
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Cardiovasc. Med., 17 January 2022
Sec. Cardiac Rhythmology
Volume 8 - 2021 | https://doi.org/10.3389/fcvm.2021.787235
This article is part of the Research TopicNew Horizons in the Management of Patients with Atrial Fibrillation: Interactions with the gastrointestinal systemView all 6 articles
 Ana Sánchez-Fuentes1
Ana Sánchez-Fuentes1 José Miguel Rivera-Caravaca2,3*
José Miguel Rivera-Caravaca2,3* Raquel López-Gálvez2
Raquel López-Gálvez2 Francisco Marín2†
Francisco Marín2† Vanessa Roldán1†
Vanessa Roldán1†Non-vitamin K antagonist oral anticoagulants (NOACs) are a therapeutic option to prevent stroke in patients with atrial fibrillation (AF). In fact, NOACs have become the recommended choice by international clinical practice guidelines over vitamin K antagonists (VKA), because of their efficacy and safety profile, especially in newly initiated patients. The more predictable pharmacokinetic and pharmacodynamic profile of this family of drugs allows preventing anticoagulation drug monitoring. Furthermore, NOACs have significantly fewer drug and food interactions in comparison with VKAs. Despite this, there are no studies that compare the effects on the quality of anticoagulation of NOACs with the intake of potential interactions drugs of P-glycoprotein and cytochrome P450 (CYP). This review brings an overview of NOACs pharmacokinetics profile and their potential drug-food interactions. We also briefly discuss the potential role of prebiotics and probiotics in patients under therapy with NOACs.
Non-vitamin K antagonist oral anticoagulants (NOACs), including rivaroxaban, apixaban and edoxaban as factor Xa inhibitors, and dabigatran etexilate as a thrombin inhibitor, are the first-line treatment for most patients with venous thromboembolism (VTE) and for stroke prevention in atrial fibrillation (AF) (1–3).
It is well known that NOACs have a lower propensity for drug and food interactions compared to vitamin K antagonists (VKAs), due to their individual coagulation proteins target and to the administration in fixed-dose without requiring routine coagulation monitoring (4). Even though, variations in NOACs concentration may occur with the concomitant use of inducers or inhibitors of P-glycoprotein (P-gp) and cytochrome P450 (CYP) 3A4, thus increasing thrombotic and bleeding risk, respectively (5–8).
To date, there is scarce evidence about the potential interactions of herbal products, dietary supplements, and food with NOACs. Moreover, the use of probiotics and prebiotics is currently increasing due to their multiple benefits described in the human body, but it is unclear whether probiotics and prebiotics might have a potential influence on NOACs pharmacokinetic parameters (9). The aim of this mini-review article is to summarize the present knowledge on potential drug-food/herbal products interactions of NOACs and the potential implications of increased use of products such as probiotics and prebiotics.
