 Xiankun Chen1,2,3
Xiankun Chen1,2,3 Wei Jiang3,4
Wei Jiang3,4 Thomas P. Olson5
Thomas P. Olson5 Cecilia Stålsby Lundborg1
Cecilia Stålsby Lundborg1 Zehuai Wen2,6*Weihui Lu3,4,7*Gaetano Marrone1
Zehuai Wen2,6*Weihui Lu3,4,7*Gaetano Marrone1- 1Health Systems and Policy, Department of Global Public Health, Karolinska Institutet, Stockholm, Sweden
- 2Key Unit of Methodology in Clinical Research, Guangdong Provincial Hospital of Chinese Medicine, Guangzhou, China
- 3The Second Affiliated Hospital of Guangzhou University of Chinese Medicine, Guangzhou, China
- 4Department of Cardiology, Guangdong Provincial Hospital of Chinese Medicine, Guangzhou, China
- 5Division of Cardiovascular Diseases, Department of Internal Medicine, Mayo Clinic and Foundation, Rochester, MN, United States
- 6National Centre for Design Measurement and Evaluation in Clinical Research, Guangzhou University of Chinese Medicine, Guangzhou, China
- 7Heart Failure Center/Department of Cardiology, Guangdong Provincial Hospital of Chinese Medicine, Guangzhou, China
Aims: The Baduanjin Eight-Silken-Movements wIth Self-Efficacy building for Heart Failure (BESMILE-HF) program is a contextually adapted cardiac rehabilitation program. It uses a traditional Chinese exercise, Baduanjin, to solve the unmet demand of exercise-based cardiac rehabilitation programs due to their scarcity and unaffordability in China. This pilot study assesses BESMILE-HF's feasibility and preliminary effects.
Methods: Eighteen patients with chronic heart failure were included: 8 in a BESMILE-HF group (age: 67 ± 5 years, EF: 40.4 ± 13.6%) and 10 in a control group (age: 70 ± 13 years, EF: 42.9 ± 12.5%). Both received the usual medications, with the intervention group receiving additionally the BESMILE-HF program for 6 weeks. Feasibility was explored by participants' involvement in the intended intervention. Clinical outcome assessments were conducted at baseline and post-intervention, while adverse events were captured throughout the study period.
Results: The BESMILE-HF program was well-received by patients, and adherence to the intervention was good. The intervention group completed all required home exercises and total home-practice time was correlated with baseline self-efficacy (r = 0.831, p = 0.011). Moreover, after 6 weeks, self-efficacy increased in the BESMILE-HF group (p = 0.028) and the change was higher than in the control [mean difference (MD): 3.2; 95% confidence interval (CI) 0.6–5.9, p = 0.004]. For the exercise capacity, the control group demonstrated a significant decline in peak oxygen consumption (p =0.018) whereas, the BESMILE-HF group maintained their exercise capacity (p = 0.063). Although the between-group difference was not statistically significance, there was clear clinical improvement in the BESMILE-HF group (1.5 mL/kg/min, 95% CI, −0.3 to 3.2 vs. minimal clinically important difference of 1 mL/kg/min). Throughout the study period, no adverse events related to the intervention were captured.
Conclusions: BESMILE-HF is feasible for patients with chronic heart failure in Chinese settings. A larger sample size and a longer follow-up period is needed to confirm its benefit on clinical outcomes.
Clinical Trial Registration: ClinicalTrials.gov: NCT03180320.
Introduction
A hallmark symptom of chronic heart failure (CHF) is impaired exercise tolerance and poor quality of life. Exercise-based cardiac rehabilitation (EBCR) is a proven therapy to improve exercise capacity and quality of life in these patients (1, 2). However, the sub-optimal use of EBCR remains troubling and warrants high priority in global healthcare (3).
While many countries have reported gaps in patient referrals to existing EBCR programs, China has faced an even greater “upstream” challenge—a lack of available EBCR programs (4). One national survey showed that only 24% of China's tertiary hospitals have EBCR programs (5). Unfortunately, the type of comprehensive EBCR programs delivered in high income countries are not feasible in China due to the dearth of rehabilitation facilities, trained professionals, as well as unaffordability (5).
Home-based exercises can empower patients to take responsibility and accountability for their own disease management (6). Most importantly, they increase patients' access to EBCR by confronting the challenge of limited healthcare resources. This includes the paucity of rehabilitation facilities, the lack of medical reimbursement, and sub-standard access to hospital services in rural areas in China (7).
One possible solution tailored to the Chinese setting is traditional Baduanjin exercise which is usually practiced at home. Baduanjin, translated as Eight Silken Movements, is a form of ancient martial arts that originated in China and has been culturally accepted as being beneficial to one's health in Chinese society (8). This practice has evolved based on traditional Chinese medicine theory and is characterized by interplay between flowing circular physical postures and movements, mindfulness, and breathing exercise in harmony (9). Baduanjin is easy to learn and has minimal physical and cognitive demands because it entails only eight simple movements.
A novel and contextually adapted EBCR program using Baduanjin, BESMILE-HF, has recently been developed at the Guangdong Provincial Hospital of Chinese Medicine (GPHCM)—a tertiary care hospital and one of the oldest and largest Chinese medicine hospital groups in China (10). BESMILE-HF is an acronym for the Baduanjin Eight-Silken-Movement wIth SeLf-Efficacy building for Heart Failure (10). In this program, Baduanjin has been applied as the core constituent in a multi-component EBCR including evaluation, consultancy, and education, as well as a series of self-efficacy building strategies to increase adherence, and to maintain exercise compliance over time.
However, uncertainties remain regarding the use of Baduanjin in an EBCR program. Therefore, we conducted a pilot study to: (1) assess the feasibility of the BESMILE-HF program regarding patients' adherence to their intended intervention protocols; and (2) attain initial estimates of the effects of the program on clinical outcomes.
Methods
The study was conducted in accordance with the Declaration of Helsinki, and the BESMILE-HF study has been approved by the Ethics Committee at the GPHCM (number: B2016–202-01) and registered (ClinicalTrials.gov: NCT03180320). All patients were informed about the study, were given the possibility to ask questions and provided consent before participating in the study. Participants were told they could withdraw at any time.
Design
This pilot study was a prospective, randomized controlled trial (RCT). This report includes the recommended elements elaborated upon in the reporting guidelines for pilot RCTs (Appendix 1: CONSORT checklist) (11).
