
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cardiovasc. Med. , 23 November 2022
Sec. Hypertension
Volume 9 - 2022 | https://doi.org/10.3389/fcvm.2022.1001878
This article is part of the Research Topic Blood Pressure in Children and Adolescents: Moving forward View all 10 articles
 Stella Stabouli1*†
Stella Stabouli1*† Athanasia Chainoglou1†
Athanasia Chainoglou1† Kleo Evripidou1Carla Simão2Christina Antza3
Kleo Evripidou1Carla Simão2Christina Antza3 Panagiotis Petrou4Gilad Hamdani5Javier Calpe6
Panagiotis Petrou4Gilad Hamdani5Javier Calpe6 Empar Lurbe7
Empar Lurbe7Accuracy of blood pressure (BP) measurement is important for the evaluation of hypertension in children and adolescents, and it is critically dependent upon the accuracy of the BP measuring device. A device that could pass validated protocols with reliable accuracy would be desirable in clinical and research settings. Several scientific organizations have published recommendations on the validation of different BP measuring devices. Most of them focus on adults but separate recommendations and validation criteria for BP devices intended for use in children and adolescents are included in some validation protocols. In this review, we compare the validation criteria for BP measuring devices among consensus documents from different scientific organizations focusing on the pediatric population and we discuss the evidence gaps targeting the needs for validated BP measuring devices in children and adolescents. We also highlight common pitfalls in the validation studies of BP measuring devices in children and adolescents using the example of office BP devices.
Accuracy of blood pressure (BP) measurement is important for the evaluation of hypertension in children and adolescents, and it is critically dependent upon the accuracy of the BP measuring device. The need for evaluation of the accuracy of automated BP measuring devices available in the market, both for use in clinical settings, as well as out-of-office environment, using validation procedures has been well-recognized by the scientific community and the manufacturers (1). A device that can pass validated protocols with reliable accuracy would be desirable in clinical and research settings.
Several scientific organizations have published consensus documents on the validation of BP measuring devices. First, in 1987, the American Association for the Advancement of Medical Instrumentation (AAMI) published a monograph on clinical validation procedures for automated BP monitors, which was recognized as a national standard in the United States (2). This protocol was subsequently revised in 1992 and 2002. In 1990, the British Hypertension Society (BHS) published another validation protocol for BP monitors, which was revised in 1993 (3, 4). The German Hypertension League (DHL) developed its own Quality Seal Protocol in 1999 (5), and in 2002, the European Society of Hypertension (ESH) introduced the ESH-International Protocol (ESH-IP) that was revised in 2010 (ESH-IP2) (6, 7). In 2009, the International Organization for Standardization (ISO) published its own protocol (8) and in 2013 the American National Standards Institute (ANSI), the AAMI, and the ISO collaboratively released a revised protocol (9). Finally, in 2018, the AAMI/ESH/ISO released the most recent validation protocol in an effort to develop a single universal protocol for the validation of BP monitors (10).
Most of the validation protocols are developed only for adults and children are regarded as a special population requiring separate validation studies. The main objective of these consensus statements was to provide practical guidance for validation studies of BP measuring devices and to ensure that conditions are fulfilled, and data are reported in detail. Still, despite previous and current recommendations performing and reporting on validation studies present significant limitations. The pitfalls are more pronounced when the validation studies are performed in children and adolescents (11).
In this review, we compared the validation criteria for BP measuring devices among the consensus documents from scientific organizations focusing on the pediatric population and we discuss the gaps in evidence targeting the needs for validated BP devices in children and adolescents. We also highlight common pitfalls in the validation studies of BP measuring devices in children and adolescents using the example of office BP devices.
The basic differences between the validation protocols are summarized in Table 1 and include the following key features:
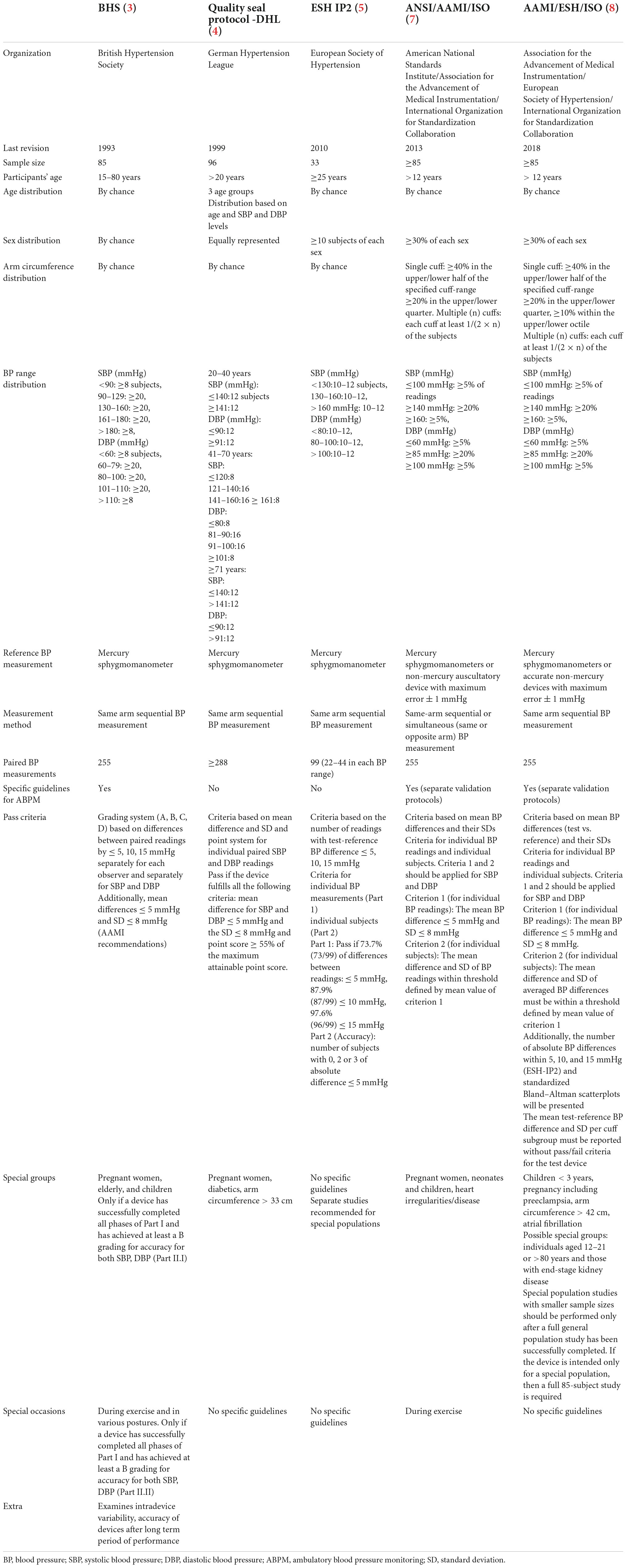
Table 1. Comparison of validation protocols for blood pressure (BP) measuring devices.
