 Rati Kumar
Rati Kumar
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Commun., 04 April 2024
Sec. Health Communication
Volume 9 - 2024 | https://doi.org/10.3389/fcomm.2024.1040895
This article is part of the Research TopicTowards 2030: Sustainable Development Goal 10: Reduced Inequalities: A Communication PerspectiveView all 4 articles
From displacement to resettlement, Burmese refugees bear high disease burdens; first as forced migrants escaping conflict and then as second-class citizens in host countries like the United States. This relegation of refugee bodies to the margins upon resettlement, warrants an examination of the contradictions of the process as a humanitarian enterprise yet in violation of the United Nations Sustainable Development Goal 10 of Reduced Inequalities, particularly through a health inequities lens. In the present study, the researcher conducted 15 semi-structured in-depth interviews with key stakeholders within the resettlement ecosystem of the city of Indianapolis, Indiana in the U.S., including Burmese community members, leaders, and health practitioners. Narrative data reveal an inverse relationship between the federally mandated metric of economic self-sufficiency (ESS) defined as job placement upon resettlement, and health self-sufficiency (HSS) defined as the ability to meaningfully engage with healthcare structures and resources. Participants articulate the precarious nature of such low-wage employment in predatory industries like meatpacking, requiring little to no language or vocational training and subjecting refugee employees to coercive practices including mandatory overtime. These practices are outlined as both dangerous to the health of employees and detracting from their time resources which would otherwise be allocated toward linguistic and vocational training—both required for socioeconomic mobility, as well as to meaningfully navigate labyrinthian healthcare structures. Faced with these structural constraints, Burmese community members demonstrate health self-sufficiency through a combination of treatment with over-the-counter (OTC) medications, traditional healing practices, and by activating familial and community networks as communal resources for accessing healthcare structures.
With an estimated 89.3 million individuals displaced due to humanitarian crises at the end of 2021 (UNHCR, 2021b), the UNHCR explicitly outlines the need for alignment between the Global Compact for Refugees (GCR) and UN Sustainable Development Goals (SDGs) (UNHCR, 2020). Specifically with relation to SDG 10, the Reduced Inequalities Goal, it calls for an examination of discriminatory laws, policies, practice, and measures that can be taken to address inequality, including systems for social protection and facilitating the mobility of refugees (in particular to third countries through resettlement and complementary pathways). The current manuscript calls for a critical examination of resettlement policies such as the economic self-sufficiency (ESS) mandates of host countries acting as a barrier to healthcare for newly resettled refugees such as the Burmese.1 Employment and self-sufficiency are considered the “greatest challenges” for resettled refugees (White, 2012), and there are studies where refugees themselves define economic outcomes such as employment as important to their resettlement experience (Valtonen, 2001). However, while laudatory as a resettlement goal, its implementation depends on federal legislation and enactment within host countries.
Despite its long history of refugee resettlement, the United States compares poorly to other industrialized nations in terms of provision of social services and health care for refugees (Bollini, 1993; Lind, 2017). In fact, as far back as 2010, a bi-partisan U.S. Committee on Foreign Relations in a self-study of the resettlement system found that “The financial and mentoring assistance required to help this (resettled refugee) population achieve self-sufficiency exceeds the resources currently provided by the Federal Government” (U.S. Committee on Foreign Relations, 2010). Broadly, this is the cumulative result of an ineffective structural safety net for refugees, coupled with inadequate training and support for NGOs and health care providers within local ecosystems of resettlement. More specifically, the current piece argues that part of this is the consequence of the neoliberally defined mandate of Economic Self-Sufficiency (ESS) and lack of community voice in healthcare policy space. Scholars such as Chen and Hulsbrink (2019) and Hess et al. (2019), highlight the cost of the ESS mandate in the United States to already vulnerable refugee health, by acting as a structural barrier to genuine self-sufficiency and socioeconomic mobility. Medical researchers, international refugee and health aid agencies such as the United Nations High Commissioner for Refugees and the World Health Organization have extensively documented the poor physical and mental health outcomes refugees face in refugee camps and their health needs and practices in resettlement contexts (Goodman, 2004; Fazel et al., 2005; Porter and Haslam, 2005; van der Velde et al., 2009; Murray et al., 2010; World Health Organization, 2019; Joseph et al., 2020; Assefa et al., 2021; UNHCR, 2021b), highlighting the specific health challenges that federal overseers and resettlement agencies need to be cognizant of within the resettlement process.
In health communication and health campaigns scholarship while there is some literature focusing on refugee health (Wieland et al., 2013; Afifi et al., 2019; Rahman and Dutta, 2023), none focuses specifically on the structural constraints to basic health capacities emerging from the federal economic self sufficiency (ESS) mandate. Hewing to critical scholarship in health communication (Airhihenbuwa, 1995; Dutta, 2008) foregrounding contexts and co-creation of health knowledge from a localized lens, this research centers Burmese refugee narratives of health amidst U.S. resettlement infrastructures. Within this ecosystem at the local level, economic self-sufficiency (ESS) is narrowly conceptualized as placement in precarious, exploitative employment, as opposed to genuine self-sufficiency (Chen and Hulsbrink, 2019) encompassing health self sufficiency (HSS). Here, health self-sufficiency (HSS) is defined as the ability to meaningfully engage in healthcare and is juxtaposed against ESS, which purportedly is written into policy to support genuine self-sufficiency (and HSS as an organic outcome of this), but fails to do so within the praxis of U.S. refugee resettlement process.
This study creates a much-needed pathway for examining refugee health narratives within national resettlement mandates, such as the Economic Self Sufficiency (ESS) mandate for refugee resettlement, undergirding humanitarian aid. It engages with these narratives as data points for examining the U.S. commitment to the UN Sustainable Development Goal 10 of reduced inequalities within U.S. refugee communities. Contextualized refugee narratives in the present case highlight the contradictions between the ESS goals imposed on refugees and the barriers it poses to accessing basic health capacities in the U.S.
The pre-existing health challenges of refugees are well-documented in the medical literature both from a physical and mental health perspective (Goodman, 2004; Fazel et al., 2005; Porter and Haslam, 2005; Davidson et al., 2008; van der Velde et al., 2009; World Health Organization, 2019; Joseph et al., 2020; Assefa et al., 2021; UNHCR, 2021a). In the immediate aftermath of the crisis and in refugee camps, preventable diseases such as measles, diarrheal diseases, respiratory infections, malnutrition and malaria can prove fatal for refugees surviving without basic health capacities such as clean drinking water, adequate food and safe shelter. These environmental conditions further increase prevalence of other health issues such as tuberculosis, meningitis, vector-borne diseases, HIV/AIDS and other sexually transmitted diseases, pregnancy and obstetric complications and vaccine-preventable childhood diseases (UNHCR, 2021a). Refugees experience greater psychological disturbance than the average population (Fazel et al., 2005; Porter and Haslam, 2005), with one in five people living in conflict-affected areas suffering from depression, anxiety, post-traumatic stress disorder, bipolar disorder or schizophrenia (World Health Organization, 2019).
Upon resettlement, this community further experiences systemic discrimination within bureaucratic aid structures, exploitative low-wage employment under the guise of economic self-sufficiency (ESS), linguistic and cultural barriers and an erasure of voice in care-seeking interactions. In the United States, refugees receive Reception & Placement assistance from resettlement agencies for 90 days, a period which is focused on securing housing, completing the Refugee Health Assessment, and becoming economically self-sufficient through employment (U.S. Department of State Bureau of Population Refugees Migration, 2023). Driving refugees toward economic self-sufficiency (ESS) is a federally mandated goal of the resettlement process in the United States (Halpern, 2008). Economic self-sufficiency is defined as “earning a total family income at a level that enables a family unit to support itself without receipt of a cash assistance grant” (Office of Refugee Resettlement, 2007) or more broadly defined as “a level of economic well-being requiring no government support” (Maryland Department of Human Services, n.d.). According to the U.S. Department of State Bureau of Population Refugees Migration (2023) “In coordination with publicly supported refugee service and assistance programs, resettlement agencies focus on assisting refugees to achieve economic self-sufficiency through employment as soon as possible after their arrival in the United States.” In practice, this translates to en masse recruitment of refugees in low wage, physically demanding, precarious jobs not requiring language or vocational skills, with predatory employers in industries infamous for poor labor conditions such as meat packing and warehouse work (Frydenlund and Dunn, 2022).
