 Carlos Cédric Ahoyo1*
Carlos Cédric Ahoyo1* Kolawolé Valère Salako2
Kolawolé Valère Salako2 Thierry Dehouegnon Houéhanou3Immaculée Montcho1Romain Lucas Glèlè Kakaï2
Thierry Dehouegnon Houéhanou3Immaculée Montcho1Romain Lucas Glèlè Kakaï2 Marcel Romuald Benjamin Houinato1
Marcel Romuald Benjamin Houinato1- 1Laboratory of Applied Ecology, Faculty of Agronomic Sciences, University of Abomey-Calavi, Cotonou, Benin
- 2Laboratoire de Biomathématiques et d’Estimations Forestières, Faculté des Sciences Agronomiques, Université d’Abomey-Calavi, Cotonou, Benin
- 3Laboratory of Ecology, Botany and Plant Biology, Faculty of Agronomy, University of Parakou, Parakou, Benin
The sustainable management of open ecosystems requires the committed participation of the neighboring people. Attention should be given to plant species ecology, which conditions the rate of vegetation growth. Sociocultural and ecological factors contribute to both the loss and the conservation of fragile ecosystems. Owing to the importance of traditional medicine in Benin, a focus has been made on the selection of species in this field as a case study for highlighting the factors that drive the selection of plant species in Benin. Further inferences highlight the conservation status of the selected woodlands and savannas. The study assessed the effects of people’s sociodemographic status and species’ ecological parameters on the variation in people’s knowledge associated with species’ usefulness in traditional medicine in Benin. An ethnobotanical survey was conducted through semi-structured individual interviews with 590 specialists in traditional medicine. A conditional inference tree model was combined with a generalized linear model to determine the factors associated with traditional medicinal knowledge (TMK). It was found that TMK varied with informant ethnicity, source of knowledge, membership position, age, instruction level, and professional activity. As for the ecological and species accessibility factors, phytodistrict, mode of reproduction of the species, reasons for the species’ disappearance, availability, and conservation status influenced TMK. When combining the two categories of factors, phytodistrict, habitat of species conservation, source of knowledge, and membership position of the informants were highlighted as the principal factors that influenced TMK. These identified factors should be integrated into a comprehensive management plan for TMK conservation and biodiversity management, and the sustainable use of savanna resources. Through this, sustainable management of open ecosystems, resulting in biodiversity conservation, livelihood improvement, and climate change mitigation, will be achieved. Such a plan should be based on the mix of ethnicities and the diversity of the species’ habitat in each phytodistrict.
1 Introduction
Plants hold an important place in human life, considering their numerous uses in food, medicine, culture, agroforestry, and technology (Goussanou et al., 2011; Mangambu et al., 2012). In developing countries, alongside agriculture, breeding animals, and fishing, the harvesting of non-woody forest products is an important income source for rural communities (Salhi et al., 2010; Allabi et al., 2011; Aniruddha and Ghosh, 2011). In developing countries, 22%–28% of household income comes from forests (Pouliot and Treue, 2013; Angelsen et al., 2014). Traditional medicine, i.e., the consumption of plants with little or no processing for the purpose of wellbeing, is of great importance in such countries. According to the World Health Organization (WHO), an estimated 3.5 billion people in such countries depend on medicinal plants as part of their primary healthcare (Balick and Cox, 1996). Thus, plants can be viewed as cultural and economic markers of human history (Kamari et al., 2009; Chibembe et al., 2015). For centuries, breeders and healers have accumulated ethnobotanical knowledge to take care of themselves and their animals. They use plants to treat pains and injuries (Benkhnigue et al., 2011). This knowledge has been orally transmitted through society and remains a specific social group patrimony (Tamboura et al., 1998). Each community has its own traditional medicine. Today, the transmission of endogenous knowledge is threatened by globalization, modernization, and market integration (Aswani et al., 2018). This knowledge is also being eroded by the decline of custodians of indigenous knowledge and the lack of interest from the younger generation in this knowledge (Brouwer et al., 2005). The gradual loss of traditional medicinal knowledge has intensified the harvesting of plants, thus threatening them (Tuttolomondo et al., 2014). Worldwide, sociocultural factors have been shown to influence traditional medicinal plant knowledge (Dapar et al., 2020). Indeed, the societal gaps caused by these factors may result in the disappearance of traditional knowledge and practices.
In Benin, some studies have shown that age is among the sociocultural factors that positively influence traditional knowledge (Assogbadjo et al., 2011; Gouwakinnou et al., 2011). Some studies report that a person’s knowledge peaks in their sixties (a curve with its maximum during a person’s sixties) (Kang et al., 2013). In contrast, other studies (e.g. Dassou, 2014) have reported a negative influence of age, indicating that the sociocultural factors contributing to traditional knowledge conservation may vary depending on context. Profession and sex were also found to have a significant effect on local people’s knowledge about plant use, and no significant effects were found for income level, education, and residency status (Byg and Balslev, 2004).
In general, ethnobotanical knowledge is influenced by sociocultural and ecological factors. Concerning sociocultural factors, the main factors highlighted in studies are ethnicity, age, sex, religion, instruction level, geographic position, and profession (Houehanou et al., 2011; Beltrán-Rodríguez et al., 2014; Ahoyo et al., 2018). Sociodemographic attributes are often correlated to local knowledge of plants’ uses (Albuquerque et al., 2011; Hanazaki et al., 2013; Gaoué et al., 2017). On the other hand, the plants used by a community also depend on some biological (e.g., specific medicinal properties) and ecological (e.g., growth forms) factors (Akerreta et al., 2007). The most accessible and available plants seem to be better known and hence used more frequently (Nzuki, 2016). The availability hypothesis states that plants are used for medicine owing to their greater accessibility or local abundance (Voeks, 2004; Albuquerque, 2006). “Availability” can include the physical distance from a home or community to the location where the plant grows in the wild, its seasonality, abundance, and price, and access to markets, gardens, or natural areas where the plant is found (Albuquerque, 2006; Estomba et al., 2006). The resource-use behavior by local people is often ecologically driven, based on the abundance of resources (Low, 1996). Ecological disturbances are influenced by climate variation (Jhariya and Yadav, 2018). Looking at this through an ecological stoichiometry lens, some researchers (Van de Waal et al., 2018) propose that humans tend to select the highly qualitative plants that could be the easiest to find. Therefore, a plant’s versatility and usefulness increase the threat to it, and this problem is worsening owing to the delayed growth of plants. The vegetation patches in Benin, comprising woodlands and savannas, are currently facing severe upheavals from global changes and the factors cited above. Traditional medicine is a wide field for the evidence of anthropogenic pressure on species in Africa, hence sharpening the vegetation patches.
To better understand the relationship between humans and plants in traditional medicine, researchers have developed a quantitative approach for such ethnopharmacological study, measuring values and indices to quantify the relationship (Reyes-García et al., 2006; Tardio and Pardo-de-Santayana, 2008; Bussmann et al., 2016).
In this context, this paper assessed the importance of species’ usefulness and ecology in their selection for traditional medicine. People’s sociodemographic factors and environmental factors were linked to traditional medicinal knowledge (TMK). Specifically, the study addresses the following questions:
-What are the sociodemographic and ecological factors that influence TMK in Benin?
-Does species accessibility increase ethnomedicinal use?
Owing to the importance of traditional medicine in Benin for people’s wellbeing (both in terms of health and income generation), this study focuses on plants used in traditional medicine. Further inferences highlight the conservation status of the selected woodlands and savannas.
2 Materials and methods
2.1 Study area
The study was carried out in Benin, which is located between 6°30′N and 12°30′N and 1°′E and 3°40′E and covers 114,763 km². The human population is about 12,909,041, of which 51.2% are women. This population’s annual growth rate is 3.5% [National Institute of Statistics and Economic Analysis (INSAE, 2016), 2016]. The annual rainfall ranges from 900 mm to 1,300 mm, forming three climatic zones (Guineo-Congolese, Sudano-Guinean, and Sudanian) split into 10 phytogeographical districts (Figure 1). The phytodistricts correspond to the smallest floristic and climatic units encountered in each climatic zone (Adomou, 2005; Adomou et al., 2011). Each climatic zone has a human population comprising multiple ethnicities, and each of them holds several specifics habits. In rural areas, where farming is the primary activity, modern healthcare services are lacking and plant species are mostly used to treat diseases. Indigenous people use traditional medicine knowledge (TMK) to maintain their health systems. TMK has been crucial for centuries and is at present because many people in African rural communities have limited access to modern medicines, owing to their high cost and the increasing circulation of fake drugs in Africa (Klein, 2019; Vorrath and Voss, 2019). The knowledge of medicinal plant uses and practices seems greater among the older generations than the younger generations. Indeed, ethnomedicinal knowledge often increases with age, and the elders have more accumulated indigenous knowledge of medicinal plants than the younger generation (Abebe and Teferi, 2021).
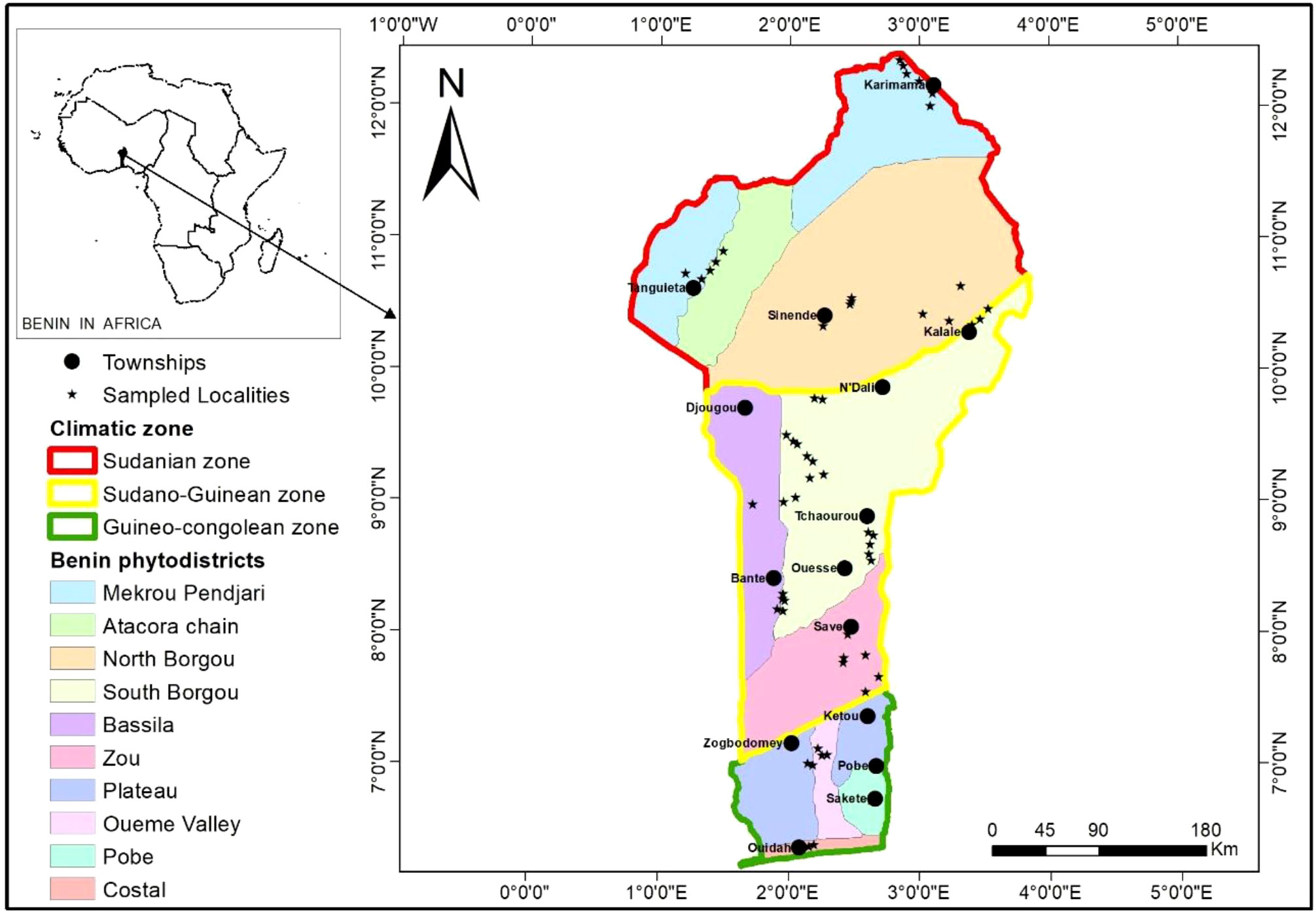
Figure 1 Situation map of the study area.