A major difference between protocols is that the ESH-IP2 is the only one that requires a smaller sample size of 33 individuals instead of 85 and 96 individuals that the other protocols require.
Most of the protocols are designed for adults, whereas the ANSI/AAMI/ISO and the AAMI/ESH/ISO include children older than 12 years.
In all protocols, the inclusion criteria for the participants vary in regard to their age, sex, arm circumference, and entry BP distribution. The sample is distributed based on age only in DHL, whereas in the others the distribution is random. Most of the protocols, except from the BHS, include participants selected with sex criteria. Only the ANSI/AAMI/ISO and AAMI/ESH/ISO protocols use sample that is selected according to the arm circumference. Finally, all protocols use BP range as a criterion for the selection of the subjects.
All protocols endorse the same-arm sequential measurement as the most accurate method except for the ANSI/AAMI/ISO, which suggest alternatively the same or the opposite arm simultaneous BP measurement procedure.
In the BHS, DHL, and ESH protocols, the recommended reference BP measurement device is a mercury sphygmomanometer, whereas the protocols of ANSI/AAMI/ISO and AAMI/ESH/ISO suggest alternatively the use of other non-mercury devices with a maximum error of 1 mmHg.
Different pass criteria have been used in all the protocols. The DHL, AANSI/AAMI/ISO, and AAMI/ESH/ISO criteria are based on calculating the mean difference and the standard deviation (SD) between the test and the reference BP measuring devices. The DHL has used additionally a point system scoring. On the other hand, the BHS and the ESH-IP2 criteria are based on summing up the cumulative incidence of the difference between the test and the reference BP devices in the categories of less than 5, 10, and 15 mmHg.
Only the BHS, ANSI/AAMI/ISO and the AAMI/ESH/ISO protocols highlight the need of separate validation studies for ABPM.
The BHS includes specific guidelines for the validation of BP devices in special occasions, such as during exercise and in different postures, whereas the AAMI provides recommendations for the validation of BP monitors only during exercise.
All the protocols recognize that BP devices should be validated in special populations and provided specific recommendations for these groups except for ESH-IP2 that recommends separate studies to be carried out.
Finally, the BHS protocol is the only one that tests the intradevice variability and the consistency in the performance of the BP monitor after prolonged use.
The recommendations for validation of BP measurement devices are mainly “tailor made” for adults. Although some organizations have addressed the validation in special populations including children, they mostly consider children as “small adults” and do not take into account several distinct characteristics of the pediatric population. Finally, most of the documents on the validation of BP measuring devices have included in the writing committees only adult hypertension specialists putting less emphasis on this special population. Given that the scientific evidence beyond the recommendations is limited and all organizations provide consensus documents the lack of statements on the validation of BP measuring devices specifically addressing to the unique characteristics and needs of children and adolescents by specialists and practitioners caring exclusively for pediatric patients gains extreme importance as a fundamental step for accurate and reliable BP measuring devices in the pediatric population.
The BHS, ANSI/AMI/ISO, and AAMI/ESH/ISO are the only protocols, which include specific recommendations for the validation of BP measuring devices in children (3, 9, 10) (Table 2). According to BHS, a sample of 30 children aged 5–15 years with specific inclusion criteria for their age, sex, and entry BP distribution is required (3). Afterwards, the mean BP difference and SD between test and reference device measurements should be reported without specified pass criteria. The ANSI/AMI/ISO and AAMI/ESH/ISO protocols share the same principles (9, 10). If the device is intended for use on both adults and children, the sample should consist of 35 children aged 3–12 years and 50 individuals aged older than 12 years. On the other hand, if the device is intended only for the use on children, a study with a sample of 85 children with specific criteria for sex and cuff size distribution should be carried out. According to the protocols, the studies should meet both two criteria for BP differences of individual readings and of individual subjects. The criterion 1 defines that the mean BP difference (test minus reference BP for all of the measurements) must be 5 mmHg or less, and its SD 8 mmHg or less for systolic and diastolic BP and the criterion 2 that the SD of averaged BP differences (test minus reference BP per subject) must be within a threshold defined by the mean of criterion 1 (9).