Setting
Guangzhou is the capital of Guangdong province and the 3rd-largest city in China. It is located in Southeastern China and has a permanent population of 13.5 million with over 7 million permanent residents in its urban areas (12). GPHCM is a tertiary care public hospital and has four branches in different urban districts of Guangzhou. In this hospital, cardiac rehabilitation is delivered one-on-one to individuals in the hospital outpatient clinic and includes exercise training. The most commonly used exercise is cycle ergometer. However, this service relies on out-of-pocket payment systems. This leads to a financial burden for most patients and results in low participation rate in cardiac rehabilitation.
Participants
Recruitment took place at GPHCM from August to November 2017. Potential participants were identified for eligibility assessment by (1) on-site screening at clinic visits; (2) regular screening of potential participants using electronic medical records; and (3) referrals from physicians (10). Participants were included if they had clinically stable CHF with a New York Heart Association functional (NYHA) classification of II or III without restriction on left ventricular ejection fraction (LVEF) class. The complete list of inclusion and exclusion criteria has been reported previously (10) and is listed in Appendix 2.
Schematic Process of the Pilot Study
The schematic process of the pilot study is shown in Figure 1. It is in accordance with the study protocol described previously (10).
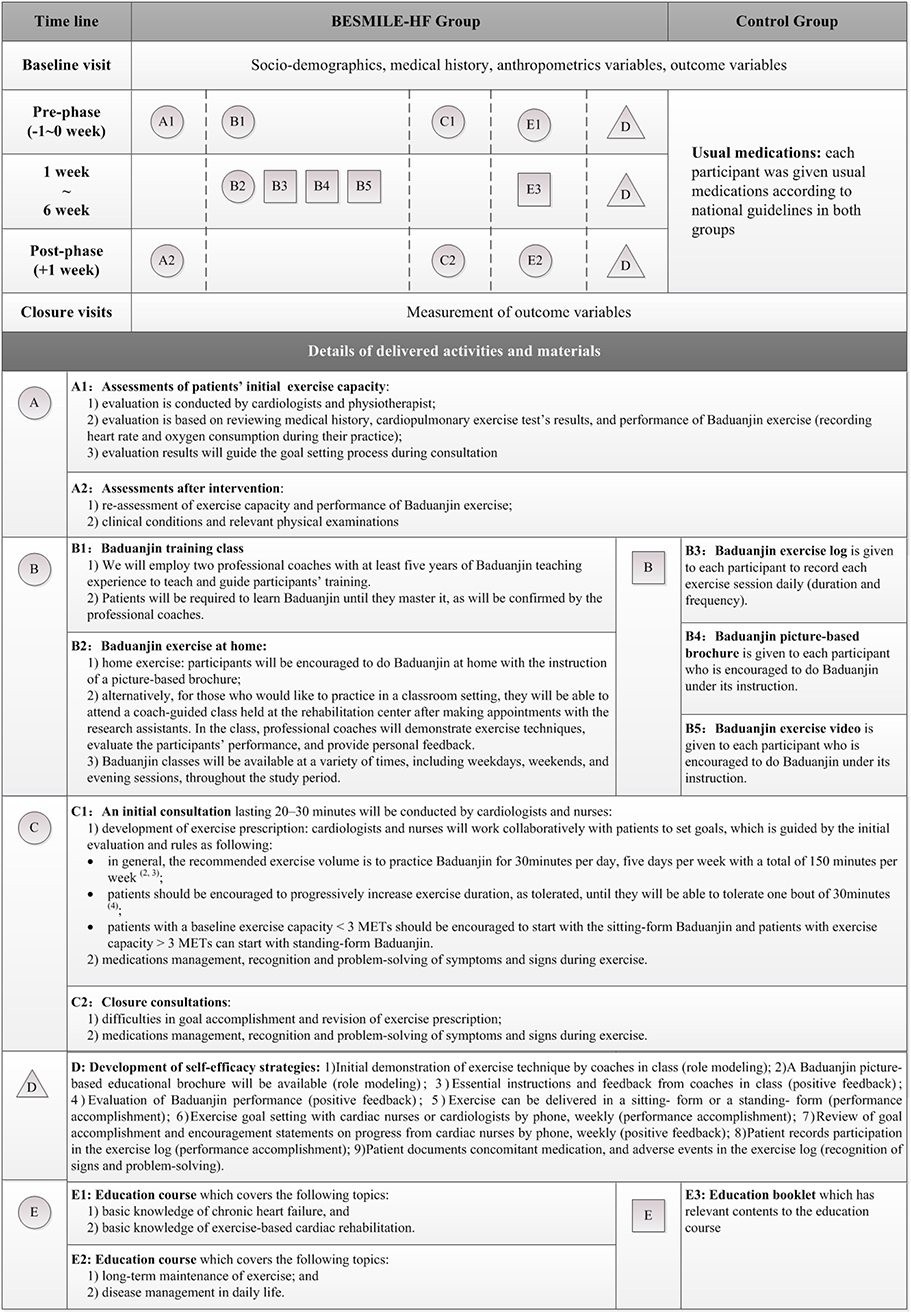
Figure 1. Graphical depiction of the BESMILE-HF program and the research schematic process for both groups, and data collection. Each component of the BESMILE-HF program is depicted separately. We regard components either as activities or materials planned to deliver to the patients. Activities are represented by circles (to reflect their flexibility) and materials by squares (to reflect their fixed nature). Different components are labeled with different letters. Below the diagram, a legend gives a brief description of each component.
Randomization, Allocation Concealment, and Blinding
Patients were informed and provided the possibility to ask questions before they signed a consent form. Eligible patients were randomized into either a BESMILE-HF group or a control group. A block randomization sequence was generated by SAS 9.2 (SAS Institute Inc., Cary, NC, USA) in a 1:1 ratio. In the pilot RCT, treatment allocation was conducted using sealed and numbered envelopes. We had made 20 numbered envelopes (a target sample size of 20 participants). As we were able to include 18 participants, hence only the first 18 envelopes were used. Given the nature of the intervention, it was not possible to blind the patients and personnel involved in conducting the programs. Outcome assessors, laboratory technicians, data managers, and statisticians were blinded to treatment allocations.
