 Esi E. Thompson
Esi E. Thompson- The Media School, Indiana University, Bloomington, IN, United States
The Ebola outbreak in 2014–2016 was the worst of its kind. Its end has been credited in part to community level communication and engagement. But scholarship has not focused much on community members agentic sensemaking expressions and processes during the outbreak. This study focuses on a Liberian community members’ agency in their sensemaking communicative processes that constituted their lived negotiations of health and wellbeing during the Ebola epidemic. The study reconstructs the narratives and reflections of community members in disease outbreaks to show how these reveal their expressions (or suppressions) of agency and quest for survival and life sustenance. Using data from in-depth interviews and focus group discussions, the study provides a conduit for foregrounding local interpretive frames into mainstream discourses through the reinterpretations of expressions of agency. The findings suggest that community members are not agentless, but their agency is enacted within constraints preceding and exacerbated by the Ebola outbreak and expressed within existing structures and knowledge economies about culture and health. The agency of community members needs to be understood and harnessed for health communication.
1 Introduction
The 2014–2016 Ebola outbreak in Liberia caused much mortality, pain, mistrust, and general unrest. This was worsened by the absence of a vaccine at the time (Buseh et al., 2015), the novelty of the virus to the West African sub-region (Thompson, 2020), and general limited knowledge about the Ebola virus in urban areas (Gatherer, 2014).
Extant studies have focused on the economic, biomedical, sociological, and clinical impacts of the outbreak (Nyenswah et al., 2016; Richardson et al., 2020). Decision and judgment scholars have also shown how individuals perceived their risk to Ebola (Sridhar et al., 2016; Sumo et al., 2019; Thompson, 2020). Other studies have analyzed the cultural and structural issues at play during the Ebola outbreak (Fairhead, 2014; Dionne, 2014; Wilkinson and Leach, 2014), moving the discussion away from the biomedical interventions and explanations that have characterized health communication research.
However, scholarship has not focused on the agency of community members and the communicative processes adopted by such marginalized communities during the outbreak. To be sure, making sense of an outbreak is not a monolithic linear process that leads to a particular end; rather it is a complex, fluid, and iterative process that is influenced by and influences historical and prevailing systems, structures, and processes to sustain health and life.
The purpose of this study is to explore the agency of Liberian community members through their sensemaking and reflections about their experiences during the Ebola outbreak. This approach provides a conduit for grounding local narratives within mainstream discourse about responses to disease outbreaks. The study focuses on reconstructing these narratives to show how they reveal community members expressions (or suppressions) of agency and quest for survival. In doing so, the study throws light on how community members made decisions about life, protecting themselves and their communities, while advocating for their health.
Although the Ebola outbreak in Liberia ended in 2016, lessons from the outbreak provide opportunities for understanding how peoples’ experiences and responses to outbreaks such as the Covid-19 outbreak, reflect their expressions of agency within novel outbreaks. Such contextual insights are needed to know how to engage individuals or communities that may be viewed as “resistant” or hesitant. I respond to the call for including the voices of the affected marginalized communities in mainstream discourse about the Ebola outbreak (Sastry and Dutta, 2017).
The study conceptualizes agency and its expression within a sensemaking process that constrains and is constrained by lived realities. It also brings the perspective of community members into knowledge production. Additionally, the value of community narratives to health promotion research and practice cannot be over emphasized.
1.1 The context
Liberia is a West African country that returned to democratic rule in 2005 after a 14-year civil war. The country has since enjoyed relative peace. The young democracy is making structural and governance reforms (Agenda for Transformation 2012). It is home to 40% of Africa’s natural rain forest and the economy is driven by iron ore and rubber (www.moci.gov). The United Nations categorizes Liberia as one of the least developed countries in the world (UNCTAD, 2015, UN Department of Economic and Social Affairs). The health sector is dependent on donor funding with many of the health facilities managed by non-governmental organizations. The country implemented its basic package of health services (BPHS) in 2008 (MOHSW, 2011) and then the essential package of health services in 2011 (Downie, 2012). In spite of these, utilization of health services and health outcomes are low due to reasons including lack of skilled human resources, lack of drugs in government facilities, and high out-of-pocket payments. Lack of adequate potable water and sanitation, electricity, and corruption worsen the health situation. It was in such a context that the Ebola virus hit the country (Thompson, 2017).
The first Ebola virus case in Liberia was reported on March 30, 2014, in Foya district within Lofa county (WHO, 2015). With a mortality rate of 25 to 90% and no known vaccine at the time (WHO, 2016), the Ebola virus disease was fatal. When no new cases were recorded by April, it was assumed that the outbreak had slowed down (WHO, 2015) only for the disease to spread to densely populated cities, including Monrovia, totally overpowering the health system by June. By the time the international community responded in September, the outbreak was out of control.
Such was the context in which community members had to make decisions and negotiations about health and wellbeing. The outbreak in West Africa was declared over in 2016 with a recorded 11,323 deaths and 28, 646 confirmed, probable or suspected cases (WHO, 2016).
2 Conceptual framework- Agentic perspective
Agency is critical to any endeavor and reflects the capacity to make decisions especially with regards to health and social experience. Although broader conceptions of agency such as the “hybrid” perspective view agency as the capacity (both human and non-human) to act (Börner et al., 2021), in this study I focus on human agency- the human capacity to act (Ahearn, 1999). Hitlin and Elder Jr (2007) identify four main overlapping ideal types of agency common to the human endeavor. These are existential (used in all circumstances), pragmatic (used in novel situations), identity (used in routine situations) and life course agency (used in life pathways to retrospectively analyze decisions made). This view of agency is more focused on agency at the personal level.
In conceptualizing agency, I draw from Bandura’s (2001, 2) broad view of agency as “embod[ying] the endowments, belief systems, self- regulatory capabilities and distributed structures and functions through which [personal] influence is exercised,” in the human quest to achieve meaning and satisfaction in life. He suggests that there are certain features that guide action as expressions of agency (Bandura, 2018). These are forethought, self-reactiveness, and self-reflectiveness. Forethought explains reflecting on and visualizing goals and expected outcomes and creating plans of action which provide direction. This process of internal dialog is viewed as foundational to all communication processes. Self-reactiveness defines the process of self-regulating and evaluating behavior and actions against adopted standards, and then self-reflection explains the process of reflecting on the adequacy of one’s action, thought, motivation, and pursuits to course correct. This process may start with internal dialog and could evolve into other forms of communication action or behavior (verbal, mass, interpersonal, group etc.; Cunningham, 1992). Bandura’s Agentic perspective then, is at the very basis a communicative process of sense-making.
Although not in this latest iterations, Bandura’s initial conceptualizations (Bandura, 2001) included a fourth feature known as intentionality, which referred to the plans and strategies that people choose and make to achieve an outcome. Generally, people are incentivized to act if they believe the action will lead to desired results (Bandura, 2001), and they believe in their ability to take or refrain from taking the action.
Agency is expressed and enacted in sociocultural or linguistic contexts. Therefore, discussions about agency should be grounded in actual human experience (Hitlin and Elder, 2007). In the current project, I explored community members’ agency using Bandura’s (2018) conceptualization of agency features, and Hitlin and Elder’s (2007) pragmatic and life course ideal types. Pragmatist agency “is expressed in the types of activities that are chosen when habitual responses to patterned social actions break down.” In such situations we “make choices within the flow of situated activity, and emotions and personality traits — along with idiosyncratic personal histories, moral codes, and predispositions—influence the choices we make in emergent situations” (Hitlin and Elder, 2007, p. 178). The Ebola outbreak was a novel situation within which individuals had to find ways to attain their needs and wants and achieve their goals.
