 Youmeng Wang
Youmeng Wang Roberto Fernandes Branco1†
Roberto Fernandes Branco1† Thomas Penzel
Thomas Penzel Christoph Schöbel
Christoph Schöbel- 1Sleep Medicine Center, Charité-Universitätsmedizin, Berlin, Germany
- 2Universitätsmedizin Essen, Ruhrlandklinik—Westdeutsches Lungenzentrum am Universitätsklinikum Essen GmbH, Essen, Germany
Transcatheter caval valve implantation (CAVI) has been evaluated as a treatment option for inoperable patients with severe symptomatic tricuspid regurgitation (TR). We studied the effect of CAVI on sleep disorder breathing (SDB) in patients with right heart failure and TR. Twenty right heart failure patients with severe symptomatic TR who underwent portable monitoring of SDB (ApneaLink), echocardiography, cardiopulmonary exercise (CPET), and laboratory testing were enrolled. This was a single-center, nonblinded study. There were no significant changes in sleep variables, echocardiographic parameters, laboratory results, lung function, and CPET after CAVI. In conclusion, these data suggest that CAVI may not have an effect on SDB; however, additional follow-up fully powered studies with appropriate statistical analyses are needed.
Introduction
Chronic heart failure (CHF) is an increasing health problem affecting more than 25 million people worldwide. The prevalence of heart failure in developed countries is about 1–2% in general and over 10% in patients above 70 years (1). Despite improvement in treatment, the prognosis of CHF is still poor, and more than 50% of hospitalized patients with CHF die within 5 years. Patients with CHF commonly suffer from breathing disorders during sleep (2, 3). Sleep disorder breathing (SDB) is a highly prevalent comorbidity in CHF patients, which has adverse effects on the prognosis of CHF. The presence of breathing disorders during sleep in patients with CHF is associated with increased risk of cardiovascular disease and mortality (4, 5). There are two different types of SDB in patients with HF: obstructive sleep apnea (OSA) and central sleep apnea (CSA) (6, 7).
Severe tricuspid regurgitation (TR) is a complex condition of the right ventricle (RV) and tricuspid valve apparatus and is frequently associated with symptomatic heart failure (8). The etiology of TR can be divided into primary and secondary causes. Primary TR may be caused by congenital, traumatic, rheumatic, and endomyocardial fibrosis. In these patients, left heart diseases could lead to chronic pressure overload of the RV, which eventually resulted in progressive RV expansion and functional TR. In patients with severe TR, medical therapy restricted to diuretics and heart failure medication is frequently infective, and surgical repair is associated with a high risk of morbidity and mortality (9, 10). In addition, neither one of these treatment options has demonstrated beneficial long-term effects. Therefore, multiple innovative interventional treatment concepts to replace or repair tricuspid valve function are currently under investigation.
CAVI has been suggested as one of these interventional concepts. In the pathological cascade of tricuspid valve disease, CAVI aims at the caval backflow that occurs at a late stage of severe TR (11). One previous study showed a decrease in the apnea–hypopnea index (AHI) after heart transplantation and medical treatment in a population of CSA patients with congestive heart failure group (n = 13) (12). Another study showed that one 64-year-old male patient with CSA improved his sleep, daytime hypersommolence, dyspnea, and fatigue after mitral valve transplantation (13). There has only been one randomized controlled trial that showed that transcatheter aortic valve replacement in patients with CHF and TR did not show positive effects on SDB (8, 10). The aim of our study was to examine whether CAVI has an effect on SDB in patients with right heart failure and TR.
