 Michael Takudzwa Pasara
Michael Takudzwa Pasara
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Commun., 20 September 2022
Sec. Culture and Communication
Volume 7 - 2022 | https://doi.org/10.3389/fcomm.2022.935097
This article is part of the Research TopicTowards 2030: Sustainable Development Goal 4: Quality Education: A Communication PerspectiveView all 5 articles
Several factors including droughts, cyclones, COVID-19, and inconsistent economic policies contributed to the challenges faced by children and persons with disabilities (PwDs) in rural areas of Zimbabwe. Consequently, there was a higher risk of low quality of life, poverty, and limited access to basic services such as education and healthcare. Various community-based rehabilitation (CBR) programs were implemented to address the violation of rights and access to services and participation by PwDs in general. This study used a mixed method approach to analyze the impact of CBR programs taking into account the five themes of the United Nations Convention of Rights of Persons with Disabilities (UN-CRPD): education, health, livelihoods, social protection, and participation. Respondents included core beneficiaries, caregivers, teachers, community health workers, and other key stakeholders. Results indicated that 61% were female respondents and 39% were males. Approximately 84% of rural families survive on less than USD 20.00 per month with the modal household having 5 to 9 members per household. Approximately 81% have received at least secondary education although some did not complete Ordinary Level mostly due to lack of funding for registration fees at the time of writing. However, none had tertiary education. The reach of CBR was as high as 92% of respondents received training on disability management; 71% on income generating projects (IGPs) and 84% on Internal Savings and Lending (ISAL) although only 32% received funding. The study recommends funding for self-help groups, increased technical support, functional disability-friendly toilets, and orthopedic centers, scaling up of programs at a national level and adoption by the relevant agencies, decentralization by government officials to reduce red tape and accelerate programs, and training of trainers for additional capacity building. Improved latitude for NGOs and consistent economic policies are also needed to sustain IGPs.
Zimbabwe has been ravaged by a myriad of challenges, including a series of droughts, floods, cyclones, and an unstable economic environment largely acerbated by inconsistent economic policies from the central bank. The effect is that the majority of rural households are prone to hunger, malnutrition, and disease outbreaks due to their vulnerability status. The situation is worse in the case of children and persons with disabilities (C_PwDs). Compounding these challenges, there has been an increase in cases of violation of the right to access services and participation by PwDs in general. This led to “implicit social acceptance of violation of rights of people with disabilities (PwDs) in the rural communities and widespread reluctance to address the issue”. There was a higher risk of low quality of life, poverty, limited or no access to healthcare, education, employment, and other economic and social opportunities compared to those without disabilities. These have had a negative impact on their quality of life and social capital and they have not participated in the mainstream community like those without disabilities.
Consequently, local non-governmental organizations have been implementing various community based rehabilitation (CBR) programs to address the violation of the right to access services and participation by PwDs in general. Specifically, the CBR project aimed at strengthening and extending rehabilitation, assistive technology, assistance and support services, and CBR in the least restrictive environments, that is, within the client's home environment. CBR activities are designed to enhance human welfare especially those with disabilities by enabling access to basic needs such as education, healthcare, livelihoods, and other social opportunities. These activities not only reduce poverty but also support the mandate of CRPD (International Disability and Development Consortium (IDDC), 2012). Disability is recognized as a national public health issue, a human rights issue, and a development priority (World Health Organization, 2005, 2015; Grandisson et al., 2017).
This study analyzes the impact and effectiveness of the CBR projects implemented across the three provinces of Mashonaland East, Masvingo and Matabeleland in Mudzi, and Bikita and Insiza district, respectively over the period 2017–2021. The project cuts across all the domains as expressed by the 2010 guidelines of the World Health Organization (WHO) and is also complementary to the Sustainable Development Goals (SDGs) (2015). In terms of operational context at the national level, Zimbabwe boasts the Disabled Act of 1992 (revised 1996) for the better part of project implementation, and is a signatory (2013) to the undomesticated United Nations Convention on Rights of Persons with Disabilities (UN-CRPD) thereby falling short of fully recognizing the diversity and challenges of persons with disabilities. The CRPD is anchored on five domains namely: education, health, livelihoods, social protection, and participation (Article 24–30). Similarly, the life-domains are also comprised of the CBR Matrix of Guidelines (World Health Organization, 2010).
The main activities underpinned by these approaches are as follows: universal health coverage, a human-rights-based approach, which includes empowering PwDs, a continuum of care as a life-course approach, a culturally-appropriate person-centered approach, multisector community-based rehabilitation, and universal design (World Health Organization, 2015) included but not limited to community mobilization, advocacy, capacity development, raising disability awareness, community education, information dissemination, therapeutic intervention, provision of aids and appliances, sexual and reproductive health rights and disability sensitization/awareness, school placement and support, and livelihoods loans and grants assistance and training.
The project areas are Mudzi district in the north-eastern part of Zimbabwe, Bikita district in the south, and Insiza district in the southwestern part. The common characteristic among these three operational areas is that they are drought-prone areas. They are all in the farming region 4/5 which implies that the most ideal farming activity is cattle ranching. However, due to high population densities and low seed capital, cattle farming has been largely at a subsistent level with most families not even owning small livestock like poultry and goats. As shall be noted in the subsequent chapters, these areas experienced several episodes of drought and cyclones during the project period. In addition to these generic challenges, Mudzi district borders Mozambique and has several places that are high risk due to landmines planted during the liberation struggle. Consequently, some of the disabilities in the area are as a result of uncontrolled landmines exploding.
The identified problems and their causes were summarized as a lack of prioritization of disability issues, poverty, inadequate knowledge of disability issues, negative social attitudes toward PwDs, limited support by regulatory frameworks, myths and misconceptions, social mythology and social capital, and low literacy levels among PwDs. Thus, the two broad project objectives were first, to improve the quality of life of people with disabilities in Masvingo, Matabeleland South, and Mashonaland East through access to healthcare, education, livelihood, and social participation and empowerment services. Second, the right to access services and participate in community development programs and decision-making systems/structures by PwDs in Masvingo, Mashonaland East, and Matebeleland South is realized. In terms of scope, the areas covered were Mudzi district, Mashonaland East province; Bikita district, Masvingo province; and Insiza district, Matebeleland South province. The five thematic areas of focus under this study are education, health, livelihood, social protection and participation.
Tofani et al. (2021) posit that community-based rehabilitation (CBR), also known as community-based inclusive development (CBID), is a multi-sectorial community strategy that fosters an environment where PwDs enjoy similar rights and opportunities as those without disabilities. The main five-component matrix is as follows: education, health, livelihoods, social participation, and empowerment. The World Health Organization (WHO) employs various CBR strategies as instruments for poverty reduction, equity, and social inclusion for PwDs. The WHO 2014–2021 Action plan calls for member countries to do the following: (a) remove barriers and improve access, (b) strengthen and extend rehabilitation, and (c) promote the collection of relevant and internationally comparable data (World Health Organization, 2015).
A significant body of literature emphasizes the significance of monitoring and evaluation of CBR programs (Hartley et al., 2009; Grandisson et al., 2014, 2017; Madden et al., 2015; Weber et al., 2016). Other studies focus more on rigorous evaluation of content and methods whilst another body places weight on impact (Rule, 2013; Raj and Thomas, 2015; Terwee et al., 2018; Shumba et al., 2020). However, Jansen-van Vuuren and Aldersey (2019) posited that the diversity and complexity of CBR pose various challenges in monitoring and evaluation such as cost, limited time, and capacity. Consequently, multiple methodological approaches are implemented. It, however, remains critical that persons with disabilities (PwDs) are involved in the evaluation process to ensure effectiveness (M'kumbuzi and Myezwa, 2016; Grandisson et al., 2017).