Under the guise of ESS, these precarious, non-skilled and dangerous job placements, exacerbate existing medical conditions, create newer labor-induced health risks, strip workers of the time-resources required to navigate labyrinthian healthcare structures, and more broadly prevent upward socioeconomic mobility by barring access to skills and language training. Unethical and illegal recruitment and retention practices in these jobs include predatory recruitment of newly arrived refugees, circumvention of labor-laws and inadequate information on their labor rights, coercion through threats of dismissal, withholding information about health rights, misrepresentation of overtime labor as mandatory, and imposition of illegal job performance requirements. These practices converge to create workplaces sustained through the erasure of refugee voices, founded upon implicit messaging about potential job-loss and the precarious immigration status of newly resettled refugees. Resettlement agencies, on the other hand, serve the purpose of reinforcing the economic self-sufficiency mandate through an overemphasis on job placement juxtaposed with inadequate resource-allocation to language and vocational training. Refugees then are relegated to the cycle of low-wage employment, without the time-resources or infrastructural support from employees or resettlement agencies, to acquire the tools for language and vocational training (Chen and Hulsbrink, 2019; Hess et al., 2019; Frydenlund and Dunn, 2022).
Barring access to language training has a particularly pernicious effect on the ability of resettled refugees to navigate services and care for traumatic injuries sustained in conflict-contexts. Further it prevents them from seeking medical support for job-related injuries that may arise from exploitative employment. Unsustainable work-schedules consistently deprive them of time-resources for acquiring language skills necessary for navigating healthcare structures and advanced vocational training necessary for higher socioeconomic mobility. Current healthcare research unequivocally demonstrates how communication, language and cultural barriers serve as compounding factors for poor health care access, health knowledge access and experience (Eckstein, 2011; McMurray et al., 2014; Bradby et al., 2015; Abdelrahim et al., 2017). Specifically, research in the United States has demonstrated how limited English proficiency (LEP) results in subpar health care for patients Flores (2005), also finding that communication barriers result in over 50% of adverse events in U.S. hospitals (Divi et al., 2007). Such language and cultural barriers have also been found to hinder access to preventative services (Jacobs et al., 2005), as well as negatively affect patient satisfaction with providers (Ebden et al., 1988) compromise the quality of care (Weech-Maldonado et al., 2003), and snowball into avoidance of subsequent care-seeking (Alison et al., 1993).
Critical health communication scholars such as Airhihenbuwa (2006) and Dutta (2008) view these communicative erasures as complicit in structural erasures of pathways to care-seeking. They call for a recentering of marginalized narratives as contextually informed data points for a restructuring of health communication and healthcare interventions in disenfranchised communities. Aligning with this critique, this paper argues that the narrow neoliberal definition of low-wage employment as economic self-sufficiency (ESS) propagates a culture of health inaccess and undercuts the ability of refugees to become health self-sufficient (HSS). It creates structural barriers to meaningful entry into mainstream health systems due to lack of language-training and education, while also creating new health issues resulting from unprotected low-wage labor. This becomes particularly problematic as it not only stunts socioeconomic mobility but may conversely exacerbate the poor health outcomes for refugees resulting from forced and prolonged displacement.
Critical health communication scholars have analyzed the ineffectiveness of top-down health interventions within spaces of marginality, which draw upon narrow individual measures of behavior change, discounting the role of structural discrimination in spaces of knowledge production and clinical care. Scholars such as Airhihenbuwa (1995, 2006), Mokros and Deetz (1996), and Dutta (2008) critique such decontextualized health interventions for failing to center community narratives (Lupton, 1994, 2003) in health communication practice. Valuing context- rich approaches to defining and solving health problems within communities (Basu and Dutta, 2007), the culture centered approach (CCA) draws on the critical scholars such as Airhihenbuwa (1995) and Dutta (2008) to centralize the role of dialog with communities, particularly when defining problems and outlining solutions based upon the lived experiences of community members as experts. It utilizes the lens of culture, structure and agency to locate spaces for change within traditionally top-down structures of knowledge-production (Dutta, 2011). With the goal of bringing to the mainstream, voices ignored in dominant health care discourse, the CCA operationalizes culture as a creating “spaces of shared meanings, values, and interactions” (Dutta, 2008) which inform meanings of health and the lived experiences of cultural participants. Acknowledging structures as both enabling and constraining entities such as health care, it locates agency in the daily practices and cultural negotiations undertaken by those navigating these structures (Dutta-Bergman, 2004b; Dutta, 2008).
In addition to the aforementioned CCA scholarship, the present study draws upon work by scholars such Dixit et al. (2018) to specifically focus on Burmese refugees resettled in the U.S and bridges it with the CCA framework to decenter top-down medically derived expertise by engaging with the agency of community members in creating solutions within their lived experiences of health. Communities of resettled Burmese refugees continue to be marginalized in policy discourse surrounding health care in the United States given their low socioeconomic and education status (Migration Policy Institute, 2015). Such explorations from a community- based, culture-centered approach aims to contribute to the growing body of critical health communication scholarship, and more specifically refugee health research in the field. Despite there being scholarship specifically focused on refugee issues in the United States (Bach, 1988; McSpadden and Moussa, 1993; Eby et al., 2011; Kenny and Lockwood-Kenny, 2011; Smith, 2013; Spivey and Lewis, 2016), it primarily focuses on medicalized interventions and the citizenship politics of being resettled refugees. Due to an evidently lacking focus on the structural marginalization of refugee voice in the broader context of resettlement and the adjacent health communication interventions, there is a strong argument to be made for engaging such communities to improve the efficacy of health communication practices and policy at the national and local levels of resettlement (Svenkerud and Singhal, 1998; Rogers, 2000; Kreuter and McClure, 2004).
Recognizing the dialogic marginalization of refugee communities as a catalyst for denial of materials resources which enhance their resettlement experience, this study advocates for Burmese refugee voices to be inserted into the broader structures of resettlement, including the ESS mandate, which hinders meaningful access to health care. With an acknowledgment that communicative erasure is a precursor to structural erasure (Dutta-Bergman, 2004a; Dutta, 2008) these narratives create space in mainstream communication literature to demonstrate how “cultural members [...] enact their choices” (Dutta, 2008, p. 11) surrounding health behaviors, amidst the structural navigations of resettlement mandates.
The city of Indianapolis is home to one of the largest resettled Burmese refugee populations within the U.S. hosting the Chin, Karen, and Karenni ethnic groups since the early 90's, more recently also resettling Rohingya refugees escaping persecution by the Burmese military (Martinez-Legrand and Verderame, 2021). The Chin, who make up a majority of those resettled in Indiana are primarily Christian. The Karen and the Karenni include a combination of practicing Christians and Buddhists, with animist spiritual beliefs intertwined with these religious practices. They often do not speak Burmese (the language of their Burmese majority persecutors) spoken by federally provided translators in the U.S. with the exception of the Chin, who sometimes speak a mix of Burmese and Hakha-Chin. However, as a consequence of linguistic barriers they further experience distance from health care structures as a result of cultural barriers and lack of support.
After being resettled in the United States, 32% of Burmese report that while they have an assigned doctor, they have difficulty in accessing care due to the absence of logistical and linguistic support from federal agencies refugees (Jeung, as cited in Bible, 2011). Instead, by federal mandate and consequently through the executing resettlement agencies, there is an emphasis on low-wage job-placement and medical screenings for public health purposes within a short 90-day period (Indiana State Department of Health, 2023). This leaves little room for educational or orientation support in the host community. The Indiana Department of Health (2018) also notes as a “major obstacle” the cumulative effective of language barriers and lack of cultural competency to receiving health care or other social services for Burmese refugees, thereby creating barriers to resources post-resettlement. Ultimately, this creates long-term issues of unemployment, health care inaccessibility, lack of education, and other vocational skills and language-related barriers which further push refugees to the margins of mainstream health discourse.
