
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Commun. , 06 July 2023
Sec. Health Communication
Volume 8 - 2023 | https://doi.org/10.3389/fcomm.2023.1205950
This article is part of the Research Topic Integrating Digital Health Technologies in Clinical Practice and Everyday Life: Unfolding Innovative Communication Practices View all 9 articles
 Johanne Stümpel1*
Johanne Stümpel1* Annika Dörrhöfer1
Annika Dörrhöfer1 Pauline Mantell2Christiane Jannes1Alinda Reimer3Christiane Woopen1
Pauline Mantell2Christiane Jannes1Alinda Reimer3Christiane Woopen1Background: In Germany, a growing number of neonatal intensive care units (NICUs) are equipped with webcams. The utilization of webcams in the NICU is gaining greater attention and the impact of this technology can be manifold. However, there has been no definite understanding of its impact. We will highlight the webcam's implications on the communication between parents and Health Care Professionals (HCPs) in German NICUs.
Methods: 20 interviews were conducted with HCPs from three German NICUs between December 2019 and August 2020 according to a qualitative research design. Seven out of them had no webcam experience, whereas for 13 of them, webcam-use is part of their working routine. Interviews were analyzed following Kuckartz's thematic analysis. Findings were assessed in accordance with the NICU Communication Framework.
Results: HCPs consider the webcams as a beneficial addition to the interaction of parents with their infants, as well as the HCP-parent interaction. At the same time, HCPs created new pathways of communication with parents via the webcam. Any negative effects feared by HCPs without webcam experience regarding the communication with parents, including a lasting shift of conversation away from the infant and toward more technical aspects of the webcams, but also an increase in phone calls from parents and an associated increase in workload, could not be confirmed by HCPs with webcam experience.
Conclusion: The findings indicate that the implementation of webcams in German NICUs not only has an influence on the communication between parents and HCPs, but it expands communicative pathways. It can be stated that they support tailored communication but are not necessarily sufficient to account for all aspects themselves. The results of this study help to assess the impact of webcams on communication between parents and HCPs and should be applied to strengthen it within NICUs equipped with webcams.
Clinical trial registration: The Neo-CamCare Study is registered at the German Clinical Trial Register. DRKS-ID: DRKS0001775; Date of registration: 05/09/2019.
The neonatal intensive care unit (NICU) provides critical medical support for pre- and new-born infants. In Germany, around 8.17% of total live births in 2019 were premature births that had to be taken care of in about 215 perinatal centers due to their very low birth weight (VLBW) of <1,500 grams (IQTIG, 2020). The working conditions of Health Care Professionals (HCPs)1 in the NICU setting are often being characterized by high stress levels due to understaffing or poor communication between the staff (Lavoie-Tremblay et al., 2016; Fiske, 2018). Overall, communication and teamwork are considered essential for establishing functioning workflows and ensuring patient safety amongst HCPs but are often hindered by a lack of confidence, lack of organization or structural hierarchies (Foronda et al., 2016). This corresponds to observations made about high communication skills among members of the same profession (e.g., nursing staff) but not between professions (e.g., nurses and physicians) which might explain different assessments of teamwork and collaboration (Lancaster et al., 2015; Profit et al., 2017; Börner et al., 2019). The influence of an introduction of new tools and technologies on teamwork and communication in the health care sector needs to be examined further.
In previous research, concepts such as family integrated care (O'Brien et al., 2015) have argued for a close collaboration between NICU staff and parents to guarantee adequate care for the NICU patients, emphasizing the involvement of parents in the provision of care for their infants (Craig et al., 2015; Maree and Downes, 2016) and the vital importance of good communication between staff and parents (Wigert et al., 2013, 2014; Adama et al., 2022).
Overall, effective communication between parents and HCPs is being reported and a majority of parents is satisfied with the provided emotional support and information given by HCPs (Wigert et al., 2013). Reported inadequacy of communication is often due to the perceived provision of confusing information or the missing treatment of parents as equals to the nurses and therefore requires a closer look at possible improvements (Enke et al., 2017; Lorié et al., 2021). Brought together in the NICU Communication Framework by Wreesmann et al. (2021), four main functions attributing to a successful communication in the NICU can be identified: (1) building and maintaining relationships, (2) exchanging information, (3) (sharing) decision-making between parents and HCPs, and (4) enabling parent self-management. Within these functions, HCPs need to deliberately focus their attention to the topic, aims, location, route, and design of their interaction with parents (see Figure 1).
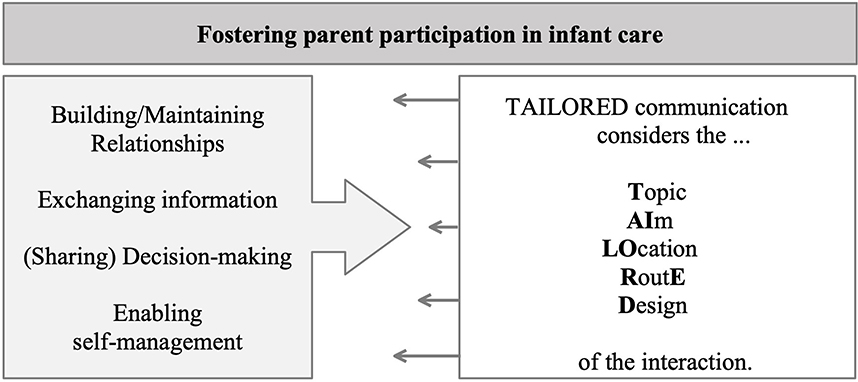
Figure 1. NICU communication framework (own illustration, adapted from Wreesmann et al., 2021).
Especially in the light of the COVID-19 pandemic, hospital restrictions have significantly limited parental presence for NICU admitted infants, necessitating new ways of supporting families after childbirth (Darcy Mahoney et al., 2020; Murray and Swanson, 2020). Also, hospital policies, the severity of the infant's condition, or the parents' own health concerns influence parents' presence in NICUs (Pineda et al., 2018; McCulloch et al., 2022). Parental absence may have negative effects on the parents' mental health and bonding with their infant, as well as the infant's development (Juneja et al., 2022). Efforts are being made to increase parental involvement in the NICU, such as implementing family-centered care models and providing education and support for parents (Franck and O'Brien, 2019; Treyvaud et al., 2019). Furthermore, to overcome physical distance between parents and infants during a NICU stay, webcams are used in few German NICUs and are mostly viewed as a positive experience by parents and families since webcams enable them to view the infants on a monitor when they cannot visit their infants in person (Kerr et al., 2017; Reimer et al., 2021).
Webcam technology is already applied in NICUs worldwide. Therefore, several studies are considering the effects this technology has on parental wellbeing, whereas the perspective of HCPs is less prominent in scientific research. HCPs are likely to recognize a positive impact of webcams, especially in terms of facilitating communication with parents and enabling them to bond with their infants (Hawkes et al., 2015; Epstein et al., 2017). Nevertheless, the scientific literature suggests that HCPs' attitudes toward webcams are weighed against a possible additional workload. The empirical findings for this concern are rather inconclusive and range from no considerable improvement of stress levels to a negative impact on quality of care with possible explanations for these different assessments being the additional effort of operating the webcams or the increased requests of parents (Joshi et al., 2016; Kubicka et al., 2021). Lastly, the level of commitment to the webcams as well as the experience of a positive influence depends on the individual willingness of the HCPs (Hoffmann et al., 2022).
In this study we aim to:
(1) Identify the pathways of communication between parents and HCPs in the NICU-setting following the introduction of webcams and to (2) determine the webcam's influence on the functions and factors relevant in this communication by utilizing Wreesmann's NICU Communication Framework (Wreesmann et al., 2021).
We seek to explore the forms of communication between parents and HCPs in the NICU and aim to contribute to the enhancement of communication between HCPs and parents of VLBW infants by engaging the HCPs perspective.
