
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cardiovasc. Med. , 27 April 2021
Sec. Cardiovascular Imaging
Volume 8 - 2021 | https://doi.org/10.3389/fcvm.2021.667984
This article is part of the Research Topic Advances in Cardiac Imaging and Heart Failure Management View all 42 articles
 Andrea Barbieri1Alessandro Albini1Anna Maisano1Gerardo De Mitri1Giovanni Camaioni1Niccolò Bonini1
Andrea Barbieri1Alessandro Albini1Anna Maisano1Gerardo De Mitri1Giovanni Camaioni1Niccolò Bonini1 Francesca Mantovani2*Giuseppe Boriani1
Francesca Mantovani2*Giuseppe Boriani1Echocardiography is the most validated, non-invasive and used approach to assess left ventricular hypertrophy (LVH). Alternative methods, specifically magnetic resonance imaging, provide high cost and practical challenges in large scale clinical application. To include a wide range of physiological and pathological conditions, LVH should be considered in conjunction with the LV remodeling assessment. The universally known 2-group classification of LVH only considers the estimation of LV mass and relative wall thickness (RWT) to be classifying variables. However, knowledge of the 2-group patterns provides particularly limited incremental prognostic information beyond LVH. Conversely, LV enlargement conveys independent prognostic utility beyond LV mass for incident heart failure. Therefore, a 4-group LVH subdivision based on LV mass, LV volume, and RWT has been recently suggested. This novel LVH classification is characterized by distinct differences in cardiac function, allowing clinicians to distinguish between different LV hemodynamic stress adaptations in various cardiovascular diseases. The new 4-group LVH classification has the advantage of optimizing the LVH diagnostic approach and the potential to improve the identification of maladaptive responses that warrant targeted therapy. In this review, we summarize the current knowledge on clinical value of this refinement of the LVH classification, emphasizing the role of echocardiography in applying contemporary proposed indexation methods and partition values.
Nowadays, the perpetual controversy between the importance of structural and functional anomalies in the failed heart appears to lack consensus (1). On the one side, the left ventricular (LV) ejection fraction (EF) calculation informs many care decisions for heart failure, on the other hand, using modern echocardiographic techniques, the quantification of LV mass and geometry is highly feasible and with a single diagnostic exam. Especially, left ventricular hypertrophy (LVH), when defined by increased ventricular mass according to the classification and partition values proposed by the American Society of Echocardiography/European Association of Cardiovascular Imaging (ASE/EACVI) (2), is a strong independent predictor of cardiovascular risk in adults undergoing assessment for any indication (3).
Importantly, in order to cover a broad variety of physiological and pathological disorders, LVH should be considered according to the classification of LV remodeling, which is the initial step of cardiac damage. The most commonly used categorization for LVH remodeling patterns is proposed by the ASE/EACVI, which uses only LV mass and relative wall thickness (RWT) as classifying variables with two known basic patterns: concentric and eccentric LVH (2). However, although patients with concentric LVH have a different clinical and biomarker phenotype compared to those with eccentric LVH (4), the knowledge of these remodeling patterns provided particularly limited incremental prognostic information beyond LVH per se. A recent systematic review and network meta-analysis of 22 echocardiographic publications (76.133 individuals) studied across various patient populations showed that concentric and eccentric LVH was associated with similar increased all-cause mortality (5). The limitations of the conventional 2-group LVH classification represent possible explanations for this observation. Indeed, since the 2-group LVH classification uses a ratio between the LV cavity diameter and the LV wall thickness, the variations in end-diastolic volume (EDV) and thickness occurring in numerous remodeling patterns cannot be differentiated. Of note, it is known that the simple LV enlargement assessed by echocardiography conveyed independent prognostic utility beyond LV mass for incident heart failure (6).