With one of the largest Burmese refugee populations resettled in the United States (Office of Refugee Resettlement, 2016), the state of Indiana served as the site for this study. The present manuscript draws on a reanalysis of qualitative data gathered during 2013. In conducting this reanalysis, we draw on Wästerfors et al. (2013) argument for reanalysis of data from “difficult to reach” populations (Bluthenthal et al., 2012), by the researcher returning to “data that he or she generated previously, analyze them again, and build on, counter or find nuance in previous findings;” enabling the current analysis of aspects “unnoticed, scarcely explored, or left behind” (p. 468; Bloor and McIntosh, 1990; Roulston, 2001; Riessman, 2003; Åkerström et al., 2004). Further following Kedia et al. (2020) reanalysis of African American mothers' narratives of antiretroviral adherence, as an “economical use of viable, existing data” (p. 1192), we argue that revisiting this data serves the function of broadening the field of health communication to engage displaced populations from the Global South, and broadly provides longitudinal context for examining resettlement policy.
According to the Burmese American Community Institute (2022), a majority (83%) of the Burmese in Indiana are of Chin ethnicity, with the rest comprising the minority Karen and Karenni communities. In Burma, most Chin, and ~20% of Karen and Karenni are Baptist Christian. Cultural practices continue to be a combination of animist, Buddhist and Christian beliefs with a majority of those resettled in Indianapolis practicing Baptist Christianity. Given the ubiquitous influence of religious organizations and refugee resettlement structures in the Burmese community, these organically emerged as the best recruitment spaces for the present research. The researcher followed a snowball sampling strategy in this community, recruiting through word-of-mouth and informational flyers, at the two largest refugee resettlement organizations, Refuge and Church Charity, subsequently being introduced to members who also belonged to the Burmese Community Center for Education (non-denominational), and the Karen and Chin churches in the city. The researcher also attended sessions of the City Refugee Coalition, including refugees and service providers within the resettlement ecosystem, including state resettlement affiliates. The final sample emerging from this snowball sampling process is outlined in Table 1.
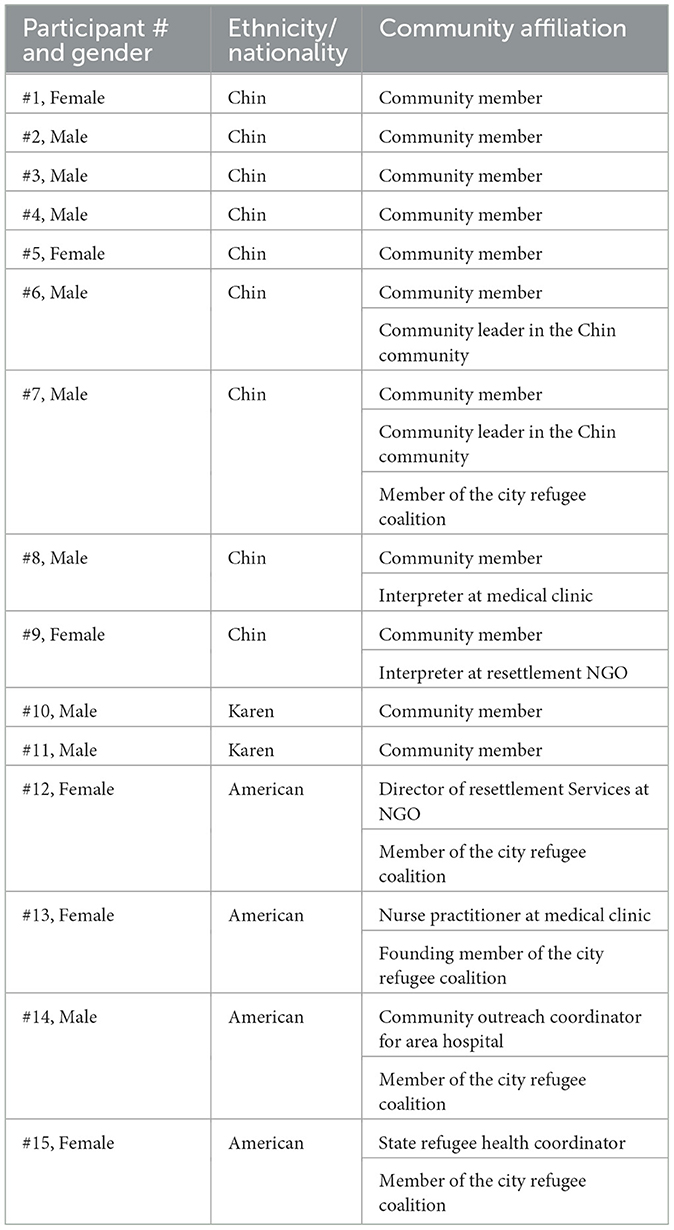
Table 1. Participant sample description: Burmese community resettlement ecosystem.
A total of 15 semi- structured in-depth interviews were conducted based on the appropriateness of such methodology for qualitative data gathering (Lindlof and Taylor, 2002). The average length of interviews was between 1 and 2 h, either at a medical clinic, resettlement agency office, homes of community members or at a local restaurant—with each of these locations being chosen by interview participants. While the confidentiality clause was explained with the option of conducting interviews in a private space, oftentimes participants preferred meeting in public places, and in the case of newly arrived refugees, preferred to meet at home in the presence of family. Consent was obtained through signatures on consent forms in English and other appropriate languages where required after an oral explanation of the same. IRB approval was secured for this study from the relevant institution with three of the interviews being conducted through an IRB certified translator from the refugee community. Interviews were conducted with concurrent data analysis to check for thematic saturation of data, i.e., until lack of new data emerging from interviews was achieved. Using a constant comparison method of analysis the researcher engaged in open coding progressing to axial coding resulting in final thematic categories for the data (Glaser and Strauss, 1967). Throughout the data analysis process, the identity of the participants was kept confidential through the use of pseudonyms and the erasure of any personally identifiable data. To ensure validity of the data, member checking was conducted with participants 7, 8, and 9 (community leaders and interpreters) 1 month after completion of all interviews and data analysis.
The primary research questions center meanings of health and healthcare in participants' lived experiences during resettlement.
RQ1. How do the cultural identities of the Burmese refugees reflect their conceptualizations of health and health care?
RQ2. How do the Burmese resettlers experience health care at the intersection of structure, culture and agency in the United States?
RQ3. What strategies do they adopt or recommend for navigating the structures of economic self-sufficiency and health care access?
Refugee narratives demonstrate meaning-making about health as access to resources, the tension between ESS and HSS, while also articulating agentic negotiations of these tensions through self-treatment based on cultural knowledge and community support. The findings provide evidence of the tensions between federally mandated measures of economic self-sufficiency, promoted as a broad-based solution for refugee welfare, and the lived experience of health inaccess as a result of exploitative work conditions.
Being healthy [is defined as] when you seek…having accessible health care..easily accessible health care. And you cannot guarantee that you will not get sick, right? But you will do everything you can, and you know what to do to stay healthy. That's why with health care, when you do get sick, you should have healthcare accessible. If not cheap for you, but it should be accessible. And then after you get the care, say you are in debt, there should be ways that you can repay your debt. So that's my definition at the top of head.
(Participant 8, Male, Chin interpreter at community clinic).
A majority of refugee participants, like Participant 8, make meaning of their lived experience of health, as entwined with the socioeconomic realities of meaningful access to healthcare within resettlement structures. Throughout participant narratives, and in participant observations at the City Refugee Coalition, two high priorities that emerge for resettlement agencies are completion of the Refugee Health Assessment, and achieving economic self-sufficiency (ESS), narrowly (federally) defined as securing employment within a 90-day period of arrival. However, within refugee participant narratives, ESS emerges as fundamentally in conflict with their ability to both access healthcare and become health self-sufficient by gaining valuable language and vocational skills. The drive to this form of ESS, often low-wage precarious employment, is driven by the resettlement agencies' need to demonstrate job-placement as part of the federally determined mandate, dictating future funding. Low-wage precarious employment such as that in meatpacking, manufacturing, and other jobs without a requirement for language or technical training fulfills the needs of both resettlement agencies as well as employers looking for cheap, unorganized labor.