A summary of the different stages of NOACs pharmacology is shown in Table 1.
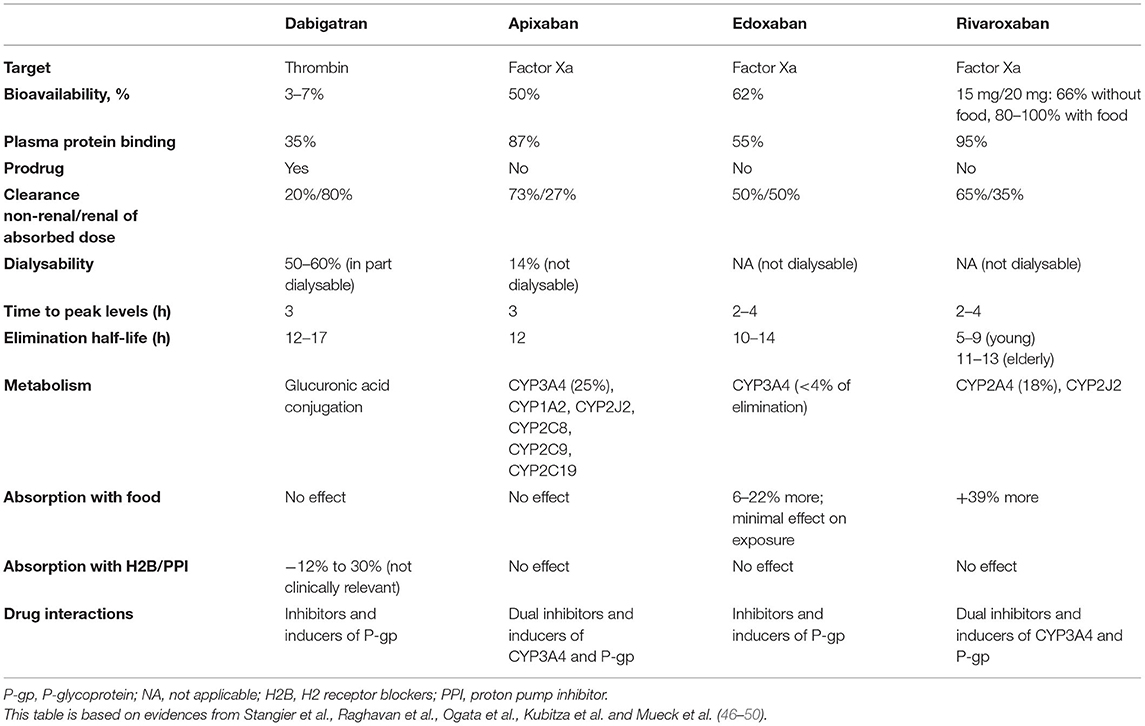
Table 1. Pharmacological properties of non-vitamin K antagonist oral anticoagulants (NOACs).
VKAs have several interactions with foods and herbal supplements (10, 11). These interactions can significantly increase the risk of thromboembolic and bleeding events due to phenomena of over or under anticoagulation (8, 11). The introduction of NOACs has partly solved this problem. Despite this family of drugs presents fewer drug-food interactions compared to VKAs, they are not free of potential interactions, and therefore some international guidelines suggest considerations with some herbal medicines or food that can affect plasma levels of NOACs (12).
Metabolism and elimination pathways of NOACs depend on the intestinal transporter P-gp (for dabigatran, apixaban, edoxaban and rivaroxaban) and the CYP3A4-type cytochrome P450 (for apixaban and rivaroxaban) (13, 14).
Firstly, P-gp transporters are efflux carriers that can be found in different epithelia of the human body, highlighting their presence and function in the luminal membrane of the small intestine, proximal renal tubules or hepatocytes (15). P-gp is essential for gastrointestinal resecretion after intestinal absorption, and it is also actively involved in the renal secretion of NOACs (12, 16). Because P-gp has high transport capacity but low specificity for different substrates, competitive inhibition or induction of the P-gp pathway will affect plasma concentration of those drugs that share the same metabolic pathway (15, 17).
Secondly, cytochrome P450, specifically isoenzyme CYP3A4, is essential for the hepatic elimination of some NOACs (apixaban and rivaroxaban) (16). Regarding clearance of other foreign substances, most of them depend on CYP1, 2, and 3 families, although up to 57 functional CYPs have been described in the human body (18). As in case of P-gp, strong inhibition or induction of CYP3A4 can affect plasma levels of NOACs (19). Thus, modifications in these metabolic pathways in the presence of certain foods and drugs could influence plasma NOACs concentrations and the safety of treated patients if the therapeutic objective is not reached (13, 14). Therefore, strong inducers or inhibitors of P-gp and CYP3A4 should be used carefully or even avoided with the concomitant intake of NOACs (20) (Figure 1).