2.2 Sampling and data collection
A total of 590 informants ranging from 22 to 96 years old were interviewed, 11% of whom were women. The data collection focused on the sociodemographic characteristics of informants as well as ecological factors. The sociodemographic characteristics recorded comprised sex, ethnicity, age, level of education, marital status, household status, knowledge source, and primary activity (Table 1).
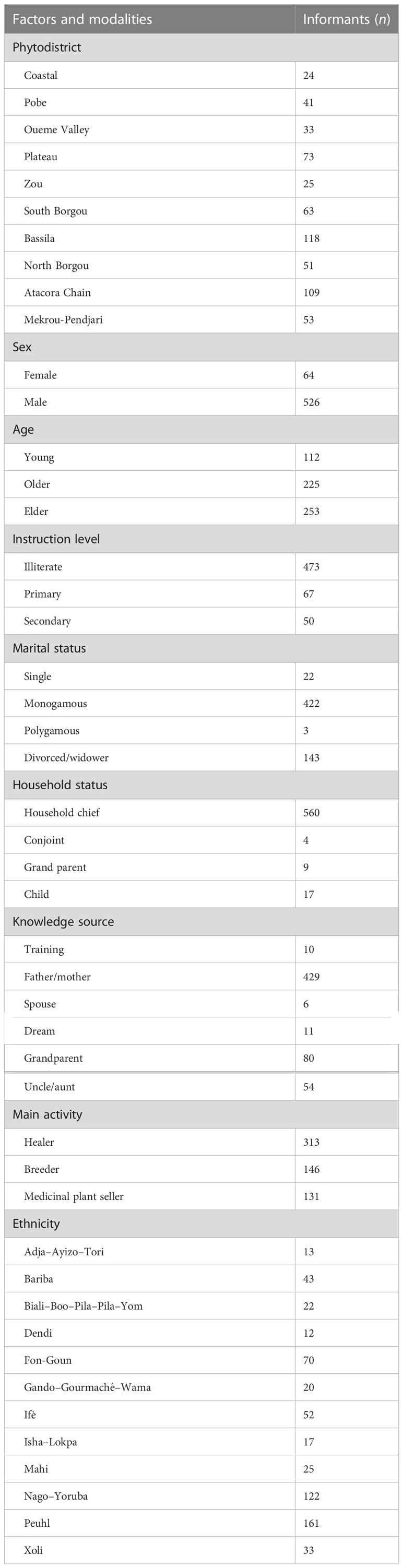
Table 1 Phytodistricts and informants sociodemographic characteristics.
Regarding the species’ ecological factors, species accessibility and ecology were considered. Species accessibility comprised the selling of its organs (availability on market: abundant, moderate, scarce), cost of its organs (free, moderate, expensive, very expensive), number of used parts (single or several), and reasons for the species’ disappearance [agriculture, medicinal overexploitation, technology, witchcraft (evil spirits)]. Ecological factors concerned ecological availability (abundant, moderate, scarce), habitat (forest, fallow, farm, home, or garden), conservation difficulty (easy or hard), and reproduction mode (slipping, seedling, rooting, or young plant).
2.3 Data analysis
To quantify the TMK held by each informant, an Ethnomedicinal Knowledge Index (EKI), adapted from Bennett and Prance’s (Bennett and Prance, 2000) relative importance index, was used and defined as follows:
where NBS = NBSi/NBSt and NP = NPi/NPt. NBS is the relative number of body systems. It was computed by dividing the number of body systems cited by informant i (NBSi) by the total number of cited body systems by all informants (NBSt). NP is the number of pharmacological properties. It was computed by dividing the number of pharmacological properties cited by a given informant (NPi) by the total number of pharmacological properties cited by all informants (NPt).
Descriptive statistics were used to describe TMK’s relationship with the sociodemographic and ecological characteristics of the informant’s area. To identify the socioeconomic and ecological factors that most influenced TMK, a conditional inference tree model was produced with “party” (Hothorn et al., 2006) and “strucchange” (Zeileis et al., 2002) packages on the matrix of sociodemographic and ecological factors (Table 1) and EKI as a response variable. A first conditional inference tree model was generated with the sociodemographic factors sex, age, instruction level, marital status, household status, knowledge source, main activity, and ethnicity. The significance of influencing factors was also examined with a generalized linear model (GLM). A second conditional inference tree model was generated with species’ ecological factors. A final model was tested that included both sociodemographic and ecological factors. This allowed us to consider possible confounding effects that might not have been caught with the individual models (i.e., the sociodemographic factors model and ecological factors model).
The medicinal species considered in the study comprised 116 woody species belonging to 90 genera and 34 families. The predominant families were Leguminosae (28 species), Moraceae (11 species), Rubiaceae (nine species), and Combretaceae (nine species) (Table 2). The Angiosperm Phylogeny Group IV (APG IV) classification of flowering plants was used to classify the species within families. Voucher specimens were also set for species identification with the help of experts from the National Herbarium, University of Abomey-Calavi (Ahoyo et al., 2021).
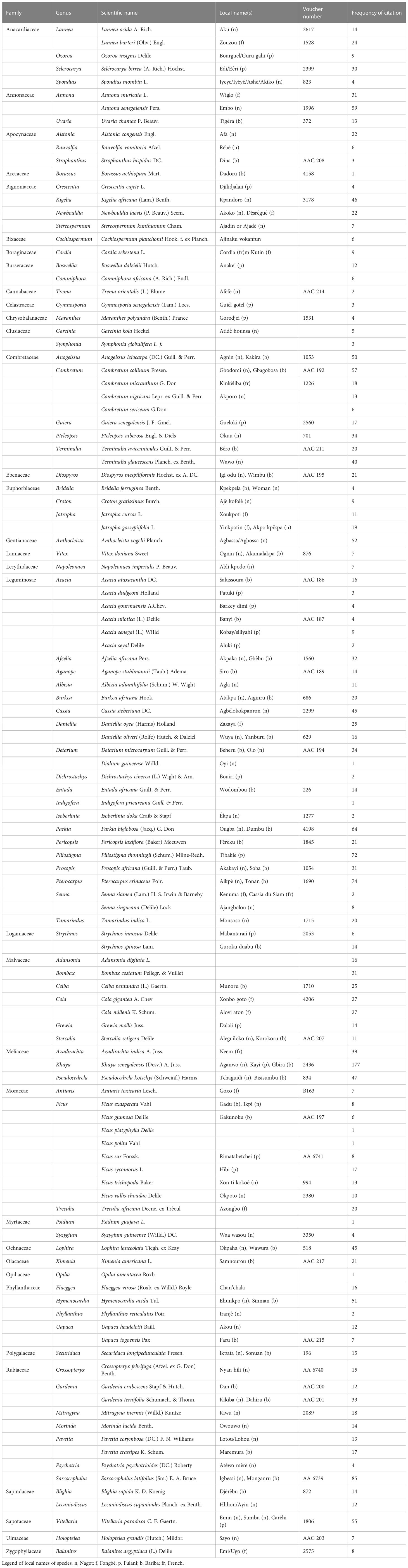
Table 2 Number of cited species.
All statistical analyses were done with R statistical freeware (R Core Team, 2017).
3 Results
3.1 Ethnomedicinal knowledge variation with sociodemographic factors
3.1.1 Descriptive statistics on sociodemographic factors
Ethnomedicinal knowledge varied with sociodemographic factors (Figure 2). EKI score varied significantly with informant sex (a). Women had higher EKI values than men. Informants with no formal education were more knowledgeable about medicinal plants than informants who had a higher instruction level (c). Medicinal plant sellers also had more medicinal knowledge than healers, breeders, and other groups such as traders, hunters, and craftsmen (e). Concerning marital status (f), EKI values of widowers or divorced were lower than those of monogamous. EKI values were lower than those of polygamists. Household mothers were the most knowledgeable; conversely, children held the least knowledge of medicinal plants (d). EKI scores were higher in informants who received their knowledge from their genitors (vertical transmission) (b).
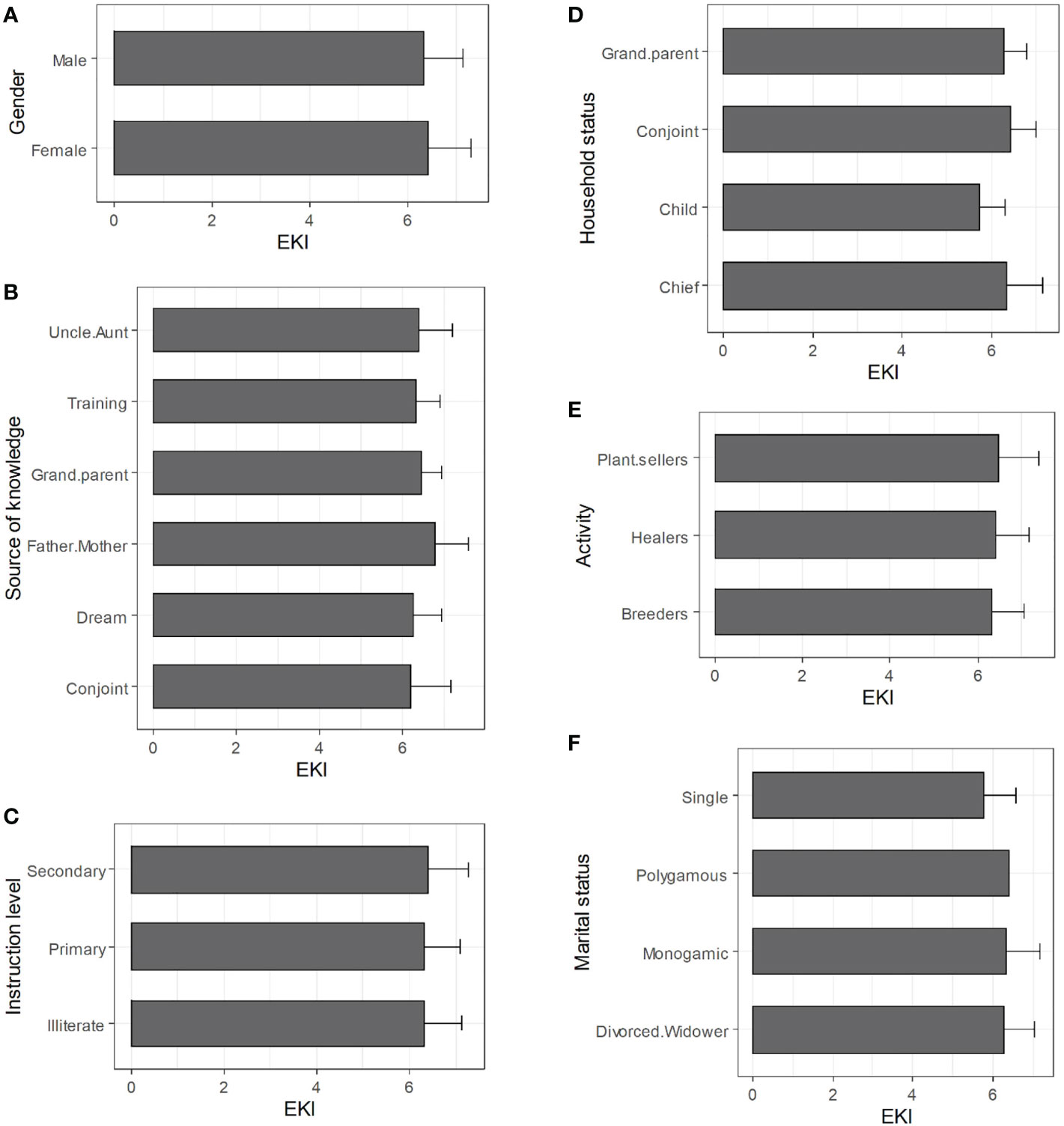
Figure 2 Ethnomedicinal knowledge variation by sociodemographic factors. (A) gender; (B): knowledge source; (C): education; (D): household status; (E): activity; (F): marital status.
