 Fadi Sawaya
Fadi Sawaya Troels H. Jørgensen1
Troels H. Jørgensen1 Ole De Backer
Ole De Backer
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cardiovasc. Med. , 04 October 2019
Sec. Structural Interventional Cardiology
Volume 6 - 2019 | https://doi.org/10.3389/fcvm.2019.00145
This article is part of the Research Topic Structural Valve Degeneration and Failure in Transcatheter and Surgical Bioprosthesis View all 6 articles
Transcatheter aortic valve replacement (TAVR) is an established alternative to surgical valve replacement for patients with severe aortic stenosis (AS) and increased surgical risk. On the basis of the favorable outcomes of recent randomized clinical trials conducted in intermediate and low risk populations, TAVR is expected in the near future to be offered to patients not only at lower surgical risk, but also with longer life expectancy. In this particular subset, the long-term durability of the bioprosthetic valve is of critical importance. The European Association of Percutaneous Cardiovascular Interventions (EAPCI), the European Society of Cardiology (ESC), and the European Association for Cardio-Thoracic Surgery (EACTS) recently introduced standardized criteria to define structural valve deterioration (SVD) and valve failure of transcatheter and surgical aortic bioprosthesis—this with the aim to generate uniformity in data reporting in future studies assessing long-term durability of aortic bioprosthesis. On this background, the aim of this article is to review the definition, incidence and predictors of transcatheter bioprosthetic valve dysfunction, including structural and non-structural valve deterioration (SVD/NSVD), valve thrombosis, and endocarditis.
The clinical impact of transcatheter aortic valve replacement (TAVR) has been important by addressing the need for a therapeutic treatment in selected inoperable patients with symptomatic severe aortic stenosis (AS), but also as an alternative to surgical aortic valve replacement (SAVR) in patients at increased surgical risk. Based on large randomized controlled trials (RCTs) comparing TAVR to SAVR in patients with severe AS and intermediate or lower surgical risk (1–3), both the guidelines from the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) as well as the guidelines from the American Heart Association (AHA) and American College of Cardiology (ACC) were updated in 2017, upgrading the indication for TAVR to patients with symptomatic severe AS and intermediate surgical risk (4–6). Within the past decade, national registries have reported a steady growth in the annual number of TAVR procedures performed (7–10) and a decrease in the mean age of patients undergoing TAVR (8). The anticipation of treating AS patients with a longer life expectancy by means of TAVR has intensified the concerns about the durability of transcatheter heart valves (THVs).
Recently, two randomized clinical trials including patients with low surgical risk were presented. The Evolut Low Risk trial reported that TAVR with a self-expanding THV was non-inferior to SAVR with regard to all-cause mortality or disabling stroke within 2 years of the procedure (11). The PARTNER 3 trial reported that TAVR with a balloon-expandable THV was superior to SAVR with regard to the 1-year risk of all-cause mortality, stroke, or re-hospitalization (12). The mean age in both trials was 74 years of age. Considering these results, it is likely that the indication for TAVR will not only expand to patients with lower surgical risk but also to patients at younger age than currently treated by TAVR. Consequently, with the increased life expectancy of these patients, it is more likely that they will outlive their implanted THV. There are only few data regarding long-term THV durability. Assessment of valve function in the early randomized TAVR trials and registries have consistently shown preserved valve function up to 5 years after TAVR (13, 14). However, it is well-documented that valve degeneration with surgical aortic bioprostheses is usually not seen until 5–10 years post-procedure (15).
The aim of this article is to review the definition, incidence and predictors of transcatheter bioprosthetic aortic valve dysfunction, including structural and non-structural valve deterioration (SVD/NSVD), valve thrombosis, and endocarditis (Figure 1).
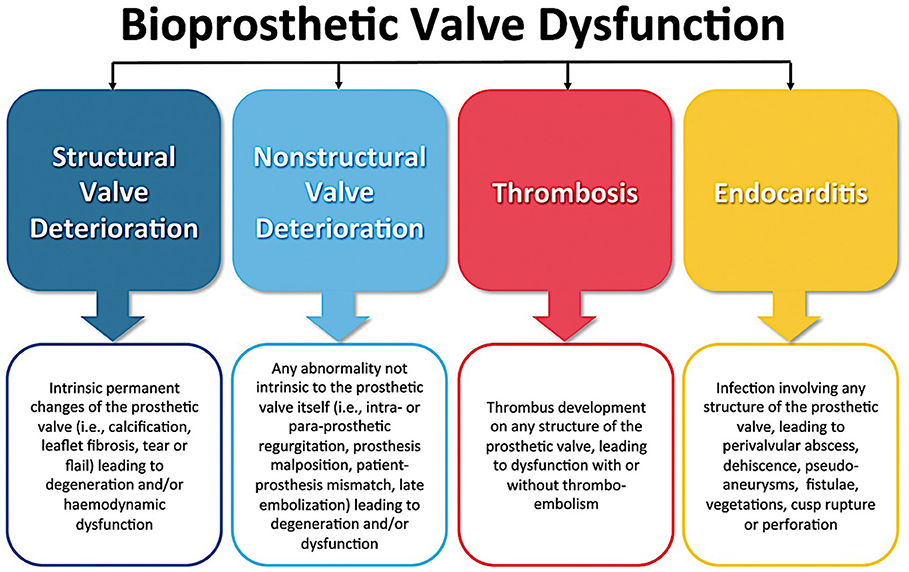
Figure 1. Causes of bioprosthetic valve dysfunction. Figure used with permission from Oxford University Press (16).