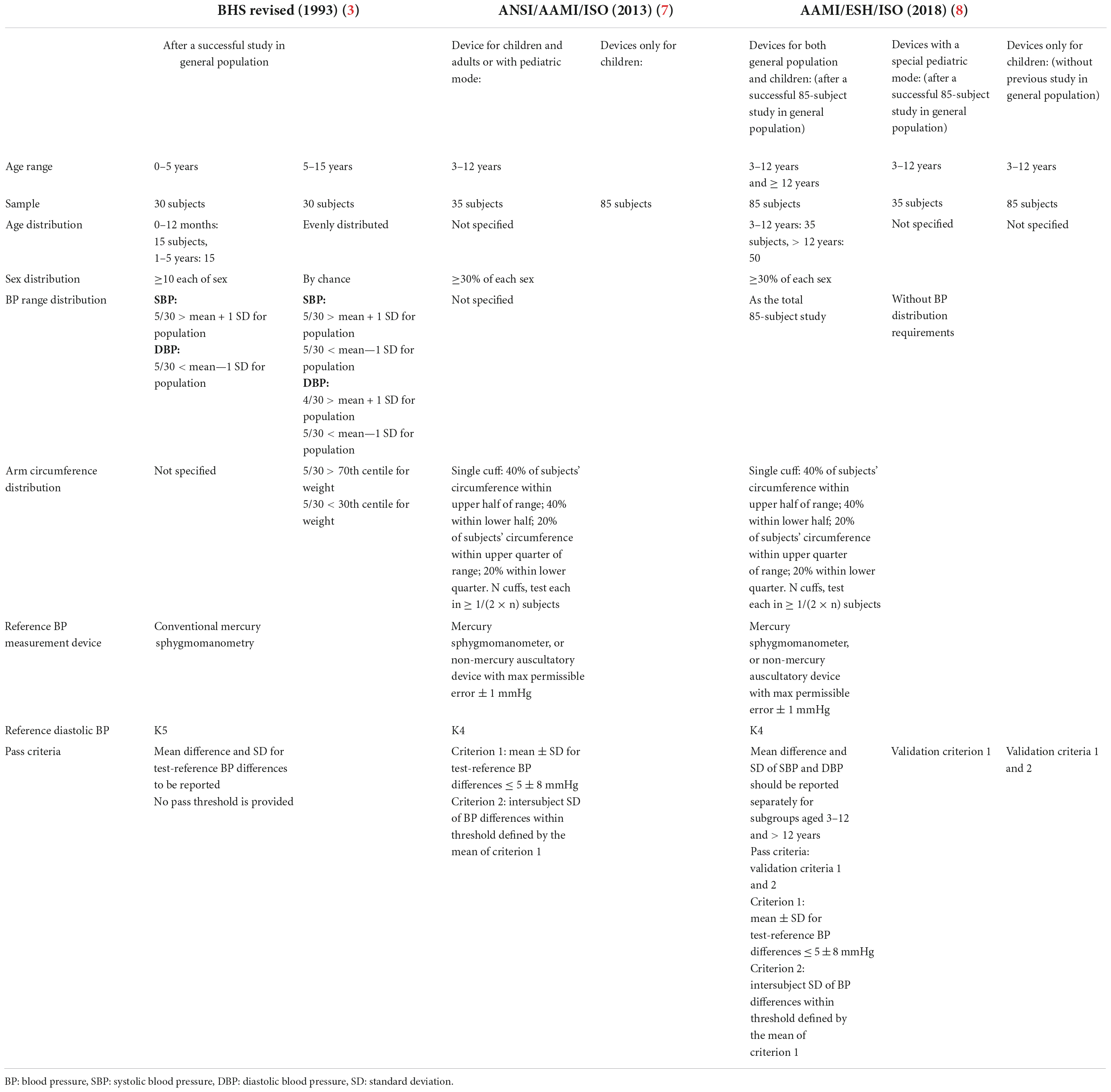
Table 2. Comparison of validation protocols for BP measuring devices in children.
The optimal sample size for a BP measuring device validation study varies among different organizations. As mentioned above the ESH validation protocol suggested a minimum of 33 subjects, while the BHS, the ANSI/AAMI/ISO as well as the AAMI/ESH/ISO required 85 participants (3, 10). The disagreement on ideal population sample sizes lies on the statistical power of the validation procedure against the cost and complexity (10, 12).
In the AAMI/ESH/ISO consensus statement, it was reported that that a validation study with a sample size of 35 subjects would be inadequate for a moderate accuracy device defined as a difference of 4 ± 5 mmHg compared to the test device, because of an unacceptably high at 28% chance to fail (10). However, according to a biostatistician report, a validation study with 35 subjects would be adequate for high- or low-accuracy devices. Then, it was calculated that a population sample of 85 subjects as previously suggested by the ANSI/AAMI/ISO has an acceptable chance of failing (18%) supporting the previous consensus of at least 85 subjects and taking into account that most devices in the market probably have moderate accuracy.
Adolescents older than 12 years are considered as general population and are evaluated within an 85-population sample. Transfer functions and in-built algorithms for the calculation of systolic and diastolic BP are not usually available by the manufacturer (13). The algorithms differ between devices, are considered proprietary for the manufacturer, and are, therefore, confidential. Of note, these algorithms are developed for adults with higher BP levels, and automated initial cuff inflations to high pressures may cause discomfort or pain in the child precluding its cooperation (14). Oscillation may also be lower in the youngest with lower BPs. For example, for a 12-year-old-boy with short stature at the 5th centile, the median level (50th centile) of systolic and diastolic BP is at 101/65 mmHg, respectively. Then, it is well described that in adolescents, the pulse wave contour is different than in older individuals with stiffer arteries (15). Whether these algorithms could evaluate with the same accuracy, the BP level in an adolescent as young as 12 years old and in a 65-year-old individual remains unanswered and uninvestigated.
