 Elena Rey Velasco
Elena Rey Velasco Hanne Sæderup Pedersen
Hanne Sæderup Pedersen Timothy Charles Skinner
Timothy Charles Skinner
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Commun. , 12 October 2022
Sec. Health Communication
Volume 7 - 2022 | https://doi.org/10.3389/fcomm.2022.1034427
Online platforms and smartphone applications that facilitate patient-provider communication are examples of how digital technologies support human interaction. Telehealth enables clinical encounters when physical consultations are not possible, and evidence confirms that face-to-face and remote healthcare encounters have comparable efficacy. Furthermore, research shows that patient-provider communication and relationship influence patient outcomes. However, we lack studies on what happens during these interactions, particularly in text-messages conversations, from a linguistic or behavioral perspective. Our research methods will evolve alongside our communication channels. Currently, there is an overall preference for qualitative methods in patient-provider communication research. Some authors argue that quantitative measures (clinical measurements, questionnaires) lack an understanding of the patients' experiences, whereas qualitative approaches (interviews, focus groups) provide the full picture. Others suggest their combination to interpret interactions thoroughly. As a result, it is often difficult for a communication researcher to choose between one or more approaches. We conducted a mini-review of qualitative approaches, such as corpus linguistics and conversation analysis, as well as quantitative approaches, such as analysis of variance and temporal pattern detection, for patient-provider communication analysis. Additionally, we distinguish relevant communicative features in synchronous or live interactions, such as video-calls, and asynchronous interactions, such as non-instant messaging. We further discuss these methods' potential for combination and their applications in digital communication research. We aim to guide researchers to choose a methodology for digital interaction studies. Our recommendations are based on these approaches' ability to answer a research question, and we suggest a mixed-methods approach in future digital communication research.
Information and communication technologies experience a steady rise since as they have proven to be an innovative, yet reliable, channel for human interaction (Rogers, 1986). These technologies provide new opportunities in our day to day life, and healthcare is a large field where they are constantly applied, particularly in terms of software applications (apps) (Mosa et al., 2012; Ventola, 2014), and instant messaging (Ezra et al., 2020; Nascimento et al., 2020). Furthermore, research has shown that telemedicine is a viable alternative to face-to-face consultations that is rapidly evolving in clinical interactions, particularly during the COVID-19 outbreak (Monaghesh and Hajizadeh, 2020). Today, both Healthcare Professionals (HCPs) and patients use digital communication on a regular basis. Telehealth facilitates clinical encounters when physical consultations are not possible, such as patients living in remote or rural areas (du Toit et al., 2019), and optimizes clinical appointments (Rienzo Renato, 2019). In addition, several studies have demonstrated a comparable efficacy when comparing face-to-face and remote encounters (Shigekawa et al., 2018), though these outcomes vary depending on the population, disease addressed, and methods used (Dellifraine and Dansky, 2008), as well as on their cost-effectiveness (Ekeland et al., 2010). Therefore, our research methodologies will evolve alongside these new communication channels. Patient-provider communication is an important component of clinical consultations that influences patient outcomes significantly (Street et al., 2009). Because of the dynamic nature of the interaction, each conversation is a one-of-a-kind result of its variables and how the parties construct the conversational sequence (Koudenburg et al., 2016). There is a preference for qualitative methods for analyzing content exchange during patient-provider communication, and how the interaction is organized sequentially (Finset, 2008). Some authors argue that quantitative measures (clinical measurements, questionnaires, or scales) lack an understanding of the patients' experiences, whereas qualitative approaches provide a full picture through more in-depth methods, such as interviews and focus group (Ngenye and Kreps, 2020). Inui and Carter started a debate about the optimal methodology for patient-provider interactions in 1982 after publishing their research on healthcare interaction analysis (IA) and its link with patient outcomes (Carter et al., 1982; Inui et al., 1982). Their investigations were inspired by the previous work on interactional processes in conversation by Bales (1950), Roter and Hall (1989), and Stiles and Putnam (1989). Patient IA can be combined with more traditional, qualitative methods to achieve a complete understanding of communication in a clinical setting that allows for improvement of patient outcomes (Mazzi, 2011; Vogl, 2017). Nevertheless, given the complexities of combining qualitative and quantitative methods, it is far from simple for a researcher to decide on the best methodology to investigate these interactions (Schegloff, 1993). To begin, it is important to distinguish between qualitative and quantitative methods, and determine their strengths and weaknesses. Figure 1 shows an overview of the framework presented on this paper.
