 Diyako Rahmani
Diyako Rahmani Cheng Zeng
Cheng Zeng Ali Moazami Goodarzi3
Ali Moazami Goodarzi3 Farhad Vahid
Farhad Vahid
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Commun., 08 February 2021
Sec. Health Communication
Volume 6 - 2021 | https://doi.org/10.3389/fcomm.2021.560451
This article is part of the Research TopicCoronavirus Disease (COVID-19): Pathophysiology, Epidemiology, Clinical Management and Public Health ResponseView all 400 articles
This study investigates the impact of anxiety, productivity, and individual characteristics on employee compliance in an Iranian medical science university during the COVID-19 outbreak. The data of 160 healthcare employees of various professions were collected with reliability and validity on the measurements performed. Two regression tests revealed that higher anxiety reduces and higher productivity increased compliance. Participants with higher education and non-medical professions were found to have higher compliance. Productivity was also found to be positively associated with tenure and having a medical position. Implication and limitation are discussed.
Coronavirus has already had enormous effects on almost all aspects of human life. The widespread of this virus since the beginning of 2020 has faced many healthcare organizations and systems worldwide with unprecedented pressure to the point of collapse. Therefore, organizational integrity and the elements related to healthcare organizational culture have become even more crucial than before in the global fight against the Coronavirus. Organizational compliance, the level of adherence to the organizational regulations, procedure, and standards (Gershon et al., 1995), is considered an essential organizational culture element (Gershon et al., 1999) with a significant role in maintaining organizational integrity.
Organizational compliance could be affected and hindered by social and organizational crises, which, in turn, can influence organizations’ output and functionality. For example, as evident in the case of recent infectious diseases such as SARS and MERS, previous studies showed that medical staff’s lack of adherence to treatment protocols contributed to the failure of the fight against pandemics (McCarthy et al., 2016; Smith et al., 2016; Adeniyi et al., 2018). Thus, to develop the current understanding of organizational compliance during crises, this study looks at the effect of two significant constructs of anxiety and productivity on compliance.
Anxiety creates affective and cognitive deterrence and interferes with employee judgment (Barlow, 1991), and causes uncertainty, helplessness, and physiological arousal (Grupe and Nitschke, 2013). Various forms of anxiety are known for their behavioral impacts (Rahmani, 2017). Productivity, perceived as the employees’ efficiency (Drewnowski, 2019), affects employee self-efficacy, the perception of being able to accomplish a specific task (Bandura, 1994). Thus, both anxiety and organizational productivity could affect compliance in organizations. Furthermore, similar to other organizational factors, compliance could be affected by individual characteristics such as gender, tenure, education, and individual characteristics such as smoking, overweighing, and stress (O’Reilly and Chatman, 1986; Gershon et al., 1995).
Contextually, this study focuses on a medical science university in the Markazi province of Iran. As one of the worse hit countries by the pandemic, Iran is a significant case study that could contribute to our understanding of the global challenges induced by the Covid-19. Previous studies showed that responding to the pandemic, Iranians showed a higher level of anxiety than the Chinese (Jahanshahi et al., 2020). Furthermore, the level of anxiety among the Iranian general public is directly associated with infection levels in the regions and provinces (Moghanibashi-Mansourieh, 2020). While almost the entire country was heavily affected by the disease, this study investigates a healthcare organization in Markazi province, one of the first epicenters of the diseases in Iran (Arab-Mazar et al., 2020).
Furthermore, as the healthcare staff’s efficiency proved to be distinctive in reducing the disease toll across the globe, an organizational approach to the pandemic’s consequences is of eminent significance. According to the World Health Organization, about 20–60% of staff and medical staff are infected with the virus; for example, in Italy, 20% of responding healthcare employees were infected (Lancet, 2020). Recent research showed that a sizeable portion of healthcare staff in Iran needs emotional and psychological support due to anxiety and distress resulting from Covid-19 (Zhang et al., 2020). Thus, it is crucial to investigate the impact of anxiety on various aspects of organizational culture and performance in an Iranian healthcare organization.