Despite the wide acknowledgment of the inclusion of PwDs in the development and delivery of training, details remain scant as to actual implementation (Gilmore et al., 2017). Both supply and demand of personnel should be matched. In other words, PwDs and their respective communities should identify training needs of CBR workers which will meet their needs. Active involvement of PwDs in the process fosters ownership, which in turn stimulates empowerment, commitment, and sustainability (Kuper and Phyllis, 2019; Pagiione et al., 2020). Complementary to this, there is also literature which highlights the gains a bottom-up approach and local trainers can produce (van Pletzen et al., 2014; Lewis Gargett et al., 2016). This ensures that CBR workers not only gain relevant skills but are also acceptable within the community. lezzoni (2009) and Rule (2013) denotes denotes that CBR training should be in an environment that promotes respect for PwDs.
Jansen-van Vuuren and Aldersey (2019) observed that CBR workers require a broad range of skills because they are diverse. These areas include but are not limited to clinical, management, social, communication, and cultural competence skills across the CBR Matrix spectrum. More specifically, there is a need to facilitate community development and empower persons with disabilities (PwDs). The study stressed the importance of mid-level workers who are usually key to effective implementation of CBR guidelines. The study concluded by highlighting the need for standardized training approaches for CBR workers to ensure meaningful comparison and evaluation across various contexts. Similar sentiments were earlier shared by Lewis Lewis Gargett et al. (2016) in their analysis of identifying a rehabilitation workforce on disability and inclusive development in the Pacific Islands.
The investigation for Italy by Tofani et al. (2021) showed that focusing on social inclusion in the labor market was lacking. Some of the identified constraints leading to this outcome included attitude, health-related matters, unemployment, and financial constraints. However, there were also reflections in the results that higher levels of physical activities or recreation were associated with better quality of life (Vanner et al., 2008). In terms of empowerment, results indicated that PwDs do not have sufficient independence to make big decisions or influence their communities. What was encouraging was that in terms of livelihoods, PwDs depended more on their income and a majority of them had obtained higher education, had a skill, and had received either formal or informal training. This is in line with other existing literature (Hästbacka et al., 2016; Lamichhane et al., 2021; Monticone et al., 2021). Thus, despite Italy being a developed nation, there are still strong indications which point to the evidence that strong differences still exist between PwDs and those without. The variances can be presumed to be notably higher in developing countries.
Support and leadership from the government is also significant to the provision of the necessary credibility and sustainability to CBR programs (Lehmann and Crimando, 2008; Lamichhane, 2013; Lewis Gargett et al., 2016; M'kumbuzi and Myezwa, 2016). This is because governments have leverage in that they develop, coordinate, and implement social welfare policies as well as provide resources (M'kumbuzi and Myezwa, 2016). In addition, governments provide a legal framework that not only guides CBR operations but also protects the rights of PwDs. Thus, politics will remain a crucial factor in CBR projects as much as it is important in other macro issues.
CBR projects were also negatively affected by the COVID-19 pandemic due to disrupted value chains and restricted movements of both goods and people. As a result, service providers such as health workers were unable to access PwDs, and neither were the intended beneficiaries able to access health institutions (Garidzirai, 2020; Pasara, 2020; Khamis et al., 2021). In their study which focused on rehabilitation systems design in a COVID-19 pandemic context, Akbari et al. (2021) proposed that home-based rehabilitation devices can be sustainable solutions in crises such as the pandemic. This is because accessing and utilizing state-of-the-art technologies became challenging due to various COVID-related challenges.
In Ethiopia, Asher et al. (2021) employed a mixed methods approach in a pilot study for people with schizophrenia. The study was aimed at exploring factors that influence competence. Results indicated that improving the competence of CBR workers through training led to notable improvements throughout the 12-month period of the pilot study. Competence factors included elements such as empathy, ability to assess social networks, and substance use. The training was multimodal in nature and it consisted of role-playing, group interactions, and fieldwork and this significantly contributed to the development of competence. However, the authors noted the need for specialist supervision.
Whilst the reviewed literature may not be exhaustive, what it reveals is that there is a need for several stakeholders to be actively involved in developing, implementing, monitoring, and evaluating the success of CBR projects. These stakeholders include but are not limited to government agencies and relevant arms, health workers, and coordinators among others. More importantly, the CBR process must ensure the participation of PwDs at all stages to ensure that there is relevancy, ownership, and sustainability. In the past, most CBR projects were crafted without the participation of the PwDs as intended beneficiaries and this has resulted in less than optimal impact. Although these traits are still present in some cases, the general trend is witnessing an improvement in inclusiveness at all stages of the CBR program.
A mixed method approach was employed to draw information from both existing literature (such as baseline reports and monitoring frameworks) and new qualitative and quantitative data in answering evaluation questions and meeting evaluation objectives. This included an assessment of project interventions by giving due consideration to the needs and capacities of various target groups and stakeholders.
The project activities upon which the methodology will be anchored are as follows: community mobilization, advocacy, capacity development, raising disability awareness, community education, information dissemination, therapeutic intervention, provision of aids and appliances, sexual and reproductive health rights and disability sensitization/awareness, school placement and livelihoods loans and grants assistance and training. Lastly, the approach used in the survey was based on the benchmarks as defined by the Organization for Economic Cooperation and Development Assistance Committee (OECD DAC) criteria which attempts to answer key evaluation questions relating to relevance, effectiveness, impact, sustainability, and coherence:
Although the community based rehabilitation (CBR) project was implemented in three provinces, the survey for this study was conducted in two of the three provinces. This represents 67% of the coverage. The areas covered were Masvingo and Mashonaland East province.
Stratification of the sample was done based on the five thematic areas listed below. Each component targeted a certain audience and samples were drawn from these audiences.
• Education—mainly school children, schools as service institutions, and parents. There were also school disability clubs as pressure (self-representing) groups. The three main instruments were access through fees payment, access through built-in infrastructure, and capacitation of children.
• Livelihoods—this component mainly targeted households with PwDs, identified poor children with disabilities and also identified about 5% of households with extreme poverty as a contributing element. This component also worked with Agritex Officers, Veterinary services for livestock, Chiefs, and Councilors as key stakeholders.
• Health—targeted PwDs with rehabilitation services and also outsourced rehabilitation services from local clinics. Also targeted PwDs with access to medical services and goods, ensuring that they could afford medical services and transportation.
• Social—targeted community at large with a bias toward PwDs with regards to participation in social development programs and sexual reproductive health and rights, social integration such as marriages, etc.
• Empowerment—rights awareness, rights insurance, and rights protection. Targeted PwDs, community leaders, and ward inclusive committees as custodians of power.
In terms of research tools, the consultant used a triangulation approach of structured questionnaires, focus group discussions (FGDs), and key informant interviews (KIIs). Questionnaires were distributed and interviews were conducted with the various target groups for relevance, thus targeting was purposive in order to get detailed information about the project.
(i) Structured questionnaires
Four sets of questionnaires were developed and tailored to the various target groups to ensure the relevance of responses and also for comparison over time (with baseline) and across provinces. The various questionnaires were designed and distributed to core beneficiaries, caregivers teachers and community health workers (CHW), community members, and provincial and district coordinators.1
(ii) Interviews
Interviews were also conducted to complement questionnaires by extracting information from various stakeholders including core beneficiaries, caregivers, and local authorities. Interviews were also effective as they give more room to respondents to express themselves in their own language, structure, and words and they provided first-hand testimonials.
