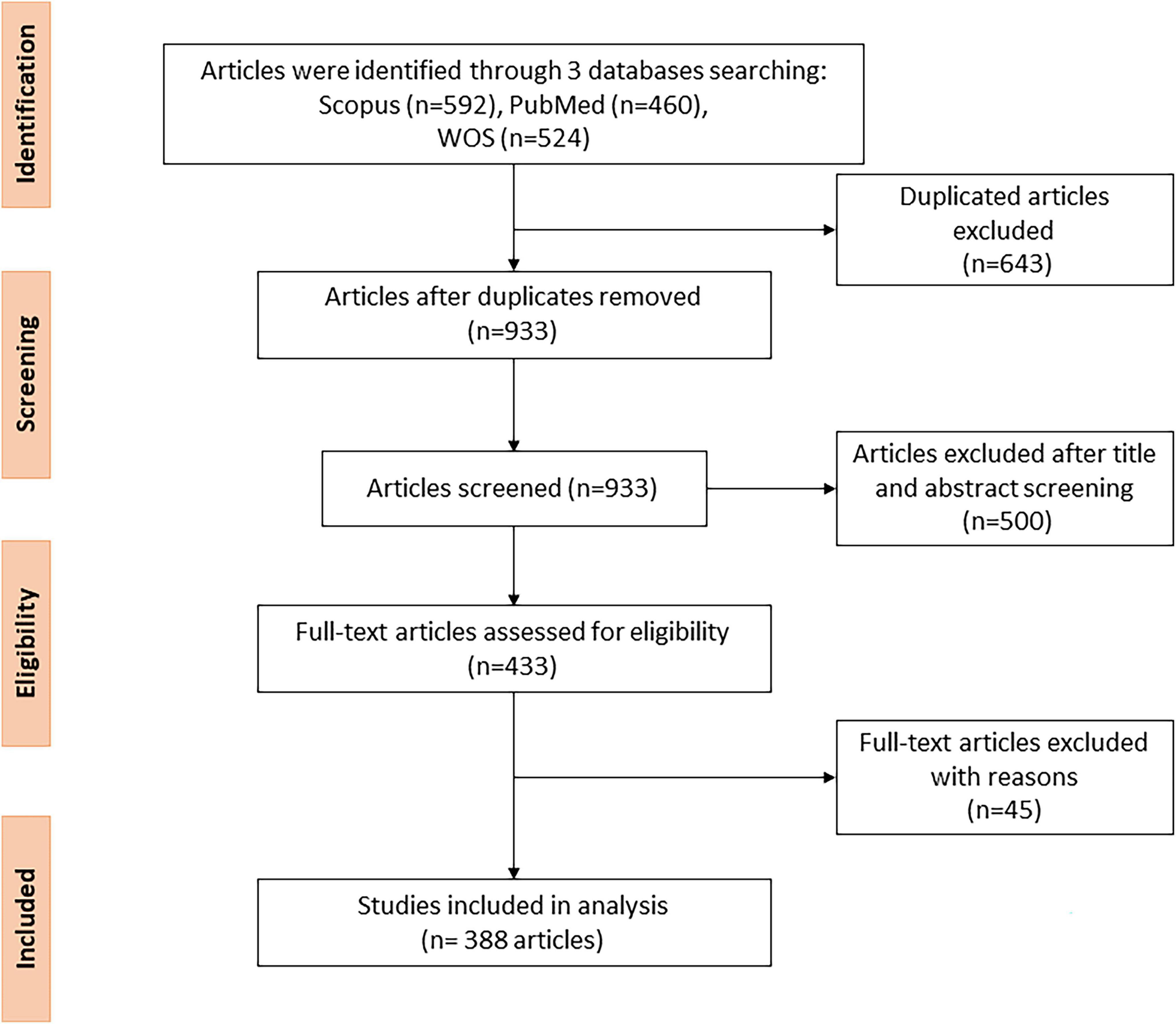
Figure 1. The PRISMA flow diagram.
We used the Bibliometrix R package (15) and Microsoft Excel (version 2013) to analyze and visualize the bibliometric parameters. The VOS Viewer (version 1.6.14) was utilized to carry out the cluster analysis, co-authorship analysis, and to establish the network maps (nodes and links) for countries and authors (17).
Figure 2 shows the growth rate of publications by year. In general, the number of publications has increased, while the average citations decreased, respectively by year. Specifically, the number of publications increased gradually over the study period and significantly grew after 2010. In particular, the number of publications peaked at 56 publications in 2020. Notably, the number of publications dropped significantly in 2021. On the other hand, the average citation per paper ranked the highest in 2006, with 118 citations.
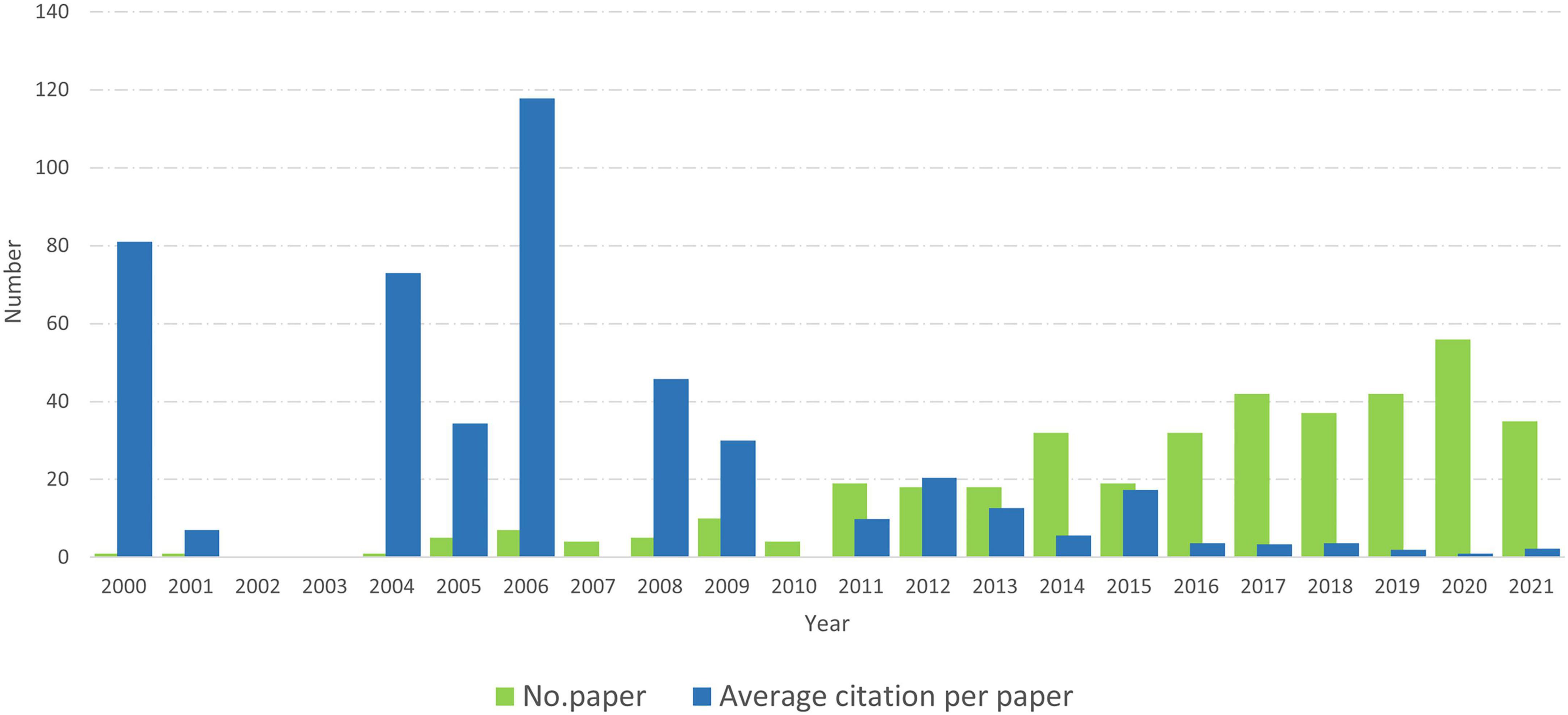
Figure 2. The growth rate of publications by year.
Figure 3 illustrates the number of publications by country. Overall, heart disease-related HL studies were conducted in 45 nations. The United States contributed the most publications, with 202 articles, followed by Australia (25 articles), and China (14 articles). Canada, Brazil, Argentina, Iran, India, Egypt, and others have less than ten articles, as indicated by the global maps.