When the age effect was considered, the maximum knowledge was found among those between 50 and 65 years old, whereas the minimum was among those approximately 65 years old (Figure 3).
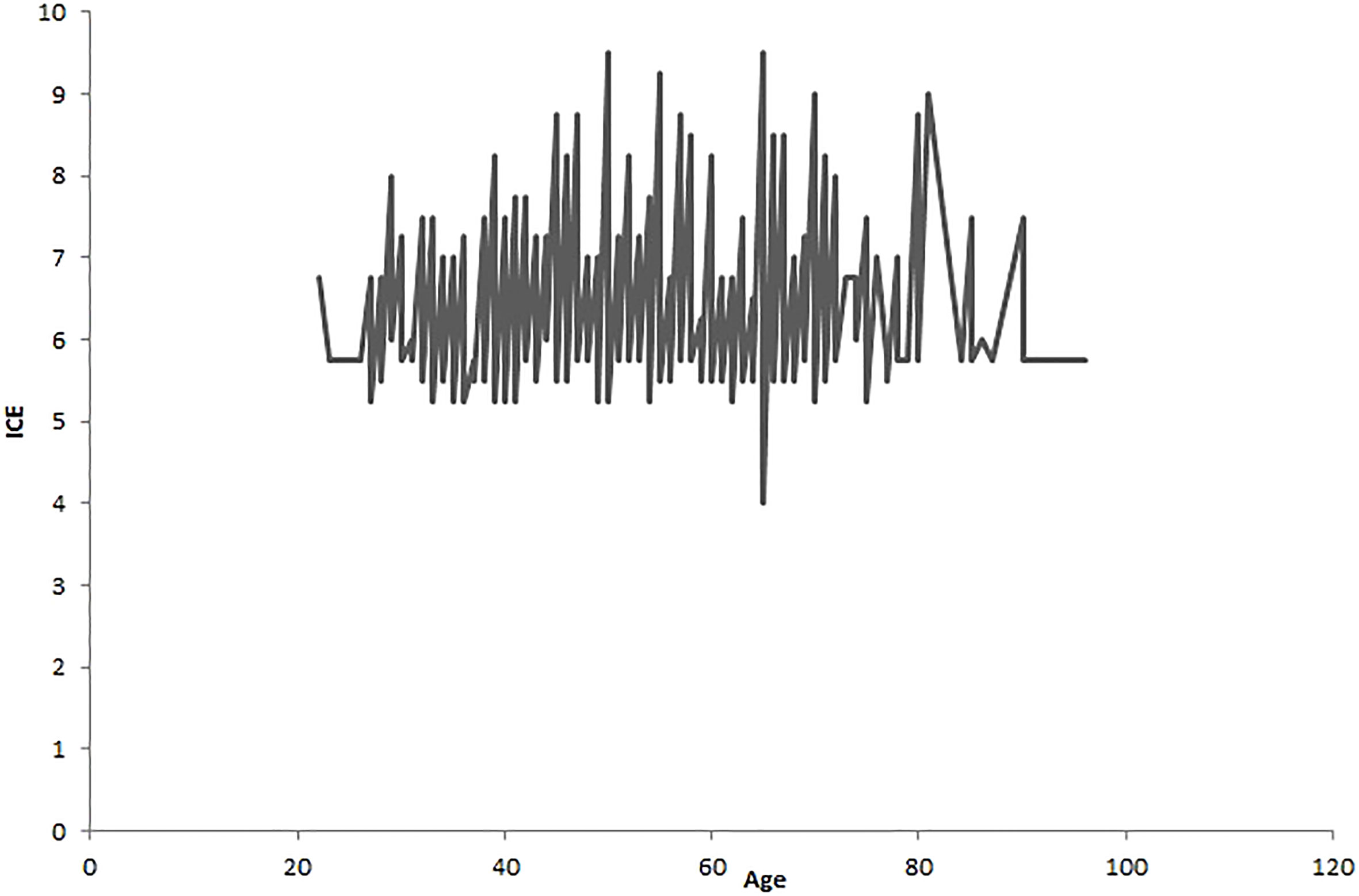
Figure 3 Ethnomedicinal knowledge variation by age.
3.1.2 Pattern effects of sociodemographic factors on ethnomedicinal knowledge
Ethnic group was the main sociodemographic factor influencing EKI (Figure 4: nodes 1 and 3). Two groupings of ethnic groups were first discriminated. Those belonging to the Gourmaché (3), Mahi (4), Fon (7), and Nago (8) groups, totaling 238 informants (node 2), were separated from those belonging to the Yoruba, Boo, Lokpa, Adja, Pila Pila, Ayizo, Goun, Tori, Wama, Biali, Gando (1), Isha (2), Xoli (5), Bariba (6), and Peuhl (9) groups (node 1). The latter grouping was further separated into two groupings: the 52 Bariba informants (6) (node 5), and the remaining 300 informants in node 4. These three groupings of informant ethnicities were delineated according to EKI. EKI values varied from 5 to 8 within the first two groups. On average, the EKI value was 7 for informants in node 2 and 6 for informants in node 4. The last group had an ethnomedicinal knowledge index of approximately 6 (leave 5). Thus, the Gourmaché, Mahi, Fon, and Nago were the most knowledgeable in ethnomedicine plant use in Benin among those cited above.
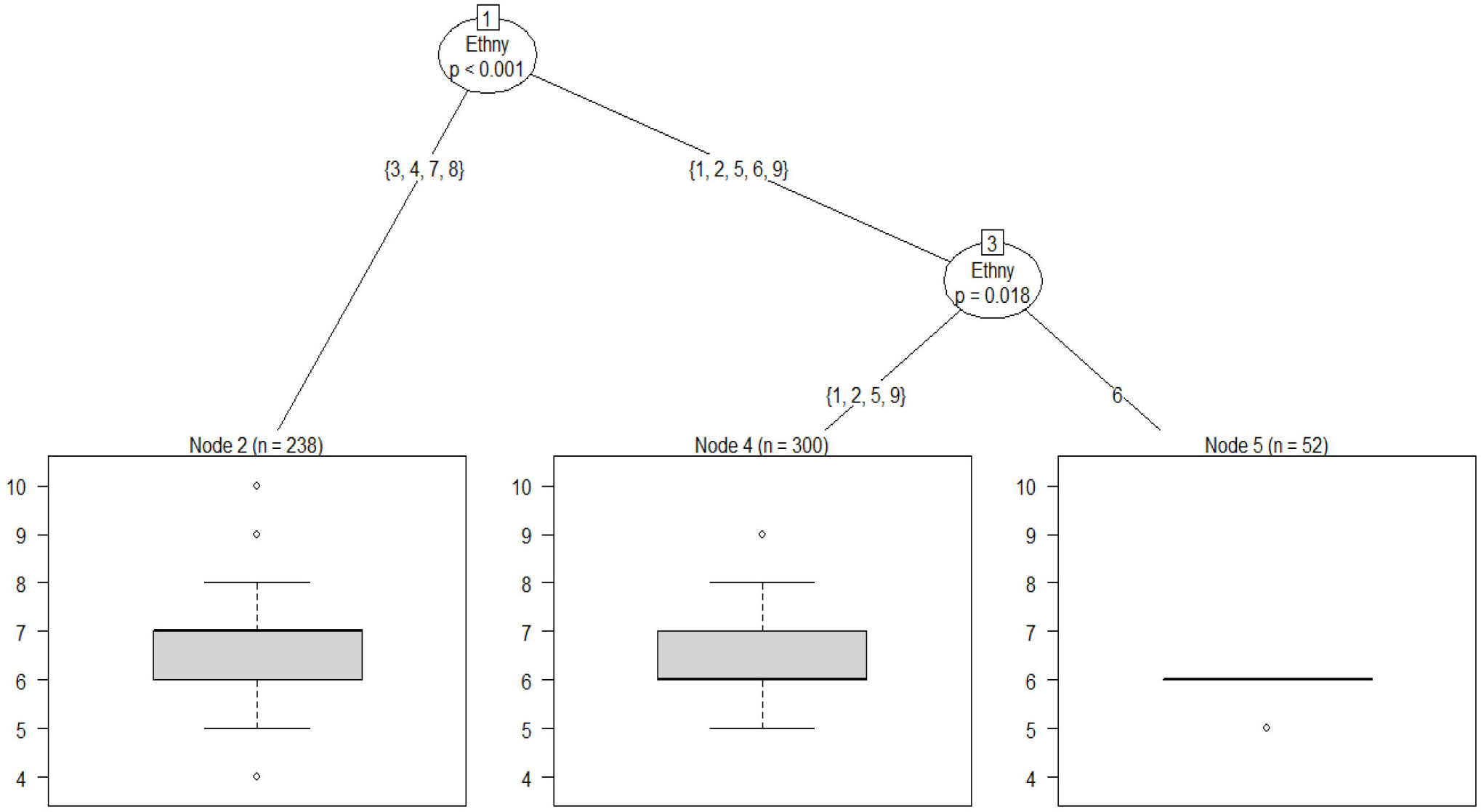
Figure 4 Inference trees showing the effects of sociodemographic factors on ethnomedicinal knowledge. 1: Yoruba, Boo, Lokpa, Adja, Pila Pila, Ayizo, Goun, Tori, Wama, Biali, Gando; 2: Isha; 3: Gourmaché; 4: Mahi; 5: Xoli; 6: Bariba; 7: Fon; 8: Nago; and 9: Peuhl.
The summary of the GLM showed that ethnic group, age, and instruction level had a significant effect on EKI value. The informants’ activity [e.g., breeder vs. other than first plant users (p = 0.041)], the source of their knowledge [e.g., friends (p = 0.008), training (p = 0.02), and parents: father/mother (p = 0.045) compared with other sources such as grandparent, uncle, and aunt as the reference level], and their membership [communal vs. departmental/national (p = 0.000)] also contributed to differences in knowledge. Likewise, some of the above factors also had a significant effect on ethnomedicinal knowledge. This was the case for the interactions between sex and membership [e.g., male: communal (p = 0.032)], marital status and membership [e.g., monogamic: communal (p = 0.011) or divorced/widower: communal (p = 0.043)], marital status and activity [e.g., monogamic: healers (p = 0.029)], and source of knowledge and membership [e.g., friends: communal (p = 0.015) or parents (father/mother): communal (p = 0.006)] (Table 3).
