 Bernadette A. M. Vermeij
Bernadette A. M. Vermeij Carin H. Wiefferink
Carin H. Wiefferink Ron H. J. Scholte2
Ron H. J. Scholte2- 1Research Department, Dutch Foundation for the Deaf and Hard of Hearing Child, Amsterdam, Netherlands
- 2Behavioural Science Institute, Radboud University, Nijmegen, Netherlands
- 3Research Department, Royal Dutch Kentalis, Sint-Michielsgestel, Netherlands
Introduction: In the Netherlands, early language intervention is offered to children with presumed Developmental Language Disorder (DLD). The intervention is a combination of group language intervention, individual speech and language therapy and parent-implemented language intervention. During the intervention, some children show more language progress than others. It is unclear what might explain this variation. In this study, we therefore explored to what extent child, parental, and treatment factors were predictive for receptive and expressive language outcomes of young children with presumed DLD during early language intervention.
Methods: Four multiple regression analyses were conducted with four child factors [pre-test receptive syntax, behavior (internalizing and externalizing), non-verbal cognitive ability and gender], one parental factor (parental stress) and one treatment factor (treatment duration) as predictors and receptive and expressive language post-test scores as outcomes. For each language post-test, the corresponding pre-test language measure was also added. Data of 183 children with presumed DLD were included.
Results: Receptive syntax problems were an important predictor of expressive language outcomes. Findings also showed a longer treatment duration to be a predictor of progress in expressive vocabulary. Internalizing behavior, externalizing behavior, non-verbal cognitive ability, gender and parental stress did not contribute to predicting language outcomes. Lower pre-intervention language scores led to lower corresponding post-intervention language scores.
Conclusions: Professionals may need to be aware that children with receptive problems may be indicative of more pervasive impairment and that it can be more difficult to improve their language problems. In fact, children with receptive language problems may need both more and different approaches. The finding that the level of the pre-intervention score has an essential influence on language outcomes underlines the importance of early diagnosis and early intervention, to prevent language problems increasing.
Introduction
Children with a developmental language disorder (DLD) (Bishop, 2017) have difficulties in expressive language development. Some children experience difficulties in receptive language too. To improve the language development of these children, it is important to start intervention early (Singleton, 2018; Nouraey et al., 2021; Kaiser et al., 2022). Therefore, in the Netherlands, an early language intervention program is offered to children with presumed DLD (see Participants) between 2 and 4 years of age. The intervention consists of a combination of group language intervention, individual speech and language therapy and parent-implemented language intervention. Language outcomes after the intervention vary, in part because some children make more progress than others. Unfortunately, it is still unclear what might explain this variation. More knowledge about factors that may account for this variation is of importance, because it can provide professionals with insights for which children or under what condition language progress is more difficult (Short et al., 2020). These children may need extra help or specific intervention strategies to accomplish improvement.
When studying factors that predict variation in language development, different types of factors need to be taken into account, because they can be hindering or facilitating (Taylor et al., 2013; Mckean et al., 2017). These include child factors, parental factors and treatment factors. Child factors are of importance, because children with DLD are a very diverse group, varying in the type of language problems and the presence of additional problems (Bishop, 2017). These differences may result in children displaying differential trajectories during the intervention. For example, the presence of additional problems may hinder language development, which can make it more difficult for children with these problems to improve their language proficiency compared to children without additional problems. Second, parental factors may influence language development, also during intervention (Shalev et al., 2020). Parental stress, for example, may influence the quality of parent-child interaction (Santelices and Cortés, 2022). Because of the stress, parents may be less sensitive in the interaction with their child and have a more authoritarian parenting style, which may lead to language use that is less facilitating for language stimulation. Third, because we study predictors in an intervention setting, we should not level out the influence of treatment factors. Treatment factors, like treatment duration, differ and may also have their influence on language outcomes (Warren et al., 2007; Law et al., 2017).
Therefore, in this study, we examine whether and to what extent child, parental and treatment factors predict variation in language outcomes after an early language intervention program for children with presumed DLD in the Netherlands. Five child and parental factors are included, namely receptive language proficiency, behavior problems, non-verbal cognitive ability, gender and parental stress. All these factors are monitored or registered during the intervention. These factors are chosen based on the experience of professional and empirical evidence indicating a relation between these factors and DLD (Gallinat and Spaulding, 2014; Leonard, 2014; Curtis et al., 2018; Rennecke et al., 2019; Yarian et al., 2021). There is, however, still less knowledge about the predictive value of such factors on language outcomes during an intervention for young children with DLD, which will be the focus in our study. Children can start the intervention at different ages and they cannot stay in the program over 4 years of age, because of the transfer to school. Therefore, treatment duration differs and is included as the sixth predictive factor. Below, each factor will be described more thoroughly.
Receptive language proficiency
Children with DLD always have expressive language problems. Some children also display receptive language problems, which can occur on different domains such as receptive syntax or receptive vocabulary. Language development of children with lower receptive language proficiency may develop differently during the intervention compared with children with lower expressive language proficiency only. Empirical evidence shows that problems in receptive language proficiency are harder to treat than expressive language problems (Law et al., 2004; Boyle et al., 2010; Heidlage et al., 2020) and that expressive language is hard to improve when children experience receptive problems too (Law et al., 2004; O'neill et al., 2019). These studies support the assumption that a low receptive proficiency hinders language development, resulting in lower language outcomes for children with receptive problems, compared to children with expressive language problems only. This applies both to language development over several years (Chiat and Roy, 2008; O'neill et al., 2019; Yarian et al., 2021), as to language development in an intervention setting (Law et al., 2004). We can thus conclude there is empirical evidence that low receptive language proficiency at the start of intervention can negatively influence language development during the intervention. What may be underlying? Mabye, lower receptive proficiency may increase language learning demands, which makes it also more difficult to develop in the expressive domains (Yarian et al., 2021). When examining the multivariate influence of several factors on language outcomes, it is therefore of importance to take receptive language proficiency into account.
Behavior problems
Children with DLD more often display behavior problems compared with their typically developing peers. They are at greater risk for developing internalizing behavior problems such as withdrawn, anxious, or depressed behavior (St Clair et al., 2011; Maggio et al., 2014; Yew and O'kearney, 2015a; Vermeij et al., 2021), as well as externalizing behavior problems such as aggression or attention deficits (Snowling et al., 2006; Maggio et al., 2014; Yew and O'kearney, 2015b, 2017; Vermeij et al., 2021). Several studies indicate that language problems may lead to behavior problems in children (Petersen et al., 2013; Morgan et al., 2015; Salmon et al., 2016). However, when behavior problems are present, they may also affect language development (Girard et al., 2016; Wang et al., 2018). Several explanations may be underlying. For example, when children display aggressive behavior or act out, this may influence the quality of parent-child interactions (Dionne et al., 2003). Parents may focus on reducing disruptive behavior, which may affect parent-child interactions negatively. Alternatively, it may be more difficult for a child with attention difficulties to learn from interaction with others (Green et al., 2014). Both explanations may result in fewer opportunities to learn language and may influence the success of an intervention. Although there are some indications that behavior problems are related to lower language scores during child development, it is unclear if behavior problems also hinder language development during language intervention for children with DLD.
Non-verbal cognitive ability
Several studies have focused on the relation between non-verbal cognitive ability and language proficiency and found that a higher non-verbal cognitive ability is related to better language proficiency (Gallinat and Spaulding, 2014; Rice and Hoffman, 2015). These studies focus both on children with a non-verbal cognitive ability of 85 and higher (Rice and Hoffman, 2015) as well as children with lower cognitive abilities (from 70 and up) (Gallinat and Spaulding, 2014). Children with a lower non-verbal cognitive ability may not only have lower language scores, it may also be more difficult for them to acquire new proficiency and benefit from intervention. However, some studies indicate that both children with a higher as well as with a lower cognitive non-verbal ability can benefit from language intervention (Boyle et al., 2007; Bowyer-Crane et al., 2011; Bishop et al., 2016). These studies focused on children over 4 and a half years of age. Yarian et al. (2021) studied children with DLD under 5 years of age and found that non-verbal cognitive ability did not predict expressive syntax. However, this was not an intervention setting. To the best of our knowledge, empirical evidence for the influence of non-verbal cognitive ability on language outcomesof children with DLD younger than four in an intervention setting is largely lacking.