The durability of surgical aortic bioprosthesis has been more extensively described compared with THVs, mainly due to SAVR being performed for a longer time. However, previous studies reporting on surgical heart valves have tended to use the need for re-intervention as a clinical endpoint for SVD (17–20)—resulting in a risk of under-estimating the incidence of SVD as some patients might have become too frail over time to undergo redo-SAVR, even though the surgical aortic bioprosthesis might have been deteriorated (20, 21). Some echocardiographic criteria for defining SVD have been applied in individual studies (22); however, the lack of a consensus definition for SVD limits the possibility for comparison across studies.
Efforts have been made to standardize the definition of SVD for both transcatheter and surgical bioprostheses. Building on existing definitions for SVD, a consensus statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI)—endorsed by the ESC and the EACTS—was published in 2017 (16). SVD was classified into either morphological or moderate and severe hemodynamic SVD based on the severity of THV stenosis and/or regurgitation (16). The VIVID (Valve in Valve International Data) group published a similar but more staged classification for SVD, Table 1 (22).
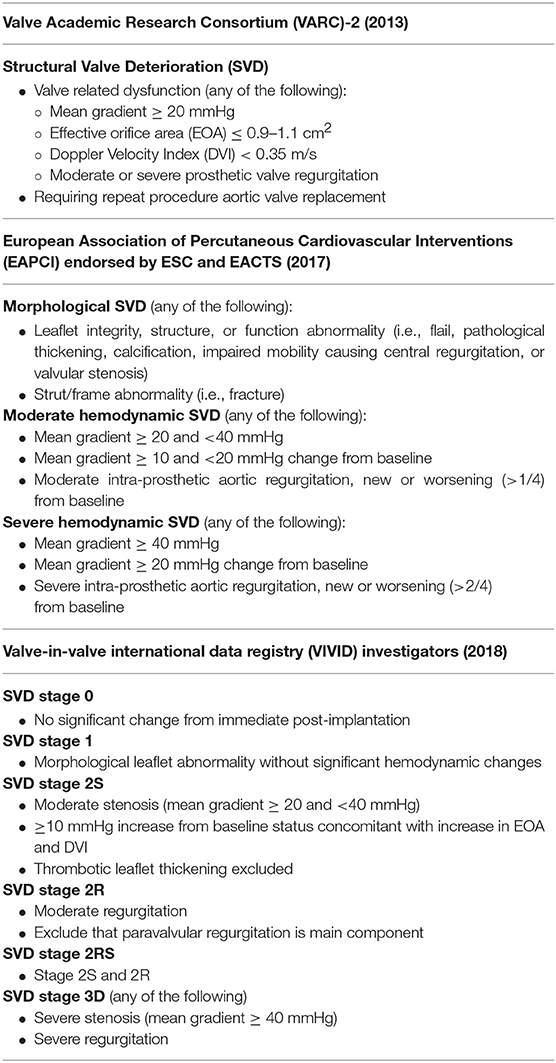
Table 1. Proposed definitions of structural valve deterioration (SVD).
SVD is commonly defined as an intrinsic permanent change of the bioprosthesis due to leaflet calcification, thickening, pannus formation, tear, or disruption. The resulting deterioration leads to stenosis and/or intra-prosthetic regurgitation (16, 21–23).
A study including 2,659 patients undergoing SAVR reported that the time to deterioration of surgical bioprostheses was similar regardless of stenotic and/or regurgitation etiology (21). Further, younger age was found as a significant risk factor for early SVD (17, 21). The increased risk of SVD in younger patients is thought to be mediated by a higher metabolic rate and a stronger immunological response to the implanted bioprosthetic heart valve (19). Other factors that have been found to increase the risk of SVD of aortic bioprostheses are patient-prosthesis mismatch (PPM), dialysis, hyperparathyroidism, and diabetes (17, 19, 24, 25).
In addition, it has been hypothesized that several risk factors of SVD might specifically apply to THVs. The need to crimp the THV into a delivery catheter may theoretically damage the bioprosthetic leaflet tissue, thereby impairing THV durability (26). During TAVR, it is not aimed to align the commissures of the THV to those of the native aortic valve, and commissural misalignment might increase the stress on the leaflets and has been reported to increase the risk of mild intra-prosthetic regurgitation (27). Lastly, there is no data on the impact of elliptical THV geometry due to calcified native aortic annulus or incomplete expansion of the THV due to oversizing.
So far, there is only limited data available on long-term durability of THVs, as those patients treated by TAVR in the early years of the procedure were typically elderly and frail patients. Consequently, the expected and observed medium-term survival rate of these initially treated TAVR-patients is relatively low, Table 2. As abovementioned, age also likely plays a crucial inverse role in the rate of SVD. This further limits the possibility to predict the rate of SVD based on the currently treated patients whom are likely older than the future TAVR patients.