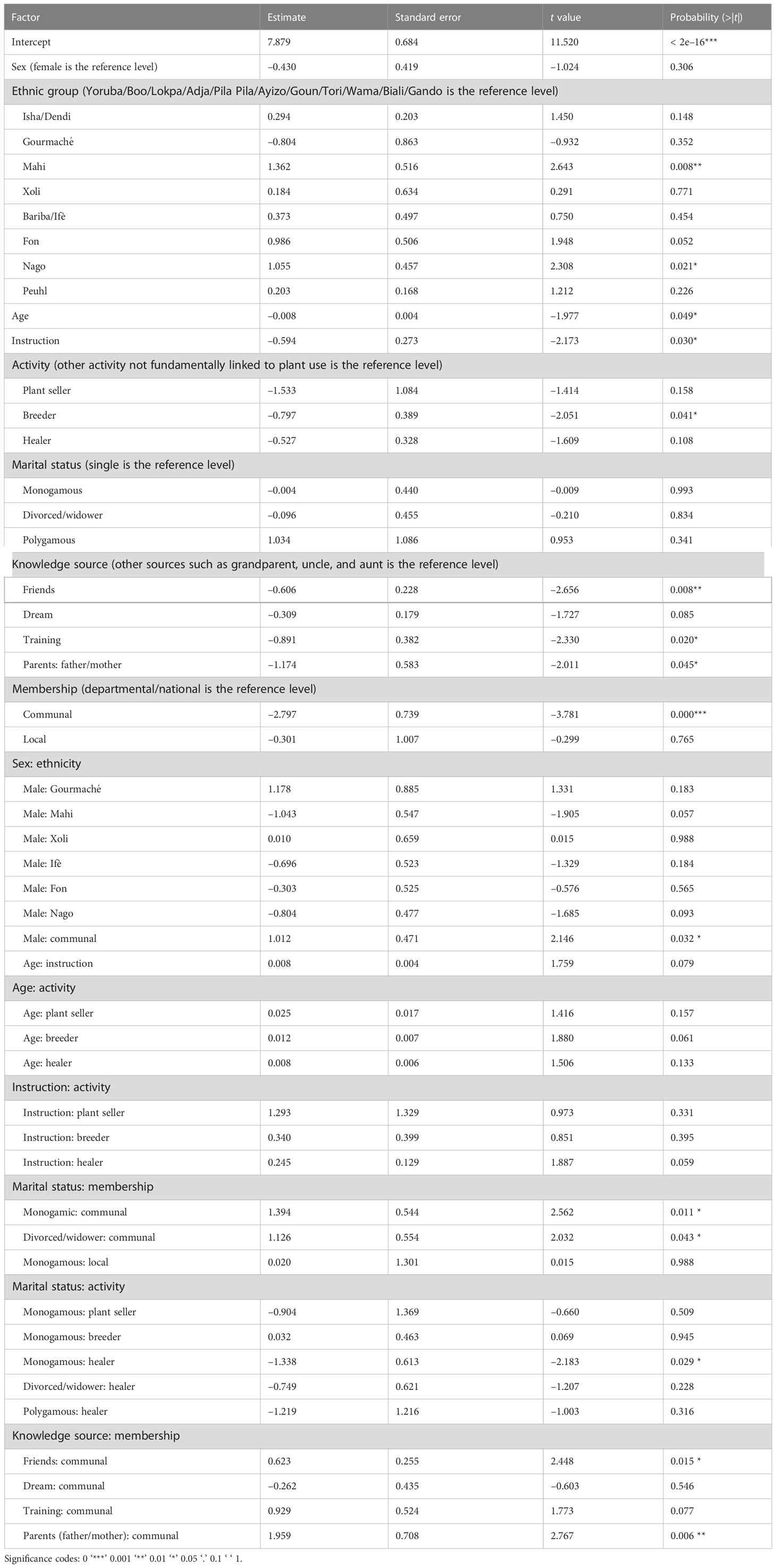
Table 3 Generalized linear model (GLM) output of the effects of sociodemography on ethnomedicinal knowledge.
Thus, the knowledge index seems to decrease with the instruction level. Considering activity, the healers gathered the most knowledge, followed by breeders and plant sellers. Considering knowledge source, the healers who received their knowledge from their grandparents had the highest ethnomedicinal knowledge index. Regarding the membership situation, the most knowledgeable healers were involved in departmental or national associations.
3.2 Effects of plant ecological factors on ethnomedicinal knowledge
3.2.1 Descriptive statistics on ethnomedicinal knowledge by plant ecological factors
Unavailable species were the least known in ethnomedicine (Figure 5A). In addition, people who often used several parts of the species appeared more knowledgeable than those who regularly used single parts of the same species (Figure 5E). The reasons for species disappearance could also lead to a variation in ethnomedicinal knowledge: species that had less availability owing mainly to their medicinal purposes appeared to be better known than those that were unavailable owing to agricultural use or witchcraft or serving of residency to evil spirits (Figure 5F). Regarding the trade of medicinal species, ethnomedicinal knowledge associated with the most available species at markets was greater than that of less available species (Figure 5B). Moreover, the ethnomedicinal knowledge associated with expensive species was less than that of cheaper species (Figure 5H). The natural habitat of species also influences the associated ethnomedicinal knowledge. Informants were more knowledgeable about species found in farmlands than those that grow in gardens (Figure 5C). In the same way, ethnomedicinal knowledge varies according to the species’ reproduction mode. Informants were more knowledgeable about species which could be reproduced by slip than those that required roots or young plants (regeneration: whole plant) (Figure 5G). The species’ ability to be conserved could also induce a variation in ethnomedicinal knowledge. Indeed, the species that require a great effort to conserve seemed to be associated with greater ethnomedicinal knowledge than those that are easy to conserve (Figure 5D).
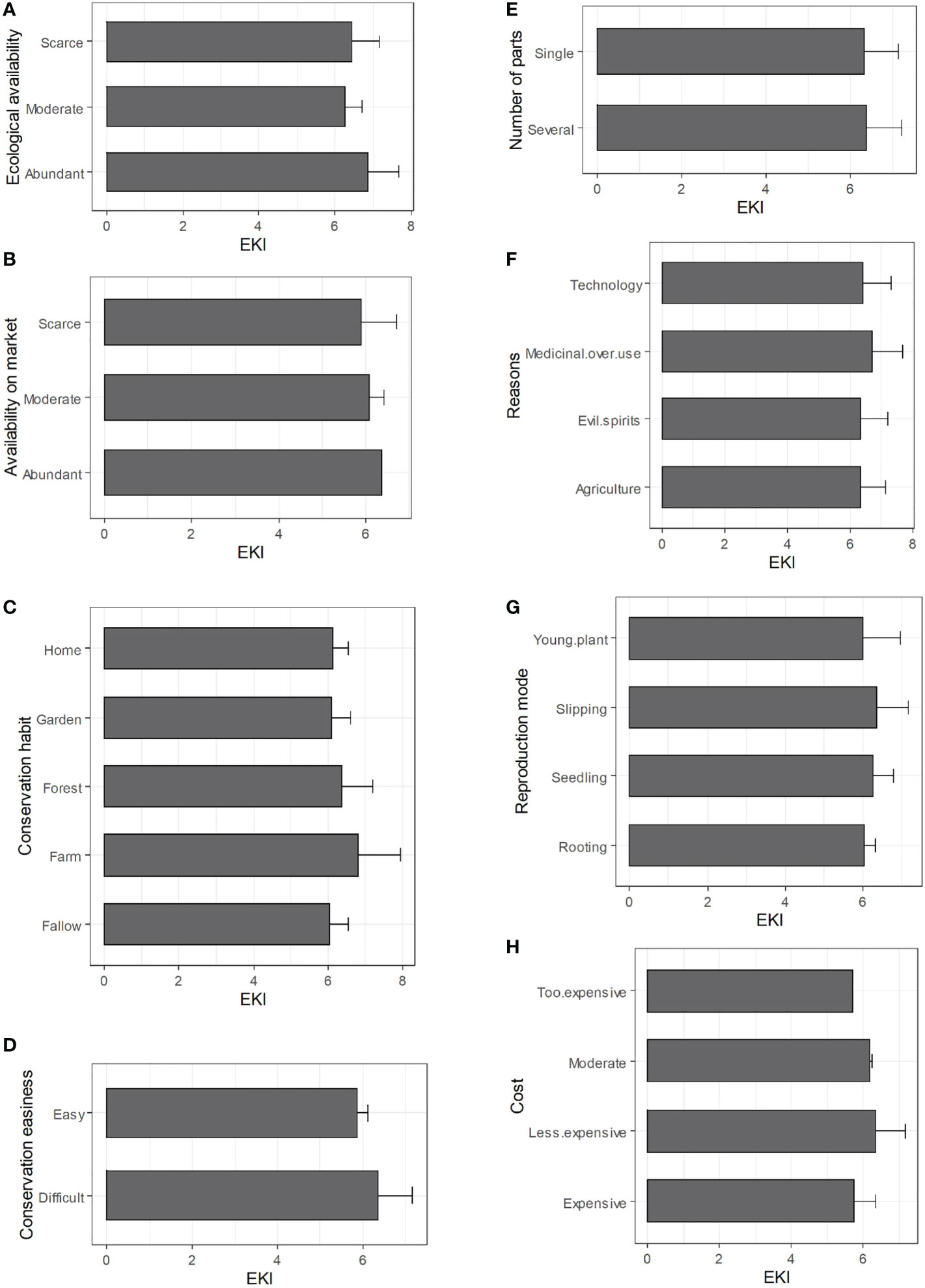
Figure 5 Ethnomedicinal knowledge variation by species ecological factors (A): ecological availability; (B): trade availability; (C): habitat; (D): conservation easiness; (E): number of used parts; (F): reasons of unavailability; (G): mod of reproduction; (H): cost.
3.2.2 Effects of species ecological factors on ethnomedicinal knowledge
Two ecological (phytodistrict and mode of reproduction) and one accessibility (reason) factors explain ethnomedicinal knowledge (Figure 6). The phytodistrict was the main ecological factor that discriminated ethnomedicinal knowledge (node 1). This discrimination separated phytodistricts 1 (Coastal), 2 (Pobè), 4 (Plateau), 5 (Zou), and 6 (South Borgou), forming a grouping of 226 informants (node 2), from 3 (Oueme), 7 (Bassila), 8 (North Borgou), 9 (Atacora Chain), and 10 (Mékrou-Pendjari) (node 3). The phytodistricts 9 and 10, forming a cluster of 162 healers (node 4), were distinguished from 3, 7, and 8 (node 5). Among phytodistricts 3, 7, and 8, the reproduction mode of species (node 5) produced a new split. The ethnomedicinal knowledge associated with species with reproduction modes 2 (from roots) and 4 (slipping/cutting) differed from that of species with reproduction modes 1 (regeneration from young plants) and 3 (seedling). Thirty-two informants (node 6) were more knowledgeable about species whose reproduction modes are 2 and 4. When considering healers with knowledge about species with reproduction modes 1 and 3, the given reasons for species unavailability (node 7) split the group into a further two categories. There were 156 informants (node 8) who acknowledged that species unavailability was due to 1 (carbonization), 3 (overexploitation for wood: technology), 5 (extensive agriculture), and 7 (cut to avoid evil spirits residency), whereas 14 informants (node 9) suggested mainly 2 (overexploitation of roots for medicine) and 4 (species ecology) as reasons for unavailability. Therefore, the phytodistrict, the mode of reproduction, and the reasons for species unavailability were the ecology and accessibility factors that determined ethnomedicinal knowledge. The healers of phytodistricts 1, 2, 4, 5, and 6 held a mean knowledge index of 7 (leave 7) whereas those of phytodistricts 9 and 10 held a mean knowledge index of 6 (leave 4). Thus, ethnomedicinal knowledge decreased from coastal meridional phytodistricts to those of septentrional savannahs. Concerning the mode of reproduction, the mean index of knowledge associated with modes 2 (from roots) and 4 (slipping/cutting) was 6 (leave 6). In addition, knowledge was lowest for the species whose unavailability was thought to be caused by overexploitation of roots for medicine (2) and species ecology (4) (leaves 8 and 9).