These findings as a whole raise the question of whether there may be other methods to distinguish high-risk phenotypes of LVH. In this context, Gaasch and Zile proposed a subdivision of LVH based on LV mass, EDV and RWT (7). Using this method, a 4-group LVH category based on ventricular concentricity and dilation can be recognized. Depending on EDV dilatation, this classification subdivides both eccentric LVH and concentric LVH into two sub-groups (Figures 1, 2). Essentially, this revised classification assumes that only if the increased LV mass is associated with increased wall thickness and/or ventricular dilation LVH should be considered pathologic.
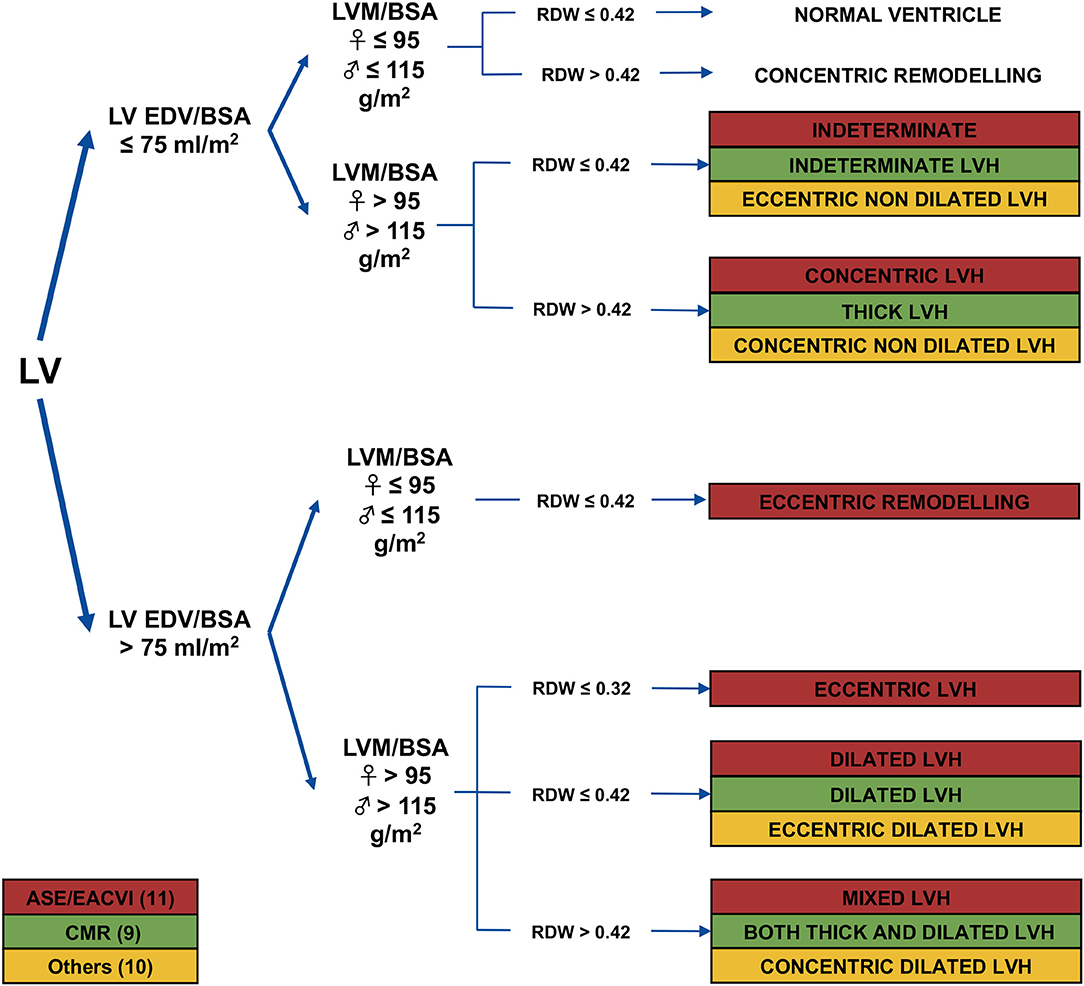
Figure 1. Schematic description of the 4-group left ventricular hypertrophy classification. The different terminology used in the literature and the normal range of parameters under consideration are highlighted. LV, left ventricular; EDV, end-diastolic volume; BSA, body surface area; LVH, left ventricular hypertrophy; RWT, relative wall thickness; ESC, European association of cardiology; CMR, Cardiac magnetic Resonance. Adapted from (8).
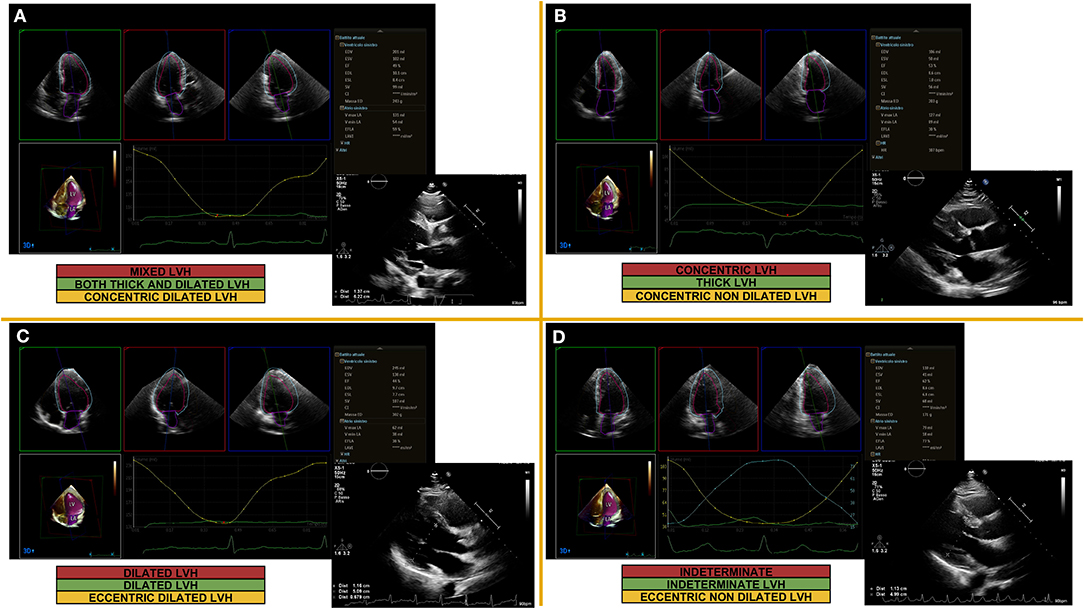
Figure 2. Examples of echocardiographic left lentricular hypertrophy classification based on concentricity, mass and volume quantification. Parasternal long axis view for linear 2D measurements (LV mass, concentricity) and 3D measurements (LV volumes) obtained from automated DHM (Dynamic Heart Model, Philips Healthcare, Andover, MA, USA) in a patient with mixed LVH (A), concentric LVH (B), dilated LVH (C), indeterminate LVH (D); 2D, two-dimensional; 3D, three-dimensional; LV, left ventricular; LVH, left ventricular hypertrophy.
Although cardiac magnetic resonance (CMR) showed better performance than echocardiography for accuracy and precision in LV mass and volumes assessment could not be served as a routine method for risk assessment of patients with LVH, since it is time-consuming and costly. Accordingly, the purpose of this review is to address the implementation in practice of the novel 4-group LVH classification, focusing on the clinical utility of currently established and widely available echocardiographic techniques.
A definition of the terminology and the normality range of parameters under consideration is required in any LV quantitative analysis. The initially proposed 4-group classification was based on CMR (9). The LVH groups were referred to as: “indeterminate LVH” (neither increased EDV nor concentricity, while LV mass was increased), “dilated LVH” (increased EDV with normal concentricity), “thick LVH” (increased concentricity with normal EDV), and “both thick and dilated LVH” (increased EDV and concentricity). Others have extrapolated successively this classification to echocardiography and have named distinctly the four LVH patterns (e.g., indeterminate LVH as “eccentric non-dilated”; dilated LVH as “eccentric dilated”; thick LVH as “concentric non-dilated”; and both thick and dilated LVH as “concentric dilated”) (10).
More recently, to define the range of normal RWT (0.32–0.42), the ASE/EACVI further divided patients with LVH and EDV dilation into three subgroups: mixed LVH (RWT> 0.42), dilated LVH (RWT 0.32–0.42), eccentric LVH (RWT <0.32). Therefore, it was proposed to evolve from the 4-group classification into a new 5-group category to identify subjects with physiological LVH or dilated LVH (e.g., pregnant women, athlete's heart) (11).
We opted to use the ASE/EACVI echocardiographic terminology in the following section for consistency and clarity of this review. Studies that divided patients with LVH and EDV dilation into three subgroups based on RWT are be specifically reported.