Gender
When examining predictors of language development or intervention-effects of language development, gender is often taken into account (Taylor et al., 2013; Rice and Hoffman, 2015; Mckean et al., 2017; Short et al., 2020), because of the possible differences between boys and girls. Although some studies suggest boys and girls with DLD not differ in the severity of their language problems (Norbury et al., 2016), there are also indications that boys and girls vary on the type of language problems and the presence of additional problems (Wiefferink et al., 2020). According to Wiefferink et al. (2020), boys more often have mixed receptive and expressive language problems and more frequently display behavior problems than girls. This raises the question if boys and girls benefit the same way of intervention. In the Dutch language intervention program, an important aspect is improving language development by facilitating the interaction with significant others. There are indications that boys and girls respond differently to their environment and therefore their environment to them (Vallotton et al., 2012). Gender may therefore impact interaction with significant others and consequently affect the results of an intervention. A study of the effects of an Early Head Start program on expressive vocabulary supports this assumption (Vallotton et al., 2012). They found for 2 year old boys, parental stress to be related to lower expressive vocabulary scores. For girls however, the program did protect expressive vocabulary from the negative influence of parental stress.
Parental stress
Several studies report that parents of children with DLD can experience higher levels of stress (Horwitz et al., 2003; Schaunig et al., 2004; Rennecke et al., 2019). This might be due to the language problems of their child. Although the language problems may lead to parental stress, the stress may also have its influence on language development. Parents experiencing stress may feel insecure in parenting and may be less open to respond to the children's needs (Coleman and Karraker, 1997; Santelices and Cortés, 2022), which can negatively influence the interaction with their child (Mckay et al., 1996; Santelices and Cortés, 2022). Parental stress may also affect parental involvement during an intervention (Shalev et al., 2020). Parents may feel less able to participate in the intervention, which may negatively affect intervention outcomes as a result. On the other hand, parents experiencing more stress might have more need for help and thus want to be more involved in the intervention, which can be beneficial for language outcomes (Strauss et al., 2012; Shalev et al., 2020). Although there are indications that parental stress may have its influence on intervention outcomes of children with autism and children of low-income families (Strauss et al., 2012; Vallotton et al., 2012), the influence and the direction of the influence on the language outcomes of children with DLD during early language intervention is still unclear.
Treatment duration
Besides child factors and parental factors, treatment factors may also influence language outcomes after intervention (Warren et al., 2007; Law et al., 2017; Segura-Pujol and Briones-Rojas, 2021). The language intervention program in the Netherlands is offered to children with presumed DLD between 2 and 4 years old. Because children can start the intervention at different ages and most of them leave the intervention around 4 years of age, because of the transfer to school, treatment duration differs. One may expect that a longer treatment duration would lead to better results: the longer the intervention time, the more vocabulary can be learned and the more syntactic structures can be practiced. Although treatment duration is known to be of importance when studying intervention effects, there is still little knowledge concerning the influence of treatment duration on language outcomes of children with DLD (Segura-Pujol and Briones-Rojas, 2021).
This study explores to what extent child, parental and treatment factors are predictive for receptive and expressive language outcomes of children with presumed DLD after an early language intervention program. More specifically, the influence of these types of factors on receptive syntax, receptive vocabulary, expressive syntax and expressive vocabulary is studied.
Based on the studies described above, there is empirical evidence that receptive language proficiency predicts language outcomes later on in development and that non-verbal cognitive ability has no effect on language outcomes in an intervention setting. Evidence for the effect of behavior problems, gender, parental stress and treatment duration on language outcomes is inconclusive or scarce for these young children. We therefore hypothesize that receptive language proficiency will contribute to predicting variation in language outcomes after the early language intervention program and that non-verbal cognitive ability will not. We want to explore the predictive value of the other four factors in this study.
Methods
Participants
In the Netherlands, children with language problems are referred to speech and hearing centers for multidisciplinary assessment (Wiefferink et al., 2020). At these centers, children are tested on receptive and expressive speech and language proficiency (phonology, vocabulary, syntax, pragmatics), hearing ability, cognitive proficiency and behavior. When children have limitations in at least one language domain that is not caused by hearing loss or lower cognitive abilities, they receive the diagnosis “presumed DLD”. This diagnosis is tentative. Due to variation in early language development, it is hard to set a definite diagnosis of DLD in young children, especially in children younger than 3 (Bishop et al., 2017). Therefore, some children may turn out to be late talkers instead of children with DLD.
When the diagnosis “presumed DLD” is set, children are referred to a specialized language intervention center where they receive early language intervention. In this study, 183 children (149 boys, 34 girls) from 17 locations were included, who received this intervention for at least 3 months between 2012 and 2016. All children had a score of 1 SD or more below the normative mean on at least one of four language domains at the intervention start, indicating language problems on that domain(s). The four language domains were receptive syntax, receptive vocabulary, expressive syntax and expressive vocabulary, respectively.
There were several exclusion criteria. First, children with a non-verbal cognitive ability that was lower than a Q-score of 80 (mean score: 100, SD = 15) were excluded. Second, multilingual children were excluded, because the norms of the language tests were only applicable to monolingual Dutch-speaking children. Third, children with only phonological problems were excluded, i.e., children with language scores above 84 on all four language tests measuring receptive syntax, receptive vocabulary, expressive syntax and expressive vocabulary. Fourth, children with a suspicion of additional problems such as ADHD, autism or other neurodevelopmental disabilities were also excluded. Professionals could get this suspicion during the intervention, but because of the young age, it was not possible to set a clear diagnosis of these disabilities.
Children started the intervention at the mean age of 38 months (range 26–45 months). The mean attendance of the children in this study was 90.6 days (SD: 36.4, range: 34–219) and mean treatment duration in months was 8.8 (SD: 3.8, range 3–21) months. All children kept the diagnosis presumed DLD during the intervention. Most mothers (96%) and fathers (99%) were medium or high educated, meaning that they had attended at least secondary education.
Early language intervention
In the Netherlands, an early language intervention program is offered to 2–4 year old children with presumed DLD. The intervention is a combination of group language intervention, speech and language therapy and parent-implemented language intervention and is carried out by two preschool teachers, a speech and language therapist (SLT) and a psychologist. Eight to ten children visit the group intervention three mornings a week. At least once a week, the SLT takes a child separately for individual speech and language therapy. Besides the direct intervention for the child, a parental program is offered to the parents. The early language intervention program is manualized and is judged to be based on latest scientific theories and empirical evidence by the Netherlands Youth Institute (www.nji.nl) (Wiefferink, 2021).
Although the intervention takes place in three different settings, the same key techniques are used by both the parent and the professional to stimulate the language development of the child. For example the technique “observe, wait and listen” (Pepper and Weitzman, 2004), in which both parents and professionals observe the child's interest, wait to give the child a chance to initiate in the interaction, and listen to what the child wants to say. Or a technique such as focused stimulation (Paul and Norbury, 2012), which means the child is frequently offered input of a sound, word, or utterance in different meaningful contexts. The use of visual input (Pepper and Weitzman, 2004) is also frequently used by both parents and professionals. This means that signs, gestures, pictures or objects are used in the interaction with the child. These techniques are chosen, because empirical evidence states they have a positive influence on language development (Paul and Norbury, 2012; Kruythoff-Broekman et al., 2019; Van Berkel-Van Hoof et al., 2019).
Group language intervention
All children in this study were included in the language intervention program. They all received group language intervention from 9.00 to 12.30, three mornings a week. Four different kinds of activities were offered during the group language intervention, namely daily routine activities, educational play, intentional language stimulation, and group speech and language therapy. Daily activities, such as welcoming and eating and drinking were used to repeatedly expose the children to the same words and sentences. Educational play was used to stimulate playing with other children and the use of turn taking. Intentional language stimulation was used by the professionals to teach children new vocabulary and sentences, for example during singing or picture book reading. Group speech and language therapy was carried out by the SLT and aimed at stimulating receptive and expressive language development.