Participant 15 (Female, State Refugee Health Coordinator) speaking to these goals of the agencies, notes:
Well, I mean that's like one of the major goals of the resettlement agency is to get them a job. So one of the first things that they do is they take them to get their medical card and a social security card so they can get a job. And the resettlement agencies I mean they are asked to do this so I mean their funding depends on their numbers so of course they're going to work on people getting them into employment, but they will often have businesses that have worked there before so like we have a lot of refugees who work in hotels cleaning or work in like chicken plants you know those kind of factories of some kind which doesn't require knowing a lot of language.
Her narrative is corroborated by researcher interactions with numerous participants and community members working in meat processing factories, housekeeping in hotels, in warehouses for companies like Amazon, Fedex, and Belkin, auto manufacturing plants for Honda and Toyota, or engaged in other forms of low paying labor, such as working in local bakeries. These jobs require no skills training and under state law can often require “mandatory overtime”, a measure known to be used as a coercive tactic in the state (see Kumar, 2021). This reduction of refugees to a source of cheap unskilled labor fundamentally challenges the humanitarian nature of these interventions viewed in juxtaposition to neoliberal interests vs. provision of long-term support for refugee integration and wellbeing. Participant 10 (Male, Karen), resettled for 3 years, and employed at a warehouse, continues to face issues arising from a lack of language and skills training, needing an interpreter for the interview. He states:
All kinds of difficulty once we get here. One thing is not being able to speak the language. English language. And, the living condition, living standard is different from there and here. It's very difficult for us to be [here]. And also when we go to work there is no English [translation] so work difficult. Also, transportation is very difficult.
Participant 10 defines a lack of self-sufficiency due to his inability to speak English, which manifests in areas such his ability to interact with supervisors at work, his ability to secure transportation, and broadly a lack of access to support structures. Participant 1 (Female, Chin), a young mother working as a housekeeper at a hotel, says that her perception of America does not match the reality.
At first I thought that I would come here and in a couple of years I could speak English and before I came here I was thinking that I would be able to learn English, but when I arrived here it was all different. It's not how I expected. I wish I was able to learn more English would help [with doctor's appointments for her child and broadly navigating life in the U.S.]. [...] I went to English classes regularly until afterwards when I started working. When I started working, I felt very tired when I come home. So sometime when I was too tired I would not go to class anymore.
P1's husband, Participant 2 (Male, Chin), works as a bellhop at the same hotel and says that after working overtime at his job he doesn't have time to attend any English classes, feeling “stuck in this kind of job”. Participants 10, 1 and 2, echo the narratives of other participants who receive support from resettlement agencies for a short 90-day period, during which time many of them are channeled into precarious low-wage employment, if in fact they are able to be employed within that time frame.
However, participants articulate how ESS becomes a barrier to accessing health care as employees are known to deploy exploitative techniques such as requiring Family & Medical Leave Act (FMLA) paperwork for doctor visits, obfuscating their legal rights for requesting leave by providing the information in English, and issuing underlying threats of termination for those that request time off (for more on employment-related barriers, see Kumar, 2021). Not only does this employment act as a barrier to more holistic resettlement, but it conversely exacerbates both the physical and mental health inequities faced by the refugees as emerging from conflict-induced trauma. P8, gives one of many examples of workplace injuries in a meatpacking factory.
In [South of the City], they have this turkey meat chopping, packing place. And this employee, he was not a patient, but at that time I work with [a resettlement agency] and I took people there to apply for jobs. So we learn from casual conversation, actually this big turkey fell on top of him, and like he slipped and fell on the ground. And he was hurt, but not injured, right. Hurt. And he was too concerned that he might lose his job, so when the supervisor came and asked if he was okay, he said yes! But he was (shakes head) for a few months.
P8 then states that the man possibly had a concussion, and he had heard of other examples such as the local Tyson foods that “when the people in white coats (union) come, they slow down the belt” but continue at high speeds once they leave. These stories of exploitative labor practices across industries including car manufacturing, meatpacking and warehouse work were commonplace in conversations with community members. A majority of them reported work-related injuries and shared that they were unable to seek care for these injuries due to being unable to take time off from work due to the assumption of being fired from their jobs if they were absent or if they complained about workplace practices.
Community members also shared concerns surrounding mental health due to the lack of federal support provided to refugee families. P8 says that many refugees used to see the United States as a “superstar country”, and a “perfect place” due to “Hollywood, all the glamor, and everything like that, so it was almost a utopian world for them”. However, their resettlement experience soon turned into an increasingly mentally challenging experience. He says:
And then they came (many during the recession), they couldn't find jobs and then they had to rely on welfare, and then they got sick, and it's just a lot of frustration. And they started thinking, maybe they regret, this is the wrong decision. And at that time, I worked with a refugee agency too – many expressed concern, and many expressed their frustration and they want to go back to Burma, or refugee camp. They thought the refugee camp was even better. And you know, we've seen some suicides in the community because of this.
P8, also echoing the earlier narrative of P2 states that many resettled Burmese feel “stuck” due to their lack of socioeconomic mobility and cycle of unending low-wage jobs, especially those that might have earlier access to education and professional degrees in Burma. He also shares stories of refugees who have been misled by their employers into believing that they need to submit FMLA paperwork even if they need time off for doctor appointments, coercion into working up to 20 h shifts based on the “mandatory overtime” laws of the state—both of which have resulted in acute injuries that P8 has witnessed being treated in the medical clinic and at the local hospital's emergency room.
In addition, the health safety net of Medicaid provided through Refugee Medical Assistance remains untouched by most refugees during its 8-month duration,2 as the first year tends to be centered around general orientation, health assessments, employment seeking and retention. This further deprives them of the time to familiarize themselves with the labyrinthian healthcare systems and establish any form of preventive care support.
P8 notes:
So, you know in the first 6 months, they are too overwhelmed with other appointments and finding jobs and getting settled down, getting settled, like they have to worry a lot about jobs and paying rent, so they cannot really focus on their health. If they stay a little bit healthy or if they are not very sick. So they cannot focus on their health within that six month period. But when they think they are ready and they can focus then Medicaid is cut off.
Participant 2 (Male, Chin), corroborates this with his personal experience of losing Medicaid saying:
My Medicaid only last for 8 months. Refugee Medicaid is only 8 months. During that 8 months, I did not get the complete shot and after that I had to get some and I have to pay on my own. Like $120.
He says that as a result of the steep cost and lack of orientation he does not have a family doctor, he never went for his follow up shot, and has only gotten the initial immunizations and health screens provided by the state health department.
Other Burmese community members voice similar concerns, outlining the financial burdens associated with seeking medical care, as well as the prevailing fear of job termination if they take time off from work to attend to their health needs. This often sets up refugees to continue in a cycle of poverty set in motion at the inception of the resettlement process in the U.S. This stands in contrast to a more integrative approach used by other countries and viewed by community leaders as a better alternative. P7 as a community leader speaks to this issue of inadequate support for genuine self-sufficiency enabling refugees to “go on themselves”, echoing the experience of the numerous new arrivals grappling with similar structural challenges within the Burmese community. P7, who has been in the U.S. for nearly a decade is also connected with Burmese community leaders in other countries and compares the U.S. experience to being resettled elsewhere.
Participant 7 (Male, Chin community leader) articulates:
But, in here (U.S. compared to other host countries), when they come they just bring them and just keep them some food for a few days, for a few months, for a few years…not year. Just a few months. They just left them. And they don't know where they are. And they don't know what they're doing. So for example, you understand that, let me go to China right now. I don't speak Chinese. I don't have any friend, any family. They bring you, and okay, they pay you money for 3 months. Some food for 2 to 3 months and then they gone. [...] If they (the government) bring the refugee, they should help them until at least until they have the ability or they have enough information to go on themselves.