Bandura (2001) also presents three modes of human agency where the features of agency are all exercised: personal, proxy and collective. Personal agency is when people individually and directly take action on controllable activities in their environment for themselves. However, in situations where people do not have control over a situation, they may resort to proxy agency, a mediated form of agency where they try to get others who have the resources to act to get their desired outcomes. Then there is collective agency where people cooperatively act in their shared interest. Each of these modes is required for success in different circumstances.
Bandura’s agentic perspective allows for exploring the sense-making process of community members and the opportunity to reflect on the entire process of expressing agency. A focus on agency engages with structure and practices because as Giddens (1984) structuration theory suggests, agency and structure (rules and resources in one’s environment) produce social practices or what health communicators might refer to as behavior.
While much scholarship on the Ebola outbreak was on health workers sacrifice and heroism (Belfroid et al., 2018; Gee and Skovdal, 2018; Perry et al., 2016; Raven et al., 2018), the narratives of local populations in enacting everyday agency in response to the disease outbreak is mostly missing (Sastry and Dutta, 2017). This study looks at expressions of agency and the communicative processes adopted during a virulent disease outbreak. By focusing on the agency of community members in Liberia, I bring the narratives and personal experiences of these community members into the discourse of an outbreak, to foreground realities within which they experienced the outbreak, and which influenced their decisions and choices. The main research question guiding the study is:
RQ 1: How do community members’ sensemaking of their experiences reflect their agency during the Ebola outbreak?
3 Methods
3.1 Approach, sample, and respondent selection
The study adopted a qualitative approach using in-depth interviews and focus group discussions with community leaders and members in the Mambah Kabah District in Margibi county, Liberia. The qualitative approach was rooted in social constructionism (Charmaz, 2006) to enable the researcher to center community members’ emotions, cultural, and social dynamics and understandings of the Ebola epidemic. This study received approval from the researcher’s institutional review board (redacted for peer review; RCS 05112016.022) as well as the Ministry of Health of Liberia and forms part of a two-country study on communicating about a public health crisis. The data presented here has not be previously published. The author is a West African indigene and has conducted risk and health communication research in Liberia and Ghana, but currently resides and works in North America.
3.2 Population and sampling
Although Margibi county (the county of focus) is host to Firestone company, the largest contiguous rubber plantation in the world (https://www.firestonenaturalrubber.com/), and the only international airport in Liberia (Roberts International Airport), the county is still very deprived. The 2000 census suggests that apart from Montserrado county, it takes an average of 80 min to commute to the nearest health facility in all other counties. Low literacy levels (44%), inadequate medical supplies, trained personnel, and infrastructure affect health delivery quality and quantity (Buseh et al., 2015). In addition, at that time, Liberia had only one laboratory that could perform Ebola tests on samples (Nyenswah et al., 2016). When the epidemic hit, these existing systemic factors contributed to delays in the response from government and disbelief on the part of respondents.
I selected the Margibi country because it was one of two counties that had towns placed under a 21-day quarantine during the Ebola outbreak. The communities of focus also received the full range of Ebola interventions. Furthermore, during data gathering there were active outbreaks within the community making the issue relevant and salient for community members. Purposive and criterion sampling were used in selecting respondents for the study. I was interested in community members, 18 years and above who were in the community during the active Ebola outbreak phase from 2014 to 2016.
After receiving permission from the Ministry of Health, the district leaders, and the county leaders, I worked with a community volunteer to approach the chief and clan leaders in the communities of focus. Respondents were from the catchment areas served by the Dolotown health center (23 communities, with a total population of 9,494) and the Unification Town health center (15 communities with a total population of 9,739). I worked with a community volunteer to make announcements at the markets, community events, and the health centers inviting participation. Working with a community volunteer enabled me to tap into the community resources and networks. Those who were interested and fit the inclusion criteria reached out and I provided more information about the project. The respondents for both the in-depth interviews and focus group discussions straddled the role of both informants and respondents by providing responses to questions, as well as explaining their settings, culture, experiences, and actions related to the Ebola epidemic (Gabor, 2017; Lindlof and Taylor, 2019; Morse, 1991). Data gathering occurred in August and September 2016 when the outbreak had subsided, but active cases were still ongoing in the county. The demographic breakdown of participants is presented in Table 1.
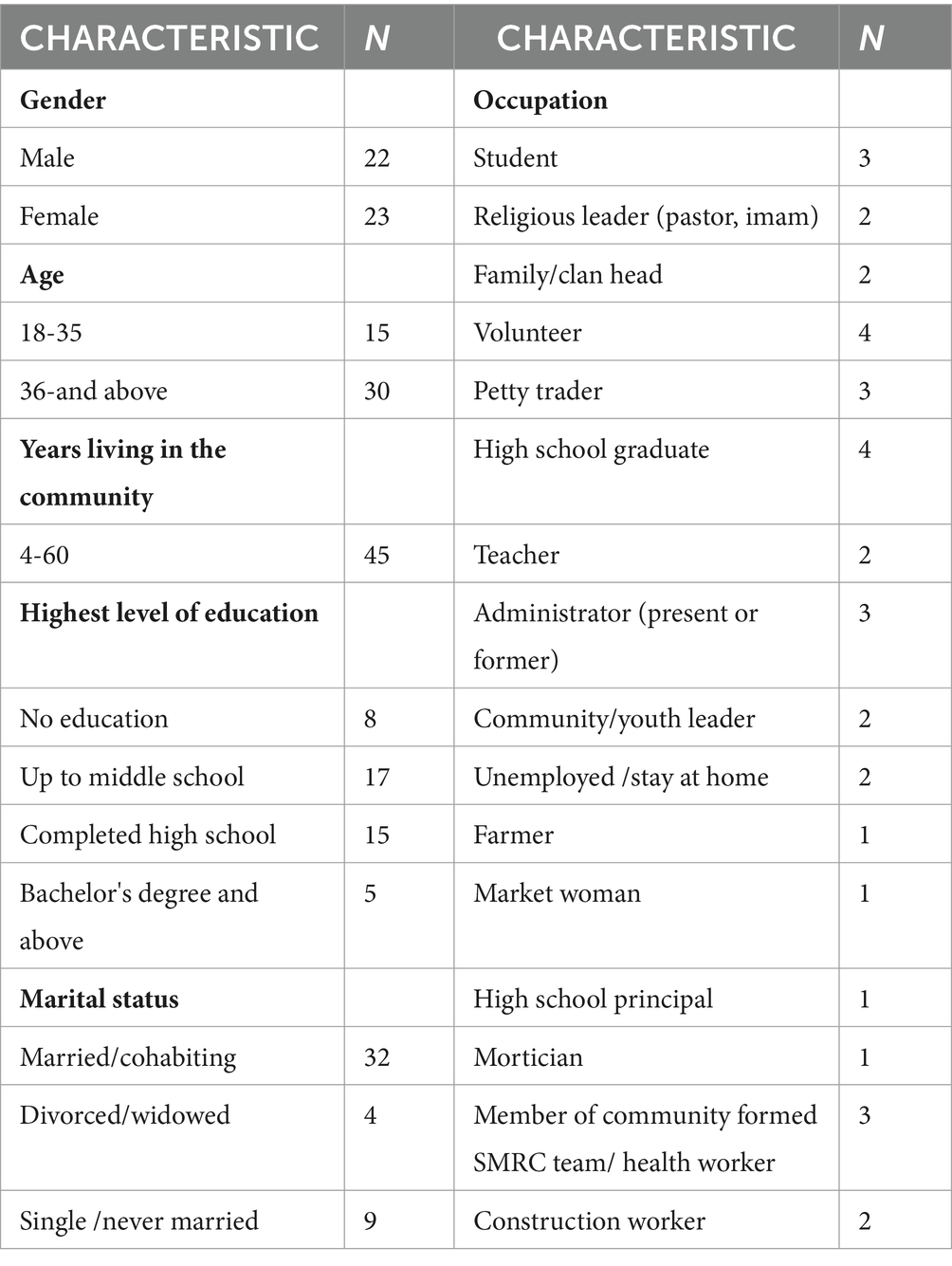
Table 1. Characteristics of respondents
3.3 Focus group discussions and in-depth interviews
I held three focus group discussions made of up of 10 participants each. This was to ensure that we had homogenous enough groups of males, females, and youth as a starting point for data gathering. The insights from the initial focus group discussion formed the foundation for further exploration in the in-depth interviews (both individual and dyadic interviews). I had one group of adult women (36 years and above), a group for adult men (36 years and above), and a group of male and female youth (young adults 18–35 years). After the purpose of the meeting was explained, each participant provided verbal consent to participate and for audio recording to be done. The meetings lasted between 60 and 90 min. A semi-structured discussion guide with open-ended items guided the discussion and conversation process. I conducted the discussions in Liberian English and the meetings were held at the Unification Town health center.
