 Bingqi Fu
Bingqi Fu Xuebiao Wei
Xuebiao Wei Qi Wang
Qi Wang Zhiwen Yang
Zhiwen Yang Jiyan Chen
Jiyan Chen Danqing Yu
Danqing Yu
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 19 November 2021
Sec. Coronary Artery Disease
Volume 8 - 2021 | https://doi.org/10.3389/fcvm.2021.743678
Background: Thrombolysis in Myocardial Infarction (TIMI) Risk Index (TRI) is a simple risk assessment tool for patients with ST-segment elevation myocardial infarction (STEMI). However, its applicability to elderly patients with STEMI undergoing percutaneous coronary intervention (PCI) is uncertain.
Methods: This was a retrospective analysis of elderly (≥60 years) patients who underwent PCI for STEMI from January 2010 to April 2016. TRI was calculated on admission using the following formula: heart rate × (age/10)2/systolic blood pressure. Discrimination and calibration of TRI for in-hospital events and 1 year mortality were analyzed.
Results: Totally 1,054 patients were divided into three groups according to the tertiles of the TRI: <27 (n = 348), 27–36 (n = 360) and >36 (n = 346). The incidence of acute kidney injury (AKI; 7.8 vs. 8.6 vs. 24.0%, p < 0.001), AHF (3.5 vs. 6.6 vs. 16.2%, p < 0.001), in-hospital death (0.6 vs. 3.3 vs. 11.6%, p < 0.001) and MACEs (5.2 vs. 5.8 vs. 15.9%, p < 0.001) was significantly higher in the third tertile. TRI showed good discrimination for in-hospital death [area under the curve (AUC) = 0.804, p < 0.001; Hosmer-Lemeshow p = 0.302], which was superior to its prediction for AKI (AUC = 0.678, p < 0.001; Hosmer-Lemeshow p = 0.121), and in-hospital MACEs (AUC = 0.669, p < 0.001; Hosmer-Lemeshow p = 0.077). Receiver-operation characteristics curve showed that TRI > 42.0 had a sensitivity of 64.8% and specificity of 82.2% for predicting in-hospital death. Kaplan-Meier analysis showed that patients with TRI > 42.0 had higher 1 year mortality (Log-rank = 79.2, p < 0.001).
Conclusion: TRI is suitable for risk stratification in elderly patients with STEMI undergoing PCI, and is thus of continuing value for an aging population.
ST-segment elevation myocardial infarction (STEMI), defined as ST-segment elevation in at least two contiguous leads, has been introduced as a subtype of acute coronary syndrome for purposes of immediate treatment. Percutaneous coronary intervention (PCI) is a class IB treatment in STEMI patients, given that early invasive revascularization therapy can greatly decrease mortality (1). As the elderly population has grown, patients older than 75 years have come to constitute more than 60% of STEMI cases (2). The mean age of candidates for PCI increased by 7 years from 1990 to 2010, and patients aged 75 and over make up 28% of those who undergo PCI in Sweden (3). Age is an independent risk factor for long-term mortality in STEMI, with every one-year increase in age equating to a 1.07 times increase in risk of death (4). The 30-day mortality is 13.4% in 70–79 year-olds and 23.9% in 80 year-olds and above according to the International Survey of Acute Coronary Syndromes in Transitional Countries (ISACS-TC) database (5).
Early risk assessment is necessary for identifying high-risk patients and developing prognoses (1, 2, 4). Thrombolysis in Myocardial Infarction (TIMI) Risk Index (TRI) was created by Morrow et al. (6) to guide rapid initial triage for STEMI patients. It has performed well in predicting 30 day mortality in the general population of patients who underwent revascularization therapy; however, the proportion of patients who received PCI was small, being <3% in Bradshaw et al. (7) 4.4% in Wiviott et al. (8) and 5.4% in Rathore et al. (9) The value of the TRI has not been confirmed in the context of PCI being the mainstay of therapy for STEMI. In an attempt to provide first-line information regarding Chinese patients, we evaluated the use of TRI to predict mortality and clinical events among elderly STEMI patients who received PCI.
Ours was a retrospective study approved by the Ethics Committee of Guangdong Provincial People's Hospital with a waiver of informed consent because of the retrospective study design (no. GDREC2016411H). Statistical analysis was performed on the patient population and identifying information was strictly concealed during the study. We consecutively enrolled 1907 patients with STEMI who had undergone PCI at cardiac care unit (CCU) from January 2010 to April 2016 at Guangdong Provincial People's Hospital, Guangzhou, China. The definition of STEMI was taken from the American College of Cardiology Foundation/American Heart Association Task Force (10). After excluding patients with a hospital stay of <24 h (n = 27), a malignant tumor (n = 22), concomitant aortic dissection (n = 6) or age <60 years (n = 798), 1,054 patients were included in our study population (Figure 1).