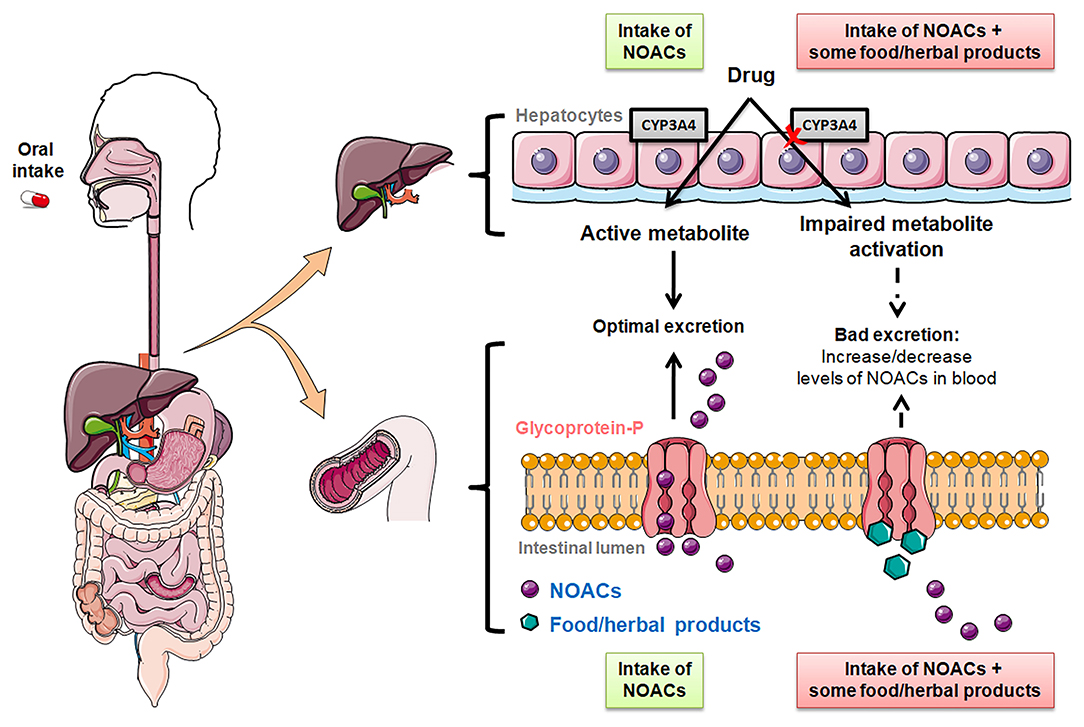
Figure 1. Effect of the intake of food/herbal products on the metabolization of NOACs. Elimination of NOAC mediated by P-glycoprotein and cytochrome P450 (CYP) 3A4 in the intestinal lumen and liver.
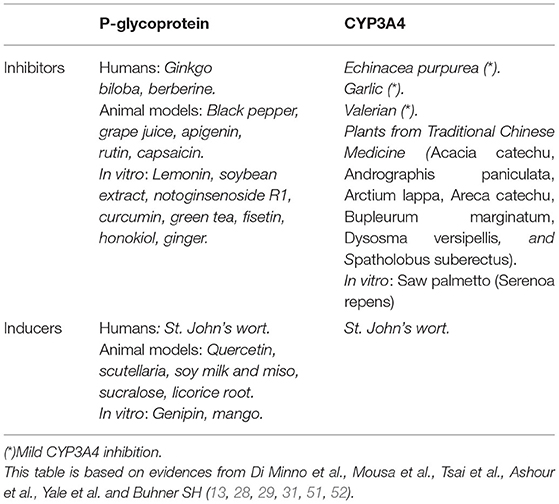
Although food and herbal inducers or inhibitors of P-gp or CYP3A4 are supposed to interfere with the pharmacokinetics of NOACs (see Table 2), no direct association of these interactions is available in humans and in vivo studies (5). Limited evidence showed that rivaroxaban bioavailability improves when the drug is taken with food (21, 22), so that it is recommended to take it with food. However, food intake does not influence the bioavailability of the other NOACs.
On the other hand, although there is no evidence from clinical studies, it has been proposed that grapefruit could influence the bioavailability of rivaroxaban (12, 13, 21–26). Another example is St. John's wort, a known potent inducer of P-gp and CYP3A4. Therefore, it is expected that NOACs, as substrates of P-gp (all of them) and CYP3A4 (rivaroxaban and apixaban), have lower plasma levels with the concomitant intake of St. John's wort, which potentially increases stroke risk (13). Thus, co-administration of this herbalist product with apixaban and edoxaban should be made with caution, and even avoided with rivaroxaban and dabigatran (13, 27). On the contrary, some herbal medicines and foods have antiplatelet and anticoagulation effects, such as garlic, ginger, ginkgo Biloba, ginseng, green tea, or horse chestnut (13, 28, 29). Nowadays, there is not enough information available to confirm possible interactions between these herbal products/foods and NOACs. Even so, as a preventive measure, caution should be exercised in patients with risk factors for bleeding or polypharmacy (17).