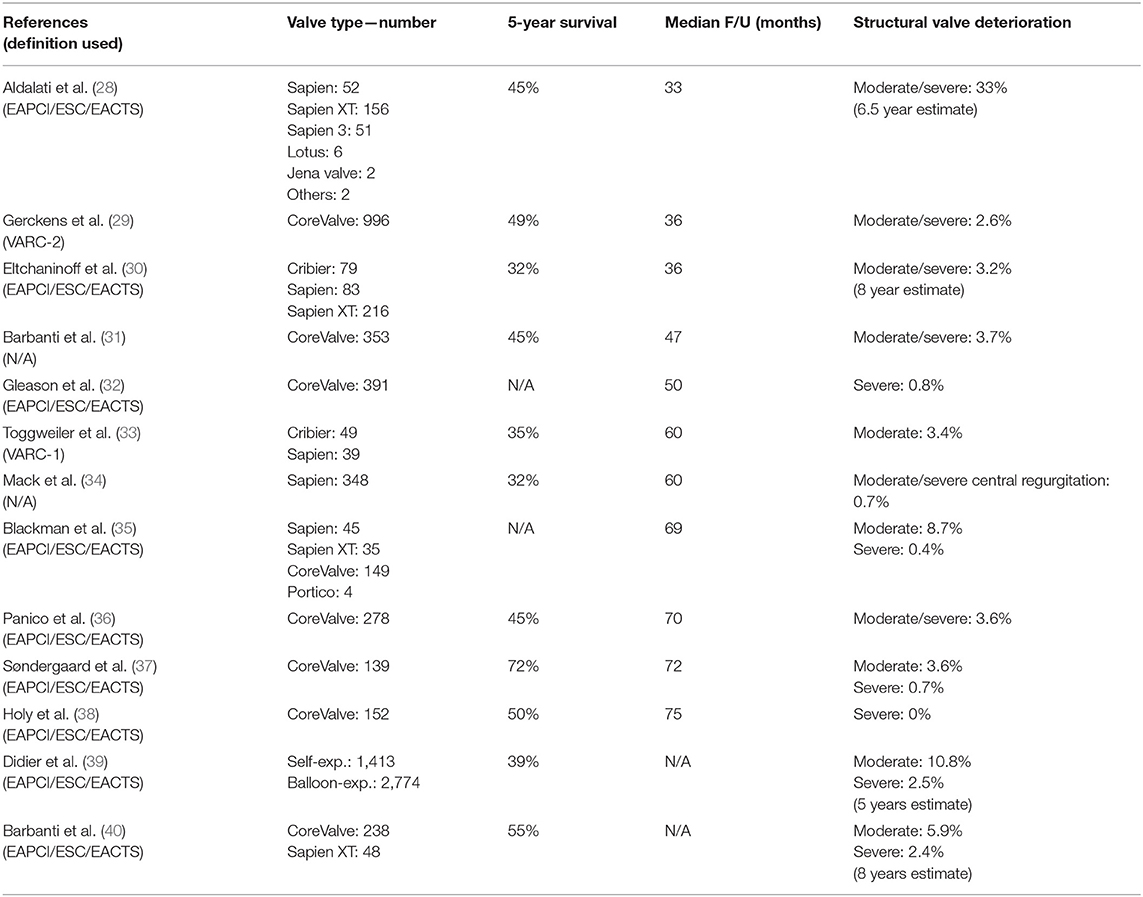
Table 2. Incidence of structural valve deterioration of transcatheter heart valves.
Only few data exist on controlled comparison of SVD between surgical and transcatheter aortic bioprosthesis. In general, these studies find the medium-long term risk of severe SVD to be low, ranging between 0 and 2.5% in studies with 4–8 years of follow-up (32, 35, 37–40). In the PARTNER-1 trial, there was no SVD reported at 5 years—although only 15 patients remained alive (13). In the CoreValve High Risk Pivotal trial, severe SVD was noted in 1.7% and 0.8% of patients at 5 years after SAVR and TAVR (p = 0.32), respectively (32). The standardized criteria of SVD from EAPCI/ESC/EACTS were recently also applied to the NOTION trial—a RCT randomizing AS patients at lower surgical risk to SAVR or TAVR. This patient population had a lower mortality rate as compared to contemporary RCTs in high-to-intermediate risk patients. The risk of SVD through 6 years for surgical and transcatheter bioprostheses was 24.0 and 4.8% (p < 0.0001), respectively (37). This difference was mainly driven by moderate SVD in the SAVR group and severe SVD was observed in 3.0% vs. 0.7% in the SAVR vs. TAVR group, respectively (p = 0.21) (37).
Non-SVD is a bioprosthetic abnormality due to extrinsic factors such as PPM, paravalvular regurgitation (PVR), device malpositioning, or abnormal frame expansion. The presence of non-SVD is not an intrinsic deterioration of the bioprosthesis or leaflets—however, it might mediate early development of SVD (16, 22, 41).
Following SAVR, the prevalence of moderate PPM ranges from 20 to 70% and that of severe PPM from 2 to 20% (42, 43). TAVI is associated with a lower prevalence of (especially severe) PPM as compared to SAVR (44, 45). Among THVs, self-expanding valves with supra-annular design are generally associated with a lower prevalence of PPM as compared with balloon-expandable valves. Patients with PPM have worse symptoms and exercise capacity, higher rate of heart failure re-hospitalization, and increased mortality after SAVR as compared with patients with no PPM (42, 46). PPM is also associated with quicker structural degeneration of surgical aortic bioprostheses (24, 47). Consequently, TAVR could be the preferred choice of treatment for patients with a small annulus (valve size < 23 mm) in whom PPM can be anticipated in case of SAVR.
On the contrary, THVs more frequently have PVR. However, with the newer generation THVs—with often an additional sealing skirt around the valve prosthesis stent frame—these PVR rates have come down to a range of 1–3% for moderate PVR and 29–36% for mild PVR in the latest low-risk TAVR trials (11, 12). The impact of mild PVR on left ventricular function, symptoms, and long-term mortality in lower risk patients with longer life expectancy is still unknown—however, data from the PARTNER-1 trial have suggested decrease survival in this subset (13).
Finally, whether abnormal stent frame expansion—as sometimes observed in case of THV in heavily calcified or bicuspid valves—has a negative impact on valve durability is unknown. In an ex-vivo bench study by Sathananthan et al., it was shown that excessive THV overexpansion may be associated with impaired hydrodynamic function, acute leaflet failure, and reduced durability. Smaller valves may be at greater risk with overexpansion than larger valves. Similar, THV undersizing can cause leaflet pin wheeling and reduced durability (48).
In conclusion, future TAVR studies including patients with longer life expectancy and bicuspid valve anatomy are needed to answer these remaining open questions.