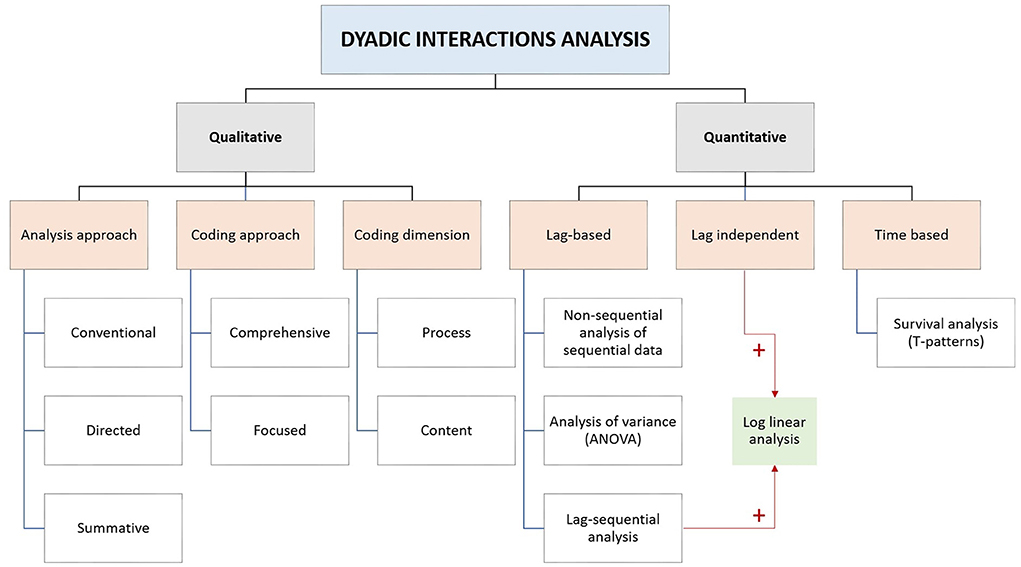
Figure 1. Schematic diagram of our dyadic interaction analysis framework.
Qualitative content analysis is the most used methodology in psycho-social research for analyzing human communication in a systematic and intersubjective manner (Mazzi, 2011). As described by Hsieh and Shannon, qualitative content methods can be grouped into three types according to the analytical approach: conventional if categories are generated during data analysis, directed if existing research is used to code the content, and summative if single words are individually screened for a pattern. The research objects should be both mutually exclusive and exhaustive (Hsieh and Shannon, 2005). Furthermore, Bell and Kravitz (2014) added two additional classifications in a patient-provider setting: first, the coding approach, which is considered comprehensive when every single unit of communication—or utterance—is classified or focused when only a particular communication element is coded e.g., a specific behavior; and second, the coding dimension, which can be process- or content-based. Processes describe abstract aspects of communication such as “asking for information”, whereas content is dependent on the topic of the conversation, such as medication. Other authors use the terms process theory, which studies a series of dependent variables or events that lead to an outcome, and variance theory, which focuses on the relationship between independent and dependent variables to explain changes in the communication system (Poole, 2007). For these qualitative content analysis purposes, some researchers have developed specific coding tools in the context of patient-provider communication research, such as MEDICODE (Richard and Lussier, 2006) and TORP (Taxonomy of Requests by Patients) (Kravitz et al., 1999).
Conversation analysis (CA) is a broadly used qualitative methodology based on a sociolinguistic approach to human interactions. CA's research object is how two identically constructed utterances can have a different meaning, depending on the actions that take place during the conversation, both verbal, such as telling or asking, and non-verbal, such as voice tone and facial gestures (Have, 2007). These actions reflect the speakers' behaviors and follow an order of turns, which forms the turn-taking structure. According to the conversational norm, each party speaks at a time (their turn), and all the parties co-construct and organize the sequence structure as the conversation moves forward. Their participation reflects their understanding and their reaction to the previous utterances. However, any of the speakers can deviate from the norm, for example, by interrupting or whispering to a speaker next to them (Hoey and Kendrick, 2017). CA has been successfully applied to several settings, such as classrooms, emergency calls, and clinical consultations (Symon and Cassell, 2012). There are two forms of CA: pure and applied (Chris, 2014). When we use a pure CA approach, we define the categories as the analysis takes place. According to Harvey Sacks and colleagues, this approach is a conventional qualitative analysis method (Sacks et al., 1974). Throughout the years, CA has become one of the most used methodologies for IA. The work of analysts in numerous conversations using CA over the years has facilitated the creation of standard categories. These categories correspond with pure CA, which includes the most found conversational structures in human interaction. Subsequently, applied CA has emerged as a qualitative analysis method where we use existing categories to code discipline-specific interactions. Additionally, it is possible to generate new categories during the analysis. Antaki (2011) differentiates six applied-CA categories: foundational, social-problem oriented, communicational, diagnostic, institutional, and interventionist. Out of these, the diagnostic, the institutional, and the interventionist CA are the most suitable to patient-provider communication analysis. Diagnostic-applied CA connects sequential speech features with clinical disorders, such as aphasia. Institutional CA observes the interaction development in society's institutions, e.g., a medical setting. Furthermore, interventionist-applied CA identifies communication issues during an interaction e.g., a clinical consultation. Such CA approaches provide a deeper understanding of context-associated challenges to advice on how to manage them.