But importantly, it should be noted that several food and herbal products with potential interactions with NOACs are common and easily accessible. A recent study involving patients taking apixaban demonstrated that the prevalence of use of over-the-counter products (i.e., Chinese herbs [including products such as danshen, dong quai, and ginseng], ginger, ginkgo biloba, herbal teas [including green and chamomile tea], St. John's wort, and turmeric) with potentially serious apixaban interactions, was high. The most common dietary supplements with potential apixaban interactions of increased bleeding were herbal teas and turmeric. Of note, less knowledge about over-the-counter products with potentially serious interactions was associated with greater use of these products (OR 0.54; 95% CI 0.35–0.85) (30). However, this study did not report association regarding potential adverse events with concomitant use of over-the-counter products and apixaban. Such results could be relevant since in vitro studies have demonstrated that widely used plants from Traditional Chinese Medicine may inhibit CYP3A4, some of them in a proportion higher than 85% when used at a dose of at least 100 μg/mL (31).
Notwithstanding this is a field still to be explored that requires further studies. Indeed, the available evidence is currently so limited that it is not possible to give firm advices. In this regard, some previous manuscripts -mostly case studies, have hypothesized the potential interaction of herbal products and NOACs. A case study reported an isolated hemopericardium in a patient with AF taking rivaroxaban. The authors suggested that a possible contributor to hemopericardium could be the concomitant use of saw palmetto, an herbal medication from the extract of the berries of Serenoa repens/Serenoa serrulata commonly used for symptom relief in benign prostate hyperplasia, which may inhibit CYP3A4 activity (32). More recently, a report introduced a case of a patient presenting severe (and fatal) gastrointestinal bleeding after the self-administration of a boiled mixture of ginger and cinnamon twice daily for 3 days in concomitant use with dabigatran. Ginger is a P-gp inhibitor, which may increase dabigatran concentration, whereas Cassia cinnamon (the most common one) is considered a rich source of coumarin. Thus, Ginger and cinnamon taken together with dabigatran, in this case, might increase dabigatran levels and also add a second oral anticoagulant (coumarin) to dabigatran, thus significantly increasing the risk of bleeding (33). In the same line, Gressenberger and collaborators published a case of a young male patient under rivaroxaban due to recurrent spontaneous deep vein thrombosis and a heterozygous Factor-V-Leiden mutation which presented sudden onset of hemoptysis. The patient was not taking any other concomitant medication which may justify the bleeding, but reported a constant intake of three liters of home-brewn ginger tea per day during the last month (34).
In summary, strong P-gp and CYP3A4 inducers and inhibitors should be avoided concomitant to NOACs. In the case of mild potential pharmacodynamic interactions, special care is needed particularly in high-risk patient groups. Patients who develop bleeding or thromboembolic events during NOAC therapy should be investigated for co-medications, intake of herbal drugs, and dietary habits (13). Pharmacokinetic interactions of accompanying drugs need to be considered when prescribing NOACs.
Gut microbiota is shaped by a large ecosystem of microorganisms that live or move through the skin, genitourinary, gastrointestinal and respiratory tracts (35). It has been related to very relevant roles in the human body, highlighting its benefits in immunological, nutritional and metabolic processes capable of influencing pharmacological reactions and even in the safety of drugs (35, 36).
However, the interaction of this complex system with oral anticoagulants has not yet been fully clarified. In the case of VKAs, the role of intestinal bacteria in vitamin K production has been suggested. For example, there are situations in which the population of the bacterial flora of the gut is reduced, causing a decrease in the source of vitamin K production, as in the case of the use of antibiotic therapies. Due to the decrease in vitamin synthesis, the anticoagulant effect may increase, as well as its possible adverse clinical effects (37, 38).
Otherwise, part of the metabolic capacity of gut microbiota is suggested to be closely associated with the presence of the cytochromes, especially CYP3A4-type cytochrome P450, which is highly expressed in the mucosa of the small intestine (38). Besides, the concomitant function of P-gp and CYP3A4 is particularly important in the gut, which could restrict oral drug bioavailability of a wide variety of substrates, without a clear known implication with NOACs to date (39).
Nowadays there is a growing interest in the use of probiotics to modify the composition and roles of the gut microbiota. Probiotics are defined as live microorganisms that, in optimal proportions, provide beneficial effects on the host and it is already known that they can have an impact on the gut ecosystem (9, 39–41). Among these actions, it has been observed that probiotics can interact with host cells through chemical signals and produce short-chain-fatty acids as metabolic products capable of influencing commensal microbes, or on the contrary, against potential pathogens as immune mechanisms (42). The species most commonly used as probiotics are Lactobacillus and Bifidobacterium, followed by the yeast Saccharomyces boulardii and some E. Coli and Bacillus species (42). In the particular context of oral anticoagulants, a recent in vitro study showed a significant change in the concentration of acenocoumarol (a VKA) after incubation with bifidobacteria, results which are compatible with biomodification of the drug due to enzymatic activity of bifidobacteria (43). However there are no data regarding NOACs.