Using the indexation methods and partition values currently proposed by the ASE/EACVI (11), LVH was seen frequently in the general echocardiographic population (42% of subjects). The most common pattern resulted in concentric LVH (16%) (12). However, the LVH pattern's prevalence depended on the population studied (Table 1). Indeed, in patients with isolated severe aortic stenosis, the most frequent remodeling pattern was concentric LVH (57.3%), followed by mixed (18.9%) and dilated LVH (8.4%). Still, the prevalence of the remodeling patterns differed between the symptomatic and asymptomatic patients (20).
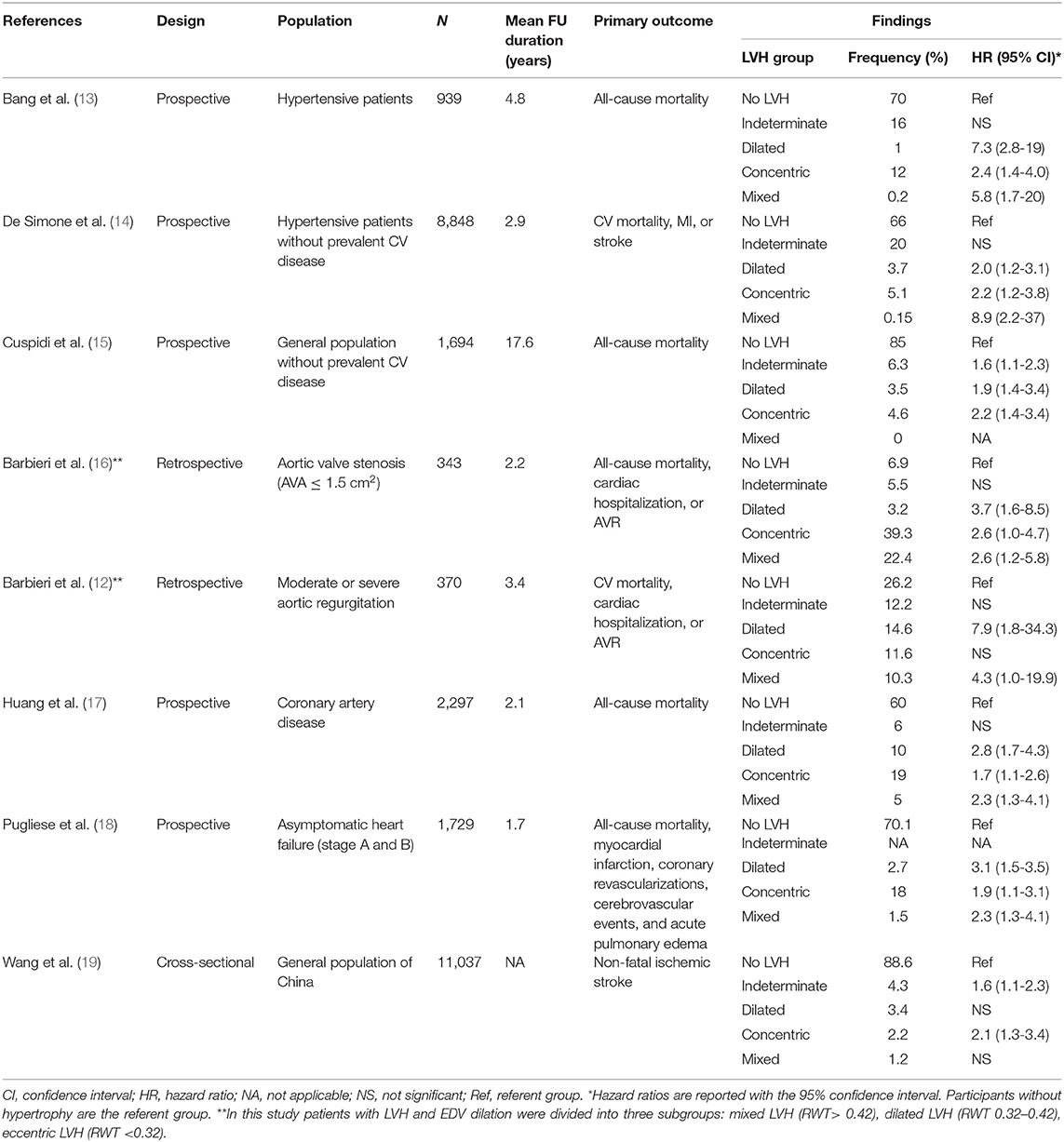
Table 1. Summary of echocardiographic studies assessing the association of the 4-group left ventricular hypertrophy classification with cardiovascular outcomes.
It is known that the curvilinear inverse relation between EF and EDV generally predicts that EF would be depressed when the LV is dilated and preserved when the volume is normal (21). The LV pump function's normality depends on maintaining the double-helical (spiral) alignment of the LV myocardial architecture determined by the LV geometry. In concentric LVH with normal EDV, the LV myocardial architecture's double-helical orientation is preserved, resulting in a normal or near-normal EF. Conversely, the LV myocardial architecture's double-helical orientation is disrupted in the eccentric LVH with unbalanced EDV dilatation, resulting in decreased EF (22). Therefore to be useful in clinical practice, the LVH remodeling patterns must be accompanied by compatible hemodynamic and functional profiles plausible from a pathophysiological perspective.
In the original Dallas heart study, the four geometric patterns of LVH were associated with different clinical characteristics, biomarkers, and ejection fractions. Compared with subjects with concentric LVH, those with mixed LVH had a lower EF and higher NT-pro-BNP and BNP levels (P < 0.001 for all). Subjects with dilated LVH had a lower EF and higher troponin T, NT-pro-BNP, and BNP levels versus those with indeterminate LVH (P < 0.001 for all). Subjects with indeterminate LVH had no elevation of markers of cardiac stress as compared with subjects without LVH (9).
These findings were extended to a sizeable echocardiographic population focusing on applying contemporary proposed indexation methods and partition values. The worst hemodynamic profile was associated with eccentric LVH. The prevalence of diastolic dysfunction (defined as mean E/E′ > 14) was 43.5% in subjects with eccentric LVH, 36% in those with dilated LVH, 20.7% in concentric LVH and 8.2% in patients without LVH (P < 0.0001). The prevalence of pulmonary hypertension (defined as derived pulmonary artery pressure ≥ 50 mmHg) was 25.7% in subjects with eccentric LVH and 1.9% in those without LVH (P < 0.0001) (12).