I also conducted in-depth interviews with 15 community members who were not part of the focus group discussions. We started the interviews with individuals and dyads recommended by the focus group participants as well as sources of primary information and experiences within the community. Interviews were discontinued when no new information was received regarding the research question. Each interview lasted between 45 and 90 min. Interviews were held at locations of the participants choosing including homes and a public school.
3.3.1 Interview/focus group guide
The semi-structured interview/discussion guide focused on (1) Initial exposure to the outbreak and outbreak (2) Information received during the initial exposure (3) Personal and familial actions and experiences for self-preservation during the outbreak (4) Reflections about actions, behaviors, and practices and responses during the outbreak. Initial questions for the guide were drafted by the researcher and shared with members of the Ebola social mobilization and risk communication sub-committee. These were discussed with the county leader, clan heads, and chiefs in the initial meeting. They suggested changes and modifications which were implemented before data gathering begun. The semi-structured nature of the guides allowed for the exploration of issues that participants raised but were not captured in the guide.
After the sessions, participants were provided with their refreshments and their transportation. Participants who could read and write in English provided written consent after reviewing the consent form. For Participants who could not read and write in English, the consent form was read and explained to them, and they provided verbal consent as per the approved protocol.
3.3.2 Sensemaking for data gathering and analysis
The constructivist approach utilized Weick et al. (2009) sensemaking as organizing. Sensemaking “unfolds as a sequence in which people concerned with identity in the social context of other actors engage ongoing circumstances from which they extract cues and make plausible sense retrospectively, while enacting more or less order into those ongoing circumstances” (Weick et al., 2009, p. 83). They add that sensemaking is, “an issue of language, talk, and communication through which meanings materialize” (p. 84). People tend to engage in intentional sensemaking when the current circumstance is different from what they expect. They thus look for ways and reasons to help them get back to the former activity. These reasons could be drawn from expectations, plans, structural constraints, social norms etc. In this way, sensemaking is viewed as an interplay of [in] action and interpretation (Weick et al., 2009, p. 84). Organized sensemaking involves, bracketing, labeling, and categorizing, and is retrospective, social and systemic. The focus is on what, why, and to what effect people construct their life worlds.
Sensemaking guided the data gathering and data analysis process. Participants, through the process of interviewing and focus group discussions, retrospectively processed their Ebola experiences, bracketed various experiences, labeled them, assigned meanings and interpretations to their (in) actions during the Ebola outbreak. The author, on the other hand, reflected on the participants narratives and engaged in a process of bracketing, labeling, categorizing and assigning meaning to them.
3.4 Analysis
I used an interpretivist-constructionist approach in data analysis (Charmaz, 2006). Data analysis started in the field with the transcribing of the three focus group discussions and 15 individual in-depth interviews. They were transcribed into English and back translated to check the authenticity. The transcription process enabled me to familiarize myself with the data. The analysis involved a constructivist approach that adopted the iterative process in grounded theory to move between data, interpretation, and conceptualization. In analysis, I followed Braun and Clarke’s (2006; 2014) thematic analysis steps in an iterative process (similar to grounded theory traditions) due to its flexibility. I generated initial codes, then searched for, and generated themes from the codes and the original data, reviewed the themes and then defined and named the themes in an iterative manner.
The three major related themes show a progression of how participants expressed their agency from their initial exposure to the outbreak (resisting agency), through living through the outbreak (repressed, suppressed, and subverting as agency) and taking actions against the outbreak (taking initiatives). I used pseudonyms to protect the identity of participants. Table 2 presents an example of how I moved from data to themes.
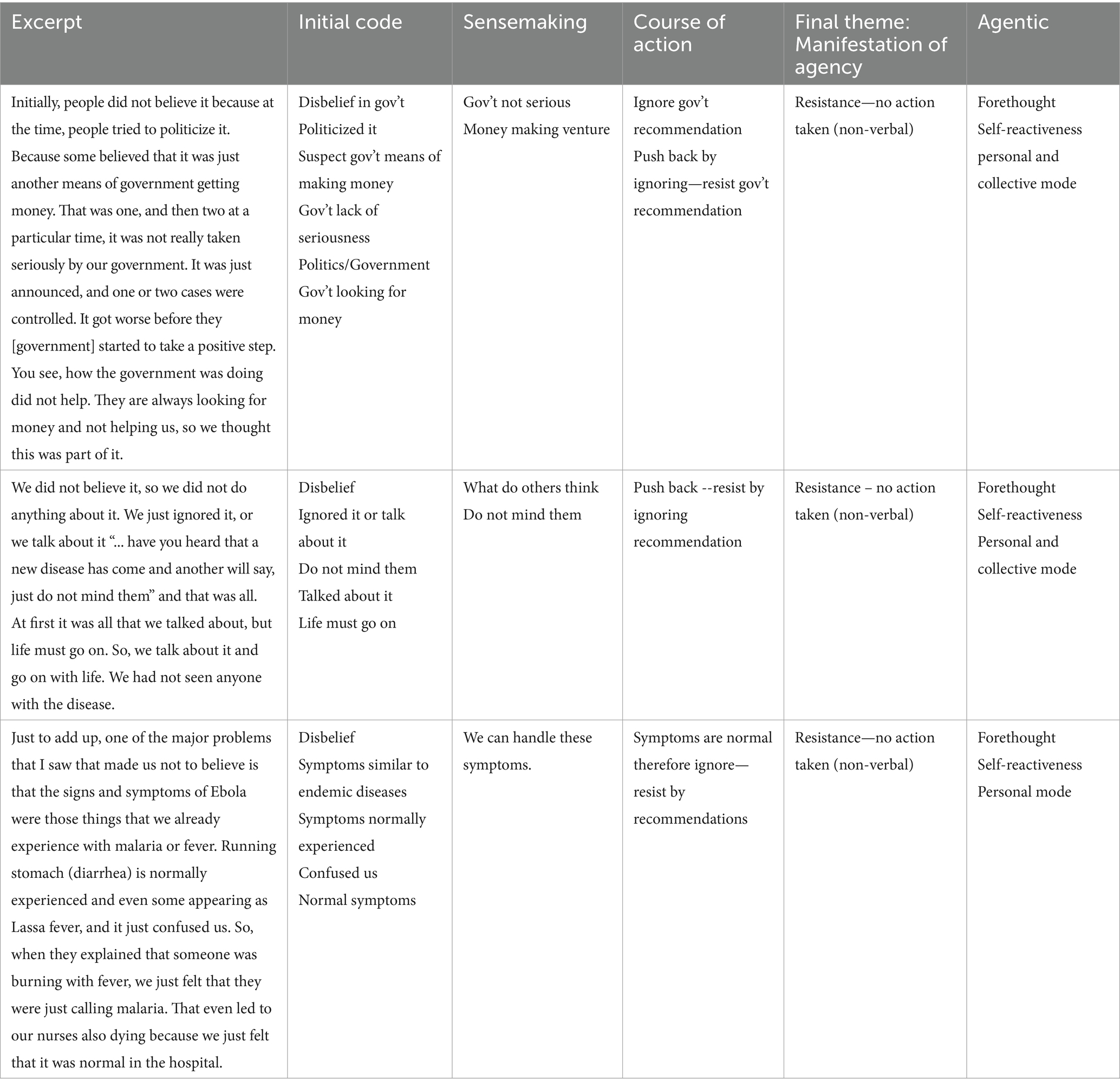
Table 2. Example of data analysis process from data to theme.