(iii) Focus group Discussions (FGDs)
FGDs also provided a complementary role in buttressing information from the individual respondents especially where group dynamics are involved, for instance, garden beneficiaries. FGDs also enhanced the level of trust between the researcher and the respondents and assists in providing a sense of ownership to the process.
(iv) Record Inspection and Site Visits
The evaluation team inspected program documents and also visited some project sites and beneficiaries to observe/witness the changes which took place. This was mainly to verify the project results.
Quantitative, qualitative data, infographic, and video graphic information were collected from the two main groups, that is, direct and indirect groups. These included:
(a) Children/Persons with Disabilities (C_PwDs)
(b) Core beneficiaries
(c) Caregivers
(d) Teachers/Educators
(e) Duty Bearers/Local leaders
(f) Provincial Coordinators
(g) District Coordinators
(h) Community Health/Rehabilitation Workers (CRWs)
(i) Field Staff
(j) Ward Councilors
(k) Ward Inclusive Committee (WIC) members
(l) Community members
(v) Data capturing and analysis
The consultant used the Census and Survey Processing System (CSPro) software for quantitative data capturing and analysis whilst recording devices were used for qualitative data on interviews2. The data collected was then consolidated, cleaned, analyzed, and results interpreted. Transcriptions and analysis were done for qualitative data. Conclusions were drawn and policy recommendations were made.
This section presents the results from the surveys and interviews which were conducted in two of the three (67%) wards of the operational areas, that is, Mudzi and Bikita district. The results reflect the respondents answers to (i) questionnaires, (ii) interviews, and (iii) focus group discussions (FGDs). Several indicators were captured to reflect on the cross-sectional picture of various aspects which include demographics; and core thematic areas (education, health, livelihoods, social, empowerment).
Table 1 above indicates that 61% were female respondents and 39% were males. Quite revealing inference was the fact that there were more males (55%) than females (45%) for those over 60 years indicating that males become more forthcoming on health and disability related issues as they age or become more dependent. The modal age ranges are 40 to 59 years. Survey results also indicate that the majority (65%) are breadwinners, only (29%) respondents were either orphans or widows, but 94% of the respondents were either PwDs or had a family member with a disability. The forms of disabilities include blindness or visual impairment, deformed leg(s) and hand(s), walking difficulty, missing body parts (fingers, cut veins/arteries), deaf or hearing impairment, fits, weak body (no strength), cerebral palsy, mental disability, amputated leg, short and long leg (leg discrepancy), urinary outlet blocked, stammering, and stroke.
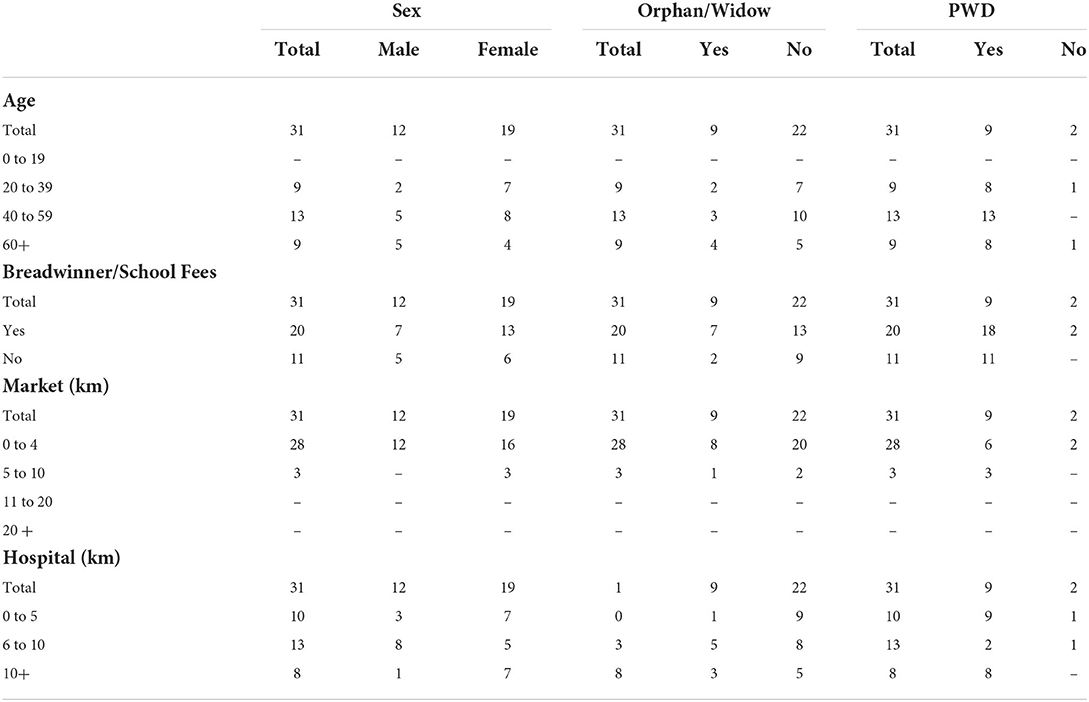
Table 1. Age, breadwinner/school fees, market (km), hospital (km) by sex, Orphan/Widow, PWD.
Results also indicate that markets are relatively closer with majority of them being found within 4 km whilst health facilities are further away with the average distance ranging between 6 and 10 km, while a significant number also travel above 10 km just to access a health facility. Thus, the services provided especially home visits and teaching PwDs become quite critical in improving the quality of lives of PwDs in the short to medium term.
Results in Table 2 below indicates that most, if not all, families live below the poverty datum line given that most families survive on monthly incomes of less than USD 20.00 per month. The dynamics become even more complex when considering the average number of family members of which the modal value is five to nine members per household. This generally translates to less than a dollar per person per day. This poverty status then explains why most households require supplementary support in both cash and kind in order to stimulate their lives and lifestyles out of poverty in line with the SDG agenda of “leave no one behind”.
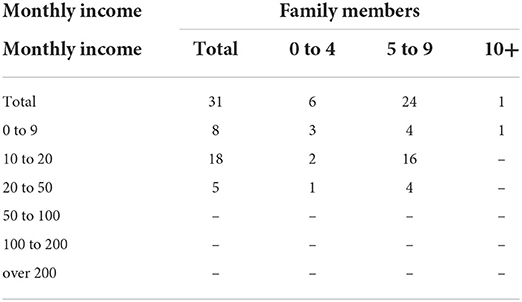
Table 2. Monthly income by family members.
In total, 81% of the respondents received, at least, secondary education although some did not complete Ordinary Level (the basic) while 19% received primary education as shown in Table 3. These results complement the national statistics, which indicate that Zimbabwe boasts one of the highest literacy levels in Africa which is around 94%.

Table 3. Sex by highest level of education and disability Mgmt training.
The results in Table 3 also indicate that 100% of male respondents and 84.2% of female respondents received training on disability management. A closer analysis indicated that for those who did not receive training, the reason was that they joined the CBA program in the latter phases of the program, that is, in 2020 and 2021, since new beneficiaries join on a continued basis as cases are coming to light. The project funded five school disability clubs from,
(a) Mamutse Primary School, Bikita,
(b) Bikita Secondary School, Bikita,
(c) Nyamapanda Primary School, Mudzi,
(d) Ngarwe Primary School, Mudzi.