Individual speech and language therapy
In addition, every child separately received individual language therapy once a week. This therapy was tailored to the specific language problems of the child, aiming at a variety of language domains, such as receptive and expressive syntax and vocabulary. Different techniques were used by the SLT to stimulate language development such as using contrasting sentences (Fey et al., 2003), emphasizing a word by placing it at the end of a sentence (Leonard, 2014) or recasting [correctly reproducing a child's words or utterance and adding new (syntactic, semantic or phonological) information, while the child's meaning is maintained] (Camarata and Nelson, 2006).
Parent-implemented language intervention
A parental program was available for the parents. First, there was a home visit, to explain to parents more about DLD and to get an impression of the situation at home. Second, parents were invited at the group, to join all the group activities of their child. Third, psycho-education was offered in several sessions. This concerned topics such as follow-up education and social-emotional development. Last, parents were encouraged to attend two trainings of six sessions. In the first training, they learned language stimulating interaction techniques to improve interaction with their child. The second training focused on using signs and gestures in communication with their child.
Parents could attend the speech and language training and the signs and gestures training. Not all parents in this study followed these trainings: 37% of the parents followed 4 or more sessions of the speech and language training, while 35% of the parents followed 4 or more sessions of the signs and gestures training. In total, 58% of the parents followed at least one training. Not all parents had to follow the speech and language training, because they had already followed such a training before the start of the early language intervention program.
Treatment quality and fidelity
Certified SLTs, preschool teachers and psychologists delivered the intervention. The quality of the treatment was monitored in several ways. First, all professionals followed additional education, necessary to appropriately deliver the intervention. This concerned for example trainings how to use signs and visual communication with children with DLD. Second, at least five times a year, monodisciplinary collegial consultation groups were organized in which professionals discussed and reflected the way they offered intervention. If professionals experienced problems in their way of working, individual coaching was available. Third, a linguist observed in all treatment groups with the aim to monitor and enhance quality and fidelity of the language offered to the child and the used key techniques. She visited each group at least once a year.
Instruments
Receptive and expressive language proficiency of the pre-test and post-test was assessed with four norm-referenced and standardized tests by an SLT. Raw scores were converted into standardized Q-scores (mean score: 100, standard deviation: 15). This way, a comparison with the test norms could be made. Receptive syntax was tested with the “Schlichting Receptive Language Test.” This test measures receptive language with an emphasis on syntax. In this test, the child had to carry out assignments, asked by the SLT. The test's internal consistency is 0.93 (lambda-2) and test-retest reliability is 0.82 (Schlichting and Lutje Spelberg, 2010a). Receptive vocabulary was assessed with the “Peabody Picture Vocabulary Test-III-NL” (Dunn et al., 2005), in which the child had to match a spoken word to one out of four pictures. The test's internal consistency ranges from 0.89 to 0.92 for children 2;3–4;5 years old (lambda-2). The test-retest reliability score is only available for adults (Dunn et al., 2005).
Expressive syntax and expressive vocabulary were assessed with two subtests of the “Schlichting Expressive Language Test” (Schlichting and Lutje Spelberg, 2010b). Expressive syntax was measured by asking the child to repeat and complete sentences of increasing grammatical complexity. The test's internal consistency is 0.90 (lambda-2) and test-retest reliability is 0.73 (Schlichting and Lutje Spelberg, 2010b). In the subtest for expressive vocabulary, children had to name pictures of objects or actions. The test's internal consistency is 0.89 (lambda-2) and test-retest reliability 0.93 (Schlichting and Lutje Spelberg, 2010b).
Furthermore, parents were asked to complete a questionnaire about the behavior of their child: the “Child Behavior Checklist 1,5–5” (CBCL) (Verhulst and Van Der Ende, 2001). The questionnaire contains two subscales: internalizing behavior problems and externalizing behavior problems. The test's internal consistency for internalizing behavior is 0.89 and for externalizing behavior is 0.92 (Cronbach's Alpha). Test-retest reliability for internalizing behavior is 0.90, for externalizing behavior 0.87 (Achenbach and Rescorla, 2000). Raw scores were converted into standardized t-scores, with a mean of 50 and a standard deviation of 10. Higher scores indicate higher levels of problem behavior, with t-scores above 59 indicating borderline and clinical scores.
Parental stress was assessed with the “Parenting Stress Questionnaire” (PSQ) (Vermulst et al., 2015). The questionnaire consists of 34 items concerning parent-child relationship problems, parenting problems, depressive mood, parental role restriction and physical health problems. The total score for parental stress was converted into a t-score, with a mean of 50 and a standard deviation of 10. Cronbach's Alpha of the test ranges between 0.89 and 0.91.
Non-verbal cognitive ability was assessed with a Dutch non-verbal intelligence test, the SON-R (Tellegen et al., 1998). This is a norm-referenced and standardized test for children between 2 and 8 years old, which generates standardized IQ-scores, with a mean score of 100 and a standard deviation of 15. During the test, children have to carry out assignments such as imitating a mosaic pattern or identifying a common feature out of several pictures. Because the SON-R can be assessed without the use of spoken or written language, is it suitable for assessment of children with language problems. Internal consistency of the IQ-score is 0.91 (stratified alpha) and test-retest reliability is 0.81.
Procedure
Test scores were gathered by professionals during the early language intervention program. Routine Outcome Monitoring (ROM) (Duncan et al., 2010; De Beurs et al., 2011; Van Sonsbeek et al., 2014; Bickman et al., 2016) was used, to follow the receptive and expressive language development of the children during the intervention. Language proficiency was assessed by the SLTs of the intervention center, the SLTs, the speech and hearing center or an SLT working in a practice. Language tests were administered in a time period ranging from 3 months before to 3 months after intervention start. The same timeframe was held for the end of the intervention. The time between testing and re-testing had to be at least 3 months. Parents completed questionnaires about behavior and parental stress at the start of the intervention. Non-verbal cognitive ability was assessed with the SON-R by a psychologist within 6 months of intervention start.
All data were entered into a web-based database, the BergOp system, version 4.0.8 (Praktikon, 2016). This study made use of Routine Outcome Monitoring data, that was gathered in clinical practice. Parents of all 183 children consented to the use of the data of their child anonymously for scientific research. Because no extra data then necessary for clinical goals was used, ethical approval from a Research Ethics Committee was not required.
Results
For the pre-test and post-test as well, the dataset was inspected for missing values. The number of missing ranged from 0 (0%, receptive syntax pre-test) to 98 (54%, receptive vocabulary post-test). For 8 of the 12 imputed variables, 14% or less of the data was missing. Only for receptive vocabulary, missing data points were more than 40%. Little's MCAR test confirmed that data was missing completely at random (p = 0.132). Multiple imputation was used to impute missing data on the language pre-tests and post-test s, internalizing and externalizing behavior scores pre-intervention and parental stress pre-intervention. This generated the dataset that was used for further analyses. Scores of non-verbal cognitive ability, gender and treatment duration were complete.
The mean pre-test and post-test scores of the four language domains are presented in Table 1. T-tests revealed significant differences between the pre-test and post-test scores for all four language domains. The mean scores, median and range of the predictors are displayed in Table 2. Gender was the only nominal variable, with 81% boys and 19% girls. The factor “receptive language proficiency” was operationalized with the receptive syntax pre-test.
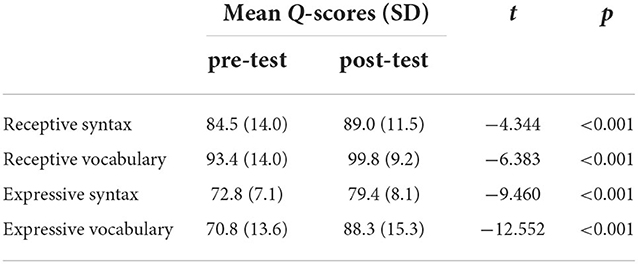
Table 1. The mean pre-test and post-test language scores of all 183 children, compared with t-tests.
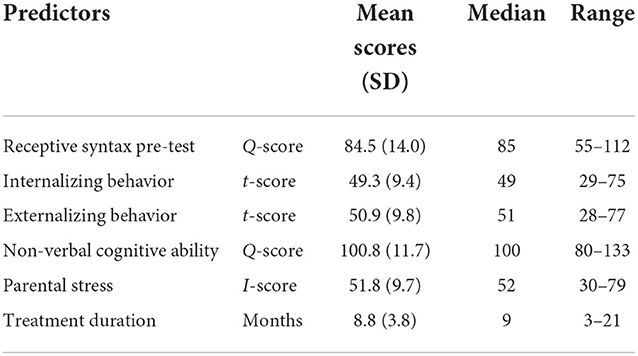
Table 2. Mean scores, medians and ranges of continuous predictors.