The nature of the communication will determine the methods we choose: synchronic interactions, such as video calls, are similar to face-to-face interactions, and thus their analysis is similar. Text messages can have the form of either synchronous or asynchronous written communication, depending on whether they are sent back and forth instantly or after a delay. The receiver is not expected by the sender to respond immediately in asynchronous communication, and has time to review and answer the message (Walther and Burgoon, 1992). Applied CA is suitable for the analysis of digital written interactions. However, some of the written language features differ from the spoken language. First, these interactions are “persistent” in time: messages remain visible for the respondent while they construct a reply and can be used for textual quotation, although quotation is possible in spoken interactions as well (Giles et al., 2015). Second, oral interaction has three distinct elements: message repair, paralinguistic cues, and number of speakers. In written communication, the responder may edit their message before sending it. The receiver is not able to see these repairs, as they are an offline function. Likewise, the online speaker cannot display paralinguistic cues in a text setting, but they can imitate them through punctuation marks and emoticons (Herring and Androutsopoulos, 2015). Accordingly, the channel shapes the interaction. There are digital-specific features such as character limitations, links, GIFs, photos, #hashtags, and so on, that may include oral communications, e.g., videos and/or voice recordings (Arminen et al., 2016). The third difference between spoken and written language concerns conversation opening and turn adjacency (Meredith, 2017). Turns are adjacent when they are associated to each other. The speaker demonstrates their understanding of the prior turn in their current turn, what constitutes an adjacency pair. If this phenomenon does not take place, turn adjacency is disrupted and it might lead to miscommunication (Sacks et al., 1974). Herring raised this issue in a digital communication setting, particularly in interactions that involve more than two participants (Herring, 1999). Besides the variable number of participants in online conversations, these may be public or private. Forums and social networks are good examples considered by digital writing research (Lindemann et al., 2016), where digital CA has emerged as a form of applied CA (Reeves and Brown, 2016; Warren, 2018). To date, digital interactions research has primarily used standard qualitative methods, such as interviews and focus groups (Hefner et al., 2019), or intervention–relevant outcomes, such as weight loss (McVay et al., 2019) or pain (Seppen et al., 2020). Surveys and self-questionnaires are helpful to assess the behavioral effects, i.e., interaction and communication outcomes. However, these methods fail to analyse the actual communication processes that occur between the provider and the patient (Verhoeven et al., 2010; de Jong et al., 2014). Some authors have recently used CA in an asynchronous digital communication context, which may appear problematic given CA's innate synchrony. However, McHoul demonstrated that the sense-making processes and methods that take place while we read a text are comparable to those described by Sacks in spoken interactions (McHoul, 1982). A text follows a structure or “reading path” (Have, 1999) that the participants negotiate during an online, written discussion in a forum, a group, or a dyadic conversation (Gibson, 2009). Garcia and Baker Jacobs (1999) conducted the first analysis of written digital communication using CA in a “quasi-synchronous” setting, a group chat. They concluded that the nature of this quasi-synchronous turn-taking system is not better or worse, but “differently abled”. In addition, that, as we previously described, this system has different features from spoken language. For example, participants write their messages with no competition for the right to post a message, and the other way around. Conversation participants receive an unalterable message, although repair is possible in further messages for any of the speakers. Furthermore, Garcia and Jacobs predicted that chat and asynchronous messages would become more familiar in day-to-day interactions as we know them today. Likewise, some authors have applied CA to digital learning environments by classifying the utterances, e.g., long-answer, short-answer, and task-oriented questions, for utterance frequency and patterning recognition studies (Irani and Chalak, 2016). Others have explored the use of conversational features such as agreements, personal experiences, and stories, and cognition verbs in this asynchronous setting (Paulus et al., 2018). Virtanen and Kääntä combined digital CA (Giles et al., 2015) and written-dialogue methods from the Textual Interaction Studies (TIS) field. Their results illustrated the dynamics of asynchronous online interactions and proved the affinity of those two perspectives (Virtanen and Kääntä, 2018). The most recent research on the topic has investigated the linguistic and paralinguistic elements (Rendle-Short, 2015; Vázquez-Cano et al., 2015) and orthographic errors (Vázquez-Cano et al., 2019) in digital communication. Another area of study are the specific resources in instant messaging conversations, such as laughter and emoticons (Petitjean and Morel, 2017; König, 2019). However, little research has been conducted on asynchronous, digital patient-provider interactions.