Similarly, The 4-group classification was correlated with LV mechanics in a cohort of hypertensive patients. Those with concentric, dilated, and mixed LVH had longitudinal, circumferential, and radial strain unfavorably affected after adjusted analysis. Of note, there was no substantial difference in strain for those with indeterminate LVH and those without LVH (15).
The new 4-group classification also showed higher discrimination of exercise-induced LVH patterns in a cohort of normotensive endurance athletes relative to the existing 2-group classification (8). Besides, other studies tested the association of the 4-group classification with biological markers. In hypertensive patients, dilated or mixed LVH was associated with an increased prevalence of subclinical renal damage (23), patients with metabolic syndrome had a higher prevalence of dilated or mixed LVH (24). Therefore, it appears that the proposed new LVH subcategories are not only mere descriptors of LV geometry but an integral component of parameters reflecting systolic properties.
To resolve the dynamic relationship between LV dilation and myocardial thickening in LVH pathophysiology, several echocardiographic studies have linked the 4-group classification system to clinical outcome in hypertensive patients (13, 14), patients with coronary artery disease (17), patients with asymptomatic (stage A and B) heart failure (18), in the general population with normal LV systolic function and no history of heart failure (25), and patients with valvular heart disease (16, 26).
Compared to participants without LVH, the 4-group LVH classification system was a robust prediction model of adverse cardiovascular outcomes in all these studies Table 1. The Losartan Intervention for Endpoint Reduction Echocardiography sub-study was the first to use readily available echocardiographic measurements to reproduce the results of CMR (9) in 939 hypertensive patients who were treated for 4.8 years. They found that of all-cause mortality risk was increased for patients with dilated, concentric, and mixed LVH [HR (95%CI)]: 7.3 (2.8–19), 2.4 (1.4–4.0), 2.4 (1.4–4.0), respectively. The same result was found for cardiovascular mortality and the composite endpoint of myocardial infarction, stroke, heart failure, and cardiovascular mortality. On the other hand, indeterminate LVH was not associated with increased relative risk compared to patients without LVH identifying a low-risk group with eccentric LVH and the same risk of all-cause mortality or cardiovascular events such as patients with normal LV mass (13). Nevertheless, in this study some of the LVH subgroups had a limited number of endpoints, thus only the primary endpoint of all-cause mortality was adjusted for multiple comparisons, reducing the power to verify the incremental prognostic value of the 4-group system in the two concentric LVH groups.
The largest cohort of 8,848 hypertensive patients with no history of cardiovascular disease from the Campania Salute Network paralleled these findings, showing that patients with indeterminate LVH were not at increased risk compared to those without LVH. Conversely, there was a substantial increase in the incidence of fatal and non-fatal cardiovascular and cerebrovascular accidents in patients with dilated, concentric, and mixed LVH compared to those without LVH [HR (95%CI)]: 2.0 (1.2–3.1), 2.2 (1.2–3.8), 8.9 (2.2–37), respectively (14). This was the first direct evidence that differences in left ventricular geometry may be relevant to the definition of risk profile in a large community-based registry of uncomplicated hypertensive patients.
Huang et al. applied the 4-group LVH classification to 2,297 patients with angiographic evidence of stable coronary artery disease and reported outcomes after a 2-year follow-up. Patients with dilated, concentric, and mixed LVH were at increased risk of all-cause mortality compared with those without LVH [HR (95%CI)]: 2.8 (1.7–4.3), 1.7 (1.1–2.6), 2.3 (1.3–4.1), respectively. Once more, the risk of primary or secondary endpoints was not increased in participants with indeterminate LVH (17). However, only baseline echocardiography data were available, and the modification in LV geometry during interventional and medical therapy was unknown. This is an important limitation considering that in hypertensive patients, only “in-treatment” LV geometry by echocardiography predicted risk of cardiovascular events, but not baseline LV geometry (27).
Our group evaluated the application of the novel LVH classification in patients with valvular heart disease. In 342 patients with aortic stenosis (functional aortic valve area ≤1.5 cm2), there was a significant association between adverse events and LV dilatation or LV remodeling pattern. After multivariate adjustment, dilated, concentric, and mixed LVH were strongly associated with death or cardiac hospitalization [HR (95%CI)]: 3.7 (1.6–8.5), 2.6 (1.0–4.7), 2.6 (1.2–5.8), respectively (16). In 370 consecutive patients with moderate or severe chronic aortic regurgitation, dilated and mixed LVH were associated with the combination of cardiovascular death, hospitalization for acute heart failure, or aortic valve replacement [HR (95%CI)]: 7.9 (1.8–34.3), 4.3 (1.0–19.9), respectively (26). In the Pressioni Monitorate e Loro Associazioni (PAMELA) study, dilated and concentric LVH predicted cardiovascular and all-cause mortality risk in the general population without valve disease and with normal EF after an average follow-up of 17.5 years [HR (95%CI)]: 1.9 (1.4–3.4), 2.2 (1.4–3.4), respectively. In contrast to the above studies, even indeterminate LVH demonstrated independent prognostic value [HR (95%CI)]: 1.6 (1.1–2.3). This may be due to the longer follow-up than other studies. However, the threshold criterion to define increased RWT was 0.45 and 0.44 for men and women, respectively, which was slightly higher than the ASE/EACVI guideline cutoff of 0.43. Of note, only concentric LVH maintained a significant predictive value for both outcomes after adjusting for baseline differences in the LV mass index (25).
In a multicenter study designed by the Italian Society of Echography and Cardiovascular Imaging (SIECVI), the novel 4-group classification was an independent predictor of adverse events during follow-up in 1.750 patients with stage A or B heart failure. Remarkably, it produced a better risk stratification in comparison to the classic 2-group one. The worst prognosis was reported for patients with dilated, concentric, and mixed LVH compared to those without LVH [HR (95%CI)]: 3.1 (1.5–3.5), 1.9 (1.1–3.1), 2.3 (1.3–4.1), respectively (18). The primary study limitation was the use of composite outcomes (all-cause death, myocardial infarction, coronary revascularization, cerebrovascular event, and acute pulmonary edema) due to the low prevalence of adverse events for the study population size and follow-up length.