4 Findings
Participants discussed various factors, that influenced the expression of agency in their lived experience with Ebola. The three main themes identified from the narratives and discussed below are resisting as agency, repressed, suppressed and subverting as agency and taking initiatives.
4.1 Resisting as a form of agency
Participants shared that initial reports about the Ebola virus in Liberia were met with disbelief and suspicion because they had no previous experience with the disease. Many community members at the initial stages doubted the existence of the virus. Consider the response of a member of the male focus group:
John (FGD): Initially people did not believe it because at the time, people tried to politicize it. Because some believed that it was just another means of government getting money. That was one, and then two at a particular time, it was not really taken seriously by our government. It was just announced, and one or two cases were controlled. It got worse before they [government] started to take a positive step.
Mamawey (IDI): We did not believe it, so we did not do anything about it. We just ignored it, or we talk about it… “have you heard that a new disease has come?” and another will say, “just do not mind them” and that was all.
Here, attribution to the central government and politics points to the embeddedness of politics and deep-seated mistrust to the everyday lived realities of community members. They thus looked to political leaders to get a sense of how they should respond to the outbreak. The perception of a seeming lack of proactive and urgent attention by the government and the perception that it was a money-making ploy, gave the impression that the outbreak was not real and did not require action. Therefore, people did not take any of the required precautions. This act of not taking any action and continuing “life as usual” was a non-verbal response to the doubts they had about the reality of Ebola. Their view of the central government as “only out to get money” and “not taking [the outbreak] seriously” influenced the decision to not take the recommended behaviors. Here, we see that people may choose not to take recommended action as a non-verbal communication expression of agency based on their assessment of the situation. This form of resistance may be guided by their determination of their purpose, their evaluation of the source of the communication, and their engagement with others within their context. This reflects Bandura’s self-reactiveness where they evaluate the actions against standards. In this case, the standard was the response of the central government. Agency is therefore expressed as resisting recommended precautions by not taking action against possible infection based on the perception of the governments’ response.
Another way in which community members made sense of the initial reports about the outbreak was by using their experience with similar disease symptoms. Ebola symptoms (severe headaches, stomachache, vomiting, stooling etc.) are similar to the symptoms of endemic diseases in the community. In explaining this association, respondents viewed these endemic diseases including malaria, cholera, and Lassa fever as normal diseases and their symptoms are normal.
Beatrice (FGD): Just to add up, one of the major problems that I saw that made us not to believe is that the signs and symptoms of Ebola were those things that we already experience with malaria or fever. Running stomach (diarrhea) is normally experienced and even some appearing as Lassa fever, and it just confused us. So, when they explained that someone was burning with fever, we just felt that they were just calling malaria. That even led to our nurses also dying because we just felt that it was normal in the hospital.
Viewing diseases such as cholera and malaria as normal in a context of limited health resources, was a process for members on the margins of society to deal with the challenges of accessing services for endemic diseases. Equating Ebola with endemic diseases was a way for the community members to normalize the “new disease.” “Normal” then, is an expression of agency in response to dealing with prevailing health challenges despite the severity and morbidity of the diseases. Furthermore, explaining away the symptoms Ebola as normal, provided the impetus to resist the communication and announcement of the central government and not to take precaution nor the recommended behaviors. That means if the symptoms we are seeing are symptoms we are familiar with, then we do not need to take any action recommended by the government. This form of resistance is guided by the social and structural realities in the context. By viewing the symptoms of Ebola as those of endemic diseases, community members were enacting agency by making sense of the outbreak in the midst of limited information and seeming disengagement of political leaders. This type of normativity is one that helps community members to deal with the structural challenge of inadequate health resources and infrastructures by reinforcing local hegemonic discourses of disease symptoms.
Another form of resistance agency was expressed in the form of pushing back against the government instituted restrictions on burials during the outbreak by secretly burying loved ones. The increased risk of infection during traditional burial practices led to the banning of all funerary practices. The President of Liberia instituted a policy of cremating all dead bodies and burials were to be done exclusively by burial teams. These policies were culturally foreign to community members as the excerpt below indicates.
Cooper (IDI): It was a question of “you mean I am going to die, and I will not have a memorial spot?” Initially the government had come out that every dead body should be cremated. They started burning at the crematorium in Margibi county, but then people saw that as cruelty. For Africans, when someone dies, they still feel as long as the person’s body is around, they are somehow connected. Then Christianity comes to say that we are all members of the communion of Saints. So, when a person is put in fire, it is almost like you are going through final judgement, like the person is turned over to hell. So, they hid their loved ones and buried them at night.
In many societies, religion and culture are systems for communicating and coping with pain, trauma, and transitions. In situations where structural issues make it challenging for daily life to be completely enjoyed, cultural and religious practices such as death and funerary ceremonies become agentic ways for community members to build their identity, familial and community cohesion, and are necessary for negotiating health and well-being. However, with Ebola such agency could no longer be expressed because they involved direct contact with dead bodies.
Added to that was the institution of cremation and burial teams that buried any person that died during the Ebola period irrespective of the cause. Ebola was therefore associated with death and total separation; one which community members could not navigate within the constraints of the restrictions of the epidemic; one within which community members had no agency for acting; one which was foreign and did not connect with what community members were used to. To take back some of the lost agency, family members engaged in secrete burials at the risk of spreading infections. Secret burials should be viewed as an expression of agency and not isolated rebellion against biomedical interventions. Secret burials and hiding sick relatives should therefore be framed an expression of resistance agency within the ambit of such a context.
The narratives above reflect the verbal and non-verbal practices (both individual and communal), through which respondents expressed their agency in varying forms of resistance, similar to what others have documented in other health contexts (Basu, 2017; Day et al., 2010; Koenig, 2011). They reflect agency expressed as pushing against structurally imposed challenges.
4.2 Repressed, suppressed and subverting agency—isolation and quarantine as triggers
Participants’ narratives also focused on the ways in which their agency was suppressed and how they subverted these constraints. Dolotown was one of two towns put under 21-day quarantine. Community members described the quarantine process and implementation as instilling fear. Here is how a member of the taskforce presented it:
Weah (FGD): We had the Armed Forces of Liberia (AFL), Police Support Unit (PSU), Emergency Response Unit (ERU) Immigration and indeed all security apparatuses here in full gear and fully armed. This brought a lot of fear. The first fear was that they gave a scenario about a community that was affected by the virus. They said because the government did not want it to spread across the entire country, they had to destroy the community. So, when we heard about the quarantine, people were escaping by other means. A lot of people left the community, but they caught other people in the community; so that was the fear. And secondly, seeing people armed—because they [security forces] surrounded the community by 4 in the morning. So, by the time community dwellers got off their beds, they started seeing armed men around who started instructing them to go back indoors and not to get out.