Intervention and Control
A graphical depiction of the intervention is shown in Figure 1 and the Baduanjin exercise video used in this study can be found online (13, 14). Both groups received the usual medications in accordance with national guidelines for 6 weeks (15). In the BESMILE-HF group, patients also received the pilot BESMILE-HF program. It included the core components of the full-scale 12-week BESMILE-HF program. Before the start of the 6-week home-exercise period, participants attended an exercise course to learn the eight postures at the hospital. A professional coach confirmed their performance. Following the exercise course, participants attended an educational course covering topics related to CHF, as well as exercise on the same day. Initial evaluation was conducted by the cardiologist by reviewing medical history, clinical examination results, and Baduanjin performance. Once the evaluation report was finalized, the initial consultation session was conducted by the cardiologist and the cardiology nurse. They would explain the exercise prescription and the results for the initial evaluation following pre-defined outlines. This was followed by 6-weeks of home exercise with guidance and instructions from a Baduanjin exercise demonstration video, a graphical exercise brochure, and weekly follow-up. Participants were generally required to do Baduanjin 30 min per day, 5 days per week, resulting in a total of 150 min per week. This was tailored according to individual evaluation results. Patients were asked to record their exercise performance in an exercise log (including duration in minutes and frequency) daily throughout the study period. After 6 weeks, participants were contacted to return to the hospital to attend the closure evaluation- and consultation-sessions.
Data Collection
Baseline Data
The following baseline data were collected by questionnaires and through medical chart review: (1) socio-demographics; (2) medical history; and (3) anthropometric variables.
Patient Adherence to the Intervention
Exercise compliance was collected from the self-reported exercise log. This information, along with course attendance rate, assessment- and consultation-session attendance rate, allowed characterization of patients' adherence to the intervention.
Clinical Outcome Measures From Both Groups
The following clinical outcomes proposed for a future full-scale study were collected at baseline and follow-up at the 6th week during an assessment appointment at GPHCM's Heart Failure Center. We used a cardiopulmonary exercise test to measure exercise capacity; a timed up-and-go test to measure balance and mobility; echocardiography to measure cardiac function; as well as biomarkers including N-terminal B-type natriuretic peptide (NT-proBNP), high sensitive C-reactive protein (hsCRP), hemoglobin, and lipid profile. For psychological aspects, we measured quality of life using both a validated disease-specific questionnaire, the Minnesota Living with Heart Failure Questionnaire (MLHFQ) and a generic questionnaire, the EQ5D-visual analog scale; we used the Self-Efficacy for Exercise scale (SEE) to measure exercise self-efficacy; as well as the Hospital Anxiety and Depression Scale to measure depression and anxiety status. Clinical events, such as hospitalizations and major adverse cardiac events (MACEs) and safety outcomes (adverse events), were captured throughout the study period. Details of outcome measurements have been reported previously (10) and are listed in Appendix 3.
Statistical Analysis
Baseline socio-demographic and clinical characteristics were summarized for both intervention and control groups. Continuous data were summarized as mean and deviation (SD), or as median and interquartile range (IQR); categorical data were summarized as counts and percentages. For outcome variables, a Wilcoxon signed-rank tests was used to examine changes from baseline to the 6th week within the groups. In addition, the analysis of the baseline, the 6th week, and change from baseline to the 6th week in the intervention group vs. control group was conducted using the Mann–Whitney U test. Moreover, Spearman correlation was used to explore the relationship between baseline self-efficacy and patients' total exercise time. Statistical analysis was performed in PASW Statistics 18.0 (IBM SPSS Inc., Armonk, New York, USA). p < 0.05 was considered statistically significant.
Results
A total of 322 individuals were identified. After exclusion of obvious exclusion criteria, such as contraindications to exercise or exercise test, not in the clinically stable stage, 47 (14.6%) were approached and screened for eligibility, and 36 (77%) met pre-defined criteria. They were all invited to participate in this pilot study and half of them (n = 18) refused to participate. Reasons were as followed: distance to the hospital (n = 9), unable to walk (n = 6), and unwilling to take the tests (n = 3). Female were more likely to refuse participations in our study (72.2% of the refused participants). Finally, a total of 18 (50% of those eligible) patients agreed to participate and were then randomized (Figure 2).
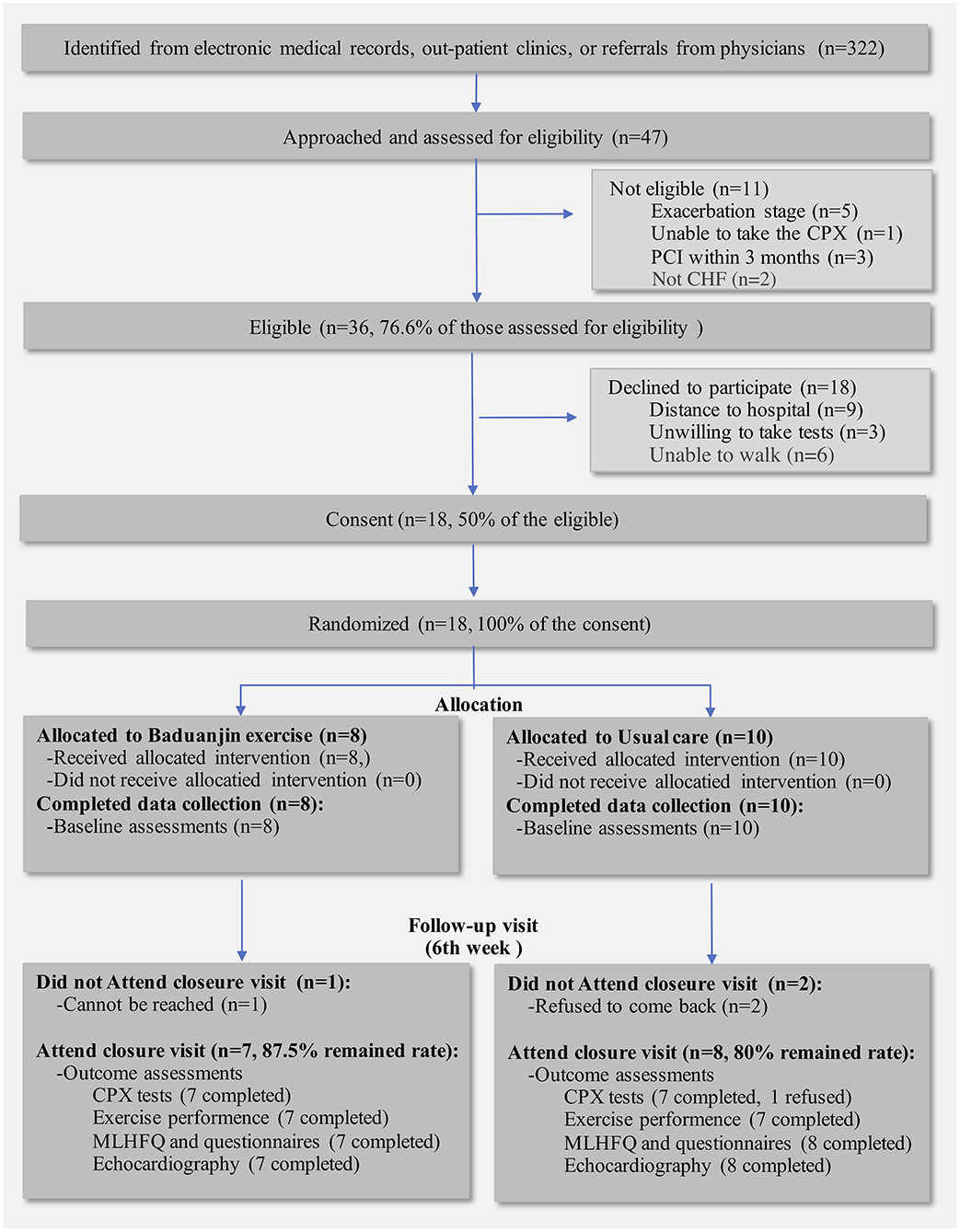
Figure 2. Flowchart of the pilot study. CPX, Cardiopulmonary exercise test; MLHFQ, Minnesota Living with Heart Failure Questionnaire.