In a large population from China with low cardiovascular risk, the presence of concentric and indeterminate LVH was associated with an increased risk of non-fatal ischemic stroke [HR (95%CI)]: 2.1 (1.3–3.4), 1.6 (1.1–2.3), respectively. Surprisingly, dilated and mixed LVH were not associated with an increased risk of ischemic stroke (19). Surprisingly, dilated and mixed LVH were not associated with an increased risk of ischemic stroke. Due to the cross-sectional nature of this study, it was difficult to assign causality to these findings. One explanation may be partially attributed to worse cardiometabolic risk factors for individuals with indeterminate LVH. However, in multivariable analysis, LV concentricity, but not LVEDV, was a significant predictor of ischemic stroke when analyzed as continuous variables. It is possible to hypothesize that both the heart and the brain are potential organs at risk for injury as a result of long-term elevated blood pressure, which emerges as critical correlations between LVH and ischemic stroke (28, 29). Furthermore, after adjusting for conventionally measured blood pressure, carotid disease was considered to parallel LV mass (30, 31) and represented a particularly sensitive marker of ischemic stroke (32).
Overall, these observational data suggest that the incorporation of LV chamber dilation into the assessment of LVH identifies important sub-phenotypes within the standard 2-group classification. In particular, LVH with RWT ≤0.42 can be split into a low-risk group (indeterminate LVH) and a high-risk group (dilated LVH). Similarly, the two phenotypes of LV dilatation (dilated and mixed LVH) should be considered a high-risk LVH phenotype.
It is necessary to recognize some potential limitations of the new 4-group LVH classification for its correct use in clinical practice. The 4-group LVH classification scheme is necessarily definite and based on numerical thresholds to be usable. However, for some authors this dichotomous definition of LVH should be reconsidered and analyzed as a continuum from normal to remodeling, with possible implications for reverse remodeling (10). Recently, Yamanaka et al., using a landmark analysis in patients with clinical heart failure and an EF ≥ 50%, found that, compared with patients without LVH or LV enlargement at baseline, subsequent adverse outcomes were more frequent in patients with LVH without LV enlargement at baseline and were even more frequent in patients with LV enlargement (33). In addition to examining the predictive value of LV mass and LVEDV as categorical variables, the authors also examined them as continuous variables: the relationships between structural category and outcome remained unchanged within a multivariate analysis adjusting for clinical variables including EF.
Also, a patient can move between categories only based on limitations in the reproducibility of echocardiographic measurements (34). At the same time, it may reflect a transitional pattern of dynamic temporal change. Previous data suggested that changes in LV geometry over time may impact prognosis similarly to many studies suggesting improvements in prognosis with regression of LVH (35). Therefore, the trajectory of the LVH pattern more than a single evaluation may be necessary to further classify patients with LVH.
The consideration of EDV, mass, and RWT does not allow all LVH remodeling changes to be classified (12% of consecutive patients for any echocardiographic indication) (12). However, in cardiology, this gap in classification is not new. Whether this misclassification has clinical implications should be investigated in more extensive research (36). Some studies are limited because they combined patients with dilated and eccentric LVH into the same group (dilated LVH). Still, these two groups may probably have a differential risk of developing incident heart failure. The dilated LVH pattern could not be differentiated by “physiological LVH,” such as athlete's heart with an early stage of a pathological condition. However, by contextualizing the clinical environment and the degree of LV dilation, these LVH profiles are easily detectable.
It should be stressed that the determination of RWT can be limited by non-uniform wall thickness and regional shape deformation (37). Three-dimensional echocardiography (3D), without geometric assumptions about LV form and wall thickening distribution, is the only echocardiographic technique that accurately measures the LV mass in these patients (38). It is worth noting that in hypertensive patients, a high 3D-LV mass/EDV ratio identified a higher incidence of concentric LVH compared to 2D-derived relative wall thickness, which is inversely correlated with the stroke volume (39) and early systolic and diastolic dysfunction (40).
The current normative values are derived from 2D-echocardiography. With the advent of artificial intelligence and automated 3D approach to LV chamber quantification (Figure 2), echocardiographic quantification practice will be changed soon and new and gender-specific cut-off values will be proposed (41).
While CMR outperformed echocardiography in terms of accuracy and precision in LV mass evaluation, no clear comparison of the two methods has been done for the ability to predict clinical events, LVH classification agreement, or cardiovascular risk reclassification.
Other LVH diagnostic methods have their risk profile, independent and complementary to the LV mass detected by echocardiography. A previous analysis from the Cardiovascular Health Study showed that both LVH detected by electrocardiography and echocardiography was predictive of future atrial fibrillation events, independent of well-known risk factors, suggesting that LVH detected by electrocardiography is an important electrophysiological marker of cardiac abnormalities independent of LV mass detected by echocardiography (42).
Finally, because the vast majority of subjects enrolled in studies were Caucasian, results may not apply to other ethnicities (43).
A key finding of the improved LVH phenotypic characterization is the demonstration of a wide range of changes in EDV, mass, and function in patients with chronic heart failure. Therefore, the main questions are whether some of the differences in LV remodeling response are due to differences in the lesion or discrepancies in the host's lesion response. However, the question will be almost impossible to address in clinical practice (44). Indeed, the occurrence of LVH geometric anomalies showed considerable variability in patients with the same heart disease (13, 17, 35, 37, 45–50). Several factors, including but not limited to gender, diabetes, previous myocardial infarction, obesity, and valve diseases, tended to affect the remodeling of LVH (51). Besides, there are likely underlying genetic factors that remain poorly identified (52). Therefore, refining the classification of LVH could distinguish the distinctive development of LV geometric changes from baseline and the transition to a maladaptive phase of remodeling in the individual patient (10). Using the conventional 2-group categorization, previous echocardiographic longitudinal studies showed that progression from concentric LVH to eccentric LVH occurred in 19% of subjects after 4 years (53) and 25% after 7 years (54). Nevertheless, how often those who converted to eccentric LVH had a dilated LV at follow-up was not mentioned. Recent CMR data indicated that in hypertensive patients, concentric LVH dilated less often than previously assumed over an extended timeframe in the absence of interval myocardial infarction (55).