This study explores to what extent child, parental and treatment factors are predictive for receptive and expressive language outcomes of children with presumed DLD after an early language intervention program. To answer this research question, first, bivariate correlations were calculated to analyze the strength of the relations between the predictors and the four language post-test s of receptive syntax, receptive vocabulary, expressive syntax and expressive vocabulary (Table 3). The post-test scores of expressive syntax correlated with all four language pre-test scores. The post-test s of receptive syntax, receptive vocabulary and expressive vocabulary correlated with the pre-test scores of all these three domains, but not with the pre-test of expressive syntax. All four language post-test scores showed a significant correlation with the pre-test scores of non-verbal cognitive ability and the post-test score of expressive vocabulary correlated with treatment duration.
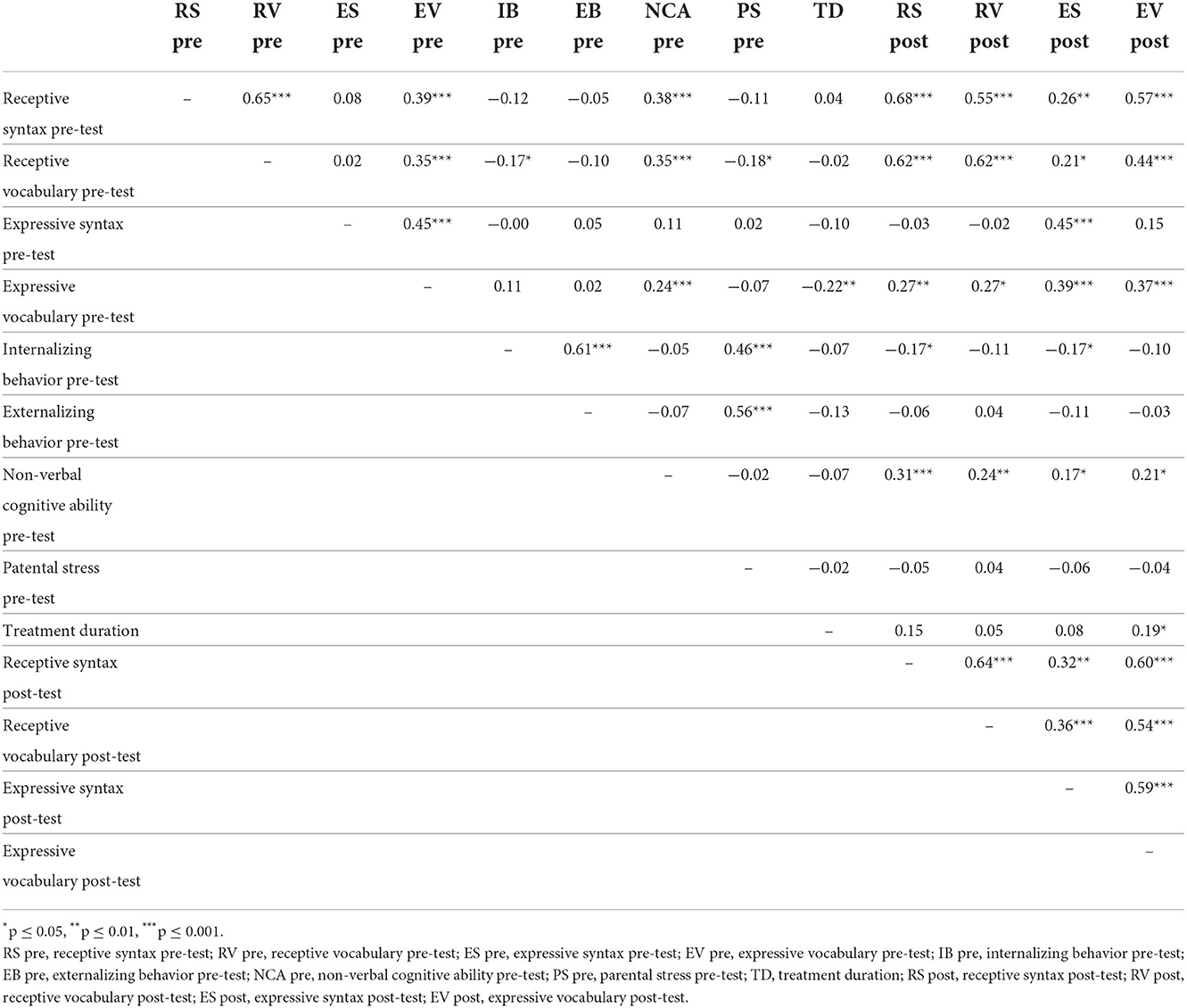
Table 3. Correlations between the pre-test language scores, predictors and post-test language scores.
Second, four multiple regression analyses were carried out with the enter method to examine which factors predict post-test language scores if the effects of all other predictors are held constant. Child factors (pre-test receptive syntax, internalizing behavior, externalizing behavior, non-verbal cognitive ability and gender), one parental factor (parental stress) and one treatment factor (treatment duration) were included as predictors of the analyses. For each language post-test, the corresponding language measure at pre-test was always included to enable analysis of the effects of the other predictors on outcome when controlling for pre-test scores (and all other potential predictors). Except for receptive syntax, each analysis therefore included two continuous language pre-test scores: the pre-test score of receptive syntax and the corresponding pre-test score. The analysis predicting the receptive syntax outcomes included the receptive syntax pre-test only. The dichotomous variable gender was converted into a dummy variable. The findings showed that both expressive language domains after intervention were not only predicted by corresponding expressive pre-test scores at start, but also by receptive syntax scores pre-intervention (significance level p < 0.05) (Table 4). We also found treatment duration to predict expressive vocabulary after intervention. This indicated that a longer treatment duration led to a higher expressive vocabulary. Treatment duration neared significance for receptive syntax (p = 0.054). Internalizing behavior, externalizing behavior, parental stress, non-verbal cognitive development and gender did not predict any of the four language domains, when controlling for pre-test scores. For all four language domains, we found that the language pre-test score was a significant predictor for the corresponding language post-test (Table 4). This means that a lower score at the start of the intervention was related to a lower score at the end and higher scores at the start with higher scores at the end. Explained variance (adjusted R2) for the models ranged from 0.30 (expressive syntax) to 0.54 (receptive syntax). For both receptive syntax and receptive vocabulary (adjusted R2 = 0.51), the pre-test score of the respective language measure solely contributed to the height of the explained variance.