Violence and intimidation were the main outcomes that participants described from the quarantine experience. Such systemic modes of enforcing power served to deprive a community of any little agency they had, instilled fear, and a constant reminder of a not-so-distant past of war and bloodshed.
Doe (FGD): And our central government quarantined us, and they sent armed men; the soldiers were armed; the police were armed where we were quarantined. There was no food. It was as if the civil war was happening again. It brought back memories of the war with the guns and everything.” You cannot move freely; they were beating and pushing people.
Added to that was the lack of food and water which made people break their quarantine and flee the community. The lockdown measures forced these community members to forsake their socio-economic support systems and patterns of living to avoid infection, but with no means of survival during the period. Families that were facing socio-economic difficulties prior to the outbreak now faced an even dire situation. In the interview with a male youth leader, he explained the situation thus:
Morris (IDI): You know the virus was in the country already and so people were not doing their normal business. And you know people sell on a daily basis; in the morning you sell, by 12 noon, you have a little something to buy your food. But by then [the time of the quarantine] everything was cut off meaning there was no food and people were starving. So, to have them confined with no food and starving, it was just a difficult situation to accept. At the end of the day, people were making their way out of the community. Some of them were arrested, they were treated harshly, beaten, or forced to go back. It was challenging. Later the government came in with food and resources.
For the security personal and health administration, quarantine was a containment measure to prevent the disease from spreading. But for the community members, without food and other resources, quarantine was not only a move to curtail personal freedoms, but it also communicated historical images and psychological trauma of the civil war causing mental and psychological turmoil. It also exacerbated socio-economic challenges that had arisen at the start of the outbreak. The quarantine enforcement thus reppressed the agency that the community members had in providing for their socio-economic upkeep. The narratives also show that the Ebola outbreak exacerbated existing structural and socio-economic constraints within which community members made health and life decisions and around which they had to make negotiations to survive.
As was explained in the “context section” existing systemic and structural factors became aggravated by the outbreak. These structural and political economic factors such as systemic poverty, lack of infrastructure, lack of medical resources and personnel, and illiteracy may explain the varied expressions of community members’ agency during the outbreak. These structure-related issues create an environment where the health decisions of community members are made within the constraints of what is possible to maintain life and livelihood.
These structural constraints also manifested within the community level with regards to isolation. When a person/family was suspected of possible Ebola virus infection, they had to undergo a 21-day isolation. The very idea that a person had been isolated for 21 days meant that even after the person or household had been declared Ebola-free, they had to endure a time of social marginalization before the community accepted them. This was in spite of the elaborate reintegration process that the Ebola response team put in place. Consider the experience of a member of the task force:
Morris (IDI): If we suspect that somebody may have died from Ebola in a house, immediately we quarantine [isolate] the entire house for 21 days. If you produce any symptoms during that period, we pull you out and take you to the treatment units. If no symptoms are produced, we go as a team and tell the community that “these people were under observation because of what took place in their home. They are done proving that they have no Ebola. We are asking you, the community leaders, to please welcome them and join them as they reintegrate into the community. They are your brothers and sisters, and their health is just as good as yours.” Of course, there was some stigmatization for some time, but in a month or two, if they see the person moving freely, they know the person does not have Ebola.
This communicative process of reintegration was to convince the community that the people were “safe.” But it seems the process was not enough to curtail the stigmatization that affected individuals and families had to endure. It is therefore important not to downplay the power of stigmatization in causing people to hide their sick loved ones as a subversion of their repressed and suppressed agency.
It seems that stigmatization as collective agency, was almost accepted as a by-product of ensuring the community is safe. Community members and individuals subconsciously (below the level of awareness) engaged in a form of collective agency in a bid to protect themselves and their community. This process in and of itself constrained and suppressed the agency of the affected person or families who had to resort to depending on proxy agency through the task force which I discuss below. The mental and emotional labor that goes into engaging in this process of acceptance and reestablishing communication channels with the community could be huge and drawn-out.
Both quarantine and isolation brought stigmatization. Stigma is explained as a social process of discrediting or isolating individuals or communities perceived as a threat from social acceptance [Goffman, 1963; see Pescosolido and Martin (2015) for a detailed analysis of the concept]. During the Ebola outbreak people (living in quarantined communities or families in isolation) and place (the physical locations) were stigmatized. People from quarantined communities were viewed as carriers of the virus. Ebola was no longer the only disease, but people and place were viewed and stigmatized as “the disease” and embodiment of the disease (Gee and Skovdal, 2018).
But community members also found ways to subvert these restrictions. The excerpt below captures a clan leader’s narrative about their successful agentic attempt to subvert the quarantine process and associated stigma to provide for their family:
Kanneh (IDI): I hid myself in the swamps here and there before I got on the road. But when I got in the car to go Kakata I was afraid. The women at the back of the car started to talk about Dolotown and Ebola. We were almost at the checkpoint when I said, ‘I am coming from Dolotown.’ The two women started to pull their dress like this [gestures to show moving away from a person]. The nearest one to me looked at me and asked, ‘you are coming from Dolotown?’ I said ‘yes.” Then she asked, ‘but how did you get out?’ Then I showed her my mark [a mark put in the index finger of a person whose temperature is normal during the 21-day quarantine] and said, ‘you see the mark they put on my finger? This mark means you can come out.’ It was actually the mark to show that I am from Dolotown and that I could not go anywhere. Yes, so when I entered Kakata quickly I got what I went there for. I passed through the market and hid myself, got on the rubber bushroad and passed through Peter town, through the swamps then I came here. They were catching people, but I was just blessed.
This narrative brings into focus the conditions under which agency is interconnected with the structural constraints of their circumstance. Lack of food and caused this leader to break their quarantine. The response of community members to break their quarantine was then an expression of their agency to get back some of their freedoms and to provide for their family members who were starving. The clan leader’s narrative is interesting in how he communicates a “signal” that should constrain him as the key to his “freedom.” Stigmatization is a form of social control in many cultures (Goffman, 1963). Avoidance and resentment rooted in fear of possible infection are some of the reactions that stigmatized individuals had to deal with. Although stigmatization is often presented in literature as negative, I argue that acts of stigmatization can be viewed as expressions of agency on the part of those who engage in the acts of stigmatizing (stigmatizers). In this case, it was in response to precaution. Therefore, agency can have both positive and negative implications. Quarantine and isolation had their biomedical purpose, but their implementation inflicted structural, emotional, and social damage that community members had to make sense of.
In all, respondents’ narratives reflect how agency can be repressed, expressed or subverted within the limitedness of social restrictions (both structural and communal). The response of community members to break their quarantine was then an expression of their agency to get back some of their freedoms and to provide for their family members who were starving.
4.3 Taking initiatives- acting in support of the community
Participants shared how individuals and groups organically emerged from the community to help in the Ebola fight prior to external support and even the quarantines. These acts of care, which were based on community knowledge and trust, were viewed as the lifeline for the community.
Alice (FGD): Those young people that were on the field, those that volunteered themselves and were working; they were not working for money. In fact, when the GCHV [general community health volunteers] came in, they took people from the taskforce and put them on the GCHV. So, they were like sacrificing freely, free service for the sake of the community. They were really heroes.
Here we see the emergence of collective agency. Young men in the community organized themselves in the face of the increasing deaths to find information about the outbreak. They relied on their knowledge of the community and the trust that community members had in them to communicate and convince community members to take precautions. Although under normal circumstances, the social hierarchy of the community does not allow young people to speak up and act, the presence of a deadly outbreak provided an opportunity for circumventing cultural and social norms in service of the community. The youth used their influence to secure resources for the community to help in the prevention efforts. Consider the excerpt from a taskforce member below:
Jenneh (FGD): In the […] area we had more than 26 people that were sick there and no one was attending to them. We will walk to the market to buy food and get it to them. If you need something, we go to get it for you, so you do not have to go. Sometimes we go to the government officials around and tell them that these people have a need and if you just let them sit there, it means they will come into the community and that will lead to infecting others. So sometimes they would give some money to buy rice and other things for them.