On the other hand, prebiotics are selectively fermented ingredients, most of them used as food ingredients like cereals, spreads, or biscuits for example (42, 44). Inclusion in these products is shaped like lactulose or breast milk oligosaccharides, oligofructose among others (40). As with probiotics, prebiotics also influence the activity and composition of the gut microbiota (44). Intake of prebiotics decreases potential pathogens and increases the number of beneficial anaerobic bacteria (42).
In addition, changes in the bacterial population, also called dysbiosis, and its metabolic products have been related to pathogenetic mechanisms of many infections, inflammatory diseases and cardiovascular diseases (45). All this evidence is increasing the interest on the use of probiotics and prebiotics, given the benefits observed in improving the antigenic immune response, regulating intestinal inflammation and bolstering the intestinal barrier (41). In some populations at risk, it could be relevant to encourage probiotic and prebiotics research to deepen knowledge of the influence of changes in bacterial activity and its composition, and how this might relate with the intake of NOACs, but this evidence is far from complete (35).
There is scarce evidence so far regarding the interaction of NOACs with food and herbal products. However, some herbals and food modulate P-gp and CYP3A4 activity, so their potential impact on the anticoagulant effect of NOACs should be carefully examined. Thus, in order to improve the safety profile of NOACs with potential interactions, more clinical studies are needed to provide information from real-world data.
Finally, novel therapies such as probiotics/prebiotics might confer health benefits by modifying gut microbiota composition and its activity, but the effect on the safety and efficacy of NOACs is still unclear.
AS-F, JMR-C, and RL-G: drafted the manuscript. RL-G: designed and performed the figure. FM and VR: conceptualized the study, supervised the study, and made a critical revision of the manuscript. All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
JMR-C has received a grant from the Sociedad Española de Trombosis y Hemostasia (grant for short international training stays 2020) and the First Contact Initiative Grant 2020 from the European Society of Cardiology Council on Basic Cardiovascular Science. This work was supported by the Spanish Ministry of Economy, Industry, and Competitiveness, through the Instituto de Salud Carlos III after independent peer review (research grant: PI17/01375 co-financed by the European Regional Development Fund) and group CB16/11/00385 from CIBERCV.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. January CT, Wann LS, Calkins H, Chen LY, Cigarroa JE, Cleveland JC, et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. (2019) 74:104–32. doi: 10.1161/CIR.0000000000000665
2. Hindricks G, Potpara T, Dagres N, Arbelo E, Bax JJ, Blomström-Lundqvist C, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association of Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2021) 42:373–498. doi: 10.1093/eurheartj/ehaa612
3. Stevens SM, Woller SC, Kreuziger LB, Bounameaux H, Doerschug K, Geersing GJ, et al. Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. Chest. (2021) 160:e545–608. doi: 10.1016/j.chest.2021.07.055
4. Chan N, Sobieraj-Teague M, Eikelboom JW. Direct oral anticoagulants: evidence and unresolved issues. Lancet. (2020) 396:1767–76. doi: 10.1016/S0140-6736(20)32439-9
5. Vranckx P, Valgimigli M, Heidbuchel H. The significance of drug-drug and drug-food interactions of oral anticoagulation. Arrhythm Electrophysiol Rev. (2018) 7:55–61. doi: 10.15420/aer.2017.50.1
6. Holt A, Blanche P, Zareini B, Rasmussen PV, Strange JE, Rajan D, et al. Gastrointestinal bleeding risk following concomitant treatment with oral glucocorticoids in patients on non-vitamin K oral anticoagulants. Heart. (2021). doi: 10.1136/heartjnl-2021-319503
7. Holm J, Mannheimer B, Malmström RE, Eliasson E, Lindh JD. Bleeding and thromboembolism due to drug-drug interactions with non-vitamin K antagonist oral anticoagulants-a Swedish, register-based cohort study in atrial fibrillation outpatients. Eur J Clin Pharmacol. (2021) 77:409–19. doi: 10.1007/s00228-020-03015-7
8. Wang CL, Wu VC, Chang KH, Tu HT, Kuo CF, Huang YT, et al. Assessing major bleeding risk in atrial fibrillation patients concurrently taking non-vitamin K antagonist oral anticoagulants and antiepileptic drugs. Eur Heart J Cardiovasc Pharmacother. (2020) 6:147–54. doi: 10.1093/ehjcvp/pvz035
9. Stojančević M, Bojić G, Salami HA, Mikov M. The influence of intestinal tract and probiotics on the fate of orally administered drugs. Curr Issues Mol Biol. (2014) 16:55–68.