Materials and Methods
Study Design and Collection of Data
Our investigation was added on top of a previous study (11). This was a single-center, nonblinded study. Between January 2015 and November 2019, 29 consecutive right heart failure patients with severe symptomatic TR were divided into the CAVI group (n = 14) and the control group (n = 15), treated with optimal medical therapy (OMT) alone. The CAVI procedures were successful in all patients. An indicator of success was that CAVI resulted in the full reduction of reverse caval flow as confirmed by a significant reduction in the inferior vena cava (IVC) v-wave in all patients; this is already known in a previous study (9). Four major complications in the CAVI group that occurred within 48 h after implantation and resulted in open-heart surgery (two cases of cardiac tamponade secondary to stent migration and two valve dislocations) were excluded. After the fourth major complication, recruitment was stopped for safety. Five patients in the control group did not receive portable monitoring results and were excluded from this study. Patients with severe symptomatic TR were screened for SDB using a three-channel screening system (ApneaLink, Resmed). Data were collected at baseline and at 1-month follow-up from medical records. Portable monitoring was performed in 20 patients for SDB assessment. To diagnose SDB, AHI had to be 10/h or above. According to the value of the AHI, we divided the patients into four groups: control-SDB (n = 8), CAVI-SDB (n = 3), CAVI-no-SDB (n = 7), and control-no-SDB (n = 2) (Figure 1). All patients provided informed consent, and treatment was performed after the approval of the local ethics committee (Landesamt fur Gesundheit und Soziales Berlin, Germany).
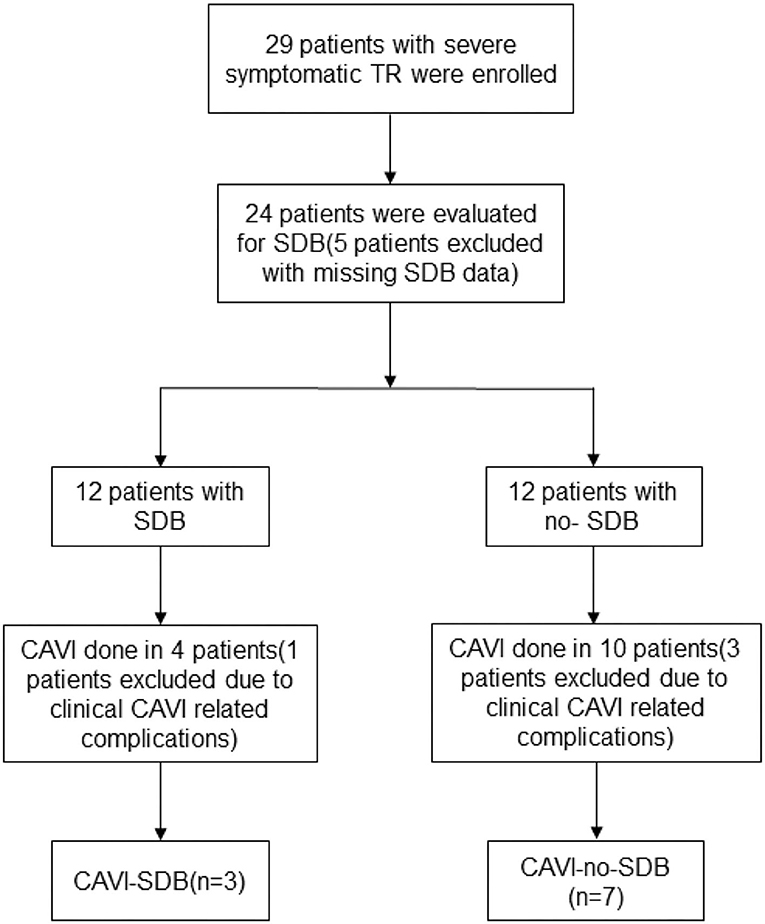
Figure 1. Patient selection and flow.
Patient Screening and Follow-Up
The inclusion criteria were the same as those defined by a previous study (11): (1) TR severity ≥ severe; (2) New York Heart Association (NYHA) functional class II or greater despite the established OMT; (3) age ≥ 50 years; and (4) high surgical risk. This study required that cardiac surgeons, interventional and non-interventional cardiologists, anesthesiologists, and imaging experts completed the evaluation and acceptance of CAVI patients. Routine preoperative examinations include transthoracic echocardiography, cardiopulmonary exercise, and laboratory examinations.
Exclusion criteria were as follows: (1) IVC diameter > 31 mm; (2) ongoing treatment of SDB; (3) inability to undergo portable monitoring; (4) serum creatinine concentration > 3.0 mg/dl; (5) patients for whom informed consent cannot be obtained; (6) chronic kidney disease undergoing regular dialysis; and (7) left ventricular ejection fraction < 30%. We offered CAVI to all severe symptomatic TR patients with SDB who met the inclusion criteria (11).