As one of the most widely used and cited health promotion models, Precede-Proceed provides concrete steps to facilitate individual health behavior changes. Essentially, the Precede-Proceed model posits that health behavior not only is driven by knowledge, beliefs, and attitudes but also needs to be enabled and reinforced (Green and Kreuter, 1991). The Precede component refers to the diagnostic and assessment phases that aim to identify health problems, existing resources, and risk factors. In contrast, Proceed stages involve intervention implementation and evaluation of the process and health outcomes and their long-term ramifications in the community (Ransdell, 2001). Highlighting people’s interactive nature and their environment, the Precede-Proceed model allows for a comprehensive approach to decipher the complexity in individual health behavior and design the most effective intervention programs.
In the past, the Precede-Proceed model has been adopted as a framework to improve heart-healthy behaviors among low-income citizens (Paradis et al., 1995), decrease children injuries (Gielen and McDonald, 1997), increase youth physical activity (Welk, 1999), improve asthma educational programs (Chiang et al., 2004), and so on. In the current study, the Precede-Proceed model serves as the theocratical basis for exploring how risk factors at the individual level influence one’s compliance in Iran’s unique cultural setting during the COVID-19 pandemic. The study’s findings will help advance our knowledge of health professionals’ organizational behaviors and provide insight into how we can better protect frontline workers during the time of significant uncertainties.
Within the broader organizational context, compliance is defined as “a state of accordance between an actor’s behaviour or products on the one side, and predefined explicit rules, procedures, conventions, standards, guidelines, principles, legislation or other norms on the other” (Foorthuis and Bos, 2011, p. 261). Organizational compliance can be reflective, i.e. self-conscious, or non-reflective, i.e. non-self-conscious (Paulsen, 2016). Compliance, or interchangeably adherence, within the healthcare context, is defined as doing or avoiding behaviors as recommended by healthcare professionals in individual (e.g. doctors) or general (e.g. public service announcement) levels to improve the quality and status of one’s health condition (Martin, 2014). Information, motivation, and strategy are the necessary elements of successful compliance (DiMatteo et al., 2012).
Employees’ compliance with organizational rules and regulations is perceived to be impacted by and, at the same time, an indicator of organizational culture (Hu et al., 2012). Investigation of compliance within healthcare organizations showed that strong and effective leadership is an essential element in healthcare professionals’ hygiene compliance during the spread of infectious diseases (De Bono et al., 2014). Emphasizing and monitoring compliance via ethical programs lead to the lower cases of unethical conduct, increased ethical advice, seeking and ethical awareness in the organizations (Weaver and Treviño, 1999).
Previous studies of compliance have studied patients’ compliance and adherence. Such studies, for example, showed that poor compliance to medical care increases the risk of health outcomes (Karvinen et al., 2013), and compliance among cancer patients could be disrupted due to the psychological or behavioral effects of the treatment procedure (Andersen et al., 1994).
Previous research on healthcare employees’ compliance investigated the precedents and outcomes of compliance in the healthcare facilities. Carthey et al. (2011) indicated that information overload causes non-compliance in the United Kingdom’s National Health Service (NHS). Flodgren et al. (2019) concluded that the local opinion leaders’ interventions, alone or in combination with other interventions, can increase compliance among healthcare professionals. Another study showed that organizational feedback and personalized action plan could increase hand-hygiene compliance (Fuller et al., 2012). Increased compliance with antidepressant therapy is correlated with reduced absenteeism costs among healthcare employees (Birnbaum et al., 2010).
Anxiety occurs when a person’s stressful life conditions become too long or frequent. If the body’s nervous system fails to endure the stress resistance phase and the body remains under pressure for a long time, it will be worn out and become vulnerable to physical and mental illness, such as anxiety (Barlow, 1991). The causes of anxiety are divided into four categories (Barlow, 1991): first, biological and physical factors such as the levels of some hormones in the blood; second, genetic and hereditary factors; third, morbid anxiety, the tendency of the nervous system to decrease the amount of excitement of condensed instincts; and fourth, environmental and social factors such as family problems, feelings of separation and rejection, or sudden and unexpected changes, such as earthquakes, illness, and death of a loved one. Anxiety and worrying can cause physical symptoms such as palpitations, shortness of breath, tremors, sweating, feeling tightness and muscle tension, decreased concentration, and insomnia.
