 Sivabaskari Pasupathy1,2,3
Sivabaskari Pasupathy1,2,3 Bertil Lindahl4Rosanna Tavella1,2,3Anna M. Nordenskjöld5Christopher Zeitz1,2,3
Bertil Lindahl4Rosanna Tavella1,2,3Anna M. Nordenskjöld5Christopher Zeitz1,2,3 Margaret Arstall1,6Matthew Worthley1,2Christopher Neil7
Margaret Arstall1,6Matthew Worthley1,2Christopher Neil7 Kuljit Singh8Stuart Turner9Adil Rajwani10John Mooney11
Kuljit Singh8Stuart Turner9Adil Rajwani10John Mooney11 John F. Beltrame1,2,3*
John F. Beltrame1,2,3*- 1Faculty of Health Sciences, The University of Adelaide, Adelaide, SA, Australia
- 2Department of Cardiology, Central Adelaide Local Health Network, Adelaide, SA, Australia
- 3Basil Hetzel Institute, Adelaide, SA, Australia
- 4Department of Medical Sciences and Uppsala Clinical Research Center, Uppsala University, Uppsala, Sweden
- 5Department of Cardiology, School of Medical Sciences, Örebro University, Örebro, Sweden
- 6Department of Cardiology, Northern Adelaide Local Health Network, Adelaide, SA, Australia
- 7Department of Medicine, University of Melbourne, Melbourne, VIC, Australia
- 8Department of Medicine, Griffith University, Gold Coast, QLD, Australia
- 9Department of Cardiology, John Hunter Hospital, Newcastle, NSW, Australia
- 10Department of Cardiology, Royal Perth Hospital, Perth, WA, Australia
- 11Department of Cardiology, Gosford Hospital, Gosford, NSW, Australia
Introduction: Myocardial infarction with non-obstructive coronary arteries (MINOCA) occurs in ~10% of all patients with acute myocardial infarction (AMI), with an over-representation amongst women. Remarkably, it is estimated that as many as 1 in 4 patients with MINOCA experience ongoing angina at 12 months despite having no flow-restricting stenoses in their epicardial arteries. This manuscript presents the rationale behind Randomized Evaluation of Beta Blocker and Angiotensin-converting enzyme inhibitors/Angiotensin Receptor Blocker Treatment (ACEI/ARB) for Post Infarct Angina in MINOCA patients—The MINOCA BAT post infarct angina sub study.
Methods: This trial is a registry-based, randomized, parallel, open-label, multicenter trial with 2 × 2 factorial design. The primary aim is to determine whether oral beta blockade compared with no oral beta blockade, and ACEI/ARB compared with no ACEI/ARB, reduce post infarct angina in patients discharged after MINOCA without clinical signs of heart failure and with left ventricular ejection fraction ≥40%. A total of 664 patients will be randomized into four groups; (i) ACEI/ARB with beta blocker, (ii) beta blocker only, (iii) ACEI/ARB only, or (iv) neither ACEI/ARB nor beta blocker and followed for 12 months.
Results: The trial is currently recruiting in Australia and Sweden. Fifty six patients have been recruited thus far. Both sexes were equally distributed (52% women and 48% men) and the mean age was 56.3 ± 9.9 years.
Conclusions: It remains unclear whether conventional secondary preventive therapies are beneficial to MINOCA patients in regard to post infarct angina. Existing registry-based literature suggest cardioprotective agents are less likely to be used in MINOCA patients. Thus, results from this trial will provide insights for future treatment strategies and guidelines specific to MINOCA patients.