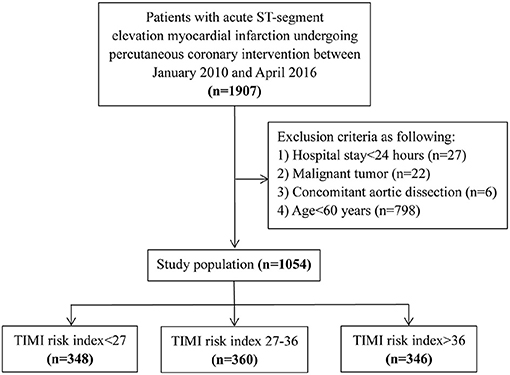
Figure 1. Flow diagram for patient screening.
Data was extracted from hospital records by trained study coordinators. Data regarding patient demographics [i.e., age, gender, weight, heart rate, systolic blood pressure (SBP), diastolic blood pressure (DBP), diabetes mellitus, hypertension, time to admission, anatomical location of myocardial infarction, Killip classification, hospital stay], laboratory test results [i.e., serum creatinine, hemoglobin, creatine kinase myocardial band (MB)], ultrasonographic results, [i.e., left ventricular ejection fraction (LVEF)], medical treatment, PCI details [i.e., use of intra-aortic balloon pump (IABP), thrombus aspiration, vessels treated, number of stents], major adverse clinical events (MACEs), acute kidney injury (AKI) and in-hospital death were collected. All in-hospital clinical events were recorded by two independent researchers who were not informed of the treatments. Other data was collected by one researcher and randomly checked by another researcher. The TRI was calculated on admission using the following formula: heart rate × (age/10)2/systolic blood pressure (6).
All patients were monitored for 1 year by trained nurses via telephone interviews or clinical visits. Oral informed consents were obtained during the first telephone interview or the first clinical visit after discharge. The data of death was recorded during follow-up and 1 year death was determined according to the date of death. The primary endpoint of the study was in-hospital death. The secondary endpoint was in-hospital MACEs, AKI, acute heart failure (AHF) or death during 1 year of follow-up. In-hospital MACEs were a composite end point of renal dialysis, stroke, target vessel revascularization (TVR). AKI was defined as a post-PCI rise in serum creatinine (sCr) ≥ 0.3 mg/dl, or a ≥ 50% elevation from baseline over the course of hospitalization as per the Kidney Disease International Global Outcomes Guidelines (11). Acute heart failure was defined as newly onset or worsening of symptoms and signs of pre-existing heart failure that required intravenous therapy (inotropes, vasodilators, or diuretics) (12, 13).
Normally distributed continuous variables were shown as mean ± standard deviation, while those with a skewed distribution were shown as median with upper and lower quartiles. Categorial variables were shown as percentages. Continuous variables were compared using variances or the Wilcoxon rank-sum test, while categorial variables were compared using the chi-square test. The cut-off value was calculated using the receiver-operation characteristics (ROC) curve analysis. All variables were included in the univariate models to assess the predictive value of TRI for adverse events. Variables with a p < 0.05 were then incorporated in the multivariate models for further evaluation. Use of the TRI in predicting adverse events was evaluated by analysis of discrimination and calibration. Discriminative performance was expressed as the area under curve (AUC) of ROC curve. Calibration was expressed as the Hosmer-Lemeshow (H-L) chi-square. For 1 year cumulative survival analysis, Kaplan-Meier curves were acquired and log-rank tests were performed. All data was processed using SPSS software version 22.0 (SPSS, Inc., Chicago, Illinois). A two-sided p < 0.05 was considered statistically significant.
A total of 1,054 patients (mean age: 70 ± 7 years; gender: 25.5% female) were divided into three groups according to the TRI tertiles: <27 (n = 348), 27–36 (n = 360) and >36 (n = 346). Comparisons among the three groups revealed significant differences between the following variables: age, weight, anterior myocardial infarction, systolic blood pressure, diastolic blood pressure, heart rate, Killip II-IV, serum creatinine, hemoglobin, LVEF, use of IABP and length of hospital stay (all p < 0.05, Table 1).