Clinical valve thrombosis after TAVR typically presents with an increase of transvalvular gradient and symptoms of heart failure caused by obstructing thrombus in the THV. On the other hand, subclinical leaflet thrombosis is an incidental finding on 4DCT or TEE imaging, which does not cause symptoms or elevated transvalvular pressure gradients outside the normal range.
In a study by Bourguignon et al. (21) with long-term follow-up data on 2,659 Carpentier-Edwards Perimount valves in the aortic position, no single case of clinical valve thrombosis was reported with a median follow-up of 6.7 years (21). In accordance, there was no clinical valve thrombosis observed in the NOTION lower-risk trial—neither in the TAVR nor in the SAVR population—with a follow-up of up to 6 years (37). In two retrospective analyses, the prevalence of clinical valve thrombosis was reported to be 0.6 and 2.8% after TAVR (49, 50), whereas the prevalence of subclinical leaflet thrombosis has been reported to be as high as 15–35% in studies assessing this phenomenon by means of TEE and/or 4DCT cardiac imaging (51–53).
Although usually an incidental finding, there has been a concern that subclinical leaflet thrombosis may progress into clinical valve thrombosis, cause stroke or other thromboembolic events, and/or impair the durability of the THV.
Reports on a potential association between subclinical leaflet thrombosis and stroke/transient ischemic attack (TIA) have raised concerns. In the SAVORY and RESOLVE registries, subclinical leaflet thrombosis with reduced leaflet motion was associated with increased incidence of TIA (53). In contrast, a prospective trial—including 4DCT or echocardiography in 434 patients that underwent TAVR—did not show any increased stroke risk at 3 years of follow-up in those patients diagnosed with (possible) subclinical leaflet thrombosis (54). One meta-analysis, although involving a limited number of retrospective studies, also reported an overall odds ratio of 3.38 (95% CI: 1.78–6.41, P < 0.001) for cerebrovascular events in case of hypo-attenuation affecting motion (HAM) as compared with hypo-attenuation affecting leaflet thickening (HALT) only—thereby suggesting an impact of “thrombus burden” on the risk for neurological events (55). However, it should be kept in mind that all these reports are based on retrospective data and often there is a very long temporal separation between the neurological event and the cardiac imaging showing subclinical leaflet thrombosis.
Anticoagulation seems to be preventive for development of both clinical valve thrombosis and subclinical leaflet thrombosis, whereas single or dual APT does not have this protective effect. In accordance, treatment with anticoagulation seems to have—at least temporarily—beneficial effects on restoration of leaflet motion and transvalvular gradients in case of THV thrombosis (50, 51, 56) (Figure 2). In addition, Del Trigo et al. reported that absence of anticoagulant therapy at hospital discharge was an independent predictor of hemodynamic valve deterioration after TAVR (57).
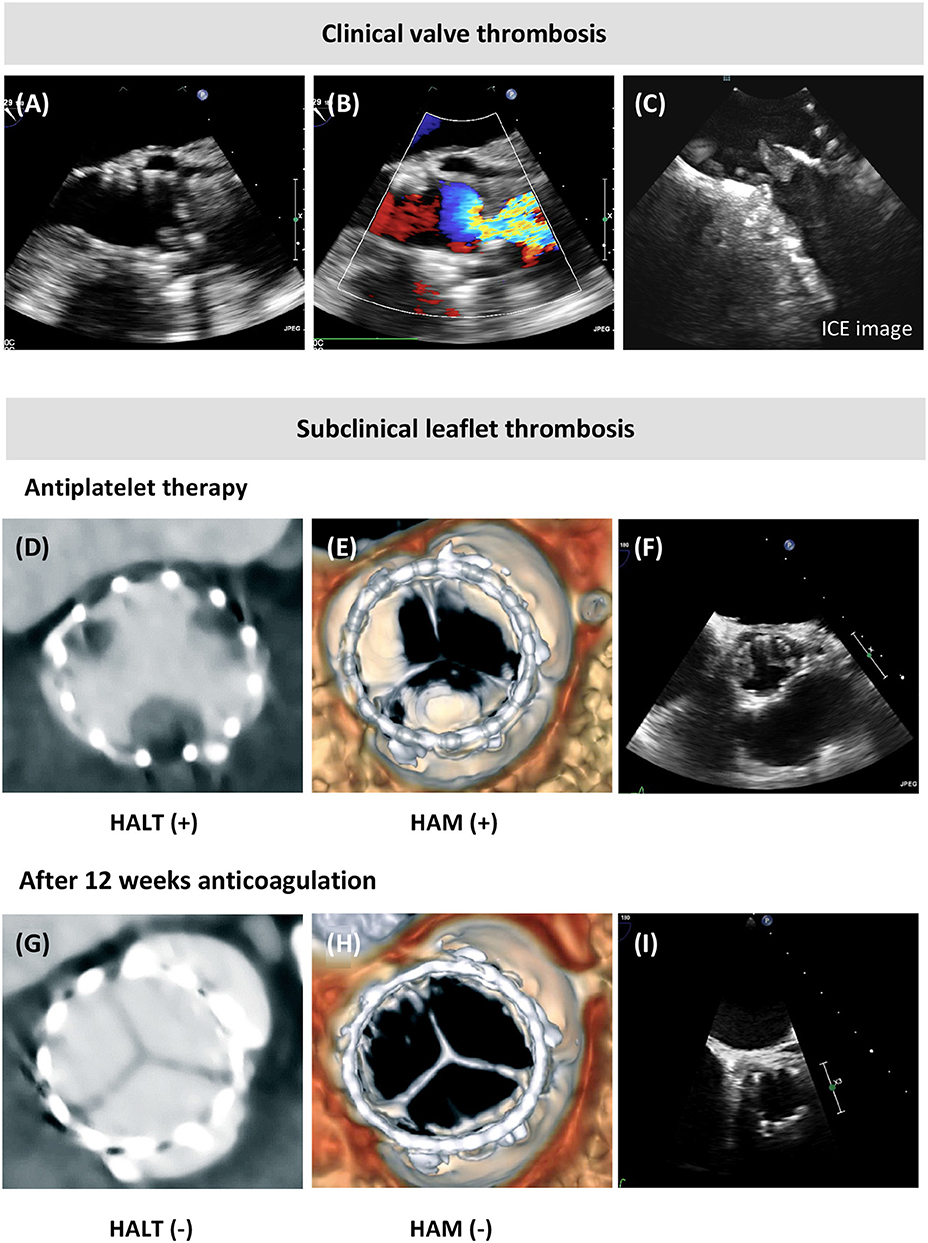
Figure 2. Clinical valve thrombosis and subclinical leaflet thrombosis. (A,B) Transesophageal echocardiography (TEE) showing valve thrombosis and turbulent color flow over the transcatheter aortic bioprosthesis in a patient presenting with an elevated mean transvalvular gradient at transthoracic echocardiography (TTE, 37 mmHg) and dyspnea NYHA class 3–4, and this few years after TAVR. (C) The thrombotic mass at the aortic side of the prosthetic leaflets was confirmed by intracardiac echocardiography (ICE). (D,E) Incidental finding of hypoattenuating leaflet thickening (HALT) at the base of the transcatheter heart valve leaflets, with hypoattenuation affecting motion (HAM) visible in systole in the volume-rendered 4D computed tomography (4DCT) images; (F) this reduced leaflet motion of two leaflets was confirmed by TEE. (G–I) Resolution of the leaflet thickening and reduced leaflet motion following 3 months of anticoagulation treatment, as shown by 4DCT and TEE imaging.