Introduction
Myocardial Infarction with Non-Obstructive Coronary Arteries (MINOCA) refers to patients presenting with acute myocardial infarction (AMI) without angiographically evident obstructive (defined as ≥50% diameter stenosis) coronary artery disease (CAD). The reported prevalence of MINOCA has been between 5 and 14% with most recent large AMI registries reports ~10% of AMI population identified as MINOCA (1). Compared to conventional AMI patients (AMI with obstructive CAD–MICAD), MINOCA patients are more likely be females, younger and have fewer cardiovascular risk factors (2). The underlying pathophysiological mechanisms are poorly understood in these patients, although several different ischemic mechanisms have been proposed including plaque disruption, coronary artery spasm, microvascular dysfunction, thromboembolism, and coronary dissection (3). Furthermore, short- and long-term prognosis of MINOCA patients is comparatively more favorable than those with MICAD and worse as compared to the general population (4, 5). Moreover, Grodzinsky et al. (6) compared the post-MI angina and health status during the MI hospitalization and at 1, 6, and 12-months following MI using the Seattle Angina Questionnaire (SAQ) between MINOCA and those with MICAD. MINOCA patients had a high prevalence of angina during follow-up, with one in four patients reporting angina at 1 year after MI. In addition, MINOCA patients also reported worse disease-specific and generic health status at 12 months post-MI, including worse quality of life due to angina and lower satisfaction with the treatment of their angina (6).
Regarding medical management of these patients, clinical registry based studies suggest MINOCA patients are often less likely to receive secondary preventive medications when compared to MICAD patients (7–9). However, studies have reported benefits of ACEI/ARB therapy (10–13), statin therapy (11, 14), and beta blocker (15) therapy in MINOCA. In particular, Lindahl et al. (13) using data from the Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies (SWEDEHEART) registry of 9,136 MINOCA patients showed that 24% experienced a Major Adverse Coronary Events (MACE) during a mean follow-up period of 4.1 years. The MACE components included a mortality of 13.4%, non-fatal MI in 7.1%, non-fatal stroke in 4.3%, and heart failure hospitalization in 6.4%. In propensity score matched comparisons, there was a significant 18% reduction in experiencing a MACE with Angiotensin-converting enzyme inhibitors/Angiotensin Receptor Blocker Therapy (ACEI/ARB) and a non-significant 14% trend with the use of beta-blockers, compared with respective control groups (13). This observational data is being evaluated in an international multicenter, randomized, controlled, open-label clinical study assessing the impact of ACEI/ARB and/or beta blockers on MACE, with the study methods recently published (16). This manuscript details the methods used in the MINOCA BAT Post Infarct Angina sub-study, which is embedded within the MINOCA BAT Trial utilizing its infrastructure to investigate the post-infarct anti-anginal benefit of Beta Blocker and ACEI/ARB in MINOCA patients.
Methods
MINOCA-BAT Post-infarct angina trial is a prospectively designed sub-study of the MINOCA-BAT trial; an investigator-initiated, registry-based, pragmatically designed, international, multicenter, open-labeled, 2 × 2 factorial design, randomized controlled trial (RCT) evaluating the impact of beta-blockers and/or ACEI/ARB on MACE. In the Post-infarct angina substudy, the impact of these therapies on health outcomes will be evaluated. Recruitment has commenced in Australia and Sweden with funding obtained from local sources, including the not-for-profit The Hospital Research Foundation in Australia and the Swedish Government's Swedish Research Council in Sweden. The intention to treat principle will be applied to analyze the study outcomes. The study is currently recruiting in Australia and Sweden.
The primary aim of this study is to determine whether oral beta-blocker and/or ACEI/ARB in patients with MINOCA and LV-EF ≥ 40% without clinical signs of heart failure impacts on post-infarct angina at 12 months, where angina frequency is assessed with SAQ-7. The secondary aims are to determine the impact of these treatment in (i) angina frequency, physical limitation, quality of life and patient satisfaction as scored by the SAQ-7 at 12 months. (ii) health related quality of life by EQ 5D at 12 months and (iii) mental health and depression scored by PHQ at 12 months.