Baseline characteristics of the included participants are shown in Table 1. The majority of the participants were male (94%) with a mean age of 68 (SD: 10). Clinically, half were NYHA Class II, and the other half were NYHA Class III; 9 (50%), 4 (22%), and 5 (28%) patients had reduced, middle-ranged, and perceived LVEF, respectively. Beta-blockers were used by 89% of the participants. The intervention and control groups were comparable on all demographic and clinical characteristics, expect for history of coronary heart disease.
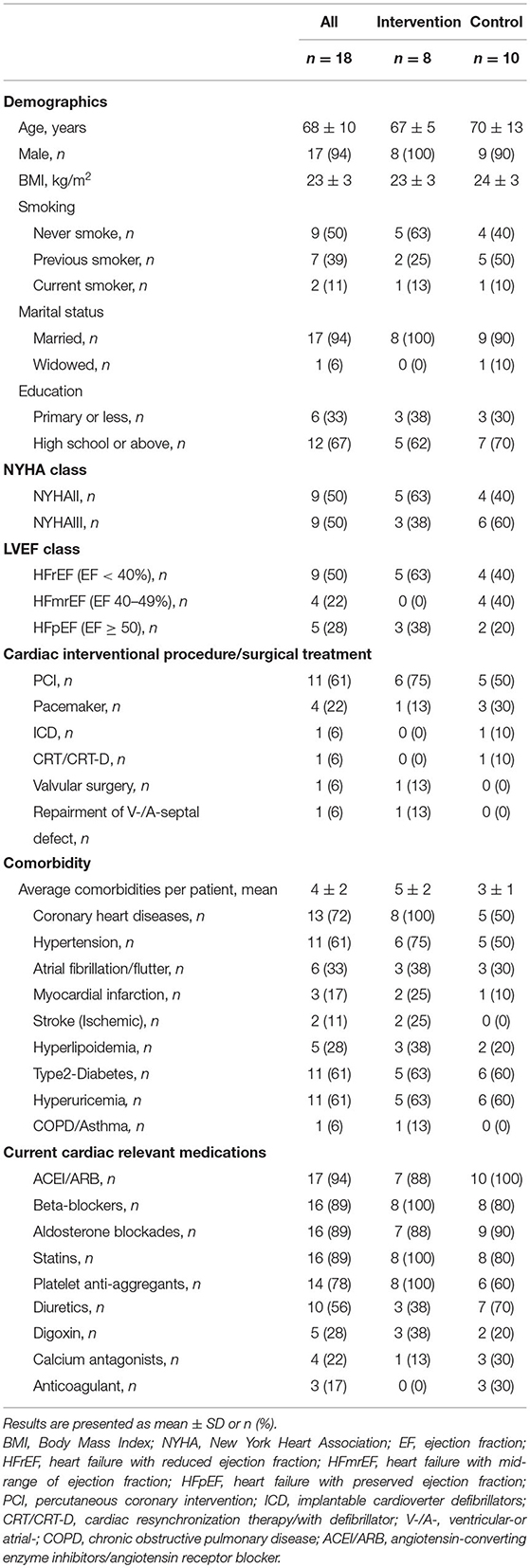
Table 1. Baseline characteristics of 18 participating patients.
High Fidelity to Intervention
Participants involved in the BESMILE-HF program regarding the self-reported home exercise and attendant rates in other scheduled sessions are shown in Figure 3. Our results showed that the BESMILE-HF program was feasible with relatively high adherence. As a home-based EBCR program, the intervention group demonstrated good compliance with the required exercises. On average, participants exercised 27.5 (SD: 11.4) minutes/day and 5.6 (SD: 2.6) days/week for 6 weeks, reaching both the general required daily exercise time (30 min/day) and exercise frequency (5 days/week), respectively (Figure 3). Moreover, the total home-practice times (mins) had a significant positive relationship with their baseline self-efficacy scores (r = 0.831, p = 0.011).