Three (3) teachers and one (1) Deputy Headmaster from the following schools participated in the End of Term Survey from Nyamapanda, Ngarwe and Mamutse. Job descriptions included supervision, management, teaching in early child development (ECD), and special education. In Nyamapanda, there is one teacher with a degree in Special Education. These teachers work with various CWDs which include,
(i) Albinism
(ii) Speech difficulties
(iii) Hearing impairments
(iv) Speech impairments
(v) Walking difficulties.
Although all the schools now have disability-friendly infrastructures such as Disability Resource Units (DRU), disability-friendly toilets, and ramps, as reflected in Table 4, the respondents indicated that they are still in need of other assistive devices such as wheelchairs, hearing aids, pavements for wheelchairs, and solar-powered boreholes due to low water tables.
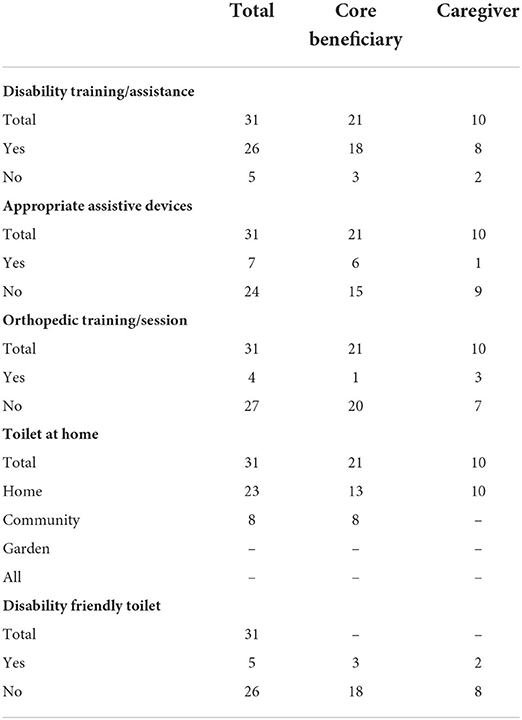
Table 4. Disability training/assistance, appropriate assistive devices, orthopedic training/session, toilet at home, disability-friendly toilet by category.
The willingness of families and communities to cooperate with schools with regards to CWDs was perceived as mixed at best, with some parents being more forthcoming while others still need more awareness and mobilization on disability programs. The former group assisted with the construction of infrastructure with labor while NGOs funded the purchase of materials. They also carry their children to school. Overall, the teachers indicated that there has been a significant positive behavioral shift among both children without disabilities and parents due to the various interventions. In the past, there were incidences such as name-calling among others. In terms of empowerment, there are 26 members (13G + 13B + 2M + 2W) in the School Disability Committees (SDC) in all schools highlighted above. These SDCs indicated that they are already implementing some of the knowledge they gathered by addressing issues concerning or raised by CwDs.
In terms of training on IGPs and ISALs, SRHR, gender-related issues, recreational activities, psycho-social health, justice for CwDs, and disability management as reflected in Table 5 above, all except one indicated having received it. This is because he was recently appointed at the school when the project had already unfolded. Some schools are running poultry projects funded by the school whilst others are not. Teachers also conduct counseling sessions with children and, in some cases, with a local Community Health Worker (CHW).
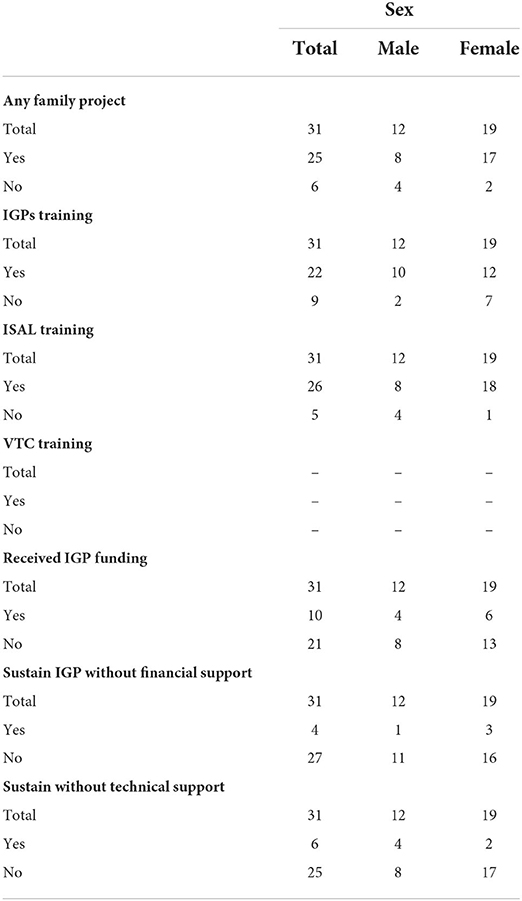
Table 5. Any family project, IGPs training, ISAL training, VTC training, received funding on IGPs, sustain IGP without finances, technical support by sex.
The main challenges were those which were COVID-19 related which affected school attendance of CwDs and also their frequency of receiving health services, PPE, and medication as movements were restricted. Another challenge was the lack of finances to improve infrastructure for CwDs and also borehole drilling. In the case of Nyamapanda, citing was already done but the school lacked the funds to finish the process. Some learners also need wheelchairs.
Of the respondents, 32% were caregivers whilst 68% were core beneficiaries. There were also three teachers and one Headmaster and interview respondents whose results were captured separately. Results also indicate that 84% of the respondents received training on disability management while 16% did not because they joined in the latter phases of the program. However, only 13% indicated that they received orthopedic training or sessions. This is because the Orthopedic center is only in Mudzi and there is none in Bikita. Although 74% indicated that they have toilets at home, only 16% indicated that they were disability friendly which reflects a significant gap. Respondents highlighted that although they were now aware of the need for disability-friendly toilets, they lacked the resources to construct them. However, members are taking an active role in assisting each other and one household already received assistance in constructing its toilet.
In terms of capacity building, majority of respondents indicated that they received training on IGPs, ISALs and vocational work as reflected by the data in the table above. Knowledge on concepts was tested during the survey and feedback was satisfactory. Projects include,
(i) Poultry (broilers, turkeys and other traditional varieties),
(ii) Piggery,
(iii) Goats,
(iv) Gardening.
Respondents indicated that some of the benefits accrued from IGPs include but are not limited to school fees, grinding mills, groceries, medical bills, transport, building their houses or expanding their fowl runs and kraals, nutritional supplements, and improved esteem and social status. However, only a number of them are implementing these ideas due to limited funding. Data confirms these sentiments showing that only 32% received funding on IGPs. In addition, respondents also indicated that whilst they are appreciative of the support they received, they are still in need of additional financial and technical support due to a variety of reasons. Some indicated that their IGPs suffered from the Newcastle disease and heat waves which killed their livestock. Others indicated that the solar powered borehole in the nutrition garden (especially in Bikita) was not pumping enough water and more drilling was required.
All (100%) respondents indicated that they received training on sexual reproductive health rights (SRHR), psycho-social health, gender-related issues, and disability rights. A significant but relatively lower percentage also received training or awareness of justice for children and persons with disabilities. This knowledge was applied in various circumstances with the major ones being (i) caregiving and (ii) advocacy for C_PwDs. However, some gaps still exist in terms of recreational activities as more than half of the respondents indicated that they are not participating in any. There were also efforts to stimulate recreational activities such as soccer, netball, poems, and galas but they happen momentarily and do not sustain their momentum.