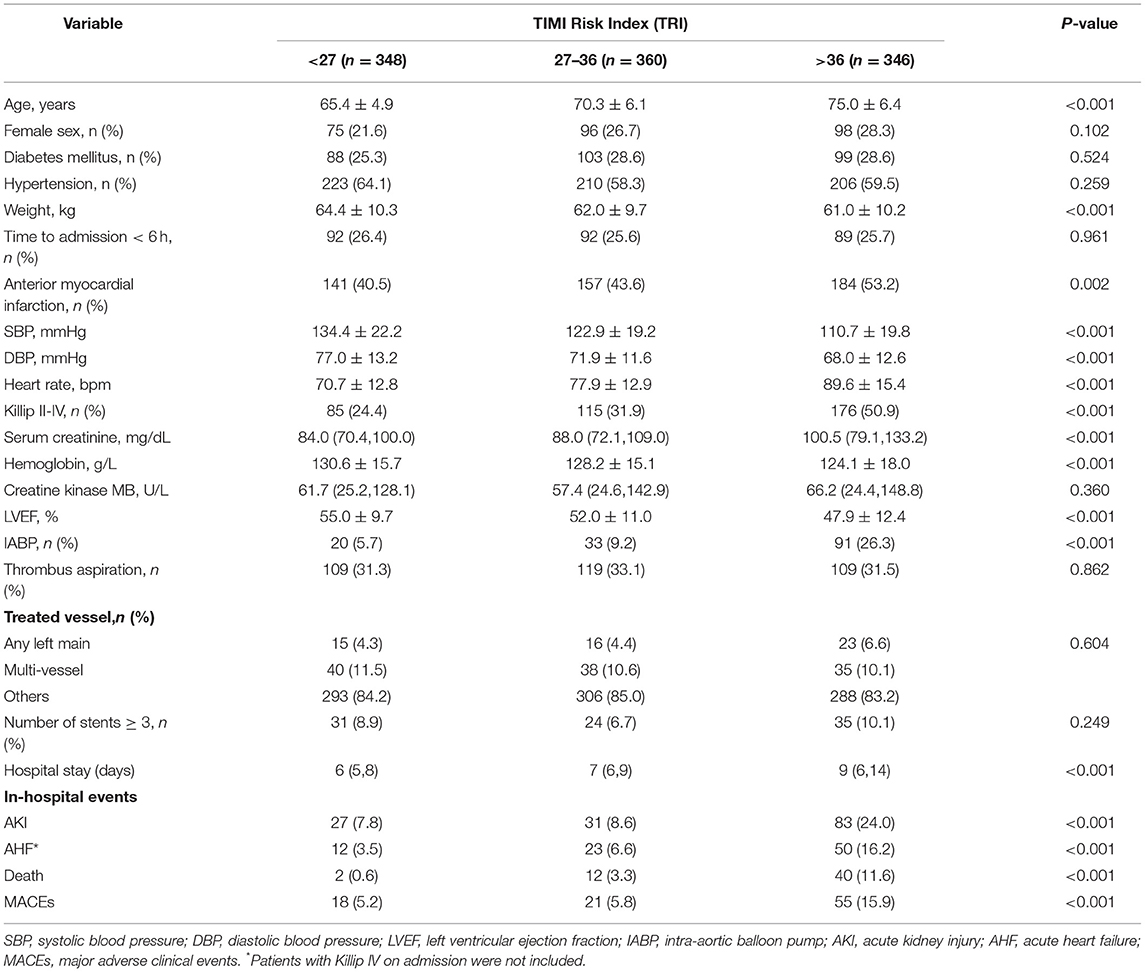
Table 1. Clinical characteristics for TRI tertiles.
The overall incidence of in-hospital death, AKI, AHF and MACEs was 54 (5.1%), 141 (13.4%), 85(8.5%) and 94(8.9%), respectively (Table 2). The frequency of clinical events varied significantly among the different groups. The incidence of AKI (7.8 vs. 8.6 vs. 24.0%, p < 0.001), AHF (3.5 vs. 6.6 vs. 16.2%, p < 0.001), in-hospital death (0.6 vs. 3.3 vs. 11.6%, p < 0.001) and MACEs (5.2 vs. 5.8 vs. 15.9%, p < 0.001) was significantly higher in the third tertile (Table 1).
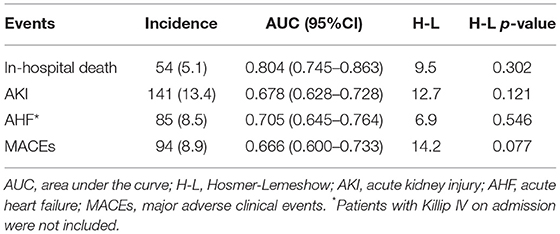
Table 2. Validation of TRI score.
Univariate analysis showed a significant correlation between TRI and AKI, in-hospital death, in-hospital MACEs and 1 year mortality. After adjustment for potential confounding factors, TRI remained to be significantly associated with AKI (OR = 1.02, 95% CI 1.01–1.04, p = 0.007), AHF (OR = 1.03, 95% CI 1.01–1.05, p = 0.005) in-hospital death (OR = 1.05, 95%CI 1.03–1.07, p < 0.001), in-hospital MACEs (OR = 1.03, 95%CI 1.01–1.05, p = 0.006) and 1 year mortality (HR = 1.03, 95% CI 1.02–1.04, p < 0.001, Table 3). ROC curve revealed that 42.0 was the optimal cut-off value of the TRI for predicting in-hospital death, with the sensitivity and specificity being 64.8% and 82.2%, respectively. The Kaplan-Meier curves showed that patients with TRI > 42.0 had higher cumulative 1 year mortality than those with TRI ≤ 42.0 (Log-rank = 79.2, p < 0.001, Figure 2). Multivariate analysis revealed that TRI > 42.0 was an independent risk factor for AKI (OR = 1.86, 95% CI 1.20–2.88, p = 0.006), AHF (OR = 1.77, 95% CI 1.03–3.04, p = 0.040), in-hospital death (OR = 3.76, 95% CI 1.97–7.18, p < 0.001), in-hospital MACEs (OR = 1.75, 95% CI 1.02–3.02, p = 0.044), and 1 year mortality (HR = 2.23, 95% CI 1.47–3.36, p < 0.001, Table 3).