Here, again, we see systemic poverty behind the spread of the virus as infected people or those in their households without resources had to move into the community to get their daily needs. The organic start of the youth taskforce was therefore viewed as tackling a much-needed deficit that the central government was unable to address.
Agency as a form of control and as part of supporting the structure or status quo also comes to play. The task force members were acting in support of the structural requirements (i.e., acting to support what the ruling power required without being asked to) by reinforcing structure and power. Representatives from the taskforce shared their strategy for supporting the Ebola fight in their community.
Kumba (FGD): So, we organized ourselves. After confirming that the symptoms were what we had heard on radio, we started raising funds amongst ourselves to buy the things needed like chlorine because chlorine at the time was scarce. So, we had somebody at Firestone who would supply, and we pay. Voluntarily we had 32 people in the taskforce who were assigned to various quarters in the community. We had to teach them [community members] what we had heard on radio. We even had to show them how to mix the chlorine solution because they did not know how to mix the solution.
The agency of the task force members in seeking information from radio as self-education to become the sources of information and communication for the community members is also worthy of note. These information seeking actions increased their understanding and made them communication channels for the community. With the task force advocating for resources and support for households in quarantine or isolation, they became the main means of securing help for individuals who would otherwise not receive any help.
The expression of this form of collective and proxy agency was not without its challenges because there was still mistrust and denial about the virus. Being young people without power (economic and political influence) in the community, the members of the taskforce connected with the chiefs and clan leaders to legitimize their efforts. An Ebola survivor explained how the support of the task force was instrumental to her family:
Melvana (IDI): The task force used to tell us ‘Do not visit a sick person. When you have a dead body, the task force will come and call the burial team and they come and take the body. They were the only people that helped me when my family got sick. There were six of us (in my family), but we are left with two.
The government relied on the structures created by the Ebola task force to leverage efforts and to scale up. However, herein lies the challenge: when the health ministry included these local groups in their interventions, the unique role and contribution of these organic groups were subsumed. Inclusion of such structures within larger interventions have to be done in a way that maintains the perspective and agency of these marginalized groups.
Besides the youth group forming a taskforce, individuals within the community also took initiatives. A case in point was the setting up of an Ebola burial team by a mortician and funeral homeowner. Unlike the taskforce, the mortician and funeral homeowner had both political and socio-economic influence. Additionally, he had expertise in handling dead bodies, and this is what legitimated the expression of his agency and the burial team’s acceptance by the community. He explained his motivation thus:
Sando (IDI): People were dying, and we depended on one burial team to handle over 30,000 square miles, which is the area space of Liberia. It would take days, if not weeks for the body to be picked. We were all in the community and people who love their loved ones were touching them (dead bodies) and they were getting sick and dying. I took people from the funeral home, and some other boys who used to assist in cemetery excavation and I trained them in how to protect ourselves. Because we deal with tropical cases like tuberculosis and cholera, we had some protective gear. So, we started using them and picking up dead bodies from the community. Later, the MOH, and the superintendent’s office, provided some PPEs (personal protective equipment) and we started collaborating with the county health team.
The responses of community members and especially the emergence of the taskforce and local burial teams reflect the fact that “human agency emerges in response to the characteristics of one’s structural environment, and structures themselves respond to human agents,” (Sastry and Basu, 2020). Furthermore, participants’ narratives and communicative experiences also offer evidence of how these emergent groups reflect indigenous collective agency where people come together to achieve a common cause and became communication and social infrastructures for community members. The narratives also reflect how interventions can be effective when they recognize and include social structures that are organically developed within communities.
These narratives demonstrate the collective action that individuals and groups took to protect their communities. They also demonstrate how communities can preserve their lives during disease outbreaks, using various strategies, and shaped and influenced by structural and social factors. Importantly, we see that young people who under normal circumstance in hierarchical communities would not be able to take such initiatives, are able to take initiatives and are lauded for their actions. Times of crisis can serve as a catalyst for the emergence and activation of agency in individuals and groups that may hitherto not be expressed.
5 Discussion and conclusion
This study foregrounds the narratives and communicative experiences of community members in Liberia to the 2013–2016 Ebola epidemic. The narratives demonstrate community members’ agency in making sense of the outbreak by adapting, accepting, pushing back, or developing processes to address the outbreak.
The narratives reflect Bandura’s (2018) three features of agency. Community members narratives about their initial responses to the outbreak reflect the communicative process of forethought. Community members reflected on their goals and lifestyles against the communicated need to be wary of a new disease outbreak along with the perception of government’s response and then decided that the news might not be true. Taking the recommended action at that time would have instantly halted all forms of economic and social activities further exacerbating the economic challenges that individuals and community members were going through. Therefore, the disbelief that community members had, and the associated refusal to take recommended precaution reflects their agency in processing information they have received along with all the contextual factors they had to live with. This form of everyday resistance questions the idea that agency is action. Sometimes, agency may be intentional refusal to take an action or refraining from an action based on the individual or communities’ forethought about the courses of action.
Forethought is further reflected in personal agency when the mortician took initiative to set up a burial team and in proxy agency when members of the task force went to elected leaders to solicit for money and other resources. It was also reflected in collective agency when youth in the community came together to form the task force.
In the very process of data gathering, respondents engaged in self-reactiveness (Bandura, 2001) as they evaluated their actions and behavior against adopted standards. The narratives suggest that respondents evaluated their initial response against the information they had. Furthermore, respondents comparing the symptoms of Ebola to those of existing health conditions showed the kinds of evaluations that community members made that led to their (in) actions. Without a clear delineation of the differences in symptoms, the “normativity” of existing health conditions gave respondents the impression that the same conditions were being talked about.
Agency can function as control (stigmatization), or resistance (escaping quarantine, not taking recommended action) or sometimes complicit, in reinforcing hegemonic discourses and practices (submitting to local leadership). In line with Zoller (2003), normative practices such as viewing the symptoms of Ebola as normal can also be viewed as agency that reinforces local hegemonic discourses of disease symptoms.
The process of data gathering provided an opportunity for respondents to engage in individual and communal self-reflection on their (in) actions during the outbreak and to decide what to do going forward. Respondents’ reflections showed the valued they had for the youth who went out of their way to support the community before external help arrived, the burial team that was set up and its effectiveness in taking out infected people from the community, as well as the community health workers who later came with community education. Extreme caution also led to community members subconsciously stigmatizing individuals and families who had been cleared of Ebola or who may have recovered from Ebola. The narratives also showed the various ways in which the agency of respondents was constrained or outright repressed during the outbreak. While some view the quarantine situation as needed and warranted, others view its implementation as problematic and a curtailing of freedoms.
The action of the task force pushes against the normalized discourse about the dependency of minoritized communities on external resources and help. The agency of these task force members may not be at the level of the medical help that was later introduced, but under the circumstance, it provided the support that the community needed. These discourses are missing in mainstream media and academic literature and devalued. However, we need to recognize that these were the actions that sustained the community until biomedical support arrived and they became the foundation for the biomedical and social mobilization approaches.
Additionally, the narratives suggest that health during the epidemic was explained as a series of daily expressions of agency on choices that needed to be made. These choices necessarily meant that some other good option had to be shelved or that health had to take a back seat for other life choices. The choices included staying put and going hungry during lockdown, or trying to find food even if it meant one could get infected or be beaten; believing the virus was real and there was a real danger or believing it was a political ploy or an endemic disease; admitting that a dead loved one may have died from Ebola and risk the body being taken by the burial team or denying the person may have died from Ebola and risk infecting the entire household. In each case, the mode and manner of agency expressed had implications and consequences for one’s health and familial and social relations either negatively or positively.