Definition of MINOCA
The definition of MINOCA has evolved over the years. In this study, utilizing the pragmatic approach, MINOCA is defined as per the European Society of Cardiology working group criteria (15). As per contemporary AMI guidelines (17), the MINOCA patients should have evidence of myocardial ischemia as the underlying cause for the myocardial injury. Therefore, in this study, efforts are made to exclude non-ischemic and non-cardiac conditions that could mimic the presentation of acute MI such as Takotsubo, Myocarditis, pulmonary embolism, etc.
Hypothesis and Study End Points
The hypothesis of this study is treatment with beta blockers and/or ACEI/ARBs will reduce angina frequency in MINOCA patients with preserved LV-EF. The primary endpoint is to assess the angina frequency measured by SAQ-7 at 12 months. Secondary endpoints are health status measurement scores at 12 months as follows: (a) Angina stability, physical limitation, quality of life and patient satisfaction as scored by the SAQ-7. (b) Health related quality of life by EQ 5D. (c) Mental health and depression scored by PHQ 9. The specifics of these instruments are detailed in Table 1. Safety endpoints include readmission because for second- or third-degree AV-block, ventricular tachycardia, ventricular fibrillation, hypotension, acute kidney injury, syncope, or need for pacemaker.
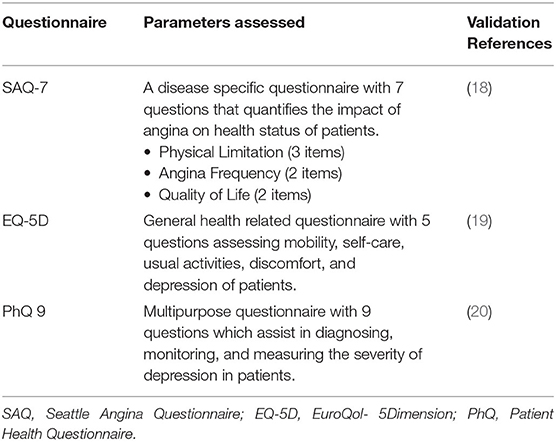
Table 1. Parameters and validity of health-related quality of life instruments.
Inclusion/Exclusion Criteria
Patients above 18 years of age with a clinical diagnosis of MINOCA as shown in Table 2 with LV-EF ≥40% (assessed by left ventriculography, echocardiography or cardiac magnetic resonance imaging) will be approached to participate in this trial. Patients will be excluded if they have any of the following conditions that may affect their ability to comply with study protocol: pregnancy, prior revascularization treatment (e.g., percutaneous coronary intervention), diagnosis of myocarditis, takotsubo or heart failure, and any known contraindication or new indication or continuation to the study drugs.
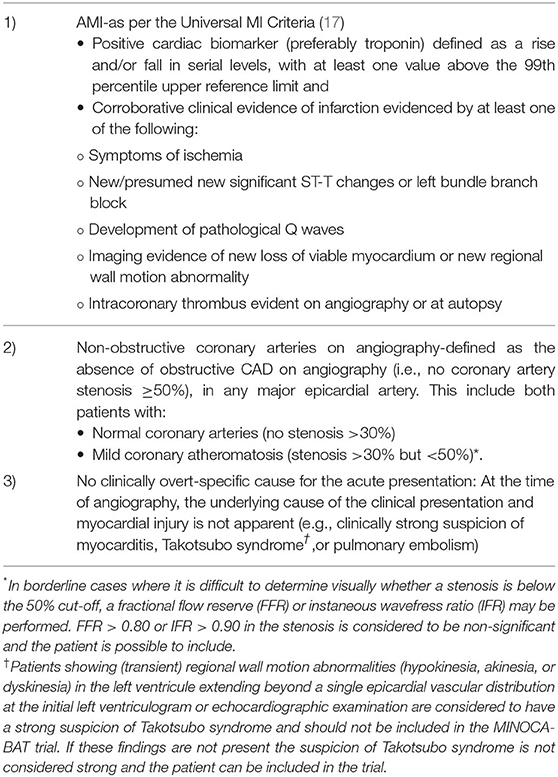
Table 2. Definition of MINOCA as described in the MINOCA-BAT Trial (16).