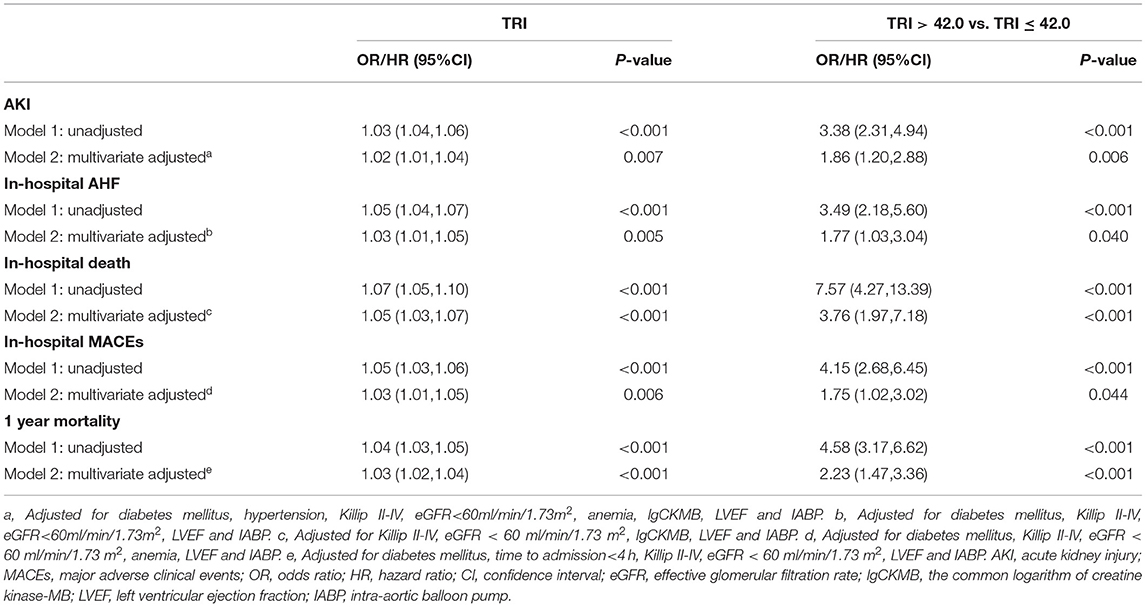
Table 3. Unadjusted and adjusted OR/HR of TRI for adverse events.

Figure 2. Kaplan-Meier analyses for 1 year mortality according to the TRI categories.
The TRI showed good discrimination for in-hospital death (AUC = 0.804, 95% CI 0.779–0.828, p < 0.001, Table 2, Figure 3), but relatively poor discrimination for AKI (AUC = 0.678, 95% CI 0.649–0.706, p < 0.001, Table 2, Figure 3), AHF (AUC = 0.705, 95% CI 0.645–0.764, p < 0.001, Table 2, Figure 3), and in-hospital MACEs (AUC = 0.669, 95% CI 0.640–0.698, p < 0.001, Table 2, Figure 3). As for calibration, there was no significant difference between expected and observed events when the TRI was used to predict in-hospital death (H-L chi-square = 9.5, p = 0.302, Table 2, Figure 4), AKI (H-L chi-square = 12.7, p = 0.121, Table 2, Figure 4), AHF (H-L chi-square = 6.9, p = 0.546, Table 2, Figure 4), and in-hospital MACEs (H-L chi-square = 14.2, p = 0.077, Table 2, Figure 4). Overall, the TRI had good discrimination for in-hospital death, which was superior to its prediction for AKI, AHF and in-hospital MACEs.

Figure 3. The receiver-operation characteristics curve of the TRI for predicting in-hospital events.