These collective narratives highlight the tensions in the U.S. between the humanitarian goals of resettlement, the neoliberal drive for cheap exploitative labor with an emphasis on low-wage jobs, and the cycle of poor health outcomes resulting from these stressors. The added precarity and entrenchment in the cycle of low-wage employment without opportunities for advancement, contribute to widening socioeconomic disparity affecting the mental health of community members already subject to the trauma of conflict and displacement.
Despite the conceptualization of economic self-sufficiency as a pathway to successful resettlement for Burmese refugees in the U.S., community narratives position this form of ESS as antithetical to their long term health and wellbeing. In fact, the strategy of employment-at-all-costs, Increases their health burdens and risk factors through dangerous employment. Lastly, this form of neoliberally defined ESS as an indicator of successful resettlement, materially impinges on their ability to become health self-sufficient, by taking away time resources for acclimating to the new host country and learning linguistic, and structural strategies needed for navigating complex healthcare infrastructures. What emerges instead is refugees' agentic operationalizing of health self-sufficiency within these structures of biomedicine, employment and resettlement as spaces of community, self-medication and traditional remedies.
In participant narratives, health self-sufficiency emerges as an agentic function of cultural beliefs about preventive care, coupled with the inaccessibility of healthcare. Put simply, at the outset, the Burmese are hesitant to engage healthcare structures, and given the poor quality of care and coverage evidenced, they further choose to disengage, instead relying on self-treatment with a combination of over the counter (OTC) medication and culturally-derived healing practices. For those that do choose to engage with health services, they do so through strategies of familial and community support activation.
Participant 9 (Female, Chin refugee/interpreter at resettlement NGO) articulates the Burmese attitude toward provider visits, saying:
Well, like I said, Burma is a poor country, and then we don't go to the doctor for check up. And then if someone go to the doctor, and we all assuming that is really serious. Because you don't usually go to a doctor unless you are really, really feel sick. So, a lot of people still have that kind of mind in here. So if you go to the doctor something really [serious]. So most of our clients when we try to take them to their first PCP appointment and they go “I am healthy. Why do I have to go to the doctor?”
She says that this sentiment is exacerbated by the difficult interactions they have with their healthcare providers due to the lack of language proficiency, long wait times at local clinics which are held against them by difficult employers; resulting in a further refusal to comply with even initial screening requirements.
Participant 3 (Male, Chin), who was recovering from an illness summarizes his situation similarly by saying:
[Even though I am sick] I do not have Medicaid. Well, two [other] things. One is that I have to work and the other thing is that difficulty in calling the doctor's office and arranging appointments [due to language and transportation difficulties].
P3 who works in a chicken processing plant, which is a relatively cold workplace, elaborates that his employee is known to become upset if employees take time off “for small things”, and this has affected his ability to stay home till his respiratory issues gets better. In this context, participants make meaning of self-medication as a form of agency, with Participant 5 (Female, Chin), a young mother of two, describing how her family dealt with the flu using a combination of over-the-counter medication and traditional remedies like herbs boiled in water. At this point, she had lost Medicaid coverage, which she would only be eligible for during pregnancy and says:
When we sick, we go to the CVS and bought over the counter medicine like Tylenol. And then, we took it for the pain. Like the traditional way, too, we do. Like traditional treatment. It sometime look like …we put some kind of oil on the back and the neck. And then something like a spoon or something like that they scratch it like that..over and over again..and it become very red, and they sweat and then the fever gone. That's the traditional way.
These traditional treatments draw upon the cultural knowledge of healing within Burmese culture, where such non-pharmacological methods form a dominant strand in the larger pathways of care and healing in the refugee community. Like P5, other refugee narratives enumerate these approaches to health as being a combination of OTC pharmacological drugs and generationally derived traditional methods of healing. Participant 11 (P11, male, Karen community member), who has been in the U.S. for 3 years (and also has no healthcare coverage), was suffering from a cough throughout our interview. Here he describes his self-treatment regimen:
I am taking over the counter medicine and I also use herbal medicine that we brought from home. I don't know the name but it's a kind of plant. So what it does is, I put the plant into hot water and drink it like a tea, and it helps with coughing and back pain and to..and increase appetite. I don't know the name of the plant, but they are plants that we brought from home and do the things I described.
Participant 10 (Male, Karen community member) notes that he finds it much easier to continue using traditional treatments used by his family, instead of “understanding this system” after resettlement in America. He recalls as a child learning a practice from his parents who would invoke a spiritual entity to help him heal faster, and even now uses this practice when he or his kids begin to feel unwell.
Within this backdrop, the refugees who do choose to engage with healthcare structures agentically activate familial and community networks to navigate labyrinthian resettlement and healthcare structures. While refugee resettlement agencies are central to the initial resettlement process, P7 says of the agencies:
Well……we know each other, but there is not a real connection or collaboration. They are working their job, but the community, we are working…try to help our people. Because these are our people, and we don't want to have a problem. And we just try to help them as much as[we] can. But the refugee [resettlement agency] people, this their job. Just as a principle they just bring and that's it..and they get money.
Given this dynamic between resettlement agencies and community participants, P1 articulates that familial networks become indispensable, especially for higher need refugees such as the elderly and those newly arrived. He says:
Many older patients, because they don't know why they should take this (medicine). Also, they don't read the labels, they cannot read the labels, and many of the times, they memorize the pills by the shape and the colors, right. So, we don't want them to mix up the doses. So, we encourage them to bring a younger aid. Grandchildren, or his children, and then we explain to the younger person, or a person who has more knowledge. And that person, usually is one of the families [sic] members, will guide the older patients, when to, how to take medications, take them to appointments, like specialist appointments, x-ray appointments, that are not here (at the clinic).
This was also corroborated by the researcher, who observed this as a common practice of younger family members serving as interpreters for older patients, or newly-arrived refugees accompanied by neighbors or friends when needing assistance with medical translation in the clinic. Through these interactions family and community are revealed to be not only cultural units or social bonds, but as necessary health network resources to be leveraged in the face of inadequate structural support. P11 recalls how his family utilized their community network as a healthcare resource.
It was difficult because we didn't know to drive (to the clinic) so we didn't have transportation so we had to get somebody who knows how to drive and has a car. For some people who have limited Burmese language skills, they would try as much as possible to communicate with the interpreter in Burmese. For instance, my mother does not speak a word of Burmese, so she would bring a Karenni person with her, to speak with the interpreter to translate from Karenni to Burmese to English. Three ways. Two steps interpreting.
His narrative demonstrates a prevalent culture of collaboration embedded in Burmese negotiations of American healthcare structures. Moreover, the efforts of community members to not only access healthcare but also secure employment and other basic health capacities, contain numerous stories of assistance from familial or community networks. P11, recalling his efforts at finding employment articulates this here:
A friend helped me. Friend told me that there is a job opening in Fedex like that. The Belkin, like that. And then they helped to went there and they filled the paper. Apply that. After we got here, like 5 month, 6 month, they [the agency] start helping to look for job. So, I cannot wait that long. They help, but I went with a friend myself too.
P11's articulation is echoed by other participants. P7, as a community leader, envisions a need for better collaboration between the funding agencies and community-centric efforts. He advocates for community-led decision-making and NGO alignment with pre-existing Burmese networks, for improved resettlement outcomes.
Many organization, agency, they are trying to do service, create the program, many many fancy program, but it's not really practical. It's not helpful for the Burmese people. I know that there are so many meeting, so many workshop, so many program created, but that all doesn't really benefit our community. Because there is still a gap. They [resettlement agencies] are doing their job. There is no connection. No real connection between the community family and those organization, so if they really want to help, they need to come to the Chin community, the community they [want to] help, and [come to] those who are well connected with the community family.
In the present manuscript, utilizing a culture centered lens, we examine the material and the symbolic dialectic between health and self-sufficiency through the narratives of Burmese resettled refugees in the United States. Lending empirical support to CCA theorizing about the role of communicative erasure as symbolic of material erasures, this study focuses on the structural erasure of the refugee voices and bodies purported to be at the center of the humanitarian aid ecosystem.