Study Protocol, Randomization, Participating Countries, and Ethics
This registry based RCT will operate within the established Coronary Angiogram Database of South Australia (CADOSA) and SWEDEHEART (Sweden) Registries, where patients with MINOCA will be readily identified following coronary angiography. Additional sites without the registries will identify patients via their treating cardiology departments. Efforts are encouraged to exclude non-ischemic conditions such as clinically undetected myocarditis prior to randomization. Patients fulfilling the inclusion criteria and without any exclusion criterion will, after signing the informed consent form, be randomized on day 1–30 after index MINOCA. The data collection is performed by trained clinical trial staff. The study timeline overview is shown in Figure 1. The study is approved by Central Adelaide Local Health Network Human Research Ethics Committee (HREC/18/CALHN/157) in Australia and by relevant ethics review board in Sweden. ANZCTR Registration: ACTRN12618001858280.
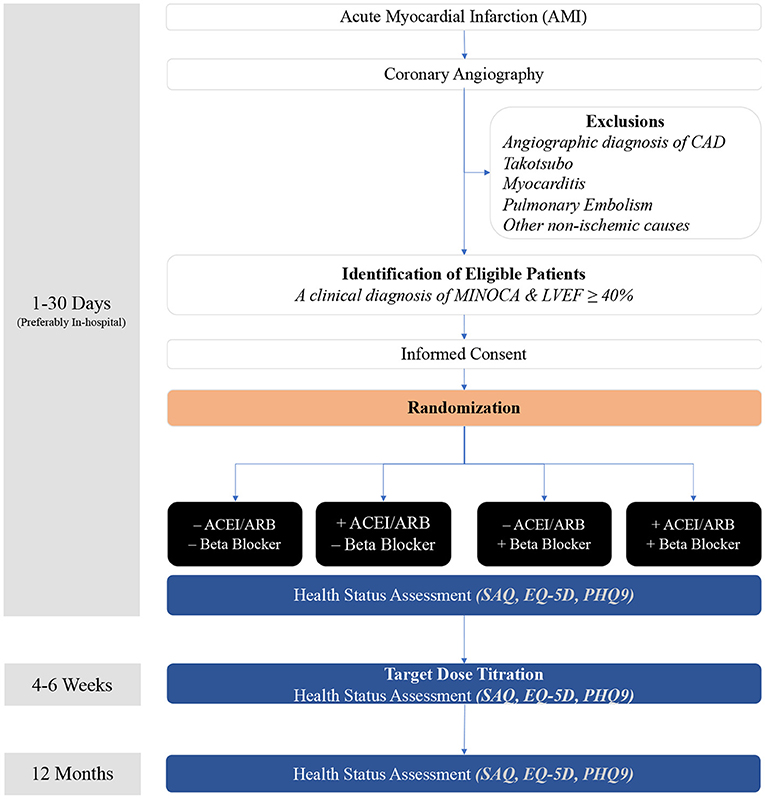
Figure 1. Study flow chart.
The randomization will be performed in the module using permuted block randomization with 1:1:1:1 ratio, stratified by country. Randomization can be performed at any time day 1–30 after index MI. Patients may be randomized the same day as index AMI, e.g., day 1. The patients will be randomized to either beta blocker alone, ACEI/ARB alone or both beta blocker and ACE/ARB, or neither beta blocker nor ACEI/ARB. If randomized to study drug groups, the investigator will record the agent(s) chosen, the starting dose(s) and target dose(s) planned in the case report form. Control group patients randomized to neither beta blocker nor ACEI/ARB will not receive these study drugs.