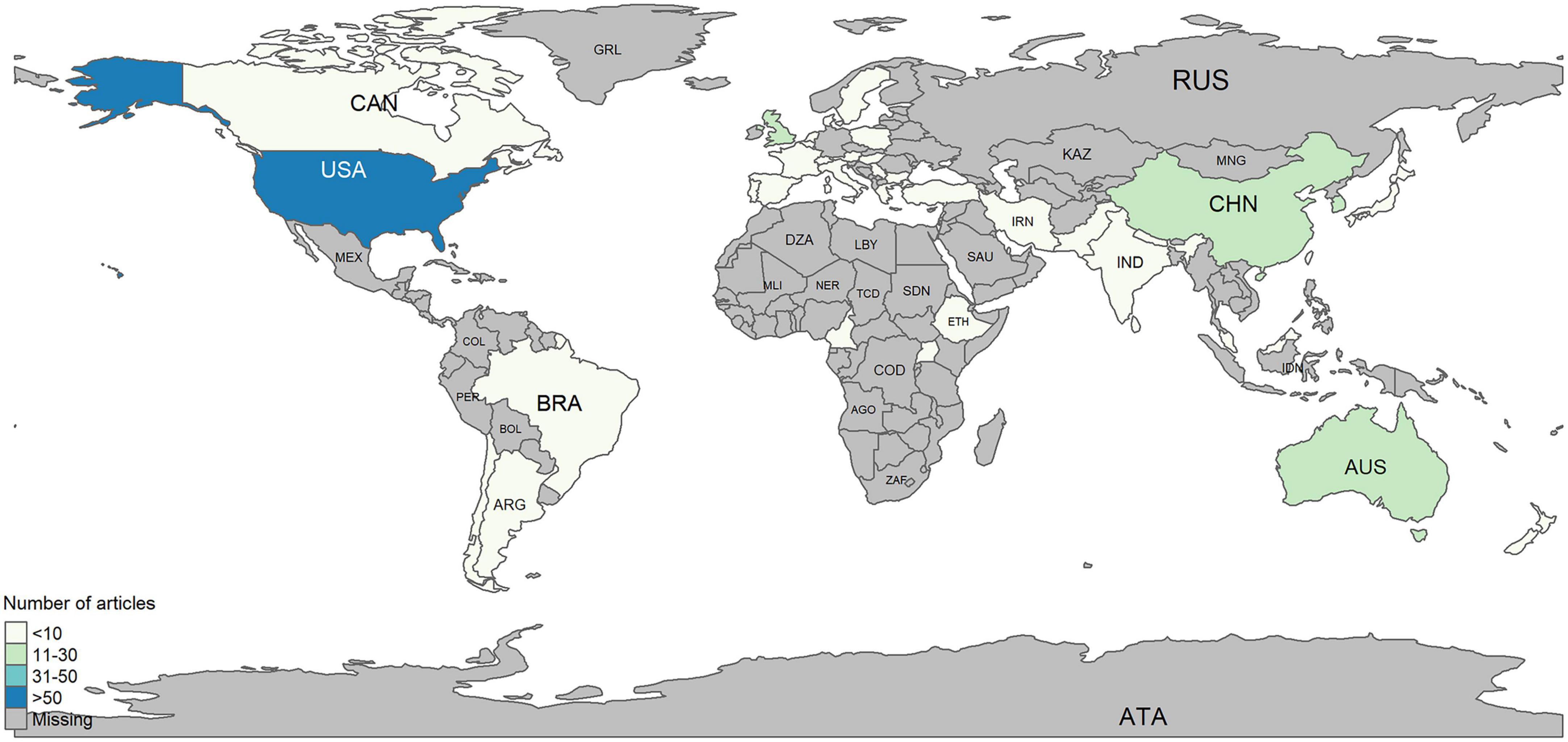
Figure 3. Global maps of publication by countries.
Co-authorship analyses were conducted to investigate the cooperation network between authors and nations, wherein publications with a stronger overall link strength between authors and countries indicate a tighter relationship (18).
As shown in Figure 4, the United States has the highest network of co-authorship in the heart disease-related research among countries, followed by Australia, the United Kingdom, Sweden, and Germany. Other representatives of Europe (e.g., Netherlands, Austria, and Spain), North America (e.g., Canada), and Asia (e.g., Japan, South Korea, and China) have often collaborated with the leading co-authorship countries in this field.
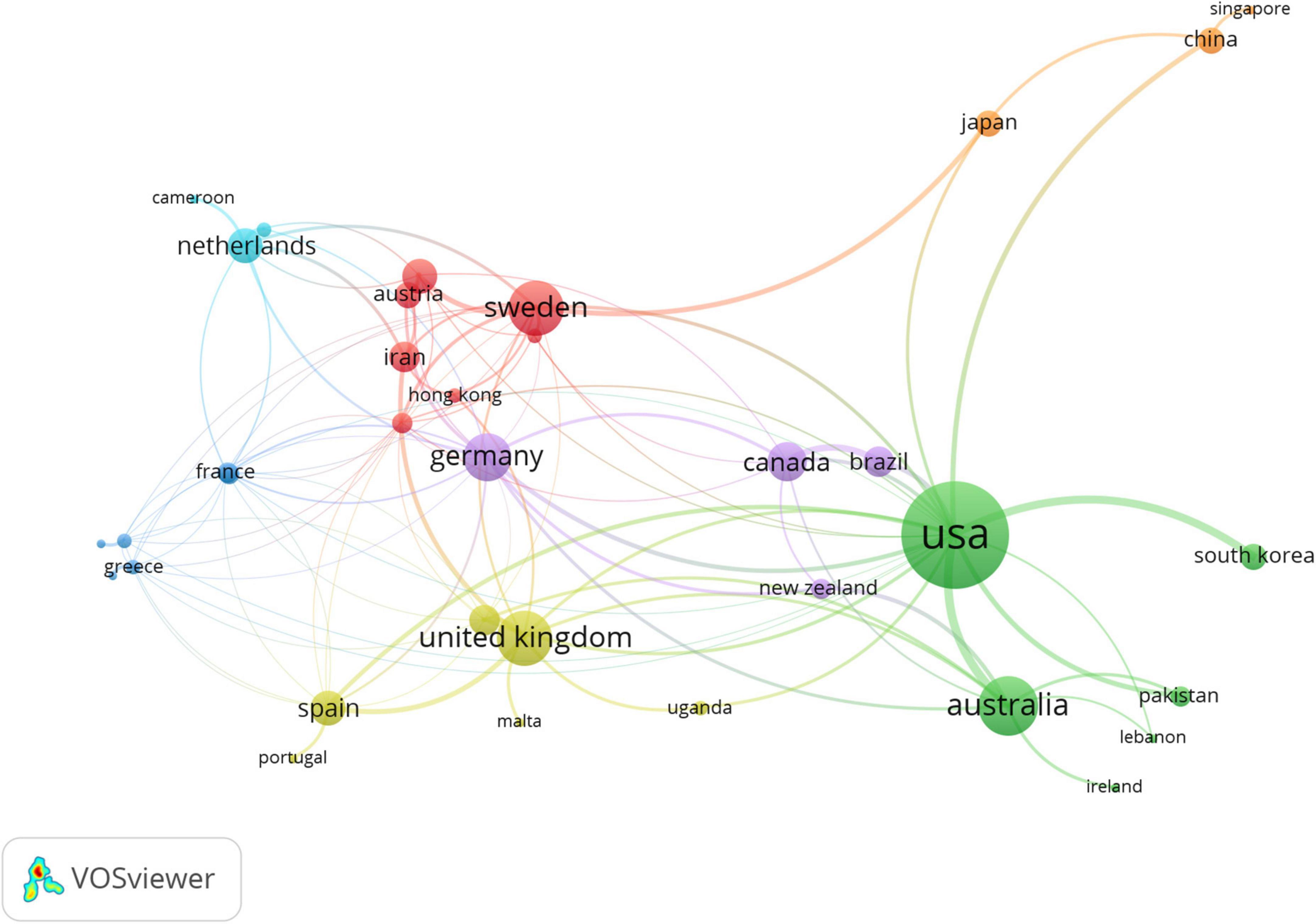
Figure 4. The country co-authorship network of heart diseases related publications.
Figure 5 illustrates the co-authorship network by countries who conducted heart diseases-related studies over time. The United States, Australia, Netherlands, Canada, and Spain (in purple) have a long history of heart disease research. Conversely, Iran, Hong Kong, Pakistan, and China (in yellow) joined this research field in the previous few years.
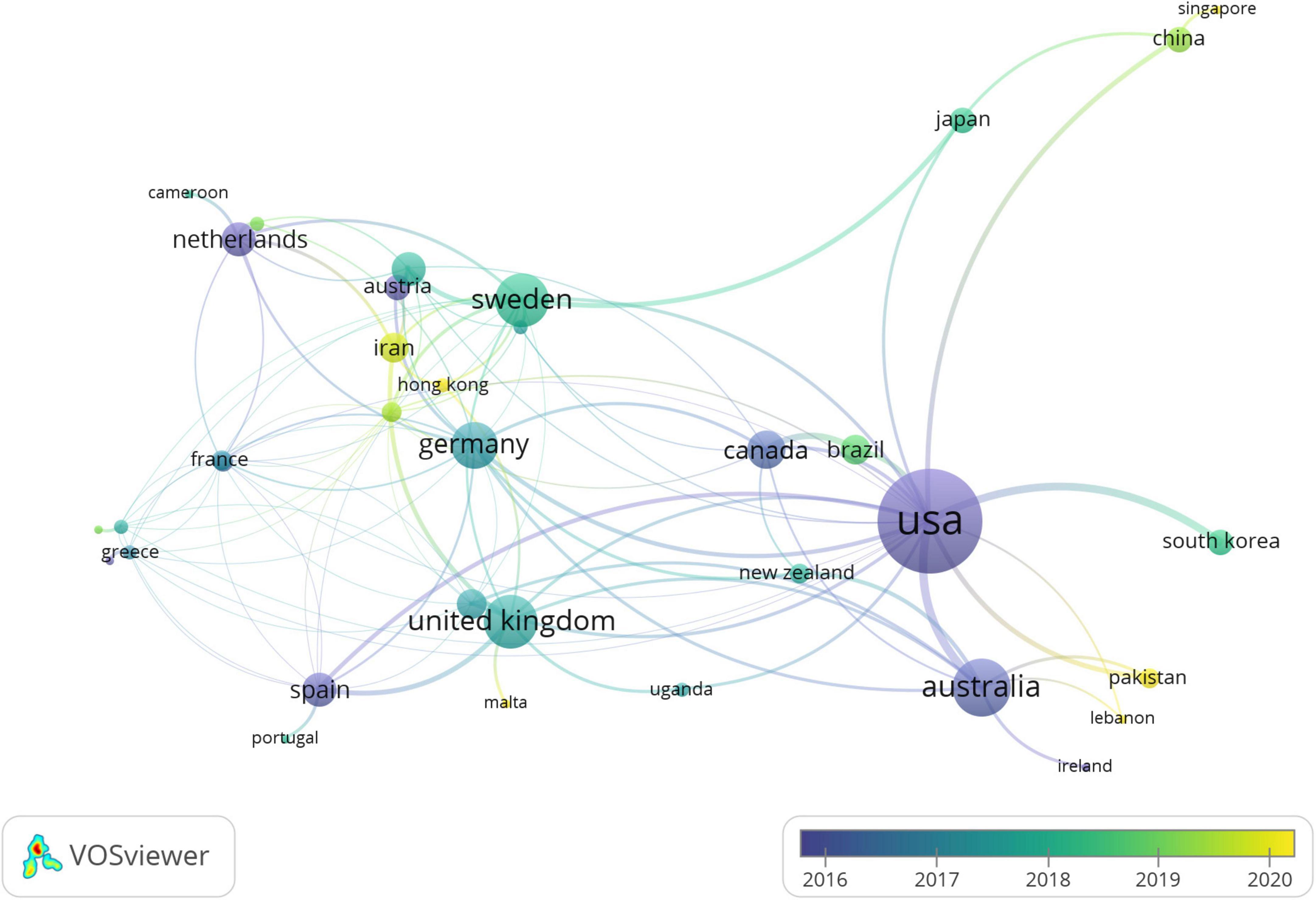
Figure 5. The country co-authorship network of heart diseases related publications over the time.