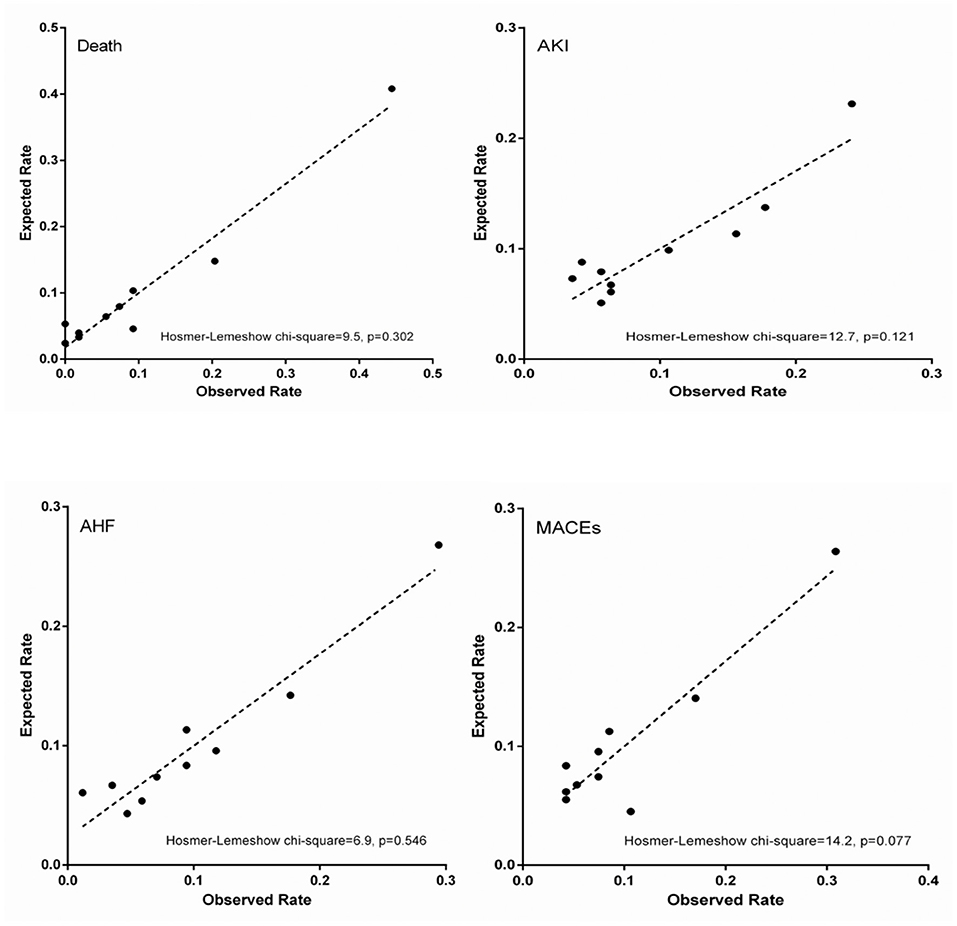
Figure 4. Calibration plots.
According to the anatomical location of myocardial infarction, patients were subdivided into anterior myocardial infarction subgroup (TRI = 34.8 ± 11.8) and non-anterior myocardial infarction subgroup (TRI = 32.2 ± 12.0). The predictive value TRI for in-hospital death was slightly higher in anterior myocardial infarction subgroup (AUC = 0.837, 95% CI 0.774–0.899, H-L p = 0.151) than that in non-anterior myocardial infarction (AUC = 0.776, 95% CI 0.682–0.869, H-L p = 0.205, Table 4).
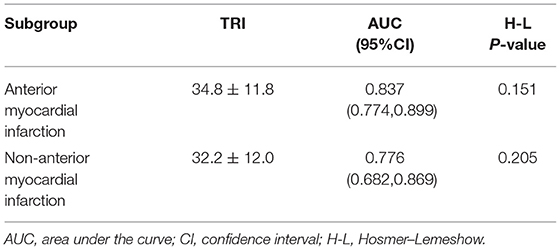
Table 4. Subgroup analysis for predicting in-hospital death.
To our best knowledge, this study is the first to validate the efficacy of the TRI in elderly patients receiving PCI. The results show that the TRI has good discrimination and calibration for in-hospital death, but not for AKI or in-hospital MACEs. Therefore, the TRI is suitable for predicting in-hospital mortality in elderly patients with STEMI who have undergone PCI.
PCI has gradually become a mainstream therapy of STEMI that has benefited survival. The most recent epidemiological study in Europe reported a decline in STEMI 30 day mortality over two decades, from 14% in 1995 to 3% in 2015 (14). In terms of the elderly, however, the prognosis remained poor (3–5), and early identification of high-risk patients was essential in clinical practice (1, 2, 4). The TRI was initially derived from the InTIME II trial by Morrow et al. (6) which involved 13,253 STEMI patients undergoing thrombolytic therapy with an in-hospital mortality of 5.4% and a 30 day mortality of 6.0%. It demonstrated good discrimination (AUC = 0.78) and calibration (Pearson goodness-of-fit statistic = 2.83, p = 0.7) for 30 day mortality among STEMI patients with thrombolysis. Rathore et al. (9) analyzed patients ≥ 65 years of age from the Cooperative Cardiovascular Project (CCP) database and showed that the discrimination (AUC = 0.62) and calibration (goodness of fit p < 0.001) of TRI for predicting 30 day mortality were unsatisfying, while Bradshaw et al. (AUC = 0.74) and Wiviott et al. (AUC = 0.71) (7, 8) showed slightly higher predictive value. These studies primarily evaluated patients who received thrombolytic or fibrinolytic therapy, while primary PCI played only a small part. The proportion of PCI was <3% in Bradshaw et al. (7) 4.4% in Wiviott et al. (8) and 5.4% in Rathore et al. (9). Thus, clinical application of the TRI in elderly STEMI patients who received PCI had yet to be tested. In our study we demonstrated good discriminative capacity with AUC of 0.804 and good calibration of the TRI in predicting 30 day mortality in elderly STEMI patients who received PCI. Given that the TRI is formulated using easily obtained variables, i.e., age, heart rate and blood pressure, it is promising for rapid risk stratification in clinical practice.