Consistent with the pragmatic design and absence of industry support, the study drug class will be specified by the randomization protocol but not the specific agent, which will be determined by local practices. In Australia, the preferred study treatments will be atenolol and perindopril/candesartan, whereas in Sweden it will include bisoprolol/metoprolol and ramipril/enalapril/losartan/candesartan; however, the choice will be at the discretion of the treating clinician. The regional preferred treatments, including initial and target doses are summarized in Table 3. At the 6-week follow-up visit, the current dosage of the study treatments will be noted. This visit will be achieved via phone/on-line follow-up. Other therapies will be at the treating clinician's discretion but will be recorded at the follow-up visits.
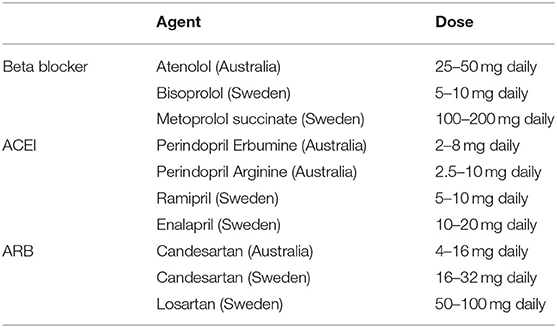
Table 3. Preferred study treatments in Australia & Sweden.
Patients will be followed-up by a visit at 4–6 weeks after randomization and then at 12 months. The study commenced with patients enrolled in Australia in January 2019 and in Sweden May 2021. The adherence to the randomized drug(s) will be assessed at the follow-up visits at 4–6 weeks, and 12 months after randomization.
Outcomes
Randomized patients will be followed regarding angina status, quality of life, mental health status, atrial fibrillation, renal failure, second- or third-degrees AV-block, hypotension, syncope and pacemaker implantation. These will be assessed at baseline, 4–6 weeks and 12 months, with the primary endpoint be the 12-month angina frequency.
Safety
The safety data will be extracted directly from patients during follow up and from hospital/medical records or administrative data at the end of follow up. In addition, participants will be queried on any hospital admissions during the follow ups. The study steering committee appointed a data safety monitoring board (DSMB), comprised of three senior clinicians, without any affiliation with the Sponsor, the Coordinating Investigator, or local Investigators and with previous experience of working in a DSMB. The DSMB will oversee the safety of the study drugs and the general execution of the trial on behalf of the trial participants.
Data Analysis
The data will be inspected graphically to establish normality prior to analysis. To identify potential confounders, chi squared or Student's t-test will be performed, to test the association between demographic or clinical characteristics of the sample at baseline and Angina Frequency as measured by the SAQ. For all endpoints, differences at baseline and 12 months between the beta-blocker treatment groups and the ACEI/ARB treatment groups will be analyzed using a repeated measures ANCOVA, adjusting for potential confounders. In addition, to investigate for trends over time in the SAQ Angina Frequency, score between the treatment groups, using all 4-time points in a mixed model approach. Subjects with missing data will be included in analyses, as data collection at every time point does not need to be adhered to in mixed models. Similar analyses will also be performed for the EQ-5D and PHQ-9.
Sample Size
The study by Grodzinsky et al. (6) reported a post-infarct SAQ angina frequency score of 85 ± 21, thus, to detect a 20% change in SAQ angina frequency with a power of 0.9 at the alpha 0.05 level, 149 patients/study group are required (i.e., 596 MINOCA patients). Allowing for a 10% dropout then 664 patients will be recruited into this trial. The data collection will continue until the target number is achieved.
Results
By 12 May 2021, 56 patients have been recruited in the study, 54 in Australia and 2 in Sweden respectively. Men and women were equally distributed (52% women and 48% men) and the mean age was 56.3 ± 9.9 years.
Discussion
MINOCA is now an established clinical entity with heterogenous pathophysiology. Despite being apparent as early as the 80s, the management of these patients has not been addressed. It cannot be assumed that proven therapies in AMI patients with obstructive CAD are effective in MINOCA since (a) AMI pathogenetic mechanisms differ, (b) the prognosis differs with reduced mortality and re-infarction, (c) observational data suggest that some established therapies in MICAD (i.e., dual anti-platelet agents) are ineffective in MINOCA. Accordingly, randomized controlled clinical trials are required to identify the optimal therapy for patients with MINOCA.