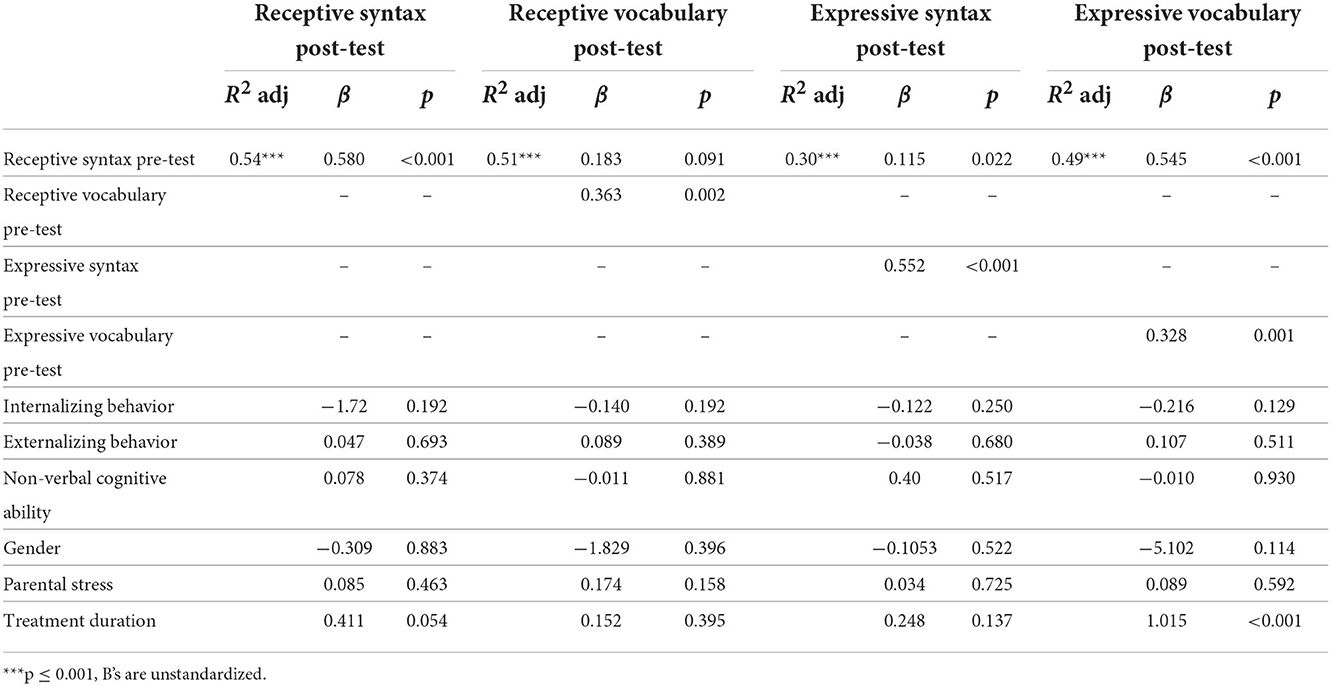
Table 4. Results of the regression analyses with the dependent variables: receptive syntax post-test, receptive vocabulary post-test, expressive syntax post-test and expressive vocabulary post-test.
Discussion
This study examined to what extent child, parental, and treatment factors were predictive for receptive and expressive language outcomes of children with presumed DLD after an early language intervention program. The findings showed that after controlling for pre-test language scores, the only significant predictors were “receptive syntax proficiency” for both expressive measures and “treatment duration” for expressive vocabulary. This indicates that children with lower receptive scores make less progress in both expressive domains. In addition, a shorter treatment duration predicted lower expressive vocabulary post-test scores after controlling for the effects of all other predictors (including pre-test expressive vocabulary scores). This suggests that both receptive syntax scores and treatment duration are important predictors of progress in expressive vocabulary. Internalizing behavior, externalizing behavior, non-verbal cognitive ability, gender and parental stress did not contribute to predicting language development in our study. The findings also showed all pre-intervention language scores predicted the corresponding post-intervention scores: lower scores at the start were related to lower scores at the end.
Both expressive language outcomes were predicted by the scores of the receptive syntax test, as a proxy of receptive language proficiency. Apparently, it is harder to improve these expressive domains with low receptive language proficiency. This is in accordance with the studies of Law et al. (2004) and O'neill et al. (2019), who also found that expressive language is harder to improve in young children with receptive delays. A possible explanation is that receptive language problems increase language learning demands, which makes it more difficult to develop in the expressive domains (Yarian et al., 2021). Children with receptive problems may therefore need different intervention strategies than children with expressive language problems only. The question arises what can be done to help children with receptive problems. Washington et al. (2011), for example, suggest that a rich semantic context might be helpful to treat expressive syntax problems in children with receptive problems. Toys or objects that are familiar to the child could be used by professionals when expressive language is practiced (Washington et al., 2011; Yarian et al., 2021). This may reduce language learning demands and facilitate the acquisition of expressive language for children with receptive problems. Tarvainen et al. (2020) also emphasize the importance of creating an optimal language environment to improve receptive language skills by improving the communication strategies used by significant others.
Treatment duration turned out to be a predictive factor for expressive vocabulary, meaning that a longer treatment duration led to learning more new words. However, treatment duration did not predict the other three language outcomes, although it did near significance for receptive syntax (p < 0.054). These findings support the assumption that the impact of treatment duration may differ between language domains (Zeng et al., 2012; Law et al., 2017). The question arises what might explain this difference? Several explanations may be underlying. First of all, most emphasis of the intervention is on stimulating vocabulary. Maybe, if there would be more emphasis on improving syntax, children may learn more syntactic structures and treatment duration may become of importance for this domain. Second, children have to acquire a certain amount of words before they can start combining words into sentences (Bates and Goodman, 2013). Maybe, expressive syntax improvement was therefore not always possible, because the children first had to learn more words. This is supported by a study of Vermeij et al. (2021), who also found children with presumed DLD showed most progress in expressive vocabulary and least progress in expressive syntax during early intervention. It would be of interest to further study the relation between treatment duration and the language outcomes in a larger study, especially because the relation neared significance for receptive syntax.
Treatment duration not only predicted the expressive vocabulary outcome, but also showed a significant correlation with the expressive vocabulary pre-test (r = −0.22), meaning that a longer treatment duration was related to lower expressive vocabulary scores at intervention start. This shows that children with more severe expressive vocabulary problems pre-intervention received intervention for a longer time period, indicating that children with more severe expressive vocabulary problems were referred sooner for intervention than children with milder problems. It has to be noted that treatment duration showed a high correlation (r = −0.91) with the age of intervention start, meaning that a higher age at intervention start was related to a shorter treatment duration. Because of this high correlation (multicollinearity) it is not possible to unravel the specific contribution of treatment duration and age at onset of treatment.
The other child factors, internalizing behavior, externalizing behavior, non-verbal cognitive ability and gender, did not predict language outcomes, after controlling for language pre-test scores. Apparently, in this study, language outcomes are not influenced by the level of the behavior problems, by more or less advanced non-verbal cognitive abilities of the children or by gender. This means that, for example, children with behavior problems or lower non-verbal cognitive abilities may benefit from treatment in equal ways during the language intervention compared with children without these problems.
Although non-verbal cognitive ability is associated with all four language post-test scores, we did not found non-verbal cognitive ability to predict language outcomes, after controlling for language pre-test scores. This finding is in agreement with our hypothesis, and in line with the study of Yarian et al. (2021), who also found that non-verbal cognitive abilities did not predict language development. This supports the assumption that children with lower cognitive abilities can also benefit of treatment (Bishop et al., 2016). In this study, children with a non-verbal IQ-score below 80 were not included. Therefore, we cannot generalize our findings to these children. It may be that non-verbal cognitive ability only predicts language outcomes if the full range of non-verbal cognitive scores are included. Although we found that non-verbal cognitive ability did not predict language outcomes, it may not be concluded that non-verbal cognitive ability is not important at all, since it is associated with most pre-test language domains at the start of the intervention. A lower non-verbal cognitive ability was associated with lower language scores. This is in accordance with studies of Rice and Hoffman (2015) who also found a lower cognitive ability to be associated with lower language scores in children with DLD. Non-verbal cognitive ability may therefore not have its influence at the progress made during the intervention, but may have its influence at the level of the language score at the start of the intervention.
Gender did not predict language development during the intervention. Apparently, boys and girls benefit the same from the intervention and possible differences in social interaction between boys and girls do not influence language development. It has to be noted that the number of boys in this study was very high compared to the number of girls. Although some studies suggested boys are more at risk of DLD than girls (Tomblin et al., 1997; Leonard, 2014), other studies suggest that the proportion boys vs. girls is more equal (Ukoumunne et al., 2012). However, because boys more often have additional problems and express their social-emotional problems in different ways than girls (Wiefferink et al., 2020), their language problems may be more readily observed and detected (Uilenburg et al., 2018). As a result, diagnosis is set earlier and intervention can be initiated. In our sample, we did not found a significant difference between boys and girls in the age at the start of the intervention or the treatment duration. However, it could still be the case that the more obvious additional difficulties in boys have led to higher rates of diagnosis across the full age range in our study. It could still be that boys are being diagnosed earlier and that a part of the girls in the age range between two to four still have not yet been diagnosed as their difficulties are still hidden.