There is a variety of quantitative methods to statistically associate qualitative categories and patient outcomes (Street et al., 2009), and to investigate whether these are influenced by specific factors such as gender (Schmid Mast et al., 2011; Shin et al., 2015), race (Mujica et al., 2020), or age (Gilbert and Hayes, 2009). Roter's Interaction Analysis System (RIAS) (Roter and Larson, 2001) is the most widely used. As we explained previously, the unit of analysis in IA is the frequency of utterances. RIAS defines specific categories for the doctors' and the patients' utterances, which coders register in a sequential order that includes time. The quantitative analysis of those categories includes percentages and doctor to patient ratios that contribute to the speakers' interaction profiling. However, there is no defined methodology for the exploration of these sequential records in a meaningful way, as stated by Roter and Larson (2002). Others authors have described sequential approaches for patient-provider conversation dynamics (Abbott, 1995; Zimmermann et al., 2007; Bensing and Verheul, 2009) and behavioral research IA (Mazzi, 2011). For example, the Relational Communication Control Coding System (RCCS) (Ericson and Rogers, 2004) codes utterances in pairs, with the second utterance categorized in relation to the preceding one. Additionally, the General Sequential Querier (GSEQ) software enables the identification of sequential patterns in the interaction coded by RCCS (Bakeman and Quera, 1995). Connor et al. (2009) conducted a critical review of existing methods for sequential analysis in dyadic interactions. These authors differentiate three analysis categories: lag-based, lag-independent, and time-based. A lag is an interval of time that precedes an utterance. There are three lag-based methodologies: non-sequential analyses of sequential data, for example, the proportion of utterances that respond to a specific process; analysis of variance (ANOVA), to compare utterances and detect changes in sequential processes; and lag-sequential analyses, that record the frequency between utterances and report statistically significant sequences. This last category is the largest in Connor et al.'s classification and can be combined with log linear analysis to draw a relationship between the lags and two or more categorical variables. A categorical variable has two or more values, and is either nominal or ordinal. For example, sex, educational level, or the groups in a randomized study (Allen et al., 2008). Lag-independent methods (for example, utterances- and turns-based) are also compatible with log linear analysis to find associations with categorical variables. These methods, however, do not consider time. If we are interested on this variable, common time-based methodologies apply what in statistics is called a survival analysis (Clark et al., 2003). This kind of analysis measures the time until an event occurs; in our context, an utterance. The timespan between utterances, known as (T-) pattern, is useful to predict the next utterance or to detect temporal patterns. For additional guidance, Allen et al. (2008) have developed a comprehensive manual for quantitative methods in communication.
This mini-review provides an overview of the methodologies that are applicable in digital health communication. The most extended approach in communication research, as we previously noted, is qualitative research, mostly because of its flexibility and adaptability. Qualitative methodologies are suitable for exploratory research on a subject that is largely un-investigated and/or calls for a human interpretation or generation of ideas (Denzin and Lincoln, 2017). This is often the case with communication research. For example, content analysis classifies the conversation themes, while quantitative approaches offer a numerical perspective of how communication unfolds. The latter facilitates the reproducibility and generalization of results, and can be used to develop a theory to explain how a phenomena occurs (Allen et al., 2008). For example, establishing the common behaviors that deal with anxiety in childhood. However, there are communication approaches that may use a qualitative and/or a quantitative approach. Similar to CA, corpus linguistics studies the meaning made through a sequence of words, although this approach is characterized by the analysis of a large language corpora (“body” in Latin). Corpus linguistics searches for lexical and grammatical patterns, such as frequency of words or sentences. This quantitative data may be interpreted qualitatively, for example, categorizing the topics or situations in which these patterns take place and why (Bennett, 2010). For these reasons, the choice between qualitative and quantitative methods is dependent on the research question that we try to answer. When the question is built upon the “how” it is convenient to rely on qualitative research (Britten, 2011). For example, “how is empathy expressed in text messages communication?” or “how do coaches build a relationship with their clients?”. Questions starting with “what” are common in quantitative studies (Allen et al., 2008), such as “what are the most common infections among pregnant women?” or “what is the relationship between TV time and child obesity?”. Nonetheless, “what” is also applicable to qualitative research questions such as “what opinions do European citizens share about refugees?”. Although they are inclined to use qualitative approaches to study communication, many communication researchers use statistical calculations. We can quantify qualitative data, for example, as the number of times that a behavior occurs, the frequency of emotions in percentages, or even the number of words. There are various approaches for this (Pope et al., 2000; Frericks, 2022). A digital setting such as text messaging facilitates the mixed-methods data collection and analysis. The use of correlations or relationships analyses can help us understand the mechanisms of communication-related elements. There is recent work that supports this statement about research in online communication. Yip performed a content analysis of types of social support in online groups for anxiety and depression, and subsequently applied CA to account for the sequential structure. He presented his results in tables showing the frequency and proportions of categories (Yip, 2020). Those results allowed him to draw conclusions about the individuals' emotions (qualitative) and to generalize how people with anxiety and/or depression use these online support groups (quantitative). Gieselmann and his team interviewed patients in an RCT for chat-based vs. face-to-face psychotherapy for insomnia (Gieselmann et al., 2021). They performed a content analysis of the interviews' transcripts and subsequent statistical difference analyses to allow for generalization of the treatment outcomes, i.e., sleep quality. Others have combined thematic analysis and quantitative language analysis methods such as keywords and collocation patterns (Lustig et al., 2021). Collocation is present in CA and corpus linguistic analyses, and studies word-combination units, where two or more words co-occur with a higher frequency than would be expected (Sinclair, 1991). Moreover, a recent mixed-methods systematic review conducted by Luo et al. (2021) on physical activity promotion via conversational agents (such as chatbots or virtual agents) showed the increasing need for mixed methods studies appraisal in future reviews. This highlights not only the increasing need for applying mixed methods in future research, for also for improving their understanding and systematic reviewing, in order to evaluate these type of studies.