Burmese refugee bodies are designated both as other and without agency upon resettlement in the United States. Their pathway to citizenship is designed in keeping with the raced, neoliberal conceptualization of worthwhile bodies of color as units of labor capable of contributing to the economy, albeit sacrificing their health and socioeconomic mobility in the process. This piece draws upon a combination of migration, work (Chen and Hulsbrink, 2019; Hess et al., 2019) and critical health communication scholarship to problematize the metric of ESS in U.S. resettlement as a barrier to genuine self-sufficiency. Locating the ability to cultivate health self-sufficiency and meaningful access to healthcare as an inextricable part of genuine self-sufficiency, refugee narratives demonstrate gaps in resettlement systems which fail to incorporate refugee voices for improved outcomes. For example, in promoting top-down forms of health communication interventions, local hospitals fail to account for the historical context of Burmese ambivalence about healthcare structures, and in promoting predatory employment, resettlement agencies discount the pre-existing physical and mental trauma borne by them and the potential exacerbating impact a cycle of poverty can have on them. The cultural meanings of what it means to be a Burmese refugee in the United States, collides with the structural expectations for what it means to be a productive citizen, often ignoring one's long-term health and wellbeing in the process. These intersections demonstrate how cultural meanings intersect with structural barriers to reproduce health inequities (Basu and Dutta, 2007; Dutta, 2008; Basu, 2010; Sun and Dutta, 2016). While problematic on its own, as an issue of health inequity, it warrants deeper critique due to the United States' purported commitment to the humanitarian project of refugee resettlement as a signatory to the UN Protocol Relating to the Status of Refugees, and the UN SDG 10 of reducing inequalities within and among countries. Deconstructing structures of humanitarian aid and resettlement through refugee articulations, we see the US commitment to refugee health and wellbeing as a conduit for cheap labor channeled into predatory industries with lax labor protections, resulting in additional physical and mental trauma for this displaced community. The concept of economic self-sufficiency (ESS), narrowly defined as job-placement by federal mandate emerges as a barrier to health self-sufficiency (HSS) in the long term. Data from community narratives point to the inverse relationship between the ability to secure and retain low wage employment within a short assistance period and access meaningful care within complex healthcare structures.
Most community members define health or being healthy as constructed within the material realities of access to healthcare resources. As outlined by one of the interpreters, the refugee health coordinator for the state, and community members themselves, job placement plays an outsize role in continued agency funding as well as serves the purpose of securing cheap labor for local industries infamous as dangerous and precarious employers. What it fails to serve is the purported humanitarian agenda of refugee integration and genuine self-sufficiency, colliding with U.S. neoliberal structural violations of healthcare as a human right. The omnipresent issue of low-wage labor exploitation in the U.S., becomes especially pronounced for bodies on the margins of citizenship, suffering from prolonged displacement. Our participants enumerate the ways in which this emphasis on job-placement within a 90-day window subjects them to labor law violations, intimidation, physical and mental stressors affecting their health as well as their ability to navigate the host country. Precarious employment coupled with a short Refugee Medical Assistance period, renders the already truncated healthcare coverage meaningless, because “when they think they are ready, and they can focus then Medicaid is cut off” (P8). Thus, the meaning making around health demonstrates the erasure of refugee voice in resettlement by laying bare the disconnect between their lived experience of health vs. federal metrics which dictate a successful resettlement experience. This communicative erasure, both linguistic and systemic, is symptomatic of material erasures in the resettlement process, including a lack of linguistic support and cultural orientation, but more insidiously through a systemic incorporation of refugees into the low-wage labor market. This neoliberal turn of humanitarian aid warrants further examination for its violations of the UN SDG 10 of reducing inequalities, and more specifically the shared prosperity target (10.1) which aims for income growth of bottom 40% of the population, coupled with the need for responsible and well-managed migration policies (10.7). The U.S. rhetoric surrounding refugee resettlement and the UNSDGs, including the reduction of inequities, stands in stark contrast to the process employed to ensure economic self-sufficiency in resettlement for the Burmese community.
Withstanding these geographic and systemic displacements, community members find voice through an enactment of the cultural knowledge of healthfulness, including self-treatment with over-the-counter medications, traditional therapies and practices, and enlisting familial and community networks when needing to access hard-to-reach healthcare structures. These agentic negotiations demonstrate a complex cultural interplay of the push-pull forces dictating engagement with healthcare structures. On the one hand, cultural beliefs emerging from poor infrastructure in Burma and in refugee camps lend an ominous aura to doctor visits, exemplified by P9, who speaks of how community members think that “I am healthy. Why do I have to go to the doctor?”. Conversely, for those who choose to go to a doctor when in need of care, they find the lack of paid leave, poor insurance coverage and absent linguistic and cultural support significant barriers to access. These barriers, combined with a long history of traditional remedies practiced in Burmese culture, ultimately result in two different strategies for navigating healthcare structures. The Burmese either favor self-treatment through OTC medicines and traditional remedies, or they utilize family and community networks as resources for deciphering and navigating opaque health systems. In this backdrop, there also exist ineffective top-down interventions outlined by community members in the form of medical information-giving sessions and the completion of the Refugee Health Assessment, again a mandatory obligation for resettlement agencies to be completed in a short period of time. Community leaders like P6 and P7, among others, highlight the ineffectiveness of these top-down interventions and emphasize the need for dialog with communities, in communities, by healthcare providers and resettlement agencies.
Broadly across narratives there emerges the need not only for a reassessment of the ESS mandate, linguistic support and vocational training, but for substantive voices of community members to be incorporated meaningfully into healthcare structures and policy spaces within the resettlement and health ecosystems in local communities. This culture centered research, with its focus on centering voices from the margins aims to serve as a bridge between health communication and resettlement structures, while adding to the discourse by critical scholars on migrant health in low-resource contexts including resettled refugees. Specifically, it envisions the role of critical health communication scholarship as drawing on community expertise to inform structural change at these very intersections of culture and structure which continue to be the domain of top-down health interventions and driven by neoliberal metrics of economic self-sufficiency. Instead, it calls upon healthcare and policy actors within the resettlement ecosystem to realign material resources with the lived health experience of community members and incorporate community agency in rewriting the allocation of humanitarian federal aid.
The datasets presented in this article are not readily available because confidentiality concerns due to the possible persecution of refugee participants by state agencies. Requests to access the datasets should be directed to cmt1bWFyQHNkc3UuZWR1.
The studies involving humans were approved by Purdue University Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants.
The author confirms being the sole contributor of this work and has approved it for publication.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^Economic self-sufficiency is defined by the Office of Refugee Resettlement (2007) as earning a total family income at a level that enables a family unit to support itself without receipt of a cash assistance grant.
2. ^On March 28, 2022, the Office of Refugee Resettlement under the U.S. Department of Health and Human Services announced the expansion of the Refugee Cash Assistance (RCA) and Refugee Medical Assistance (RMA) period from 8 months to a 12-month period as announced by the Federal Register at https://www.federalregister.gov/documents/2022/03/28/2022-06356/extending-refugee-cash-assistance-and-refugee-medical-assistance-from-8-months-to-12-month.
Åkerström, M., Jacobsson, K., and Wästerfors, D. (2004). “Reanalysis of previously collected material,” in Qualitative Research Practice (London: Sage Publications, Inc.), 344–357.
Abdelrahim, H., Elnashar, M., Khidir, A., Killawi, A., Hammoud, M., Al-Khal, A. L., et al. (2017). Patient perspectives on language discordance during health care visits: findings from the extremely high-density multicultural state of Qatar. J. Health Commun. 22, 355–363. doi: 10.1080/10810730.2017.1296507
Afifi, T. D., Afifi, W. A., Acevedo Callejas, M., Shahnazi, A., White, A., and Nimah, N. (2019). The functionality of communal coping in chronic uncertainty environments: the context of palestinian refugees in Lebanon. Health Commun. 34, 1585–1596. doi: 10.1080/10410236.2018.1514682
Airhihenbuwa, C. O. (1995). Health and Culture: Beyond the Western Paradigm. Thousand Oaks, CA: Sage Publications.