10. Zhou S, Gao Y, Jiang W, Huang M, Xu A, Paxton JW. Interactions of herbs with cytochrome P450. Drug Metab Rev. (2003) 35:35–98. doi: 10.1081/DMR-120018248
11. Zou L, Harkey MR, Henderson GL. Effects of herbal components on cDNA-expressed cytochrome P450 enzyme catalytic activity. Life Sci. (2002) 71:1579–89. doi: 10.1016/S0024-3205(02)01913-6
12. Steffel J, Collins R, Antz M, Cornu P, Desteghe L, Haeusler KG, et al. 2021 European heart rhythm association practical guide on the use of non-vitamin K antagonist oral anticoagulants in patients with atrial fibrillation. EP Europace. (2021). doi: 10.1093/europace/euab157
13. Di Minno A, Frigerio B, Spadarella G, Ravani A, Sansaro D, Amato M, et al. Old and new oral anticoagulants: Food, herbal medicines and drug interactions. Blood Rev. (2017) 31:193–203. doi: 10.1016/j.blre.2017.02.001
14. Walenga JM, Adiguzel C. Drug and dietary interactions of the new and emerging oral anticoagulants. Int J Clin Pract. (2010) 64:956–67. doi: 10.1111/j.1742-1241.2009.02286.x
15. Wessler JD, Grip LT, Mendell J, Giugliano RP. The P-glycoprotein transport system and cardiovascular drugs. J Am Coll Cardiol. (2013) 61:2495–502. doi: 10.1016/j.jacc.2013.02.058
16. Gnoth MJ, Buetehorn U, Muenster U, Schwarz T, Sandmann S. In vitro and in vivo P-glycoprotein transport characteristics of rivaroxaban. J Pharmacol Exp Ther. (2011) 338:372–80. doi: 10.1124/jpet.111.180240
17. Wang L, Zhang D, Raghavan N, Yao M, Ma L, Frost CE, et al. In vitro assessment of metabolic drug-drug interaction potential of apixaban through cytochrome P450 phenotyping, inhibition, and induction studies. Drug Metab Dispos. (2010) 38:448–58. doi: 10.1124/dmd.109.029694
18. Zanger UM, Schwab M. Cytochrome P450 enzymes in drug metabolism: regulation of gene expression, enzyme activities, and impact of genetic variation. Pharmacol Ther. (2013) 138:103–41. doi: 10.1016/j.pharmthera.2012.12.007
19. Mueck W, Kubitza D, Becka M. Co-administration of rivaroxaban with drugs that share its elimination pathways: pharmacokinetic effects in healthy subjects. Br J Clin Pharmacol. (2013) 76:455–66. doi: 10.1111/bcp.12075
20. Gronich N, Stein N, Muszkat M. Association Between Use of pharmacokinetic-interacting drugs and effectiveness and safety of direct acting oral anticoagulants: nested case-control study. Clin Pharmacol Ther. (2021) 110:1526–36. doi: 10.1002/cpt.2369
21. Kubitza D, Becka M, Mück W, Krätzschmar J. Pharmacodynamics and pharmacokinetics during the transition from warfarin to rivaroxaban: a randomized study in healthy subjects. Br J Clin Pharmacol. (2014) 78:353–63. doi: 10.1111/bcp.12349
22. Stampfuss J, Kubitza D, Becka M, Mueck W. The effect of food on the absorption and pharmacokinetics of rivaroxaban. Int J Clin Pharmacol Ther. (2013) 51:549–61. doi: 10.5414/CP201812
23. Bailey DG, Dresser G, Arnold JM. Grapefruit-medication interactions: forbidden fruit or avoidable consequences? Cmaj. (2013) 185:309–16. doi: 10.1503/cmaj.120951