Portable Monitoring
ApneaLink (Resmed) is a three-channel, portable device that uses a nasal pressure transducer to derive the AHI, flow limitation, and snoring, in addition to monitoring oxygen saturation during sleep. The oxygen desaturation index (ODI) was measured with the AL during the simultaneous study. The AL device operates on battery power, with a sampling rate of 100 Hz, and has a 16-bit signal processor. The internal memory storage is 15 MB, which allows ~10 h of data collection. The software analyzes the data generated by the flow signal, whereas full disclosure of data is available for review and rescoring by the clinician. AHI ≥ 10/h was defined as SDB in this study.
CAVI Procedure
All implantations were performed through transfemoral venous access under local anesthesia and transthoracic echocardiography. After preparing the landing area by implanting a self-expanding stent (Sinus-XL, Optimed, Ettlingen, Germany) to facilitate valve fixation, the Sapien XT transcatheter valve (Edwards Lifesciences, Irvine, CA) was implanted in the IVC at the level of the diaphragm and protruding ≈5 mm into the right atrium (RA) (11).
Laboratory Testing and Echocardiography
Blood sample collection: a nurse collected 2 ml venous blood, injected it into an anticoagulation tube, and fully blended it for later use. A biochemical auto-analyzer was applied to examine the eGFR. All patients underwent our standard 2-D and 3-D transthoracic and transesophageal echocardiography. Echocardiographic parameters included LVEF, RV-FAC, TAPSE, and the tissue Doppler E/E′ ratio. All recordings were performed on ultrasound systems.
Lung Function and Cardiopulmonary Exercise Testing
Spirometry (FEV1, FVC; FEV1/FVC ratio), measurement of static lung volumes (total lung capacity (TLC) by body box plethysmography), and measurement of diffusing capacity of the lung for carbon monoxide (DLCO) by the single-breath technique were performed (Vmax22, SensorMedics, Yorba Linda, CA, USA) with the patient in the seated position. Testing protocols adhered to guidelines for calibration and testing recommended by the ATS/ERS standards. All patients performed a symptom-limited CPET by using a cycle ergometer protocol, which is cycling with a pedal speed of 60 rpm, starting at a workload of 20 W, followed by a stepwise 20-W increment every 2 min until exhaustion. AT was identified through a V-slope analysis of VO2 and CO2 production (VCO2), and it was confirmed through the specific behavior of the ventilatory equivalents of O2 (VE/VO2) and CO2 (VE/VCO2), as well as through the end-tidal O2 and CO2 pressure. The relation between VE and VCO2 was analyzed as the slope (VE/VCO2 slope).
Statistical Analysis
Descriptive statistics (means and standard deviations) were used to describe baseline characteristics. Categorical variables are expressed as numbers (n) and percentages (%). Our data follow a normal distribution and were analyzed using a paired t-test and independent sample t-test for within-group and between-group comparisons, respectively. A value of p < 0.05 means statistically significant. All statistical data were performed using SPSS version 25.0 (IBM, Armonk, NY, USA).
Results
The general characteristics of the participants at baseline are presented in Table 1. No significant differences in sex, age, body mass index (BMI), ejection fraction, NYHA functional class, and medications were observed between groups. All patients were taking loop diuretics, and they all had severe symptomatic TR. There were no changes in medication during the study.
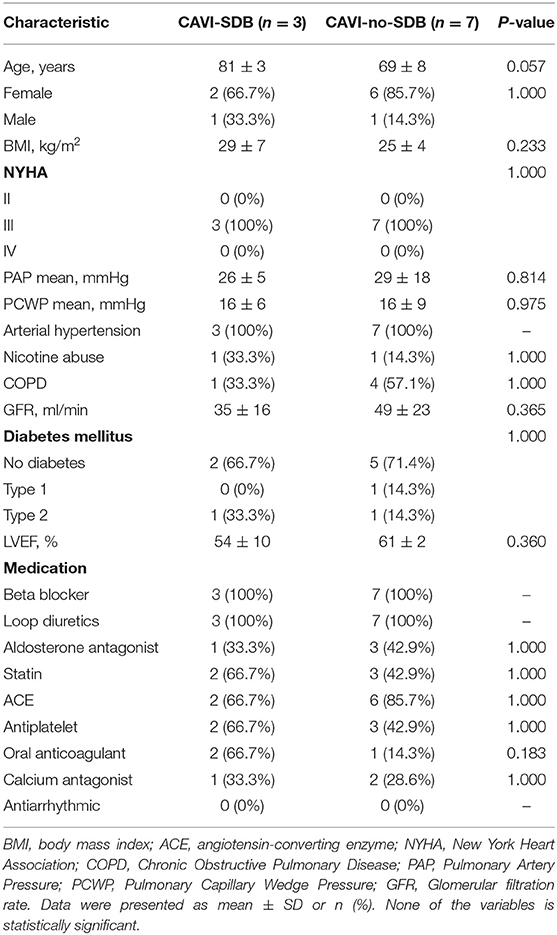
Table 1. Baseline clinical data comparisons.