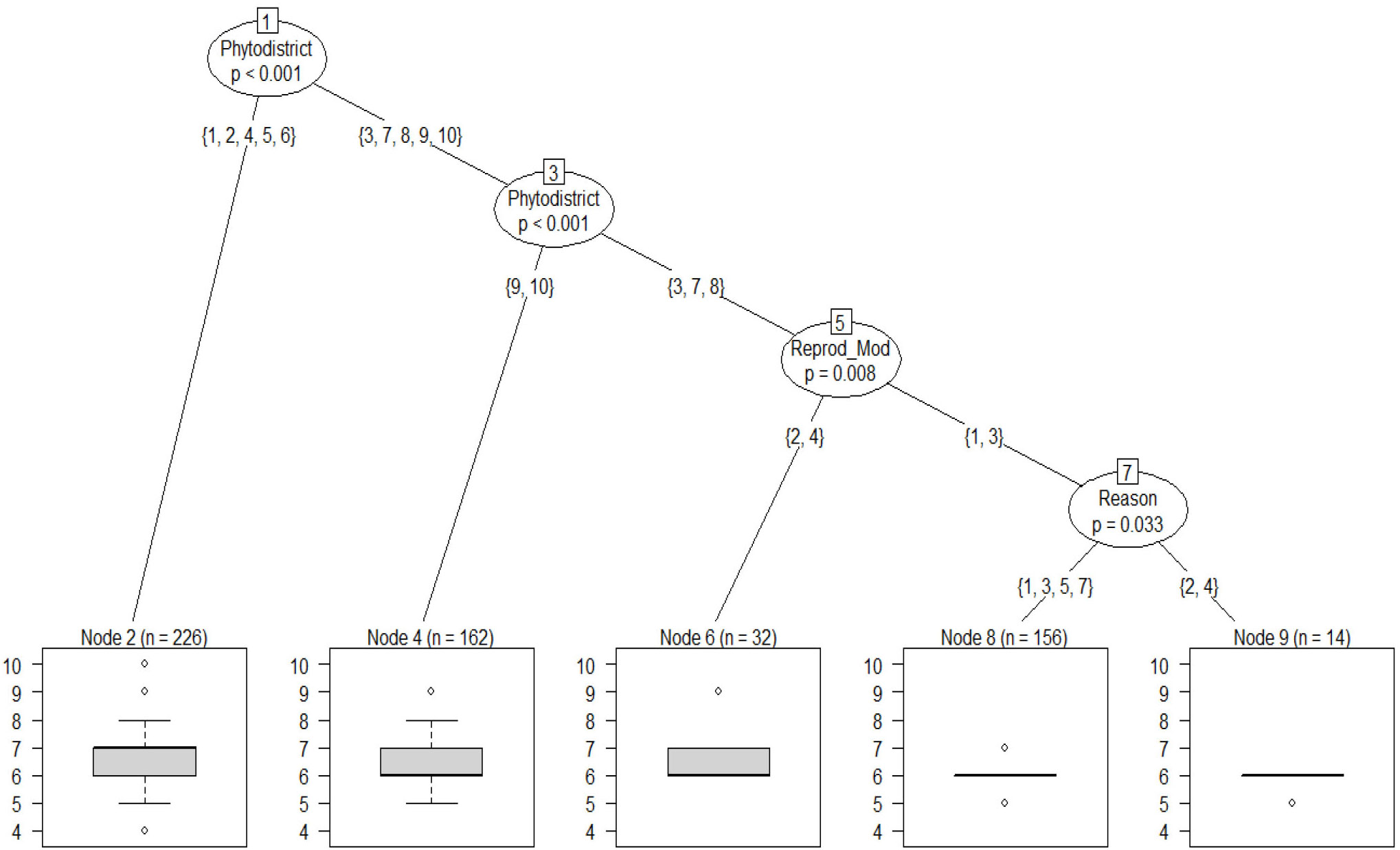
Figure 6 Effects of species ecological factors on ethnomedicinal knowledge. Legend: phytodistricts. 1: Côtier; 2: Pobè; 3: Oueme Valley; 4: Plateau; 5: Zou; 6: South Borgou; 7: Bassila; 8: North Borgou; 9: Atacora Chain; 10: Mékrou-Pendjari. Legend: reproduction mode. 1: young plants; 2: roots; 3: seedling; 4: slipping/cutting. reasons of species unavailability. 1: carbonization; 2: overexploitation of roots for medicine; 3: overexploitation for wood (technology); 4: species ecology; 5: extensive agriculture; 7: cut to avoid habitation by evil spirits.
In addition to the main factors identified above, the interactions between species availability (β = –0.129, p = 0.001) and conservation status (E = –0.926, p = 0.006), phytodistrict, and mode of reproduction [e.g., Zou: young plant (E = 1.762, p = 0.001)], and the used part and reproduction mode of species [e.g., part: young plant (E = –0.166, p = 0.021)] also induced significant differences in the ethnomedicinal knowledge. Furthermore, the knowledge associated with well conserved (locally vulnerable or endangered) and less available species was greater than that associated with non-conserved species (Table 4).
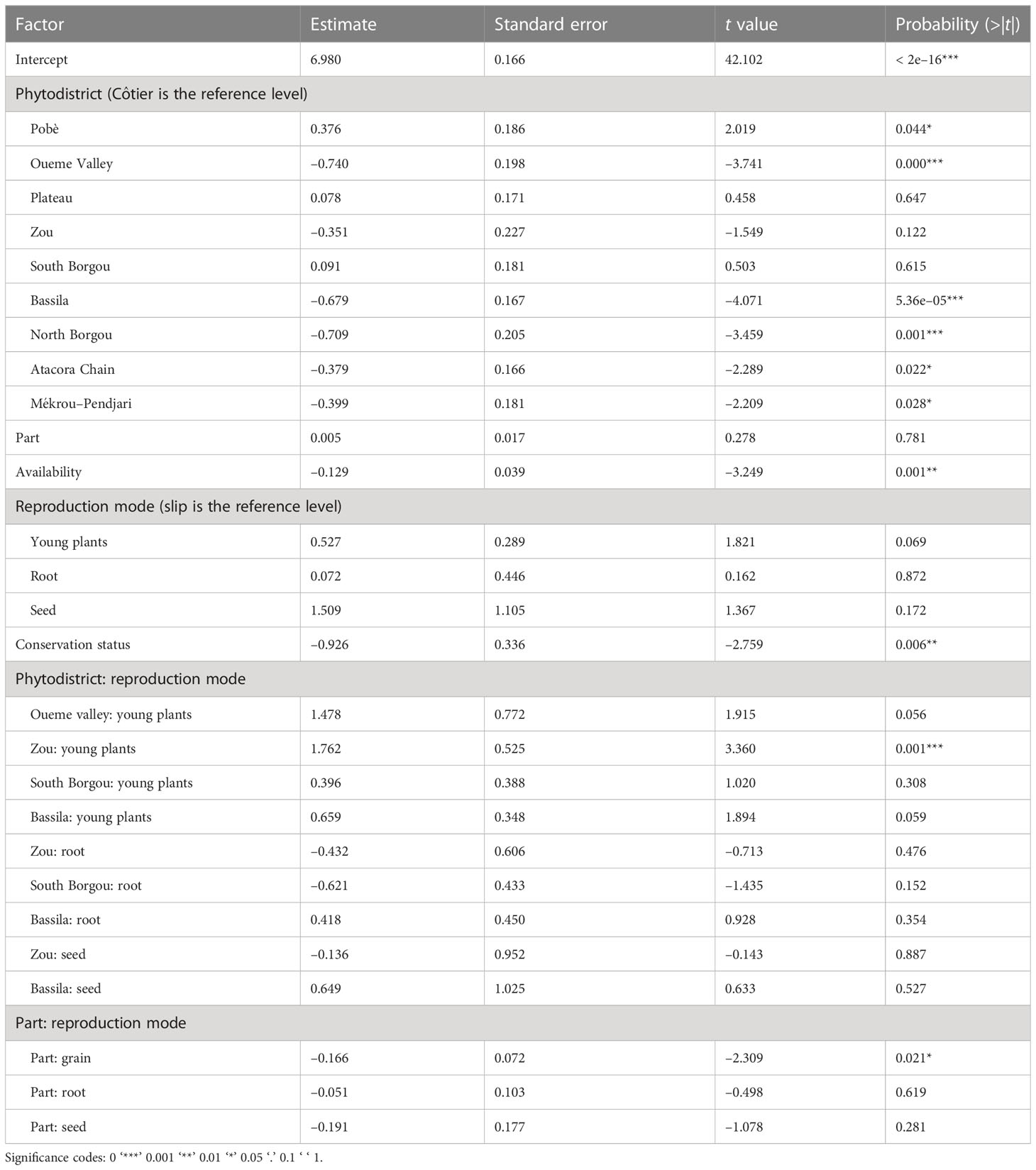
Table 4 Generalized linear model (GLM) output of the of the effects of species environment on ethnomedicinal knowledge.
3.3 Synergic effects of social, plant ecology, and accessibility factors
Phytodistrict (nodes 1 and 3) and habitat of species conservation (node 5) were revealed to have the greatest effects on ethnomedicinal knowledge in Benin (Figure 7). The ethnomedicinal knowledge associated with species that were generally conserved in fallow (2), the farm (3), and fallow and the home (7) seemed greater than that associated with species conserved in the forest (1), the home (4), fallow and the forest (5), the forest and home (6), the farm and home (8), the home and forest and fallow (10), and the farm and fallow and home (11).
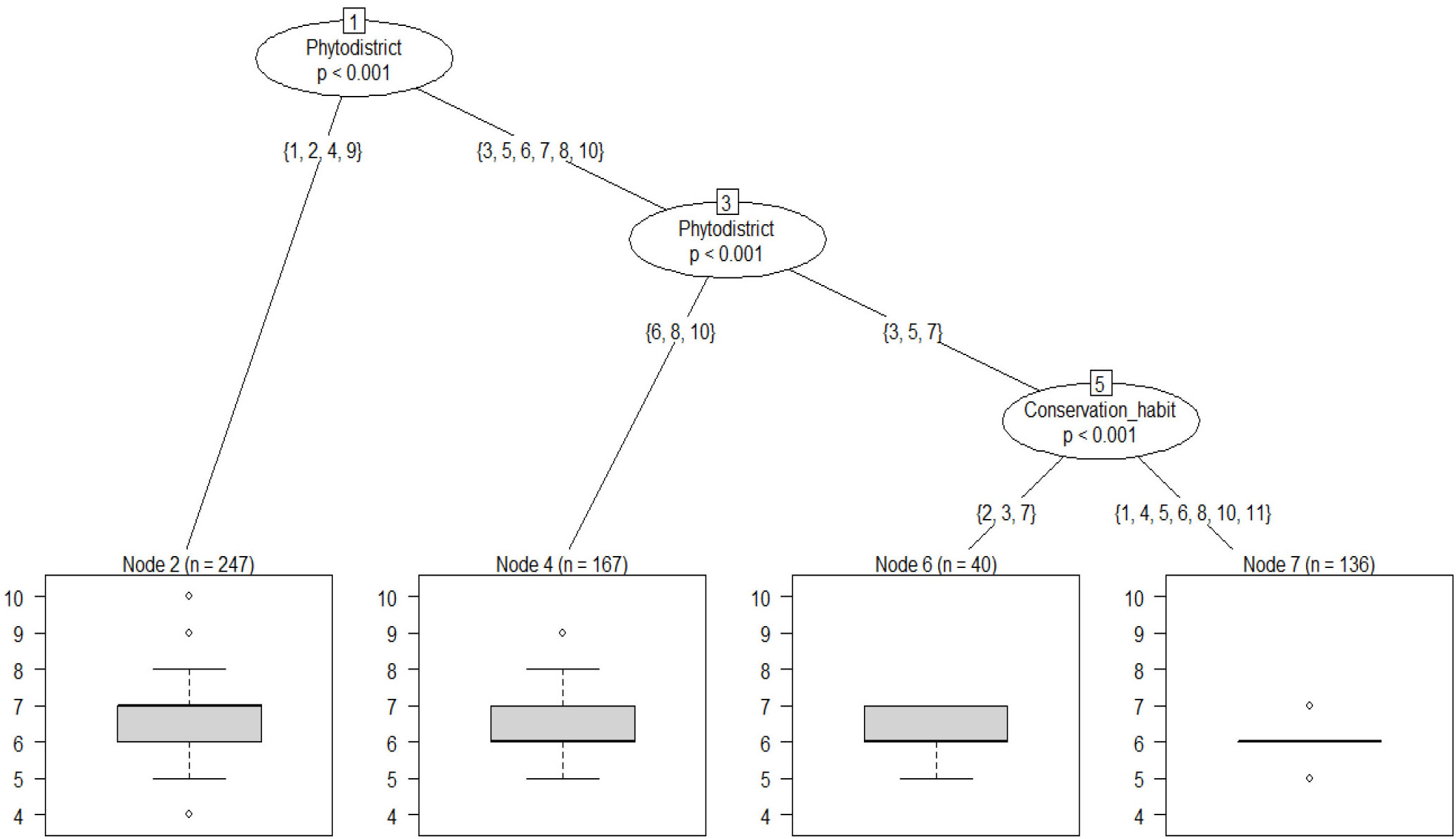
Figure 7 Effects of social and plant ecological factors on ethnomedicinal knowledge. Legend: phytodistricts. 1: Côtier; 2: Pobè; 3: Oueme Valley; 4: Plateau; 5: Zou; 6: South Borgou; 7: Bassila; 8: North Borgou; 9: Atacora Chain; 10: Mékrou-Pendjari. conservation habitat. 1: forest; 2: fallow; 3: farm; 4: home; 5: fallow and forest; 6: forest and home; 7: fallow and home; 8: farm and home; 10: home, forest, and fallow; 11: farm, fallow, and home.