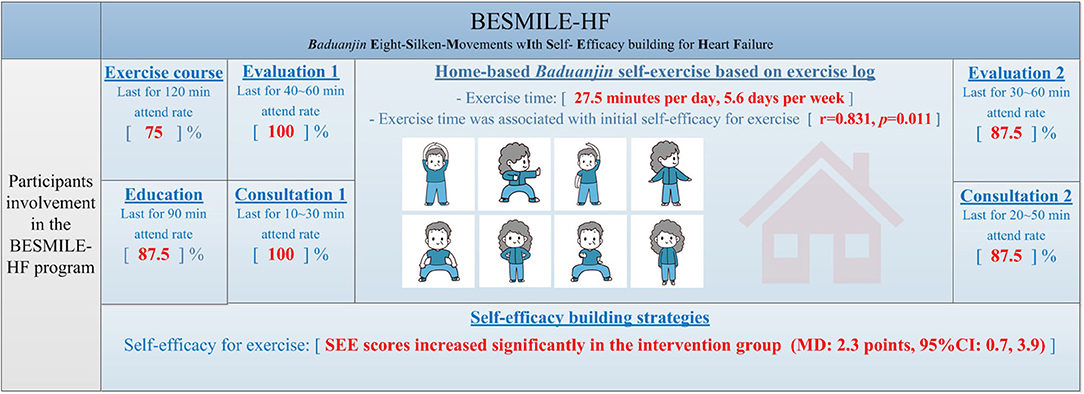
Figure 3. Participants involvement in the BESMILE-HF program (n = 8). Participants' involvement in the BESMILE-HF program regarding the self-report home exercise and attendant rates in other scheduled sessions are shown in red. The intervention group had done the required home exercises and total home-practice time was significantly related to baseline self-efficacy. SEE, Self-efficacy for exercise; MD, mean difference.
In terms of other part of the BESMILE-HF program, all patients participated in the Baduanjin course which lasted for about 120 minutes and their performances were confirmed by the professional coach, except for 2 patients who preferred to learn the exercise via the video (attendance rate: 75%). All patients took the education course at baseline and at 6th week except one patient (overall attendance rate: 87.5%). All patients underwent baseline evaluation-session which included the collection of general assessments as well as individual cardiorespiratory data of Baduanjin exercise performance, except for two patients had only the general assessment data. All patients participated to the baseline consultation-session which mainly includes development of exercise prescription. For the closure evaluation- and consultation- sessions, all patients participated except one who died within 6-week (attendance rate: 87.5% for both sessions).
Effects of the BESMILE-HF Program
In terms of the exercise capacity, the control group demonstrated a significant decline in VO2peak (MD: −2.6, 95% CI −4.3 to −0.9), whereas, the BESMILE-HF group maintained their exercise capacity (MD: −1.2, 95% CI −1.2 to 0). Although the between-group difference was not statistically significance, there was a clear clinical improvement in the BESMILE-HF group (1.5 mL/kg/min, 95% CI: −0.3 to 3.2 vs. minimal clinically important difference of 1 mL/kg/min; Table 2.1).
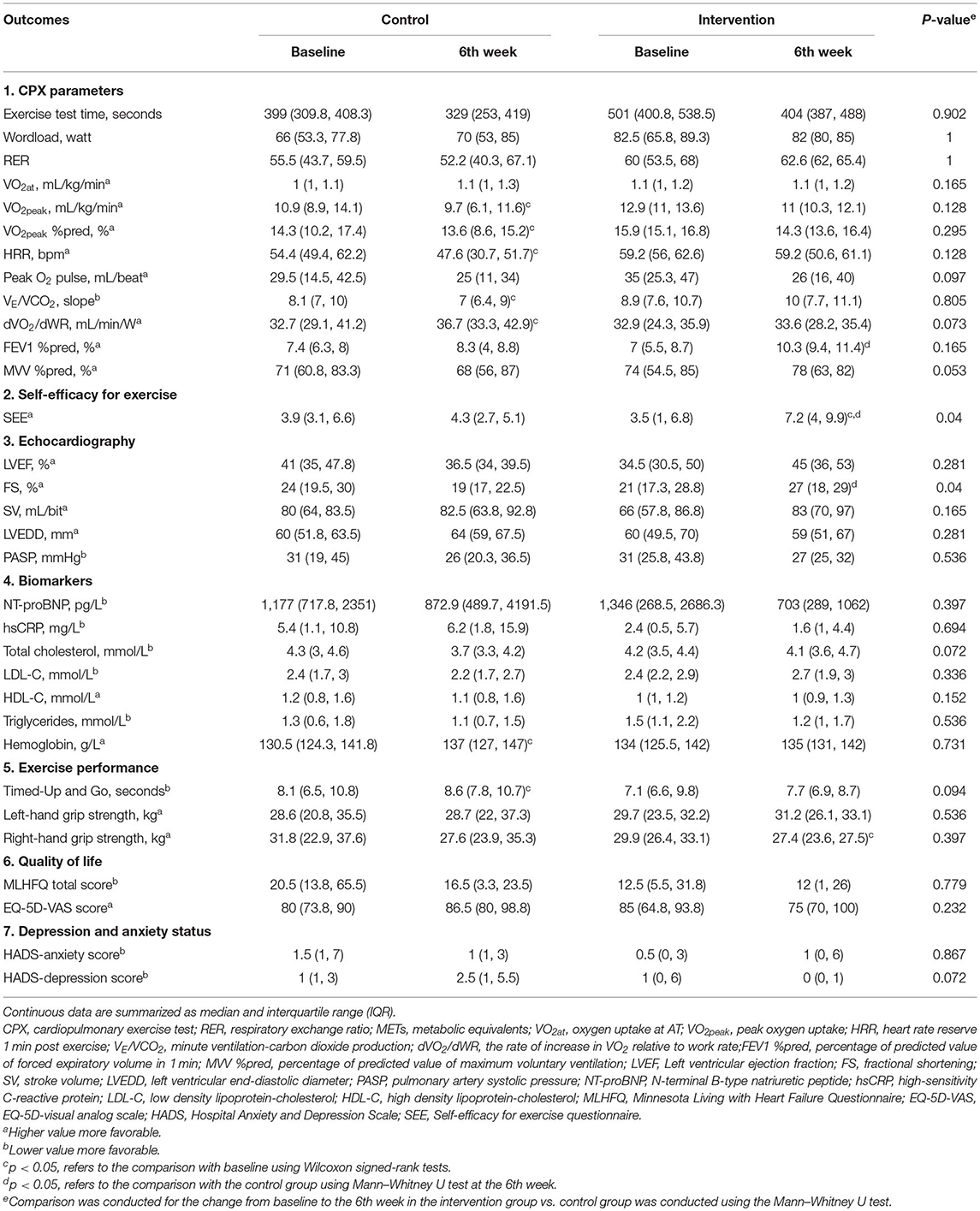
Table 2. Clinical outcomes in each group and between-group comparison (n = 18).
After 6 weeks, SEE scores improved significantly in the BESMILE-HF group [mean difference (MD): 2.3, 95% confidence interval (CI) 0.7–3.9, p = 0.014; Table 2.2], but decreased slightly in the control group (MD: −0.9, 95% CI −3.2 to 1.4, p = 0.377; Table 2.2). When comparing the score changes between the two groups, a significant difference was found (MD: 3.2; 95% CI 0.6–5.9, p = 0.004).
