 Nils Perrin1,2
Nils Perrin1,2 Réda Ibrahim1Nicolas Dürrleman1Arsène Basmadjian1Lionel Leroux3Philippe Demers1Thomas Modine3
Réda Ibrahim1Nicolas Dürrleman1Arsène Basmadjian1Lionel Leroux3Philippe Demers1Thomas Modine3 Walid Ben Ali1*
Walid Ben Ali1*- 1Structural Heart Intervention Program, Montreal Heart Institute, Montreal, QC, Canada
- 2Cardiology Division, Geneva University Hospitals, Geneva, Switzerland
- 3Service Médico-Chirurgical, Valvulopathies-Chirurgie Cardiaque-Cardiologie Interventionelle Structurelle, Hôpital Cardiologique de Haut Lévèque, CHU Bordeaux, Bordeaux, France
Bicuspid aortic valve (BAV) is the most frequent congenital anomaly and has a natural evolution toward aortic regurgitation or stenosis due to the asymmetrical valve function associated with an evolutive ascending aortopathy. Several BAV classifications exist describing the presence and number of raphe, amount and location of calcium, and the symmetry of the functional cusps. The impact of BAV morphology on transcatheter aortic valve implantation (TAVI) outcomes still remains little investigated. Pivotal randomized trials comparing TAVI with surgery have excluded BAV until yet. However, data from registries and observational studies including highly selected patients have shown promising results of TAVI in BAV. With this review, we aimed at describing anatomical and pathophysiological characteristics of BAV, discussing the main aspects to assess diagnostic imaging modalities, and giving an overview of TAVI outcomes and technical considerations specific to BAV morphology.
Introduction
Transcatheter aortic valve implantation (TAVI) has become the standard of care for patients with symptomatic severe aortic stenosis at intermediate and high surgical risk, especially if suitable from a transfemoral approach, and is considered as a valuable option for patients at low surgical risk (1–6). However, in pivotal randomized trials comparing TAVI with surgery, bicuspid aortic valve stenosis (BAV), either congenital or acquired, has been excluded until yet. BAV is the most frequent congenital anomaly and is found in up to 2.25% of the general population. Its natural evolution toward aortic regurgitation and/or stenosis is mainly due to the asymmetrical valve function associated with an evolutive ascending aortopathy. Moreover, BAV was described in >20% of high-risk elderly patients undergoing surgical aortic valve replacement for aortic stenosis (7). This category of patients would largely be considered for TAVI nowadays. In an analysis from the Society of Thoracic Surgeons (STS)/American College of Cardiology (ACC) Transcatheter Valve Therapy (TVT) registry regarding transcatheter heart valve off-label use, Hira et al. reported that about 2% of patients treated for BAV (8). A higher prevalence of BAV was demonstrated in the Chinese TAVR registries (up to 5.8%) (9). In addition to a possible impact of ethnicity difference in BAV prevalence, the younger and lower risk population included in the Chinese BAV studies may lead to interpretation bias. In the worldwide current trend toward younger patients treated by TAVI, transcatheter heart valve operators will face an increasing number of patients with BAV.
With this review, we aimed at describing anatomical and pathophysiological characteristics of BAV, discussing the main aspects to assess with diagnostic imaging modalities, and giving an overview of TAVI outcomes and technical considerations specific to BAV morphology.
Nomenclature
The BAV is defined by the presence of 2 functional commissures with <3 zones of parallel apposition between them (10). The presence and orientation of the commissural fusion and raphe are highly variable among the population. Fused commissures can be either congenital or acquired through the development of a rheumatological valvular disease or progression of age-related atherosclerosis. In theory, all degrees and combinations of fused cusps can be possible. Most BAV classifications reported in the literature were derived from the surgical analysis yet. Fused commissures most often involve the right and left coronary cusps (80% of the cases), followed by the right and non-coronary cusps and, rarely, the left and non-coronary cusps (10). Sievers is the most widely known and used classification of BAV describing the number and orientation of the raphe based on surgical models (10). Briefly, type 0 has no raphe with 2 normal functioning symmetrical cusps. Type 1 presents one raphe connecting two underdeveloped cusps. Finally, type 2 has two raphes with two underdeveloped cusps and commissures, and one fully developed cusp and commissure. The 2014 International BAV Consortium (BAVCon) adopted a similar but simplified classification system according to the 2 fused cusps. All 3 types (type 1: right-left cusp fusion; type 2: right-non fusion; and type 3: left-non fusion) may or may not have a raphe (11). De Kerchove et al. suggested a classification system assessing the surgical repairability of the BAV, such as commissural orientation (varying from symmetrical to very asymmetrical cusp angles), length of fusion, and non-functional commissure height (12). Very recently, a new international consensus statement on the nomenclature of BAV has been developed with a simple and comprehensive classification system based on imaging modalities (echocardiographic, CT, and MRI) and anatomical surgical pathology (Figure 1) (13). The authors described 3 types of BAV: the fused (similar to Sievers type 1), the 2-sinus (latero-lateral and antero-posterior phenotypes), and the partial-fusion types. The fused-type is thereafter subclassified according to the symmetry of the functional cusps and commissure angle of the non-fused cusp. The present descriptive classification derives from a multidisciplinary consortium and aims at better identifying anatomical features of BAV that best predict the surgical valve replacement or repair success and TAVI outcomes.

Figure 1. The 2021 international consensus statement on nomenclature and classification of BAV (13).
Jilaihawi et al. adapted the traditional Sievers classification to better address the transcatheter heart valve interaction with the aortic root (14). BAV morphologies were defined as bicommissural non-raphe (equivalent to Sievers type 0), bicommissural raphe (equivalent to Sievers type 1), and tricommissural (sharing characteristics between Sievers type 1 and tricuspid valves) types (Figure 2). In an early exploratory study, 30-day mortality, cerebrovascular events, and new pacemaker implantation across the BAV morphologies were similar (14). Interestingly, the intercommissural distance (for bicommissural bicuspids) was associated to ≥moderate paravalvular leak, with respect to the limited power of the study (n = 130).
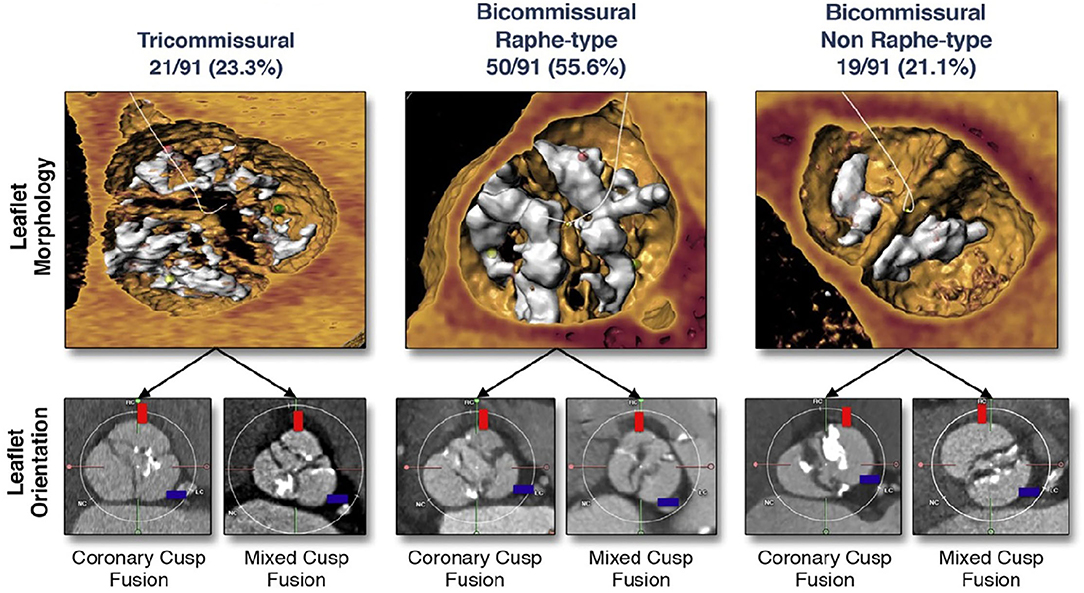
Figure 2. Bicuspid aortic valve classification in the TAVI era (14).