24. Barrett YC, Wang J, Song Y, Pursley J, Wastall P, Wright R, et al. A randomised assessment of the pharmacokinetic, pharmacodynamic and safety interaction between apixaban and enoxaparin in healthy subjects. Thromb Haemost. (2012) 107:916–24. doi: 10.1160/TH11-09-0634
25. Kubitza D, Becka M, Schwers S, Voith B. Investigation of Pharmacodynamic and Pharmacokinetic Interactions Between Rivaroxaban and Enoxaparin in Healthy Male Subjects. Clin Pharmacol Drug Dev. (2013) 2:270–7. doi: 10.1002/cpdd.26
26. Zahir H, Matsushima N, Halim AB, He L, Zhang G, Lee F, et al. Edoxaban administration following enoxaparin: a pharmacodynamic, pharmacokinetic, and tolerability assessment in human subjects. Thromb Haemost. (2012) 108:166–75. doi: 10.1160/TH11-09-0676
27. Gelosa P, Castiglioni L, Tenconi M, Baldessin L, Racagni G, Corsini A, et al. Pharmacokinetic drug interactions of the non-vitamin K antagonist oral anticoagulants (NOACs). Pharmacol Res. (2018) 135:60–79. doi: 10.1016/j.phrs.2018.07.016
28. Mousa SA. Antithrombotic effects of naturally derived products on coagulation and platelet function. Methods Mol Biol. (2010) 663:229–40. doi: 10.1007/978-1-60761-803-4_9
29. Tsai HH, Lin HW, Lu YH, Chen YL, Mahady GB. A review of potential harmful interactions between anticoagulant/antiplatelet agents and Chinese herbal medicines. PLoS ONE. (2013) 8:e64255. doi: 10.1371/journal.pone.0064255
30. Tarn DM, Barrientos M, Wang AY, Ramaprasad A, Fang MC, Schwartz JB. Prevalence and knowledge of potential interactions between over-the-counter products and apixaban. J Am Geriatr Soc. (2020) 68:155–62. doi: 10.1111/jgs.16193
31. Ashour ML, Youssef FS, Gad HA, Wink M. Inhibition of cytochrome P450 (CYP3A4) activity by extracts from 57 plants used in Traditional Chinese Medicine (TCM). Pharmacogn Mag. (2017) 13:300–8. doi: 10.4103/0973-1296.204561
32. Shivamurthy P, Brar N, Therrien ML. Isolated hemopericardium associated with rivaroxaban: first case report. Pharmacotherapy. (2014) 34:e169–72. doi: 10.1002/phar.1474
33. Maadarani O, Bitar Z, Mohsen M. Adding herbal products to direct-acting oral anticoagulants can be fatal. Eur J Case Rep Intern Med. (2019) 6:001190. doi: 10.12890/2019_001190
34. Gressenberger P, Rief P, Jud P, Gütl K, Muster V, Ghanim L, et al. Increased bleeding risk in a patient with oral anticoagulant therapy and concomitant herbal intake—a case report. EJIFCC. (2019) 30:95–8.
35. Gerritsen J, Smidt H, Rijkers GT, de Vos WM. Intestinal microbiota in human health and disease: the impact of probiotics. Genes Nutr. (2011) 6:209–40. doi: 10.1007/s12263-011-0229-7
36. Goldin BR. Intestinal microflora: metabolism of drugs and carcinogens. Ann Med. (1990) 22:43–8. doi: 10.3109/07853899009147240
37. Conly JM, Stein K. The production of menaquinones (vitamin K2) by intestinal bacteria and their role in maintaining coagulation homeostasis. Prog Food Nutr Sci. (1992) 16:307–43.