For other clinical outcomes, no significant differences between groups, for either post-intervention values or changes, were observed for: most of the echocardiography parameters (Table 2.3); biomarkers such as NT-proBNP and hsCRP (Table 2.4); balance/mobility as measured by Timed up-and-go test (Table 2.5); quality of life (Table 2.6), or status of depression/anxiety (Table 2.7).
Safety of the BESMILE-HF Program
Throughout the pilot RCT, no adverse events related to the intervention were captured. However, we documented several MACEs during the study period, one patient in the BESMILE-HF group died due to heart failure exacerbation, and two patients from the control group experienced acute heart failure exacerbation resulting in hospitalization.
Discussion
The findings of this pilot study support the feasibility of the contextually adapted BESMILE-HF program using traditional Baduanjin exercise for patients with CHF in China. The BESMILE-HF program was well-received by patients. As a home-based EBCR program, the intervention group demonstrated exceptional compliance with the required exercises. We also found that one's initial self-efficacy had a positive effect on the total exercise time. More importantly, intervention can improve participants' exercise self-efficacy and may have benefit on exercise capacity.
The BESMILE-HF program's feasibility is primarily attributed to its in-home nature and the use of traditional Baduanjin exercise. According to a recent consensus statement on EBCR delivery in low-resource settings, safe, equipment-free, low-cost, and easy-to-implement exercise modalities provide the most practical options for Chinese settings (16). Compared to other low-cost outdoor activities such as walking, biking, running, and swimming, a home-based modality might be a more attractive and sensible option for optimal EBCR flexibility, given the fact that one-third of Chinese HF patients had difficulty or were unable to leave their homes due to their symptoms (17). In addition, Baduanjin exercise is an adaptable form of exercise that can be practiced in any place, and at any time. It also requires no special equipment and is not time-consuming. Hence, it is easy to be incorporated into daily routines.
Generally, adherence to exercise programs is low among CHF patients, which may limit its effect on clinical outcomes (18). In practice, self-efficacy plays a crucial role in adherence (19). In this study, a statistically significant positive relationship was found between baseline self-efficacy scores and individual exercise time. This result is supported by emerging literature in which self-efficacy is reported as the dominant factor in exercise uptake and maintenance among the CHF population (20). Therefore, it is reasonable to assume that the BESMILE-HF program might increase participants' adherence and maintenance of exercise compliance over time.
It is important to highlight that there was a significant improvement in self-efficacy score in the intervention group, but not in the control group. The between-group difference was found to be statistically significant, even within the context of this pilot study. However, the lack of periodic contact with doctors or nurses in the control group could have resulted in bias since the frequent contact with rehabilitation staff may explain some of the improvement in the intervention group. Nevertheless, a recent RCT reported that the 16-week Baduanjin training could improve self-efficacy for managing chronic diseases in community-living adults, such as increased confidence to mitigate fatigue, physical discomfort/pain, and emotional distress, and to be able to accomplish various tasks and activities (21). Our results also dovetail with previous evidence which shows that Tai Chi, a similar style of exercise, can improve CHF patients' self-efficacy (22).
Self-efficacy is defined as “the perceived confidence in the ability to take successful action and perform a specific task.” It is centered on four core elements: “role modeling,” “positive feedback,” “performance accomplishment,” and “recognition of problems and problem-solving” (23). In the BESMILE-HF program, specific adherence strategies for each of the four elements of self-efficacy were adopted and delivered as adjuncts to the Baduanjin exercise. Examples include an exercise course with an initial demonstration of exercise techniques by a coach and a graphic exercise brochure (role modeling); an evaluation session with feedback on Baduanjin performance and a weekly phone-call follow-up to review the progress by cardiac nurses (positive feedback); an exercise log to record individuals' own daily home-exercise (performance accomplishment); an educational course about disease management in daily life (recognition of problems and problem-solving).
The BESMILE-HF program is a complex intervention with several interacting components. This means that there will be a certain number of behaviors required by those delivering or receiving the intervention, as well as difficulties. Moreover, flexibility and tailoring of the intervention was permitted, as ensuring strict fidelity to a protocol may have been inappropriate. Evaluations of clinical outcomes are often undermined by problems such as delivery of the intervention, recruitment and retention, and smaller-than-expected effect sizes (24). Our small sample size was under-powered to reach a statistically significant effect on clinical outcomes such as VO2peak. However, there was a favorable trend with a clinically significant difference between two groups at the week 6 follow-up. In addition, our research team has recently confirmed that Baduanjin training intensity fulfilled ACSM's recommendations for bodily stimulation resulting in physiologically oriented outcomes (25). Moreover, previous studies have reported that Baduanjin improves exercise capacity (26–31). Therefore, the benefits of Baduanjin on exercise capacity should be expected from continued practice. Of note, Baduanjin can also be practiced in a sitting-form. Hece, for those patients with orthopedic limitations or other concomitant illness, the clinicians can also proposed this exercise to their patients to practice at home.
Limitations
As with all studies, there are potential limitations to note. Firstly, the generalizability of the results might be limited by the characteristics of the included patients: NYHA II and III CHF patients who are relatively young and suffer from heart failure of mild-moderate severity. However, we still believe that our main findings described above are mostly applied to other parts of China. This is because the demographic and clinical characteristics of the study participants are similar to the those CHF patients undergoing a cross-sectional survey in Guangzhou (32) and in China as a whole (17). In addition, although we only recruited CHF patients with NYHA classification of II or III, the findings on Baduanjin intensity also apply to CHF patients in general. This is because patients with NYHA classification of II or III account for 83% of the HF patients in the stable stage in this setting (17). Secondly, 94% of the pilot study population was male. Sex has been showed to be an influencing factor in the change of VO2peak and time spent on exercise (18, 33). Additional studies should strive to include an equal distribution of men and women. Thirdly, due to the nature of the intervention, blinding of patients and implementors was impossible. Trials with inadequate blinding are likely to exaggerate treatment effects, especially with regard to subjective results (such as SEE) and with participants with knowledge of traditional Chinese culture (34). However, we have blinded outcome assessors to minimize the detection bias. Fourthly, although the intervention group completed the required home exercises as reported through exercise logs, it should be noted that self-reported practice exercise tends to be overestimated (20). Assessing and ensuring adequate levels of intervention adherence is a challenge in most self-directed home-based interventions. However, self-reported exercise records, because of their ease of use, remain one of the most common tools for recording exercise data (20). Future, full-scale clinical trials should consider use of objective data collection methods to validate self-reported exercise data. Finally, given the scope of the pilot study and limited resources, the sample size was small. Therefore, the pilot RCT was not powered to test efficacy. However, the primary aim of the pilot study is to explore intervention feasibility, such as the recruitment rate, data collection process, and retention rate. Moreover, this small size study can still provide us some information regarding the preliminary efficacy of this intervention, as there is no data available regarding the BESMILE-HF program.