The study shows the applicability of the Bandura (2018) agentic perspective to disease outbreaks. The study extends studies such as Basu (2017) on sex worker resistance and Meyer (2016) on women’s attempt to manage intimate partner violence to the expression of agency in a virulent disease outbreak. It provides evidence about the dynamic and complicated ways that agency is expressed, manifested, and explained in contrast to the ways, these same (in) actions and behaviors are conceived in Western biomedical literature. In extending scholarship, the current study shows how both actions and inactions can be expressions or conceptualizations of agency. Stigmatization can also be a form of agency. While dominant knowledge discourses present some of these agentic actions as ignorance and crude (Gerlach, 2016), the community members narratives suggest these are the outcomes of thoughtful sensemaking processes based on lived realities and circumstances. How agency is theorized from the perspective of the powerful is vastly different from the perspective of the marginalized.
The findings of the study provide insights to responses to recent outbreaks including Covid-19 and the Mpox outbreak. In both outbreaks, responses of individuals and community members are influenced by forces that impede and facilitate the expression of their agency. In the case of Covid-19, scholarship has shown how different respondents push back on what they perceive as government overreach (Stead et al., 2022). Other studies suggest that push back and hesitancy to receive the Covid-19 vaccines are associated with perceptions that Covid-19 is similar to the flu, previous experiments on black and brown bodies, and misinformation (Ackah et al., 2022; Dhama et al., 2021; Troiano and Nardi, 2021) etc. In each case, rather than viewing respondents as ignorant, this study suggests a reframing to view the responses as expressions of agency when it is perceived that one’s agency is being curtailed by an external force in one direction or the other. This form of reframing opens up opportunities for engaging with the concerns and working with them to not only understand them, but to find a middle ground that serves both individual and public health needs. In the case of the Mpox outbreak, which is currently confined to East Africa, the discourse of a “local” outbreak seems to be driving the response with limited support from developed countries who have stockpiles of the vaccine.
5.1 Practical implications
The findings suggest that foregrounding the agency of community members in disease outbreak communication requires certain steps. It begins with identifying what the community wants and how it has been successfully handling the outbreak (local theories, explanations, resources, cultural processes used) before external interventions were presented. This should be followed by a process of reinforcing to the community the centrality of their ideas, actions, resources etc. and how they have been effective. External interventions should be included as supporting what has already been started by the community rather than taking over or subsuming the community initiatives allowing communal ownership and leadership of the process. To be able to effectively do this, the health promoter or health communicator must be willing to decenter/give up their position as the “holder” of knowledge or expert and engage in collaboration with community members.
The findings reiterate the need to foreground the narratives, experiences and communicative processes of affected community members to engage with the perceived irrational or resistive behaviors instead of implementing top-down biomedical interventions that are often alien to these communities. This will require processes that allow solutions to emerge collaboratively with the community members. Such a decentering of scholar/interventionist is needed if the viewpoint and agency of the community is to be the focus.
5.2 Limitations and conclusions
While I endeavored to include diverse perspectives in the study, the study reflects the views of the sample in the district of study. Official voices were also not included in this analysis. A contribution of this study to scholarship, is that it shows that community members are not agentless, but their agency is enacted within constraints preceding and exacerbated by the Ebola outbreak. It also theorizes agency to demonstrate its building and expression in a contradictory and complex manner within individual, familial, community, social, economic, and biomedical structures with varying implications. Furthermore, agency is not expressed only as a personal desire, but it is understood and expressed within the constraints of familial, social/communal desires and expectations bearing in mind the implications of actions and inactions.
Without the viewpoint of the community members, the discourse of denial and ignorance, already built up from the system of colonialism, gets disseminated (Sastry and Dutta, 2017). In summary, inaction, everyday resistance, forms of stigmatization and communal organizing are all forms of agency when they are viewed as intentional actions by individuals who process, evaluate and reflect on these acts as part of their sensemaking processes.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the University of Oregon Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written or verbal informed consent to participate in this study.
Author contributions
ET: Writing – review & editing, Writing – original draft, Methodology, Investigation, Formal analysis, Conceptualization.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The publication of this paper was made possible by Indiana University’s Open Access Article Publishing Fund.
Acknowledgments
I would like to thank God for the grace to complete this manuscript and to all the participants. I am also indebted to the reviewers who provided feedback to improve the paper.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Ackah, B. B., Woo, M., Stallwood, L., Fazal, Z. A., Okpani, A., Ukah, U. V., et al. (2022). COVID-19 vaccine hesitancy in Africa: a scoping review. Glob. Health Res. Policy 7:21. doi: 10.1186/s41256-022-00255-1
Bandura, A. (2001). Social cognitive theory: an agentic perspective. Annu. Rev. Psychol. 52, 1–26. doi: 10.1146/annurev.psych.52.1.1
Bandura, A. (2018). Toward a psychology of human agency: pathways and reflections. Perspect. Psychol. Sci. 13, 130–136. doi: 10.1177/1745691617699280
Basu, A. (2017). Reba and her insurgent prose: Sex work, HIV/AIDS, and subaltern narratives. Qualitative health Research, 27, 1507–1517. doi: 10.1177/1049732316675589
Belfroid, E., van Steenbergen, J., Timen, A., Ellerbroek, P., Huis, A., and Hulscher, M. (2018). Preparedness and the importance of meeting the needs of healthcare workers: a qualitative study on Ebola. J. Hosp. Infect. 98, 212–218. doi: 10.1016/j.jhin.2017.07.001
Börner, S., Kraftl, P., and Giatti, L. L. (2021). Blurring the ‘-ism’ in youth climate crisis activism: everyday agency and practices of marginalized youth in the Brazilian urban periphery. Child. Geo. 19, 275–283. doi: 10.1080/14733285.2020.1818057
Braun, V., and Clarke, V. (2006). Using thematic analysis in psychology. Qual. Res. Psychol. 3, 77–101. doi: 10.1191/1478088706qp063oa
Braun, V., and Clarke, V. (2014). What can “thematic analysis” offer health and wellbeing researchers? Int. J. Qual. Stud. Health Well Being 9:26152. doi: 10.3402/qhw.v9.26152
Buseh, A. G., Stevens, P. E., Bromberg, M., and Kelber, S. T. (2015). The Ebola epidemic in West Africa: challenges, opportunities, and policy priority areas. Nurs. Outlook 63, 30–40. doi: 10.1016/j.outlook.2014.12.013
Charmaz, K. (2006). Constructing grounded theory: A practical guide through qualitative analysis. Thousand Oaks, CA: Sage.
Cunningham, S. B. (1992). Intrapersonal communication: A review and critique. Annals of the International Communication Association, 15, 597–620. doi: 10.1080/23808985.1992.11678829
Day, K., Johnson, S., Milnes, K., and Rickett, B. (2010). Exploring women’s agency and resistance in health-related contexts: contributors’ introduction. Fem. Psychol. 20, 238–241. doi: 10.1177/0959353509359761
Dhama, K., Sharun, K., Tiwari, R., Dhawan, M., Emran, T. B., Rabaan, A. A., et al. (2021). COVID-19 vaccine hesitancy–reasons and solutions to achieve a successful global vaccination campaign to tackle the ongoing pandemic. Hum. Vaccin. Immunother. 17, 3495–3499. doi: 10.1080/21645515.2021.1926183
Dionne, K. Y. (2014). Why West African governments are struggling in response to Ebola. The Washington Post. Available at: https://www.washingtonpost.com/blogs/monkey-cage/wp/2014/07/15/why-west-african-governments-are-struggling-in-response-to-ebola/ (Accessed January 15, 2015).