In contrast with the STS Surgical Database Form who started to collect specific anatomical characteristics of BAV in 2017, the large STS/ACC TVT registry does not provide information on BAV sub-type classification. The impact of BAV morphology on TAVI outcomes still remains little investigated yet. In an international multicenter BAV TAVI registry, BAV were classified according to a modified Sievers nomenclature differentiating a calcified raphe to a non-calcified raphe type 1 morphology. Death at 1 year increased significantly between type 0 (no raphe), type 1 with a non-calcified raphe, and type 1 with a calcified raphe (2.4, 4.8, and 9.5%, p = 0.006 between the groups, respectively). Moreover, patients with both calcified raphe and excess leaflet calcifications presented significantly higher 2-year mortality and ≥ moderate paravalvular regurgitation in comparison with patients with one or none of these characteristics (15).
Pathophysiological Characteristics
In comparison with tricuspid valves, BAV has different localization and excess calcification of the aortic valve (16). Asymmetrical BAV leaflet motion and a higher leaflet coaptation point increase the shear stress through the valve leading to a calcification process starting already at a young age. As another consequence of the shear stress, patients with BAV develop progressive aortic root and ascending aorta dilatation. Larger annular and sinus of Valsalva dimensions have been reported among the patient undergoing TAVI for BAV vs. tricuspid valves, respectively (annulus mean area-derived diameter 26.3 ± 3.0 vs. 23.2 ± 1.9 mm, p < 0.01 and sinus of Valsalva 930.0 vs. 866.6 mm2, p = 0.005) (17). Recent MRI blood flow analysis was able to confirm the increased aortic wall shear stress, namely, induced by eccentric jets (11). A small cohort study reported an increased aortic growth associated with the degree of the aortic jet angle (18). Interestingly, other blood flow imaging analysis has suggested a different degree of flow abnormality severity according to the BAV type, thus it remains preliminary investigations (19).
Concomitant congenital anomalies of coronary origin are more frequent with the congenital BAV in comparison with tricuspid aortic valves (7 vs. 3%, p = 0.001), affecting mainly anomalous origin of the right coronary artery (20). Whereas, the similar prevalence of anomalous origin of the left main has been observed between BAV and tricuspid valves, the absence of the left main with separate left anterior descending and circumflex artery ostia has been more frequently reported in BAV than tricuspid valves (21). Moreover, from a TAVI perspective, a higher distance from the aortic annulus to coronary ostia has been reported in BAV (22). As discussed later in this review, the origin and height of coronary ostia will be a specific parameter to assess the pre-procedural multislice CT (MSCT).
Imaging
Echocardiography
Transthoracic (TTE) and transesophageal echocardiography (TEE) remain the first-line imaging for BAV diagnosis and commissural morphology classification. However, inpatient candidates for TAVI, the important calcification burden of aortic root may limit acoustic windows and participation in misclassification (23). Echocardiography has the best accuracy for aortic valve function analysis. Quantification of BAV aortic stenosis severity is similar to the tricuspid valve and should follow the latest guidelines for valvular heart disease of the European Society of Cardiology (ESC) (24). However, in BAV, maximal velocity flows are most of the time measured at the right parasternal window due to eccentricity of the aortic jet (25). In cases of very eccentric jets, misalignment of the beam leads to maximal velocity underestimation. On the other hand, aortic valve regurgitation severity is more difficult to assess since laminar flow may be falsely assumed at the sinotubular junction leading to inaccurate regurgitation volume calculations. Integration of several parameters, such as aortic holodiastolic retrograde flow velocity, may help to address these limitations. Since BAV is frequently associated with the ascending aorta dilatation, echocardiography often offers favorable visualization of the initial part of the proximal part of the ascending aorta and is thus preferentially used in the clinical practice for patient follow-up.
Multislice CT
In the current TAVI era, MSCT has an integral part in procedural planning investigations. MSCT has the best accuracy for BAV morphological analysis (26). Detailed analysis of amount and location of aortic root calcification as well as precise aortic and surrounding structures measurements play a pivotal role for prosthesis choice. In comparison with tricuspid valves, BAV has a larger annulus and sinus of Valsalva diameters. In addition, BAV has less elliptical aortic annulus with more eccentric calcifications (27).
Prosthesis Sizing
Prosthesis sizing is mainly dependent on annular diameter measurement in tricuspid valves. A certain degree of prosthesis oversizing (5–20 and 12–25% for balloon- and self-expandable devices, respectively) is recommended to limit the paravalvular leak and prosthesis embolization (28, 29). Calcified and fibrotic leaflets as well as commissural fusion with or without raphe modify the aortic root anatomy and increase the challenge of valve sizing in BAV. Interaction and interference of the prosthesis with the aortic root can occur from the level of the left ventricular outflow tract to above the sinotubular junction according to the prosthesis design. Balloon sizing with waste measurements and sequential aortography has been suggested by some operators for valve sizing in BAV but has never been meticulously investigated by studies (30). The behavior of calcified leaflets and raphe with respect to the surrounding structures (such as coronary ostia) may also be appreciated during balloon inflation.
Initial evidence from post-TAVI MSCT studies has shown that the maximal stent frame interaction with aortic root in BAV anatomies occurred rather at the supra-annular than annular level, typically between 4 and 8 mm above the annulus (31, 32). Perimeters and area at the supra-annular level will have to be circumscribed by taking into account the border of the leaflets and commissural fusions. Unlike tricuspid valves where the virtual basal ring is easily defined by 3 anatomic distinct hinge points at the nadir part of the cusps, defining the virtual basal ring in BAV is challenging and may lead to inaccurate prosthesis sizing.
Prosthesis sizing according to the level of estimated prosthesis anchoring at a supra-annular plane in raphe-type BAV has been recently suggested by a multicenter MSCT study (33). The so-called level of implantation at the raphe (LIRA) plane is identified where the plane cuts the raphe at the level of its maximum protrusion. The perimeter around the internal border of the leaflet is then traced excluding fused commissures or heavy calcifications. The smallest perimeter between the LIRA plane and the virtual basal ring is then chosen for prosthesis sizing (33). The Calcium Algorithm Sizing for bicusPid Evaluation with Raphe (CASPER) algorithm adapted the perimeter/area derived annulus diameter according to 3 main characteristics: raphe length/annulus diameter ratio, calcium score, and prevalence of calcium distribution on raphe site (34). According to the algorithm, operators detracted 0–2 mm from the area/perimeter derived mean annular diameter for valve sizing. In a validation cohort (n = 21), Petronio et al. reported 100% VARC-2 defined procedural success (34).