A low-accuracy device for adolescents with an in-built algorithm resulting in high accuracy in older subjects would result in a medium-accuracy device with the inclusion of subjects 12–18 years in general population study. While the impact of this result would be moderate for the adult population, it may have important implications for adolescents regarding misclassification of their BP status and possibly undiagnosed hypertension.
The ESH 2016 guidelines on the management of high BP in children and adolescents consider that only older adolescents (≥16 years) are evaluated for hypertension using the adult BP threshold (16). It may be prudent that this age limit of 16 years would also apply for the validation studies in the general population. Then, a separate validation study considering adolescents <16 years as a special population may offer the opportunity for more precise assessment of accuracy before a device is suggested in the adolescent age range.
Children are considered as a special population if younger than 12 years. According to the BHS, the number of pediatric patients 3–12 years needed for a BP measurement device validation study is 30, if the device has been successfully validated in the general population. The ANSI/AAMI/ISO and the AAMI/ESH/ISO recommend a sample size is of at least 85 subjects if the study includes only children, but in the case of an existent validation study for the general population, the required sample size is 35 children. For validation, studies including both children and adults’ general population, a total sample size of at least 85 is required, with children consisting of 35 out of 85 participants. The same concerns about the transfer functions and in-built algorithms may apply for children 3–12 years. Again, given all the above considerations, it is unclear if the sample of 35 children would be adequate for this age range with low oscillation and different vascular functions for moderate accuracy devices (13).
Most monitors included two cuffs for the adult population. Special-size cuffs are not always available and in case of minors, children, and adolescents, this is an important issue. In the same concept as in the previous section, younger adolescents may erroneously be considered as general populations as they have different characteristics. It is recommended that the cuffs used for reference auscultatory BP measurement must have an inflatable bladder length that covers 75–100% of the upper arm circumference of each participant and a width that covers 37–50% of the arm circumference measured at the upper arm midpoint between acromion and olecranon (10). Many manufacturers include adult cuffs that are suitable for arm length >22 cm. For 12–15–years-old girls, the 5th–25th centile of midarm circumference is <20 cm and adult cuffs are not suitable for reliable BP measurement (17, 18). Similarly, the 25th centile of midarm circumference of a 12-year-old boy is <20 cm and for 14- and 15-years-old boys is at 22 and 23 cm, respectively. In the AAMI/ESH/ISO, it is recommended that inflatable bladder dimensions should be 12 cm for 12–15 years old and 15 cm for 15–18 years old.
If a device is considered for validation in children and adolescents, commercially available cuffs sizes both for the validation study but also for routine use should be a prerequisite criterion. Although not specifically reported in the consensus documents using cuffs from other manufacturers or from the test device, not designed for the device under evaluation, for the reference BP measurement during the validation study may result in significant measurement errors and significant bias of the validation study methodology.
The latest ESH and American Academy Pediatrics (AAP) guidelines for the diagnosis of high BP in children and adolescents recommend the use of Korotkoff sound 5 (K5) during office BP measurement (16, 19). The most frequently used validation protocol, the ANSI/AAMI/ISO recommends the use of Korotkoff sound 4 (K4) during the validation procedure which constitutes a major inconsistency between validation and clinical use of a device (9). However, in line with the guidelines for diagnosis of the hypertension in children and adolescents, the BHS, as well as the universal AAMI/ESH/ISO 2018 protocol recommend the use of K5 (3, 20). The latter recommends that if K5 is not audible, the child should be excluded.
In all consensus validation documents, two criteria as defined by the ANSI/AAMI/ISO are used to evaluate the successful validation of devices usually reported as pass or fail in review articles (9). The same criteria apply for pediatric studies although no studies have been performed to evaluate the suitability of these criteria in pediatric patients. However, only criterion 1 is necessary to be reported in the case of 35 subject studies. Of note, in case of a validation study including children in a general population study, both criteria should be reported separately for the pediatric subgroup.
A systematic search using Medline from inception to May 30, 2022, was performed to identify studies validating the accuracy of office BP monitors in the pediatric population alone or as a subgroup of the study population. We used the following search terms: (Office) AND (Blood Pressure) AND (Validation) AND (Monitor) OR (Device) AND (Children) OR (Adolescents). A hand-searching was also conducted for eligible studies. The reference list of each article included was checked for extra bibliography. Duplicates were removed. We included studies in the English language only. Two independent reviewers (KE and CS) screened titles and abstracts independently, and full texts were investigated for eligible studies. Differences between the two reviewers regarding study eligibility were resolved by a third reviewer (SS). Finally, study and population characteristics were extracted from each included study.
The search resulted in 21 studies with successful validation in children and adolescents (Supplementary Figure 1) (21–39). Validated devices for office BP measurement, children and adolescents using different available validation protocols are presented in Table 3. The accuracy of BP measuring devices was assessed using the ANSI/AAMI and the AMSI/AAMI/ISO protocol in almost 80% of the validation studies in children and adolescents (Figure 1). About half of the studies were performed before 2010. Few office BP devices were validated based on two different protocols, both the ANSI/AAMI and the BHS protocols (n = 4) (21, 29, 37, 38) or the BHS and the ESH-IP (n = 2) (23, 24, 39). In all studies, devices passed the validation criteria by both protocols for systolic and diastolic BP with the exception of the Dinamap Procare-200 device that failed for the diastolic BP with ESH protocol criteria (24). One device that has been assessed by two studies was evaluated as passed in one of them but failed in the other one (23, 39). In one study, 3 devices were evaluated simultaneously (23).