This research is part of the Neo-CamCare project that examined the use of webcams in German NICUs in a multicentric cross-over design (Scholten et al., 2021). Participation in the Neo-CamCare study was subject to comprehensive information and the written consent of the parents. They were comprehensively informed about the study, the study objectives and the procedure. The webcams were installed at the new-borns' incubators enrolled in the study and could be accessed by the parents via a personalized password online 24 h a day, except for short time periods when diagnostic or invasive procedures were performed on the child. The present study focuses on webcam devices that transfer moving images of the infant's upper body. Health data or sound is not transmitted. A standby mode can be turned on if there should be an occurrence of medical procedures or health related crises. In order to participate in the study, parents had to have access to an internet-enabled device (e.g., laptop or tablet) at home.
In Neo-CamCare, amongst others, qualitative data has been collected via narrative interviews and focus groups to assess effects of webcam-use. This present paper addresses the qualitative evaluation by focusing on the perspective of HCPs as it seeks to explore the influence of the implementation of webcams on the communication and its pathways in the NICU. This qualitative research presented here has been conducted in accordance with the “Consolidated criteria for reporting qualitative research (COREQ)” (Tong et al., 2007) (see Supplementary material). The study protocol was approved by the Ethical Review Committee of the Medical Faculty of the University of Cologne in accordance with the Ethics Committee of the Medical Faculty of the University of Bonn (Number: 19-1232).
Inclusion criteria for study participation were: Current employment as a HCP in the field of neonatal care, to be a trained nurse in the field of neonatology or a medical physician specialized in neonatology. HCPs who had previous experience with webcam-use in the NICU were included in the study, as well as HCPs without webcam experience. The sample size in the context of qualitative research is assumed to be less relevant than in quantitative research, with the suitability of respondents to adequately answer the questions being the main goal (Crouch and McKenzie, 2006). We recruited participants and collected data until the necessary data saturation was reached. The concept of saturation describes a level in data collection where no new information of aspects can be observed in the data (Guest et al., 2006). In the present study data saturation was reached at n = 20. Recruiting the HCPs was facilitated by the nursing management of the respective clinics. Flyers with the invitation to participate in the study were displayed on the wards involved in the project. In addition, the nursing and medical directors of the participating wards/hospitals were personally approached to encourage their colleagues to participate in the study. We aimed to obtain a sample that was as diverse as possible with regard to experiences with the webcam in everyday ward routine. Subsequently, the sample was stratified according to the previous use of webcams and the time they had been using them, in order to ensure equal representation along these dimensions. Also, consideration was given with respect to an equal distribution in terms of the two occupational dimensions (physician vs. nursing health professions) in order to cover both of these perspectives as broadly as possible.
If individuals were interested in participating in the study, they received an information sheet, a short personal questionnaire on socio-economic data, a declaration of consent and a transfer form for the expense allowance. Prior to the interview, the participants were informed and made aware of the purpose and objectives of the study and gave their written consent (by post or in person). For participating in the interview, the participants received an expense allowance of 50€. Upon receipt of the completed forms, a date for the interview was set. Nine interviews were conducted in person and due to the COVID-19 pandemic situation, some of the interviews (6 out of 20) had to be conducted virtually (via Zoom or Adobe Connect) or, if internet access was not available, by phone (n = 5). After a personal introduction and welcome, the interview guide was followed throughout the interview. The main topics of the interview guide are presented in Figure 2. Participants were asked to freely respond to the questions. A pseudo-anonymized evaluation and rigid data protection-compliant processing of the data were guaranteed. The interviews were audio recorded and transcribed verbatim. Any information that could potentially lead to an identification of the individual, such as names, specific locations, or other details, were removed. In total, 20 interviews with HCPs were conducted separately by members of two research teams: 12 interviews by the Research Unit Ethics (JS, PM, and CJ) and 8 additional interviews by the Institute of Medical Sociology, Health Services Research and Rehabilitation Science (IMVR) (conducted by AR) were considered due to a jointly developed interview guide. The leading author, JS (Research Associate, Health Economist, M. Sc.) in association with PM (Research Associate, Health Economist, Dipl.-Ges.oec.), CJ (Research Associate, Health Management, M.A.) and AR (Research Associate, Health Services Researcher, M.Sc.) conducted all interviews. All four female researchers are qualified experts in the field of qualitative research and possess years of experience in this field. Conducting the interviews with two research groups, allowed for researcher triangulation. Thus, a consistently high level of data quality, both at the time of the data collection and during the analysis, was achieved through mutual exchange between the two research groups. Interviews took place between December 2019 and August 2020.
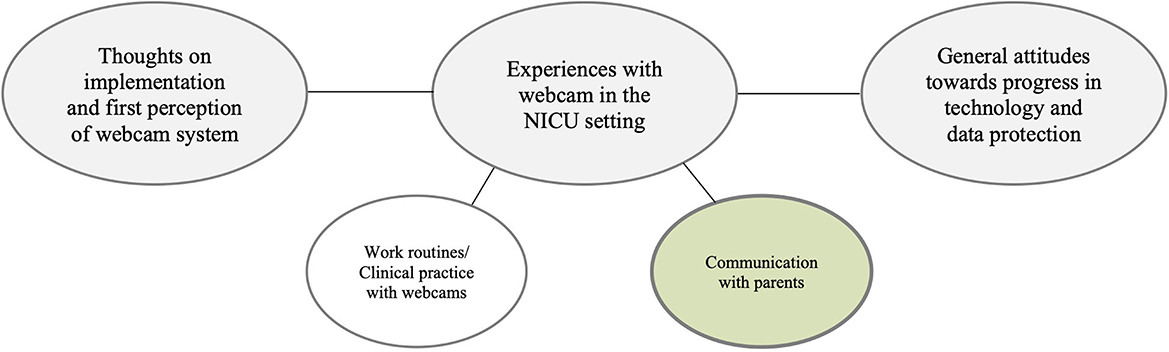
Figure 2. Aspects covered in interview guide (own illustration).
After transcribing, the interviews were cross-checked by a student assistant for accuracy. Two researchers (JS and PM) conducted the thematic qualitative analysis following a combined deductive-inductive approach (Kuckartz, 2018). The analysis of the categorized based analysis was carried out in a multilevel process of category development and coding of text segments. In a first step, two researchers (JS and PM) independently coded the data deductively based on the research question. Deductively, categories were formed based on factors that may have an impact on communication. New codes were then inductively formed within these categories. The data was then reviewed and checked by the two researchers. After coding part of the material, the analysts conducted credibility checks to continuously verify the accuracy of the coding. Inconsistencies in coding were corrected when necessary. The codes were then grouped into main themes and sub-themes. After re-checking by the two researchers, all transcribed material was systematically coded. MAXQDA (version 2020) was used for the qualitative coding. An overview of the identified themes and sub-themes is provided in Supplementary material. Finally, in particular the coded text segments from the themes “implementation of webcam,” “daily work routines with the webcams,” “parent-NICU contact,” and “parent-staff relationship” were revisited to explore how statements referred to aspects of communication brought up in Wreesmann et al.'s NICU Communication Framework.
The participants age ranged from 21 to 58 years. The HCPs experiences with webcams varied between no experience to 3 years of experience. The share of HCPs without any webcam experience was 35%. Participating HCPs had an average of 12.4 years of work experience and a mean age of 36.2 years. An overview of the demographic data of the participants and further sample characteristics can be found in Table 1.