Even though prosthesis maximal constraint seems to occur at a supra-annular level in imaging studies, the Bicuspid Aortic Valve Anatomy and Relationship with Devices (BAVARD) retrospective registry reported a tapered aortic root configuration (intercommissural distance < annular diameter) in only 13.8% of the BAV raising the question whether supra-annular or annular measurements should be best used for prosthesis sizing (22). Importantly, in this registry, the intercommissural distance was systematically measured 4 mm above the annulus for standardization purposes, leading to a possible higher proportion of tapered configuration according to the level of prosthesis maximal constraints. Tubular (intercommissural distance = annular diameter) and flared (intercommissural distance > annular diameter) configuration accounted for 33.7 and 52.5% of the BAV. According to the BAVARD algorithm, size of the prosthesis should best be chosen according to the smallest measure between the annulus diameter (tubular or flared configuration) or the intercommissural distance (tapered configuration) (22).
The specific anatomical particularities of BAV highlight the importance of detailed aortic root analysis taking into account supra-annular structures (including calcification and raphe) in the prosthesis sizing process (Figure 3). A possible trend toward the prosthesis down-sizing according to standard measurements at the annulus level is to be considered, particularly in cases of tapered aortic root configuration. All these sizing algorithms need, however, further validation, namely, with special regards to the clinical outcomes according to different BAV morphologies (35).
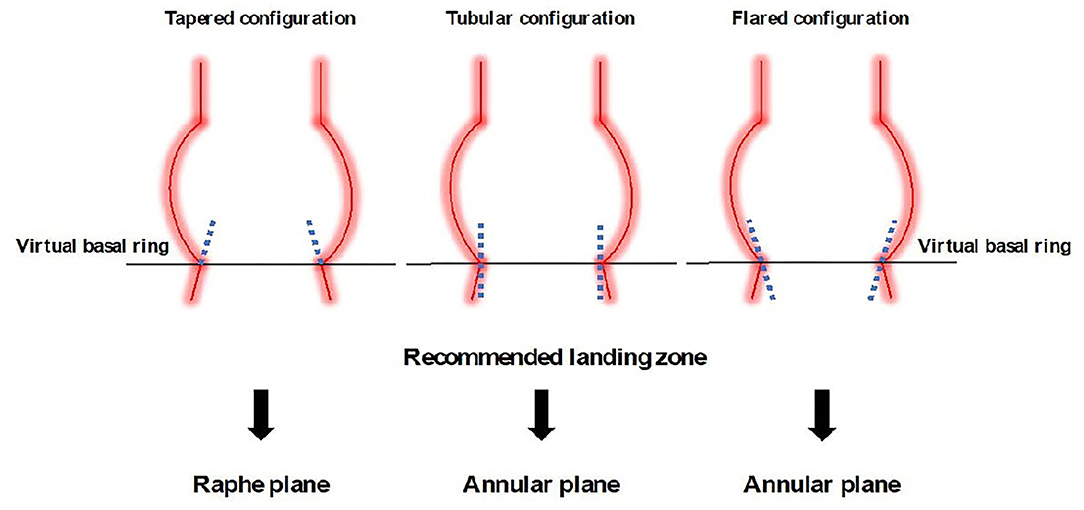
Figure 3. Recommended prosthesis sizing according to the aortic root morphology in BAVs.
Evaluation of Coronary Obstruction Risk
Bicuspid aortic valve is associated with the higher coronary ostia take-off and larger sinuses of Valsalva (36). While these characteristics would rather prevent coronary obstruction, other specific characteristics of BAV have to be considered before TAVI. Excessive raphe calcification between the non-coronary cusp and the left or right coronary cusp may lead to the prosthesis displacement after deployment in the opposite direction obstructing either the left main or right coronary ostium. Furthermore, coronary ostia have been described closer to commissures leading to an increased risk of coronary obstruction, especially when leaflets are very asymmetrical or bulky (36). In case of a borderline situation despite the pre-procedural MSCT imaging analysis, balloon inflation with simultaneous aortography may identify aortic root at risk for coronary obstruction. Overall, the risk of coronary obstruction in BAV after TAVI of well-selected patients remains, however, low and similar to tricuspid valves (37). In the case of BAV anatomies at high risk for coronary obstruction, a similar to tricuspid valves approach is recommended, going from simple coronary pre-procedural wiring to chimney technique or Bioprosthetic or native Aortic Scallop Intentional Laceration to prevent Iatrogenic Coronary Artery obstruction during TAVR.
Aortic Valve Replacement In BAV Stenosis
Surgery
Comparison between TAVI and surgery for BAV relies on propensity-matched studies as no randomized trial exists yet. BAV stenosis was considered as an exclusion criterion in existing randomized studies comparing TAVI with surgery. Using Medicare data, Mentias et al. compared 699 matched pairs of BAV patients undergoing TAVI and surgery (38). In-hospital mortality and stroke rate were similar between TAVI and surgery (2.2 vs. 2.3%, p = 0.90/2.9 vs. 2.7%, p = 0.90/2.7 vs. 2.9%, p = 0.90, respectively). Thirty-day mortality and 1-year mortality were similar between both groups. Patients undergoing TAVI presented, however, a higher rate of new permanent pacemaker implantation in comparison with surgery (12.2 vs. 7.6%, p = 0.009, respectively). Interestingly, clinical outcomes remained similar after excluding patients undergoing concomitant coronary artery bypass graft or aortic root replacement surgery (38). A similar propensity-score matched study was conducted by Elbadawi et al. analyzing patients undergoing TAVI and isolated surgery for BAV (n = 975 pairs). Data were retrospectively collected from the US National Inpatient Sample database. After matching, in-hospital mortality and stroke rate were similar between TAVI and surgery (3.1 vs. 3.1 and 2.6 vs. 2.1%, respectively). Here again, patients undergoing TAVI had a higher permanent pacemaker implantation rate. The results of these 2 propensity-matched score studies are encouraging in the light of similar outcomes than studies randomizing patients with tricuspid valves to TAVI or surgery. However, dedicated randomized trials including patients with BAV still need to be designed. As TAVI indication has been progressively extended to younger patients, an increasing number of TAVI will be performed in BAV stenosis. Strong evidence is still lacking since patients with BAV were largely excluded from pivotal randomized trials. Registries of TAVI in BAV have reported excellent outcomes, though result interpretation is limited by significant selection bias related to registries. Before considering TAVI instead of surgery for most BAV stenosis, direct comparison between surgery and TAVI is mandatory, particularly when considering the excellent result of surgery in BAV. In addition, long-term outcomes will be needed with respect to the younger age of patients with BAV but data over 10 years are challenging to collect. In the latest and very recent ESC valvular heart guidelines (2021), the role of TAVI in BAV stenosis remains a gap of evidence, though the consensus paper considers a BAV as an unfavorable anatomical characteristic for TAVI (24). Interestingly, the U.S. FDA approved Edwards Sapien valve and Medtronic Corevalve for patients with aortic stenosis at low surgical risk patients in August 2019. At the same time, the Corevalve Evolut TAVI system obtained the approval for the treatment of BAV deemed at intermediate or greater risk for surgery followed by CE Mark and Health Canada approval, respectively, in June 2020 and January 2021.
Transcatheter Aortic Valve Implantation
Outcomes
Data reporting performances of TAVI in patients with BAV rely mainly on comparative retrospective and small prospective studies. Currently, the BAV stenosis candidates for TAVI are highly selected. Moreover, their younger age and reduced risk profile may definitively bias the comparison with tricuspid valve patients. The challenges raised by the non-standardized BAV patient selection process for TAVI may impact the procedural and clinical outcomes in-between the studies. Table 1 summarizes main studies reporting outcomes of TAVI in BAV using current generation devices (9, 15, 22, 35, 37, 39–43).