In addition to these main factors, source of knowledge [e.g., friends (E = –0.457, p = 0.032), training (E = –0.841, p = 0.023)], membership position [e.g., communal (E = –0.503, p = 0.019)], and their interactions [e.g., friends: communal (E = 0.494, p = 0.039); and parents (father/mother): communal (E = 1.599, p = 0.021)] also played an important role in ethnomedicinal knowledge variation (Table 5).
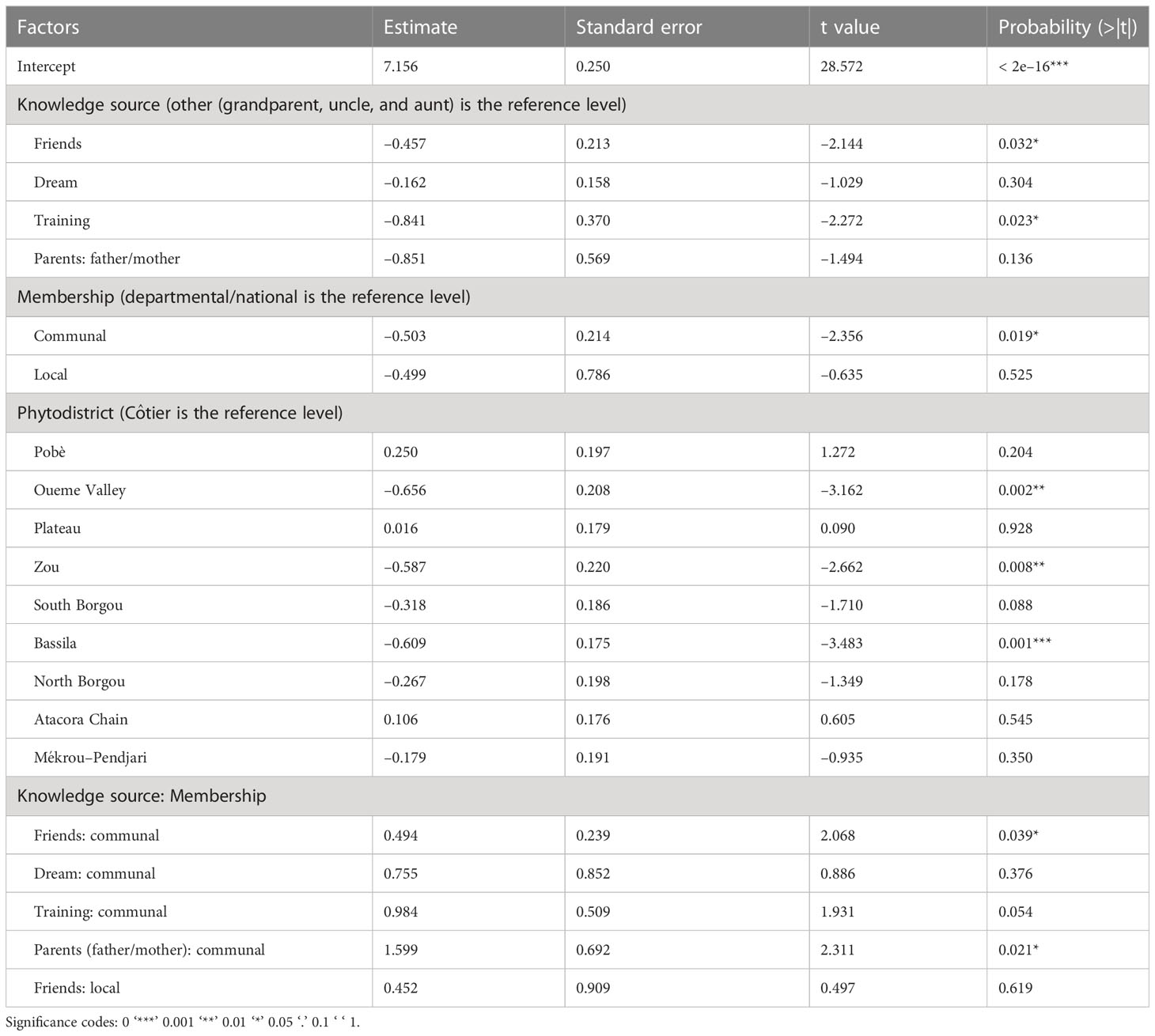
Table 5 General linearized model output of social, and plants ecological factors effects on the ethnomedicinal knowledge.
4 Discussion
4.1 Ethnic group, source of knowledge, membership position, instruction level, age, and activity determine knowledge associated with wood selection for traditional medicine
Sociodemographic attributes have an immense impact on the valuation of ecosystem services and govern indigenous ecological knowledge (Das et al., 2022). Hence, they determine the usefulness of a species and contribute to the tailoring of vegetation patches. In a study of children’s health in the south of Benin, Kouchadé et al. (2016) found that ethnomedicinal knowledge varied with ethnicity, source of knowledge, and phytodistrict. These findings were also found by other authors (Dassou et al., 2015; Kouchadé et al., 2016), who also cited instruction level as a determining factor of ethnomedicinal knowledge for traditional veterinary medicine in Benin. As in the present study, age and sex were found to be main factors accounting for variation in ethnomedicinal knowledge in Benin (Assogbadjo et al., 2011; Gouwakinnou et al., 2011; Ahoyo et al., 2018); women held more ethnomedicinal knowledge than men, as they often trade medicinal plants as their main activity. In addition, women are more engaged in primary healthcare within their families (Albuquerque et al., 2011). The ethnicities Gourmaché, Mahi, Fon, and Nago, were the most knowledgeable. This may be explained by the fact that most of these people are originally from the south: the most diversified area of Benin in terms of plant species. The Gourmaché are originally hunters, and thus seem closely familiar with traditional remedies.
The greatest ethnomedicinal knowledge was found to be held by people who gained it from their grandparents. Indeed, in traditional Beninese pharmacy, knowledge was orally passed down through the generations and, thus, owned by sociocultural groups (Upadhyay et al., 2011; Yoro, 2012). Vertical transmission remains the main diffusion method for ethnomedicinal knowledge. This tendency has been confirmed by previous studies, which argue that skills and medicinal knowledge are usually transferred from grandparents to their grandchildren (Shapi et al., 2009; Cheikhyoussef et al., 2011).
Instruction level was negatively correlated with ethnomedicinal knowledge, as also found by Ahoyo et al. (2018). People with higher levels of education seek office jobs and give up traditional knowledge. In contrast, those with less formal education remain dependent on forest resources and studies have shown that the majority of traditional healers are illiterate (Dassou et al., 2015; Ouachinou et al., 2019).
Membership position was also an important factor that contributed to ethnomedicinal knowledge. Local healers who were involved in national or at least departmental associations were found to be the most knowledgeable. In such associations, they have more access to modern medicine, which deepens their knowledge. Owing to the constant proximity of local healers and elders to plants, the local healers were expected to be more knowledgeable than those involved in national or departmental associations, who often travel for meetings, training with western (i.e., modern) medicine practitioners, etc. However, Vandebroek et al. (2004) found that, in South America, medicinal plant knowledge does not necessarily depend on the level of plant diversity, degree of modernization, or absence of western healthcare infrastructure in the healer’s environment. Therefore, the role of social factors in ethnomedicinal knowledge determination still varies with people’s history.
Regarding informants’ main activity, medicinal plant sellers and healers were the most knowledgeable. Their activities contribute widely to the nature of neighboring shrublands. They are also always in contact with plants and other people who use them widely. These people are often traders, healers, or patients, and thus knowledge is continually shared and renewed (Dassou et al., 2015). They derive their incomes from the plant, and thus were aware of saving this cultural patrimony.
4.2 Ecological parameters driving vegetation shape through ethnomedicinal knowledge variation
The main factors which determine ethnomedicinal knowledge were phytodistrict, mode of reproduction, reasons for disappearance, species availability, habitat of species conservation, and conservation status.
Ethnomedicinal knowledge was found to be greater in the southern phytodistricts (Guineo-Congolese climate) than the northern ones (Sudanian climate). This decreasing trend moving northwards was also found by Kouchadé et al. (2016). Dassou et al. (2015) found the inverse trend in their study for traditional veterinary medicine. The inverse findings of Dassou et al. (2015) could be due to the study’s aim. The northern phytodistricts appear more knowledgeable on livestock breeding, owing to the importance of this activity in the region. Indeed, phytodistricts are ecosystems or habitats for particular animals or plant organisms. They each have homogeneous conditions regarding soils and climate, which determines the partitioning of different peoples in the country. Thus, the floristic diversity in an area depends strongly on the ecology of the zone and its inhabitants. The plants found in an ecological zone are considered to be owned by its people, and the zones are characterized by their relative ethnomedicinal knowledge (Dassou et al., 2015). Therefore, the variation of ethnomedicinal knowledge found among phytodistricts could be due to species diversity among phytodistricts. Moreover, the Guineo-Congolese climate of the south seems more favorable to biodiversity than the Sudanian climate in the north. Correspondingly, ethnomedicinal knowledge, which is often linked to available diversity, will be greater in the south than in the north.
The mode of reproduction and the reason for the disappearance of species also affect ethnomedicinal knowledge. The species that can be reproduced from roots and slipping/cutting were associated with the greatest ethnomedicinal knowledge. Those that needed to be reproduced in a nursery were associated with the weakest ethnomedicinal knowledge. This trend could be attributed to the ease of this reproduction mode. Indeed, healers were most able to remember and share knowledge about the easiest reproducible species. Moreover, the ethnomedicinal knowledge associated with species that were unavailable because of human pressure (i.e., carbonization, overexploitation for wood technology, extensive agriculture, and cutting to avoid habitation by evil spirits) seemed to be the greatest.
The species that were locally protected, and often less available, were found to be associated with the greatest ethnomedicinal knowledge. A similar tendency has been shown elsewhere (Sharafatmandrad and Khosravi Mashizi, 2020). The harvesting of species with high popularity levels, and thus associated with high knowledge levels, may lead to sustainability problems (Posthouwer et al., 2016). Therefore, it needs to reverse the decline in wild populations of these woody species, otherwise important ethnomedicinal knowledge associated with the threatened species will be lost. The effects of ecological availability and the used part (single or several) on ethnomedicinal knowledge have been proposed elsewhere (ecological apparency hypothesis) although no significant effects were found for them in this study.
The ecological availability of species has for several decades been found to be highest for the most numerous species that are the most used by people (Philips and Gentry, 1993; Nzuki, 2016). In this sense, the local therapeutic use of woody species may be associated with their wide visibility and availability throughout the year. The perennial and most available species were found to play a major part in medicinal plant trading in Benin (Kouchadé et al., 2016). However, this study seems to show that ethnomedicinal knowledge is greater when the species are scarce. Thus, the ethnomedicinal knowledge of woody species is not necessarily dependent on species availability. This change could be due to anthropogenic pressure exerted on the distribution area of the species, with its negative impacts on the sustainable conservation of forests (Sinsin et al., 2009; Djego et al., 2011). Moreover, in the case of some species, although availability has decreased over the years, people are willing to travel far to collect them because of their importance.