Previous studies of anxiety and stress concerning organizational compliance showed that the higher levels of compliance with medical care indicated less stress measured by heart rate variability (Karvinen et al., 2013). Gershon et al. (1999) indicated that anxiety at the workplace could reduce organizational compliance. Healthcare employees are high-risk groups during the prevalence of infectious diseases and are more prone to mental disorders such as anxiety due to high awareness, changing working hours, insufficient rest, and other factors (Ciorlia and Zanetta, 2005; Huttunen and Syrjänen, 2014). Covid-19 is a pandemic with an unprecedented impact on healthcare organizations, which has increased anxiety and distress among healthcare staff (Zhang et al., 2020). The following hypothesis is proposed to investigate the possible effect of anxiety on healthcare staff’s compliance:
H1. The higher level of anxiety reduces organizational compliance of healthcare employees
Workplace productivity is defined in terms of absenteeism i.e. taking workdays off, and presenteeism i.e. reduced performance, measured using work disability, work loss, and work limitation (Drewnowski, 2019). Lofland et al. (2004) added compensation to absenteeism and presenteeism to measure productivity. Two approaches to human capital and friction cost are used to measure the components of productivity. In the first method, monetary value is assigned to lost productivity, while the second approach associates frequency, length, and cost of friction with the friction period (Lofland et al., 2004). Moon et al. (2012) proposed that organizational productivity, synonymous with efficiency, could be measured by the overall output of a specific number of employees based on a fixed amount of input.
Previous organizational healthcare research has generally approached productivity as an outcome of the research (Riedel et al., 2001). For example, employees with a higher Body Mass Index (BMI) and employees with sleep disturbance were less productive (Gates et al., 2008; Rosekind et al., 2010). Riedel et al. (2001) proposed a healthcare organizational productivity model to increase productivity and reduce costs. In this model, disease prevention, health promotion, acute and chronic illness management, environmental health and safety, and health corporate culture are the model’s antecedents. The antecedents’ impact is mediated by reduced absenteeism, improved performance, creativity and motivation, reduced accident and saving costs, and reduced healthcare cost.
While the possible effect of productivity on compliance with workplace precautions is understudied, some previous research included productivity and compliance as study variables. A study of medical adherence to workplace productivity among Asthma patients did not reveal a significant impact on the total health-related quality of life (Joshi et al., 2006). A study of the association between preventive service compliance, productivity, and employee dental claim showed that those with preventive dental claims showed higher compliance and productivity; however, the study did not directly link productivity and compliance (Burton et al., 2017).
Previous organizational compliance studies confirmed the impact of cognitive processes on employees’ compliance with organizational regulation (Carthey et al., 2011; Flodgren et al., 2019). Perception of self-productivity in the organization could impact one’s role in the organization and how one is competent in the organizational culture. As compliance is a manifestation of organizational culture (Hu et al., 2012), we propose the following hypothesis to investigate the impact of productivity on organizational compliance:
H2: Productivity increases organizational compliance.
Previous studies showed that individual factors such as gender, tenure, profession, and education could be correlated with compliance (Gershon et al., 1995). Gershon et al. (1995) found a difference in the compliance level based on profession and education, but they did not find a difference based on gender and tenure in their United States healthcare employee sample. As culturally, Iran is considered to be higher in masculinity and power difference than the United States (Farzianpour et al., 2016), it is possible that gender and tenure also affect compliance among the Iranian healthcare employees. Masculine cultures strive to distinguish between how men and women are expected to think and behave, and power difference refers to the accepted and expected inequality in power distribution (Liu et al., 2019). Moreover, in another study, tenure was found to negatively correlate with compliance, which shows that while newer employees develop their relationship with their organization based on compliance, over time, internalization of organization goals and values and pride in affiliation may develop instead (O’Reilly and Chatman, 1986). Along with personal characteristics, individual risk factors such as smoking, experiencing a high level of stress, overweighing, and being at risk at the workplace, (e.g. having direct contact with COVID-19 patients) can affect compliance with organizational regulations in healthcare services (Gershon et al., 1995; Gershon et al., 1999). The following hypotheses are proposed to investigate these possibilities:
H3: Organizational compliance level differs based on personal characteristics (including gender, tenure, profession, and education).
H4: Organizational compliance level differs based on individual risk factors (including smoking, taking stress medicine, weight, and direct contact with COVID-19 patients).