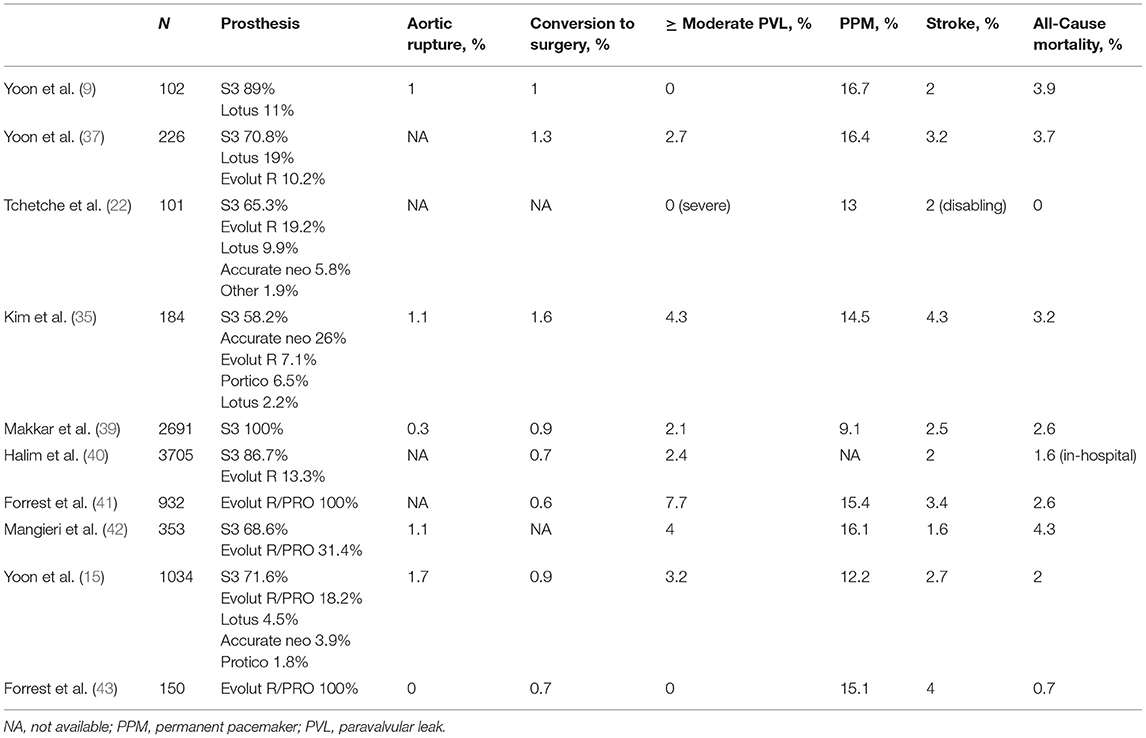
Table 1. Summarizes major published studies including >100 patients treated for bicuspid aortic valve (BAV) severe stenosis with the current generation of transcatheter heart valves.
The largest report comes from the STS/ACC TVT registry (40). BAV stenosis represented 3.2% of the 170,959 TAVI procedures performed between 2011 and 2018. Patients with BAV were younger (74 vs. 82 years old, p < 0.001, respectively) with a lower risk profile in comparison with those with tricuspid valves. Although the device success (using only current-generation devices) was slightly lower in BAV than tricuspid valves with a higher incidence of ≥ moderate aortic regurgitation, 1-year mortality and stroke risk were not affected. Indeed, patients with BAV had a lower 1-year adjusted mortality [hazard ratio (HR), 0.88 (95% CI, 0.78–0.99)] with similar adjusted stroke rate [HR, 1.14 (95% CI, 0.94–1.39)] in comparison with patients with a tricuspid valve (40). Caution should be paid when interpreting the results in light of a statistically significant difference in prosthesis type used in BAV and tricuspid valves. Indeed, the Sapien 3 (Edwards Lifesciences, CA, USA) prosthesis was more frequently used in BAV (73 vs. 69%, p < 0.001, respectively), but remained the most used prosthesis in both groups (40).
A second analysis from the STS/ACC TVT registry analyzed data from all patients treated with the third-generation Sapien 3 prosthesis (Edwards Lifesciences) between 2015 and 2018. Similar 30-day [2.6 vs. 2.5% (95% CI, 0.74–1.47), respectively], and 1-year mortality [10.5 vs. 12.0% (95% CI, 0.73–1.10), respectively], were reported among 2,691 matched pairs of BAV and tricuspid valves (39). Stroke rate was, however, higher [2.5 vs. 1.6% (95% CI, 1.06–2.33)] and patients with BAV required more frequent open heart surgery conversion in comparison with tricuspid valves [0.9 vs. 0.4%, respectively, absolute risk difference 0.5% (95% CI, 0–0.9%)]. No difference in ≥ moderate aortic regurgitation was, however, reported at 30 days between both groups (39). More recent results of this registry were presented at the EuroPCR congress 2021 reporting outcomes of the same 3,168 propensity match pairs. Authors confirmed similar adjusted 1-year mortality (12 vs. 10.5%, p = 0.31) between BAV and tricuspid valves. Even though the stroke rate was higher at 30 days in the BAV group (2.4 vs. 1.6%, p = 0.02, respectively for BAV and tricuspid valves), the difference was no longer true when considering adjusted results. One-year stroke rate was similar among matched patients (3.4 vs. 3.1%, p = 0.16, respectively) (44).
Similarly, Forrest et al. analyzed data from all patients treated with the Evolut R or PRO valves (Medtronic) included in the STS/ACC TVT registry between 2015 and 2018. One-year all-cause mortality and stroke rate were similar between 1,858 matched pairs of BAV and tricuspid valves (10.4 vs. 12.4%, p = 0.63 and 3.9 vs. 4.4%, p = 0.93, respectively) (41). Interestingly, patients with BAV had higher rate of ≥ moderate aortic regurgitation post-procedure (5.6 vs. 2.1%, p < 0.001) but this difference was no longer significant at 1-year follow-up (4.7 vs. 3.9%, p = 0.60) (41).
A recent large meta-analysis compared outcomes between BAV and tricuspid valve among 17 studies and 181,433 patients undergoing TAVI, including 6,669 patients with BAV (0.27%). While the device success and 1-year mortality were similar between BAV and tricuspid valves in the matched population (97 vs. 94%, p = 0.55 and 91 vs. 91%, p = 0.22, respectively), patients had higher incidence of cerebral ischemic events (2.4 vs. 1.6%, p = 0.015) as well as moderate to severe aortic regurgitation (relative risk 1.42, p < 0.0001). Patients treated for BAV presented more frequent procedural complications with higher rate of annular rupture (p = 0.014) or conversion to surgery (p = 0.018) (45).
Finally, at the 2021 TVT structural heart summit, data from PARTNER 3 TAVI BAV registry were presented comparing 148 matched pairs of patients with BAV and tricuspid valves. No difference in terms of death, stroke, or rehospitalization were reported at 1 year between both anatomies (10.9 vs. 10.2%, p = 0.8, respectively, for BAV vs. tricuspid valves) (46).
Substantial iterative technical development of TAVI devices, in addition to the increasing experience and better preprocedural planning of operators, allowed for outcome improvement in BAV patients treated with current-generation devices. Indeed, in the STS/ACC TVT registry, the use of current-generation devices translated into device success increase and aortic regurgitation decline (40). A similar increase in device success and decrease in the paravalvular leak was already described in an earlier but smaller bicuspid TAVI international registry comparing outcomes of early- vs. new-generation devices (47). In a propensity score-matched study (n = 546 pairs) by Yoon et al. comparing TAVI in BAV vs. tricuspid valves, device success as well as mortality up to 2 years (17.2 vs. 19.4%, p = 0.28, respectively), was similar in patients receiving current generation devices (37).