Comparisons between CAVI -SDB and CAVI-no-SDB groups are displayed in Table 2. There were no significant changes of all parameters before and after treatment in both groups (p > 0.05). By design, significant differences of tissue Doppler E/E, FVC % pred, FEV1, and FEV1 % pred were observed before the treatment between groups (p < 0.05). There were significant differences of LVEF, RVFAC, AHI, and ODI after the treatment between groups (p < 0.05).
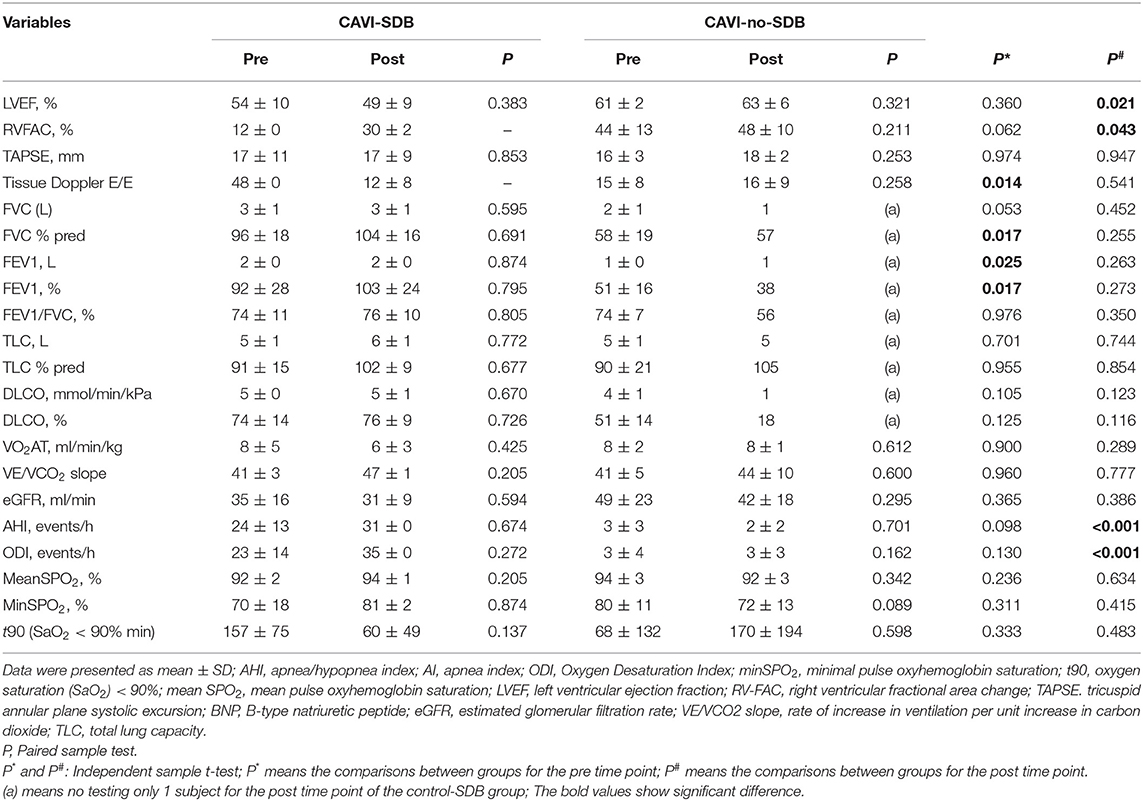
Table 2. Comparisons between CAVI-SDB and CAVI-no-SDB group.