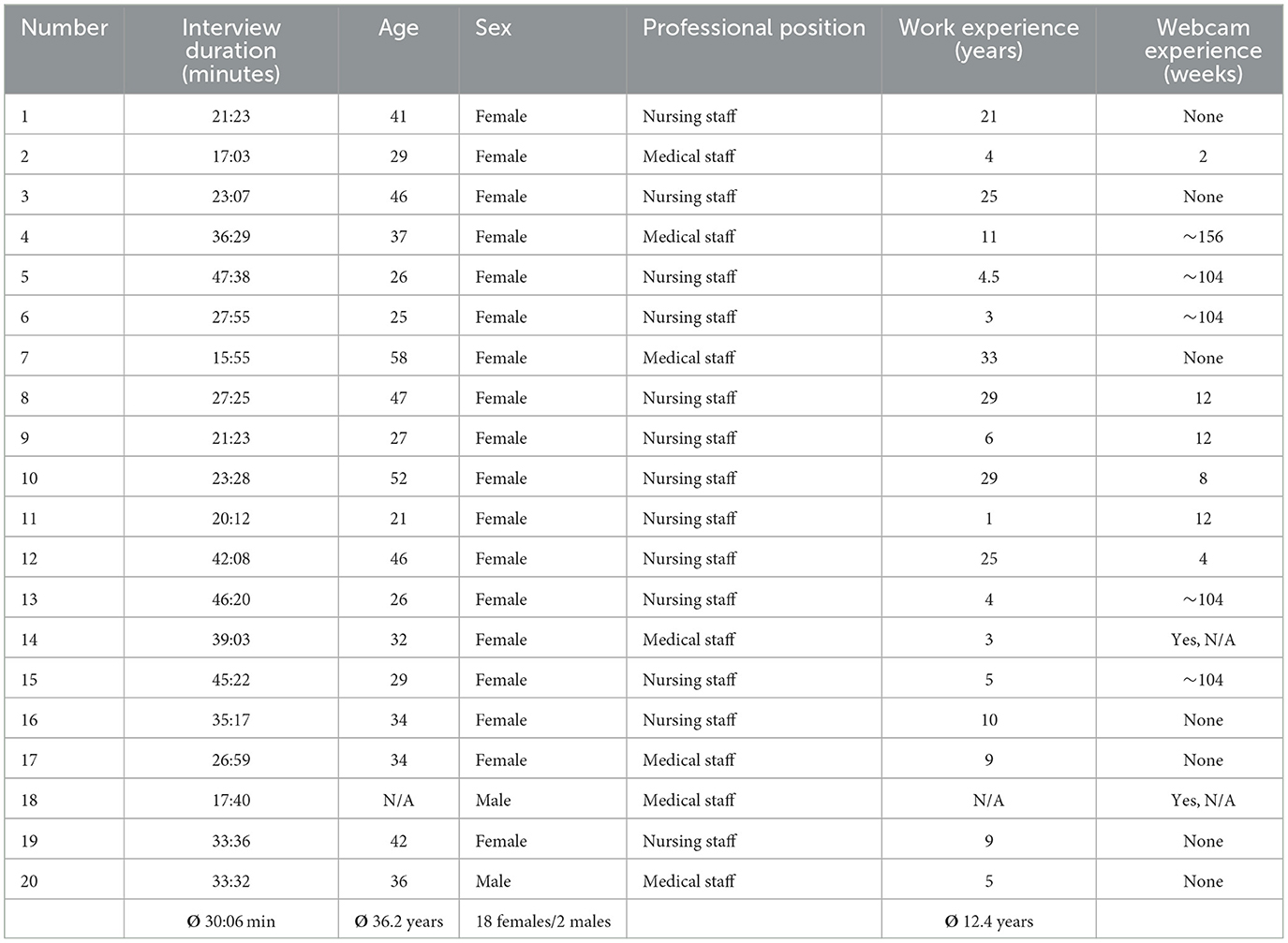
Table 1. Demographical data of participants.
Several different medical professions could be identified from the professional background of the surveyed staff. An overview is provided in Figure 3.
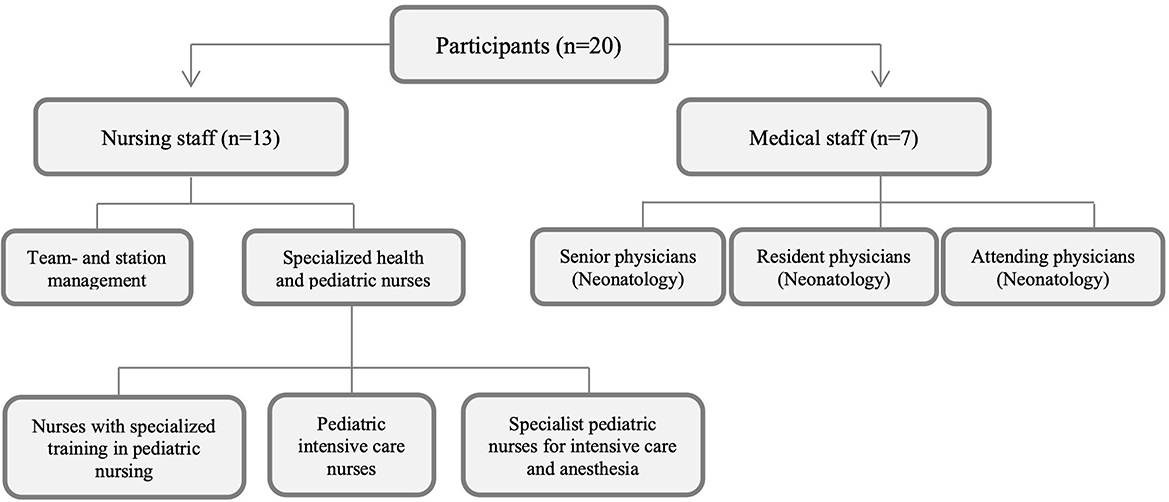
Figure 3. Professional background of participants (own illustration).
Prior to the introduction of the webcam technology, the communication practice in the NICU setting already reflected Wreesmann et al.'s factors (topic, aims, location, route, and design) for a tailored communication across all four functions [building and maintaining relationships, exchanging information, (sharing) decision-making between parents and HCPs, enabling parent self-management]. In conversation with parents, topics mostly relate to health information about the infant. HCPs aim to combat concerns, provide emotional support and reassurance, and build trust. They continuously interact transparently and involve parents in the care provision as equal partners. HCPs additionally put a lot of their effort into designing the conversation as balanced between direct, empathetic and informative. They mostly communicate in person or via telephone. To provide an overview of the communication practices in the NICU prior to the webcams, we include quotes corresponding to the NICU Communication Framework in the following table (Table 2).
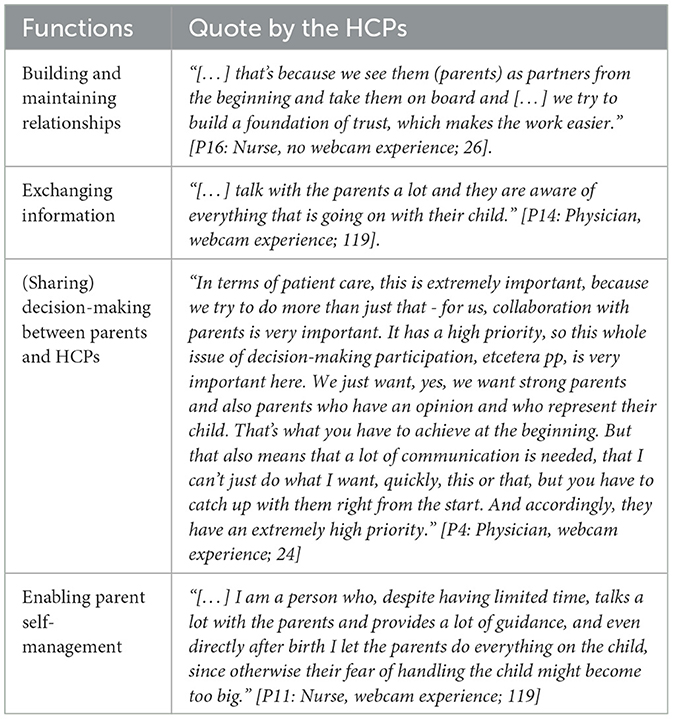
Table 2. Exemplary statements by HCPs in accordance with Wreesmann et al. (2021).