Enhanced LVH characterization will also provide opportunities for LV geometry-directed therapeutic intervention in order to reduce incident heart failure. Recent data suggested that, in patients with heart failure with reduced EF, patients with concentric LVH did not experienced similar benefits from up-titration angiotensin-converting enzyme inhibitors/angiotensin receptor blockers and beta-blockers compared to patients with eccentric LVH (4).
Chronic heart failure is a dynamic clinical condition with a broad phenotypic variability that makes the “one-size-fits-all” approach inadequate to care. In clinical practice, many patients have a combination of chronic pressure and volume overload, leading to distinct and more complex LVH geometric patterns than previously considered, underscoring the need for a better LVH classification. With this in mind, conventional 2-group patterns are not adequate for risk stratifying patients with LVH. Conversely, preliminary findings supported the use of LV remodeling assessment based on EDV, mass, and RWT by echocardiography. As clinicians, it is time to start thinking about new LVH classification proposals that will consider many parameters of LV morphology and function, including underlying remodeling abnormalities that can be obtained with current echocardiographic technology. However, further evidence is needed to understand how it can be integrated into clinical decision-making.
AB: substantial contributions to the conception or design of the work and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. AB, AA, AM, GD, GC, and NB: acquisition, analysis or interpretation of data for the work. AB, GB, AA, AM, FM, GD, GC, and NB: drafting the work or revising it critically for important intellectual content and provide approval for publication of the content. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Triposkiadis F, Butler J, Abboud FM, Armstrong PW, Adamopoulos S, Atherton JJ, et al. The continuous heart failure spectrum: moving beyond an ejection fraction classification. Eur Heart J. (2019) 40:2155–63B. doi: 10.1093/eurheartj/ehz158
2. Lang RM, Badano LP, Mor-Avi V, Afilalo J, Armstrong A, Ernande L, et al. Recommendations for cardiac chamber quantification by echocardiography in adults: an update from the American society of echocardiography and the European association of cardiovascular imaging. Eur Heart J Cardiovasc Imaging. (2015) 16:233–71. doi: 10.1093/ehjci/jev014
3. Barbieri A, Bursi F, Mantovani F, Valenti C, Quaglia M, Berti E, et al. Prognostic impact of left ventricular mass severity according to the classification proposed by the American society of echocardiography/European association of echocardiography. J Am Soc Echocardiogr. (2011) 24:1383–91. doi: 10.1016/j.echo.2011.08.012
4. Nauta JF, Hummel YM, Tromp J, Ouwerkerk W, van der Meer P, Jin X, et al. Concentric vs. eccentric remodelling in heart failure with reduced ejection fraction: clinical characteristics, pathophysiology and response to treatment. Eur J Heart Fail. (2020) 22:1147–55. doi: 10.1002/ejhf.1632
5. Zheng Q, Loo G, Le T-T, Shi L, Chan ES-Y, Chin CWL. Prognosis associated with geometric patterns of left ventricular remodeling: systematic review and network meta-analysis. F1000Res. (2019) 8:1130. doi: 10.12688/f1000research.19907.1
6. Zile MR, Gaasch WH, Patel K, Aban IB, Ahmed A. Adverse left ventricular remodeling incommunity-dwelling older adults predicts incident heart failure and mortality. JACC Hear Fail. (2014) 2:512–22. doi: 10.1016/j.jchf.2014.03.016
7. Gaasch WH, Zile MR. Left ventricular structural remodeling in health and disease: with special emphasis on volume, mass, and geometry. J Am Coll Cardiol. (2011) 58:1733–40. doi: 10.1016/j.jacc.2011.07.022
8. Trachsel LD, Ryffel CP, De Marchi S, Seiler C, Brugger N, Eser P, et al. Exercise-induced cardiac remodeling in nonelite endurance athletes: Comparison of 2-tiered and 4-tiered classification of left ventricular hypertrophy. PLoS ONE. (2018) 13:1–12. doi: 10.1371/journal.pone.0193203
9. Khouri MG, Peshock RM, Ayers CR, De Lemos JA, Drazner MH. A 4-tiered classification of left ventricular hypertrophy based on Left ventricular geometry the dallas Heart study. Circ Cardiovasc Imaging. (2010) 3:164–71. doi: 10.1161/CIRCIMAGING.109.883652
10. Garg S, Drazner MH. Refining the classification of left ventricular hypertrophy to provide new insights into the progression from hypertension to heart failure. Curr Opin Cardiol. (2016) 31:387–93. doi: 10.1097/HCO.0000000000000299
11. Marwick TH, Gillebert TC, Aurigemma G, Chirinos J, Derumeaux G, Galderisi M, et al. Recommendations on the use of echocardiography in adult hypertension: a report from the european association of cardiovascular imaging (EACVI) and the American society of echocardiography (ASE). J Am Soc Echocardiogr. (2015) 28:727–54. doi: 10.1016/j.echo.2015.05.002
12. Barbieri A, Rossi A, Gaibazzi N, Erlicher A, Mureddu GF, Frattini S, et al. Refined 4-group classification of left ventricular hypertrophy based on ventricular concentricity and volume dilatation outlines distinct noninvasive hemodynamic profiles in a large contemporary echocardiographic population. Echocardiography. (2018) 35:1258–65. doi: 10.1111/echo.14031
13. Bang CN, Gerdts E, Aurigemma GP, Boman K, De Simone G, Dahlöf B, et al. Four-group classifcation of left ventricular hypertrophy based on ventricular concentricity and dilatation identifes a low-risk subset of eccentric hypertrophy in hypertensive patients. Circ Cardiovasc Imaging. (2014) 7:422–9. doi: 10.1161/CIRCIMAGING.113.001275
14. De Simone G, Izzo R, Aurigemma GP, De Marco M, Rozza F, Trimarco V, et al. Cardiovascular risk in relation to a newclassification of hypertensive left ventricular geometric abnormalities. J Hypertens. (2015) 33:745–54. doi: 10.1097/HJH.0000000000000477
15. Tadic M, Cuspidi C, Majstorovic A, Kocijancic V, Celic V. The relationship between left ventricular deformation and different geometric patterns according to the updated classification: findings from the hypertensive population. J Hypertens. (2015) 33:1954–61. doi: 10.1097/HJH.0000000000000618