Finally, although subclinical leaflet thrombosis seems to be more common after TAVR as compared with SAVR, medium-term durability of THVs has been reported to be non-inferior to surgical aortic bioprosthesis in several large randomized trials (32, 34). Whether, subclinical leaflet thrombosis may be a precursor and/or predictor of valve dysfunction on the longer-term is unknown. Long-term follow-up data on THV and surgical bioprosthesis—including leaflet-imaging studies—will be needed in order to give an answer to this question.
Another important reversible mechanism of non-SVD is the development of valve failure due to infective endocarditis. In the NOTION lower-risk trial, the risk of infective endocarditis was similar after SAVR (5.9%) as compared to TAVR (5.8%) after 6 years of follow-up (37). In accordance, Butt et al. (58) recently reported long-term follow-up data from a Danish nationwide observational study comprising 2,632 TAVR patients and 3,777 matched SAVR patients. During a mean follow-up of 3.6 years, 115 patients (4.4%) with TAVR and 186 patients (4.9%) with SAVR were admitted with infective endocarditis. The median time from procedure to infective endocarditis hospitalization was 352 days in the TAVR group and 625 days in the SAVR group. The cumulative 5-year risk of infective endocarditis was 5.8% and 5.1% in the TAVR and SAVR population, respectively—hence, the long-term risk of infective endocarditis was similar following TAVR and SAVR (58).
In a large collaborative study, a total of 250 cases of infective endocarditis occurred in 20,006 patients after TAVR (incidence, 1.1% per person-year; 95% CI, 1.1–1.4%; median age, 80 years; 64% men). Median time from TAVR to infective endocarditis was 5.3 months [interquartile range (IQR), 1.5–13.4 months]. The characteristics associated with higher risk of progressing to infective endocarditis after TAVR was younger age [78.9 years vs. 81.8 years; hazard ratio (HR), 0.97 per year], male sex (62.0% vs. 49.7%; HR, 1.69), diabetes mellitus (41.7% vs. 30.0%; HR, 1.52), and moderate to severe aortic regurgitation (22.4% vs. 14.7%; HR, 2.05). Patients who developed endocarditis had high rates of in-hospital mortality (36%) and 2-year mortality (66.7%) (59).
The same prophylactic measurements to prevent infective endocarditis have to be implemented following AVR with a surgical or transcatheter aortic bioprosthesis. In case of suspicion of prosthetic valve endocarditis in a TAVR patient, the diagnosis with TEE may sometimes be challenging—in such cases, use of intracardiac echocardiography (ICE) and PET-CT could be considered (58, 60). In case of prosthetic valve endocarditis following TAVR, the therapeutic options are most of the time limited to antibiotic medical treatment. Limited data from the Copenhagen group indicate that such conservative approach is associated with a 22% mortality rate. As reported by Olsen et al. (60), 17 out of 18 TAVR patients with infective endocarditis were treated conservatively and one with surgery. Four patients (22%) died from endocarditis or complications to treatment, two of those (11%) during initial hospitalization for prosthetic valve endocarditis (60).
With the expansion of TAVR to patients with longer life expectancy, data on long-term THV durability are essential. The first studies reporting on SVD up to 8 years after TAVR show low rates of THV degeneration. Importantly, the release of standardized definitions on bioprosthetic valve dysfunction represents a fundamental step in allowing obtaining a better insight into its real incidence.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, et al. Transcatheter or surgical aortic-valve replacement in intermediate-risk patients. N Engl J Med. (2016) 374:1609–20. doi: 10.1056/NEJMoa1514616
2. Reardon MJ, Van Mieghem NM, Popma JJ, Kleiman NS, Søndergaard L, Mumtaz M, et al. Surgical or transcatheter aortic-valve replacement in intermediate-risk patients. N Engl J Med. (2017) 376:1321–31. doi: 10.1056/NEJMoa1700456
3. Thyregod HGH. Five-Year Outcomes From the All-Comers Nordic Aortic Valve Intervention Randomized Clinical Trial in Patients with Severe Aortic Valve Stenosis. Orlando, FL: ACC (2018).
4. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, et al. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. (2017) 38:2739–91. doi: 10.1093/eurheartj/ehx391
5. Barbanti M, Webb J, Gilard M, Capodanno D, Tamburino C. Transcatheter aortic valve implantation in 2017: state of the art. EuroIntervention. (2017) 13:AA11–21. doi: 10.4244/EIJ-D-17-00567
6. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Fleisher LA, et al. 2017 AHA/ACC focused update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Circulation. (2017) 135:e1159–95. doi: 10.1161/CIR.0000000000000503
7. De Backer O, Bieliauskas G, Søndergaard L. Current status and future perspectives for transcatheter and surgical aortic valve replacement: the role of aortic valve surgery in the era of transcatheter-based therapies. EuroIntervention. (2018) 14:e965–7. doi: 10.4244/EIJV14I9A172
8. Grover FL, Vemulapalli S, Carroll JD, Edwards FH, Mack MJ, Thourani VH, et al. 2016 annual report of the society of thoracic surgeons/American college of cardiology transcatheter valve therapy registry. J Am Coll Cardiol. (2017) 69:1215–30. doi: 10.1016/j.jacc.2016.11.033
9. Auffret V, Lefevre T, Van Belle E, Eltchaninoff H, Iung B, Koning R, et al. Temporal trends in transcatheter aortic valve replacement in France. J Am Coll Cardiol. (2017) 70:42–55. doi: 10.1016/j.jacc.2017.04.053
10. Gaede L, Blumenstein J, Liebetrau C, Dörr O, Kim W-K, Nef H, et al. Outcome after transvascular transcatheter aortic valve implantation in 2016. Eur Heart J. (2018) 39:667–75. doi: 10.1093/eurheartj/ehx688
11. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O'Hair D, et al. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N Engl J Med. (2019) 380:1706–15. doi: 10.1056/NEJMoa1816885
12. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med. (2019) 380:1695–705. doi: 10.1056/NEJMoa1814052
13. Kapadia SR, Leon MB, Makkar RR, Tuzcu EM, Svensson LG, Kodali S, et al. 5-year outcomes of transcatheter aortic valve replacement compared with standard treatment for patients with inoperable aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. (2015) 385:2485–91. doi: 10.1016/S0140-6736(15)60290-2
14. Sawaya F, Kappetein AP, Wisser W, Nataf P, Thomas M, Schächinger V, et al. Five-year haemodynamic outcomes of the first-generation SAPIEN balloon-expandable transcatheter heart valve. EuroIntervention. (2016) 12:775–82. doi: 10.4244/EIJV12I6A126
15. Puri R, Auffret V, Rodés-Cabau J. Bioprosthetic valve thrombosis. J Am Coll Cardiol. (2017) 69:2193–211. doi: 10.1016/j.jacc.2017.02.051
16. Capodanno D, Petronio AS, Prendergast B, Eltchaninoff H, Vahanian A, Modine T, et al. Standardized definitions of structural deterioration and valve failure in assessing long-term durability of transcatheter and surgical aortic bioprosthetic valves: a consensus statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI) endorsed by the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. (2017) 38:3382–90. doi: 10.1093/eurheartj/ehx303
17. Johnston DR, Soltesz EG, Vakil N, Rajeswaran J, Roselli EE, Sabik JF, et al. Long-term durability of bioprosthetic aortic valves: implications from 12,569 implants. Ann Thorac Surg. (2015) 99:1239–47. doi: 10.1016/j.athoracsur.2014.10.070
18. Salaun E, Clavel M-A, Rodés-Cabau J, Pibarot P. Bioprosthetic aortic valve durability in the era of transcatheter aortic valve implantation. Heart. (2018) 104:1323–32. doi: 10.1136/heartjnl-2017-311582
19. Côté N, Pibarot P, Clavel M-A. Incidence, risk factors, clinical impact, and management of bioprosthesis structural valve degeneration. Curr Opin Cardiol. (2017) 32:123–9. doi: 10.1097/HCO.0000000000000372
20. Rodriguez-Gabella T, Voisine P, Puri R, Pibarot P, Rodés-Cabau J. Aortic bioprosthetic valve durability. J Am Coll Cardiol. (2017) 70:1013–28. doi: 10.1016/j.jacc.2017.07.715
21. Bourguignon T, Bouquiaux-Stablo A-L, Candolfi P, Mirza A, Loardi C, May M-A, et al. Very long-term outcomes of the carpentier-edwards perimount valve in aortic position. Ann Thorac Surg. (2015) 99:831–7. doi: 10.1016/j.athoracsur.2014.09.030
22. Dvir D, Bourguignon T, Otto CM, Hahn RT, Rosenhek R, Webb JG, et al. Standardized definition of structural valve degeneration for surgical and transcatheter bioprosthetic aortic valves. Circulation. (2018) 137:388–99. doi: 10.1161/CIRCULATIONAHA.117.030729
23. Dvir D, Webb JG, Bleiziffer S, Pasic M, Waksman R, Kodali S, et al. Transcatheter aortic valve implantation in failed bioprosthetic surgical valves. JAMA. (2014) 312:162. doi: 10.1001/jama.2014.7246
24. Flameng W, Herregods MC, Vercalsteren M, Herijgers P, Bogaerts K, Meuris B. Prosthesis-patient mismatch predicts structural valve degeneration in bioprosthetic heart valves. Circulation. (2010) 121:2123–9. doi: 10.1161/CIRCULATIONAHA.109.901272