In terms of empowerment, the results in Table 6 above also indicate there was 100% participation in a Self-Help or Disability Group. The results also indicate that these respondents joined these groups at various phases (years) throughout the project life cycle. In terms of growth of membership, 5(16%) joined in 2017, 19% joined in 2018, and another 19% in the following year while 42% joined in 2020. This indicates that awareness, acceptance, and momentum were increasing as the project unfolded, a significant indicator of progress and sustainability. Results also indicated that 20 (65%) indicated that they had raised some advocacy issues in one way or the other as a result of increased knowledge and awareness. Some of the raised issues include
(i) Marital abuse,
(ii) Disability abuse like neglect or verbal abuse,
(iii) Rape,
(iv) Neglect of C_PwDs,
(v) Lack of representation in community and leadership structures.
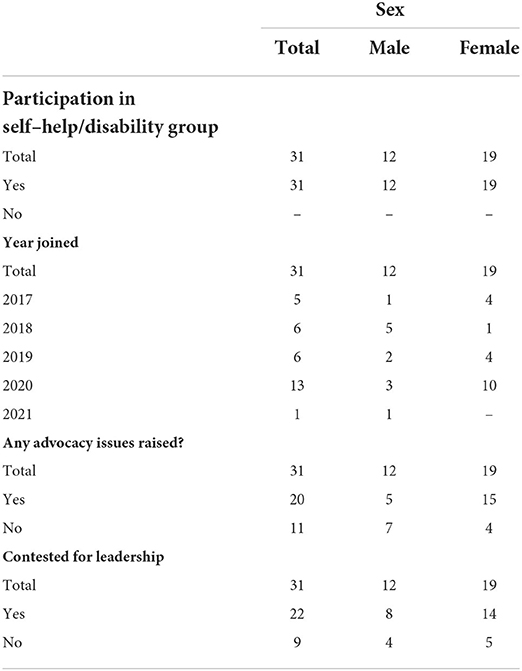
Table 6. Participation in self-help/disability group, year joined, advocacy, leadership by sex.
Moreover, 71% of the respondents indicated that they had either campaigned for or are currently holding a leadership position in local community structures. Some of the positions include village head, Church Bishops and Elders, secretaries of various portfolios from ward level, DCGs, gardens, and church. Moreover, some PwDs have indicated their strong intention to run for Councilor positions in the next local elections.
The general observation in this empowerment category has also been that, in terms of structure, most Disability Committee Groups (DCGs) are largely composed of females. This is perhaps because the local society is still largely patriarchal in nature and the majority of caregiving is done by females. To build on this, 100% of the respondents from the survey were female caregivers as highlighted earlier. However, one could also argue that strong gender awareness and movements have contributed to such representations. DCGs have also been encouraging other community members with CwDs so that they send their children to school instead of hiding them. As confirmed by the teachers, the enrollment, participation, and acceptance of C_PwDs have significantly increased. Those with disabilities now feel accepted and those without disabilities went through a significant behavioral transformation with issues such as “name calling” or stigmatization being a thing of the past. DCG members are continuously involved in the process of actively searching and identifying PwDs with needs and assist them in various ways such as advocating for their rights, assisting them with core duties such as cleaning their houses, farming for them, and helping them to build their houses among others. This led to a lot of acceptance of the CBR programs.
The project also produced some positive unanticipated results. There has been an increase in people with disabilities from adjacent wards coming to the office to seek assistance from service providers. This reflects that the level of awareness has spread outside the operational ward. Notably, some PwDs are beginning to establish their own IGPs without waiting for funds from the program. An interesting story in Bikita occurred in this regard. Disability Committee Members Ward 18 mobilized seed capital in the form of 31 chickens and assisted those in Ward 31 to start their own income-generating poultry project. Ward 31 is outside operational areas which were being serviced at the time of this study.
Neighboring wards are now also practicing disability inclusion and are in the process of forming their own committees to start their own CBID program. They have made several consultations with community leaders and officials in order to be guided on the process. The cash transfers from non-governmental organizations during the COVID-19 lockdown not only cushioned the lives of PwDs but also brought an unanticipated increase in visibility. In terms of gender balance, deliberate efforts were made to ensure equal participation of both men and women and boys and girls with disabilities or without. Recruitment also took into account gender and a balance was created in recruiting fieldworkers to ensure equal participation. The project is addressing gender disparities among PwDs through livelihood IGP activities where equal opportunities for participation for men and women with disabilities have been created. This has resulted in women having equal access to finances and improved decision making in the use of money at the household level. Women now hold leadership positions within community structures such as dip tank committees and disability-inclusive committees. In addition, assets have been a prerogative for men, but through advocacy noticeable changes have been noted on the part of women with disabilities owning household assets.
The project also raised awareness of the need for fathers and male caregivers to also be involved in the care of their children with disabilities as this area was being dominated by mothers/female caregivers. However, as reflected in the End of Term Evaluation results, all (100%) respondents who indicated that their caregivers were females. On a positive note, there has been a significant change in male involvement in disability issues in the project areas of operation as evidenced by the increased number of males participating in self-advocacy groups and training workshops. The target group was orientated to environmental and climate change issues during awareness and training platforms such as business management and community nutritional gardens. The business proposals developed by PwDs parents/caregivers and farming methods such as conservation agriculture (CA) like pfumvudza show that they are now aware of environmentally friendly practices.
Through the establishment of community structures such as Ward Inclusive Committees (WICs), Disability Committees, and School Disability Clubs (SDC), the project encouraged local ownership as these operate independently. The discriminatory practices of denying access to information on sexual reproductive health rights to men and women with disabilities have been challenged by the project. As a result of sexual reproductive health rights training, some women have begun claiming their rights to make decisions in relation to their sexual reproductive health lives. Furthermore, some are now getting married, and this has been evidenced by three marriages recorded in the Insiza district and four marriages in Mudzi district.
However, several challenges were also experienced and highlighted. More specifically, the project was implemented within a context of inconsistent economic policies which was characterized by incidences of hyperinflation in the earlier periods, especially 2017/18, and unavailability of basic commodities that resulted in hoarding. This led to Nostro accounts making and receiving foreign currency. The complexity was that a three-tier system for transactions now existed between bond notes, bank transfers, and foreign currency. NGOs faced challenges in accessing cash, which delayed the implementation of activities. The situation was then addressed by establishing a system of accessing cash in advance and also the opening of the Nostro accounts for better access to the USD.
The announcement of new Monetary Policy changes by the Finance Ministry and the Reserve Bank of Zimbabwe on the 24th of June 2019 promulgated Statutory Instrument 142 of 2019, which led to the abandonment of the multi-currency system. The instrument then implied that only RTGS dollars, which could be either in bond notes, coins, or electronic balances, became legal tender. Thus, according to the instrument, all other currencies US dollars, Botswana Pula, South African Rands, and British pounds were no longer legal tender in Zimbabwe. Gradually though, NGOs and Embassies were said to be exempted and some specific companies such as specific fuel companies were allowed to trade in foreign currency. Thus, the three-tier system also continued as goods could either be purchased in bond notes, bank transfers, or foreign currency which was mostly USD.
The change from the 1:1 between the USD and the Zimbabwean dollar resulted in shortages of cash and the organization like all other entities in the country were forced to change and fall in line with the legally presented financial systems. Though the organization was faced with challenges in changing to the legalized currency, it was generally not as difficult to access cash for activities. Though this may have affected the implementation of some activities which temporarily came to a halt as the organization, together with civil society, was trying to understand the implications of the new instrument. The frequent and constant power cuts have made it imperative to establish Standby Power Systems and/or Solar Installations as organizations and companies in the country. Rising price levels driven by hyperinflation have necessitated the need to buy in foreign currency which is more stable.