Our research focus in this paper is based on the experiences of HCPs with webcam experience, nevertheless, for a broader understanding and mapping of the context on NICUs, we would like to briefly address which concerns and expectations were expressed by HCPs without webcam experience regarding the impact of the implementation of webcams on communication between parents and them. As one HCP recalls, the overarching concern expressed by HCPs without previous webcam experience was that the implementation of webcams would not only repeatedly disrupt their workflow, but also negatively impact the relationship between parents and HCPs. They mostly worried about technical issues, a sense of being monitored unnecessarily by parents and increasing phone calls caused by the visual images of the webcam being confusing.
“On the one hand, everyone was happy to be able to try it out. And on the other hand, there was also the fear that the phone will ring more often because there is something wrong or you can't see the baby properly and things like that.” [P09: Nurse, webcam experience; 11]
“Some were also afraid that they would be monitored at work and that they would feel a bit restricted.” [P10: Nurse, webcam experience; 17]
Following this brief outline, we will contrast them with the actual experiences made by HCPs. We will do so within the NICU Communication Framework and address how the webcams were expected to, and actually did, impact the aspects of tailored communication between parents and HCPs in nexus with the four mentioned functions and five factors.
To establish a lasting and trusting relationship between parents and HCPs, it is considered helpful to pay respect to aspects of tailored communication. In the context of relationships, the topics of these conversations can be both medical, about the infant, but also more trivial (Wreesmann et al., 2021). In our study, particularly in the early days of the implementation of the webcams in the NICU and whenever parents received a webcam for the first time, the topic of the conversations shifted from medical toward more technical content. Nevertheless, this quickly reverted as parents became comfortable with the webcams and only asked specific medical instead of trivial questions about the state of the infant when calling.
“I think this topic of the camera was of course also bigger in the parents' discussion when we introduced it than it still is now. Now, as a doctor, you are more focused on talking to parents about the medical side: ‘How is the child doing right now? What is the outlook?' These are also the questions parents ask us, which is why we talk less about the camera. So, it's more about the clinical condition of the child and not about the camera.” [P4: Neonatologist, webcam experience; 53]
The HCPs reported that one or two nurses in the teams were normally assigned to set up the initial access to the webcams and also to provide the initial information to the parents. Regular first contact persons, even regarding the technical aspects, served as a useful route to strengthen the trust and the relationship between parents and HCPs after implementing the webcams. The webcams themselves provided an additional way of building trust between parents and HCPs.
“And little by little, we created a team of people who are, so to speak, like the primary instructors, who then train the entire team and can pass on information to parents [...].” [P15: Nurse, webcam experience; 3]
“[...], I believe that a basis of trust is also created between HCPs and parents. So, you can already see how my child is being cared for. And also, this trust, we'll call you if something happens. The camera is not off because we have an emergency, but we would call at any time if something is wrong. I think that also has a lot to do with trust between the HCPs and the parents.” [P13: Nurse, webcam experience; 87]
Whereas, prior to the introduction of webcams, a great deal of interpersonal communication between parents and HCPs took place over the phone, as parents would often inquire about their infant's wellbeing, webcams started to contribute to an increased quieting of the phone. As mentioned above, webcams reduced the need to talk about trivial topics, therefore parts of the conversation had shifted in terms of location. Sensitive topics or specific medical information is still communicated face-to face or over the phone.
“Before the webcam, we simply had the phone ringing very, very often and then parents just asked what the child was doing. And very often you could only say, yes, it was very sweet and is sleeping now.” [P9: Nurse, webcam experience; 51]
“[...]It's more about the clinical condition of the child and not about the camera. Those are the moments when you really have time to talk to parents for a longer period of time. And then maybe the conversation turns occasionally to the camera. But in the stressful daily routine of intensive care, that's rarely the case for doctors.” [P04: Physician, webcam experience; 53]
Most parents view the NICU as a stressful and frightening environment, and therefore HCPs aim at communicating with parents with the goal of making the NICU as comforting as possible. HCPs report that the webcams help parents briefly check in on their infants on a recurring basis to see if they are doing well and feel more reassured.
“And now that it's up and running and working, I think it's really great, because parents can be much more relaxed when they're at home.” [P9: Nurse, webcam experience; 85]
Lastly, in order to build and maintain relationships, HCPs continuously try to design the communication as transparent, clear and benevolent, also when using the webcams. This included, for example, providing information and explanations about the procedures being performed on the infant. The webcams contributed to trust-building because they helped to increase the transparency of even minor care procedures on the infant if the webcams are not turned off in those procedures.
“If you talk to the parents well and explain it to them well, then it's no problem at all.” [P15: Nurse, webcam experience; 57]
“[…] I am a person who, despite having limited time, talks a lot with the parents and provides a lot of guidance, and even directly after birth I let the parents do everything on the child, since otherwise their fear of handling the child might become too big.” [P11: Nurse, webcam experience; 119]
In terms of exchanging information, HCPs report that the webcams serve to provide the parents with day-to-day and trivial information about their infants, like if they are awake, how they look and how big they have gotten. Because the webcam enables parents to gain more insights into their infants' wellbeing, these topics are already addressed and not part of personal interactions between parents and HCPs anymore.
“As I said, the parents now get to see a bit more or see things that they normally do NOT see because they can't be on the ward.” [P13: Nurse, webcam experience; 125]
“These calls about ‘what is it doing right now and is it sleeping or...', they have clearly, clearly become less.” [P9: Nurse, webcam experience; 55]
HCPs reported that the amount of information and the way of exchanging certain information via webcam depended on both sides. Parents let HCPs know if there were medical or nursing procedures they did not want to see via webcam and vice versa. It was individually agreed upon, in which cases the webcams served as the best route and location to exchange information.
“Of course, if you have to do something on the child for the examination, we turn the camera off. That is actually better for the parents. They also feel safer. Because then they only see hands and don't know what's happening […] But in normal care, when you're just changing diapers, for example, it's always individual. Some leave the monitor on; others turn it off. Sometimes the parents say we'd rather not see it. Then we turn it off and don't turn it on again until the child is completely cared for.” [P8: Nurse, webcam experience; 21]
This arrangement served the HCPs' aim to ensure that the parents receive all the relevant information they seek without overwhelming them. It was also important to the HCPs to ensure that when they exchange information with parents, there would not be misunderstandings. They realized that unambiguous scenes on the livestream feed would necessitate additional dialogue which would then have to be communicated personally.
“Basically, however, it [the webcams] is not different from the quality […]. But I think what's missing is simply the communication with the parents during care. […] you are not able to talk to them while they watch. You can't tell them the reasons for your actions and you are unable to communicate details. […] I think, it always is a bit difficult to do something without being able to talk about it in some way, because that is just a bit of our culture here, that you just talk/explain to parents while caring for their child.” [P16: Nurse, no webcam experience; 84]
Thus, in order to keep the clear and comprehensible design of an information exchange, the HCPs addressed any questions the parents might have about the webcam, as well as situations they saw on the webcam.
“There are moments like that in between, because either it was a situation where you might even have consciously said to the parents: ‘Maybe you saw it on the camera, that and the other thing' or something like that. But that was actually, I would say, more in the early days, when we first started with the camera, that you also talked about it somehow with parents. Now, to be honest, it's not something I talk about with parents and the parents actually don't contact […] in relation to the camera. No.” [P4: Neonatologist, webcam experience; 33]
Within our study population, the possibility, and the implicit invitation to the parents to participate in the decision-making process at any time is based on the HCPs' aim at involving the parents in infant's care at an early stage and at any time and being available for discussions and questions. The webcams provided an additional way for the parents to get involved in the care of their infants, as they were able to voice concerns about specific situations, they experienced via webcam:
“They see that the child is crying or has spat or I don't know, something else that can be seen in the picture, which somehow worries the parents or seems strange and then they simply call again and ask.” [P6: Nurse, webcam experience; 39]
HCPs see the continuous communication with and the involvement of the parents into the care process as a fundamental principle of their work and try to design transparent and encouraging interactions.