25. Okada N, Tajima K, Takami Y, Kato W, Fujii K, Hibino M, et al. Valve selection for the aortic position in dialysis patients. Ann Thorac Surg. (2015) 99:1524–31. doi: 10.1016/j.athoracsur.2014.11.055
26. Alavi SH, Groves EM, Kheradvar A. The effects of transcatheter valve crimping on pericardial leaflets. Ann Thorac Surg. (2014) 97:1260–6. doi: 10.1016/j.athoracsur.2013.11.009
27. Fuchs A, Kofoed KF, Yoon S-H, Schaffner Y, Bieliauskas G, Thyregod HG, et al. Commissural alignment of bioprosthetic aortic valve and native aortic valve following surgical and transcatheter aortic valve replacement and its impact on valvular function and coronary filling. JACC Cardiovasc Interv. (2018) 11:1733–43. doi: 10.1016/j.jcin.2018.05.043
28. Aldalati O, Kaura A, Khan H, Dworakowski R, Byrne J, Eskandari M, et al. Bioprosthetic structural valve deterioration: how do TAVR and SAVR prostheses compare? Int J Cardiol. (2018) 268:170–5. doi: 10.1016/j.ijcard.2018.04.091
29. Gerckens U, Tamburino C, Bleiziffer S, Bosmans J, Wenaweser P, Brecker S, et al. Final 5-year clinical and echocardiographic results for treatment of severe aortic stenosis with a self-expanding bioprosthesis from the ADVANCE Study. Eur Heart J. (2017) 38:2729–38. doi: 10.1093/eurheartj/ehx295
30. Eltchaninoff H, Durand E, Avinée G, Tron C, Litzler P-Y, Bauer F, et al. Assessment of structural valve deterioration of transcatheter aortic bioprosthetic balloon-expandable valves using the new European consensus definition. EuroIntervention. (2018) 14:e264–71. doi: 10.4244/EIJ-D-18-00015
31. Barbanti M, Petronio AS, Ettori F, Latib A, Bedogni F, De Marco F, et al. 5-year outcomes after transcatheter aortic valve implantation with corevalve prosthesis. JACC Cardiovasc Interv. (2015) 8:1084–91. doi: 10.1016/j.jcin.2015.03.024
32. Gleason TG, Reardon MJ, Popma JJ, Deeb GM, Yakubov SJ, Lee JS, et al. 5-year outcomes of self-expanding transcatheter versus surgical aortic valve replacement in high-risk patients. J Am Coll Cardiol. (2018) 72:2687–96. doi: 10.1016/j.jacc.2018.08.2146
33. Toggweiler S, Humphries KH, Lee M, Binder RK, Moss RR, Freeman M, et al. 5-year outcome after transcatheter aortic valve implantation. J Am Coll Cardiol. (2013) 61:413–9. doi: 10.1016/j.jacc.2012.11.010
34. Mack MJ, Leon MB, Smith CR, Miller DC, Moses JW, Tuzcu EM, et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. (2015) 385:2477–84. doi: 10.1016/S0140-6736(15)60308-7
35. Blackman DJ, Saraf S, MacCarthy PA, Myat A, Anderson SG, Malkin CJ, et al. Long-term durability of transcatheter aortic valve prostheses. J Am Coll Cardiol. (2019) 73:537–45. doi: 10.1016/j.jacc.2018.10.078
36. Panico RA, Giannini C, De Carlo M, Angelillis M, Spontoni P, Pieroni A, et al. Long-term results and durability of the CoreValve transcatheter aortic bioprosthesis: outcomes beyond five years. EuroIntervention. (2019) 14:1639–1647. doi: 10.4244/EIJ-D-18-00779
37. Søndergaard L, Ihlemann N, Capodanno D, Jørgensen TH, Nissen H, Kjeldsen BJ, et al. Durability of transcatheter and surgical bioprosthetic aortic valves in patients at lower surgical risk. J Am Coll Cardiol. (2019) 73:546–53. doi: 10.1016/j.jacc.2018.10.083
38. Holy EW, Kebernik J, Abdelghani M, Stämpfli SF, Hellermann J, Allali A, et al. Long-term durability and haemodynamic performance of a self-expanding transcatheter heart valve beyond five years after implantation: a prospective observational study applying the standardised definitions of structural deterioration and valve failure. EuroIntervention. (2018) 14:e390–6. doi: 10.4244/EIJ-D-18-00041
39. Didier R, Eltchaninoff H, Donzeau-Gouge P, Chevreul K, Fajadet J, Leprince P, et al. Five-year clinical outcome and valve durability after transcatheter aortic valve replacement in high-risk patients: FRANCE-2 registry. Circulation. (2018) 138:2597–607. doi: 10.1161/CIRCULATIONAHA.118.036866
40. Barbanti M, Costa G, Zappulla P, Todaro D, Picci A, Rapisarda G, et al. Incidence of long-term structural valve dysfunction and bioprosthetic valve failure after transcatheter aortic valve replacement. J Am Heart Assoc. (2018) 7:e008440. doi: 10.1161/JAHA.117.008440
41. Kataruka A, Otto CM. Valve durability after transcatheter aortic valve implantation. J Thorac Dis. (2018) 10:S3629–36. doi: 10.21037/jtd.2018.07.38
42. Fallon JM, DeSimone JP, Brennan JM, O'Brien S, Thibault DP, DiScipio AW, et al. The incidence and consequence of prosthesis-patient mismatch after surgical aortic valve replacement. Ann Thorac Surg. (2018) 106:14–22. doi: 10.1016/j.athoracsur.2018.01.090
43. Pibarot P, Weissman NJ, Stewart WJ, Hahn RT, Lindman BR, McAndrew T, et al. Incidence and sequelae of prosthesis-patient mismatch in transcatheter versus surgical valve replacement in high-risk patients with severe aortic stenosis. J Am Coll Cardiol. (2014) 64:1323–34. doi: 10.1016/j.jacc.2014.06.1195