16. Barbieri A, Bartolacelli Y, Bursi F, Manicardi M, Boriani G. Remodeling classification system considering left ventricular volume in patients with aortic valve stenosis: Association with adverse cardiovascular outcomes. Echocardiography. (2019) 36:639–50. doi: 10.1111/echo.14299
17. Huang BT, Peng Y, Liu W, Zhang C, Huang FY, Wang PJ, et al. Subclassification of left ventricular hypertrophy based on dilation stratifies coronary artery disease patients with distinct risk. Eur J Clin Invest. (2014) 44:893–901. doi: 10.1111/eci.12320
18. Pugliese NR, Fabiani I, La Carrubba S, Conte L, Antonini-Canterin F, Colonna P, et al. Classification and prognostic evaluation of left ventricular remodeling in patients with asymptomatic heart failure. Am J Cardiol. (2017) 119:71–7. doi: 10.1016/j.amjcard.2016.09.018
19. Wang H, Wang S, Yi X, Tao Y, Qian H, Jia P, et al. Estimate of ischemic stroke prevalence according to a novel 4-tiered classification of left ventricular hypertrophy: insights from the general Chinese population. Ann Med. (2018) 50:519–28. doi: 10.1080/07853890.2018.1500702
20. Di Nora C, Cervesato E, Cosei I, Ravasel A, Popescu BA, Zito C, et al. New classification of geometric ventricular patterns in severe aortic stenosis: could it be clinically useful? Echocardiography. (2018) 35:1077–84. doi: 10.1111/echo.13892
21. Gaasch WH, Delorey DE, St. John Sutton MG, Zile MR. Patterns of structural and functional remodeling of the left ventricle in chronic heart failure. Am J Cardiol. (2008) 102:459–62. doi: 10.1016/j.amjcard.2008.03.081
22. Triposkiadis F, Giamouzis G, Boudoulas KD, Karagiannis G, Skoularigis J, Boudoulas H, et al. Left ventricular geometry as a major determinant of left ventricular ejection fraction: physiological considerations and clinical implications. Eur J Heart Fail. (2018) 20:436–44. doi: 10.1002/ejhf.1055
23. Ratto E, Viazzi F, Bonino B, Gonnella A, Garneri D, Parodi EL, et al. Left ventricular dilatation and subclinical renal damage in primary hypertension. J Hypertens. (2015) 33:605–11. doi: 10.1097/HJH.0000000000000430
24. Ratto E, Viazzi F, Verzola D, Bonino B, Gonnella A, Parodi EL, et al. Metabolic syndrome is associated with left ventricular dilatation in primary hypertension. J Hum Hypertens. (2016) 30:158–63. doi: 10.1038/jhh.2015.67
25. Cuspidi C, Facchetti R, Bombelli M, Sala C, Tadic M, Grassi G, et al. Risk of mortality in relation to an updated classification of left ventricular geometric abnormalities in a general population: the pamela study. J Hypertens. (2015) 33:2133–40. doi: 10.1097/HJH.0000000000000658
26. Barbieri A, Giubertoni E, Bartolacelli Y, Bursi F, Manicardi M, Boriani G. New classification of geometric patterns considering left ventricular volume in patients with chronic aortic valve regurgitation: prevalence and association with adverse cardiovascular outcomes. Echocardiography. (2019) 36:38–46. doi: 10.1111/echo.14190
27. Gerdts E, Cramariuc D, Simone G, De Wachtell K, Devereux RB. Impact of left ventricular geometry on prognosis in hypertensive patients with left ventricular hypertrophy (the LIFE study). Eur J Echocardiogr. (2008) 809–15. doi: 10.1093/ejechocard/jen155
28. Bikkina M, Levy D, Evans JC, Larson MG, Benjamin EJ, Wolf PA, et al. Left Ventricular mass and risk of stroke in an elderly cohort: the framingham heart study. JAMA. (1994) 272:33–6. doi: 10.1001/jama.272.1.33
29. Selvetella G, Notte A, Maffei A, Calistri V, Scamardella V, Frati G, et al. Left ventricular hypertrophy is associated with asymptomatic cerebral damage in hypertensive patients. Stroke. (2003) 34:1766–70. doi: 10.1161/01.STR.0000078310.98444.1D
30. Di Bello V, Carerj S, Perticone F, Benedetto F, Palombo C, Talini E, et al. Carotid intima-media thickness in asymptomatic patients with arterial hypertension without clinical cardiovascular disease: relation with left ventricular geometry and mass and coexisting risk factors. Angiology. (2009) 60:705–13. doi: 10.1177/0003319708329337
31. Pierdomenico SD, Mancini M, Cuccurullo C, Guglielmi MD, Pierdomenico AM, Di Nicola M, et al. Prediction of carotid plaques in hypertensive patients by risk factors, left ventricular hypertrophy, and epicardial adipose tissue thickness. Heart Vessels. (2013) 28:277–83. doi: 10.1007/s00380-012-0240-y
32. Roman MJ, Saba PS, Pini R, Spitzer M, Pickering TG, Rosen S, et al. Parallel cardiac and vascular adaptation in hypertension. Circulation. (1992) 86:1909–18. doi: 10.1161/01.CIR.86.6.1909
33. Yamanaka S, Sakata Y, Nochioka K, Miura M, Kasahara S, Sato M, et al. Prognostic impacts of dynamic cardiac structural changes in heart failure patients with preserved left ventricular ejection fraction. Eur J Heart Fail. (2020) 22:2258–68. doi: 10.1002/ejhf.1945
34. Gottdiener JS, Bednarz J, Devereux R, Gardin J, Klein A, Manning WJ, et al. American Society of Echocardiography recommendations for use of echocardiography in clinical trials: a report from the american society of echocardiography's guidelines and standards committee and the task force on echocardiography in clinical trials. J Am Soc Echocardiogr. (2004) 17:1086–119. doi: 10.1016/S0894-7317(04)00675-3
35. Milani RV, Lavie CJ, Mehra MR, Ventura HO, Kurtz JD, Messerli FH. Left ventricular geometry and survival in patients with normal left ventricular ejection fraction. Am J Cardiol. (2006) 97:959–63. doi: 10.1016/j.amjcard.2005.10.030
36. Carerj S, La Carrubba S, Antonini-Canterin F, Di Salvo G, Erlicher A, Liguori E, et al. The incremental prognostic value of echocardiography in asymptomatic stage a heart failure. J Am Soc Echocardiogr. (2010) 23:1025–34. doi: 10.1016/j.echo.2010.06.017
37. Savage DD, Garrison RJ, Kannel WB, Levy D, Anderson SJ, Stokes J 3rd, et al. The spectrum of left ventricular hypertrophy in a general population sample: the Framingham Study. Circulation. (1987) 75(1 Pt 2):I26–33.