Whereas, most of TAVI procedural complications and clinical outcomes in tricuspid aortic valve stenosis have significantly improved over time to reach non-inferiority if not superiority in comparison with surgery, high-grade conduction disorders remain a major issue post-TAVI. Several predictors of new permanent pacemaker implantation in tricuspid valves have been identified. Patient (such as baseline conduction disorders and aortic annulus anatomical characteristics) and procedural (such as, prosthesis oversizing, type, and implantation depth) characteristics are associated with an increased risk of high-grade conduction disorders (48, 49). The impact of valve morphology (BAV vs. tricuspid valves) on the new permanent pacemaker implantation rate is still controversial with conflicting results. Shorter membranous septum or asymmetrical radial forces of the prosthesis compressing the conduction system in BAV have been suggested as risk factors for conduction disorders (50). In the large STS/ACC TVT registry, permanent pacemaker implantation rate was slightly but significantly higher among the BAV matched to tricuspid valve patients (7.3 vs. 5.9%, p = 0.05, respectively), treated by the third generation Sapien 3 (Edwards Lifesciences) prosthesis (39). The difference became higher (9.1 vs. 7.5%, p = 0.03) in the recent up-to-date data presented at the 2021 EuroPCR congress (44). These results are in opposition to a recent meta-analysis including 19 studies (4,040 BAV vs. 8,084 tricuspid valves) where authors reported similar new permanent pacemaker implantation rates between both groups [risk ratio 1.06 (95% CI, 0.93–1.20)] (51). Device type (self-expandable vs. balloon-expandable) seems not to influence the pacemaker implantation rate among new-generation devices. Indeed, in the BEAT (balloon vs. self-expandable valve for the treatment of bicuspid aortic valve stenosis) international registry, BAV treated with self-expandable Evolut R/PRO (n = 111), or balloon-expandable Sapien 3 (n = 242) prosthesis were compared. The rate of permanent pacemaker was similar in both groups (16.0 vs. 16.1%, p = 0.98, respectively, for self- vs. balloon-expandable devices) (42). Interestingly, results remained similar after propensity-score matching. Higher rates of permanent pacemaker implantation were reported by Jilaihawi but, here again, with similar rates between self- and balloon-expandable devices (26.9 vs. 25.5%, p = 0.83, respectively) (14).
Technical Considerations for TAVI in BAV
Specific technical considerations related to the different valve morphology and physiopathology in BAV are considered when considering TAVI. BAV opening orifice eccentricity increases the difficulty of retrograde valve crossing in case of severe stenosis. Fine analysis of MSCT pre-procedural imaging may help to identify the fused cusps and predict the location of wire crossing. A step-by-step approach has been suggested by Frangieh and Kasel starting from the non-fused cusp and rotating the catheter clockwise or counter-clockwise in case of left-right or non-right types, respectively (52). In case of no raphe type, no specific rule exists. When retrograde valve crossing remains impossible, transseptal puncture with anterograde aortic valve crossing can be performed.
Asymmetrical and increased burden of calcium deposition, and non-circular shape of BAV increase the risk of device malpositioning during the prosthesis deployment as well as the risk of annular rupture. Non-circular or valve underexpansion has been documented by imaging studies in BAV treated with both self- and balloon-expandable devices (53, 54). Use of the 2 orthogonal views after prosthesis implantation helps to identify the stent frame underexpansion that may be missed with a single fluoroscopic projection. The impact of prosthesis eccentricity on long-term valve function remains unestablished yet with no difference in hemodynamic parameters at short-term (17). In the BIVOLUT-X registry, systematic pre-dilatation (87% of the cases) and post-dilatation according to the angiography appearance of the prosthesis (55%) in BAV have shown favorable ellipticity index (1.2) with encouraging hemodynamic parameters of the self-expandable prosthesis at 30 days (mean gradient of 7.3 mmHg and ≥moderate paravalvular leak in 2% of the patients) (55). However, these anatomical challenges are to be better targeted in light of the higher rate of second valve implanted in BAV vs. tricuspid valves in the large STS/ACC TVT registry (40). The use of a recapturable device may here be a special interest in case of predicted challenging prosthesis deployment. Pre- and post-dilatation may help in optimizing the prosthesis landing zone at the price of an increased risk of annular rupture and stroke. In different analyses of the STS/ACC registry, the rate of conversion to open surgery was higher in BAV vs. tricuspid valves when a balloon-expandable device was used (0.9 vs. 0.4%, p = 0.03, respectively), whereas no significant difference was reported with self-expandable devices (0.6 vs. 0.2%, p = 0.29, respectively) (39, 41). When comparing self- to balloon-expandable devices in BAV, the BEAT registry reported higher rate of pre- and post-dilatation with self-expandable prosthesis (pre-dilatation: 57.3 vs. 37.9%; post-dilatation: 42.7 vs. 14.3%; p < 0.001 for both) (42). Balloon post-dilatation should be limited to cases with significant prosthesis dysfunction, including more than the mild paravalvular leak or mean gradient >15 mmHg. Indication for post-dilatation of non-circular valve geometry without a hemodynamic impact needs further investigations with long-term data on valve performances and leaflet thrombosis.
A horizontal aorta is frequently associated with BAV and may interfere with both retrograde valve crossing and prosthesis deployment (27). Although different techniques have been described to facilitate the valve crossing or delivery system orientation (56, 57), alternative accesses (transcarotid or axillary as the first alternative choices) can be decided at the time of pre-procedural planning (58).
Coronary re-access following TAVI in BAV is of particular interest according to the younger age of patients developing severe aortic stenosis in BAV in comparison with the tricuspid valve. However, similarly to tricuspid valves, no clear recommendation on commissural alignment during the prosthesis deployment exists yet. Eccentric coronary ostia in the leaflet as well as anomalous coronary origin may significantly complicate commissural alignment and thus coronary re-access in the future.
Future Perspectives And Conclusions
Data coming from specific designed randomized studies are needed to confirm the results of registries. To date, the NOTION-2 trial (NCT02825134) is randomizing low-risk patients with severe aortic stenosis to surgery or TAVI, such as BAV. A Chinese randomized non-inferiority trial (NCT03163329) comparing long-term results of TAVI and surgery in BAV is ongoing and results are expected by the middle of 2024. Long-term data assessing prosthesis hemodynamic performances over time are still lacking. Incomplete stent expansion or prosthesis distortion may influence the prosthesis durability and follow-up studies focusing on the structural valve failure and valve thrombosis become primordial with respect to the low-risk population of patients with BAV. Figure 4 suggests a treatment algorithm of patients with symptomatic severe BAV stenosis.