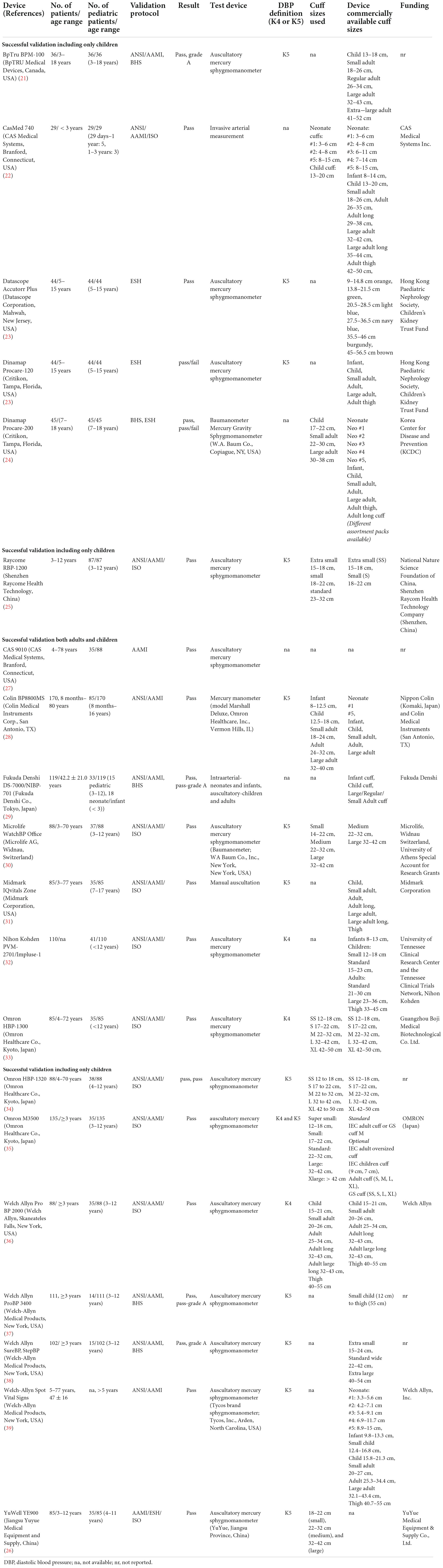
Table 3. Validated devices for office BP measurement in children and adolescents.
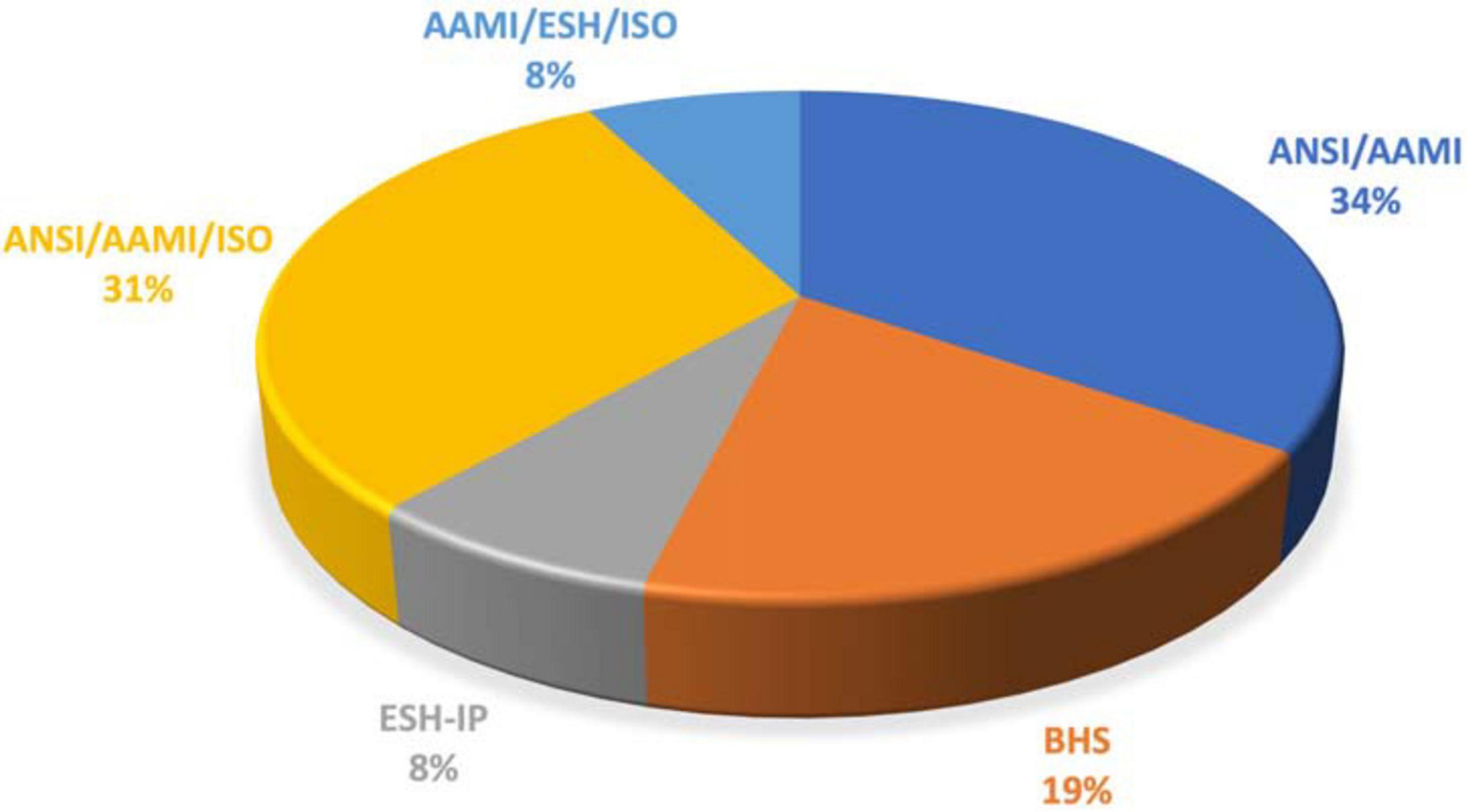
Figure 1. Validation protocols used in studies assessing accuracy of BP measuring devices in children and adolescents.