Airhihenbuwa, C. O. (2006). Healing Our Differences: The Global Crisis of Health and Politics of Identity. Lanham, MD: Rowman and Littlefield.
Alison, M., Bowes Teresa, M., and Domokos (1993). South Asian women and health services: a study in Glasgow. New Commun. 19, 611–626. doi: 10.1080/1369183X.1993.9976391
Assefa, M. T., Frounfelker, R. L., Tahir, S. A., Berent, J. M., Abdi, A., and Betancourt, T. S. (2021). Traditional medicine and help-seeking behaviors for health problems among somali bantu refugees resettled in the United States. Qual. Health Res. 31, 484–497. doi: 10.1177/1049732320970492
Bach, R. L. (1988). State intervention in Southeast Asian refugee resettlement in the United States. J. Refugee Stud. 1, 38–56. doi: 10.1093/jrs/1.1.38
Basu, A. (2010). Communicating health as an impossibility: sex work, HIV/ AIDS, and the dance of hope and hopelessness. Southern Commun. J. 75, 413–432. doi: 10.1080/1041794x.2010.504452
Basu, A., and Dutta, M. (2007). Centralizing context and culture in the co-construction of health: localizing and vocalizing health meanings in rural India. Health Commun. 21, 187–196. doi: 10.1080/10410230701305182
Bible, E. (2011). Oakland's Refugees From Burma Face Extreme Poverty, Study Finds. The San Francisco State News. Available online at: http://www.sfsu.edu/~news/2011/fall/44.html (accessed December 14, 2023).
Bloor, M., and McIntosh, J. (1990). “Surveillance and concealment: a comparison of techniques of client resistance in therapeutic communities and health visiting,” in Readings in Medical Sociology, eds. S. Cunningham-Burley, and N. McKegany (London: Tavistock), 159–181.
Bluthenthal, R. N., Palar, K., Mendel, P., Kanouse, D. E., Corbin, D. E., and Derose, K. P. (2012). Attitudes and beliefs related to HIV/AIDS in urban religious congregations: Barriers and opportunities for HIV-related interventions. Soc. Sci. Med. 74, 1520–1527.
Bollini, P. (1993). Health for immigrants and refugees in the 1990s. A comparative study in seven receiving countries. Innovation 6, 101–110. doi: 10.1080/13511610.1993.9968337
Bradby H. Humphris R. Newall D. Phillimore J. Health Evidence Network and World Health Organization . (2015). Public health aspects of migrant health: a review of the evidence on health status for refugees and asylum seekers in the European region.
Burmese American Community Institute (2022). Happy New Year! Retrieved from https://thebaci.org/wp-content/uploads/2022/01/Happy-New-Year-2022-and-Newsletter-Default.pdf (accessed December 15, 2023).
Chen, X., and Hulsbrink, E. B. (2019). Barriers to achieving “economic self-sufficiency”: the structural vulnerability experienced by refugee families in Denver, Colorado. Hum. Org. 78, 218–229. doi: 10.17730/0018-7259.78.3.218
Davidson, G. R., Murray, K. E., and Schweitzer, R. D. (2008). Review of refugee mental health and wellbeing: Australian perspectives. Aust. Psychol. 43, 160–174. doi: 10.1080/00050060802163041
Divi, C., Koss, R. G., Schmaltz, S. P., and Loeb, J. M. (2007). Language proficiency and adverse events in US hospitals: a pilot study. Int. J. Qual. Health Care 19, 60–67. doi: 10.1093/intqhc/mzl069
Dixit, A., Miner, E., Wiehe, S., and McHenry, M. (2018). Adolescent Burmese refugees perspectives on determinants of health. J. Immigr. Minor. Health 20, 370–379. doi: 10.1007/s10903-017-0648-7
Dutta-Bergman, M. (2004a). The unheard voices of Santalis:communicating about health from the margins of India. Commun. Theory 14, 237–263. doi: 10.1093/ct/14.3.237
Dutta-Bergman, M. (2004b). Poverty, structural barriers and health: a Santali narrative of health communication. Qual. Health Res. 14, 1107–1122. doi: 10.1177/1049732304267763
Ebden, P., Bhatt, A., Carey, O., and Harrison, B. (1988). The bilingual consultation. Lancet 331:347. doi: 10.1016/S0140-6736(88)91133-6
Eby, J., Iverson, E., Smyers, J., and Kekic, E. (2011). The faith community's role in refugee resettlement in the United States. J. Refugee Stud. 24:586. doi: 10.1093/jrs/fer038
Fazel, M., Wheeler, J., and Danesh, J. (2005). Prevalence of serious mental disorder in 7000 refugees resettled in western countries: a systematic review. Lancet 365, 1309–1314. doi: 10.1016/S0140-6736(05)61027-6
Flores, G. (2005). The impact of medical interpreter services on the quality of health care: a systematic review. Med. Care Res. Rev. 62, 255–299. doi: 10.1177/1077558705275416
Frydenlund, S., and Dunn, E. C. (2022). Refugees and racial capitalism: meatpacking and the primitive accumulation of labor. Polit. Geogr. 95, 0962–6298. doi: 10.1016/j.polgeo.2021.102575
Glaser, B. G., and Strauss, A. L. (1967). The Discovery of Grounded Theory: Strategies for Qualitative Research. New York, NY: Aldine De Gruyter.
Goodman, J. H. (2004). Coping with trauma and hardship among unaccompanied refugee youths from Sudan. Qual. Health Res. 14, 1177–1196. doi: 10.1177/1049732304265923
Halpern, P. (2008). Refugee Economic Self-sufficiency: An Exploratory Study of Approaches Used in Office of Refugee Resettlement Programs. Available online at: https://aspe.hhs.gov/sites/default/files/private/pdf/75561/report.pdf (accessed December 14, 2023).
Hess, J. M., Isakson, B. L., Amer, S., Ndaheba, E., Baca, B., and Goodkind, J. R. (2019). Refugee mental health and healing: understanding the impact of policies of rapid economic self-sufficiency and the importance of meaningful work. J. Int. Migrat. Integrat. 20, 769–786. doi: 10.1007/s12134-018-0628-3
Indiana Department of Health (2018). Indiana State Health Assessment and Improvement Plan. Retrieved from https://www.in.gov/health/directory/office-of-the-commissioner/data-and-reports/ (accessed December 20, 2023).
Indiana State Department of Health (2023). Refugee Health Data and Statistics. Cumulative Arrivals by Country of Origin. Available online at: https://www.in.gov/health/idepd/files/refugee-health/Cumulative-Data-Arrivals-by-Country-of-Origin-NEW-BRANDING.pdf (accessed February 14, 2024).
Jacobs, E. A., Karavolos, K., Rathouz, P. J., Ferris, T. G., and Powell, L. H. (2005). Limited English proficiency and breast and cervical cancer screening in a multiethnic population. Am. J. Public Health 95, 1410–1416. doi: 10.2105/AJPH.2004.041418
Joseph, L., Ismail, S. A., Gunst, M., Jarman, K., Prior, D., Harris, M., et al. (2020). A qualitative research study which explores humanitarian stakeholders' views on healthcare access for refugees in Greece. Int. J. Environ. Res. Public Health 17:6972. doi: 10.3390/ijerph17196972
Kedia, S., Dillon, P., and Basu, A. (2020). A Qualitative exploration of “Mother First” identity and antiretroviral adherence among African American women living with HIV in the mid-south region of the United States. Health Commun. 35, 1190–1199. doi: 10.1080/10410236.2019.1623641
Kenny, K., and Lockwood-Kenny, K. (2011). A mixed blessing: Karen resettlement to the United States. J. Refug. Stud. 24, 217–238. doi: 10.1093/jrs/fer009
Kreuter, M., and McClure, S. M. (2004). The role of culture in health communication. Annu. Rev. Public Health 25, 439–455. doi: 10.1146/annurev.publhealth.25.101802.123000
Kumar, R. (2021). Refugee articulations of health: a culture-centered exploration of burmese refugees' resettlement in the United States. Health Commun. 36, 682–692. doi: 10.1080/10410236.2020.1712035
Lind, D. (2017). The Trump Administration Doesn't Believe in the Global Refugee Crisis. Available online at: https://www.vox.com/policy-and-politics/2017/10/3/16379016/trump-refugees (accessed December 14, 2023).