Discussion
To the best of our knowledge, this is the first time to investigate the effect of CAVI on SDB in patients with right heart failure and severe symptomatic TR. The main finding from this investigation showed that CAVI had no obvious effect on SDB in patients with HF and TR.
Previous studies have indicated that SDB is associated with postoperative complications after general and cardiac surgery (14–16). In another study, they found SDB to be associated with a higher rate of long-term cardiovascular events after coronary artery bypass grafting (17). A study found that SDB is highly prevalent in patients undergoing cardiovascular surgery. However, in this population, the authors did not find an association between SDB and adverse postoperative outcomes due to a relatively small sample size (107 patients) (18). In our study, we also did not find any association between SDB and adverse outcome after CAVI.
SDB is known to be associated with heart disease, e.g., heart failure, coronary artery disease, and atrial fibrillation (19), but less is known about its prevalence in valve diseases. Past studies indicated a high prevalence of SDB in patients with severe aortic stenosis. Printz et al. (20) reported SDB in 15 out of 42 individuals (36%) with high-grade aortic stenosis. In our study cohort of patients with severe symptomatic tricuspid regurgitation before CAVI, the prevalence of SDB was as high as 50%. Although the total number of subjects is very small, these findings should increase the awareness of existence of SDB in patients with severe symptomatic tricuspid regurgitation.
The relation of subclinical lung function impairment with cardiovascular diseases in the absence of diagnosed pulmonary diseases has recently drawn more attention. In a cohort with long-term follow-up, low FEV1 was strongly and independently associated with incident CHF (21). A population-based study of middle-aged men observed the association between moderately reduced FEV1 and FVC and incident heart failure hospitalization (22). In our population based on relatively older subjects and limited patients sample, we demonstrated that there were no significant differences between FEV1, FEV1/FVC, and TLC after CAVI (p > 0.05; Table 2).
A previous study showed that an increasing VE/VCO2 slope was a potential negative sign (23). As presented in Table 2, the VE/VCO2 slope showed no obvious changes post-CAVI probably due to our very small sample size. The past study showed that the VE/VCO2 slope was insignificantly correlated with the AHI, and patients with CHF-SDB have hyperpnea not only during sleep but also during exercise (24). However, the correlation coefficient between the VE/VCO2 slope and the AHI was less than between chemosensitivity and the AHI. Chemosensitivity could not be observed, and it was speculated that the steeper VE/VCO2 slope was caused by augmented chemosensitivity (25). The VE/VCO2 slope of CHF-SDB patients increases due to increased abnormal ventilation and perfusion and physiological lung dead space.
In a mixed sample of patients with HF and mitral or aortic valve disease, they showed an improvement of SDB after heart valve surgery (26). The CAVI procedure is a recently developed method of valve replacement for use in patients with severe tricuspid regurgitation, who cannot undergo surgery or who have a high perioperative risk (27). There were no significant differences for sleep variables between pre- and post-CAVI. This could not support that SDB is another manifestation of cardiac dysfunction. Additionally, the risk for four patients experiencing severe clinical issues after CAVI in our study was 28%. Although, to date, only limited clinical data are available regarding the efficacy of transcatheter tricuspid valve intervention (TTVI), feasibility has been shown with different techniques, including annuloplasty devices (28–30) and leaflet and coaptation devices (31, 32), both in the heterotopic (CAVI; to reduce the backflow in the venous system) and the orthotopic positions. Despite the increased risk of the patients, the current report confirms the safety and feasibility of TTVI: intraprocedural mortality was 0%, 30-day mortality and periprocedural adverse events did not change, and procedural success improved significantly, from 62 to 72.8%. Clinical experience started in 2011, when CAVI was first reported for compassionate treatment of patients with severe TR using investigational self-expandable valves. Since then, compassionate clinical use has confirmed the technical feasibility of CAVI (33). Improved procedural success is likely multifactorial and related to the following: the early learning curve effect in CAVI, which is common and universal for new devices and techniques; a better understanding of TV anatomy and disease pathophysiology; and improved and more standardized intraprocedural guidance (34).