38. Camelo-Castillo A, Rivera-Caravaca JM, Orenes-Piñero E, Ramírez-Macías I, Roldán V, Lip GYH, et al. Gut microbiota and the quality of oral anticoagulation in vitamin k antagonists users: a review of potential implications. J Clin Med. (2021) 10:715. doi: 10.3390/jcm10040715
39. Bezirtzoglou EE. Intestinal cytochromes P450 regulating the intestinal microbiota and its probiotic profile. Microb Ecol Health Dis. (2012) 23. doi: 10.3402/mehd.v23i0.18370
40. Hill C, Guarner F, Reid G, Gibson GR, Merenstein DJ, Pot B, et al. Expert consensus document. The International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol. (2014) 11:506–14. doi: 10.1038/nrgastro.2014.66
41. Martinez MN, Amidon GL. A. mechanistic approach to understanding the factors affecting drug absorption: a review of fundamentals. J Clin Pharmacol. (2002) 42:620–43. doi: 10.1177/00970002042006005
42. Guarner F, Khan AG, Garisch J, Eliakim R, Gangl A, Thomson A, et al. World gastroenterology organisation global guidelines: probiotics and prebiotics october 2011. J Clin Gastroenterol. (2012) 46:468–81. doi: 10.1097/MCG.0b013e3182549092
43. Fragomeno M, Assad S, Mobili P, Peruzzo PJ, Minnaard J, Pérez PF. Biomodification of acenocoumarol by bifidobacteria. FEMS Microbiol Lett. (2021) 368:fnab125. doi: 10.1093/femsle/fnab125
44. Gibson GR, Roberfroid MB. Dietary modulation of the human colonic microbiota: introducing the concept of prebiotics. J Nutr. (1995) 125:1401–12. doi: 10.1093/jn/125.6.1401
45. Ramírez-Macías I, Orenes-Piñero E, Camelo-Castillo A, Rivera-Caravaca JM, López-García C, Marín F. Novel insights in the relationship of gut microbiota and coronary artery diseases. Crit Rev Food Sci Nutr. (2021) 1–13. doi: 10.1080/10408398.2020.1868397 [Epub ahead of print].
46. Stangier J, Rathgen K, Stähle H, Gansser D, Roth W. The pharmacokinetics, pharmacodynamics and tolerability of dabigatran etexilate, a new oral direct thrombin inhibitor, in healthy male subjects. Br J Clin Pharmacol. (2007) 64:292–303. doi: 10.1111/j.1365-2125.2007.02899.x
47. Raghavan N, Frost CE, Yu Z, He K, Zhang H, Humphreys WG, et al. Apixaban metabolism and pharmacokinetics after oral administration to humans. Drug Metab Dispos. (2009) 37:74–81. doi: 10.1124/dmd.108.023143
48. Ogata K, Mendell-Harary J, Tachibana M, Masumoto H, Oguma T, Kojima M, et al. Clinical safety, tolerability, pharmacokinetics, and pharmacodynamics of the novel factor Xa inhibitor edoxaban in healthy volunteers. J Clin Pharmacol. (2010) 50:743–53. doi: 10.1177/0091270009351883
49. Kubitza D, Becka M, Voith B, Zuehlsdorf M, Wensing G. Safety, pharmacodynamics, and pharmacokinetics of single doses of BAY 59-7939, an oral, direct factor Xa inhibitor. Clin Pharmacol Ther. (2005) 78:412–21. doi: 10.1016/j.clpt.2005.06.011
50. Mueck W, Stampfuss J, Kubitza D, Becka M. Clinical pharmacokinetic and pharmacodynamic profile of rivaroxaban. Clin Pharmacokinet. (2014) 53:1–16. doi: 10.1007/s40262-013-0100-7
51. Yale SH, Glurich I. Analysis of the inhibitory potential of Ginkgo biloba, Echinacea purpurea, and Serenoa repens on the metabolic activity of cytochrome P450 3A4, 2D6, and 2C9. J Altern Complement Med. (2005) 11:433–9. doi: 10.1089/acm.2005.11.433
Keywords: non-vitamin K antagonist oral anticoagulants (NOACs), drug interactions, food interactions, P-glycoprotein, cytochrome P450 (CYP) 3A4, probiotics
Citation: Sánchez-Fuentes A, Rivera-Caravaca JM, López-Gálvez R, Marín F and Roldán V (2022) Non-vitamin K Antagonist Oral Anticoagulants and Drug-Food Interactions: Implications for Clinical Practice and Potential Role of Probiotics and Prebiotics. Front. Cardiovasc. Med. 8:787235. doi: 10.3389/fcvm.2021.787235
Received: 30 September 2021; Accepted: 27 December 2021;
Published: 17 January 2022.
Edited by:
Shimon Rosenheck, Hebrew University of Jerusalem, IsraelReviewed by:
Julie Kalabalik-Hoganson, Fairleigh Dickinson University, United StatesCopyright © 2022 Sánchez-Fuentes, Rivera-Caravaca, López-Gálvez, Marín and Roldán. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: José Miguel Rivera-Caravaca, am1yaXZlcmE0MjlAZ21haWwuY29t
†These authors share senior authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.