ERV conducted the mini-review, synthesized the results, and prepared and edited the manuscript until submission. HP contributed to the data analysis and interpretation processes and participated in the manuscript reviewing process. TS conceived the research, supported the interpretation and discussion of results, and reviewed the final manuscript. All authors contributed to the article and approved the submitted version.
This research is part of an Industrial PhD project sponsored by Innovation Fund Denmark, the University of Copenhagen, and Liva Healthcare.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbott, A. (1995). Sequence analysis: new methods for old ideas. Ann. Rev. Sociol. 21, 93–113. doi: 10.1146/annurev.so.21.080195.000521
Allen, M., Titsworth, B. S., Hunt, S., and Allen, M. (2008). Quantitative Research in Communication. New York, NY: SAGE Publications, Incorporated. doi: 10.4135/9781452274881
Antaki, C. (2011). “Six kinds of applied conversation analysis,” in Applied Conversation Analysis: Intervention and Change in Institutional Talk, ed C. Antaki (London: Palgrave Macmillan UK), 1–14. doi: 10.1057/9780230316874
Arminen, I., Licoppe, C., and Spagnolli, A. (2016). Respecifying mediated interaction. Res. Lang. Soc. Interact. 49, 290–309. doi: 10.1080/08351813.2016.1234614
Bakeman, R., and Quera, V. (1995). Analyzing Interaction: Sequential Analysis with SDIS and GSEQ. New York, NY: Cambridge University Press.
Bales, R. F. (1950). A set of categories for the analysis of small group interaction. Am. Sociol. Rev. 15, 257–263. doi: 10.2307/2086790
Bell, R. A., and Kravitz, R. (2014). “Direct observation and coding of physician—patient interactions,” in Research Methods in Health Communication: Principles and Application (Milton Park: Taylor and Francis), 141–168.
Bennett, G. (2010). Using Corpora in the Language Learning Classroom: Corpus Linguistics for Teachers, Illustrated Edn. Ann Arbor: University of Michigan Press. doi: 10.3998/mpub.371534
Bensing, J., and Verheul, W. (2009). Towards a better understanding of the dynamics of patient provider interaction: the use of sequence analysis. Patient Educ. Counsel. 75, 145–146. doi: 10.1016/j.pec.2009.03.002
Britten, N. (2011). Qualitative research on health communication: what can it contribute? Patient Educ. Counsel. 82, 384–388. doi: 10.1016/j.pec.2010.12.021
Carter, W. B., Inui, T. S., Kukull, W. A., and Haigh, V. H. (1982). Outcome-based doctor-patient interaction analysis: II. Identifying effective provider and patient behavior. Med. Care 20, 550–566. doi: 10.1097/00005650-198206000-00002
Chris, J. (2014). “Conversation analysis,” in The Routledge Companion to English Studies, 1st Edn, eds C. Leung, and B. V. Street (New York, NY: Routledge).
Clark, T. G., Bradburn, M. J., Love, S. B., and Altman, D. G. (2003). Survival analysis part I: basic concepts and first analyses. Br. J. Cancer 89, 232–238. doi: 10.1038/sj.bjc.6601118
Connor, M., Fletcher, I., and Salmon, P. (2009). The analysis of verbal interaction sequences in dyadic clinical communication: a review of methods. Patient Educ. Counsel. 75, 169–177. doi: 10.1016/j.pec.2008.10.006
de Jong, C. C., Ros, W. J., and Schrijvers, G. (2014). The effects on health behavior and health outcomes of internet-based asynchronous communication between health providers and patients with a chronic condition: a systematic review. J. Med. Internet Res. 16, e19–e19. doi: 10.2196/jmir.3000
Dellifraine, J. L., and Dansky, K. H. (2008). Home-based telehealth: a review and meta-analysis. J. Telemed. Telecare 14, 62–66. doi: 10.1258/jtt.2007.070709
Denzin, N. K., and Lincoln, Y. S. (2017). The SAGE Handbook of Qualitative Research, 5th Edn. New York, NY: SAGE Publications.