Downie, R. (2012). The road to recovery: Rebuilding Liberia's health system. The CSIS global health policy center. A report. Washington, CSIS. Retrieved from CSIS website: https://www.csis.org/analysis/road-recovery
Fairhead, J. (2014). The significance of death, funerals and the after-life in Ebola-hit Sierra Leone, Guinea and Liberia: Anthropological insights into infection and social resistance. Briefing note. Ebola Response Anthropology Platform. Available at: http://www.ebola-anthropology.net/key_messages/the-significance-of-death-funerals-and-the-after-life-in-ebola-hit-sierra-leone-guinea-and-liberia-anthropological-insights-into-infection-and-social-resistance/ (Accessed March 15, 2017).
Gabor, E. (2017). “Informant interviews” in The sage encyclopedia of communication research methods. ed. M. Allen , vol. 1 (Thousand Oaks, CA: Sage), 700–702.
Gatherer, D. (2014). The 2014 Ebola virus disease outbreak in West Africa. J. Gen. Virol. 95, 1619–1624. doi: 10.1099/vir.0.067199-0
Gee, S., and Skovdal, M. (2018). Public discourses of Ebola contagion and courtesy stigma: the real risk to international health care workers returning home from the West Africa Ebola outbreak? Qual. Health Res. 28, 1499–1508. doi: 10.1177/1049732318759936
Gerlach, N. A. (2016). From outbreak to pandemic narrative: Reading newspaper coverage of the 2014 Ebola epidemic. Can. J. Commun. 41, 611–630. doi: 10.22230/cjc.2016v41n4a3098
Goffman, E. (1963). Stigma: Notes on the management of spoiled identity. Englewood Cliffs: Prentice Hall.
Hitlin, S., and Elder, G. H. Jr. (2007). Time, self, and the curiously abstract concept of agency. Sociol Theory 25, 170–191. doi: 10.1111/j.1467-9558.2007.00303.x
Koenig, C. J. (2011). Patient resistance as agency in treatment decisions. Soc. Sci. Med. 72, 1105–1114. doi: 10.1016/j.socscimed.2011.02.010
Lindlof, T. R., and Taylor, B. C. (2019). Qualitative communication research methods (4th Ed.). Thousand Oaks, CA: Sage.
Meyer, S. (2016). Examining women\u0027s agency in managing intimate partner violence and the related risk of homelessness: The role of harm minimisation. Global Public Health, 11, 198–210. doi: 10.1080/17441692.2015.1047390
MOHSW (2011). National Health and social welfare policy. Available at: http://www.nationalplanningcycles.org/sites/default/files/country_docs/Liberia/ndp_liberia.pdf (Accessed December 20, 2016).
Morse, J. M. (1991). Subjects, respondents, informants, and participants? Qual. Health Res. 1, 403–406. doi: 10.1177/104973239100100401
Nyenswah, T. G., Kateh, F., Bawo, L., Massaquoi, M., Gbanyan, M., Fallah, M., et al. (2016). Ebola and its control in Liberia, 2014–2015. Emerg. Infect. Dis. 22, 169–177. doi: 10.3201/eid2202.151456
Perry, H. B., Dhillon, R. S., Liu, A., Chitnis, K., Panjabi, R., Palazuelos, D., et al. (2016). Community health worker programmes after the 2013–2016 Ebola outbreak. Bull. World Health Organ. 94, 551–553. doi: 10.2471/BLT.15.164020
Pescosolido, B. A., and Martin, J. K. (2015). The stigma complex. Annu. Rev. Sociol. 41, 87–116. doi: 10.1146/annurev-soc-071312-145702
Raven, J., Wurie, H., and Witter, S. (2018). Health workers’ experiences of coping with the Ebola epidemic in Sierra Leone’s health system: a qualitative study. BMC Health Serv. Res. 18, 1–9. doi: 10.1186/s12913-018-3072-3
Richardson, E. T., Barrie, M. B., Kelly, J. D., Dibba, Y., Koedoyoma, S., and Farmer, P. E. (2020). Biosocial approaches to the 2013-2016 Ebola pandemic. Health and Human Rights, 18.
Sastry, S., and Basu, A. (2020). How to have (critical) method in a pandemic: outlining a culture-centered approach to health discourse analysis. Front. Commun. 5:585954. doi: 10.3389/fcomm.2020.585954
Sastry, S., and Dutta, M. (2017). Health communication in the time of Ebola: a culture-centered interrogation. J. Health Commun. 22, 10–14. doi: 10.1080/10810730.2016.1216205
Sridhar, S., Brouqui, P., Fontaine, J., Perivier, I., Ruscassier, P., Gautret, P., et al. (2016). Risk perceptions of MSF healthcare workers on the recent Ebola epidemic in West Africa. New Microbes New Infect. 12, 61–68. doi: 10.1016/j.nmni.2016.04.010
Stead, M., Ford, A., Eadie, D., Biggs, H., Elliott, C., Ussher, M., et al. (2022). A “step too far” or “perfect sense”? A qualitative study of British adults’ views on mandating COVID-19 vaccination and vaccine passports. Vaccine 40, 7389–7396. doi: 10.1016/j.vaccine.2022.05.072
Sumo, J., George, G., Weah, V., Skrip, L., Rude, J. M., Clement, P., et al. (2019). Risk communication during disease outbreak response in post-Ebola Liberia: experiences in Sinoe and Grand Kru counties. Pan Afr. Med. J. 33:4. doi: 10.11604/pamj.supp.2019.33.2.16877
Thompson, E. E. (2017).Communicating in a public health crisis: the case of Ebola in West Africa (doctoral dissertation). ProQuest Dissertations & Theses Global (Order No. 10279436).
Thompson, E. E. (2020). Knowledge and risk perception about an Ebola virus outbreak: a comparative study of Ghana and Liberia. J. Commun. Healthc. 13, 271–283. doi: 10.1080/17538068.2020.1803644
Troiano, G., and Nardi, A. (2021). Vaccine hesitancy in the era of COVID-19. Public Health 194, 245–251. doi: 10.1016/j.puhe.2021.02.025
UNCTAD (2015). What are least developed countries. Available at: http://unctad.org/en/pages/PressRelease.aspx?OriginalVersionID=277 (Accessed September 23, 2024).
Weick, K., Sutcliffe, K., and Obstfeld, D. (2009). Organizing and the process of sensemaking. In Handbook of decision making, Eds. P. Nutt and D. Wilson. Wiley. 83–103.
WHO (2015). One year into the Ebola epidemic: a deadly tenacious and unforgiving virus. Available at: www.who.int/csr/disease/ebola/one-year-report/introduction/en/ (Accessed August 20, 2016).
WHO (2016). Ebola virus disease. Available at: www.who.int/mediacentre/news/releases/2016/ebola-zero-liberia/en/ (Accessed March 20, 2023).
Wilkinson, A., and Leach, M. (2014). Briefing: Ebola – myths, realities, and structural violence. Afr. Aff. 114, 136–148. doi: 10.1093/afraf/adu080
Keywords: Ebola, agency, Liberia, agentic perspective, sensemaking, indepth interviews, focus group discussion
Citation: Thompson EE (2024) Narratives of living through Ebola: An exploration of a Liberian community’s agency. Front. Commun. 9:1371754. doi: 10.3389/fcomm.2024.1371754
Edited by:
John Parrish-Sprowl, Purdue University Indianapolis, United StatesReviewed by:
Timothy L. Sellnow, University of Central Florida, United StatesKelly Ann Zongo, The END Fund, United States
Copyright © 2024 Thompson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Esi E. Thompson, RXNpZXRob21AaXUuZWR1