Parental stress also did not predict language outcomes, after controlling for language pre-test scores. This means that the language development of children of parents with elevated levels of stress developed the same during the intervention compared with children of parents without stress. Maybe, the stress parents experienced had no or less influence on parent-child interaction, because parents also learn techniques how to improve the interaction with their child during the intervention. Another explanation might be that parental stress is not related to the language domains, but to the behavior problems. The bivariate correlations displayed that parental stress did not correlate with any of the language pre-tests and post-test s, except with the pre-test of receptive vocabulary (r = −0.18). Parental stress, however, did show higher correlations with internalizing (r = 0.46) and externalizing behavior (r = 0.56) at pre-test, indicating that higher levels of behavior problems are related to higher levels of parental stress. This relation is supported by several studies (Baker et al., 2003; Neece et al., 2012). It may therefore be that parental stress is especially elevated in parents of children with language problems combined with behavior problems. This would be of interest to investigate further in future studies. It has to be noted that we used a questionnaire that studied parental stress in general. For future studies it might be of importance to study stress related to the language problems of the child and explore if this would lead to different relations between parental stress and language development.
Although the language pre-tests were included in the analyses to enable analysis of the effects of the other predictors on outcome when controlling for pre-test scores, they turned out to be important predictors of outcomes. The results showed that children with lower pre-intervention scores showed relatively lower post-intervention scores in the corresponding language domains. Children with higher scores at intervention start, on the other hand, gained relatively higher scores at the end. Although Chiat and Roy (2008) did not study a specific intervention setting, they also found that language scores in 2;6–3;6 year old children with language problems predicted corresponding language scores when they were between 4 and 5 years old, indicating that early language scores are important predictors for language proficiency later on.
Limitations
This study has some limitations. First, we included treatment duration as an independent variable. Treatment duration, however, is one of several aspects of treatment intensity. Other aspects like dose and dose frequency may also be of importance (Warren et al., 2007). Therefore, when examining the influence of treatment factors in future studies, it may be of interest to take more aspects of treatment intensity into account.
Second, the results of this study are not generalizable to multilingual children and children of parents with a low education level. About 20% of the children visiting the early language intervention center is multilingual. Unfortunately, language test are normed for monolingual Dutch speaking children, and not for multilingual children. This makes the interpretation of language results less reliable which made us decide not to include multilingual children in this study. It also has to be noted that we included a relatively well educated sample. Results therefore can also not be generalized to children of parents with a lower education level. Third, this study used multiple imputation to handle the missing data. Imputing data is advised when 40% or less of the data is missing (Jakobsen et al., 2017). For one of the twelve imputed variables however, namely the post-test of receptive vocabulary, more than 40% of the data was missing. Therefore, in this case, some caution should be adopted with interpreting the data (Jakobsen et al., 2017).
Last, we only took factors into account that are routinely monitored or registered during the intervention. Other factors, like parent-child interaction, home situation, SES or parental involvement may also have its influence on language outcomes, after controlling for language pre-test scores. For future studies it may be of interest to take more of these factors into account.
Conclusion
In this study, we explored to what extent child, parental, and treatment factors were predictive for receptive and expressive language outcomes of children with presumed DLD after an early language intervention program. We found that low receptive syntax proficiency can negatively influence expressive language development. Children with receptive problems may need other intervention strategies to improve language proficiency, such as decreasing language learning demands. These strategies are not necessarily needed for children with expressive problems only. We therefore need to be aware of the difference in language profiles between children with lower and higher receptive scores and tailor the intervention to the specifics needs of a child.
We also found the severity of the language problem at the intervention start to be an important predictor of language outcomes. Lower scores at start led to relatively lower scores post-intervention. This finding supports the importance of early diagnosis and early intervention (Singleton, 2018; Kaiser et al., 2022). The sooner children are diagnosed, the sooner they can start with intervention to stimulate language development.
Data availability statement
The datasets presented in this article are not readily available because research data cannot be shared due to privacy restrictions and lack of permission.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Achenbach, T. M., and Rescorla, L. A. (2000). Manual for the Aseba Preschool Forms and Profiles: An Integrated System of Multi-Informant Assessment; Child Behavior Checklist For Ages 1 1/2-5; Language Development Survey; Caregiver-Teacher Report Form. Burlington, VT: University of Vermont.
Baker, B. L., Mcintyre, L. L., Blacher, J., Crnic, K., Edelbrock, C., and Low, C. (2003). Pre-school children with and without developmental delay: behaviour problems and parenting stress over time. J. Intellect. Disabil. Res. 47, 217–230. doi: 10.1046/j.1365-2788.2003.00484.
Bates, E., and Goodman, J. C. (2013). On the emergence of grammar from the lexicon. In The emergence of language Psychology Press. 47–98.
Bickman, L., Lyon, A. R., and Wolpert, M. (2016). Achieving precision mental health through effective assessment, monitoring, and feedback processes introduction. Admin. Policy Mental Health Mental Health Serv. Res. 43, 271–276. doi: 10.1007/s10488-016-0718-5
Bishop, D. V. (2017). Why is it so hard to reach agreement on terminology? The case of developmental language disorder (Dld). Int. J. Lang. Commun. Disord. 52, 671–680. doi: 10.1111/1460-6984.12335
Bishop, D. V., Snowling, M. J., Thompson, P. A., Greenhalgh, T., Consortium, C., Adams, C., et al. (2017). Phase 2 of catalise: a multinational and multidisciplinary delphi consensus study of problems with language development: terminology. J. Child Psychol. Psychiatry 58, 1068–1080. doi: 10.1111/jcpp.12721
Bishop, D. V. M., Snowling, M. J., Thompson, P. A., Greenhalgh, T., and Consortium, C. (2016). Catalise: a multinational and multidisciplinary delphi consensus study. identifying language impairments in children. PLoS ONE 11, E0158753. doi: 10.1371/journal.pone.0158753
Bowyer-Crane, C., Snowling, M. J., Duff, F., and Hulme, C. (2011). Response to early intervention of children with specific and general language impairment. Learn. Disabil. Contemp. J. 9, 107–121.
Boyle, J., Mccartney, E., Forbes, J., and O'hare, A. (2007). A randomised controlled trial and economic evaluation of direct vs. indirect and individual vs. group modes of speech and language therapy for children with primary language impairment. Health Technol. Assess. 11, Iii. doi: 10.3310/hta11250
Boyle, J., Mccartney, E., O'hare, A., and Law, J. (2010). Intervention for mixed receptive-expressive language impairment: a review. Dev. Med. Child Neurol. 52, 994–999. doi: 10.1111/j.1469-8749.2010.03750.x
Camarata, S. M., and Nelson, K. E. (2006). Conversational Recast Intervention with Preschool and Older Children. In Treatment of language disorders in children, eds, R. J. McCauley and M. E. Fey Eds, (Brookes Publishings) 237–264.
Chiat, S., and Roy, P. (2008). Early phonological and sociocognitive skills as predictors of later language and social communication outcomes. J. Child Psychol. Psychiatry 49, 635–645. doi: 10.1111/j.1469-7610.2008.01881.x
Coleman, P. K., and Karraker, K. H. (1997). Self-efficacy and parenting quality: findings and future applications. Dev. Rev. 18, 47–85.
Curtis, P. R., Frey, J. R., Watson, C. D., Hampton, L. H., and Roberts, M. Y. (2018). Language disorders and problem behaviors: a meta-analysis. Pediatrics 142, e20173551. doi: 10.1542/peds.2017-3551
De Beurs, E. D., Den Hollander-Gijsman, M. E., Van Rood, Y. R., Van Der Wee, N. J., Giltay, E. J., Van Noorden, M. S., et al. (2011). Routine outcome monitoring in the netherlands: practical experiences with a web-based strategy for the assessment of treatment outcome in clinical practice. Clin. Psychol. Psychother. 18, 1–12. doi: 10.1002/cpp.696
Dionne, G., Tremblay, R., Boivin, M., Laplante, D., and Pérusse, D. (2003). Physical aggression and expressive vocabulary in 19-month-old twins. Dev. Psychol. 39, 261. doi: 10.1037/0012-1649.39.2.261
Duncan, B. L., Miller, S. D., Wampold, B. E., and Hubble, M. A. (2010). The Heart and Soul of Change: Delivering What Works in Therapy. Washington, DC: American Psychological Association. doi: 10.1037/12075-000
Dunn, L. M., Dunn, L. M., and Schlichting, J. E. P. T. (2005). Peabody Picture Vocabulary Test-Iii-Nl. Amsterdam: Harcourt Test Publishers.