Conclusion
This pilot study indicates that the BESMILE-HF program using traditional Baduanjin exercise, is feasible for patients with CHF in the Chinese setting. This practice may also increase patients' long-term adherence to exercise by improving exercise self-efficacy. Its potential benefits on clinical outcomes need confirmation with a larger sample size and a longer follow-up period. A full-scale RCT has been launched to determine the efficacy and safety of the BESMILE-HF program in patients with CHF.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Ethics Committee at the Guangdong Provincial Hospital of Chinese Medicine (number: B2016–202-01). The patients/participants provided their written informed consent to participate in this study.
Author Contributions
XC, WJ, CL, ZW, WL, and GM contributed to the conception and design of the research. ZW and WL contributed to obtaining funding and supervising the work. XC drafted the first version of the manuscript and revised it based on other authors: WJ, TO, CL, ZW, WL, and GM contribution. All authors contributed important intellectual content to the critical revision of the manuscript and read and approved the final manuscript.
Funding
This work was supported by the General Research Fund of Traditional Chinese Medicine Science and Technology from Guangdong Provincial Hospital of Chinese Medicine (YN2018ML02), the Clinical Research Funding of Traditional Chinese Medicine Science and Technology (Project 1010) from Guangdong Provincial Hospital of Chinese Medicine (YN10101910), and the China Scholarships Council (201608440264).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors wish to thank the professional coach (Haojian Yu) from the GPHCM Department of Cardiology in teaching the exercise; cardiology nurses (Yunxiang Fan) from the GPHCM Department of Cardiology for assistance with conducting the education-/evaluation-/consultation-sessions and collecting data; as well as research assistants from the GPHCM for assistance with collecting data. Results of the upload manuscript were partially presented as an abstract at the 23rd Annual Scientific Meeting of the Heart-Failure-Society-of-America (HFSA) and the American Association of Cardiovascular and Pulmonary Rehabilitation 34th Annual Meeting. Some parts of the results of the upload manuscript were included the doctoral thesis of XC and have been appeared online.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2021.715207/full#supplementary-material
Abbreviations
BESMILE-HF, Baduanjin Eight-Silken-Movement wIth SeLf-Efficacy building for Heart Failure; CHF, Chronic heart failure; CI, Confidence interval; EBCR, Exercise-based cardiac rehabilitation; GPHCM, Guangdong Provincial Hospital of Chinese Medicine; hsCRP, High sensity C-reactive protein; LVEF, Left ventricular ejection fraction; MACEs, Major adverse cardiac events; MD, Mean difference; MLHFQ, Minnesota Living with Heart Failure Questionnaire; NT-proBNP, N-terminal B-type natriuretic peptide; NYHA, New York Heart Association functional; RCT, Randomized controlled trial; SD, Standard deviation; SEE, Self-Efficacy for Exercise; VO2peak, Peak oxygen consumption.
References
1. Fleg JL, Cooper LS, Borlaug BA, Haykowsky MJ, Kraus WE, Levine BD, et al. Exercise training as therapy for heart failure: current status and future directions. Circ Heart Fail. (2015) 8:209–20. doi: 10.1161/CIRCHEARTFAILURE.113.001420
2. Taylor RS, Sagar VA, Davies EJ, Briscoe S, Coats AJ, Dalal H, et al. Exercise-based rehabilitation for heart failure. Cochrane Database Syst Rev. (2014) 2014:CD003331. doi: 10.1002/14651858.CD003331.pub4
3. Turk-Adawi K, Sarrafzadegan N, Grace SL. Global availability of cardiac rehabilitation. Nat Rev Cardiol. (2014) 11:586–96. doi: 10.1038/nrcardio.2014.98
4. Sun XG. Rehabilitation practice patterns for patients with heart failure: the Asian perspective. Heart Fail Clin. (2015) 11:95–104. doi: 10.1016/j.hfc.2014.09.001
5. Zhang Z, Pack Q, Squires RW, Lopez-Jimenez F, Yu L, Thomas RJ. Availability and characteristics of cardiac rehabilitation programmes in China. Heart Asia. (2016) 8:9–12. doi: 10.1136/heartasia-2016-010758
6. Zwisler AD, Norton RJ, Dean SG, Dalal H, Tang LH, Wingham J, et al. Home-based cardiac rehabilitation for people with heart failure: a systematic review and meta-analysis. Int J Cardiol. (2016) 221:963–9. doi: 10.1016/j.ijcard.2016.06.207
7. David R. Thompson, Yu C-M. Cardiac Rehabilitation: China. In: Joep P, Helmut G, Irene H, Philippe S, Peter M, Catherine M, et al., edtiors. Cardiovascular Prevention and Rehabilitation. London: Springer (2007).
8. Koh TC. Baduanjin – an ancient Chinese exercise. Am J Chin Med. (1982) 10:14–21. doi: 10.1142/S0192415X8200004X
9. Wang N, Guo Y. Traditional Chinese practice, a promising integrative intervention for chronic non-infectious disease management. Chin J Integr Med. (2018) 24:886–90. doi: 10.1007/s11655-018-2572-7
10. Chen X, Jiang W, Lin X, Lundborg CS, Wen Z, Lu W, et al. Effect of an exercise-based cardiac rehabilitation program “Baduanjin Eight-Silken-Movements with self-efficacy building” for heart failure (BESMILE-HF study): study protocol for a randomized controlled trial. Trials. (2018) 19:150. doi: 10.1186/s13063-018-2531-9
11. Eldridge SM, Chan CL, Campbell MJ, Bond CM, Hopewell S, Thabane L, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. (2016) 355:i5239. doi: 10.1136/bmj.i5239
12. 2015 Population Scope and Distribution in Guangzhou Population Department of Guangzhou Statistics Bureau. (2015). Available online at: www.gzstats.gov.cn (accessed November 11, 2016).