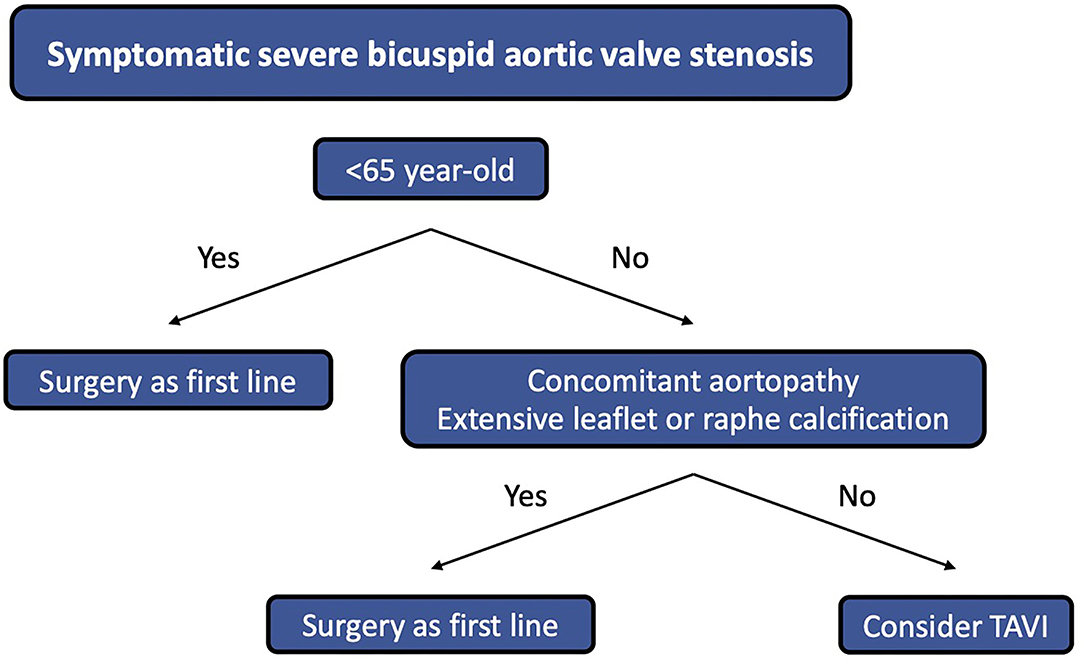
Figure 4. Treatment algorithm of patients with symptomatic severe BAV stenosis.
Bicuspid aortic valve is frequently associated with ascending aortopathy, such as aortic root and proximal ascending aorta dilatation. Currently, TAVI addresses only BAV stenosis and surgery remains the only option to treat the associated ascending aortopathy. The recent ESC guidelines recommend aortic root/proximal ascending aorta replacement in case of a diameter ≥ 45 mm when surgery is planned for BAV severe stenosis (24). If those patients are deemed inoperable, TAVI may be considered for the aortic stenosis, taking into account the higher risk of aortic dissection in this setting (59, 60). Whereas, it is well-known that aortic root dilatation progresses with time in BAV, the rate of progression after TAVI remains unknown. Protheses treating aortic valve and ascending aortopathy simultaneously (Endo-Bentall) are under development with encouraging first-in-man cases, however, reserved for compassionate use yet (61).
In conclusion, BAV stenosis has distinct anatomical characteristics in comparison with tricuspid valves leading to specific aortic root distortion. Several sub-types classifications have been developed over time to better address the therapeutic options. When TAVI is considered for BAV, pre-procedural MSCT imaging is essential to assess the number of cusps, presence of a raphe, and location of calcifications. Aortic root, such as supra-annular structures, should be integrated in the device selection and sizing process as prosthesis interaction with the aortic root can occur from the level of the left ventricular outflow tract to above the sinotubular junction. Favorable clinical and safety outcomes have been reported from large international registries with similar outcomes in comparison with tricuspid valves. However, data from randomized trials are needed.
Author Contributions
NP contributed to the design of the review and writing of the manuscript. RI, ND, AB, LL, PD, and TM revised the manuscript. WB contributed to the design of the review and reviewed critically the manuscript. All authors contributed to the article and approved the submitted version.
Funding
NP has received research support from the Swiss National Science Foundation (P400PM_194483) and the Geneva University Hospitals.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Adams DH, Popma JJ, Reardon MJ. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. (2014) 371:967–8. doi: 10.1056/NEJMc1408396
2. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. (2010) 363:1597–607. doi: 10.1056/NEJMoa1008232
3. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med. (2019) 380:1695–705. doi: 10.1056/NEJMoa1814052
4. Makkar RR, Thourani VH, Mack MJ, Kodali SK, Kapadia S, Webb JG, et al. Five-Year outcomes of transcatheter or surgical aortic-valve replacement. N Engl J Med. (2020) 382:799–809. doi: 10.1056/NEJMoa1910555
5. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O'Hair D, et al. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N Engl J Med. (2019) 380:1706–15. doi: 10.1056/NEJMoa1816885
6. Reardon MJ, Van Mieghem NM, Popma JJ, Kleiman NS, Sondergaard L, Mumtaz M, et al. Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J Med. (2017) 376:1321–31. doi: 10.1056/NEJMoa1700456
7. Roberts WC, Janning KG, Ko JM, Filardo G, Matter GJ. Frequency of congenitally bicuspid aortic valves in patients ≥80 years of age undergoing aortic valve replacement for aortic stenosis (with or without aortic regurgitation) and implications for transcatheter aortic valve implantation. Am J Cardiol. (2012) 109:1632–6. doi: 10.1016/j.amjcard.2012.01.390
8. Hira RS, Vemulapalli S, Li Z, McCabe JM, Rumsfeld JS, Kapadia SR, et al. Trends and outcomes of off-label use of transcatheter aortic valve replacement: insights from the NCDR STS/ACC TVT registry. JAMA Cardiol. (2017) 2:846–54. doi: 10.1001/jamacardio.2017.1685
9. Yoon SH, Ahn JM, Hayashida K, Watanabe Y, Shirai S, Kao HL, et al. Clinical outcomes following transcatheter aortic valve replacement in asian population. JACC Cardiovasc Interv. (2016) 9:926–33. doi: 10.1016/j.jcin.2016.01.047
10. Sievers HH, Schmidtke C. A classification system for the bicuspid aortic valve from 304 surgical specimens. J Thorac Cardiovasc Surg. (2007) 133:1226–33. doi: 10.1016/j.jtcvs.2007.01.039
11. Michelena HI, Prakash SK, Della Corte A, Bissell MM, Anavekar N, Mathieu P, et al. Bicuspid aortic valve: identifying knowledge gaps and rising to the challenge from the international bicuspid aortic valve consortium (BAVCon). Circulation. (2014) 129:2691–704. doi: 10.1161/CIRCULATIONAHA.113.007851
12. de Kerchove L, Mastrobuoni S, Froede L, Tamer S, Boodhwani M, van Dyck M, et al. Variability of repairable bicuspid aortic valve phenotypes: towards an anatomical and repair-oriented classification. Eur J Cardiothorac Surg. (2019) 56:351–9. doi: 10.1093/ejcts/ezz033
13. Michelena HI, Della Corte A, Evangelista A, Maleszewski JJ, Edwards WD, Roman MJ, et al. International consensus statement on nomenclature and classification of the congenital bicuspid aortic valve and its aortopathy, for clinical, surgical, interventional and research purposes. J Thorac Cardiovasc Surg. (2021) 162:e383–414. doi: 10.1016/j.jtcvs.2021.06.019
14. Jilaihawi H, Chen M, Webb J, Himbert D, Ruiz CE, Rodes-Cabau J, et al. A bicuspid aortic valve imaging classification for the TAVR Era. JACC Cardiovasc Imaging. (2016) 9:1145–58. doi: 10.1016/j.jcmg.2015.12.022
15. Yoon SH, Kim WK, Dhoble A, Milhorini Pio S, Babaliaros V, Jilaihawi H, et al. Bicuspid aortic valve morphology and outcomes after transcatheter aortic valve replacement. J Am Coll Cardiol. (2020) 76:1018–30. doi: 10.1016/j.jacc.2020.07.005
16. van Rosendael PJ, Kamperidis V, Kong WK, van Rosendael AR, Marsan NA, Bax JJ, et al. Comparison of quantity of calcific deposits by multidetector computed tomography in the aortic valve and coronary arteries. Am J Cardiol. (2016) 118:1533–8. doi: 10.1016/j.amjcard.2016.08.021
17. Kawamori H, Yoon SH, Chakravarty T, Maeno Y, Kashif M, Israr S, et al. Computed tomography characteristics of the aortic valve and the geometry of SAPIEN 3 transcatheter heart valve in patients with bicuspid aortic valve disease. Eur Heart J Cardiovasc Imaging. (2018) 19:1408–18. doi: 10.1093/ehjci/jex333
18. Hope MD, Wrenn J, Sigovan M, Foster E, Tseng EE, Saloner D. Imaging biomarkers of aortic disease: increased growth rates with eccentric systolic flow. J Am Coll Cardiol. (2012) 60:356–7. doi: 10.1016/j.jacc.2012.01.072