During the reporting period of 2019, the harsh economic environment made it more difficult for persons with disabilities to access goods and services as the cost of commodities and prices continued to escalate and inflation generally continued to deflate employee and customer disposable incomes thus eroding demand or buying power. Thus, because the chances and opportunities of persons with disabilities are already limited, their survival in this period is more challenging making them more vulnerable as they are at the mercy of society. However, through the project, persons with disabilities identified in the three CBID operational wards were supported with services and information making them less vulnerable. Activities such as payment of school fees and assessment by the school psychological services enabled children with disabilities to access educational opportunities like their able-bodied peers.
In 2019, several changes in the country's monetary policies during the reporting period resulted in breaks in project implementation as the organization tried to figure out the legal way of purchasing commodities. The unavailability of fuel and high cost of commodities resulted from companies or persons taking advantage of the changes in the monetary policies and ultimately project implementation. The project was able to purchase in USD after NGOs and embassies were given an exemption and this positively improved the project implementation as the foreign currency was available in the banks. On 21 August 2020, a key economic highlight was introduced which is still operational to date; the foreign exchange auction system. This auction system placed limits on electronic money transfers for international transactions as companies and organizations had to first seek approval through the central bank. Despite its rationale of intending to curtail inflation and externalization of foreign currency, the effect on ordinary citizens was increased shortages of basic goods and services. Thus, the gap between the official and black-market currency rates pushed prices further up. The story has been largely the same, stagflation (that is, a combination of both inflation and unemployment-twin devils).
Second, Zimbabwe was not spared from the effects of climate change which manifested itself in the form of droughts. The reporting period of the 2017/2018 cropping season did not yield many results due to the very low and erratic rains. Since the project beneficiaries are already located in drought-prone areas of farming regions 4/5, they had their already existing food challenges compounded. A similar narrative could be said of the 2018/19 season. However, the 2020/21 season had significantly higher yields. This was largely attributed to above average rains, the introduction of the pfumvudza conservation agriculture technique within the operational areas, and the introduction of nutritional gardens whose impact was becoming noticeable.
The country was hit by Cyclone Idai in March 2019 which affected Manicaland, Masvingo, Mashonaland Central and Mashonaland East provinces, the hardest hit being Manicaland Province. Cyclone Idai caused flooding, mudslides, and destruction of homes and 95% of road networks in the affected areas were damaged thereby limiting access. People lost their lives and livelihoods as houses and crops were destroyed. Subsequent experiences were heat waves in September to November 2019 which brought with it some diseases and pests, especially to Newcastle, and added to the challenges thereby affecting some poultry projects funded under the program. Rivers became dry in most parts resulting in shortages of safe drinking water and increased risks and incidences of water-borne diseases: three (2M, 1F) children with disabilities were hospitalized for severe malnutrition and unfortunately two of them (2M) passed on. The three operational areas under study were among the hardest hit, due to their historical dry weather patterns. Program activities such as workshop attendance were affected as people would opt to go to drought relief programs (hardware vs. software programming) and there was no proper coordination among NGOs to plan activities/events in a structured manner. It also became challenging to administer physiotherapy to children, school attendance also dropped as well as their overall welfare. Cyclone Chalane then followed in 2020 making it challenging to access the operational areas using the usual road networks. Thus, activities became costly due to increased needs for time and fuel. Crops were also hit by waterlogging.
Other challenges were compounded by the political environment. The 2017/18 period was characterized by tensions between the government and civil society due to a harsh economic environment (fuel shortages, stay-away strikes, and marches in some cases). In 2017/18 was also an election season which resulted in tension as results were disputed in the Constitutional Court. The government responded with a heavy military presence citing protection of property and curbing civil violence. These tensions posed difficulties to vulnerable people, especially PwDs, as efforts to fundraise and increase the resource base became challenging. Moreover, it was difficult to enable a holistic approach in meeting the operational needs of PwDs in the three operational wards in that environment. During that period, project activities had to be understandably reduced in order to manage the operational risk although this came at a huge developmental expense. In addition to that, project activities were also affected by the cholera outbreak in 2018 and gatherings of people were discouraged by health workers. However, NGOs operating within the area translated this challenge into a win by taking an active role in raising awareness of the cholera disease since PwDs were not spared from its effects. In 2019 was also characterized by food and fuel shortages thereby threatening the food security status of vulnerable groups. Thus, conflict between civil society and the government also continued.
In addition to already existing health challenges and disease outbreaks such as cholera, Newcastle (livestock), and malnutrition, the COVID-19 pandemic compounded the challenges especially for PwDs. Lockdown restrictions affected the whole value chain which implied that activities were either scaled down, stalled, or had to be stopped until it was safe to resume. Thus, implementation, monitoring, and evaluation of program activities were affected for obvious reasons. The lockdown also led to the total closure of schools and children were impacted heavily in terms of their progress in accessing appropriate quality education. There was pressure to conduct the remaining activities for the year despite the challenges of social distancing, sanitizing and limited numbers for workshops and or awareness raising activities. In 2020, the project was not able to conduct audiological assessments and purchase of hearing aids due to the lockdown challenges as there were many activities to be conducted at the end of the year.
PwDs are rehabilitated through the provision of medical rehabilitation services that include physiotherapy, occupational and speech therapy. These include conducting activities of daily living, functional training, and other mobility orientations which were significantly affected by the lockdown as workshops and activities had to be stopped. Therapy provision was also disrupted leading to PwDs failing to access therapy. For the activities that were conducted, the project took advantage of the time when lockdown restrictions were relaxed, and even though this mounted a lot of pressure on the project staff to catch up with the set deadlines for the year 2020.
The COVID-19 pandemic and induced lockdowns affected the attainment of the education component of the goal leading to changes being made in the CBID thematic areas. The national lockdown which resulted in school closures and regulatory measures such as wearing face masks and physical social distancing had a particularly negative impact on the project's primary target group who are persons with disabilities. The closure of schools resulted in other challenges arising, such as an increase in teenage pregnancies and increased exposure to different forms of abuse. Some learners with disabilities resorted to illegal artisanal mining which exposes them further to other forms of abuse such as child labor and sexually transmitted diseases (STDs). Illegal artisanal mining became the most feasible option for most households especially those who were not beneficiaries of the cash transfer programs when the COVID-induced lockdowns ensued. This posed more risk of abuse. Thus, it is recommended that the project supports more households with funding for the establishment of income-generating activities for sustainability. Thus, taking into account the well-known stylized fact that poverty and disability are intertwined, these challenges posed significant difficulties because they either stagnated or negated progress made among the core indicators.
In conclusion, the project was able to implement more than 93% of its planned project activities with most indicators being surpassed by a significant margin. The various success stories clearly reflected the depth and breadth with which this project has impacted people both with and without disabilities in the three operational areas. All the five themes reflected significantly positive outcomes irrespective of the constraining environment in which the project was being implemented. PwDs now feel empowered through their increased knowledge and awareness. There have also been significant behavioral changes and reduced cases of various forms of abuse as both caregivers and the community at large are now aware of the rights of C_PwDs.
School enrolment and completion also increased as well as the inclusion of disability-friendly infrastructures in the target schools within the operational areas. Cases that reflect empowered disabled persons were on the rise during the course of the project reflecting their ability to apply acquired knowledge on both rights of PwDs and disability management. This was done through various groups such as Ward Inclusive Committees (WICs) and Self-Advocacy Groups.