Clinical adverse events such as congestive heart failure, in-hospital death, and acute kidney injury following STEMI are known to frequently be correlated with a higher TRI, but the predictive value of the TRI for these potential clinical adverse events was unknown (15–18). In our study, the ability of the TRI to predict AKI and in-hospital MACEs were relatively poor. This was probably the result of inadequate involvement of independent risk factors (19, 20). Age is an independent risk factor for AKI and in-hospital MACEs (16, 17, 21), and since age is one component of the TRI, this might explain why the TRI was partially, though poorly, predictive of these events. Apart from age, there are many other variables that contribute to specific clinical events. Variables such as serum creatinine, estimated glomerular filtration rate, contrast media volume, and underlying comorbidities (i.e., hypertension, diabetes mellitus, etc.) anticipate the rate of AKI and the need for renal dialysis (11, 16, 22), but are not included in the TRI. Nor are stroke-associated predictors such as carotid artery disease and atrial fibrillation (23). As for repeat coronary revascularization, Atti et al. (24) showed in a recent meta-analysis that risk of multivessel revascularization was reduced by 66% compared to culprit-only revascularization, which is also not incorporated into the TRI. Since most variables that were valuable for predicting the above-mentioned clinical events are only obtained from laboratory results and PCI, risk assessment is delayed. The TRI, on the other hand, can provide rapid initial triage of STEMI patients.
The discriminative capacity and calibration of TRI for predicting mortality in elderly STEMI patients in our study was better than that in Rathore's study, which might be explained by the variation of baseline characteristics and mortality. Compared to CCP-RT cohort, our study cohort varied in terms of patient demographics, medical history, admission characteristics and short-term mortality (Table 5) (9). On one hand, our study cohort included Asian ethnic people, while CCP-RT cohort recruited majorly white ethnic people. Other variables including proportion of female patients, medical history of myocardial infarction, on-admission status such as shock, systolic pressure and timing on arrival, were all possibly responsible for the different discriminative and calibration results of TRI between CCP-RT cohort and our cohort. On the other hand, our cohort had a 9.5% reduction of short-term mortality compared to CCP-RT cohort, which might be due to the fact that only 5.4% of CCP-RT cohort received PCI therapy, while the rest received thrombolytic therapy (9). PCI therapy has now recognized as the preferred reperfusion therapy within 120 min of STEMI diagnosis, as it benefits the clinical outcomes compared to thrombolysis (25).
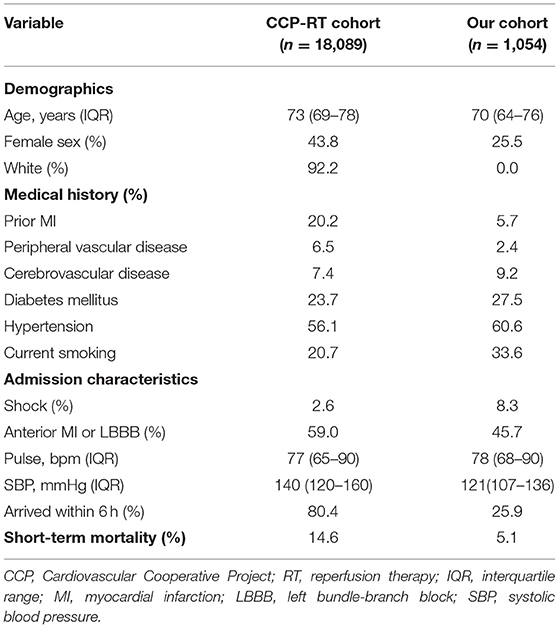
Table 5. Comparison of patient characteristics.
Our study had several limitations. Firstly, although the TRI has the advantage of rapid risk assessment, caution should be applied to long-term prognosis, which is a combination of multiple intertwined factors such as acute physiological change (e.g., serum creatinine, white blood cell count, etc.), timing of PCI, location of culprit vessels, in-hospital complications, frailty and cognitive function (9, 20, 26–30). Therefore, after initial triage, risk assessment should be updated dynamically through treatment to more accurately predict mortality (1, 8). Secondly, our study was designed as a retrospective analysis, and although bias was therefore unavoidable, efforts were made to minimize it. Finally, the study population was relatively small, and the results might be different with a larger cohort. Multi-centered, prospective studies with larger samples are needed to confirm our results.
In summary, the TRI remains suitable for risk stratification in elderly patients with STEMI who underwent PCI. The TRI has advantages of good discrimination and calibration, as well as a simple formula that allows rapid initial risk assessment.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Ethics Committee of Guangdong Provincial People's Hospital. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
DY and JC were involved in the conception and design of this study. BF, XW, ZY, and QW contributed to data collection and data interpretation. BF, XW, and QW constructed the manuscript, which was revised and approved by all the authors for publication.