Only 6 out of 7 studies that included exclusively pediatric population fulfilled the pass criteria. Three used the ESH-IP protocol (23, 24), which is not designed for children, two the BHS protocol, and three the ANSI/AAMI/ISO protocol. Among studies that used the ANSI/AAMI/ISO protocol, two had an inadequate sample size, leaving only 1 study that used the ANSI/AAMI/ISO protocol to provide the best available validation evidence for office BP devices in children (25).
The test device used in almost all studies was a mercury sphygmomanometer measuring BP by the auscultatory method. Intra-arterial measurement as a test method was used in 2 studies (22, 29), one of them including only neonates and infants (29). Most studies included two trained observers for the BP measurements as recommended and most of them were health professionals.
Seven out of twenty-one validating studies did not meet the criteria for the age range required based on the selected protocols. None of the studies reported the required age distribution in the population. Only five studies met both the sample age and sample size required for a validation study. Although the available protocols do not specify the required ratio of female–male participants for children’s studies, most of the studies that defined their population, recruited the same percentage of patients of each sex.
Among studies that used the AAMI protocol the one that included 85 children reported both validation criteria 1 and 2. Also in studies including both the general population and children both validation criteria 1 and 2 were used. In the studies including 35 children with an existent validation study for adults, only criterion 1 was used. Funding by the industry was reported in eight studies (25, 28–33, 35, 36).
Several validation studies in children or including children in the general population lack adequate reporting of validation data according to validation recommendations or not fulfill all requirements (Table 3). Common pitfalls include:
The requirements for sample size were satisfied in 12 out of 21 studies. For example, the validation study by Alpert et al., using the ANSI/AAMI/ISO protocol included only children, but the sample size was less than the required sample size of at least 85 subjects (36). The same number of subjects was included by Mattu et al. (21) in a validation study for a BP measuring device intended for use in children but considered adequate as there was already an existent validation study for the general population (21).
In about half of the studies, no data were reported regarding the cuffs used for the validation procedure. Moreover, in several cases, information about commercially available cuffs for the validated device was not reported in manufacturer’s sites. Manufacturers may provide only one adult cuffs with the device and pediatric cuff sizes are usually sold separately as extra accessories. In the validation studies that included both children and adults, 6 out of 13 studies used for the validation procedure the cuffs provided by the manufacturer along with the device (Table 3). Cuff sizes used during the validation with the description of cuffs’ length and width were usually reported, but only 4 of them reported the number of subjects tested for different cuff sizes. In the validation studies that included only children, 2 out of 6 studies used the same size cuffs as provided for the validation, and only 3 out of 6 studies reported the number of subjects tested for each cuff size. Details on the selection of cuff size, midarm circumference of the population and/or midarm circumference by cuff size used were scarcely reported.
Most of the included studies used K5 for the definition of diastolic BP, as it is suggested by BHS and AAMI protocols. Some studies didn’t report by which Korotkoff sound (K4 or K5) was diastolic BP defined. K4 was reported in four studies while one study reported both K4 and K5 for all participants (35). Five studies used ANSI/AAMI/ISO protocol but reported K5 (25, 26, 30, 31, 33).
Validation criterion 1 was used in all studies. Results for children were reported together with those of older participants (adults) in the case of studies in the general population, and only one study (1 out of 13) reported data on criterion 1 separately for children (28).
The level of evidence-based upon pediatrics studies for the established validation criteria in children and adolescents needs to be assessed to evaluate the suitability of these criteria in children and adolescents. When evidence does not exist then extrapolation of data from adult studies is usually applied, but limitations of such strategy need to be acknowledged and gaps of evidence would serve as motivation for designing the new research activities. This is the case for BP measuring devices validation studies in children and adolescents. In addition, most validation studies analyzed children’s data along with adult ones posing significant uncertainty on the accuracy of the BP measuring validated devices in the pediatric population. Given that automated oscillometric BP devices become extensively popular in routine clinical practice for the diagnosis of high BP in childhood the need of validation protocols addressing the needs and special characteristics of children and adolescents is emerging to ensure accurate evaluation of BP levels in childhood.
This publication is based on the work of the COST Action HyperChildNET (CA19115).
SS an EL: conceptualization. SS, AC, KE, CS, CA, PP, JC, and GH: writing—original draft preparation. SS and AC: writing—review and editing. All authors have read and agreed to the current version of the manuscript.
This work was supported by COST (European Cooperation in Science and Technology), and the Horizon 2020 Framework Program of the European Union.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2022.1001878/full#supplementary-material
1. O’Brien E, Alpert BS, Stergiou GS. Accurate blood pressure measuring devices: influencing users in the 21st century. J Clin Hypertens. (2018) 20:1138–41. doi: 10.1111/jch.13278
2. American National Standards Institute, Association for the Advancement of Medical Instrumentation. ANSI/AAMI Sp10:1987, Electronic or Automated Sphygmomanometers. Arlington, VA: AAMI (1987).