Fey, M. E., Finestack, L., and Long, S. (2003). Ten principles of grammar facilitation for children with specific language impairments. Am. J. Speech-Lang. Pathol. 12, 48. doi: 10.1044/1058-0360(2003/048)
Gallinat, E., and Spaulding, T. J. (2014). Differences in the performance of children with specific language impairment and their typically developing peers on non-verbal cognitive tests: a meta-analysis. J. Speech Lang. Hear. Res. 57, 1363–1382. doi: 10.1044/2014_JSLHR-L-12-0363
Girard, L.-C., Pingault, J.-B., Doyle, O., Falissard, B., and Tremblay, R. E. (2016). Developmental associations between conduct problems and expressive language in early childhood: a population-based study. J. Abnormal Child Psychol. 44, 1033–1043. doi: 10.1007/s10802-015-0094-8
Green, B. C., Johnson, K. A., and Bretherton, L. (2014). Pragmatic language difficulties in children with hyperactivity and attention problems: an integrated review. Int. J. Lang. Commun. Disord. 49, 15–29. doi: 10.1111/1460-6984.12056
Heidlage, J. K., Cunningham, J. E., Kaiser, A. P., Trivette, C. M., Barton, E. E., Frey, J. R., et al. (2020). The effects of parent-implemented language interventions on child linguistic outcomes: a meta-analysis. Early Childhood Res. Q. 50, 6–23. doi: 10.1016/j.ecresq.2018.12.006
Horwitz, S. M., Irwin, J. R., Briggs-Gowan, M. J., Heenan, J. M. B., Mendoza, J., and Carter, A. S. (2003). Language delay in a community cohort of young children. J. Am. Acad. Child Adolescent Psychiatry 42, 932–940. doi: 10.1097/01.CHI.0000046889.27264.5E
Jakobsen, J. C., Gluud, C., Wetterslev, J., and Winkel, P. (2017). When and how should multiple imputation be used for handling missing data in randomised clinical trials: a practical guide with flowcharts. BMC Med. Res. Methodol. 17, 1–10. doi: 10.1186/s12874-017-0442-1
Kaiser, A. P., Chow, J. C., and Cunningham, J. E. (2022). A case for early language and behavior screening: implications for policy and child development. Policy Insights Behav. Brain Sci. 9, 120–128. doi: 10.1177/23727322211068886
Kruythoff-Broekman, A., Wiefferink, C., Rieffe, C., and Uilenburg, N. (2019). Parent-implemented early language intervention programme for late talkers: parental communicative behaviour change and child language outcomes at 3 and 4 years of age. Int. J. Lang. Commun. Disord. 54, 451–464. doi: 10.1111/1460-6984.12451
Law, J., Dennis, J. A., and Charlton, J. J. (2017). Speech and language therapy interventions for children with primary speech and/or language disorders. Cochrane Database Syst. Rev. 2017, 4758. doi: 10.1002/14651858.CD012490
Law, J., Garrett, Z., and Nye, C. (2004). The efficacy of treatment for children with developmental speech and language delay/disorder: a meta-analysis. J. Speech Lang. Hear. Res. 47, 924–943. doi: 10.1044/1092-4388(2004/069)
Leonard, L. B. (2014). Children With Specific Language Impairment. Massachusetts: Mit Press. doi: 10.7551/mitpress/9152.001.0001
Maggio, V., Granana, N. E., Richaudeau, A., Torres, S., Giannotti, A., and Suburo, A. M. (2014). Behavior problems in children with specific language impairment. J. Child Neurol. 29, 194–202. doi: 10.1177/0883073813509886
Mckay, J. M., Pickens, J., and Stewart, A. L. (1996). Inventoried and observed stress in parent-child interactions. Curr. Psychol. 15, 223–234.
Mckean, C., Reilly, S., Bavin, E. L., Bretherton, L., Cini, E., Conway, L., et al. (2017). Language outcomes at 7 years: early predictors and co-occurring difficulties. Pediatrics 139, e20161684. doi: 10.1542/peds.2016-1684
Morgan, P. L., Farkas, G., Hillemeier, M. M., Hammer, C. S., and Maczuga, S. (2015). 24-month-old children with larger oral vocabularies display greater academic and behavioral functioning at kindergarten entry. Child Dev. 86, 1351–1370. doi: 10.1111/cdev.12398
Neece, C. L., Green, S. A., and Baker, B. L. (2012). Parenting stress and child behavior problems: a transactional relationship across time. Ajidd-Am. J. Intellect. Dev. Disabil. 117, 48–66. doi: 10.1352/1944-7558-117.1.48
Norbury, C. F., Gooch, D., Wray, C., Baird, G., Charman, T., Simonoff, E., et al. (2016). The impact of non-verbal ability on prevalence and clinical presentation of language disorder: evidence from a population study. J. Child Psychol. Psychiatry 57, 1247–1257. doi: 10.1111/jcpp.12573
Nouraey, P., Ayatollahi, M. A., and Moghadas, M. (2021). Late language emergence: a literature review. Sultan Qaboos Univ. Med. J. 21, E182. doi: 10.18295/squmj.2021.21.02.005
O'neill, H., Murphy, C.-A., and Chiat, S. (2019). What our hands tell us: a 2-year follow-up investigating outcomes in subgroups of children with language delay. J. Speech Lang. Hear. Res. 62, 356–366. doi: 10.1044/2018_JSLHR-L-17-0261
Paul, R., and Norbury, C. F. (2012). Language Disorders from Infancy Through Adolescence. Amsterdam: Elsevier
Pepper, J., and Weitzman, E. (2004). It Takes Two to Talk: A Practical Guide for Parents of Children With Language Delays. Toronto: The Hanen Centre.
Petersen, I. T., Bates, J. E., D'onofrio, B. M., Coyne, C. A., Lansford, J. E., Dodge, K. A., et al. (2013). Language ability predicts the development of behavior problems in children. J. Abnorm. Psychol. 122, 542–557. doi: 10.1037/a0031963
Rennecke, L., Ronniger, P., Petermann, F., and Melzer, J. (2019). Developmental language disorder: maternal stress level and behavioural difficulties of children with expressive and mixed receptive-expressive dld. J. Commun. Disord. 80, 1–10. doi: 10.1016/j.jcomdis.2019.03.006
Rice, M. L., and Hoffman, L. (2015). Predicting vocabulary growth in children with and without specific language impairment: a longitudinal study from 2; 6 to 21 years of age. J. Speech Lang. Hear. Res. 58, 345–359. doi: 10.1044/2015_JSLHR-L-14-0150
Salmon, K., O'kearney, R., Reese, E., and Fortune, C.-A. (2016). The role of language skill in child psychopathology: implications for intervention in the early years. Clin. Child Fam. Psychol. Rev. 19, 352–367. doi: 10.1007/s10567-016-0214-1
Santelices, M.-P., and Cortés, P. A. (2022). Mentalization and parental stress: how do they predict mother–child interactions? Children 9, 280. doi: 10.3390/children9020280
Schaunig, I., Willinger, U., Diendorfer-Radner, G., Hager, V., Jorgl, G., Sirsch, U., et al. (2004). Parenting stress index and specific language impairment. Praxis Der Kinderpsychologie Und Kinderpsychiatrie 53, 395–405.
Schlichting, J., and Lutje Spelberg, H. (2010a). Schlichting Test Voor Taalbegrip. Houten: Bohn Stafleu Van Loghum.
Schlichting, J., and Lutje Spelberg, H. (2010b). Schlichting Test Voor Taalproductie-Ii. Houten: Bohn Stafleu Van Loghum.