As shown in Table 2, the Patient Education and Counseling journal has published the highest number of papers, with 20 articles accounting for 5.15% of the total journals publishing about HL and heart diseases. In addition, articles in the Journal of General Internal Medicine had the highest number of citations per paper (53.58) and total citations (643).
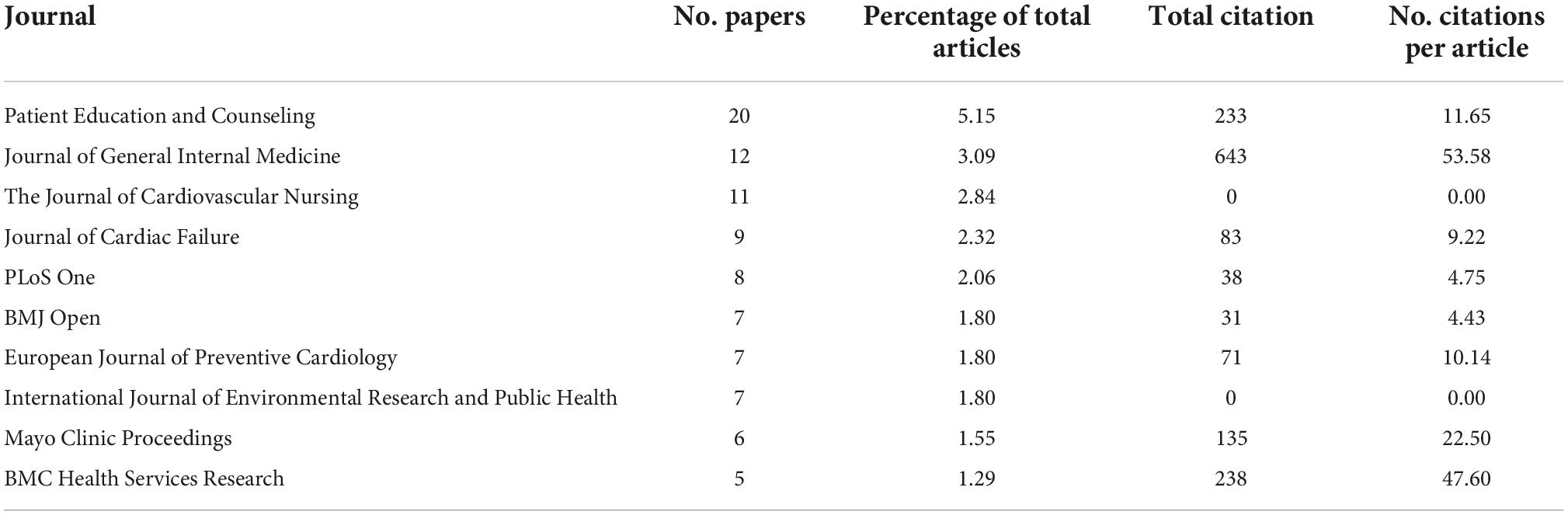
Table 2. Top 10 journals published health literacy articles related to heart diseases.
Figure 6 illustrates the network map of co-authorship. There were six different color clusters of close cooperation (with at least three papers). The thickness of the lines indicates the strength of the relationship. For example, Kripalani S. cooperated closely with Cawthon C., Rothman RL., Rothman R., Bachmann IM., and Bell SP (Red cluster). In addition to being in close contact with co-authors in the green cluster, DeWalt DA. frequently collaborated with Rothman R., Dracup K., etc. Our findings indicate that the two most prolific group of authors include Kripalani S. and colleagues (Green cluster in Figure 6) and DeWalt D.A. and colleagues (Red cluster in Figure 6). The first group mainly focuses on medical adherence (19–21), medication errors (22, 23) and health outcomes regarding mortality (24, 25) and readmission risk (26). On the other hand, DeWalt’s group mainly conducted research on the relationship between the HL and heart failure (27–29). Apart from the well-established research groups, there were emerging research teams (e.g., Plake Kimberly S., Albert Nancy M., Chen Aleda M.H.) who actively investigated the role of digital HL in cardiac outcomes (30–32).
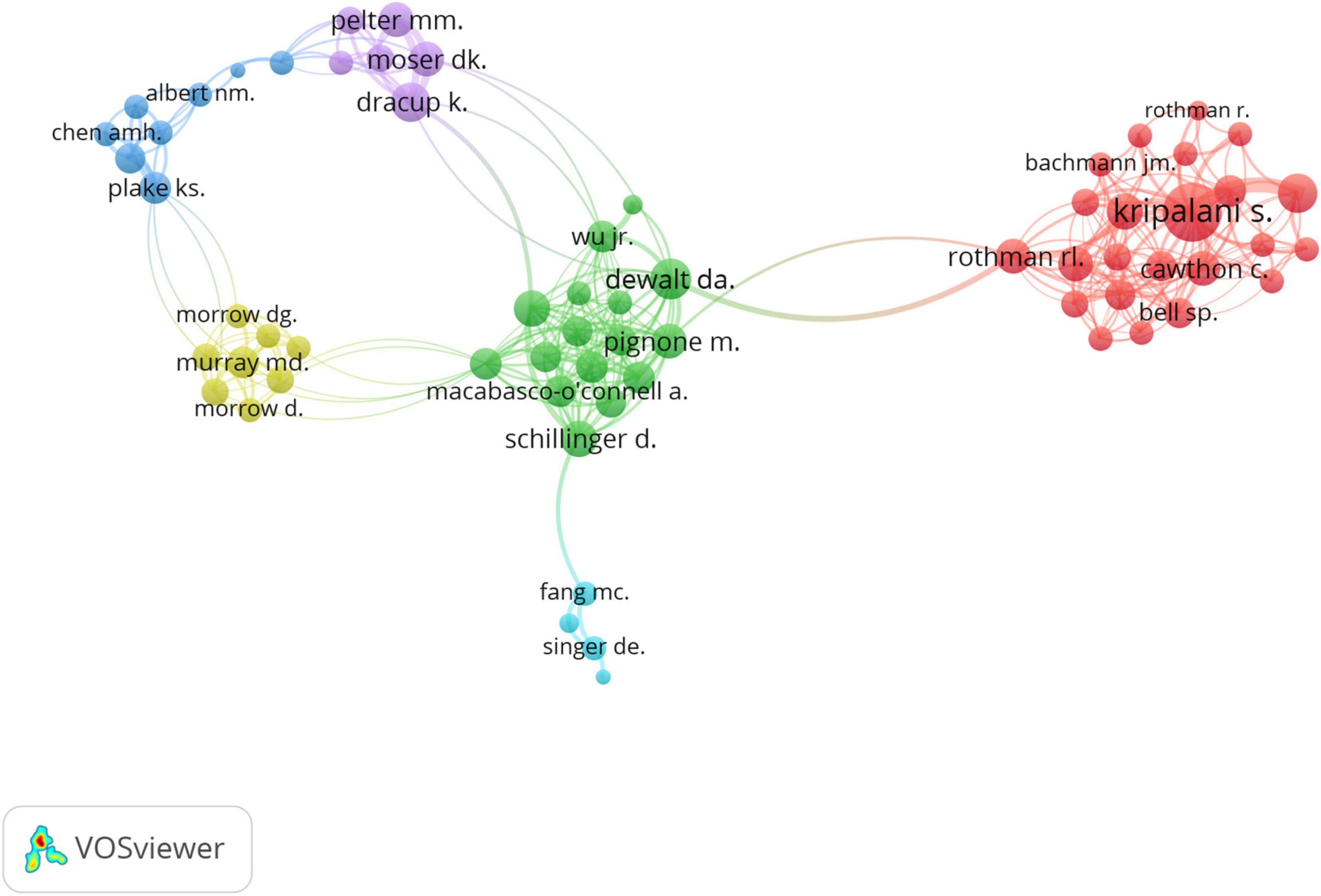
Figure 6. The distribution of co-authorship network.
Considering the co-authorship network between 2008 and 2016 (Figure 7), Morrow DG., Murray MD., and Morrow D. (in purple) have collaborated since 2008 in the HL research related to heart diseases. Moreover, Kripalani S. has joined this research field in the past few years and actively expanded his collaboration network with other authors.