Minoca Bat Trial and Post Infarct Angina Sub Study
The ongoing main MINOCA BAT trial (16) will address the impact of ACEIs/ARBs and beta-blockers on MACE (defined as all-cause mortality, readmission because of MI, ischemic stroke, or heart failure) by randomizing ~3,500 patients with MINOCA. The post-infarct angina sub study will provide insights into the effectiveness of the trial therapies in controlling post-infarct angina, nestled within the construct of the main MINOCA-BAT clinical trial. Since the ischemic pathophysiology in MINOCA may differ to MICAD [i.e., coronary vasospasm, coronary microvascular dysfunction, coronary embolism/thrombosis, or spontaneous coronary artery dissection (21) may contribute], then conventional therapies may be ineffective.
Beta-blockers are a well-established anti-anginal agents in patients with obstructive CAD (22) and are effective in patients with coronary microvascular dysfunction (23); however they may be detrimental in patients with epicardial coronary artery spasm (24). Thus, whether their use will prevent/limit the occurrence of post-infarct angina in the heterogenous MINOCA disorder will be a key finding of this study. Furthermore, ACEI have been shown to have anti-anginal effects in patients with coronary microvascular dysfunction (25), although their benefits in other coronary vasomotor disorders remains unclear. Hence this study will provide key insights into the impact of blocking beta receptors and inhibiting the renin-angiotensin pathway.
Strength and Limitations
The strength of this study is its pragmatic design as it evaluates effects of treatment in a real-world context; a positive result in this study can inform practice because it provides evidence that the treatment/intervention is effective in routine clinical practice. The findings of the study will be limited by (i) the undefined heterogeneity in pathophysiologic ischemic mechanisms—i.e., unable to delineate which patients have coronary spasm, microvascular dysfunction, or other causes of the myocardial infarct; (ii) therapeutic heterogeneity—i.e., variability in specific agents and dosages used within the randomized treatment drug classes; (iii) pharmacokinetic heterogeneity of drugs used within the class (iv) open label study design; (v) patients without a predisposition for ongoing angina may be randomized. The impact of some of these prospectively identified limitations will become apparent on the completion of the trial.
Conclusions
MINOCA patients are less likely to receive cardio-protective therapies and have a significant prevalence of post infarct angina and poor quality of life. There are no clinical trials to date that have examined the benefit of these agents in MINOCA and thus there are no clinical guidelines currently available for the preventive management of these patients. There is a clear need to study these patients post infarct angina management strategies and this study is designed to meet this need.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Central Adelaide Local Health Network Human Research Ethics Committee. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
SP wrote the first draft of the manuscript. JB and BL critically revised the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
Funding