du Toit, M., Malau-Aduli, B., Vangaveti, V., Sabesan, S., and Ray, R. A. (2019). Use of telehealth in the management of non-critical emergencies in rural or remote emergency departments: a systematic review. J. Telemed. Telecare 25, 3–16. doi: 10.1177/1357633X17734239
Ekeland, A. G., Bowes, A., and Flottorp, S. (2010). Effectiveness of telemedicine: a systematic review of reviews. Int. J. Med. Inform. 79, 736–771. doi: 10.1016/j.ijmedinf.2010.08.006
Ericson, P., and Rogers, L. (2004). New procedures for analyzing relational communication. Family Process 12, 245–267. doi: 10.1111/j.1545-5300.1973.00245.x
Ezra, O., Toren, A., Tadmor, O., and Katorza, E. (2020). Secure instant messaging application in prenatal care. J. Med. Syst. 44, 73. doi: 10.1007/s10916-020-01552-3
Finset, A. (2008). Qualitative methods in communication and patient education research. Patient Educ. Counsel. 73, 1–2. doi: 10.1016/j.pec.2008.08.004
Frericks, P. (2022). How to quantify qualitative characteristics of societal differences: a method for systematic comparison of qualitative data (SCQual). Int. J. Soc. Res. Methodol. 25, 311–322. doi: 10.1080/13645579.2021.1883537
Garcia, A. C., and Baker Jacobs, J. (1999). The eyes of the beholder: understanding the turn-taking system in quasi-synchronous computer-mediated communication. Res. Lang. Soc. Interact. 32, 337–367. doi: 10.1207/S15327973rls3204_2
Gibson, W. (2009). Negotiating textual talk: conversation analysis, pedagogy and the organisation of online asynchronous discourse. Br. Educ. Res. J. 35, 705–721. doi: 10.1080/01411920802688754
Gieselmann, A., Podleschka, C., Rozental, A., and Pietrowsky, R. (2021). Communication formats and their impact on patient perception and working mechanisms: a mixed-methods study of chat-based vs. face-to-face psychotherapy for insomnia. Behav. Therapy 52, 430–441. doi: 10.1016/j.beth.2020.06.001
Gilbert, D. A., and Hayes, E. (2009). Communication and outcomes of visits between older patients and nurse practitioners. Nurs. Res. 58, 283–293. doi: 10.1097/NNR.0b013e3181ac1413
Giles, D., Stommel, W., Paulus, T., Lester, J., and Reed, D. (2015). Microanalysis of online data: the methodological development of “digital CA”. Discourse Context Media 7, 45–51. doi: 10.1016/j.dcm.2014.12.002
Have, P. T. (1999). Structuring writing for reading: hypertext and the reading body. Hum. Stud. 22, 273–298.
Have, P. T. (2007). “Doing conversation analysis”, in Introducing Qualitative Methods, 2nd Edn (London: SAGE Publications).
Hefner, J. L., MacEwan, S. R., Biltz, A., and Sieck, C. J. (2019). Patient portal messaging for care coordination: a qualitative study of perspectives of experienced users with chronic conditions. BMC Fam. Pract. 20, 57. doi: 10.1186/s12875-019-0948-1
Herring, S. C. (1999). Interactional coherence in CMC. J. Comput. Med. Commun. 4, 106. doi: 10.1109/HICSS.1999.772674
Herring, S. C., and Androutsopoulos, J. (2015). “Computer-mediated discourse 2.0,” in The Handbook of Discourse Analysis 2 (Hoboken, NJ: John Wiley and Sons), 127–151. doi: 10.1002/9781118584194.ch6
Hoey, E., and Kendrick, K. (2017). “Conversation analysis,” in Research Methods in Psycholinguistics: A Practical Guide, ed A. M. B. G. P. Hagoort (Hoboken: Wiley Blackwell).
Hsieh, H. F., and Shannon, S. E. (2005). Three approaches to qualitative content analysis. Qual. Health Res. 15, 1277–1288. doi: 10.1177/1049732305276687
Inui, T. S., Carter, W. B., Kukull, W. A., and Haigh, V. H. (1982). Outcome-based doctor-patient interaction anaylsis: I. Comparison of techniques. Med. Care 20, 535–549. doi: 10.1097/00005650-198206000-00001
Irani, H. F., and Chalak, A. (2016). Interaction analysis in an international asynchronous learning environment. Teach. English Technol. 16, 33–47. Available online at: https://tewtjournal.org/download/4-interaction-analysis-in-an-international-asynchronous-learning-environment-by-fariba-haghighi-irani-and-azizeh-chalak/
König, K. (2019). Stance taking with “laugh” particles and emojis: sequential and functional patterns of “laughter” in a corpus of German WhatsApp chats. J. Pragmat. 142, 156–170. doi: 10.1016/j.pragma.2019.01.008
Koudenburg, N., Postmes, T., and Gordijn, E. H. (2016). Beyond content of conversation: the role of conversational form in the emergence and regulation of social structure. Person. Soc. Psychol. Rev. 21, 50–71. doi: 10.1177/1088868315626022
Kravitz, R. L., Bell, R. A., and Franz, C. E. (1999). A taxonomy of requests by patients (TORP): a new system for understanding clinical negotiation in office practice. J. Fam. Pract. 48, 872–878.