A previous study suggested that perioperative continuous positive airway pressure (CPAP) treatment could improve the AHI. Effective treatment of SDB can alleviate diastolic dysfunction (35). Whereas SDB did not improve significantly after CAVI, in this small patient cohort, we were unable to demonstrate a direct correlation between SDB improvement and CAVI procedure. The pathogenesis of SDB in HF is complex and remains to be incompletely understood. It is unclear whether SDB directly affects chronic HF pathophysiology. Therefore, the causal link to the prognosis of HF is not clear. Possibly SDB is rather an index for the severity of HF. Further studies with larger sample sizes and with pre- and post-operative evaluations are necessary.
Study Limitations
There are many limitations of the current pilot study that need to be addressed. Our study was nonblinded and conducted about 30 days after the intervention. This is a fairly short interval for the patients to adapt to the new hemodynamic condition. Therefore, it is recommended to repeat a double-blinded study with longer periods for follow-up. The individual differences of the participants, such as their gender, age, and psychological condition, might also influence the pattern and quality of sleep. Moreover, our results are based on single-night portable monitoring; therefore, internight variations remain to be unaccounted for. Finally, this study was stopped early because of a major complication after CAVI, carried out in a single center and on a small sample of elderly people. Multicenter studies with large sample sizes are needed for improving outcomes.
Conclusion
In summary, these data suggest that CAVI may not have an effect on SDB; however, additional follow-up fully powered studies with appropriate statistical analyses are needed.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Ethics Statement
The studies involving human participants were reviewed and approved by Landesamt fur Gesundheit und Soziales Berlin, Germany. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
YW, RB, and RF contributed to the data collection and analysis. CS planed the study, is the guarantor of the manuscript, and assumes responsibility for the integrity of the data. TP contributed to coordinating this project. All authors contributed to drafting or revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
YW was financially supported by the China Scholarship Council (CSC) for her MD study in Sleep Medicine Center, Charité Universitätsmedizin. The CSC had no role in the design or conduct of this research.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We also thank Dr. rer. nat. Rui Zhang (Interdisciplinary Center for Transfer-oriented Research in Natural Sciences, Martin-Luther University Halle-Wittenberg, Germany) for the help in editing the formation of this manuscript.
References
1. Mosterd A, Hoes AW. (2007). Clinical epidemiology of heart failure. Heart. 93, 1137–46. doi: 10.1136/hrt.2003.025270
2. Peppard PE, Young T, Barnet JH, Palta M, Hagen EW, Hla KM. Increased prevalence of sleep-disordered breathing in adults. Am J Epidemiol. (2013) 177:1006–14. doi: 10.1093/aje/kws342
3. Sánchez-De-La-Torre M, Campos-Rodriguez F, Barbé F. Obstructive sleep apnoea and cardiovascular disease. Lancet Respir Med. (2013) 1:61–72. doi: 10.1016/S2213-2600(12)70051-6
4. Farrell PC, Richards G. Recognition and treatment of sleep-disordered breathing: an important component of chronic disease management. J Transl Med. (2017) 15:114. doi: 10.1186/s12967-017-1211-y
5. Vazir A, Sundaram V. Management of sleep apnea in heart failure. Heart Fail Clin. (2018) 14:635–42. doi: 10.1016/j.hfc.2018.06.008