“Parents should know what we do with their child or what the therapy looks like, they should know what is on the monitor, so they should be able to assess it. And they are also involved in therapy decisions, yes. And that is another integral part of this camera system, that we say we have maximum transparency.” [P6: Nurse, webcam experience; 35]
In this way, the webcams served as a route and a location that enabled parents to gain more insight into their infant's care and helped them to feel as an equal partner of care provision. Nevertheless, HCPs left it to the parents to individually decide, if they felt comfortable using the webcams as part of the care process, therefore also sharing decision-making competencies in terms of the webcam implementation itself:
“And the people who are offered this are very different, because some reject the camera and say, ‘no, we don't think that's something for us, it's more important for us to be here on site', and that's totally fine. And the others who just say, ‘we think it's totally great, we'd like to think about it, and as soon as a camera becomes available, we'd like to have one'.” [P3: Nurse, no webcam experience; 10]
As already stated, in the beginning of the introduction of webcams, the HCPs recognized a temporary shift of topics away from the infant and toward the technical details of the webcams. Topics like insecurities about the technical features, data security and the proper handling of the webcam which needed to be addressed by HCPs prior to use, could therefore potentially influence parents' involvement. Nevertheless, HCPs mostly viewed the webcams as a positive feature and could not confirm that the level of parent-HCP decision-making was negatively influenced.
“Most of the time they are enthusiastic. Sometimes they are also insecure because they worry, ‘oh, camera on my child, who's going to see all that? Especially if it is somehow connected to the internet.' But basically, once you have installed the camera and the parents can really see their child, all negative thoughts about it are usually out of the room. Instead, they are actually more positively surprised and give positive feedback that they can see their child even when they are not there.” [P6: Nurse, webcam experience; 49]
Enabling self-management of healthcare providers in German NICUs can improve the quality of care and promote better outcomes for infants and their families. Self-management empowers healthcare providers to take ownership of their work, make decisions based on their expertise, and collaborate more effectively with other members of the healthcare team. Regarding self-management of HCPs, they report that the topic of conversation, especially in the first period of the webcam implementation, mainly revolved around technical features and problem solving of the webcams. In this phase, the conversation within the HCP-Team mainly addressed mitigating possible additional workload and aimed at allocating responsibilities within the NICU-team and combating feelings of uncertainty in dealing with the webcams due to a lack of technical knowledge.
Regarding the tailored communication between healthcare professionals and parents, webcams became an integral part to enabling self-management of parents as well. They influenced the communication by supporting the HCPs in their aim to increase in parental satisfaction and autonomy, so that the parents gain more freedom in their day-to-day life:
“For me personally, it makes no difference in my daily routine whether I take care of a child with or without a webcam. And you really notice that the number of telephone calls has decreased, where the only questions would have been: ‘Is my baby asleep or what is he or she doing?' That's a lot more relaxed. So, I'm really happy so far.” [P9: Nurse, webcam experience; 85]
Additionally, as one HCP highlights, the webcams represent an additional route and location of communication, but never a substitute for face-to-face communication with parents. Nevertheless, webcams can help to broaden the options for self-management by providing a new way of functioning. Parents can frequently access their infant's condition via the webcams, something that studies have demonstrated lowers parental stress levels. HCPs also highlight the importance of enabling parents to find their own way of incorporating the webcams into their daily life and acknowledge the diversity of handling webcam-use:
“There is such a variety of parents. Some are here all day, even if they have the camera. There is one person, for instance, who is here around the clock despite having the camera. And others come only once or only briefly. So, it varies. But I don't think that the camera influences that, it's simply up to the parents themselves.” [P10: Nurse, webcam experience; 109]
“And I think that parents can decide: ‘Do I want to see it now?', which also gives them the opportunity to say ‘I don't want to see it all day' […].” [P4: Neonatologist, webcam experience, 47]
Through the implementation of the webcams, the design of an understanding and empowering interaction and environment with parents can further be strengthened.
“And I think you also get something back in return if you take care of it a bit, ensuring that the camera runs well, and offering that to the parents. The parents are very grateful.” [P18: Neonatologist, webcam experience; 23]
Subsequently to the presentation that the four functions and five factors of the NICU communication framework also apply when webcams are added to the communication practice, we will now consider in more detail how the HCPs created new ways of communicating whilst using the webcams.
A main objective of this research was to identify communication pathways that have not been in the focus of previous research and that are not obvious at first glance. Webcams themselves can be considered as a tool that is used to communicate, as well as a supplement for the communication that previously took place. According to several HCPs, any interaction between the parents and their infant is important. The HCPs recognize the webcams as a means of communication and valuable contribution toward tailored communication and are therefore very supportive of the webcams:
“However, that's because I totally approve of modern ways of communication and all that, and I also think it's really important that parents have a lot of communication with their infants in any form.” [P15: Nurse, webcam experience; 5]
“For example, I had this situation where a child was still totally awake after being cared for professionally and lay awake in the incubator. And then the parents somehow called again anyway and wanted to know how the child was doing […]. And then I said to my colleague: No, everythin g's okay with the child, the parents should turn on the camera, little XY is awake right now. And I personally thought that was nice […]. We perceive many moments of the infants that the parents cannot experience because they are asleep at home or cannot be there for other reasons. And I think that's actually nice, that you can share that with the parents […] So, I actually see that as more of a positive than a negative thing.” [P12: Nurse, webcam experience; 51]
In addition to the webcams contribution of creating a feeling of closeness between parents and infant, the webcams were also utilized in HCP-parent communication. It was previously observed that communication between parents and HCPs occurred primarily verbally in face-to-face conversations (in the NICU) or by telephone. The latter was mainly utilized by the parents at night. To address the missing ability to reassure parents or answer upcoming questions overnight via webcams, HCPs sought a new way to keep up tailored communication:
New pathways that we were able to identify included the communication via short notes that were placed in the incubator by HCPs when needed. Some HCP-teams jointly agreed that the webcams would not be turned off during everyday procedures that required the infant to be taken out of the incubator, but that small notes would be left for the parents to bridge missing interpersonal conversation. These notes provided information such as: “Being washed, be right back” or “Short breastfeeding break, be right back”. Also, if anything particularly noteworthy had happened that day, it was written on the notes by the nurses, if time allowed:
“It' s great when you don't see them [the parents] and you're on nightshift, and then you can write them a message saying: ‘I was happy today' or ‘I'm so and that tall today and I weigh this and that, greetings', and the name of the child. You can even add it as a comment. They are totally happy. You can make parents happy.” [P8: Nurse, webcam experience; 23]
HCPs thus sought to offer comfort and guidance to parents during an emotionally distressing time, as well as providing transparency for their actions. They sought to create a way to communicate everyday information in a supportive and educational way. The HCPs also acted very compassionate toward parents and used the webcams to share moments with parents, so they were able to engage with the infants personally.
However, it should be pointed out that especially in the first period of the implementation of the webcams, the HCPs report that there was an additional workload due to technical problems, the allocation of responsibilities within the NICU-team and feelings of uncertainty in dealing with the webcams due to a lack of technical knowledge. The webcams, as one HCP highlights, represent an additional means of communication, but never a substitute for face-to-face communication with parents.
In conclusion, contrary to some worries, the introduction of webcams to the NICU did not negatively impact the quality of communication and provision of care from the HCPs point of view. We were able to outline shifts in the communication between parents and HCPs along Wreesmann et al.'s framework but can still confirm the HCPs efforts to comply with the functions and address the factors for tailored communication when using the webcams. Maintaining tailored communication and creatively shaped webcam-use in times when shortcomings of the webcams arose, highlights the effort HCPs put into shaping good communication with parents at all times. In addition, we were able to identify and describe new ways of communication between parents and HCPs that emerged because of the webcams.