The Australian study sites are supported by the funding from The Hospital Research Foundation, a not-for-profit organization, which provides research grants to South Australian public hospitals. The grant awarded was entitled The Basil Hetzel Translational Grant 2017. The Swedish Government's Swedish Research Council have contributed to the Swedish part of the study as well as for design and maintenance of the database and the international randomization module (Grant 2017-00478).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Najib K, Boateng S, Sangodkar S, Mahmood S, Whitney H, Wang CE, et al. Incidence and characteristics of patients presenting with acute myocardial infarction and non-obstructive coronary artery disease. Catheter Cardiovasc Interv. (2015) 86:S23–7. doi: 10.1002/ccd.26043
2. Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation. (2015) 131:861–70. doi: 10.1161/CIRCULATIONAHA.114.011201
3. Pasupathy S, Tavella R, Beltrame JF. Myocardial infarction with Nonobstructive Coronary Arteries (MINOCA): the past, present, and future management. Circulation. (2017) 135:1490–3. doi: 10.1161/CIRCULATIONAHA.117.027666
4. Eggers KM, Hjort M, Baron T, Jernberg T, Nordenskjöld AM, Tornvall P, et al. Morbidity and cause-specific mortality in first-time myocardial infarction with nonobstructive coronary arteries. J Intern Med. (2019) 285:419–28. doi: 10.1111/joim.12857
5. Williams MJA, Barr PR, Lee M, Poppe KK, Kerr AJ. Outcome after myocardial infarction without obstructive coronary artery disease. Heart. (2019) 105:524–30. doi: 10.1136/heartjnl-2018-313665
6. Grodzinsky A, Arnold SV, Gosch K, Spertus JA, Foody JM, Beltrame J, et al. Angina frequency after acute myocardial infarction in patients without obstructive coronary artery disease. Eur Heart J Qual Care Clin Outcomes. (2015) 1:92–9. doi: 10.1093/ehjqcco/qcv014
7. Smilowitz NR, Dubner R, Hellkamp AS, Widmer RJ, Reynolds HR. Variability of discharge medical therapy for secondary prevention among patients with myocardial infarction with non-obstructive coronary arteries (MINOCA) in the United States. PLoS ONE. (2021) 16:e0255462. doi: 10.1371/journal.pone.0255462
8. Choo EH, Chang K, Lee KY, Lee D, Kim JG, Ahn Y, et al. Prognosis and predictors of mortality in patients suffering myocardial infarction with non-obstructive coronary arteries. J Am Heart Assoc. (2019) 8:e011990. doi: 10.1161/JAHA.119.011990
9. Abdu FA, Liu L, Mohammed AQ, Luo Y, Xu S, Auckle R, et al. Myocardial infarction with non-obstructive coronary arteries (MINOCA) in Chinese patients: clinical features, treatment and 1year follow-up. Int J Cardiol. (2019) 287:27–31. doi: 10.1016/j.ijcard.2019.02.036
10. Manfrini O, Morrell C, Das R, Barth JH, Hall AS, Gale CP, et al. Effects of angiotensin-converting enzyme inhibitors and beta blockers on clinical outcomes in patients with and without coronary artery obstructions at angiography (from a Register-Based Cohort Study on Acute Coronary Syndromes). Am J Cardiol. (2014) 113:1628–33. doi: 10.1016/j.amjcard.2014.02.015
11. Paolisso P, Bergamaschi L, Saturi G, D'Angelo EC, Magnani I, Toniolo S, et al. Secondary prevention medical therapy and outcomes in patients with myocardial infarction with non-obstructive coronary artery disease. Front Pharmacol. (2019) 10:1606. doi: 10.3389/fphar.2019.01606
12. Ahn JH, Hyun JY, Jeong MH, Kim JH, Hong YJ, Sim DS, et al. Comparative effect of angiotensin converting enzyme inhibitor versus angiotensin ii type i receptor blocker in acute myocardial infarction with non-obstructive coronary arteries; from the Korea Acute Myocardial Infarction Registry - National Institute of Health. Cardiol J. (2020) 28:738–45. doi: 10.5603/CJ.a2020.0130
13. Lindahl B, Baron T, Erlinge D, Hadziosmanovic N, Nordenskjöld A, Gard A, et al. Medical therapy for secondary prevention and long-term outcome in patients with myocardial infarction with nonobstructive coronary artery disease. Circulation. (2017) 135:1481–9. doi: 10.1161/CIRCULATIONAHA.116.026336