44. Jilaihawi H, Chin D, Spyt T, Jeilan M, Vasa-Nicotera M, Bence J, et al. Prosthesis-patient mismatch after transcatheter aortic valve implantation with the Medtronic-Corevalve bioprosthesis. Eur Heart J. (2010) 31:857–64. doi: 10.1093/eurheartj/ehp537
45. Ewe SH, Muratori M, Delgado V, Pepi M, Tamborini G, Fusini L, et al. Hemodynamic and clinical impact of prosthesis–patient mismatch after transcatheter aortic valve implantation. J Am Coll Cardiol. (2011) 58:1910–8. doi: 10.1016/j.jacc.2011.08.027
46. Pibarot P. Prosthesis-patient mismatch: definition, clinical impact, and prevention. Heart. (2006) 92:1022–9. doi: 10.1136/hrt.2005.067363
47. Pibarot P, Simonato M, Barbanti M, Linke A, Kornowski R, Rudolph T, et al. Impact of pre-existing prosthesis-patient mismatch on survival following aortic valve-in-valve procedures. JACC Cardiovasc Interv. (2018) 11:133–41. doi: 10.1016/j.jcin.2017.08.039
48. Sathananthan J, Sellers S, Barlow A, Fraser R, Stanová V, Cheung A, et al. Overexpansion of the SAPIEN 3 transcatheter heart valve. JACC Cardiovasc Interv. (2018) 11:1696–705. doi: 10.1016/j.jcin.2018.06.027
49. Latib A, Naganuma T, Abdel-Wahab M, Danenberg H, Cota L, Barbanti M, et al. Treatment and clinical outcomes of transcatheter heart valve thrombosis. Circ Cardiovasc Interv. (2015) 8:e001779. doi: 10.1161/CIRCINTERVENTIONS.114.001779
50. Jose J, Sulimov DS, El-Mawardy M, Sato T, Allali A, Holy EW, et al. Clinical bioprosthetic heart valve thrombosis after transcatheter aortic valve replacement. JACC Cardiovasc Interv. (2017) 10:686–97. doi: 10.1016/j.jcin.2017.01.045
51. Makkar RR, Fontana G, Jilaihawi H, Chakravarty T, Kofoed KF, De Backer O, et al. Possible subclinical leaflet thrombosis in bioprosthetic aortic valves. N Engl J Med. (2015) 373:2015–24. doi: 10.1056/NEJMoa1509233
52. Leetmaa T, Hansson NC, Leipsic J, Jensen K, Poulsen SH, Andersen HR, et al. Early aortic transcatheter heart valve thrombosis: diagnostic value of contrast-enhanced multidetector computed tomography. Circ Cardiovasc Interv. (2015) 8:e001596. doi: 10.1161/CIRCINTERVENTIONS.114.001596
53. Chakravarty T, Søndergaard L, Friedman J, De Backer O, Berman D, Kofoed KF, et al. Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study. Lancet. (2017) 389:2383–92. doi: 10.1016/S0140-6736(17)30757-2
54. Vollema EM, Kong WKF, Katsanos S, Kamperidis V, van Rosendael PJ, van der Kley F, et al. Transcatheter aortic valve thrombosis: the relation between hypo-attenuated leaflet thickening, abnormal valve haemodynamics, and stroke. Eur Heart J. (2017) 38:1207–17. doi: 10.1093/eurheartj/ehx031
55. Rashid HN, Brown AJ, McCormick LM, Amiruddin AS, Be KK, Cameron JD, et al. Subclinical leaflet thrombosis in transcatheter aortic valve replacement detected by multidetector computed tomography — a review of current evidence. Circ J. (2018) 82:1735–42. doi: 10.1253/circj.CJ-17-1363
56. Fuchs A, De Backer O, Brooks M, de Knegt M, Bieliauskas G, Yamamoto M, et al. Subclinical leaflet thickening and stent frame geometry in self-expanding transcatheter heart valves. EuroIntervention. (2017) 13:e1067–75. doi: 10.4244/EIJ-D-17-00373
57. Del Trigo M, Muñoz-Garcia AJ, Wijeysundera HC, Nombela-Franco L, Cheema AN, Gutierrez E, et al. Incidence, timing, and predictors of valve hemodynamic deterioration after transcatheter aortic valve replacement. J Am Coll Cardiol. (2016) 67:644–55. doi: 10.1016/j.jacc.2015.10.097
58. Butt JH, Ihlemann N, Backer OD, Søndergaard L, Havers-Borgersen E, Gislason GH, et al. Long-term risk of infective endocarditis after transcatheter aortic valve replacement. J Am Coll Cardiol. (2019) 73:1646–55. doi: 10.1016/j.jacc.2018.12.078
59. Regueiro A, Linke A, Latib A, Ihlemann N, Urena M, Walther T, et al. Association between transcatheter aortic valve replacement and subsequent infective endocarditis and in-hospital death. JAMA. (2016) 316:1083–92. doi: 10.1001/jama.2016.12347
Keywords: aortic valve replacement, transcatheter, valve dysfunction, valve deterioration, thrombosis, endocarditis
Citation: Sawaya F, Jørgensen TH, Søndergaard L and De Backer O (2019) Transcatheter Bioprosthetic Aortic Valve Dysfunction: What We Know So Far. Front. Cardiovasc. Med. 6:145. doi: 10.3389/fcvm.2019.00145
Received: 22 June 2019; Accepted: 23 September 2019;
Published: 04 October 2019.
Edited by:
Chiara Fraccaro, University Hospital of Padua, ItalyReviewed by:
Pablo Codner, Rabin Medical Center, IsraelCopyright © 2019 Sawaya, Jørgensen, Søndergaard and De Backer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ole De Backer, b2xlLmRlYmFja2VyQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.