Livelihood projects were varied and impactful. Projects ranged from community nutritional gardens to poultry and piggery. Beneficiaries indicated various gains such as supplementary income for school fees, nutritional gains, and social integration, especially in gardens among others. Although a majority of them indicated that they received training on IGPs and ISALs, they also highlighted that they could still benefit if additional funding and technical training were to be provided as most of these projects were still at the subsistence level.
The positive response from the communities far outweighed the anticipated figures resulting in resources being constrained especially on the budget side. There were also other challenges that were exogenous in nature such as cyclones, droughts, and inconsistent economic policies. However, service providers had efficient risk and project management strategies that allowed them to adjust their operational plans without compromising the intended outcomes. Thus, the CBR project remained on a positive trajectory and was gaining momentum over time as reflected in the survey results by the increased number of PwDs who joined and benefited from the program as the years unfolded.
The evaluation recommends funding for self-help groups who, despite their willingness to assist PwDs within their communities, they are always constrained by a lack of resources. They work on a voluntary basis but are also between a frying pan and fire. On one hand, they have their own families to feed, whilst on the other hand, they need resources to help other PwDs with, for instance, money for transportation, soap, and basic food supplements. Technical support is still needed, not only Agritex Officers who are usually readily available at the community level but also from other technicians such as plumbers and electricians who can assist them in their community nutrition gardens.
Despite 74% of respondents indicating that they have a toilet at home, a paltry 16% indicated that these toilets were actually disability friendly. However, upon physical visits by the consultant, it was observed that an even lower percentage actually met the basic requirements of either a normal toilet or a disability-friendly toilet. The narrative was relatively different in schools since they received financial support from non-governmental organizations (NGOs). Thus, there is a greater need for disability-friendly toilets in homes. Most households are using improvised toilets which leave disabled persons very exposed.
Existing orthopedic centers need to be fully equipped in terms of both equipment and human resources for them to be fully functional. In other cases, there is actually a need to establish the orthopedic units at convenient locations. At present, the existing centers are not yet being fully utilized and there is a need to expedite the processes toward that end.
The community-based approach proved to be effective and yielded significant results in bringing behavioral changes toward PwDs. However, this approach also implies that the initial or sunk costs will be relatively high as coordinators or implementing partners need to be on the field and empowering both PwDs and their communities. Consequently, there is a reasonable need to expand to other wards or regions to increase the footprint and gain from the momentum and multiplier effects of the experiences of this project. In terms of scaling up the project, the evaluation also recommends “training of trainers” at the community and district levels. This will ensure that skills are not centralized as this usually slows up processes and reach given the two main challenges of red tape and also COVID-19 which was constraining movement. In general, decentralization is key in accelerating program activities, especially now that a successful pioneer project was implemented. In schools, there is also a need for additional training for capacity building in schools to increase the number of teachers who can work with CWDs who have special needs.
The evaluation also recommends Increased investment in awareness programs on the rights of C_PwDs through various channels such as newspapers, social media, and mobile applications. These tools can be combined with success stories from the already existing operational areas to make the matter more relatable, practical, and impactful. Recommendation for funding of additional drilling in Bikita and solar-powered boreholes in some schools is required due to low water tables. A series of droughts experienced during the implementation years of this program compounded already existing challenges. Thus, without additional drilling, the sustainability of the community nutritional garden project will be highly threatened. Thus, a multi-stakeholder approach will remain key in mobilizing resources in a sustainable manner.
Going forward, there is also a need to introduce home-schooling programs in the communities to bridge the education gap. The emergence of COVID-19 disadvantaged so many vulnerable children including CWDs. Moreover, some CWDs and caregivers are also dissuaded by long distances to school they have to either walk or accompany their children on a daily basis. Some travel in the range of seven to ten kilometers, which is way too long even for an able-bodied child. However, certain generic constraints still exist for successful home-schooling programs. For instance, homeschooling requires capacitated parents in terms of both intellect and resources such as smart devices.
Schools also need additional infrastructure especially pavements for wheelchairs and solar-powered boreholes in some cases for ease of water access. This will enhance the quality of life for both CWDs and those responsible for caregiving. Additional resources such as wheelchairs and hearing aids are also needed for both children and adults. There is also a need for additional training for capacity building in schools to increase the number of teachers who can work with CWDs who have special needs. The student/teacher ratio is generally high leaving little room for those with special needs. This then puts them in an even greater disadvantaged position, something which the program is aiming to achieve as one of the core thematic outcomes, that is, access to quality education or educational equality.
Additional technical and financial support is still needed as most of the existing projects are still at a subsistence level. These additional resources will allow for scaling up projects so that they not only survive but can actually expand and start creating employment within the rural communities. At present, Zimbabwe is faced with a more than 90% (debatable, of course) unemployment rate. Most of these employment and economic opportunities are concentrated in the urban centers leading to high rates of rural-urban migration thereby leaving the rural folk exposed and vulnerable. Scaling up projects will not only create employment opportunities but also give a sustainable solution for PwDs to meaningfully participate and contribute to the economic value chain at both local and national levels as they will be able to supply their produce to retailers.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by JJA. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
The author confirms being the sole contributor of this work and has approved it for publication.
Publication Funding by North-West University, South Africa.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^See Annex B for Questionnaires and Interview Questions.
2. ^See Annex C for attached docfile with captured quantitative responses.
Akbari, A., Haghverd, F., and Behbahani, S. (2021). Robotic home-based rehabilitation systems design: from a literature review to a conceptual framework for community-based remore therapy during COVID-19 pandemic. Front. Robot. AI 8, 612331. doi: 10.3389/frobt.2021.612331
Asher, L., Birhane, R., Teferra, S., Milkias, B., Worku, B., Habtamu, A., et al. (2021). Like a doctor, like a brother: Achieving competence amongst lay health workers delivering community-based rehabilitation for people with schizophrenia in Ethiopia. PLoS ONE 16, e0246158. doi: 10.1371/journal.pone.0246158
Garidzirai, R. (2020). Covid-19 and its economic impact on the South African Economy. Agricagrowth Agenda 17, 10–12. Available online at: https://hdl.handle.net/10520/ejc-afgrow_v1_i1_a1
Gilmore, B., MacLachlan, M., McVeigh, J., Chiedza, M., Stuart, C., Antony, D., et al. (2017). A study of human resource competencies required to implement community rehabilitation in less resourced settings. Hum. Resour. Health. 15, 70 doi: 10.1186/s12960-017-0240-1
Grandisson, M., Hébert, M., and Thibeault, R. (2014). A systematic review on how to conduct evaluations in community-based rehabilitation. Disabil. Rehabil. 36, 265–275. doi: 10.3109/09638288.2013.785602
Grandisson, M., Hébert, M., and Thibeault, R. (2017). Practice guidelines for program evaluation in community-based rehabilitation. Disabil. Rehabil. 39, 1243–1251. doi: 10.1080/09638288.2016.1189604
Hartley, S., Finkenflügel, H., Kuipers, P., and Thomas, M. (2009). Community-based rehabilitation: opportunity and challenge. Lancet 374, 1803–1804. doi: 10.1016/S0140-6736(09)62036-5
Hästbacka, E., Nygård, M., and Nyqvist, F. (2016). Obstacles et facilitateurs à la participation dans la société des personnes qui présentent une incapacité: vue d'ensemble des études portant sur la situation en Europe. Alter 10, 201–220. doi: 10.1016/j.alter.2016.02.002
International Disability and Development Consortium (IDDC) (2012). IDDC Policy Briefing on HIV & AIDS and Disability. IDDC HIV & AIDS and Disability Task Group. Available online at: https://www.iddcconsortium.net/wp-content/uploads/2019/11/2012-HIV-TG-IDDC-Policy-Briefing-on-HIV-AIDS-and-Disability.pdf (accessed April 25, 2022).