This study was supported by grants from National Natural Science Foundation of China (Grant No. 82002014), Natural Science Foundation of Guangdong Province (Grant No. 2021A1515010107), Science and Technology Projects of Guangzhou (Grant No. 201903010097), and Guangdong Provincial Key Laboratory of Coronary Heart Disease Prevention (Grant No. 2017B030314041). The funders had no role in the study design, data collection and analysis, decision to publish, nor preparation of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European society of cardiology (ESC). Eur Heart J. (2018) 39:119–77. doi: 10.1093/eurheartj/ehx393
2. Townsend N, Wilson L, Bhatnagar P, Wickramasinghe K, Rayner M, Nichols M. Cardiovascular disease in Europe: epidemiological update 2016. Eur Heart J. (2016) 37:3232–45. doi: 10.1093/eurheartj/ehw334
3. Fokkema ML, James SK, Albertsson P, Akerblom A, Calais F, Eriksson P, et al. Population trends in percutaneous coronary intervention: 20-year results from the SCAAR (Swedish Coronary Angiography and Angioplasty Registry). J Am Coll Cardiol. (2013) 61:1222–30. doi: 10.1016/j.jacc.2013.01.007
4. Pedersen F, Butrymovich V, Kelbaek H, Wachtell K, Helqvist S, Kastrup J, et al. Short- and long-term cause of death in patients treated with primary PCI for STEMI. J Am Coll Cardiol. (2014) 64:2101–8. doi: 10.1016/j.jacc.2014.08.037
5. Ricci B, Manfrini O, Cenko E, Vasiljevic Z, Dorobantu M, Kedev S, et al. Primary percutaneous coronary intervention in octogenarians. Int J Cardiol. (2016) 222:1129–35. doi: 10.1016/j.ijcard.2016.07.204
6. Morrow DA, Antman EM, Giugliano RP, Cairns R, Charlesworth A, Murphy SA, et al. A simple risk index for rapid initial triage of patients with ST-elevation myocardial infarction: an InTIME II substudy. Lancet. (2001) 358:1571–5. doi: 10.1016/S0140-6736(01)06649-1
7. Bradshaw PJ, Ko DT, Newman AM, Donovan LR, Tu JV. Validation of the thrombolysis in myocardial infarction (TIMI) risk index for predicting early mortality in a population-based cohort of STEMI and non-STEMI patients. Can J Cardiol. (2007) 23:51–6. doi: 10.1016/S0828-282X(07)70213-1
8. Wiviott SD, Morrow DA, Frederick PD, Giugliano RP, Gibson CM, McCabe CH, et al. Performance of the thrombolysis in myocardial infarction risk index in the national registry of myocardial infarction-3 and−4: a simple index that predicts mortality in ST-segment elevation myocardial infarction. J Am Coll Cardiol. (2004) 44:783–9. doi: 10.1016/S0735-1097(04)01110-6
9. Rathore SS, Weinfurt KP, Gross CP, Krumholz HM. Validity of a simple ST-elevation acute myocardial infarction risk index: are randomized trial prognostic estimates generalizable to elderly patients? Circulation. (2003) 107:811–6. doi: 10.1161/01.CIR.0000049743.45748.02
10. O'Gara PT, Kushner FG, Ascheim DD, Casey DE, Chung MK, de Lemos JA, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American college of cardiology foundation/American heart association task force on practice guidelines. J Am Coll Cardiol. (2013) 6:e78–140. doi: 10.1016/j.jacc.2012.11.019
11. McCullough PA, Choi JP, Feghali GA, Schussler JM, Stoler RM, Vallabahn RC, et al. Contrast-induced acute kidney injury. J Am Coll Cardiol. (2016) 68:1465–73. doi: 10.1016/j.jacc.2016.05.099
12. Chioncel O, Mebazaa A, Harjola VP, Coats AJ, Piepoli MF, Crespo-Leiro MG, et al. Clinical phenotypes and outcome of patients hospitalized for acute heart failure: the ESC heart failure long-term registry. Eur J Heart Fail. (2017) 19:1242–54. doi: 10.1002/ejhf.890
13. Arrigo M, Jessup M, Mullens W, Reza N, Shah AM, Sliwa K, et al. Acute heart failure. Nat Rev Dis Primers. (2020) 6:16. doi: 10.1038/s41572-020-0151-7
14. Puymirat E, Simon T, Cayla G, Cottin Y, Elbaz M, Coste P, et al. Acute myocardial infarction: changes in patient characteristics, management, and 6-month outcomes over a period of 20 years in the FAST-MI program (French registry of acute ST-elevation or non-ST-elevation myocardial infarction) 1995 to 2015. Circulation. (2017) 136:1908–19. doi: 10.1161/CIRCULATIONAHA.117.030798
15. Tsai TT, Patel UD, Chang TI, Kennedy KF, Masoudi FA, Matheny ME, et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: insights from the NCDR Cath-PCI registry. JACC Cardiovasc Interv. (2014) 7:1–9.