Lindemann, K., Ruoss, E., and Weinzinger, C. (2016). Dialogical text competence: writing routines in online teams. Zeitschrift fur Angewandte Linguistik 65, 159–182. doi: 10.1515/zfal-2016-0021
Luo, T. C., Aguilera, A., Lyles, C. R., and Figueroa, C. A. (2021). Promoting physical activity through conversational agents: mixed methods systematic review. J. Med. Internet Res. 23, e25486. doi: 10.2196/25486
Lustig, A., Brookes, G., and Hunt, D. (2021). Linguistic analysis of online communication about a novel persecutory belief system (Gangstalking): mixed methods study. J. Med. Internet Res. 23, e25722. doi: 10.2196/25722
Mazzi, M. A. (2011). “Quantitative methods for the analysis of verbal interactions in psychotherapy,” in Communication in Cognitive Behavioral Therapy, ed M. Rimondini (New York, NY: Springer Science + Business Media), 233–247. doi: 10.1007/978-1-4419-6807-4_10
McHoul, A. W. (1982). Telling How Texts Talk: Essays on Reading and Ethnomethodology. New York, NY: Routledge and K. Paul.
McVay, M., Steinberg, D., Askew, S., and Bennett, G. G. (2019). Provider counseling and weightloss outcomes in a primary care-based digital obesity treatment. J. Gen. Internal Med. 34, 992–998. doi: 10.1007/s11606-019-04944-5
Meredith, J. (2017). Analysing technological affordances of online interactions using conversation analysis. J. Pragmat. 115, 42–55. doi: 10.1016/j.pragma.2017.03.001
Monaghesh, E., and Hajizadeh, A. (2020). The role of telehealth during COVID-19 outbreak: a systematic review based on current evidence. BMC Public Health 20, 1193. doi: 10.1186/s12889-020-09301-4
Mosa, A. S. M., Yoo, I., and Sheets, L. (2012). A systematic review of healthcare applications for smartphones. BMC Med. Inform. Decis. Mak. 12, 67. doi: 10.1186/1472-6947-12-67
Mujica, C., Tendulkar, S., Alvarez, K., Cruz-Gonzalez, M., and Alegría, M. (2020). Association between patient-provider racial and ethnic concordance and patient-centered communication in outpatient mental health clinics. J. Psychother. Integr. 30, 423–439. doi: 10.1037/int0000195
Nascimento, I., Oliveira, J. A. Q., Wolff, I. S., Ribeiro, L. D., Silva, M., Cardoso, C. S., et al. (2020). Use of smartphone-based instant messaging services in medical practice: a cross-sectional study. São Paulo Med. J. 138, 86–92. doi: 10.1590/1516-3180.2020.0010.r1.28032020
Ngenye, L., and Kreps, G. (2020). A review of qualitative methods in health communication research. Qualit. Rep. 25, 631–645. doi: 10.46743/2160-3715/2020.4488
Paulus, T., Warren, A., and Lester, J. (2018). Using Conversation Analysis to Understand How Agreements, Personal Experiences, and Cognition Verbs Function in Online Discussions. Available online at: https://www.languageatinternet.org/articles/2018/paulus
Petitjean, C., and Morel, E. (2017). “Hahaha”: laughter as a resource to manage WhatsApp conversations. J. Pragmat. 110, 1–19. doi: 10.1016/j.pragma.2017.01.001
Poole, M. S. (2007). Generalization in process theories of communication. Commun. Methods Meas. 1, 181–190. doi: 10.1080/19312450701434979
Pope, C., Ziebland, S., and Mays, N. (2000). Analysing qualitative data. BMJ 320, 114–116. doi: 10.1136/bmj.320.7227.114
Reeves, S., and Brown, B. (2016). “Embeddedness and sequentiality in social media”, in Proceedings of the ACM Conference on Computer Supported Cooperative Work (New York, NY: CSCW), 1052–1064. doi: 10.1145/2818048.2820008
Rendle-Short, J. (2015). Dispreferred responses when texting: delaying that “no” response. Discourse Commun. 9, 643–661. doi: 10.1177/1750481315600309
Richard, C., and Lussier, M. T. (2006). MEDICODE: an instrument to describe and evaluate exchanges on medications that occur during medical encounters. Patient Educ. Couns. 64, 197–206. doi: 10.1016/j.pec.2006.02.002
Rienzo Renato, A. (2019). “An analysis of telemedicine experiences and services in Chile,” in Telehealth, ed T. F. Heston (London: IntechOpen). doi: 10.5772/intechopen.81756
Rogers, E. M. (1986). Communication Technology: The New Media in Society. New York; London: Free Press; Collier Macmillan.