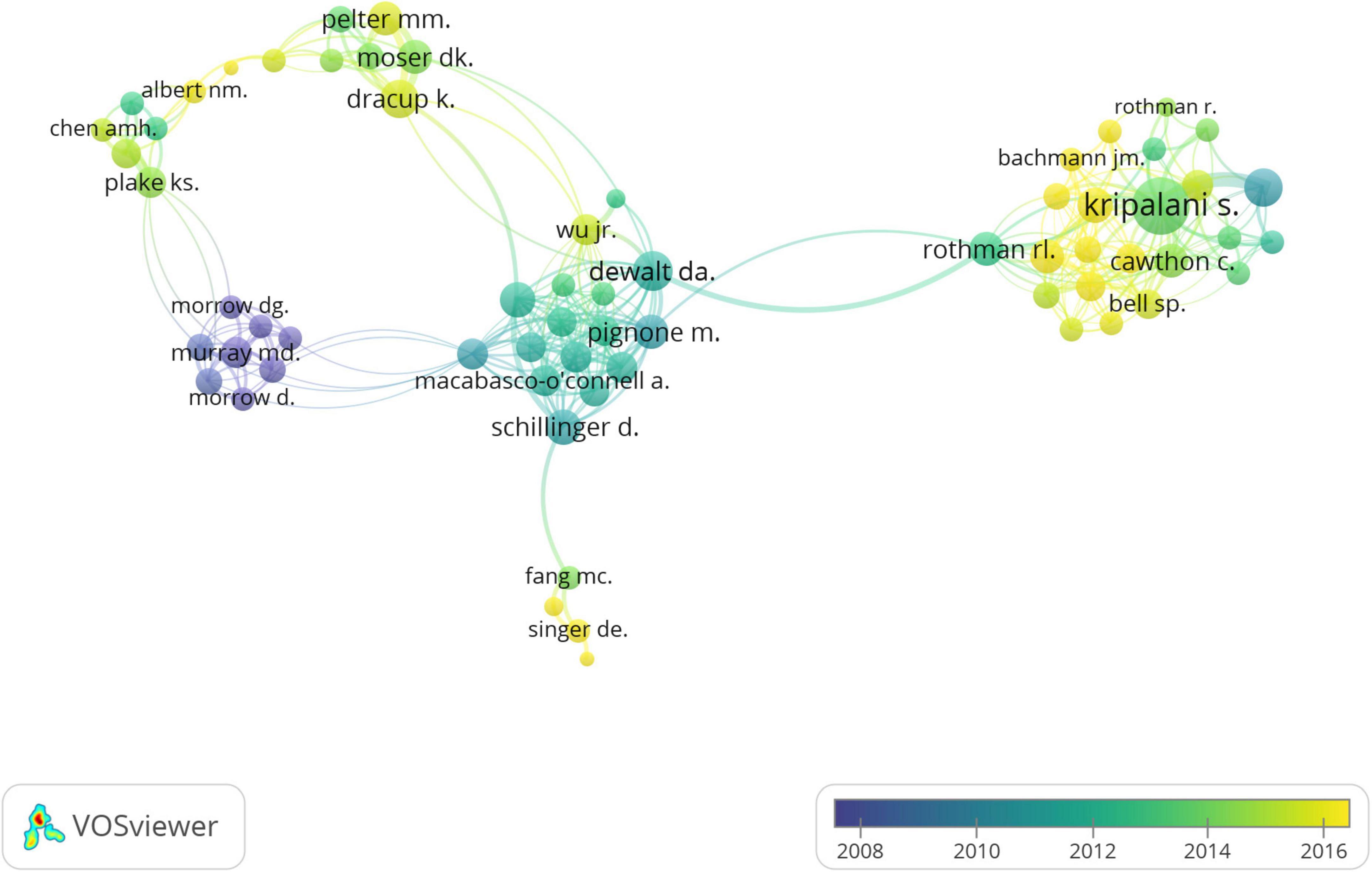
Figure 7. Distribution of co-authorship network over the time.
Figure 8 indicates that observational studies were a dominant study design between 2004 to 2021. The number of papers on qualitative studies, systematic reviews, and meta-analyses also increased steadily after 2010. Meanwhile, the number of interventional studies varied during this period of time and reached the peak in 2016 and 2019 with 7 to 8 articles, respectively.
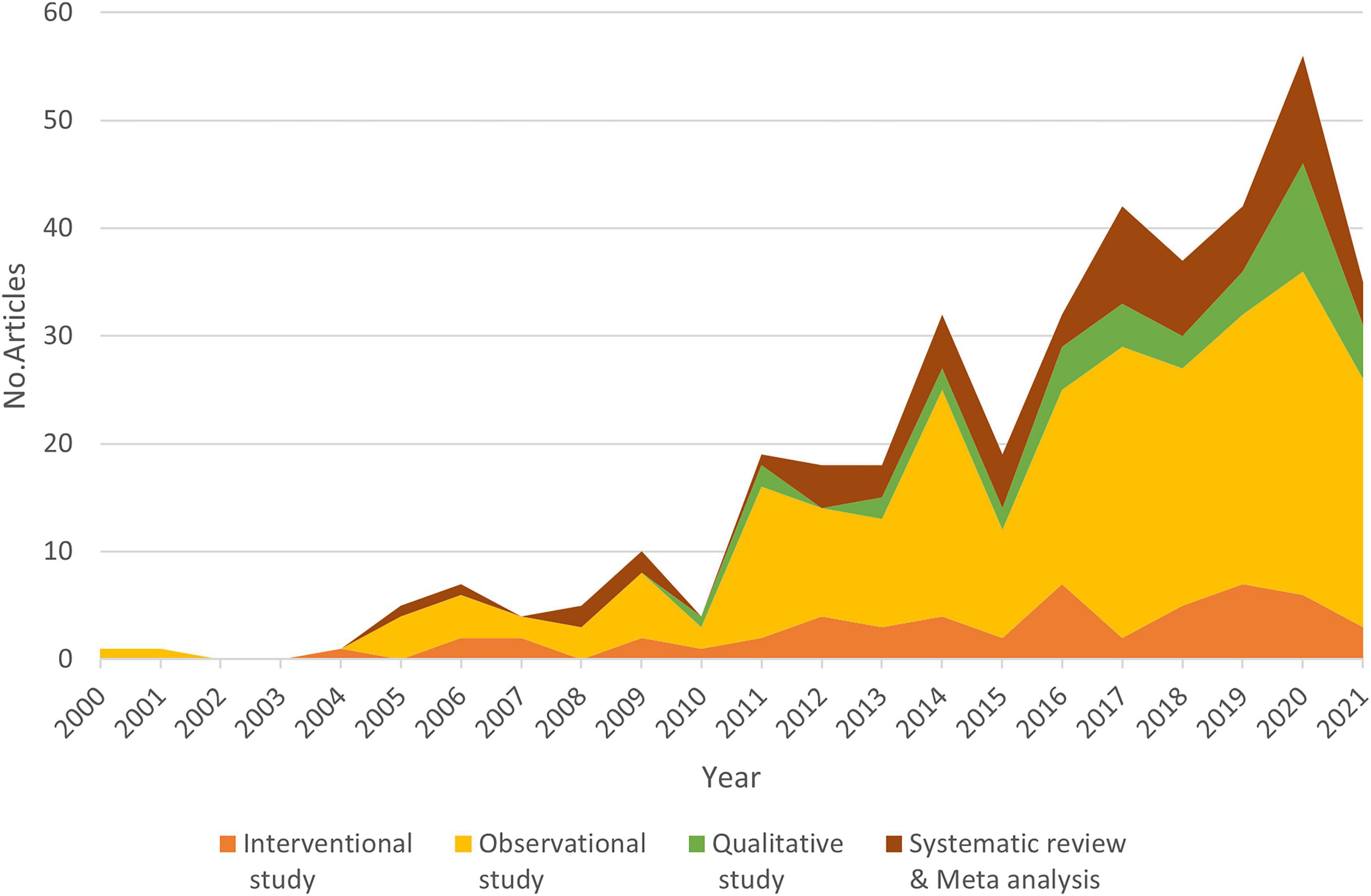
Figure 8. The distribution of papers classified by study design over the time.
Table 3 shows that among 20 countries, the United States had the highest number of papers (n = 202) and the number of papers utilizing an observational study design was the highest (125/202, 61.9%). Australia ranked second regarding the number of papers (n = 25). The number of papers from other countries; namely, Germany, the United Kingdom, South Korea, and China, ranged from 10 to 14. Meanwhile, Austria and New Zealand had the smallest number of papers (three papers for each).
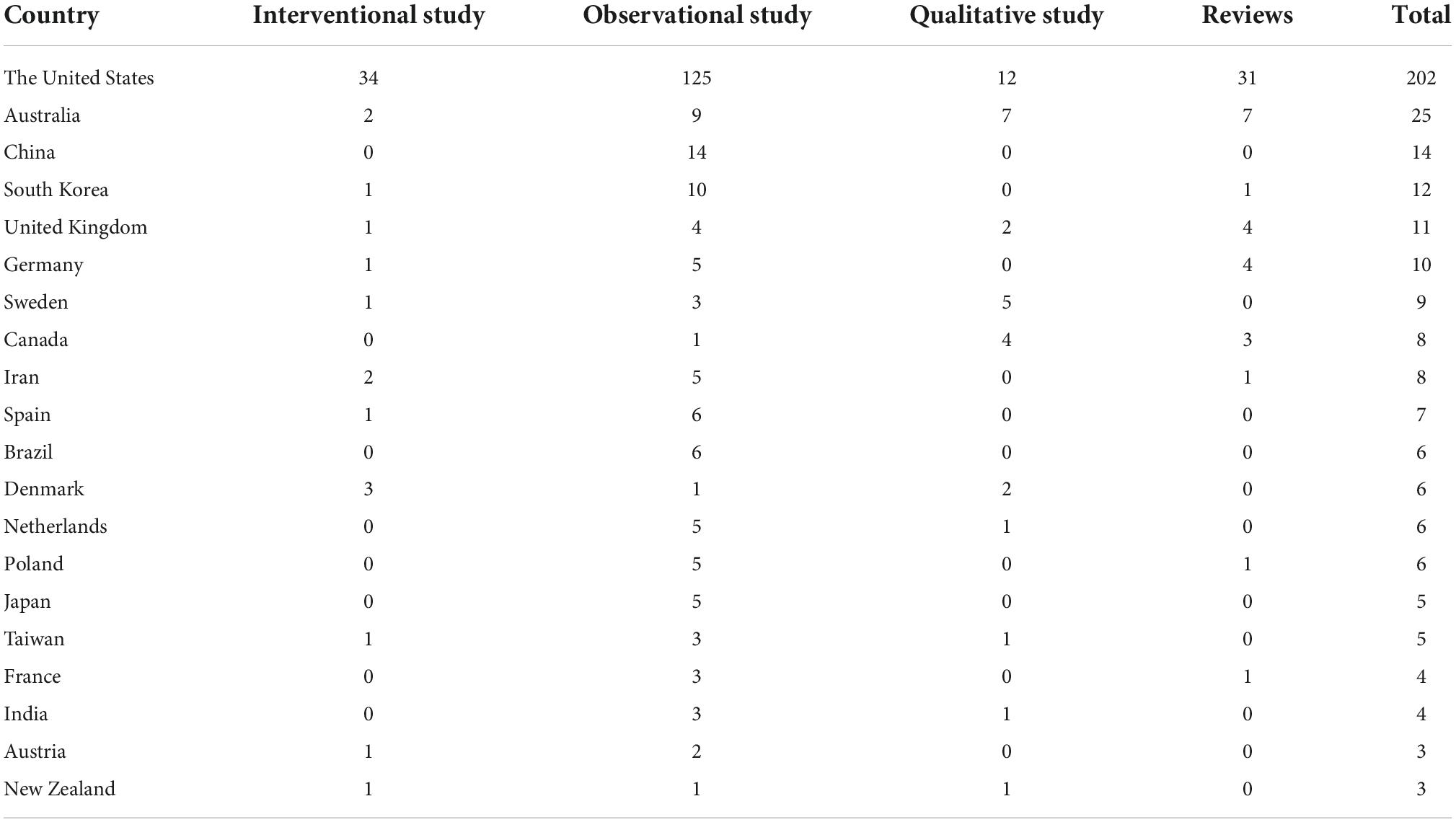
Table 3. The number of papers with different study designs in top 20 productive countries.