16. Tziakas D, Chalikias G, Stakos D, Apostolakis S, Adina T, Kikas P, et al. Development of an easily applicable risk score model for contrast-induced nephropathy prediction after percutaneous coronary intervention: a novel approach tailored to current practice. Int J Cardiol. (2013) 163:46–55. doi: 10.1016/j.ijcard.2011.05.079
17. Lin KY, Zheng WP, Bei WJ, Chen SQ, Islam SM, Liu Y, et al. A novel risk score model for prediction of contrast-induced nephropathy after emergent percutaneous coronary intervention. Int J Cardiol. (2017) 230:402–12. doi: 10.1016/j.ijcard.2016.12.095
18. Truong QA, Cannon CP, Zakai NA, Rogers IS, Giugliano RP, Wiviott SD. Thrombolysis in myocardial infarction (TIMI) risk index predicts long-term mortality and heart failure in patients with ST-elevation myocardial infarction in the TIMI 2 clinical trial. Am Heart J. (2009) 157:673–9. doi: 10.1016/j.ahj.2008.12.010
19. Steyerberg EW, Vickers AJ, Cook NR, Gerds T, Gonen M, Obuchowski N, et al. Assessing the performance of prediction models: a framework for traditional and novel measures. Epidemiology. (2010) 21:128–38. doi: 10.1097/EDE.0b013e3181c30fb2
20. Van Calster B, McLernon DJ, van Smeden M, Wynants L, Steyerberg EW, Topic Group 'Evaluating diagnostic t, et al. Calibration: the Achilles heel of predictive analytics. BMC Med. (2019) 17:230. doi: 10.1186/s12916-019-1466-7
21. Smilowitz NR, Mahajan AM, Roe MT, Hellkamp AS, Chiswell K, Gulati M, et al. Mortality of myocardial infarction by sex, age, and obstructive coronary artery disease status in the ACTION registry-GWTG (acute coronary treatment and intervention outcomes network registry-get with the guidelines). Circ Cardiovasc Qual Outcomes. (2017) 10:e003443. doi: 10.1161/CIRCOUTCOMES.116.003443
22. Mehran R, Aymong ED, Nikolsky E, Lasic Z, Iakovou I, Fahy M, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. (2004) 44:1393–9. doi: 10.1016/S0735-1097(04)01445-7
23. Alkhouli M, Alqahtani F, Tarabishy A, Sandhu G, Rihal CS. Incidence, predictors, and outcomes of acute ischemic stroke following percutaneous coronary intervention. JACC Cardiovasc Interv. (2019) 12:1497–506. doi: 10.1016/j.jcin.2019.04.015
24. Atti V, Gwon Y, Narayanan MA, Garcia S, Sandoval Y, Brilakis ES, et al. Multivessel versus culprit-only revascularization in STEMI and multivessel coronary artery disease: meta-analysis of randomized trials. JACC Cardiovasc Interv. (2020) 13:1571–82. doi: 10.1016/j.jcin.2020.04.055
25. Vogel B, Claessen BE, Arnold SV, Chan D, Cohen DJ, Giannitsis E, et al. ST-segment elevation myocardial infarction. Nat Rev Dis Primers. (2019) 5:39. doi: 10.1038/s41572-019-0090-3
26. Mitnitski AB, Rutenberg AD, Farrell S, Rockwood K. Aging, frailty and complex networks. Biogerontology. (2017) 18:433–46. doi: 10.1007/s10522-017-9684-x
27. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. (2013) 381:752–62. doi: 10.1016/S0140-6736(12)62167-9
28. Scholz KH, Maier SKG, Maier LS, Lengenfelder B, Jacobshagen C, Jung J, et al. Impact of treatment delay on mortality in ST-segment elevation myocardial infarction (STEMI) patients presenting with and without haemodynamic instability: results from the German prospective, multicentre FITT-STEMI trial. Eur Heart J. (2018) 39:1065–74. doi: 10.1093/eurheartj/ehy004
29. Pandharipande PP, Girard TD, Jackson JC, Morandi A, Thompson JL, Pun BT, et al. Long-term cognitive impairment after critical illness. N Engl J Med. (2013) 369:1306–16. doi: 10.1056/NEJMoa1301372
Keywords: ST-segment elevation myocardial infarction, thrombolysis in myocardial infarction risk index, percutaneous coronary intervention, elderly patients, in-hospital death risk
Citation: Fu B, Wei X, Wang Q, Yang Z, Chen J and Yu D (2021) Use of the Thrombolysis in Myocardial Infarction Risk Index for Elderly Patients With ST-Segment Elevation Myocardial Infarction. Front. Cardiovasc. Med. 8:743678. doi: 10.3389/fcvm.2021.743678
Received: 19 July 2021; Accepted: 28 October 2021;
Published: 19 November 2021.
Edited by:
Hai-Yan Qian, Chinese Academy of Medical Sciences and Peking Union Medical College, ChinaReviewed by:
Lin Fan, Fujian Medical University Union Hospital, ChinaCopyright © 2021 Fu, Wei, Wang, Yang, Chen and Yu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Danqing Yu, Z2R5ZHExMDBAMTI2LmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.