38. Volpato V, Mor-Avi V, Narang A, Prater D, Gonçalves A, Tamborini G, et al. Automated, machine learning-based, 3D echocardiographic quantification of left ventricular mass. Echocardiography. (2019) 36:312–9. doi: 10.1111/echo.14234
39. Lembo M, Esposito R, Santoro C, Lo Iudice F, Schiano-Lomoriello V, Fazio V, et al. Three-dimensional echocardiographic ventricular mass/end-diastolic volume ratio in native hypertensive patients: relation between stroke volume and geometry. J Hypertens. (2018) 36:1697–704. doi: 10.1097/HJH.0000000000001717
40. Lembo M, Santoro C, Sorrentino R, Trimarco B, Galderisi M, Esposito R. Impact of left ventricular mass/end-diastolic volume ratio by three-dimensional echocardiography on two-dimensional global longitudinal strain and diastolic function in native hypertensive patients. J Hypertens. (2019) 37:2041–7. doi: 10.1097/HJH.0000000000002147
41. Jenkins C, Tsang W. Three-dimensional echocardiographic acquisition and validity of left ventricular volumes and ejection fraction. Echocardiography. (2020) 37:1646–53. doi: 10.1111/echo.14862
42. Patel N, O'Neal WT, Whalen SP, Soliman EZ. Electrocardiographic left ventricular hypertrophy predicts atrial fibrillation independent of left ventricular mass. Ann Noninvasive Electrocardiol. (2017) 22:1–5. doi: 10.1111/anec.12419
43. Ejiofor L, Di Nora C, Cervesato E, Cosei I, Ravasel A, Popescu BA, et al. Differences in left ventricular geometry in hypertensive African-Europeans and Caucasian patients. Eur J Intern Med. (2019) 62:43–7. doi: 10.1016/j.ejim.2019.01.006
44. Carabello BA. Concentric versus eccentric remodeling. J Card Fail. (2002) 8(6 Suppl):258–63. doi: 10.1054/jcaf.2002.129250
45. Huwez FU, Pringle SD, Macfarlane PW. A new classification of left ventricular geometry in patients with cardiac disease based on M-mode echocardiography. Am J Cardiol. (1992) 70:681–8. doi: 10.1016/0002-9149(92)90213-I
46. Koren MJ, Devereux RB, Casale PN, Savage DD, Laragh JH. Relation of left ventricular mass and geometry to morbidity and mortality in uncomplicated essential hypertension. Ann Intern Med. (1991) 114:345–52. doi: 10.7326/0003-4819-114-5-345
47. Ganau A, Devereux RB, Roman MJ, De Simone GS, Pickering TG, Saba PS, et al. Patterns of left ventricular hypertrophy and geometric remodeling in essential hypertension. J Am Coll Cardiol. (1550) 19:1550–8. doi: 10.1016/0735-1097(92)90617-V
48. Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Battistelli M, Bartoccini C, et al. Adverse prognostic significance of concentric remodeling of the left ventricle in hypertensive patients with normal left ventricular mass. J Am Coll Cardiol. (1995) 25:871–8. doi: 10.1016/0735-1097(94)00424-O
49. Krumholz HM, Larson M, Levy D. Prognosis of left ventricular geometric patterns in the Framingham heart study. J Am Coll Cardiol. (1995) 25:879–84. doi: 10.1016/0735-1097(94)00473-4
50. Garg S, De Lemos JA, Ayers C, Khouri MG, Pandey A, Berry JD, et al. Association of a 4-tiered classification of LV hypertrophy with adverse CV outcomes in the general population. JACC Cardiovasc Imaging. (2015) 8:1034–41. doi: 10.1016/j.jcmg.2015.06.007
51. Oktay AA, Lavie CJ, Milani RV, Ventura HO, Gilliland YE, Shah S, et al. Current Perspectives on left ventricular geometry in systemic hypertension. Prog Cardiovasc Dis. (2016) 59:235–46. doi: 10.1016/j.pcad.2016.09.001
52. Litwin SE. Cardiac “morphomics” do we need to measure lv mass and geometry in everyone? JACC Cardiovasc Imaging. (2015) 8:1016–8. doi: 10.1016/j.jcmg.2015.06.008
53. Lieb W, Gona P, Larson MG, Aragam J, Zile MR, Cheng S, et al. The natural history of left ventricular geometry in the community: clinical correlates and prognostic significance of change in LV geometric pattern. JACC Cardiovasc Imaging. (2014) 7:870–8. doi: 10.1016/j.jcmg.2014.05.008
54. Desai RV, Ahmed MI, Mujib M, Aban IB, Zile MR, Ahmed A. Natural history of concentric left ventricular geometry in community-dwelling older adults without heart failure during seven years of follow-up. Am J Cardiol. (2011) 107:321–4. doi: 10.1016/j.amjcard.2010.09.019
Keywords: left ventricular mass, left ventricular function, left ventricular volume, echocardiograghy, clinical value, prognosis
Citation: Barbieri A, Albini A, Maisano A, De Mitri G, Camaioni G, Bonini N, Mantovani F and Boriani G (2021) Clinical Value of Complex Echocardiographic Left Ventricular Hypertrophy Classification Based on Concentricity, Mass, and Volume Quantification. Front. Cardiovasc. Med. 8:667984. doi: 10.3389/fcvm.2021.667984
Received: 15 February 2021; Accepted: 24 March 2021;
Published: 27 April 2021.
Edited by:
Giulia Elena Mandoli, University of Siena, ItalyReviewed by:
Iacopo Fabiani, Gabriele Monasterio Tuscany Foundation (CNR), ItalyCopyright © 2021 Barbieri, Albini, Maisano, De Mitri, Camaioni, Bonini, Mantovani and Boriani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Francesca Mantovani, ZnJhbmN5X21hbnRvQGhvdG1haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.