In addition to compliance, productivity could also be associated with the individual (risk) factors. Previous studies showed personal risk factors, such as smoking and overweight, cause illnesses, increase absenteeism, and reduce productivity (Riedel et al., 2001). Regarding tenure, previous research showed contradictory findings. While more tenured staff are more likely to control their negative emotions and engage in less counterproductive behaviors, it is also possible that the power and influence related to their long tenure lessen their conformity at work (Ng and Feldman, 2010). Thus, the following research questions are presented to understand the possible impact of personal factors on organizational productivity:
RQ3: Do personal characteristics (including gender, tenure, profession, and education) impact organizational productivity?
RQ4: Do individual risk factors (including smoking, taking stress medicine, weight, and direct contact with COVID-19 patients) impact organizational productivity?
Figure 1 illustrates the relational study model.
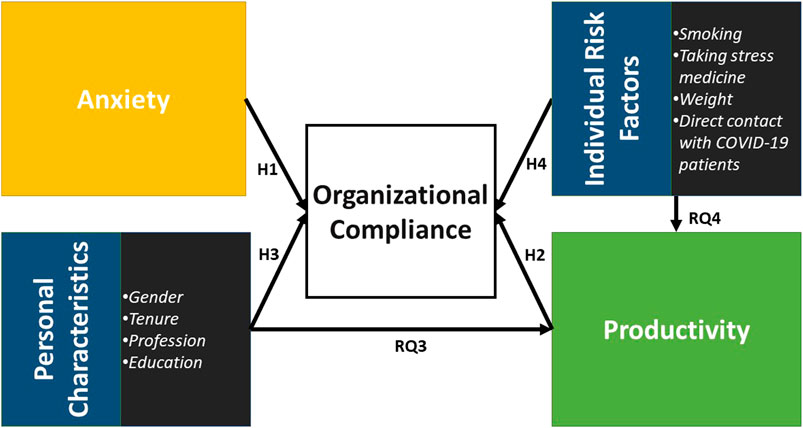
FIGURE 1. The study model.
Firstly, the scales’ construct validity was established by examining their factor structure using confirmatory factor analysis (CFA). We relied on several fit indices to ascertain the model fit, including the comparative fit index (CFI), Tucker Lewis index (TLI), the root mean square error of approximation (RMSEA), and the standardized root mean square residual (SRMR). “Good fit,” in terms of CFI and TLI values means greater than 0.90, while RMSEA and SRMR should ideally be less than 0.08 (Hu and Bentler, 1999). Convergent validity of the constructs was measured using Average Variance Extracted (AVE), which should be higher than 0.5 (Hair et al., 2014). Also, two hierarchical multiple regressions were conducted with compliance and productivity as the dependent variables. For compliance, demographic variables, including income, gender, tenure, and education, were entered at stage one of the regression to control for background characteristics. Dummy variables are used to measure the categorical variables’ effect with more than two categories, and different sets of dummy variables should be added to the regression models at different stages (Field, 2009). Thus, the dummy variables related to profession were added at the second level. The individual risk factors, including taking stress medication, direct contact with COVID-19 patients, BMI, and smoking habits, were added to the third model. Finally, model four was formed using anxiety and productivity. The first three models were replicated for productivity. Data management and statistical analysis were performed using SPSS version 25.0 (SPSS Inc., Chicago, Illinois).
Participants were 160 employees of a medical university in the city of Arak in central Iran, one of the country’s initial epicenters of COVID-19. The university consists of different medical and educational sections and is responsible for planning and implementing medical services in the region. Following the ethic committee approval by the university (research ethic code: IR.ARAKMU.REC.1398.330), this study used self-report questionnaires to collect participants’ gender (male or female), age, profession (the type of occupation at the university), education (the last achieved educational degree), financial condition (monthly income in Iranian rial) and individual risk factors (i.e. smoking habit, Body Mass Index (BMI), taking stress medication and direct contact with the COVID-19 patients). The questionnaire was uploaded to Google Forms, and the link to the survey was distributed using organizational email lists. To ensure the validity of translation, the Farsi draft of the questionnaire items was translated back to English by two different translators and compared with the original English items. The information on the participants is presented in Table 1.