The ethnomedicinal knowledge associated with species that were conserved in fallow, the farm, and the home seemed greater than that associated with species conserved in the forest. Thus, people are more knowledgeable about species that grow or are available in their vicinity.
The regularly used parts of the species also determined the level of associated ethnomedicinal knowledge, although its effect was not significant. People who regularly used fewer species or single organs seemed more knowledgeable than those who used numerous species or several parts of the same species. The users of several parts for different therapeutic uses were generally the most numerous (Hseini, 2008; Mehdioui, 2008; Lahsissene, 2010). The wide use of some organs such as roots and barks could threaten the wild populations of species (Gaoué & Ticktin, 2007; Yaoitcha, 2016). Generally, the researched utility and the knowledge about them drive the sampled plant parts.
Furthermore, an initial approach based on the chemosensory perception of taste was developed to find a biological basis in the selection of medicinal plants in the human species. However, there was no correlation between the ability to identify tastes associated with plant chemicals and the identification of plants with pharmacological properties (da Silva et al., 2020).
An examination of the synergy between the effects of social, plant ecology, and accessibility factors on ethnomedicinal knowledge revealed phytodistrict and habitat of species conservation as the most important factors. These factors seem strongly correlated with ethnicity and the mode of reproduction. Indeed, ethnic groups are clustered around phytodistricts and, thus, a variation among phytodistricts also implies variation among ethnicities. In turn, the knowledge associated determines the pressure on the species.
Different environmental stressors have an effect on the reproductive potential of species (Lazarus et al., 2021). The presence of these stressors in a species conservation habitat could affect the species reproduction viability, depending on its mode of reproduction.
5 Conclusion
Ethnicity, source of knowledge, membership position, age, instruction level, and activity are the main sociodemographic factors that influence the ethnomedicinal knowledge of woody species in Benin. As for ecological and ecological factors, phytodistrict, mode of species reproduction, reasons for species disappearance, availability, and conservation status have the most effect on ethnomedicinal knowledge variation. The integration of these two kinds of factors highlighted phytodistrict, habitat of species conservation, source of knowledge, and membership of informants as the principal factors affecting ethnomedicinal knowledge in Benin.
Hence, sociocultural factors determining people’s importance in a region and thus sampling pressure, combined with the ecological factors of the species themselves, act as key regulators of vegetation growth, and thus woodlands and savanna management in Benin. This traditional knowledge may be lost or forgotten, owing to migration, acculturation, and declining interest from the younger generation in response to the increasing availability of commercial over-the-counter medicines. Thus, the factors identified in this study as important for ethnomedicinal knowledge should be integrated into a comprehensive plan for knowledge conservation, which has a positive impact on biodiversity management and, hence, the sustainable use of wood resources. This research will also be helpful in paving the way for better collaboration between traditional and modern medicine. This will allow better endogenous knowledge conservation via its transcription into formal notes. Finally, savanna and woodlands in Benin and similar ecosystems elsewhere could be better managed through attention to the most useful species in the region and the integration of their ecology.
Data availability statement
The original contributions presented in the study are included in the article. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethical Committee of the University of Abomey-Calavi (EC approval 2019/1134/UAC/Benin). The Code of Ethics of the International Society of Ethnobiology (ISE, 2008) was strictly followed, and the purpose of the study was explained before conducting the interviews. Verbal informant consent was obtained from the participants, who were assured of confidentiality and anonymity. A cordial relationship was established with the informants at the beginning of the study. The informants were interviewed after introducing and explaining the purpose of the visit and the aims of the survey. Written informed consent for participation was not required for this study, in accordance with national legislation and institutional requirements.
Author contributions
CCA and TDH conceived the research. CCA and IM gathered the data. CCA and KVS analyzed the data. CCA drafted the manuscript. RLGK and MRBH supervised the whole work. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the “Fonds National de la Recherche Scientifique et de l’Innovation Technologique (FNRSIT) du Bénin” through the project “Biologie de la Conservation et Ethnopharmacologie des Ligneux médicinaux de la pharmacopée béninoise (BIOCEL)” (Grant No. 05/MESRS/FNRSIT/SSE/SA).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abebe B. A., Teferi S. C. (2021). Ethnobotanical study of medicinal plants used to treat human and livestock ailments in hulet eju enese woreda, East gojjam zone of amhara region, Ethiopia. Evidence-Based Complement. Altern. Med. 2021, 29, 6668541. doi: 10.1155/2021/6668541
Adomou A. C. (2005). Plant vegetation patterns and ecological gradients inBenin: Implications for biogeography and conservation (WAGENINGEN: PhD thesis Wageningen University), 133.
Adomou A. C., Agbani O. P., Sinsin B. (2011). “Plants,” in Protection de la nature en afrique de l’Ouest: Une liste rouge pour le bénin. nature conservationin West Africa: Red list for Benin. Ed. Neuenschwander P. S., Sinsin B., Goergen G. (Ibadan, Nigeria: International Institute of Tropical Agriculture).
Ahoyo C. C., Houehanou T. D., Yaoitcha A. S., Prinz K., Assogbadjo A. E., Adjahossou C. S. G., et al. (2018). A quantitative ethnobotanical approach toward biodiversity conservation of useful woody species in wari-maro forest reserve (Benin, West Africa). Environ. Dev. Sustain. 20 (5), 2301–2320. doi: 10.1007/s10668-017-9990-0
Ahoyo C. C., Houehanou T. D., Yaoitcha A. S., Prinz K., Glèlè Kakaï R. L., Sinsin B. A., et al. (2021). Traditional medicinal knowledge of woody species across climatic zones in Benin (West Africa). J. Ethnopharmacol. 265, 113417. doi: 10.1016/j.jep.2020.113417
Akerreta S., Cavero R. Y., López V., Calvo M. I. (2007). Analyzing factors that influence the folk use and phytonomy of 18 medicinal plants in navarra. J. Ethnobiol. Ethnomed. 3, 16. doi: 10.1186/1746-4269-3-16
Albuquerque U. P. (2006). Re-examining hypotheses concerning the use and knowledge of medicinal plants a study in the caatinga vegetation of NE Brazil. J. Ethnobiol. Ethnomed. 2 (30), 1–10. doi: 10.1186/1746-4269-2-30
Albuquerque U. P., Soldati G. T., Sieber S. S., Ramos M. A., De Sá J. C., De Souza L. C. (2011). The use of plants in the medical system of the fulni–ô people (NE brazil): A perspective on age and gender. J. Ethnopharmacol. 133 (2), 866–873. doi: 10.1016/j.jep.2010.11.021
Allabi A. C., Busiac K., Ekanmiana V., Bakiono F. (2011). The use of medicinal plants in self-care in the agonlin region of Benin. J. Ethnopharmol. 133, 234–243. doi: 10.1016/j.jep.2010.09.028
Angelsen A., Jagger P., Babigumira R., Belcher B., Hogarth N. J., Bauch S., et al. (2014). Environmental Income and Rural Livelihoods: A Global-Comparative Analysis. World Dev. 64 (S1), S12–S28. doi: 10.1016/j.worlddev.2014.03.006
Aniruddha S., Ghosh P. (2011). A note on the ethnobotanical studies of some pteridophytes in Assam. India J. Tradit. Knowld 10 (2), 292–295. Available at: http://nopr.niscpr.res.in/handle/123456789/11506.
Assogbadjo A. E., Glèlè Kakaï R., Adjallala F. H., Azihou A. F., Vodouhê G. F., Kyndt T., et al. (2011). Ethnic differences in use value and use patterns of the threatened multipurpose scrambling shrub (Caesalpinia bonduc l.) in Benin. J. Med. Plants Res. 5, 1549–1557.
Aswani S., Lemahieu A., Sauer W. H. H. (2018). Global trends of local ecological knowledge and future implications. PloS One 13 (4), e0195440. doi: 10.1371/journal.pone.0195440
Balick M. J., Cox P. A. (1996). Plants, people and culture: The science of ethnobotany (New York: The Scientific American Library).
Beltrán-Rodríguez L., Ortiz-sánchez A., Mariano N. A., Maldonado-Almanza B., Reyes-García V. (2014). Factors affecting ethnobotanical knowledge in a mestizo community of the Sierra de huautla biosphere reserve, Mexico. J. Ethnobiol. Ethnomed. 10, 14. doi: 10.1186/1746-4269-10-14
Benkhnigue O., Zidane L., Fadli M., Elyacoubi H., Rochdi A., Douira A. (2011). Etude ethnobotanique des plantes médicinales dans la région de mechraâ Bel ksiri (Région du gharb du maroc). Acta Botanica Barcinonensia 53, 191–216. Available at: https://raco.cat/index.php/ActaBotanica/article/view/25292.
Bennett B. C., Prance G. T. (2000). Introduced plants in the indigenous pharmacopoeia of northern south America. Econ. Bot. 54, 90–102. doi: 10.1007/BF02866603
Brouwer N., Liu Q., Harrington D., Kohen J., Vemulpad S., Jamie J., et al. (2005). An ethnopharmacological study of medicinal plants in new south Wales. Molecules 10, 1252–1262. doi: 10.3390/10101252
Bussmann R. W., Paniagua Zambrana N. Y., Sikharulidze S., Kikvidze Z., Kikodze D., Tchelidze D., et al. (2016). A comparative ethnobotany of khevsureti, samtskhe-javakheti, tusheti, svaneti, and racha-lechkhumi, republic of Georgia (Sakartvelo). Caucasus. J. Ethnobiol. Ethnomed. 12, 43. doi: 10.1186/s13002-016-0110-2
Byg A., Balslev H. (2004). Factors affecting local knowledge of palms in nangaritza valley, south eastern Ecuador. J. Ethnobiol. 24 (2), 255–278.
Cheikhyoussef A., Shapi M., Matengu K., Ashekele H. M. (2011). Ethnobotanical study of indigenous knowledge on medicinal plant use by traditional healers in oshikoto region, Namibia. J. Ethnobiol. Ethnomed. 7, 10. doi: 10.1186/1746-4269-7-10
Chibembe A. S., Birhashirwa N. R., Kamwanga F., Mangambu M. (2015). Exploitation de bambous (Sinarundinaria alpina (K. schum.) C.S. chao et renvoize), cause des conflits entre le parc national de kahuzi-biega et la population environnante: Stratégie de conservation et de résolution de conflit. Int. J. Environ. Sci. Technol. 72 (2), 265–287. doi: 10.1080/00207233.2014.961270
Dapar M. L. G., Alejandro G. J. D., Meve U., Liede-Schumann S. (2020). Quantitative ethnopharmacological documentation and molecular confirmation of medicinal plants used by the manobo tribe of agusan del sur, Philippines. J. Ethnobiol. Ethnomed. 16, 14. doi: 10.1186/s13002-020-00363-7
Das M., Das A., Seikh S., Pandey R. (2022). Nexus between indigenous ecological knowledge and ecosystem services: A socio-ecological analysis for sustainable ecosystem management. Environ. Sci. Pollut. Res. 29, 61561–61578. doi: 10.1007/s11356-021-15605-8
da Silva T. L. L., Junior W. S. F., Albuquerque U. P. (2020). Is there a biological basis in the selection of medicinal plants in the human species? An initial approach based on chemosensory perception of taste. Ethnobiol. Conserv. 9, 3. doi: 10.15451/ec2020-01-9.03-1-15
Dassou H. G. (2014). Diversité, usages vétérinaires et vulnérabilité des plantes médicinales au nord-bénin. Int. J. Biol. Chem. Sci. 8 (1), 189–210. doi: 10.4314/ijbcs.v8i1.18
Dassou H. G., Yedomonhan H., Adomou A. C., Ogni C. A., Tossou M. G., Akoegninou A. (2015). Facteurs socioculturels et environnementaux déterminant la connaissance ethno vétérinaire au bénin. Afrique Sci. 11 (5), 335–360.