Lindlof, T. R., and Taylor, B. C. (2002). Qualitative Communication Research Methods, 2nd Edn. Thousand Oaks, CA: Sage.
Lupton, D. (1994). Toward the development of critical health communication praxis. Health Commun. 6, 55–67. doi: 10.1207/s15327027hc0601_4
Martinez-Legrand, N., and Verderame, J. A. (2021). Burmese. Encyclopedia of Indianapolis. Available online at: https://indyencyclopedia.org/burmese/ (accessed December 14, 2023).
Maryland Department of Human Services (n.d.). Maryland Office for Refugees and Asylees: Employment Services. Available online at: https://dhs.maryland.gov/maryland-office-for-refugees-and-asylees/moras-programs/economic-self-sufficiency-programs/ (accessed December 14 2023)..
McMurray, J., Breward, K., Breward, M., Alder, R., and Arya, N. (2014). Integrated primary care improves access to health care for newly arrived refugees in Canada. J. Immigr. Minor. Health 16, 576–585. doi: 10.1007/s10903-013-9954-x
McSpadden, L. A., and Moussa, H. (1993). I have a name: the gender dynamics in asylum and in resettlement of Ethiopian and Eritrean refugees in North America. J. Refug. Stud. 6, 203–225.
Migration Policy Institute (2015). The Integration Outcomes of U.S. Refugees: Successes and Challenges. Available online at: https://www.migrationpolicy.org/research/integration-outcomes-us-refugees-successes-and-challenges (accessed December 14, 2023).
Mokros, H. B., and Deetz, S. (1996). “What counts as real? A constitutive view of communication and the disenfranchised in the context of health,” in Communication and Disenfranchisement: Social Issues and Implications, ed E. B. Ray (Mahwah, NJ: Lawrence Erlbaum), 29–44.
Murray, K. E., Davidson, G. R., and Schweitzer, R. D. (2010). Review of refugee mental health interventions following resettlement: best practices and recommendations. Am. J. Orthopsychiatry 80, 576–585. doi: 10.1111/j.1939-0025.2010.01062.x
Office of Refugee Resettlement (2007). ORR Recommendations and Proposed Reporting Requirements and Guidelines for Economic Self-Sufficiency. Available online at: https://www.acf.hhs.gov/orr/policy-guidance/state-letter-07-08 (accessed December 14, 2023).
Office of Refugee Resettlement (2016). FYI 2015 Served Populations by Country and State of Origin. Available online at: https://www.acf.hhs.gov/orr/resource/fy-2015-served-populations-by-state-and-country-of-origin-refugees-only (accessed December 14, 2023).
Porter, M., and Haslam, N. (2005). Predisplacement and postdisplacement factors associated with mental health of refugees and internally displaced persons: a meta-analysis. J. Am. Med. Assoc. 294, 602–612. doi: 10.1001/jama.294.5.602
Rahman, M. M., and Dutta, M. J. (2023). The United Nations (UN) card, identity, and negotiations of health among Rohingya refugees. Int. J. Environ. Res. Public Health 20:3385. doi: 10.3390/ijerph20043385
Riessman, C. K. (2003). Performing identities in illness narrative: masculinity and multiple sclerosis. Qual. Res. 3, 5–33. doi: 10.1177/146879410300300101
Roulston, K. (2001). Data analysis and “theorizing as ideology.” Qual. Res. 1, 279–302. doi: 10.1177/146879410100100302
Smith, Y. J. (2013). Resettlement of Somali Bantu refugees in an era of economic globalization. J. Refugee Stud. 26, 477–494. doi: 10.1093/jrs/fes039
Spivey, S. E., and Lewis, D. C. (2016). Harvesting from a repotted plant: a qualitative study of Karen refugees' resettlement and foodways. J. Refug. Stud. 29, 60–81. doi: 10.1093/jrs/fev013
Sun, K., and Dutta, M. J. (2016). Meanings of care: a culture-centered approach to left-behind family members in the countryside of China. J. Health Commun. 21, 1141–1147. doi: 10.1080/10810730.2016.1225869
Svenkerud, P. J., and Singhal, A. (1998). Enhancing the effectiveness of HIV/AIDS prevention programs targeted to unique population groups in Thailand: lessons learned from applying concepts of diffusion of innovation and social marketing. J. Health Commun. 3, 193–216. doi: 10.1080/108107398127337
U.S. Committee on Foreign Relations (2010). Available online at: https://www.govinfo.gov/content/pkg/CPRT-111SPRT57483/html/CPRT-111SPRT57483.htm (accessed December 14, 2023).
U.S. Department of State Bureau of Population Refugees and Migration (2023). Reception and Placement. Available online at: https://www.state.gov/refugee-admissions/reception-and-placement/ (accessed December 14, 2023).
UNHCR (2020). The Sustainable Development Goals and the Global Compact on Refugees. Available online at: https://www.unhcr.org/media/sustainable-development-goals-and-global-compact-refugees (accessed December 14, 2023).
UNHCR (2021a). 2021 Annual Public Health Global Review. Available online at: https://www.unhcr.org/media/40241 (accessed December 14, 2023).
UNHCR (2021b). Global Trends Report. Available online at: https://www.unhcr.org/media/40152 (accessed December 14, 2023).
Valtonen, K. (2001). Social work with immigrants and refugees: developing a participation based framework for anti-oppressive practice. Br. J. Soc. Work 31, 955–960. doi: 10.1093/bjsw/31.6.955
van der Velde, J., Williamson, D. L., and Ogilvie, L. D. (2009). Participatory action research: practical strategies for actively engaging and maintaining participation in immigrant and refugee communities. Qual. Health Res. 19:1293. doi: 10.1177/1049732309344207
Wästerfors, D., Åkerström, M., and Jacobsson, K. (2013). “Reanalysis of qualitative data” in The SAGE Handbook of Qualitative Data Analysis, ed. U. Flick (London: SAGE Publications, Inc.), 467–480.
Weech-Maldonado, R., Morales, L. S., Elliott, M., Spritzer, K., Marshall, G., and Hays, R. D. (2003). Race/ethnicity, language, and patients' assessments of care in Medicaid managed care. Health Serv. Res. 38, 789–808. doi: 10.1111/1475-6773.00147
White, A. G. (2012). A Pillar of Protection: Solidarity Resettlement for Refugees in Latin America. UN High Commissioner for Refugees (UNHCR). Available online at: https://www.refworld.org/reference/research/unhcr/2012/en/91253 (accessed December 27, 2023).
Wieland, M. L., Nelson, J., Palmer, T., O'Hara, C., Weis, J. A., Nigon, J. A., et al. (2013). Evaluation of a tuberculosis education video among immigrants and refugees at an adult education center: a community-based participatory approach. J. Health Commun. 18, 343–353. doi: 10.1080/10810730.2012.727952
World Health Organization (2019). A72/25: Promoting the health of refugees and migrants. Draft global action plan, 2019–2023. Report by the Director-General, 2019. Available online at: https://www.who.int/publications-detail/promoting-the-health-of-refugees-and-migrants-draft-global-action-plan-2019-2023
Keywords: Burmese refugee health, culture-centered approach, economic self-sufficiency, meaning-making of health, health self-sufficiency
Citation: Kumar R (2024) Economic self-sufficiency (ESS) as a barrier to health self-sufficiency (HSS) for Burmese refugees in the United States: a culture-centered analysis. Front. Commun. 9:1040895. doi: 10.3389/fcomm.2024.1040895
Received: 09 September 2022; Accepted: 07 February 2024;
Published: 04 April 2024.
Edited by:
Rukhsana Ahmed, University at Albany, United StatesReviewed by:
Shamshad Khan, University of Texas at San Antonio, United StatesCopyright © 2024 Kumar. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rati Kumar, cmt1bWFyQHNkc3UuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.