Roter, D., and Larson, S. (2002). The Roter interaction analysis system (RIAS): utility and flexibility for analysis of medical interactions. Patient Educ. Couns. 46, 243–251. doi: 10.1016/S0738-3991(02)00012-5
Roter, D. L., and Hall, J. A. (1989). Studies of doctor-patient interaction. Ann. Rev. Public Health 10, 163–180. doi: 10.1146/annurev.pu.10.050189.001115
Roter, D. L., and Larson, S. (2001). The relationship between residents' and attending physicians' communication during primary care visits: an illustrative use of the roter interaction analysis system. Health Commun. 13, 33–48. doi: 10.1207/S15327027HC1301_04
Sacks, H., Schegloff, E. A., and Jefferson, G. (1974). A simplest systematics for the organization of turn-taking for conversation. Language 50, 696–735. doi: 10.1353/lan.1974.0010
Schegloff, E. A. (1993). Reflections on quantification in the study of conversation. Res. Lang. Soc. Interact. 26, 99–128. doi: 10.1207/s15327973rlsi2601_5
Schmid Mast, M., Hall, J. A., Cronauer, C. K., and Cousin, G. (2011). Perceived dominance in physicians: are female physicians under scrutiny? Patient Educ. Counsel. 83, 174–179. doi: 10.1016/j.pec.2010.06.030
Seppen, B. F., den Boer, P., Wiegel, J., Ter Wee, M. M., van der Leeden, M., de Vries, R., et al. (2020). Asynchronous mHealth interventions in rheumatoid arthritis: systematic scoping review. JMIR mHealth uHealth 8, e19260–e19260. doi: 10.2196/19260
Shigekawa, E., Fix, M., Corbett, G., Roby, D. H., and Coffman, J. (2018). The current state of telehealth evidence: a rapid review. Health Aff. 37, 1975–1982. doi: 10.1377/hlthaff.2018.05132
Shin, D. W., Roter, D. L., Roh, Y. K., Hahm, S. K., Cho, B., Park, H. K., et al. (2015). Physician gender and patient centered communication: the moderating effect of psychosocial and biomedical case characteristics. Patient Educ. Counsel. 98, 55–60. doi: 10.1016/j.pec.2014.10.008
Sinclair, J. M. (1991). “Corpus, concordance, collocation”, in Describing English language (Oxford: Oxford University Press).
Stiles, W. B., and Putnam, S. M. (1989). Analysis of verbal and nonverbal behavior in doctor-patient encounters. Commun. Med. Patients 1989,211–222.
Street, R. L., Makoul, G., Arora, N. K., and Epstein, R. M. (2009). How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Educ. Couns. 74, 295–301. doi: 10.1016/j.pec.2008.11.015
Symon, G., and Cassell, C. (2012). Qualitative Organizational Research: Core Methods and Current Challenges. New York, NY: SAGE Publications. doi: 10.4135/9781526435620
Vázquez-Cano, E., González, A. I. H., and Sáez-López, J. M. (2019). An analysis of the orthographic errors found in university students' asynchronous digital writing. J. Comput. Higher Educ. 31, 109–134. doi: 10.1007/s12528-018-9189-x
Vázquez-Cano, E., Mengual-Andrés, S., and Roig-Vila, R. (2015). Lexicometric analysis of the specificity of teenagers' digital writing in WhatsApp. RLA 53, 83–105. doi: 10.4067/S0718-48832015000100005
Ventola, C. L. (2014). Mobile devices and apps for health care professionals: Uses and benefits. Pharm. Ther. (2014) 39:356–364.
Verhoeven, F., Tanja-Dijkstra, K., Nijland, N., Eysenbach, G., and van Gemert-Pijnen, L. (2010). Asynchronous and synchronous teleconsultation for diabetes care: a systematic literature review. J. Diabet. Sci. Technol. 4, 666–684. doi: 10.1177/193229681000400323
Virtanen, M. T., and Kääntä, L. (2018). At the intersection of text and conversation analysis: analysing asynchronous online written interaction. AFinLA-e Soveltavan Kielitieteen Tutkimuksia 11, 155. doi: 10.30660/afinla.69081
Vogl, S. (2017). Quantifying transformation of qualitative data in quantitative data in mixed methods studies. Kolner Zeitschrift Fur Soziologie Und Sozialpsychologie 69, 287–312. doi: 10.1007/s11577-017-0461-2
Walther, J. B., and Burgoon, J. K. (1992). Relational communication in computer-mediated interaction. Hum. Commun. Res. 19, 50–88. doi: 10.1111/j.1468-2958.1992.tb00295.x
Warren, A. N. (2018). Navigating assigned roles for asynchronous online discussions: Examining participants' orientation using conversation analysis. Online Learn. J. 22, 27–45. doi: 10.24059/olj.v22i4.1512
Yip, J. W. C. (2020). Evaluating the communication of online social support: a mixed-methods analysis of structure and content. Health Commun. 35, 1210–1218. doi: 10.1080/10410236.2019.1623643
Keywords: communication, digital health, patient-provider, conversation analysis, online interaction
Citation: Rey Velasco E, Pedersen HS and Skinner TC (2022) Methodological approaches applicable to patient-provider interaction analysis: A mini-review. Front. Commun. 7:1034427. doi: 10.3389/fcomm.2022.1034427
Received: 01 September 2022; Accepted: 28 September 2022;
Published: 12 October 2022.
Edited by:
Steven Bellman, University of South Australia, AustraliaReviewed by:
Bryan Abendschein, Western Michigan University, United StatesCopyright © 2022 Rey Velasco, Pedersen and Skinner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elena Rey Velasco, ZXJ2QHBzeS5rdS5kaw==; Hanne Sæderup Pedersen, c2JjODQ2QGh1bS5rdS5kaw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.