3. O’Brien E, Petrie J, Littler W, de Swiet M, Padfield PL, O’Malley K, et al. The British hypertension society protocol for the evaluation of automated and semi-automated blood pressure measuring devices with special reference to ambulatory systems. J Hypertens. (1990) 8:607–19. doi: 10.1097/00004872-199007000-00004
4. O’Brien E, Petrie J, Littler WA, De Swiet M, Padfield PL, Altman D, et al. The British hypertension society protocol for the evaluation of blood pressure measuring devices. J Hypertens. (1993) 11:43–63.
5. Tholl U, Lüders S, Bramlage P, Dechend R, Eckert S, Mengden T, et al. The German hypertension league (deutsche hochdruckliga) quality seal protocol for blood pressure-measuring devices: 15-year experience and results from 105 devices for home blood pressure control. Blood Press Monit. (2016) 21:197–205. doi: 10.1097/MBP.0000000000000186
6. O’Brien E, Atkins N, Stergiou G, Karpettas N, Parati G, Asmar R, et al. European society of hypertension international protocol revision 2010 for the validation of blood pressure measuring devices in adults. Blood Press Monit. (2010) 15:23–38. doi: 10.1097/MBP.0b013e3283360e98
7. O’Brien E, Pickering T, Asmar R, Myers M, Parati G, Staessen J, et al. Working Group on blood pressure monitoring of the european society of hypertension international protocol for validation of blood pressure measuring devices in adults. Blood Press Monit. (2002) 7:3–17. doi: 10.1097/00126097-200202000-00002
8. International Organization for Standardization. Noninvasive Sphygmomanometers: Clinical Validation of Automated Measurement Type. Geneva: International Organization for Standardization (2009).
9. ISO. Noninvasive Sphygmomanometers - Part 2: Clinical Investigation of Automated Measurement Type. New York, NY: American National Standards Institute (2013).
10. Stergiou GS, Alpert B, Mieke S, Asmar R, Atkins N, Eckert S, et al. A universal standard for the validation of blood pressure measuring devices: association for the Advancement of Medical Instrumentation/European Society of Hypertension/International Organization for Standardization (Aami/Esh/Iso) Collaboration Statement. Hypertension. (2018) 71:368–74. doi: 10.1161/HYPERTENSIONAHA.117.10237
11. Stergiou GS, Boubouchairopoulou N, Kollias A. Accuracy of automated blood pressure measurement in children: evidence, issues, and perspectives. Hypertension. (2017) 69:1000–6. doi: 10.1161/hypertensionaha.116.08553
12. Friedman BA, Alpert BS, Osborn D, Prisant LM, Quinn DE, Seller J. Assessment of the validation of blood pressure monitors: a statistical reappraisal. Blood Press Monit. (2008) 13:187–91. doi: 10.1097/MBP.0b013e3283071a64
13. Stabouli S. Office and out of office blood pressure measurements. In: Lurbe E, Wühl E editors. Hypertension in Children and Adolescents Updates in Hypertension and Cardiovascular Protection. Cham: Springer (2019). doi: 10.1007/978-3-030-18167-3_4
14. Butani L, Morgenstern BZ. Are pitfalls of oxcillometric blood pressure measurements preventable in children? Pediatr Nephrol. (2003) 18:313–8. doi: 10.1007/s00467-003-1075-7
15. Nilsson PM, Lurbe E, Laurent S. The early life origins of vascular ageing and cardiovascular risk: the eva syndrome. J Hypertens. (2008) 26:1049–57. doi: 10.1097/HJH.0b013e3282f82c3e
16. Lurbe E, Agabiti-Rosei E, Cruickshank JK, Dominiczak A, Erdine S, Hirth A, et al. 2016 European society of hypertension guidelines for the management of high blood pressure in children and adolescents. J Hypertens. (2016) 34:1887–920. doi: 10.1097/hjh.0000000000001039
17. Addo OY, Himes JH, Zemel BS. Reference ranges for midupper arm circumference, upper arm muscle area, and upper arm fat area in Us children and adolescents Aged 1-20 Y. Am J Clin Nutr. (2017) 105:111–20. doi: 10.3945/ajcn.116.142190
18. Mramba L, Ngari M, Mwangome M, Muchai L, Bauni E, Walker AS, et al. A growth reference for mid upper arm circumference for age among school age children and adolescents, and validation for mortality: growth curve construction and longitudinal cohort study. BMJ. (2017) 358:j3423. doi: 10.1136/bmj.j3423
19. Flynn JT, Kaelber DC, Baker-Smith CM, Blowey D, Carroll AE, Daniels SR, et al. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. (2017) 140:e20171904. doi: 10.1542/peds.2017-1904
20. Stergiou GS, Alpert BS, Mieke S, Wang J, O’Brien E. Validation protocols for blood pressure measuring devices in the 21st century. J Clin Hypertens. (2018) 20:1096–9. doi: 10.1111/jch.13294
21. Mattu GS, Heran BS, Wright JM. Comparison of the automated non-invasive oscillometric blood pressure monitor (Bptru) with the auscultatory mercury sphygmomanometer in a paediatric population. Blood Press Monit. (2004) 9:39–45. doi: 10.1097/00126097-200402000-00008
22. Lang SM, Giuliano JS Jr., Carroll CL, Rosenkrantz TS, Eisenfeld L. Neonatal/infant validation study of the cas model 740 noninvasive blood pressure monitor with the orion/maxiq nibp module. Blood Press Monit. (2014) 19:180–2. doi: 10.1097/mbp.0000000000000036
23. Wong SN, Tz Sung RY, Leung LC. Validation of three oscillometric blood pressure devices against auscultatory mercury sphygmomanometer in children. Blood Press Monit. (2006) 11:281–91. doi: 10.1097/01.mbp.0000209082.09623.b4
24. Lee CG, Park HM, Shin HJ, Moon JS, Hong YM, Kim NS, et al. Validation study of the dinamap procare 200 upper arm blood pressure monitor in children and adolescents. Korean J Pediatr. (2011) 54:463–9. doi: 10.3345/kjp.2011.54.11.463
25. Dong J, Dong H, Ye P, Yan Y, Xi B, Mi J. Validation of the raycome Rbp-1200 upper-arm pulse wave device in children aged 3-12 years according to the association for the advancement of medical instrumentation protocol. Blood Press Monit. (2017) 22:40–3. doi: 10.1097/mbp.0000000000000217
26. Zhang HJ, Zhang J, Wang SL, Zhang J, Teng LN, Zhang SJ, et al. Validation of the Yuwell Ye900 oscillometric blood pressure monitor for professional office use in adults and children according to the Aami/Esh/Iso Universal Standard (Iso 81060-2:2018). Blood Press Monit. (2021) 26:396–9. doi: 10.1097/mbp.0000000000000541
27. Alpert BC. Validation of Cas Model 9010 automated blood pressure monitor:children/adult and neonatal studies. Blood Press Monit. (1996) 1:69–73.