6. Yoshihisa A, Suzuki S, Yamauchi H, Sato T, Oikawa M, Kobayashi A, et al. Beneficial effects of positive airway pressure therapy for sleep-disordered breathing in heart failure patients with preserved left ventricular ejection fraction. Clin Cardiol. (2015) 38:413–21. doi: 10.1002/clc.22412
7. Orr JE, Malhotra A, Sands SA. Pathogenesis of central and complex sleep apnoea. Respirology. (2017) 22:43–52. doi: 10.1111/resp.12927
8. Takagi H, Hari Y, Kawai N, Ando T, Group A. Impact of concurrent tricuspid regurgitation on mortality after transcatheter aortic-valve implantation. Catheter Cardiovasc Interv. (2019) 93:946–53. doi: 10.1002/ccd.27948
9. Lauten A, Dreger H, Schofer J, Grube E, Beckhoff F, Jakob P, et al. Caval valve implantation for treatment of severe tricuspid regurgitation. J Am Coll Cardiol. (2018) 71:1183–4. doi: 10.1016/j.jacc.2017.12.056
10. Fan J, Liu X, Yu L, Sun Y, Jaiswal S, Zhu Q, et al. Impact of tricuspid regurgitation and right ventricular dysfunction on outcomes after transcatheter aortic valve replacement: a systematic review and meta-analysis. Clin Cardiol. (2019) 42:206–12. doi: 10.1002/clc.23126
11. Laule M, Mattig I, Schobel C, Knebel F, Lauten A, Lembcke A, et al. Inferior caval valve implantation versus optimal medical therapy for severe tricuspid regurgitation. J Am Coll Cardiol. (2019) 74:473–5. doi: 10.1016/j.jacc.2019.05.019
12. Mansfield DR, Solin P, Roebuck T, Bergin P, Kaye DM, Naughton MT. The effect of successful heart transplant treatment of heart failure on central sleep apnea. Chest. (2003) 124:1675–81. doi: 10.1378/chest.124.5.1675
13. Rubin AE, Gottlieb SH, Gold AR, Schwartz AR, Smith PL. Elimination of central sleep apnoea by mitral valvuloplasty: the role of feedback delay in periodic breathing. Thorax. (2004) 59:174–6. doi: 10.1136/thorax.2003.007799
14. Abdelsattar ZM, Hendren S, Wong SL, Campbell DAJr, Ramachandran SK. The impact of untreated obstructive sleep apnea on cardiopulmonary complications in general and vascular surgery: a cohort study. Sleep. (2015) 38:1205–10. doi: 10.5665/sleep.4892
15. Wong JK, Maxwell BG, Kushida CA, Sainani KL, Lobato RL, Woo YJ, et al. Obstructive sleep apnea is an independent predictor of postoperative atrial fibrillation in cardiac surgery. J Cardiothorac Vasc Anesth. (2015) 29:1140–7. doi: 10.1053/j.jvca.2015.03.024
16. De Raaff CA, Bindt DM, De Vries N, Van Wagensveld BA. Positional obstructive sleep apnea in bariatric surgery patients: risk factor for postoperative cardiopulmonary complications? Sleep Breath. (2016) 20:113–9. doi: 10.1007/s11325-015-1192-0
17. Uchôa CHG, Danzi-Soares NJ, Nunes FS, de Souza AAL, Nerbass FB, Pedrosa RP. Impact of OSA on cardiovascular events after coronary artery bypass surgery. Chest. (2015) 147:1352–60. doi: 10.1378/chest.14-2152
18. Foldvary-Schaefer N, Kaw R, Collop N, Andrews ND, Bena J, Wang L, et al. Prevalence of undetected sleep apnea in patients undergoing cardiovascular surgery and impact on postoperative outcomes. J Clin Sleep Med. (2015) 11:1083–9. doi: 10.5664/jcsm.5076
19. Bradley TD, Floras JS. Obstructive sleep apnoea and its cardiovascular consequences. Lancet. (2009) 373:82–93. doi: 10.1016/S0140-6736(08)61622-0
20. Prinz C, Bitter T, Oldenburg O, Faber L, Horstkotte D, Piper C. Sleep apnoea in severe aortic stenosis. Postgrad Med J. (2011) 87:458–62. doi: 10.1136/pgmj.2010.112052
21. Agarwal SK, Heiss G, Barr RG, Chang PP, Loehr LR, Chambless LE, et al. Airflow obstruction, lung function, and risk of incident heart failure: the Atherosclerosis Risk in Communities (ARIC) study. Eur J Heart Fail. (2012) 14:414–22. doi: 10.1093/eurjhf/hfs016
22. Engstrom G, Melander O, Hedblad B. Population-based study of lung function and incidence of heart failure hospitalisations. Thorax. (2010) 65:633–8. doi: 10.1136/thx.2010.135392
23. Servantes DM, Javaheri S, Kravchychyn ACP, Storti LJ, Almeida DR, De Mello MT, et al. Effects of exercise training and CPAP in patients with heart failure and OSA: a preliminary study. Chest. (2018) 154:808–17. doi: 10.1016/j.chest.2018.05.011