The present study provides insights into webcam-use and its impact on collaboration and communication between parents and HCPs. With the focus being set on experiences, thoughts and opinions from HCPs instead of parents, the study is able to fill in the prevalent gap of research on webcam-use in German NICUs. Our findings regarding the communication between parents and HCPs were analyzed in the context of the NICU Communication Framework by Wreesmann et al. (2021). Overall, despite a few initial technical difficulties in the implementation phase of the webcams, we can conclude that tailored communication between parents and HCPs in the NICU-setting is possible and well perceived with regard to the four functions of communication [1. building/maintaining relationships, 2. exchanging information, 3. (sharing) decision-making, 4. enabling parent self-management] (Wreesmann et al., 2021) after the introduction of webcams. Our results indicate a positive impact of the webcams, as HCPs state that the webcam implementation results in fewer telephone calls, a perceived increase in parental satisfaction due to lower stress levels, and an expansion of communication between parents and HCPs due to new communication pathways such as the communication via notes in the incubator. Further, our results corroborate the findings of previous scientific studies and complement them by providing new insights into parent-HCP communication in the NICU. Kilcullen et al. (2020) describe the fears and challenges that HCPs experience when implementing webcams on the NICU, but likewise acknowledge the perceived benefit to parents of VLBWs that HCPs witness. Moreover, despite negative impacts feared by HCPs without webcam experience our results reveal that the HCPs with webcam experience do not feel any additional stress caused by the implementation of the webcams, neither for themselves and their workflow, or the parents. These findings are well in line with the work of Kubicka et al. (2021) who similarly report no effect of webcam related stress for the nursing staff but instead lower parental stress levels. Our work reveals that there are specific topics within the four functions of the NICU Communication Framework that can easily be addressed via webcam, such as descriptive information (about the infant). Other research based on Wreesmann's NICU Communication Framework such as Labrie et al. (2021) and Lorié et al. (2021) highlight the importance of unambiguous information as well as the value of casual conversation and continuous interactions between HCPs and parents, which our findings about communication practices with webcams corroborate. For the webcams, the main focus of communication lies on maintaining a balance between informative and interpersonal conversations (design). However, it is also clear that there are certain topics that require personal, private conversations (locations). In the context of this study, webcams represent a facilitating tool, which alone, however, cannot necessarily meet all the requirements of HCP-parent communication/relationship.
At this point, potential limitations and improvements should be mentioned.
Firstly, the study was conducted under extraordinary circumstances which might have influenced the observations and findings. The COVID-19 pandemic especially affected the healthcare sector, leading to a further increase in psychological stress and reinforcing the already existing discrepancies in the work environment that put healthcare workers in high pressure situations and have them face increased workload (Petzold et al., 2020; Stuijfzand et al., 2020). Additionally, Vindrola-Padros et al. (2020) remarks that, compared with other research designs, the conduct of qualitative research in the context of infectious epidemics like the COVID-19 pandemic in general remains to lag in terms of delivery, credibility, and timeliness of findings. During the pandemic, hospitals and HCPs often faced increased amounts of workload, disruptions to the usual workflows as well as social distancing regulations for visitors, which in sum might have influenced the conditions under which the webcams were introduced and also evaluated during the interviews. The pandemic and its social distancing regulations also influenced the recruitment of participants and the execution of the interviews. In order to continue the research, a switch from standard face-to-face data collection methods to remote data collection was necessary. The interviews were conducted virtually via video conferencing, with regular phone calls being the exception when the participant did not have the technical equipment at disposal. This relates to limitations regarding the diversity of experience and representativeness (Torrentira, 2020; Hensen et al., 2021). In our study this corresponds to the sample including more females than males, leading to the male perspective potentially being underrepresented. Moreover, it can be assumed that HCPs who had already used a webcam system might be more approving of the system than those who never had the opportunity to experience webcam-use and had to adapt to it first (Kilcullen et al., 2020; Hoffmann et al., 2022). Potential effects on results due to demographic characteristics of the respondents were not part of the in-depth analysis in our research. Further studies might reveal impacts upon the communication between parents and HCPs in the NICU in terms of age, professional experience or general perceptions of technological innovations.
Also, the existence of potential linguistic barriers was not investigated in our study due to limitations of time and available capacity. In particular, linguistic barriers that may occur in the course of differing native languages among both parents and HCPs seem to be relevant in the context of the communication in the NICU and potentially impact the face-to-face and digital parent-HCP communication (Hendson et al., 2015; Kynoe et al., 2020).
This work is based on the NICU Communication Framework according to Wreesmann et al. (2021) which, due to its wide applicability in different settings, makes it a useful tool for improving communication. The framework is also comprehensive as it covers a wide range of communication factors, including communication skills, teamwork and collaboration, use of visual aids, cultural and linguistic competency, and emotional support and counseling. This comprehensive approach helps to ensure that all aspects of communication are considered when applied to the individual NICU setting. Also, the framework has an evidence-based approach, was developed based on the best available research, and incorporates the experiences of HCPs, parents, and caregivers which helps ensure that the framework is effective in practice. The framework is designed to be used in a variety of settings, including academic medical centers, community hospitals, and other neonatal health care settings (Wreesmann et al., 2021). Beside our study, the framework has not been used to examine parent-HCP communication via digital communication tools in NICUs. One the one hand, this fact presents a potential limitation of our findings. At the same time this makes our study a valuable contribution to questions about successful patient engagement in digital health care and the nursing perspective which are raised in Auxier et al. (2023) and therefore indicates an opportunity for further research.
Since the aim of qualitative research is to investigate and to explore interactions instead of making generalizable statements, achieving representativeness for a population when choosing the sample is only the secondary objective (Marshall, 1996). Our sample is appropriate concerning sample size and heterogeneity for the research purpose of contrasting experiences and influences of webcam-use; thus, the results hold scientific value. The investigator triangulation also allowed for the inclusion of various research perspectives and therefore increased the credibility of data.
In summary, our results are to be understood as a valuable snapshot under the condition of a pandemic and would benefit from additional studies and interviews under regular circumstances. Furthermore, since our study is embedded in a cross-sectional research design, a longitudinal study regarding the expectation and the actual change in communication over time between parents and HCPs would be desirable.
This study provides, to the best of our knowledge, first insights into the impact of webcam implementation in German NICUs on communication and communicative pathways between parents and HCPs. The results also reveal new pathways for communication between parents and HCPs, which will inevitably become more important in the wake of increasing digitization. These new pathways of communication help to foster a culture of collaboration and open dialogue in NICU settings. Nevertheless, our results also reveal that webcam-use should be understood as an additional means of communication and not a replacement for interpersonal conversations. The results of this study indicate that the communication model described by Wreesmann et al. (2021) can also be applied to NICUs with webcams. We are confident that our research can provide a basis of orientation and best-practice learnings for NICUs interested in the implementation of webcams. For subsequent research, consideration should be given to applying the model to technical/digitized communication practices in the NICU as well as gathering longitudinal data about communication patterns in NICUs.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study protocol was approved by the Ethical Review Committee of the Medical Faculty of the University of Cologne in accordance with the Ethics Committee of the Medical Faculty of the University of Bonn (Number: 19-1232). The participants provided their written informed consent to participate in this study.
JS, PM, CJ, and AR recruited participants, conducted all interviews, and were part of the team who generated the interview guide and analyzed the data. CW contributed to this work as the senior author and provided to the study's conceptualization, design, data interpretation, and manuscript preparation. JS and AD prepared the manuscript. PM contributed to the study design, the analysis, and interpretation of the data. CJ and AR provided revisions of the intellectual content critically reviewed the manuscript. All authors proofread and agreed upon the final version of the manuscript.