28. Ling J, Ohara Y, Orime Y, Noon GP, Takatani S. Clinical evaluation of the oscillometric blood pressure monitor in adults and children based on the 1992 Aami Sp-10 standards. J Clin Monit. (1995) 11:123–30. doi: 10.1007/bf01617734
29. Alpert BS, Blakely DW. Validation of the Fukuda Denshi Ds-7000/Nibp-701 patient monitor by Aami standard testing. Blood Press Monit. (2009) 14:274–6.
30. Kollias A, Ntineri A, Kyriakoulis KG, Stambolliu E, Lagou S, Boubouchairopoulou N, et al. Validation of the professional device for blood pressure measurement microlife watchbp office in adults and children according to the American National Standards Institute/Association for the Advancement of Medical Instrumentation/International Organization for Standardization Standard. Blood Press Monit. (2018) 23:112–4. doi: 10.1097/mbp.0000000000000307
31. Alpert BS. Validation of the step deflation algorithm of the midmark iqvitals zone vital signs monitor: part of a novel clinical ecosystem. Blood Press Monit. (2021) 26:234–6. doi: 10.1097/mbp.0000000000000524
32. Alpert BS. Validation of the Nihon Kohden Pvm-2701/impulse-1 automated device by both Aami (2002) and Iso standards testing. Blood Press Monit. (2012) 17:207–9. doi: 10.1097/MBP.0b013e328359c48e
33. Meng L, Zhao D, Pan Y, Ding W, Wei Q, Li H, et al. Validation of Omron Hbp-1300 professional blood pressure monitor based on auscultation in children and adults. BMC Cardiovasc Disord. (2016) 16:9. doi: 10.1186/s12872-015-0177-z
34. Saito K, Hishiki Y, Takahashi H. Validation of the Omron Hbp-1320 for Professional Use According to the Ansi/Aami/Iso 81060-2: 2013 protocol and the 2010 revision of the European society of hypertension international protocol. Blood Press Monit. (2020) 25:162–6. doi: 10.1097/mbp.0000000000000437
35. Chahine MN, Assemaani N, Sayed Hassan G, Cham M, Salameh P, Asmar R. Validation of the Omron M3500 blood pressure measuring device using normal- and high-speed modes in adult and specific populations (obese and children) according to AAMI protocol. J Clin Hypertens. (2015) 17:622–9. doi: 10.1111/jch.12540
36. Alpert BS. Validation of the Welch Allyn Pro Bp 2000, a professional-grade inflation-based automated sphygmomanometer with arrhythmia detection in a combined pediatric and adult population by Ansi/Aami/Iso standard testing. Blood Press Monit. (2018) 23:315–7. doi: 10.1097/mbp.0000000000000350
37. Alpert BS. Validation of the Welch Allyn Probp 3400: a device for modern medical practice. Blood Press Monit. (2011) 16:156–8. doi: 10.1097/MBP.0b013e328346d61b
38. Alpert BS. Validation of the Welch Allyn Surebp (Inflation) and Stepbp (Deflation) algorithms by aami standard testing and bhs data analysis. Blood Press Monit. (2011) 16:96–8. doi: 10.1097/MBP.0b013e328345232f
Keywords: blood pressure, device, validation, children, adolescents
Citation: Stabouli S, Chainoglou A, Evripidou K, Simão C, Antza C, Petrou P, Hamdani G, Calpe J and Lurbe E (2022) Comparison of validation protocols for blood pressure measuring devices in children and adolescents. Front. Cardiovasc. Med. 9:1001878. doi: 10.3389/fcvm.2022.1001878
Received: 24 July 2022; Accepted: 31 October 2022;
Published: 23 November 2022.
Edited by:
Kyriakos Dimitriadis, National and Kapodistrian University of Athens, GreeceReviewed by:
Rafal Adam Januszek, University Hospital in Kraków, PolandCopyright © 2022 Stabouli, Chainoglou, Evripidou, Simão, Antza, Petrou, Hamdani, Calpe and Lurbe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Stella Stabouli, c3N0YWJvdWxAYXV0aC5ncg==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.