13. Baduanjin Exercises [YouTube]. Available online at: https://www.youtube.com/watch?v=i2YY6t1JhCY&list=PLPCWVScVb76hNWtgDyXyiI9tz4977_6N6 (accessed June 29, 2020).
14. Baduanjin Exercise (Tutorial) [YouTube]. Available online at: https://www.youtube.com/watch?v=UculAU8mWd8 (accessed June 29, 2020).
15. Chinese Society of Cardiology of Chinese Medical Association EBoCJoC. The Chinese guidelines for diagnosis and treatmen for heart failure 2018. Chin J Cardio. (2018) 46:760–89. doi: 10.3760/cma.j.issn.0253-3758.2018.10.004
16. Grace SL, Turk-Adawi KI, Contractor A, Atrey A, Campbell N, Derman W, et al. Cardiac rehabilitation delivery model for low-resource settings. Heart. (2016) 102:1449–55. doi: 10.1136/heartjnl-2015-309209
17. Jackson JD, Cotton SE, Bruce Wirta S, Proenca CC, Zhang M, Lahoz R, et al. Burden of heart failure on patients from China: results from a cross-sectional survey. Drug Des Dev Ther. (2018) 12:1659–68. doi: 10.2147/DDDT.S148949
18. Barbour KA, Miller NH. Adherence to exercise training in heart failure: a review. Heart Fail Rev. (2008) 13:81–9. doi: 10.1007/s10741-007-9054-x
19. Rajati F, Sadeghi M, Feizi A, Sharifirad G, Hasandokht T, Mostafavi F. Self-efficacy strategies to improve exercise in patients with heart failure: a systematic review. ARYA Atherosclerosis. (2014) 10:319–33.
20. Deka P, Pozehl B, Williams MA, Yates B. Adherence to recommended exercise guidelines in patients with heart failure. Heart Fail Rev. (2017) 22:41–53. doi: 10.1007/s10741-016-9584-1
21. Xiao X, Wang J, Gu Y, Cai Y, Ma L. Effect of community based practice of Baduanjin on self-efficacy of adults with cardiovascular diseases. PLoS ONE. (2018) 13:e0200246. doi: 10.1371/journal.pone.0200246
22. Yeh GY, McCarthy EP, Wayne PM, Stevenson LW, Wood MJ, Forman D, et al. Tai chi exercise in patients with chronic heart failure: a randomized clinical trial. Arch Intern Med. (2011) 171:750–7. doi: 10.1001/archinternmed.2011.150
23. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. (1977) 84:191–215. doi: 10.1037/0033-295X.84.2.191
24. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. (2008) 337:a1655. doi: 10.1136/bmj.a1655
25. Chen XK, Marrone G, Olson TP, Lundborg CS, Zhu H, Wen ZH, et al. Intensity level and cardiorespiratory responses to baduanjin exercise in patients with chronic heart failure (forthcoming). ESC Heart Fail. (2020) 7:3782–91. doi: 10.1002/ehf2.12959
26. Xiong X, Xu D. Therapeutic effect of Baduanjin on patients with coronary heart disease and chronic heart failure [in Chinese]. China Modern Med J. (2016) 18:55–6. doi: 10.3969/j.issn.1672-9463.2016.05.016
27. Yang X, Feixiang Huang, Yongchao Shi, Yanxia Wang, Ye L. Effect of aerobics training on exercise tolerance in patients with chronic heart failure [in Chinese]. Chin J Nurs. (2015) 50:193–7. doi: 10.3761/j.issn.0254-1769.2015.02.015
28. Yan X. Effects of Liuzi and Ba Duan Jin training on exercise tolerance in patients with chronic heart failure [in Chinese]. Chin Trad Med Modern Distance Educ. (2016) 14:126–8. doi: 10.3969/j.issn.1672-2779.2016.16.055
29. Jing Y. Effect of TCM aerobics on exercise endurance in patients with chronic heart failure [in Chinese]. Chin Trad Med Modern Distance Educ. (2015) 13:12–4. doi: 10.3969/j.issn.1672-2779.2015.21.006
30. Chen DM, Yu WC, Hung HF, Tsai JC, Wu HY, Chiou AF. The effects of Baduanjin exercise on fatigue and quality of life in patients with heart failure: a randomized controlled trial. Eur J Cardiovasc Nurs. (2017) 17:456–66. doi: 10.1177/1474515117744770
31. Li R. Observation on the improvement of cardiac function and quality of life in elderly patients with chronic heart failure by Ba Duan Jin [in Chinese]. Massage Rehabil Med. (2017) 8:23–5. doi: 10.3969/j.issn.1008-1879.2017.24.009
32. Lai SW. The Investigation of the Current Status of the Use of Traditional Chinese Medicine (TCM) Exercise Regimen in Patients With Chronic Heart Failure (PhD). Guangzhou University of Traditional Chinese Medicine (2014).
33. Tierney S, Mamas M, Woods S, Rutter MK, Gibson M, Neyses L, et al. What strategies are effective for exercise adherence in heart failure? A systematic review of controlled studies. Heart Fail Rev. (2012) 17:107–15. doi: 10.1007/s10741-011-9252-4
Keywords: exercise-based cardiac rehabilitation, chronic heart failure, pilot randomized controlled trial, self-efficacy for exercise, Baduanjin exercise
Citation: Chen X, Jiang W, Olson TP, Lundborg CS, Wen Z, Lu W and Marrone G (2021) Feasibility and Preliminary Effects of the BESMILE-HF Program on Chronic Heart Failure Patients: A Pilot Randomized Controlled Trial. Front. Cardiovasc. Med. 8:715207. doi: 10.3389/fcvm.2021.715207
Received: 26 May 2021; Accepted: 05 July 2021;
Published: 27 July 2021.
Edited by:
Jian Yang, Fudan University, ChinaReviewed by:
Jianqing She, The First Affiliated Hospital of Xi'an Jiaotong University, ChinaFerdinando Iellamo, University of Rome Tor Vergata, Italy
Copyright © 2021 Chen, Jiang, Olson, Lundborg, Wen, Lu and Marrone. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Weihui Lu, d2VpaHVpLmx1QDE2My5jb20=; Zehuai Wen, d2VuemhAZ3p1Y20uZWR1LmNu