This work was supported by the Joint Federal Committee's innovations fund (G-BA- Innovationsfonds) under grant number: 01VSF18037.
A special thank goes to the Health Care Professionals from the NICUs who shared their concerns, opinions and experiences about the webcams with us. This work would not have been made possible without these valuable interviews. We would also like to thank PD Dr. Nadine Scholten (University Cologne) and Dr. Till Dresbach (University Hospital of Bonn) who supported our work as scientific heads of Neo-CamCare. The paper is part of the Neo-CamCare project, with the participation of the following applicants: Dr. Nadine Scholten (IMVR, University of Cologne), Prof. Dr. Andreas Müller (Neonatology and Pediatric Intensive Care Medicine, University Hospital Bonn), Dr. Till Dresbach (Neonatology and Pediatric Intensive Care Medicine, University Hospital Bonn), Prof. Dr. Martin Hellmich (IMSB, University Hospital Cologne), Christina Samel (IMSB, University Hospital Cologne), Prof. Dr. CW (Center for Life Ethics/Hertz Chair TRA 4, University of Bonn), CJ (Center for Life Ethics, University of Bonn), Prof. Dr. Ludwig Kuntz (Health Care Management, University of Cologne), Prof. Dr. Indra Spiecker gen. Döhmann (Data Protection Research Unit, Goethe-University of Frankfurt), Dr. Sebastian Bretthauer (Data Protection Research Unit, Goethe-University of Frankfurt), Dr. Dirk Horenkamp-Sonntag (Techniker Krankenkasse), and Stefanie Wobbe-Ribinski (DAK Gesundheit).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcomm.2023.1205950/full#supplementary-material
NICU, Neonatological Intensive Care Units; HCP, Health Care Professional; VLBW, Very Low Birth Weight.
1. ^References to Health Care Professionals (HCPs) in this paper relate equally to the nursing and medical staff working in the NICU. Due to the anonymization process,we decided not to providemore detailed information on the individual educational levels and professional functions, such as team leader or senior physician, of the staff on the NICU.
Adama, E. A., Adua, E., Bayes, S., and Mörelius, E. (2022). Support needs of parents in neonatal intensive care unit: An integrative review. J. Clin. Nurs. 31, 532–547. doi: 10.1111/jocn.15972
Auxier, J. N., Bender, M., Hakojärvi, H. R., and Axelin, A. M. (2023). Patient engagement practice within perinatal eHealth: a scoping review. Nursing Open. doi: 10.1002/nop2.1822. [Epub ahead of print].
Börner, N., Mache, S., Scutaru, C., Metze, B., and Bührer, C. (2019). Kommunikation im klinischen Alltag neonatologischer Intensivmedizin [Communication in the clinical routine of neonatologists]. Z. Geburtshilfe Neonatol. 223, 92–98. doi: 10.1055/a-0651-5162
Craig, J. W., Glick, C., Phillips, R., Hall, S. L., Smith, J., and Browne, J. (2015). Recommendations for involving the family in developmental care of the NICU baby. J. Perinatol. 35 (Suppl. 1), 5–8. doi: 10.1038/jp.2015.142
Crouch, M., and McKenzie, H. (2006). The logic of small samples in interview-based qualitative research. Soc. Sci. Inform. 45, 483–499. doi: 10.1177/0539018406069584
Darcy Mahoney, A., White, R. D., Velasquez, A., Barrett, T. S., Clark, R. H., and Ahmad, K. A. (2020). Impact of restrictions on parental presence in neonatal intensive care units related to coronavirus disease 2019. J. Perinatol. 40 (Suppl. 1), 36–46. doi: 10.1038/s41372-020-0753-7
Enke, C., Oliva Y Hausmann, A., Miedaner, F., Roth, B., and Woopen, C. (2017). Communicating with parents in neonatal intensive care units: the impact on parental stress. Patient Educ. Couns. 100, 710–719. doi: 10.1016/j.pec.2016.11.017
Epstein, E. G., Arechiga, J., Dancy, M., Simon, J., Wilson, D., and Alhusen, J. L. (2017). Integrative review of technology to support communication with parents of infants in the NICU. J. Obstetr. Gynecol. Neonatal Nurs. 46, 357–366. doi: 10.1016/j.jogn.2016.11.019
Fiske, E. (2018). Nurse stressors and satisfiers in the NICU. Adv. Neonatal Care 18, 276–284. doi: 10.1097/ANC.0000000000000514
Foronda, C., MacWilliams, B., and McArthur, E. (2016). Interprofessional communication in healthcare: an integrative review. Nurse Educ. Pract. 19, 36–40. doi: 10.1016/j.nepr.2016.04.005
Franck, L. S., and O'Brien, K. (2019). The evolution of family-centered care: from supporting parent-delivered interventions to a model of family integrated care. Birth Defects Res. 111, 1044–1059. doi: 10.1002/bdr2.1521
Guest, G., Bunce, A., and Johnson, L. (2006). How many interviews are enough? Field Methods 18, 59–82. doi: 10.1177/1525822X05279903
Hawkes, G. A., Livingstone, V., Ryan, C. A., and Dempsey, E. M. (2015). Perceptions of webcams in the neonatal intensive care unit: here's looking at you kid! Am. J. Perinatol. 30, 131–136. doi: 10.1055/s-0034-1376388
Hendson, L., Reis, M. D., and Nicholas, D. B. (2015). Health care providers' perspectives of providing culturally competent care in the NICU. J. Obstetr. Gynecol. Neonatal Nurs. 44, 17–27. doi: 10.1111/1552-6909.12524
Hensen, B., Mackworth-Young, C. R. S., Simwinga, M., Abdelmagid, N., Banda, J., Mavodza, C., et al. (2021). Remote data collection for public health research in a COVID-19 era: ethical implications, challenges and opportunities. Health Policy Plan. 36, 360–368. doi: 10.1093/heapol/czaa158
Hoffmann, J., Reimer, A., Mause, L., Müller, A., Dresbach, T., and Scholten, N. (2022). Driving new technologies in hospitals: association of organizational and personal factors with the readiness of neonatal intensive care unit staff toward webcam implementation. BMC Health Serv. Res. 22, 787. doi: 10.1186/s12913-022-08072-5
IQTIG (2020). Qualitätsreport. Berlin: Institut für Qualitätssicherung und Transparenz im Gesundheitswesen. Available online at: https://iqtig.org/downloads/berichte/2019/IQTIG_Qualitaetsreport-2020_2021-02-11.pdf (accessed March 17, 2022).
Joshi, A., Chyou, P.-H., Tirmizi, Z., and Gross, J. (2016). Web camera use in the neonatal intensive care unit: impact on nursing workflow. Clin. Med. Res. 14, 1–6. doi: 10.3121/cmr.2015.1286
Juneja, M., Gupta, A., Sairam, S., Jain, R., Sharma, M., Thadani, A., et al. (2022). Diagnosis and management of global development delay: consensus guidelines of growth, development and behavioral pediatrics chapter, neurology chapter and neurodevelopment pediatrics chapter of the Indian Academy of Pediatrics. Indian Pediatr. 59, 401–415. doi: 10.1007/s13312-022-2522-5
Kerr, S., King, C., Hogg, R., McPherson, K., Hanley, J., Brierton, M., et al. (2017). Transition to parenthood in the neonatal care unit: a qualitative study and conceptual model designed to illuminate parent and professional views of the impact of webcam technology. BMC Pediatr. 17, 158. doi: 10.1186/s12887-017-0917-6
Kilcullen, M. L., Kandasamy, Y., Evans, M., Kanagasignam, Y., Atkinson, I., van der Valk, S., et al. (2020). Neonatal nurses' perceptions of using live streaming video cameras to view infants in a regional NICU. J. Neonatal Nurs. 26, 207–211. doi: 10.1016/j.jnn.2020.01.012
Kubicka, Z., Zahr, E., Clark, P., Williams, D., Berbert, L., and Arzuaga, B. (2021). Use of an internet camera system in the neonatal intensive care unit: parental and nursing perspectives and its effects on stress. J. Perinatol. 41, 2048–2056. doi: 10.1038/s41372-021-00934-w
Kuckartz, U. (2018). Qualitative Inhaltsanalyse. Methoden, Praxis, Computerunterstützung (4. Auflage). Grundlagentexte Methoden. Beltz Juventa.