24. Meguro K, Adachi H, Oshima S, Taniguchi K, Nagai R. Exercise tolerance, exercise hyperpnea and central chemosensitivity to carbon dioxide in sleep apnea syndrome in heart failure patients. Circ J. (2005) 69:695–9. doi: 10.1253/circj.69.695
25. Arzt M, Harth M, Luchner A, Muders F, Holmer SR, Blumberg FC, et al. Enhanced ventilatory response to exercise in patients with chronic heart failure and central sleep apnea. Circulation. (2003) 107:1998–2003. doi: 10.1161/01.CIR.0000065227.04025.C2
26. Redline S, Lewis EF. Gravitational influences and shifting propensity for sleep apnea: another source of heterogeneity or a new intervention target? Circulation. (2010) 121:1583–5. doi: 10.1161/CIR.0b013e3181dd3e5f
27. Del Forno B, Lapenna E, Dalrymple-Hay M, Taramasso M, Castiglioni A, Alfieri O, et al. Recent advances in managing tricuspid regurgitation. F1000Res. (2018) 7:355. doi: 10.12688/f1000research.13328.1
28. Lin G, Nishimura RA, Connolly HM, Dearani JA, Sundt TM 3rd, Hayes DL. Severe symptomatic tricuspid valve regurgitation due to permanent pacemaker or implantable cardioverter-defibrillator leads. J Am Coll Cardiol. (2005) 45:1672–5. doi: 10.1016/j.jacc.2005.02.037
29. Hahn RT, Meduri CU, Davidson CJ, Lim S, Nazif TM, Ricciardi MJ, et al. Early feasibility study of a transcatheter tricuspid valve annuloplasty: SCOUT trial 30-day results. J Am Coll Cardiol. (2017) 69:1795–806. doi: 10.1016/j.jacc.2017.01.054
30. Kuwata S, Taramasso M, Nietlispach F, Maisano F. Transcatheter tricuspid valve repair toward a surgical standard: first-in-man report of direct annuloplasty with a cardioband device to treat severe functional tricuspid regurgitation. Eur Heart J. (2017) 38:1261. doi: 10.1093/eurheartj/ehw660
31. Nickenig G, Kowalski M, Hausleiter J, Braun D, Schofer J, Yzeiraj E, et al. Transcatheter treatment of severe tricuspid regurgitation with the edge-to-edge MitraClip technique. Circulation. (2017) 135:1802–14. doi: 10.1161/CIRCULATIONAHA.116.024848
32. Fam NP, Ho EC, Zahrani M, Samargandy S, Connelly KA. Transcatheter tricuspid valve repair with the PASCAL system. JACC Cardiovasc Interv. (2018) 11:407–8. doi: 10.1016/j.jcin.2017.12.004
33. Lauten A, Doenst T, Hamadanchi A, Franz M, Figulla HR. Percutaneous bicaval valve implantation for transcatheter treatment of tricuspid regurgitation: clinical observations and 12-month follow-up. Circ Cardiovasc Interv. (2014) 7:268–72. doi: 10.1161/CIRCINTERVENTIONS.113.001033
34. Taramasso M, Zuber M, Kuwata S, Nietlispach F, Maisano F. Clipping of the tricuspid valve: proposal of a “Rosetta Stone” nomenclature for procedural 3D transoesophageal guidance. Eurointervention. (2017) 12:e1825–e7. doi: 10.4244/EIJ-D-16-00307
Keywords: sleep-disordered breathing, tricuspid regurgitation, right heart failure, transcatheter caval valve implantation, ApneaLink
Citation: Wang Y, Fernandes Branco R, Fietzeck A, Penzel T and Schöbel C (2021) Feasibility of Transcatheter Caval Valve Implantation to Improve Sleep-Disordered Breathing in Patients With Severe Tricuspid Regurgitation—A Pilot Study. Front. Cardiovasc. Med. 8:673164. doi: 10.3389/fcvm.2021.673164
Received: 26 February 2021; Accepted: 03 June 2021;
Published: 19 July 2021.
Edited by:
Andrew T. Lovering, University of Oregon, United StatesReviewed by:
Sophie Lalande, University of Texas at Austin, United StatesJonathan E. Elliott, Oregon Health and Science University, United States
Sophie Crinion, Queen's University, Canada
Copyright © 2021 Wang, Fernandes Branco, Fietzeck, Penzel and Schöbel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Youmeng Wang, eW91bWVuZy53YW5nJiN4MDAwNDA7Y2hhcml0ZS5kZQ==
†These authors have contributed equally to this work and share first authorship