14. Kovach CP, Hebbe A, O'Donnell CI, Plomondon ME, Hess PL, Rahman A, et al. Comparison of patients with nonobstructive coronary artery disease with versus without myocardial infarction (from the VA Clinical Assessment Reporting and Tracking [CART] Program). Am J Cardiol. (2021) 146:1–7. doi: 10.1016/j.amjcard.2021.01.015
15. Agewall S, Beltrame JF, Reynolds HR, Niessner A, Rosano G, Caforio AL, et al. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J. (2017) 38:143–53. doi: 10.1093/eurheartj/ehw149
16. Nordenskjöld AM, Agewall S, Atar D, Baron T, Beltrame J, Bergström O, et al. Randomized evaluation of beta blocker and ACE-inhibitor/angiotensin receptor blocker treatment in patients with myocardial infarction with non-obstructive coronary arteries (MINOCA-BAT): rationale and design. Am Heart J. (2021) 231:96–104. doi: 10.1016/j.ahj.2020.10.059
17. Thygesen K, Alpert JS, Alpert JS, Jaffe AS, Chaitman BR, Chaitman BR, et al. Fourth universal definition of myocardial infarction. Circulation. (2018) 138:e618–51. doi: 10.1161/CIR.0000000000000617
18. Chan PS, Jones PG, Arnold SA, Spertus JA. Development and validation of a short version of the Seattle angina questionnaire. Circ Cardiovasc Qual Outcomes. (2014) 7:640–7. doi: 10.1161/CIRCOUTCOMES.114.000967
19. Nowels D, McGloin J, Westfall JM, Holcomb S. Validation of the EQ-5D quality of life instrument in patients after myocardial infarction. Qual Life Res. (2005) 14:95–105. doi: 10.1007/s11136-004-0614-4
20. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. (2001) 16:606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
21. Tamis-Holland JE, Jneid H, Reynolds HR, Agewall S, Brilakis ES, Brown TM, et al. Contemporary diagnosis and management of patients with myocardial infarction in the absence of obstructive coronary artery disease: a scientific statement from the american heart association. Circulation. (2019) 139:e891–908. doi: 10.1161/CIR.0000000000000670
22. Gibbons RJ, Chatterjee K, Daley J, Douglas JS, Fihn SD, Gardin JM, et al. ACC/AHA/ACP-ASIM guidelines for the management of patients with chronic stable angina: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Patients With Chronic Stable Angina). J Am Coll Cardiol. (1999) 33:2092–197. doi: 10.1016/s0735-1097(99)00150-3
23. Lanza GA, Colonna G, Pasceri V, Maseri A. Atenolol versus amlodipine versus isosorbide-5-mononitrate on anginal symptoms in syndrome X. Am J Cardiol. (1999) 84:854–6, a8. doi: 10.1016/S0002-9149(99)00450-6
Keywords: myocardial infarction, coronary angiogram, normal coronary angiography, non-obstructive coronary artery disease (NOCAD), Myocardial Infarction with Non Obstrucrive Coronary Arteries (MINOCA)
Citation: Pasupathy S, Lindahl B, Tavella R, Nordenskjöld AM, Zeitz C, Arstall M, Worthley M, Neil C, Singh K, Turner S, Rajwani A, Mooney J and Beltrame JF (2021) Randomized Evaluation of Beta Blocker and ACE-Inhibitor/Angiotensin Receptor Blocker Treatment for Post Infarct Angina in Patients With Myocardial Infarction With Non-obstructive Coronary Arteries: A MINOCA-BAT Sub Study Rationale and Design. Front. Cardiovasc. Med. 8:717526. doi: 10.3389/fcvm.2021.717526
Received: 31 May 2021; Accepted: 07 September 2021;
Published: 08 October 2021.
Edited by:
Tim van de Hoef, Academic Medical Center, NetherlandsReviewed by:
Raffaele Bugiardini, University of Bologna, ItalyRenata Cífková, Thomayer University Hospital, Czechia
Copyright © 2021 Pasupathy, Lindahl, Tavella, Nordenskjöld, Zeitz, Arstall, Worthley, Neil, Singh, Turner, Rajwani, Mooney and Beltrame. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: John F. Beltrame, am9obi5iZWx0cmFtZUBhZGVsYWlkZS5lZHUuYXU=