Djego J., Djego-Djossou S., Cakpo Y., Agnani P., Sinsin B. (2011). Evaluation du potentiel ethnobotanique des populations rurales au sud et au centre du bénin. Int. J. Biol. Chem. Sci. 5 (4), 1432–1447. doi: 10.4314/ijbcs.v5i4.10
Estomba D., Ladio A., Lozada M. (2006). Medicinal wild plant knowledge and gathering patterns in a mapuche community from northwestern Patagonia. J. Ethnopharmacol. 103, 109–119. doi: 10.1016/j.jep.2005.07.015
Gaoué O. G., Coe M. A., Bond M., Hart G., Seyler B. C., McMillen H. (2017). Theories and major hypotheses in ethnobotany. Econ. Bot. 71 (3), 269–287. doi: 10.1007/s12231-017-9389-8
Gaoué O. G., Ticktin T. (2007). Patterns of harvesting foliage and bark from the multipurpose tree khaya senegalensis in Benin: Variation across ecological regions and its impacts on population structure. Biodivers. Conserv. 137, 424–436. doi: 10.1016/j.biocon.2007.02.020
Goussanou C., Tente B., Djego J., Agbani P., Sinsin B. (2011). Inventaire, caractérisation et mode de gestion de quelques produits forestiers non ligneux du bassin versant de la donga. Annales Des. Sci. Agronom. 14 (1), 77–99.
Gouwakinnou G. N., Lykke A. M., Assogbadjo A. E., Sinsin B. (2011). Local knowledge, pattern and diversity of use of Sclerocarya birrea. J. Ethnobiol. Ethnomed. 7 (8), 1746–4269. doi: 10.1186/1746-4269-7-8
Hanazaki N., Herbst D. F., Marques M. S., Vandebroek I. (2013). Evidence of the shifting baseline syndrome in ethnobotanical research. J. Ethnobiol. Ethnomed. 9, 75. doi: 10.1186/1746-4269-9-75
Hothorn T., Hornik K., Zeileis A. (2006). Unbiased recursive partitioning: A conditional inference framework. J. Comput. Graphic. Stat 14 (3), 675–699. doi: 10.1198/106186006X133933
Houehanou T., Assogbadjo A., Glèlè Kakaï R., Houinato M., Sinsin B. (2011). Valuation of local preferred uses and traditional ecological knowledge in relation to three multipurpose tree species in Benin (West Africa). For. Policy Econ. 13, 554–562. doi: 10.1016/j.forpol.2011.05.013
Hseini S. (2008). Etude ethnobotanique de la flore médicinale dans la région de Rabat, (Maroc occidental) (Rabat, Maroc: Thèse de Doctorat National, Université Mohamed V, Facultés des Sciences), 173.
INSAE (2016). Rapport du quatrième recensement général de la population et de l’Habitation (Bénin: Ministère du Plan et du Développement. République du Bénin).
Jhariya M. K., Yadav D. K. (2018). Biomass and Carbon Storage Pattern in Natural and Plantation Forest Ecosystem of Chhattisgarh, India. J. Environ. Sci. 34 (1), 1–11. doi: 10.7747/JFES.2018.34.1.1
Kamari P., Otaghvaria A. M., Govindapyari H., Bahuguna M., Uniyal P. (2009). Some ethno-medically important plants of India. Int. J. Med. Aroma. Plants 1 (1), 18–22.
Kang Y., Łuczaj Ł, Kang J., Zhang S. (2013). Wild food plants and wild edible fungi in two valleys of the qinling mountains (Shaanxi, central China). J. Ethnobiol. Ethnomed. 9, 26. doi: 10.1186/1746-4269-9-26
Klein A. (2019). Drug problem or medicrime? Distribution and use of falsified tramadol medication in Egypt and West Africa. J. Illicit Econ. Dev. 1 (1), 52–62. doi: 10.31389/jied.10
Kouchadé A. S., Adomou A. C., Tossou G. M., Yédomonhan H., Dassou G. H., Akoègninou A. (2016). Étude ethnobotanique des plantes médicinales utilisées dans le traitement des maladies infantiles et vendues sur les marchés au sud du bénin. J. Anim. Plant Sci. 28 (2), 4418–4438.
Lahsissene H. (2010). Recherches ethnobotaniques et floristiques des plantes médicinales utilisées dans la région de zaîr (Maroc occidental) (Rabat, Maroc: Thèse de Doctorat National, Université Mohamed V, Facultés des Sciences), 258.
Lazarus M., Mazur J., Wszałek-Rożek K., Zwolicki A. (2021). How environmental stressors affect reproductive potential in a saltmarsh plant species Plantago maritima. Ecol. Evol. 11, 3274–3285. doi: 10.1002/ece3.7277
Low B. S. (1996). Behavioral ecology of conservation in traditional societies. Hum. Nat. 7, 353–379. doi: 10.1007/BF02732899
Mangambu M., Van Diggelen R., Mwanga Mwanga J.-C., Ntahobavuka H., Malaisse F., Robbrecht E. (2012). Etude ethnoptéridologique, évaluation des risques d’extinction et stratégies de conservation aux alentours du parc national de kahuzi biega en R.D. Congo. Rev. int. géol. géogr. d'écol. tropicales 36 (1/2), 137–158.
Mehdioui R. (2008). Etude ethnobotanique et socio-économique auprès de la population des communes d’Imi N’Tilt et d’Imgrade (Province d’Essaouira, maroc) (Rabat, Maroc: Thèse de Doctorat National, Université Mohamed V, Facultés de Sciences), 166.
Nzuki B. F. (2016). Recherches ethnobotaniques sur les plantes médicinales dans la région de mbanza-ngungu, RDC (Belgique: Thèse de Doctorat (PhD), Faculté des Sciences en Bio-Ingénierie, Université de Gand), 349.
Ouachinou J. M. A. S., Dassou G. H., Idohou R., Adomou A. C., Yédomonhan H. (2019). National inventory and usage of plant-based medicine to treat gastrointestinal disorders with cattle in Benin (West Africa). South Afr. J. Bot. 122, 432–446. doi: 10.1016/j.sajb.2019.03.037
Philips O., Gentry A. H. (1993). The useful plants of tambopata, Peru, II statistical hypothesis tests with a new quantitative technique. Econ. Bot. 47 (1), 33–43. doi: 10.1007/BF02862204
Posthouwer C., Verheijden T. M. S., van Andel T. R. (2016). A rapid sustainability assessment of wild plant extraction on the Dutch Caribbean island of St. Eustatius. Econ. Bot. 70, 320–331. doi: 10.1007/s12231-016-9356-9
Pouliot M., Treue T. (2013). Rural People’s Reliance on Forests and the Non-Forest Environment in West Africa: Evidence from Ghana and Burkina Faso. World Dev. 43, 180–193. doi: 10.1016/j.worlddev.2012.09.010
R Core Team (2017). A language and environment for statistical computing (Vienna, Austria.: R Foundation for Statistical Computing). Available at: https://www.R-project.org/.
Reyes-García V., Huanca T., Vadez V., Wilkie D. (2006). Cultural, practical, and economic value of wild plants: A quantitative study in the Bolivian Amazon. Econ Bot 60, 62–74. doi: 10.1663/0013-0001(2006)60[62:CPAEVO]2.0.CO;2
Salhi S., Fadli M., Zidane L., Douira A. (2010). Etudes floristique et ethnobotanique des plantes médicinales de la ville de kénitra (Maroc). Lazaroa 31, 133–146. doi: 10.5209/rev_LAZA.2010.v31.9
Shapi M., Matengu K., Mu Ashekele H. (2009). Indigenous knowledge system pilot study - oshikoto region (University of Namibia, Windhoek: Multidisciplinary Research Centre).
Sharafatmandrad M., Khosravi Mashizi A. (2020). Ethnopharmacological study of native medicinal plants and the impact of pastoralism on their loss in arid to semiarid ecosystems of southeastern Iran. Sci. Rep. 10, 15526. doi: 10.1038/s41598-020-72536-z
Sinsin B., Djègo J., Adomou A., Houéssou L. (2009). Etude ethnobotanique des forêts classées de goungoun, de sota et de la rôneraie de goroubi au bénin (Bénin: Rapport d’étude Cerget-Ong/PGFTR), 91.
Tamboura H., Kaboré H., Yaméogo S. M. (1998). Ethnomédecine vétérinaire et pharmacopée traditionnelle dans le plateau central du Burkina Faso: cas de la province du passoré. Biotechnol. Agronom. Société Environ. 2 (3), 181–191. Available at: https://popups.uliege.be/1780-4507/index.php?id=15886.
Tardio J., Pardo-de-Santayana M. (2008). Cultural importance indices: A comparative analysis based on the useful wild plants of southern cantabria (Northern Spain). Econ. Bot. 62, 24–39. doi: 10.1007/s12231-007-9004-5
Tuttolomondo T., Licata M, Leto C, Savo V, Bonsangue G, Gargano ML, et al. (2014). Ethnobotanical investigation on wild medicinal plants in the monti sicani regional park (Sicily, Italy). J. Ethnopharmacol. 153, 568–586. doi: 10.1016/j.jep.2014.02.032
Upadhyay B., Singh K. P., Kumar A. (2011). Ethno-veterinary uses and informants consensus factor of medicinal plants of sariska region, rajasthan, India. J. Ethnopharmacol. 133, 14–25. doi: 10.1016/j.jep.2010.08.054
Vandebroek I., Van Damme P., Van Puyvelde L., Arrazola S., De Kimpe N. (2004). A comparison of traditional healers’ medicinal plant knowledge in the Bolivian Andes and Amazon. Soc. Sci. Med. 59, 837–849. doi: 10.1016/j.socscimed.2003.11.030
Van de Waal D. B., Elser J. J., Martiny A. C., Sterner R. W., Cotner J. B. (2018). Editorial: Progress in ecological stoichiometry. Front. Microbiol. 9. doi: 10.3389/fmicb.2018.01957
Voeks R. A. (2004). Disturbance pharmacopoeias: Medicine and myth from the humid tropics. Ann. Assoc. Am. Geogr. 94, 868–888.
Vorrath J., Voss M. (2019). The hidden dangers of falsified and substandard medicines: developing countries are most affected by the illegal trade. (SWP comment, 25/2019) (Berlin: Stiftung Wissenschaft und Politik-SWP Deutsches Institut für Internationale Politik und Sicherheit). doi: 10.18449/2019C25
Yaoitcha A. S. (2016). Biologie de la conservation des plantes ligneuses médicinales au bénin (République du Bénin: Diversité, Vulnérabilité et Priorisation, Thèse de Doctorat, FSA/UAC), 194.
Yoro B. M. (2012). Pluralisme thérapeutique et recours aux soins en milieu rural ivoirien: Approche méthodologique. Recherches Qualit. 31 (1), 47–61. doi: 10.7202/1085022ar
Keywords: open ecosystems management, traditional medicine, knowledge source, phytodistrict, species availability
Citation: Ahoyo CC, Salako KV, Houéhanou TD, Montcho I, Glèlè Kakaï RL and Houinato MRB (2023) Sociodemographic, environmental and biological factors affecting uses of plants from open ecosystems: Insights for improved livelihoods and biodiversity conservation. Front. Conserv. Sci. 4:1127567. doi: 10.3389/fcosc.2023.1127567
Received: 19 December 2022; Accepted: 15 February 2023;
Published: 24 March 2023.
Edited by:
Orsolya Valkó, Hungarian Academy of Sciences, HungaryReviewed by:
Lukasz Luczaj, University of Rzeszow, PolandEmin Ugurlu, Bursa Technical University, Türkiye
Copyright © 2023 Ahoyo, Salako, Houéhanou, Montcho, Glèlè Kakaï and Houinato. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Carlos Cédric Ahoyo, YWhveW9jYXJsb3NAZ21haWwuY29t