Table 4 presents the top six heart diseases investigated in the top 20 countries, including atrial fibrillation, cardiac valve disorders, congenital cardiac malformations, chronic rheumatic heart diseases, ischemic heart diseases, and heart failure. Among those, most were heart failure (189/388 articles, 48.7%), and the United States conducted the majority of studies (202/388, 52.0%).
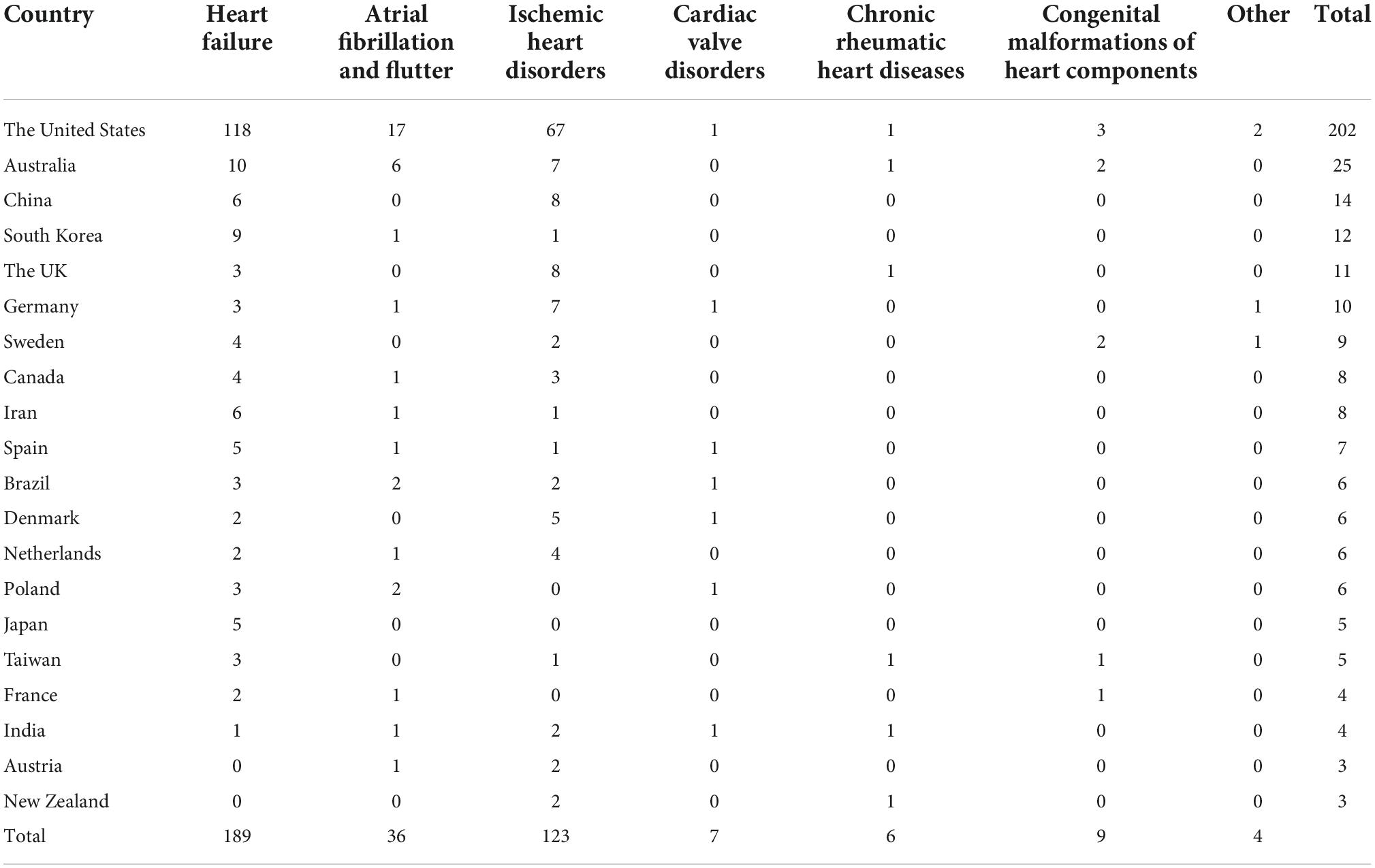
Table 4. Number of papers regarding six most common heart diseases in top 20 productive countries.
Supplementary Figure 1 presents the distribution of studies on different types of heart diseases. Heart failure and ischemic heart diseases accounted for the most significant number of publications over the study period. After 2015, HL research related to atrial fibrillation and flutter witnessed a considerable growth in publications, and the number of studies about congenital malformations or cardiac valvular diseases increased slightly.
Table 5 shows citation analysis across heart disease types. Ischemic heart diseases had the highest average citation per paper (10.52), followed by heart failure and atrial fibrillation diseases. Although ischemic heart diseases account for the highest mortality and morbidity burden (2,421 patients and 118 deaths per 100,000 inhabitants), heart failure is the focus of most publications related to HL globally (with over 50% publications).
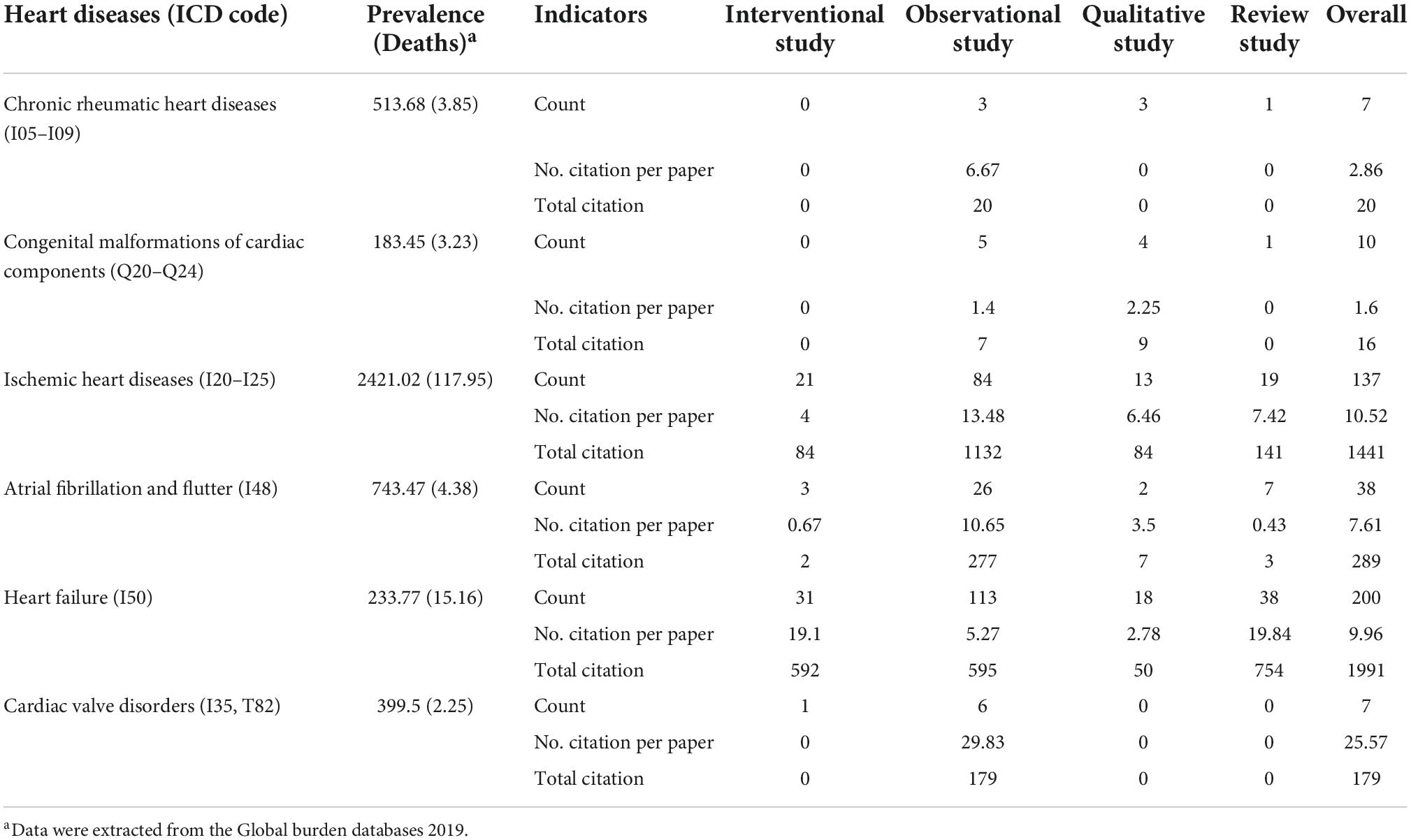
Table 5. Number of papers regarding six most popular heart diseases among different study design.