Kynoe, N. M., Fugelseth, D., and Hanssen, I. (2020). When a common language is missing: nurse-mother communication in the NICU. A qualitative study. J. Clin. Nurs. 29, 2221–2230. doi: 10.1111/jocn.15212
Labrie, N. H., van Veenendaal, N. R., Ludolph, R. A., Ket, J. C., van der Schoor, S. R., and van Kempen, A. A. (2021). Effects of parent-provider communication during infant hospitalization in the NICU on parents: a systematic review with meta-synthesis and narrative synthesis. Patient Educ. Couns. 104, 1526–1552. doi: 10.1016/j.pec.2021.04.023
Lancaster, G., Kolakowsky-Hayner, S., Kovacich, J., and Greer-Williams, N. (2015). Interdisciplinary communication and collaboration among physicians, nurses, and unlicensed assistive personnel. J. Nurs. Scholarship 47, 275–284. doi: 10.1111/jnu.12130
Lavoie-Tremblay, M., Feeley, N., Lavigne, G. L., Genest, C., Robins, S., and Fréchette, J. (2016). Neonatal intensive care unit nurses working in an open ward: stress and work satisfaction. Health Care Manag. 35, 205–216. doi: 10.1097/HCM.0000000000000122
Lorié, E. S., Willem-jan, W. W., van Veenendaal, N. R., van Kempen, A. A., and Labrie, N. H. (2021). Parents' needs and perceived gaps in communication with healthcare professionals in the neonatal (intensive) care unit: a qualitative interview study. Patient Educ. Couns. 104, 1518–1525. doi: 10.1016/j.pec.2020.12.007
Maree, C., and Downes, F. (2016). Trends in family-centered care in neonatal intensive care. J. Perinat. Neonatal Nurs. 30, 265–269. doi: 10.1097/JPN.0000000000000202
Marshall, M. N. (1996). Sampling for qualitative research. Fam. Pract. 13, 522–525. doi: 10.1093/fampra/13.6.522
McCulloch, H., Campbell-Yeo, M., Richardson, B., Dol, J., Hundert, A., Dorling, J., et al. (2022). The impact of restrictive family presence policies in response to COVID-19 on family integrated care in the NICU: a qualitative study. HERD 15, 49–62. doi: 10.1177/19375867211065178
Murray, P. D., and Swanson, J. R. (2020). Visitation restrictions: is it right and how do we support families in the NICU during COVID-19? J. Perinatol. 40, 1576–1581. doi: 10.1038/s41372-020-00781-1
O'Brien, K., Bracht, M., Robson, K., Ye, X. Y., Mirea, L., Cruz, M., et al. (2015). Evaluation of the family integrated care model of neonatal intensive care: a cluster randomized controlled trial in Canada and Australia. BMC Pediatr. 15, 210. doi: 10.1186/s12887-015-0527-0
Petzold, M. B., Plag, J., and Ströhle, A. (2020). Umgang mit psychischer Belastung bei Gesundheitsfachkräften im Rahmen der Covid-19-Pandemie [Dealing with psychological distress by healthcare professionals during the COVID-19 pandemia]. Nervenarzt 91, 417–421. doi: 10.1007/s00115-020-00905-0
Pineda, R., Bender, J., Hall, B., Shabosky, L., Annecca, A., and Smith, J. (2018). Parent participation in the neonatal intensive care unit: predictors and relationships to neurobehavior and developmental outcomes. Early Hum. Dev. 117, 32–38. doi: 10.1016/j.earlhumdev.2017.12.008
Profit, J., Sharek, P. J., Kan, P., Rigdon, J., Desai, M., Nisbet, C. C., et al. (2017). Teamwork in the NICU setting and its association with health care-associated infections in very low-birth-weight infants. Am. J. Perinatol. 34, 1032–1040. doi: 10.1055/s-0037-1601563
Reimer, A., Mause, L., Hoffmann, J., Mantell, P., Stümpel, J., Dresbach, T., et al. (2021). Webcam use in German neonatological intensive care units: an interview study on parental expectations and experiences. BMC Health Serv. Res. 21, 970. doi: 10.1186/s12913-021-06901-7
Scholten, N., Bretthauer, S., Eilermann, K., Hagemeier, A., Hellmich, M., Hoffmann, J., et al. (2021). The effects of webcams on German neonatal intensive care units - study protocol of a randomised crossover trial (Neo-CamCare). BMC Health Serv. Res. 21, 456. doi: 10.1186/s12913-021-06387-3
Stuijfzand, S., Deforges, C., Sandoz, V., Sajin, C.-T., Jaques, C., Elmers, J., et al. (2020). Psychological impact of an epidemic/pandemic on the mental health of healthcare professionals: a rapid review. BMC Public Health 20, 1230. doi: 10.1186/s12889-020-09322-z
Tong, A., Sainsbury, P., and Craig, J. (2007). Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 19, 349–357. doi: 10.1093/intqhc/mzm042
Torrentira, M. C. Jr. (2020). Online data collection as adaptation in conducting quantitative and qualitative research during the Covid-19 Pandemic. Eur. J. Educ. Stud. 7, 78–87. doi: 10.46827/ejes.v7i11.3336
Treyvaud, K., Spittle, A., Anderson, P. J., and O'Brien, K. (2019). A multilayered approach is needed in the NICU to support parents after the preterm birth of their infant. Early Hum. Dev. 139, 104838. doi: 10.1016/j.earlhumdev.2019.104838
Vindrola-Padros, C., Chisnall, G., Cooper, S., Dowrick, A., Djellouli, N., Symmons, S. M., et al. (2020). Carrying out rapid qualitative research during a pandemic: emerging lessons from COVID-19. Qual. Health Res. 30, 2192–2204. doi: 10.1177/1049732320951526
Wigert, H., Dellenmark, M. B., and Bry, K. (2013). Strengths and weaknesses of parent-staff communication in the NICU: a survey assessment. BMC Pediatr. 13, 71. doi: 10.1186/1471-2431-13-71
Wigert, H., Dellenmark, M. B., and Bry, K. (2014). Parents' experiences of communication with neonatal intensive-care unit staff: an interview study. BMC pediatr. 14, 1–8.
Wreesmann, W.J. W., Lorié, E. S., van Veenendaal, N. R., van Kempen, A. A. M. W., Ket, J. C. F., and Labrie, N. H. M. (2021). The functions of adequate communication in the neonatal care unit: a systematic review and meta-synthesis of qualitative research. Patient Educ. Couns. 104, 1505–1517. doi: 10.1016/j.pec.2020.11.029
Keywords: webcam-use, neonatal, NICU, health care provider, very low birth infants, parent-provider communication, tailored communication
Citation: Stümpel J, Dörrhöfer A, Mantell P, Jannes C, Reimer A and Woopen C (2023) Webcam-use in the NICU-setting from the perspective of Health Care Professionals and its implication for communication with parents. Front. Commun. 8:1205950. doi: 10.3389/fcomm.2023.1205950
Received: 14 April 2023; Accepted: 21 June 2023;
Published: 06 July 2023.
Edited by:
Sylvie Grosjean, University of Ottawa, CanadaReviewed by:
Geneviève Rouleau, Université du Québec Outaouais, CanadaCopyright © 2023 Stümpel, Dörrhöfer, Mantell, Jannes, Reimer and Woopen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Johanne Stümpel, am9oYW5uZS5zdHVlbXBlbEB1bmktYm9ubi5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.