Jansen-van Vuuren, J. M., and Aldersey, H. M. (2019). Training needs of community-based rehabilitation workers for the effective implementation of CBR programmes. Disabil. CBR Inc. Dev. 29. doi: 10.5463/dcid.v29i3.742
Khamis, M., Prinz, D., Newhouse, D., Palacious-Lopez, A., Pape, U., and Weber, M. (2021). The Early Labour Market Impacts of COVID-19 in Developing Countries: Evidence from High Frequency Phone Surveys. Policy Research Working Paper 9510. World Bank Group. doi: 10.1596/1813-9450-9510
Kuper, H., and Phyllis, H. (2019). The Missing Billion Access to Health Services for 1 Billion People with Disabilities. London: London School of Hygiene and Tropical Medicine.
Lamichhane, B., Jayasekera, D., Jakes, R., Ray, W. Z., Leuthardt, E. C., and Hawasli, A. H. (2021). Functional disruptions of the brain in low back pain: a potential imaging biomarker of functional disability. Front. Neurol. 12:669076. doi: 10.3389/fneur.2021.669076
Lamichhane, K. (2013). Disability and barriers to education: evidence from Nepal. Scand. J. Disabil. Res. 15, 311–324. doi: 10.1080/15017419.2012.703969
Lehmann, I., and Crimando, W. (2008). Unintended consequences of state and federal antidiscrimination and family medical leave legislation on the employment rates of persons with disabilities. Rehabil. Couns. Bull. 51, 159–169. doi: 10.1177/0034355207312111
Lewis Gargett, A., Llewellyn, G., Short, S., and Kleinitz, P. (2016). Identifying rehabilitation workforce strengths, concerns and needs: a case study from the Pacific Islands. Disabil. CBR Inc. Dev. 27, 19–36. doi: 10.5463/dcid.v27i2.520
lezzoni, L. I. (2009). Public health goals for persons with disabilities: looking ahead to 2020. Disabil. Health J. 2, 111–115. doi: 10.1016/j.dhjo.2009.03.002
Madden, R. H., Lukersmith, S., Millington, M. J., Scarf, D. C., Fortune, N., Hartley, S., et al. (2015). Participatory monitoring of community-based rehabilitation and other disability inclusive development programmes: the development of a manual and menu. Disabil. CBR Inc. Dev. 26, 26–52. doi: 10.5463/dcid.v26i4.472
M'kumbuzi, V. R. P., and Myezwa, H. (2016). Conceptualisation of community-based rehabilitation in Southern Africa: a systematic review. South Afr. J. Physiother. 72, 1–8. doi: 10.4102/sajp.v72i1.301
Monticone, M., Galeoto, G., Berardi, A., and Tofani, M. (2021). “Psychometric properties of assessment tools,” in Measuring Spinal Cord Injury. (Berlin/Heidelberg: Springer International Publishing), 7–15. doi: 10.1007/978-3-030-68382-5_2
Pagiione, L., Bargagli, A. M., Agabiti, I. N., Calandrini, E., Salvatori, L. M., Marceca, M., et al. (2020). Urban health and inequalities in highly socially marginalised settings in Rome. Epidemiol. Prev. 44, 38–44. doi: 10.19191/ep20.5-6.s1.p038.072
Pasara, M. T. (2020). Covid-19: challenges and opportunities for Africa. Afr. Agenda 17, 4–8. Available online at: https://hdl.handle.net/10520/ejc-afgrow_v17_n3_a1
Raj, V. S., and Thomas, M. (2015). Effectiveness of training community-based rehabilitation workers on multiple disabilities: A pilot study. In. J. Health Allied Sci. 4, 259. Available online at: https://link.gale.com/apps/doc/A432164999/HRCA?u=anon~351aec6e&sid=googleScholar&xid=f8976edf
Rule, S. (2013). Training CBR personnel in South Africa to contribute to the empowerment of persons with disabilities. Disability CBR Incl. Develop. 24, 6–21. doi: 10.5463/dcid.v24i2.180
Shumba, T. W., Haufiku, D., and Mitonga, K. H. (2020). The evolution of community-based rehabilitation (CBR) programmes: a call for mixed evaluation methodologies. J. Health Res. 34, 505–514. doi: 10.1108/JHR-08-2019-0183
Terwee, C. B., Prinsen, C. A. C., Chiarotto, A., Westerman, M. J., Patrick, D. L., Alonso, J., et al. (2018). COSMIN methodology for evaluating the content validity of patient-reported outcome measures: a Delphi study. Qual. Life Res. 27, 1159–1170. doi: 10.1007/s11136-018-1829-0
Tofani, M., Esposito, G., Berardi, A., Galeoto, G., Iorio, S., and Marceca, M. (2021). Community-based rehabilitation indicators: validation and preliminary evidence for disability in Italy. Int. J. Environ. Res. Public Health 18, 11256. doi: 10.3390/ijerph182111256
van Pletzen, E., Zulliger, R., Moshabela, M., and Schneider, H. (2014). The size, characteristics and partnership networks of the health-related non-profit sector in three regions of South Africa: implications of changing primary health care policy for community-based care. Health Policy Plan. 29, 742–752. doi: 10.1093/heapol/czt058
Vanner, E. A., Block, P., Christodoulou, C. C., Horowitz, B. P., and Krupp, L. B. (2008). Pilot study exploring quality of life and barriers to leisure-time physical activity in persons with moderate to severe multiple sclerosis. Disabil. Health J. 1, 58–65. doi: 10.1016/j.dhjo.2007.11.001
Weber, J., Polack, S., and Hartley, S. (2016). An online survey on identification of evaluation capacity, needs and current practice of programme evaluation in community-based rehabilitation. Disabil. CBR Inc. Dev. 27, 5–18. doi: 10.5463/dcid.v27i2.565
World Health Organization (2005). Disability, Including Prevention, Management and Rehabilitation. Available at online: https://www.who.int/disabilities/WHA5823_resolution_en.pdf?ua−1 (accessed April 25, 2022).
World Health Organization (2010). Community Based Rehabilitation: CBR Guidelines. Towards Community Inclusive Development. World Health Organisation: WB 320. Available online at: https://www.who.int/publications/i/item/9789241548052 (accessed April 23, 2022).
World Health Organization (2015). WHO Global Disability Action Plan 2014–2021. Available at online: https://apps.who.int/iris/bitstream/handle/10665/199544/9789241509619_eng.pdf?sequence=1&isAllowed=y (accessed March 26, 2022).
Keywords: community based rehabilitation (CBR), sustainable development goals-SDGs, education, health, livelihoods, social protection and inclusive growth, Zimbabwe
Citation: Pasara MT (2022) Impact of community-based rehabilitation on attainment of sustainable development goals: The case of selected districts in Zimbabwe. Front. Commun. 7:935097. doi: 10.3389/fcomm.2022.935097
Received: 03 May 2022; Accepted: 17 August 2022;
Published: 20 September 2022.
Edited by:
Philippa Rappoport, Smithsonian Office of Educational Technology, United StatesReviewed by:
Kayi Ntinda, University of Eswatini, EswatiniCopyright © 2022 Pasara. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Michael Takudzwa Pasara, bWljaGFlbHBhc2FyYUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.