Figure 9 shows the distribution of HL questionnaire usage for different heart diseases and types of study designs. The results show that STOFHLA and TOFHLA were the two most popular questionnaires administered to measure HL among patients with varying heart conditions. Other popular questionnaires for HL measurement among cardiac patients included BHLS, REALM, and NVS. Apart from these widely validated questionnaires, many studies used self-developed questionnaires to study knowledge of a specific disease such as coronary heart disease (CHD). Only health literacy of patients with heart failure were assessed using validated instruments such as a questionnaire about self-care and heart failure and heart failure-specific health literacy scale. STOFHLA and TOFHLA were widely utilized in observation and intervention studies. BHLS and REALM were more likely to be used in observational studies rather than the interventional ones.
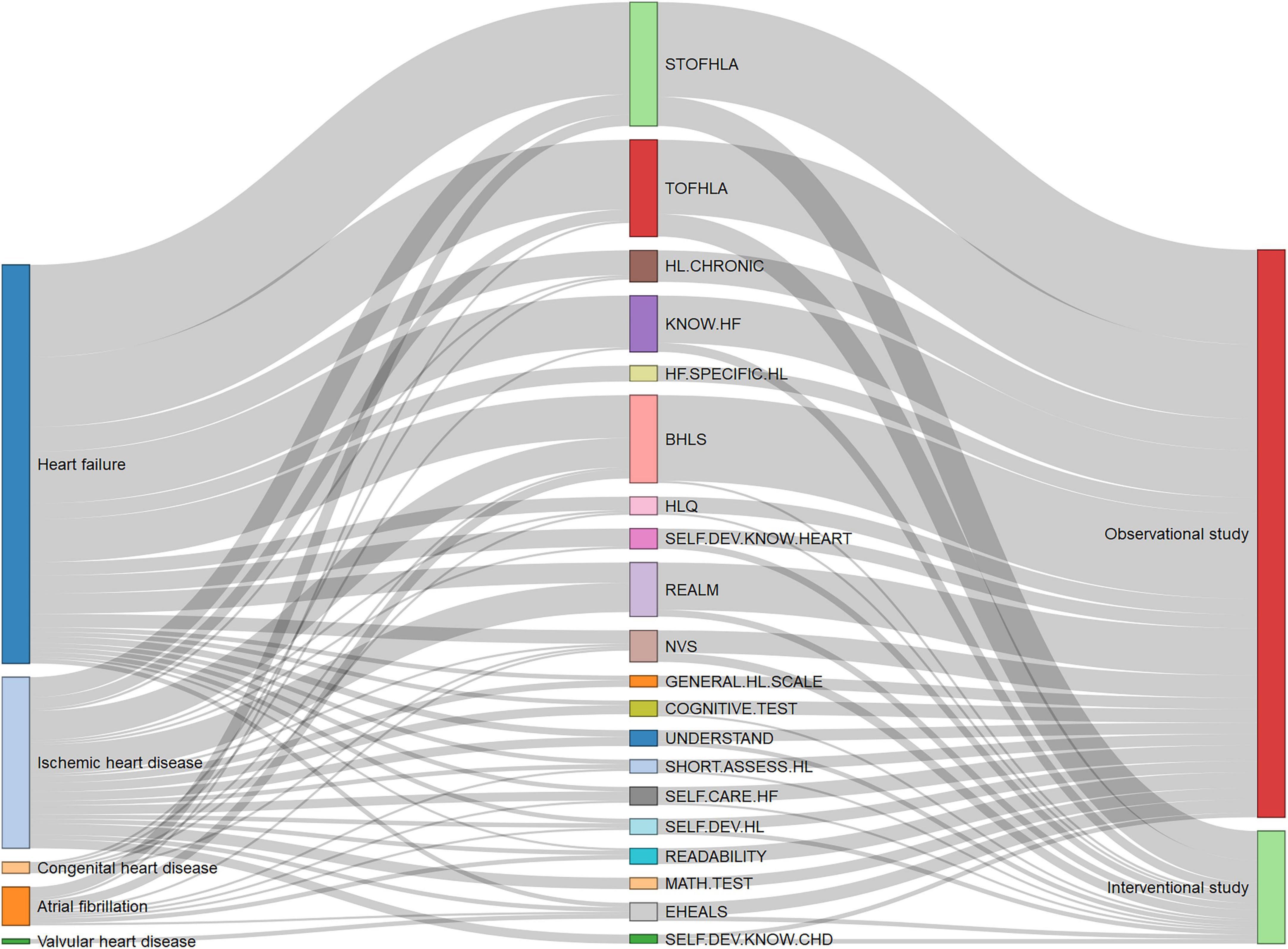
Figure 9. Distribution of health literacy (HL) instrument usage across heart diseases and type of study designs. BHLS, Brief Health Literacy Screen; COGNITIVE.TEST, Cognitive tests; EHEALS, eHealth literacy scale; GENERAL.HL.SCALE, General health literacy scale; HF.SPECIFIC.HL, Heart Failure-Specific Health Literacy Scale; HL.CHRONIC, Health Literacy in Patients with Chronic Diseases; HLQ, Health literacy questionnaire; KNOW.HF, Questionnaire about Heart Failure Patients Knowledge of Disease; MATH.TEST, Numeracy tests; NVS, Newest Vital Sign; READABILITY, Questionnaires about the readability of patient education materials; REALM, Rapid Estimate of Adult Literacy in Medicine; SELF.CARE.HF, Questionnaire about self-care and heart failure; SELF.DEV.HL, Self-developed questionnaires about health literacy; SELF.DEV.KNOW.CHD, Self-developed questionnaires about knowledge of coronary heart disease; SELF.DEV.KNOW.HEART, Self-developed questionnaires about knowledge of heart diseases; SHORT.ASSESS.HL, Short Assessment of Health Literacy; STOFHLA, Short Test of Functional Health Literacy in Adults; TOFHLA, Test of Functional Health Literacy in Adults; UNDERSTAND, Questionnaire about understandability.
Figure 10 indicates the frequency of questionnaire utilization and their citations over time. Before 2011, most studies on heart disease and HL utilized general HL questionnaires. A typical tool was the readability test of patient education materials, which has been used since the very beginning of the domain and continues to be applied in recent years. The other questionnaires, notably TOFHLA, STOFHLA, and REALM, have a long history and widespread use in HL research. Although general HL measures continued to dominate after 2011, the number of studies utilizing questions focused on cardiac illness increased significantly, primarily related to heart failure. The short versions of the HL scale also increased in recent years (e.g., BHLS, STOFHLA, short assessment HL, NVS). After 2017, there was notable growth in the number of studies focusing on digital HL, with increased usage of the EHEALS tool. The full list of questionnaires is available in Supplementary Figure 2.
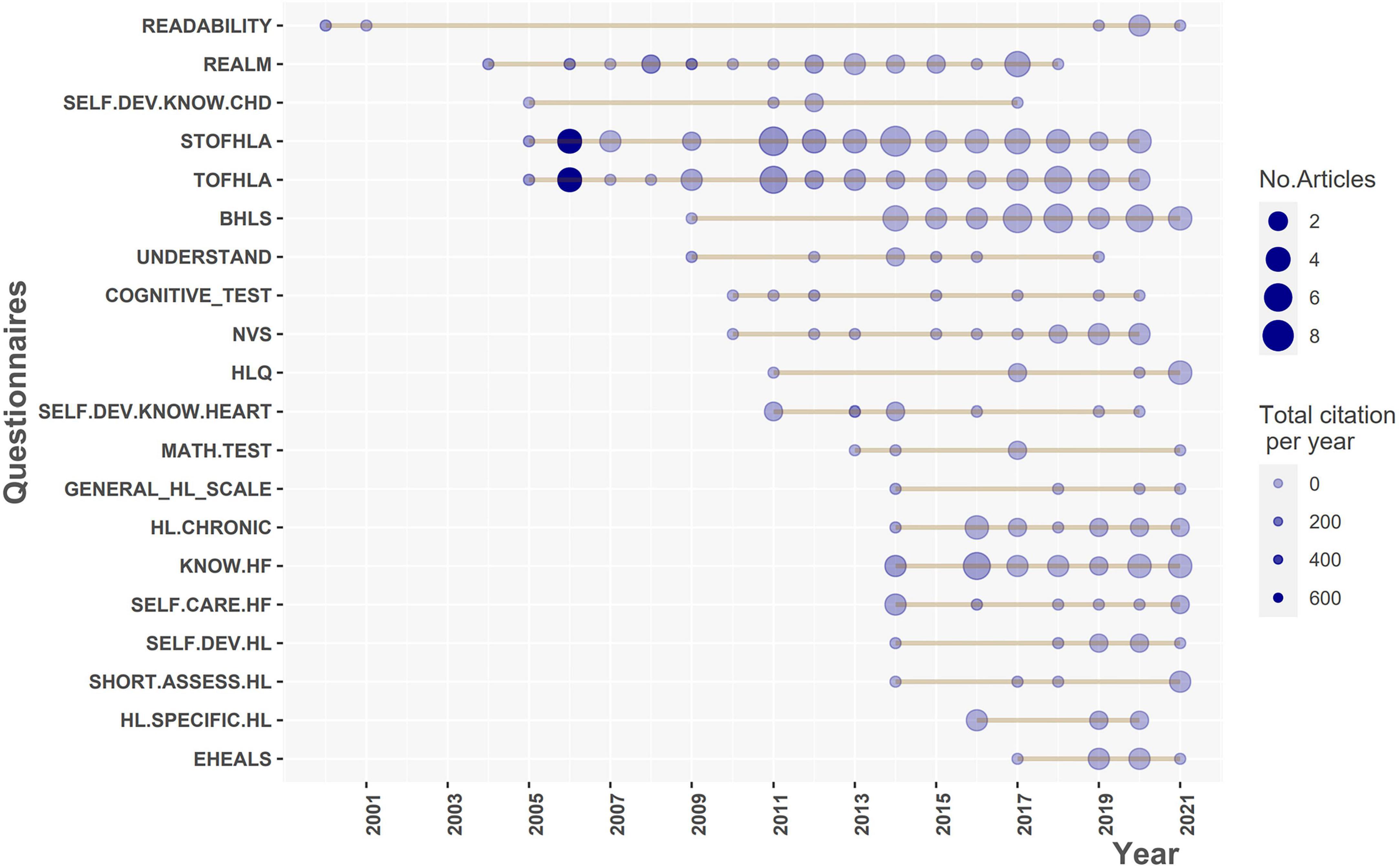
Figure 10. Top 20 questionnaires of health literacy (HL) used over the time. BHLS, Brief Health Literacy Screen; COGNITIVE.TEST, Cognitive tests; EHEALS, eHealth literacy scale; GENERAL.HL.SCALE, General health literacy scale; HF.SPECIFIC.HL, Heart Failure-Specific Health Literacy Scale; HL.CHRONIC, Health Literacy in Patients with Chronic Diseases; HLQ, Health literacy questionnaire; KNOW.HF, Questionnaire about Heart Failure Patients Knowledge of Disease; MATH.TEST, Numeracy tests; NVS, Newest Vital Sign; READABILITY, Questionnaires about the readability of patient education materials; REALM, Rapid Estimate of Adult Literacy in Medicine; SELF.CARE.HF, Questionnaire about self-care and heart failure; SELF.DEV.HL, Self-developed questionnaires about health literacy; SELF.DEV.KNOW.CHD, Self-developed questionnaires about knowledge of coronary heart disease; SELF.DEV.KNOW.HEART, Self-developed questionnaires about knowledge of heart diseases; SHORT.ASSESS.HL, Short Assessment of Health Literacy; STOFHLA, Short Test of Functional Health Literacy in Adults; TOFHLA, Test of Functional Health Literacy in Adults; UNDERSTAND, Questionnaire about understandability.