Segura-Pujol, H., and Briones-Rojas, C. (2021). Treatment intensity for developmental language disorder: a systematic review. Int. J. Speech-Lang. Pathol. 23, 465–474. doi: 10.1080/17549507.2020.1856412
Shalev, R. A., Lavine, C., and Di Martino, A. (2020). A systematic review of the role of parent characteristics in parent-mediated interventions for children with autism spectrum disorder. J. Dev. Phys. Disabil. 32, 1–21. doi: 10.1007/s10882-018-9641-x
Short, K., Eadie, P., and Kemp, L. (2020). Influential factor combinations leading to language outcomes following a home visiting intervention: a qualitative comparative analysis (Qca). Int. J. Lang. Commun. Disord. 55, 936–954. doi: 10.1111/1460-6984.12573
Singleton, N. C. (2018). Late talkers: why the wait-and-see approach is outdated. Pediatric Clin. 65, 13–29. doi: 10.1016/j.pcl.2017.08.018
Snowling, M. J., Bishop, D. V. M., Stothard, S. E., Chipchase, B., and Kaplan, C. (2006). Psychosocial outcomes at 15 years of children with a preschool history of speech-language impairment. J. Child Psychol. Psychiatry 47, 759–765. doi: 10.1111/j.1469-7610.2006.01631.x
St Clair, M. C., Pickles, A., Durkin, K., and Conti-Ramsden, G. (2011). A longitudinal study of behavioral, emotional and social difficulties in individuals with a history of specific language impairment (Sli). J. Commun. Disord. 44, 186–199. doi: 10.1016/j.jcomdis.2010.09.004
Strauss, K., Vicari, S., Valeri, G., D'elia, L., Arima, S., and Fava, L. (2012). Parent inclusion in early intensive behavioral intervention: the influence of parental stress, parent treatment fidelity and parent-mediated generalization of behavior targets on child outcomes. Res. Dev. Disabil. 33, 688–703. doi: 10.1016/j.ridd.2011.11.008
Tarvainen, S., Stolt, S., and Launonen, K. (2020). Oral language comprehension interventions in 1–8-year-old children with language disorders or difficulties: a systematic scoping review. Autism Dev. Lang. Impairm. 5, 2396941520946999. doi: 10.1177/2396941520946999
Taylor, C. L., Christensen, D., Lawrence, D., Mitrou, F., and Zubrick, S. R. (2013). Risk factors for children's receptive vocabulary development from 4 to 8 years in the longitudinal study of Australian children. PLoS ONE 8, E73046. doi: 10.1371/annotation/a730446c-0150-4079-98ea-95b12e1e3c28
Tellegen, P., Winkel, M., Wijnberg-Williams, B., and Laros, J. (1998). “Snijders-oomen niet-verbale intelligentietest son-R 2,5-7,” in Handleiding En Verantwoording [Snijders–Oomen Non-verbal Intelligence Test: Son-R 2.5-7 Manual And Justification]. Lisse: Swets.
Tomblin, J. B., Records, N. L., Buckwalter, P., Zhang, X., Smith, E., and O'brien, M. (1997). Prevalence of specific language impairment in kindergarten children. J. Speech Lang. Hear. Res. 40, 1245–1260.
Uilenburg, N., Wiefferink, K., Verkerk, P., Van Denderen, M., Van Schie, C., and Oudesluys-Murphy, A.-M. (2018). Accuracy of a screening tool for early identification of language impairment. J. Speech Lang. Hear. Res. 61, 1–10. doi: 10.1044/2017_JSLHR-L-16-0173
Ukoumunne, O., Wake, M., Carlin, J., Bavin, E., Lum, J., Skeat, J., et al. (2012). Profiles of language development in pre-school children: a longitudinal latent class analysis of data from the early language in victoria study. Child Care Health Dev. 38, 341–349. doi: 10.1111/j.1365-2214.2011.01234.x
Vallotton, C., Harewood, T., Ayoub, C., Pan, B., Mastergeorge, A., and Brophy-Herb, H. (2012). Buffering boys and boosting girls: the protective and promotive effects of early head start for children's expressive language in the context of parenting stress. Early Childhood Res. Q. 27, 695–707. doi: 10.1016/j.ecresq.2011.03.001
Van Berkel-Van Hoof, L., Hermans, D., Knoors, H., and Verhoeven, L. (2019). Effects of signs on word learning by children with developmental language disorder. J. Speech Lang. Hear. Res. 62, 1798–1812. doi: 10.1044/2019_JSLHR-L-18-0275
Van Sonsbeek, M., Hutschemaekers, G., Veerman, J. W., and Tiemens, B. B. G. (2014). Effective components of feedback from routine outcome monitoring (ROM) in youth mental health care: study protocol of a three-arm parallel-group randomized controlled trial. BMC Psychiatry 14, 1–11. doi: 10.1186/1471-244X-14-3
Verhulst, F. C., and Van Der Ende, J. (2001). Child Behavior Checklist for Ages 1,5-5, Dutch Translation. Rotterdam: Erasmus Mc.
Vermeij, B. A., Wiefferink, C. H., Scholte, R. H., and Knoors, H. (2021). Language development and behaviour problems in toddlers indicated to have a developmental language disorder. Int. J. Lang. Commun. Disord. 56, 1249–1262. doi: 10.1111/1460-6984.12665
Vermulst, A. A., Kroes, G., De Meyer, R. E., Nguyen, L., and Veerman, J. W. (2015). Handleiding Obvl [Manual Psq]. Nijmegen: Praktikon Bv.
Wang, M. V., Aarø, L. E., and Ystrom, E. (2018). Language delay and externalizing problems in preschool age: a prospective cohort study. J. Abnorm. Child Psychol. 46, 923–933. doi: 10.1007/s10802-017-0391-5
Warren, S. F., Fey, M. E., and Yoder, P. J. (2007). Differential treatment intensity research: a missing link to creating optimally effective communication interventions. Mental Retard. Dev. Disabil. Res. Rev. 13, 70–77. doi: 10.1002/mrdd.20139
Washington, K. N., Warr-Leeper, G., and Thomas-Stonell, N. (2011). Exploring the outcomes of a novel computer-assisted treatment program targeting expressive-grammar deficits in preschoolers with sli. J. Commun. Disord. 44, 315–330. doi: 10.1016/j.jcomdis.2011.01.002
Wiefferink, C. (2021). Databank Effectieve Jeugdinterventies: Beschrijving ‘Methodiek Tos'. Utrecht: Nederlands Jeugdinstituut. Available online at: www.Nji.Nl/Jeugdinterventies (accessed March 17, 2022).
Wiefferink, K., Van Beugen, C., Wegener Sleeswijk, B., and Gerrits, E. (2020). Children with language delay referred to dutch speech and hearing centres: caseload characteristics. Int. J. Lang. Commun. Disord. 55, 573–582. doi: 10.1111/1460-6984.12540
Yarian, M., Washington, K. N., Spencer, C. E., Vannest, J., and Crowe, K. (2021). Exploring predictors of expressive grammar across different assessment tasks in preschoolers with or without dld. Commun. Disord. Q. 42, 111–121. doi: 10.1177/1525740119868238
Yew, S. G. K., and O'kearney, R. (2015a). Early language impairments and developmental pathways of emotional problems across childhood. Int. J. Lang. Commun. Disord. 50, 358–373. doi: 10.1111/1460-6984.12142
Yew, S. G. K., and O'kearney, R. (2015b). The role of early language difficulties in the trajectories of conduct problems across childhood. J. Abnorm. Child Psychol. 43, 1515–1527. doi: 10.1007/s10802-015-0040-9
Yew, S. G. K., and O'kearney, R. (2017). Language difficulty at school entry and the trajectories of hyperactivity-inattention problems from ages 4 to 11: evidence from a population-representative cohort study. J. Abnorm. Child Psychol. 45, 1105–1118. doi: 10.1007/s10802-016-0241-x
Keywords: developmental language disorder, receptive language proficiency, behavior problems, non-verbal cognitive ability, gender, parental stress, treatment duration
Citation: Vermeij BAM, Wiefferink CH, Scholte RHJ and Knoors H (2022) Predictors in language proficiency of young children with presumed developmental language disorder within the setting of early language intervention. Front. Commun. 7:1011175. doi: 10.3389/fcomm.2022.1011175
Received: 03 August 2022; Accepted: 28 November 2022;
Published: 15 December 2022.
Edited by:
David Saldaña, Sevilla University, SpainReviewed by:
Sheena Reilly, Griffith University, AustraliaLisa Archibald, Western University, Canada
Susan Ebbels, Moor House School and College, United Kingdom
Copyright © 2022 Vermeij, Wiefferink, Scholte and Knoors. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bernadette A. M. Vermeij, bvermeij@nsdsk.nl