19. Bissell MM, Hess AT, Biasiolli L, Glaze SJ, Loudon M, Pitcher A, et al. Aortic dilation in bicuspid aortic valve disease: flow pattern is a major contributor and differs with valve fusion type. Circ Cardiovasc Imaging. (2013) 6:499–507. doi: 10.1161/CIRCIMAGING.113.000528
20. Naito S, Petersen J, Reichenspurner H, Girdauskas E. The impact of coronary anomalies on the outcome in aortic valve surgery: comparison of bicuspid aortic valve versus tricuspid aortic valve morphotype. Interact Cardiovasc Thorac Surg. (2018) 26:617–22. doi: 10.1093/icvts/ivx396
21. Michalowska IM, Hryniewiecki T, Kwiatek P, Stoklosa P, Swoboda-Rydz U, Szymanski P. Coronary artery variants and anomalies in patients with bicuspid aortic valve. J Thorac Imaging. (2016) 31:156–62. doi: 10.1097/RTI.0000000000000205
22. Tchetche D, de Biase C, van Gils L, Parma R, Ochala A, Lefevre T, et al. Bicuspid aortic valve anatomy and relationship with devices: the BAVARD multicenter registry. Circ Cardiovasc Interv. (2019) 12:e007107. doi: 10.1161/CIRCINTERVENTIONS.118.007107
23. Cramer PM, Prakash SK. Misclassification of bicuspid aortic valves is common and varies by imaging modality and patient characteristics. Echocardiography. (2019) 36:761–5. doi: 10.1111/echo.14295
24. Vahanian A, Beyersdorf F, Praz F, Milojevic M, Baldus S, Bauersachs J, et al. 2021 ESC/EACTS guidelines for the management of valvular heart disease. Eur Heart J. (2021) ehab395. doi: 10.1093/eurheartj/ehab395. [Epub ahead of print].
25. Michelena HI, Chandrasekaran K, Topilsky Y, Messika-Zeitoun D, Della Corte A, Evangelista A, et al. The bicuspid aortic valve condition: the critical role of echocardiography and the case for a standard nomenclature consensus. Prog Cardiovasc Dis. (2018) 61:404–15. doi: 10.1016/j.pcad.2018.11.003
26. Tanaka R, Yoshioka K, Niinuma H, Ohsawa S, Okabayashi H, Ehara S. Diagnostic value of cardiac CT in the evaluation of bicuspid aortic stenosis: comparison with echocardiography and operative findings. AJR Am J Roentgenol. (2010) 195:895–9. doi: 10.2214/AJR.09.3164
27. Philip F, Faza NN, Schoenhagen P, Desai MY, Tuzcu EM, Svensson LG, et al. Aortic annulus and root characteristics in severe aortic stenosis due to bicuspid aortic valve and tricuspid aortic valves: implications for transcatheter aortic valve therapies. Catheter Cardiovasc Interv. (2015) 86:E88–98. doi: 10.1002/ccd.25948
28. Blanke P, Willson AB, Webb JG, Achenbach S, Piazza N, Min JK, et al. Oversizing in transcatheter aortic valve replacement, a commonly used term but a poorly understood one: dependency on definition and geometrical measurements. J Cardiovasc Comput Tomogr. (2014) 8:67–76. doi: 10.1016/j.jcct.2013.12.020
29. Dvir D, Webb JG, Piazza N, Blanke P, Barbanti M, Bleiziffer S, et al. Multicenter evaluation of transcatheter aortic valve replacement using either SAPIEN XT or CoreValve: degree of device oversizing by computed-tomography and clinical outcomes. Catheter Cardiovasc Interv. (2015) 86:508–15. doi: 10.1002/ccd.25823
30. Liu X, He Y, Zhu Q, Gao F, He W, Yu L, et al. Supra-annular structure assessment for self-expanding transcatheter heart valve size selection in patients with bicuspid aortic valve. Catheter Cardiovasc Interv. (2018) 91:986–94. doi: 10.1002/ccd.27467
31. Xiong TY, Feng Y, Li YJ, Zhao ZG, Liao YB, Ou Y, et al. Supra-Annular sizing for transcatheter aortic valve replacement candidates with bicuspid aortic valve. JACC Cardiovasc Interv. (2018) 11:1789–90. doi: 10.1016/j.jcin.2018.06.002
32. Xiong TY, Li YJ, Feng Y, Liao YB, Zhao ZG, Mylotte D, et al. Understanding the interaction between transcatheter aortic valve prostheses and supra-annular structures from post-implant stent geometry. JACC Cardiovasc Interv. (2019) 12:1164–71. doi: 10.1016/j.jcin.2019.02.051
33. Iannopollo G, Romano V, Buzzatti N, De Backer O, Sondergaard L, Merkely B, et al. A novel supra-annular plane to predict TAVI prosthesis anchoring in raphe-type bicuspid aortic valve disease: the LIRA plane. EuroIntervention. (2020) 16:259–61. doi: 10.4244/EIJ-D-19-00951
34. Petronio AS, Angelillis M, De Backer O, Giannini C, Costa G, Fiorina C, et al. Bicuspid aortic valve sizing for transcatheter aortic valve implantation: development and validation of an algorithm based on multi-slice computed tomography. J Cardiovasc Comput Tomogr. (2020) 14:452–61. doi: 10.1016/j.jcct.2020.01.007
35. Kim WK, Renker M, Rolf A, Fischer-Rasokat U, Wiedemeyer J, Doss M, et al. Annular versus supra-annular sizing for TAVI in bicuspid aortic valve stenosis. EuroIntervention. (2019) 15:e231–8. doi: 10.4244/EIJ-D-19-00236
36. Siu SC, Silversides CK. Bicuspid aortic valve disease. J Am Coll Cardiol. (2010) 55:2789–800. doi: 10.1016/j.jacc.2009.12.068
37. Yoon SH, Bleiziffer S, De Backer O, Delgado V, Arai T, Ziegelmueller J, et al. Outcomes in transcatheter aortic valve replacement for bicuspid versus tricuspid aortic valve stenosis. J Am Coll Cardiol. (2017) 69:2579–89. doi: 10.1016/j.jacc.2017.03.017
38. Mentias A, Sarrazin MV, Desai MY, Saad M, Horwitz PA, Kapadia S, et al. Transcatheter versus surgical aortic valve replacement in patients with bicuspid aortic valve stenosis. J Am Coll Cardiol. (2020) 75:2518–9. doi: 10.1016/j.jacc.2020.02.069
39. Makkar RR, Yoon SH, Leon MB, Chakravarty T, Rinaldi M, Shah PB, et al. Association between transcatheter aortic valve replacement for bicuspid vs tricuspid aortic stenosis and mortality or stroke. JAMA. (2019) 321:2193–202. doi: 10.1001/jama.2019.7108
40. Halim SA, Edwards FH, Dai D, Li Z, Mack MJ, Holmes DR, et al. Outcomes of transcatheter aortic valve replacement in patients with bicuspid aortic valve disease: a report from the society of thoracic surgeons/American college of cardiology transcatheter valve therapy registry. Circulation. (2020) 141:1071–9. doi: 10.1161/CIRCULATIONAHA.119.040333
41. Forrest JK, Kaple RK, Ramlawi B, Gleason TG, Meduri CU, Yakubov SJ, et al. Transcatheter aortic valve replacement in bicuspid versus tricuspid aortic valves from the STS/ACC TVT registry. JACC Cardiovasc Interv. (2020) 13:1749–59. doi: 10.1016/j.jcin.2020.03.022
42. Mangieri A, Tchetche D, Kim WK, Pagnesi M, Sinning JM, Landes U, et al. Balloon versus self-expandable valve for the treatment of bicuspid aortic valve stenosis: insights from the BEAT international collaborative registrys. Circ Cardiovasc Interv. (2020) 13:e008714. doi: 10.1161/CIRCINTERVENTIONS.119.008714
43. Forrest JK, Ramlawi B, Deeb GM, Zahr F, Song HK, Kleiman NS, et al. Transcatheter aortic valve replacement in low-risk patients with bicuspid aortic valve stenosis. JAMA Cardiol. (2021) 6:50–7. doi: 10.1001/jamacardio.2020.4738
44. Makkar R. Outcomes of Transcatheter Aortic Valve Replacement for Bicuspid Aortic Valve Stenosis in the Low-Surgical Risk Population. Paris: EuroPCR (2021).