To our knowledge, this is the first bibliometric analysis of the evidence of HL related to cardiac diseases, which comprehensively includes systematic reviews, meta-analysis, interventional studies, and observational studies in the three largest databases (Web of Science, Scopus, and PubMed).
Our results show that the number of publications increased gradually over the study period and experienced significant growth after 2010. However, in 2021, the number of studies dropped significantly. A possible reason could be the influence of COVID-19 on research activities (33). The restriction on gatherings, workplace closures and internal movement restrictions might have created various challenges in conducting research projects. Observational studies were the dominant study design during the study period. In the latter phase of the study period, the number of interventional studies, systematic reviews, and meta-analyses witnessed an upward trend. Since the HL field has become more mature and gained more attention from different researchers and societies, the types of study designs have become more diverse.
The role of HL in cardiac disease has gained attention from global researchers (9). HL studies related to heart diseases have been investigated in 45 countries, with most studies carried out in developed countries. Of these, the United States made the largest contribution to this field, accounting for over 50% of the studies. Previous bibliometric research related to cardiac diseases also showed similar results, with the United States emerging as the most prolific country in research quantity (34, 35).
According to the results of the country’s collaboration network, we found that besides traditional collaborations among well-developed western countries (e.g., The United States, Australia, Canada, Netherlands), increasingly strong research networks among developing countries have been established in recent years, particular in Asia. This might be due to the fact that most Asian countries are in the second stage of a rapidly increasing cardiovascular diseases (CVD) epidemic (36). A recent study showed that the number of CVD deaths in Asia doubled (from 5.6 million to 10.8 million), and the proportion of CVD deaths in total deaths increased (from 23% to 35%) between 1990 and 2019 (36). In addition, there were increasing lifestyle-related risk factors (e.g., tobacco, hypertension, and obesity) (37).
In terms of authorship networks, we found that the largest research groups usually include the leading and most prolific authors in the field. Our findings support the idea that building up a large and strong co-authorship network is crucial for increasing the productivity of publications in the field (35).
In the present study, heart failure and ischemic heart diseases gained most researchers’ attention. These two diseases accounted for the highest prevalence and mortality rates in high-income countries where made the largest contribution to the structure of HL research related to heart diseases, meanwhile, the prevalence and mortality of rheumatic diseases and congenital heart diseases were much more popular in low-to-middle income countries (38). In addition, previous meta-analyses have shown that HL could influence self-care behaviors and other health outcomes among patients suffering from heart failure (39). Although the literature on chronic rheumatic heart disease and cardiac valve disorders was very limited, these kinds of diseases are creating the largest heart related health burdens on society, even larger than heart failure in low-to-middle income countries. The lack of evidence on the role of HL in heart diseases might be a barrier to improving and initiating new strategies for the prevention and advancement of treatments for cardiac diseases. We suggest that further study is necessary to clarify the role of HL in patients with these diseases.
Our findings indicate that TOFHLA, STOFHLA, and BHLS were the most common instruments used for measuring HL among patients with heart diseases. The TOFHLA was developed by Ruth M. Parker et al. in 1995, consisting of 67 questions (50-item reading comprehension and 17-item numerical ability test) (40). The questionnaire was frequently used to evaluate patients’ ability to read and understand information they often encounter in health care settings (40). In 1999, David W. Baker developed an abbreviated version of TOFHLA, including 40 questions, which reduced completion time by 10 min compared to TOFHLA (41). The short-form version (STOFHLA) has demonstrated comparable reliability and validity to the previous version but is more practical due to its shorter administration time and fewer complicated questions (41). The BHLS questionnaire was developed by Chew et al. to screen patients with inadequate HL (42). Since the instrument only includes three items, it can increase the feasibility of use in crowded clinical settings and quickly identify the patients who need special communication methods (42). Despite being developed in 2004, the number of research studies utilizing the BHLS increased significantly after 2015.
Interestingly, an increasing number of recent studies have been using HL questionnaires focused on heart diseases. A typical example is heart failure specific HL developed by Matsuoka et al. (43); this questionnaire includes 12 items measuring comprehensive HL initiated by World Health Organization (5, 44). Apart from the functional HL domain mainly focused on readability, the instrument added more questions to measure the ability to access information (communicative HL) and critically evaluate that information (critical HL) (44).
After 2017, a new trend in evaluation focused on the use of the eHealth Literacy Scale (EHEALS) among patients with heart diseases. The questionnaire was developed by Norman et al. to measure patients’ knowledge and perceived skills related to researching, criticizing, and adopting electronic health information related to health problems (45). Recent bibliometric research demonstrates that eHealth is becoming a trending issue, with the number of studies rapidly growing over the past 5 years, particularly during the COVID-19 epidemic (46). Therefore, further studies investigating the role of eHealth Literacy in specific heart diseases would be essential.
Our study had some limitations. First, we only included studies written in English; hence, we may have missed articles published in other languages. Second, we did not examine the quality of methodological studies. Since there are various types of research designs with different subtypes, it would be challenging to identify a standard and universal method for evaluating the quality of various study designs. However, further analysis of quality would be useful in a future study. Our research did not include all databases, such as Embase and clinical trials. It is therefore possible that we missed some studies published in these databases.
Comparison with prior work, our study has some outstanding strengths. We included the three most popular published databases: PubMed, Web of Science, and Scopus. Therefore, our results are more inclusive as compared to prior studies, which focused on only one of the aforementioned databases (34, 35, 46). To our knowledge, this is the first study to provide a comprehensive picture of the HL tools used in observational and interventional studies related to heart diseases. Knowing which instruments are most often used in HL would be useful to find and select the appropriate tool for research related to cardiac diseases. In addition, researchers might update the latest research instruments with more specificity for different purposes or diseases based on the historical and frequent usage of HL tools.
Based on our findings, we conclude that apart from two common heart diseases (heart failure and heart ischemic diseases), it is necessary to carry out more research on other types of heart diseases (including valvular disorders and rheumatic disorders). The number of interventions studies is limited and fluctuated over the study period. More HL intervention research would be beneficial to provide initiatives in improving outcomes of heart disease treatment and management. Finally, development of HL scales for different types of heart diseases would also be essential to further research in this area.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding authors.
Ethical review and approval was not required for this study in accordance with the local legislation and institutional requirements. Written informed consent was not required for this study in accordance with the local legislation and institutional requirements.
LH, TD, and S-HY designed the research. LH, TD, S-HY, LD, NT, and NH conducted the literature review. LH, NT, NH, NN, TN, and LD collected the primary data. LH, TD, S-HY, Y-HH, and EC analyzed and visualized the data. NT, NH, NN, Y-MC, Y-HH, C-CH, and C-LS screened out the irregular literature. LH, TD, NT, NH, NN, TN, LD, and S-HY wrote the original draft. LH, TD, C-CH, Y-MC, C-LS, Y-HH, and EC reviewed and revised the manuscript. All authors contributed to the article and approved the submitted version.
This study was supported by the National Science and Technology Council, Taiwan (MOST 111-2923-H-038-001-MY2).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.1012531/full#supplementary-material
1. Roth GA, Mensah GA, Johnson CO, Addolorato G, Ammirati E, Baddour LM, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. (2020) 76:2982–3021. doi: 10.1016/j.jacc.2020.11.010
2. Graham I. European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Atherosclerosis. (2007) 194:1–45. doi: 10.1016/j.atherosclerosis.2007.08.024
3. Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice: developed by the task force for cardiovascular disease prevention in clinical practice with representatives of the European society of cardiology and 12 medical societies with the special contribution of the European association of preventive cardiology (EAPC). Eur Heart J. (2021) 42:3227–337. doi: 10.1093/eurheartj/ehab484
4. Sudore RL, Schillinger D. Interventions to improve care for patients with limited health literacy. J Clin Outcomes Manag. (2009) 16:20–9.
5. Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promot Int. (2000) 15:259–67. doi: 10.1093/heapro/15.3.259
6. Simonds SK. Health education as social policy. Health Educ Monogr. (1974) 2:1–10. doi: 10.1177/10901981740020S102
7. Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. (HLS-EU) Consortium health literacy project european. health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. (2012) 12:80. doi: 10.1186/1471-2458-12-80
8. Kanejima, Y, Shimogai T, Kitamura M, Ishihara K, Izawa KP. Impact of health literacy in patients with cardiovascular diseases: a systematic review and meta-analysis. Patient Educ Couns. (2021) 105:1793–800. doi: 10.1016/j.pec.2021.11.021
9. Magnani JW, Mujahid MS, Aronow HD, Cené CW, Dickson VV, Havranek E, et al. Health literacy and cardiovascular disease: fundamental relevance to primary and secondary prevention: a scientific statement from the American Heart Association. Circulation. (2018) 138:e48–74. doi: 10.1161/CIR.0000000000000579
10. Schaefer CT. Integrated review of health literacy interventions. Orthop Nurs. (2008) 27:302–17. doi: 10.1097/01.NOR.0000337283.55670.75
11. Donthu N, Kumar S, Mukherjee D, Pandey N, Lim WM. How to conduct a bibliometric analysis: an overview and guidelines. J Bus Res. (2021) 133:285–96. doi: 10.1016/j.jbusres.2021.04.070
12. Fan J, Gao Y, Zhao N, Dai R, Zhang H, Feng X, et al. Bibliometric analysis on COVID-19: a comparison of research between English and Chinese studies. Front Public Health. (2020) 8:477. doi: 10.3389/fpubh.2020.00477
13. Tavousi M, Mohammadi S, Sadighi J, Zarei F, Kermani RM, Rostami R, et al. Measuring health literacy: a systematic review and bibliometric analysis of instruments from 1993 to 2021. PLoS One. (2022) 17:e0271524. doi: 10.1371/journal.pone.0271524
14. World Health Organization [WHO]. ICD-10 Version:2019. (2019). Available online at: https://icd.who.int/browse10/2019/en#/ (accessed June 12, 2022).
15. Aria M, Cuccurullo C. bibliometrix?: an R-tool for comprehensive science mapping analysis. J Informetr. (2017) 11:959–75. doi: 10.1016/j.joi.2017.08.007
16. Moher D, Liberati A, Tetzlaff J, Altman DG, The Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
17. van Eck NJ, Waltman L. Software survey: VOSviewer, a computer program for bibliometric mapping. Scientometrics. (2010) 84:523–38. doi: 10.1007/s11192-009-0146-3
18. Fonseca BPF, Sampaio RB, Fonseca MVA, Zicker F. Co-authorship network analysis in health research: method and potential use. Health Res Policy Syst. (2016) 14:34. doi: 10.1186/s12961-016-0104-5
19. Kripalani S, Gatti ME, Jacobson TA. Association of age, health literacy, and medication management strategies with cardiovascular medication adherence. Patient Educ Couns. (2010) 81:177–81. doi: 10.1016/j.pec.2010.04.030
20. Risser J, Jacobson TA, Kripalani S. Development and psychometric evaluation of the self-efficacy for appropriate medication use scale (SEAMS) in low-literacy patients with chronic disease. J Nurs Meas. (2007) 15:203–19. doi: 10.1891/106137407783095757
21. Kripalani S, Schmotzer B, Jacobson TA. Improving medication adherence through graphically enhanced interventions in coronary heart disease (IMAGE-CHD): a randomized controlled trial. J Gen Intern Med. (2012) 27:1609–17. doi: 10.1007/s11606-012-2136-z
22. Mixon AS, Myers AP, Leak CL, Lou Jacobsen JM, Cawthon C, Goggins KM, et al. Characteristics associated with postdischarge medication errors. Mayo Clinic Proc. (2014) 89:1042–51. doi: 10.1016/j.mayocp.2014.04.023
23. Kripalani S. Effect of a pharmacist intervention on clinically important medication errors after hospital discharge: a randomized trial. Ann Intern Med. (2012) 157:1. doi: 10.7326/0003-4819-157-1-201207030-00003
24. Roumie CL, Patel NJ, Muñoz D, Bachmann J, Stahl A, Case R, et al. Design and outcomes of the patient centered outcomes research institute coronary heart disease cohort study. Contemp Clin Trials Commun. (2018) 10:42–9. doi: 10.1016/j.conctc.2018.03.001
25. Mayberry LS, Schildcrout JS, Wallston KA, Goggins K, Mixon AS, Rothman RL, et al. Health literacy and 1-year mortality: mechanisms of association in adults hospitalized for cardiovascular disease. Mayo Clinic Proc. (2018) 93:1728–38. doi: 10.1016/j.mayocp.2018.07.024
26. Sterling MR, Safford MM, Goggins K, Nwosu SK, Schildcrout JS, Wallston KA, et al. Numeracy, health literacy, cognition, and 30-day readmissions among patients with heart failure. J Hosp Med. (2018) 13:145–51. doi: 10.12788/jhm.2932
27. DeWalt DA, Pignone M, Malone R, Rawls C, Kosnar MC, George G, et al. Development and pilot testing of a disease management program for low literacy patients with heart failure. Patient Educ Couns. (2004) 55:78–86. doi: 10.1016/j.pec.2003.06.002
28. Wu J-R, DeWalt DA, Baker DW, Schillinger D, Ruo B, Bibbins-Domingo K, et al. A single-item self-report medication adherence question predicts hospitalisation and death in patients with heart failure. J Clin Nurs. (2014) 23:2554–64. doi: 10.1111/jocn.12471
29. DeWalt DA, Malone RM, Bryant ME, Kosnar MC, Corr KE, Rothman RL, et al. A heart failure self-management program for patients of all literacy levels: a randomized, controlled trial [ISRCTN11535170]. BMC Health Serv Res. (2006) 6:30. doi: 10.1186/1472-6963-6-30
30. Chen AMH, Yehle KS, Albert NM, Ferraro KF, Mason HL, Murawski MM, et al. Health literacy influences heart failure knowledge attainment but not self-efficacy for self-care or adherence to self-care over time. Nurs Res Pract. (2013) 2013:353290. doi: 10.1155/2013/353290
31. Chen AMH, Yehle KS, Plake KS, Rathman LD, Heinle JW, Frase RT, et al. The role of health literacy, depression, disease knowledge, and self-efficacy in self-care among adults with heart failure: an updated model. Heart Lung. (2020) 49:702–8. doi: 10.1016/j.hrtlng.2020.08.004
32. Chen AMH, Yehle KS, Albert NM, Ferraro KF, Mason HL, Murawski MM, et al. Relationships between health literacy and heart failure knowledge, self-efficacy, and self-care adherence. Res Soc Admin Pharm. (2014) 10:378–86. doi: 10.1016/j.sapharm.2013.07.001
33. Weiner DL, Balasubramaniam V, Shah SI, Javier JR. COVID-19 impact on research, lessons learned from COVID-19 research, implications for pediatric research. Pediatr Res. (2020) 88:148–50. doi: 10.1038/s41390-020-1006-3
34. Yeung AWK, Kulnik ST, Parvanov ED, Fassl A, Eibensteiner F, Völkl-Kernstock S, et al. Research on digital technology use in cardiology: bibliometric analysis. J Med Int Res. (2022) 24:e36086. doi: 10.2196/36086
35. Manyangu G, Dineen B, Geoghegan R, Flaherty G. Descriptive bibliometric analysis of global publications in lifestyle-based preventive cardiology. Eur J Prev Cardiol. (2021) 28:1303–14. doi: 10.1177/2047487319854827
36. Zhao D. Epidemiological features of cardiovascular disease in Asia. JACC Asia. (2021) 1:1–13. doi: 10.1016/j.jacasi.2021.04.007
37. Martinez-Amezcua P, Haque W, Khera R, Kanaya AM, Sattar N, Lam CSP, et al. The upcoming epidemic of heart failure in South Asia. Circ Heart Fail. (2020) 13:e007218. doi: 10.1161/CIRCHEARTFAILURE.120.007218
38. Leggiadro RJ. Global, regional and national burden of rheumatic heart disease, 1990–2015. Pediatr Infect Dis J. (2017) 36:1155. doi: 10.1097/INF.0000000000001805
39. Cajita MI, Cajita TR, Han H-R. Health literacy and heart failure. J Cardiovasc Nurs. (2016) 31:121–30. doi: 10.1097/JCN.0000000000000229
40. Parker RM, Baker DW, Williams MV, Nurss JR. The test of functional health literacy in adults. J Gen Intern Med. (1995) 10:537–41. doi: 10.1007/BF02640361
41. Baker DW, Williams MV, Parker RM, Gazmararian JA, Nurss J. Development of a brief test to measure functional health literacy. Patient Educ Couns. (1999) 38:33–42. doi: 10.1016/S0738-3991(98)00116-5
42. Chew LD, Bradley KA, Boyko EJ. Brief questions to identify patients with inadequate health literacy. Fam Med. (2004) 36:588–94.
43. Matsuoka S, Kato N, Kayane T, Yamada M, Koizumi M, Ikegame T, et al. Development and validation of a heart failure-specific health literacy scale. J Cardiovasc Nurs. (2016) 31:131–9. doi: 10.1097/JCN.0000000000000226
44. Ishikawa H, Takeuchi T, Yano E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care. (2008) 31:874–9. doi: 10.2337/dc07-1932
45. Norman CD, Skinner HA. eHEALS: the eHealth literacy scale. J Med Int Res. (2006) 8:e27. doi: 10.2196/jmir.8.4.e27
Keywords: heart diseases, health literacy, bibliometric analysis, instruments, heart failure, ischemic heart diseases
Citation: Huy LD, Truong NLT, Hoang NY, Nguyen NTH, Nguyen TTP, Dang LT, Hsu Y-HE, Huang C-C, Chang Y-M, Shih C-L, Carbone ET, Yang S-H and Duong TV (2022) Insight into global research on health literacy and heart diseases: A bibliometric analysis. Front. Cardiovasc. Med. 9:1012531. doi: 10.3389/fcvm.2022.1012531
Received: 05 August 2022; Accepted: 10 November 2022;
Published: 24 November 2022.
Edited by:
Gen-Min Lin, Hualien Armed Forces General Hospital, TaiwanReviewed by:
Thereza Maria Magalhães Moreira, State University of Ceará, BrazilCopyright © 2022 Huy, Truong, Hoang, Nguyen, Nguyen, Dang, Hsu, Huang, Chang, Shih, Carbone, Yang and Duong. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shwu-Huey Yang, c2hlcnJ5QHRtdS5lZHUudHc=; Tuyen V. Duong, dHZkdW9uZ0B0bXUuZWR1LnR3
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.