45. Montalto C, Sticchi A, Crimi G, Laricchia A, Khokhar AA, Giannini F, et al. Outcomes after transcatheter aortic valve replacement in bicuspid versus tricuspid anatomy: a systematic review and meta-analysis. JACC Cardiovasc Interv. (2021) 14:2144–55. doi: 10.1016/j.jcin.2021.07.052
46. Webb J, Williams M. The PARTNER 3 Bicuspid Registry for SAPIEN 3 TAVR in Low-risk Patients. Miami: TVT structural heart (2021).
47. Yoon SH, Lefevre T, Ahn JM, Perlman GY, Dvir D, Latib A, et al. Transcatheter aortic valve replacement with early- and new-generation devices in bicuspid aortic valve stenosis. J Am Coll Cardiol. (2016) 68:1195–205. doi: 10.1016/j.jacc.2016.06.041
48. Husser O, Pellegrini C, Kessler T, Burgdorf C, Thaller H, Mayr NP, et al. Predictors of permanent pacemaker implantations and new-onset conduction abnormalities with the SAPIEN 3 balloon-expandable transcatheter heart valve. JACC Cardiovasc Interv. (2016) 9:244–54. doi: 10.1016/j.jcin.2015.09.036
49. Siontis GC, Juni P, Pilgrim T, Stortecky S, Bullesfeld L, Meier B, et al. Predictors of permanent pacemaker implantation in patients with severe aortic stenosis undergoing TAVR: a meta-analysis. J Am Coll Cardiol. (2014) 64:129–40. doi: 10.1016/j.jacc.2014.04.033
50. Hamdan A, Nassar M, Schwammenthal E, Perlman G, Arow Z, Lessick J, et al. Short membranous septum length in bicuspid aortic valve stenosis increases the risk of conduction disturbances. J Cardiovasc Comput Tomogr. (2021) 15:339–47. doi: 10.1016/j.jcct.2020.10.002
51. Majmundar M, Kumar A, Doshi R, Shah P, Arora S, Shariff M, et al. Meta-Analysis of transcatheter aortic valve implantation in patients with stenotic bicuspid versus tricuspid aortic valve. Am J Cardiol. (2021) 145:102–10. doi: 10.1016/j.amjcard.2020.12.085
52. Frangieh AH, Kasel AM. TAVI in bicuspid aortic valves 'made easy'. Eur Heart J. (2017) 38:1177–81. doi: 10.1093/eurheartj/ehx167
53. Himbert D, Pontnau F, Messika-Zeitoun D, Descoutures F, Detaint D, Cueff C, et al. Feasibility and outcomes of transcatheter aortic valve implantation in high-risk patients with stenotic bicuspid aortic valves. Am J Cardiol. (2012) 110:877–83. doi: 10.1016/j.amjcard.2012.04.064
54. Perlman GY, Blanke P, Dvir D, Pache G, Modine T, Barbanti M, et al. Bicuspid aortic valve stenosis: favorable early outcomes with a next-generation transcatheter heart valve in a multicenter study. JACC Cardiovasc Interv. (2016) 9:817–24. doi: 10.1016/j.jcin.2016.01.002
55. De Biase C, on on behalf to the Bivolut-X registry. Transcatheter Treatment of Bicuspid Valves With the Evolut Platform: Interim Analysis From the BIVOLUT-X Registry. London: PCR London Valves (2019).
56. Noble S, Roffi M. Retrograde aortic valve crossing of the CoreValve prosthesis using the buddy balloon technique. Catheter Cardiovasc Interv. (2014) 84:897–9. doi: 10.1002/ccd.25215
57. Sarkar K, Ussia GP, Tamburino C. Trans catheter aortic valve implantation with core valve revalving system in uncoiled (horizontal) aorta. Overcoming anatomical and technical challenges for successful deployment. Catheter Cardiovasc Interv. (2011) 78:964–9. doi: 10.1002/ccd.23133
58. Perrin Nils GB, Leroux L, Ibrahim R, Modine T, Ben Ali W. transcatheter aortic valve implantation: all transfemoral? Front Cardiovasc Med. (2021) 8:747583. doi: 10.3389/fcvm.2021.747583
59. Jacobzon E, Wolak A, Fink D, Silberman S. Delayed aortic dissection and valve thrombosis after transcatheter aortic valve implantation. Catheter Cardiovasc Interv. (2019) 93:E391–3. doi: 10.1002/ccd.27994
60. Rylski B, Szeto WY, Bavaria JE, Walsh E, Anwaruddin S, Desai ND, et al. Transcatheter aortic valve implantation in patients with ascending aortic dilatation: safety of the procedure and mid-term follow-updagger. Eur J Cardiothorac Surg. (2014) 46:228–33; discussion 33. doi: 10.1093/ejcts/ezt594
Keywords: bicuspid aortic valve stenosis bicuspid aortic valve, nomenclature, transcatheter aortic valve implantation, sizing approaches, review
Citation: Perrin N, Ibrahim R, Dürrleman N, Basmadjian A, Leroux L, Demers P, Modine T and Ben Ali W (2022) Bicuspid Aortic Valve Stenosis: From Pathophysiological Mechanism, Imaging Diagnosis, to Clinical Treatment Methods. Front. Cardiovasc. Med. 8:798949. doi: 10.3389/fcvm.2021.798949
Received: 20 October 2021; Accepted: 28 December 2021;
Published: 08 February 2022.
Edited by:
Mao Chen, Sichuan University, ChinaReviewed by:
Nicolas Amabile, L'Institut Mutualiste Montsouris, FranceAdel Aminian, Centre Hospitalier Universitaire de Charleroi, Belgium
Copyright © 2022 Perrin, Ibrahim, Dürrleman, Basmadjian, Leroux, Demers, Modine and Ben Ali. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Walid Ben Ali, dr.walidbenali@gmail.com