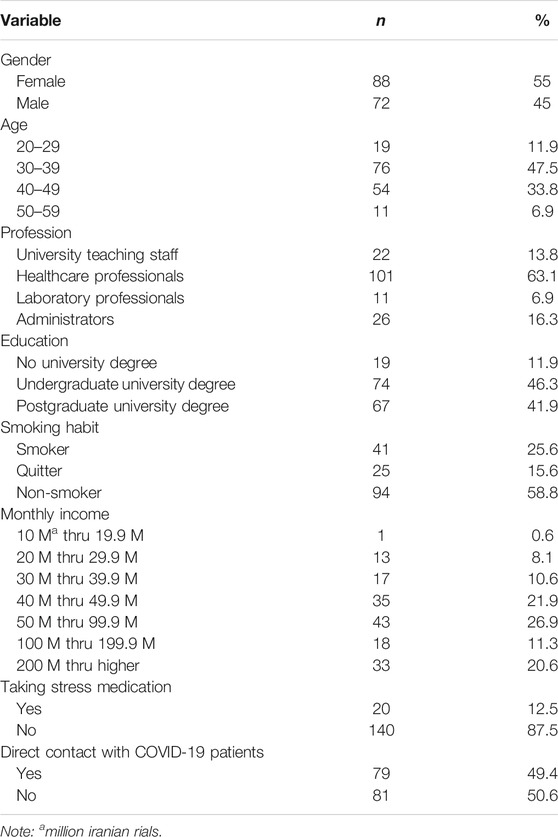
TABLE 1. Participant demographics.
Anxiety was measured by six descriptive symptoms of anxiety (e.g., “unable to relax”) derived from the scale developed and validated by Beck et al. (1988). All items were scored on a seven-point scale, ranging from ‘1 = have not had at all’ to ‘7 = Have had too much to bear’. The Cronbach’s alphas for this scale was 0.89. Also, CFA results revealed that despite the slightly high RMSEA, the six-item model showed a satisfactory model fit (chi2(9) = 21.2; CFI = 0.97; TLI = 0.96; RMSEA = 0.09; SRMR = 0.02), indicating the acceptable construct validity of the scale. AVE for anxiety was 0.6, which reflects the convergent validity of this construct.
Compliance was measured by eight items (e.g., “wear disposable gloves whenever there is a possibility of exposure to blood or other body fluids”) derived from the scale developed and validated by (Gershon et al., 1999). All items were scored on a range of 0–100, where 0 means never and 100 means always. The Cronbach’s alphas for this scale was 0.96. Also, CFA results revealed that despite the slightly high RMSEA, the eight-item model showed a satisfactory model fit (chi2 (20) = 33.36; CFI = 0.99; TLI = 0.99; RMSEA = 0.07; SRMR = 0.02), indicating the acceptable construct validity of the scale. AVE for anxiety was 0.77, which reflects the convergent validity of this construct.
Productivity was measured using a question asking for the perceived change in the level of efficiency due to the COVID-19 based on a scale ranging from 1 = has become much less to 7 = has become much more. Means, SD, reliability, and correlations of the constructs are presented in Table 2.
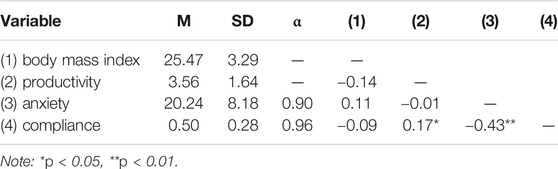
TABLE 2. Means, standard deviation, reliability coefficients, and correlations.
The hierarchical multiple regression with compliance as the dependent variable was formed (Table 3) and revealed that at stage one, income, gender, tenure, and dummy variables contributed significantly to the regression model, [F (5, 154) = 7.52, p < 0.001] and accounted for 17% of the variation in “compliance”. Introducing the dummy variable of profession to the second model improved it significantly: [F (5, 154) = 6.40, p < 0.001] and accounted for 25% of the variation in “compliance”. This change in R2 was significant, [F (3, 151) = 3.83, p < 0.05]. Introducing the BMI, smoking habit, dummy variables for stress medication and COVID-contact variables explained an additional 4.3% of the variation in compliance, but this change in R2 was not significant, [F (5, 146) = 1.80, p = 0.117]. Adding stress and productivity to the regression model explained an additional 18.9% of the variation in compliance, and this change in R2 was significant [F (2, 144) = 26.39, p < 0.001]. Thus, this model was retained for analysis purposes. When all 15 independent variables were included in stage three of the regression model, only stress, performance, education, and job were significant predictors of compliance. Together, the 15 independent variables accounted for 49% of the variance in compliance.
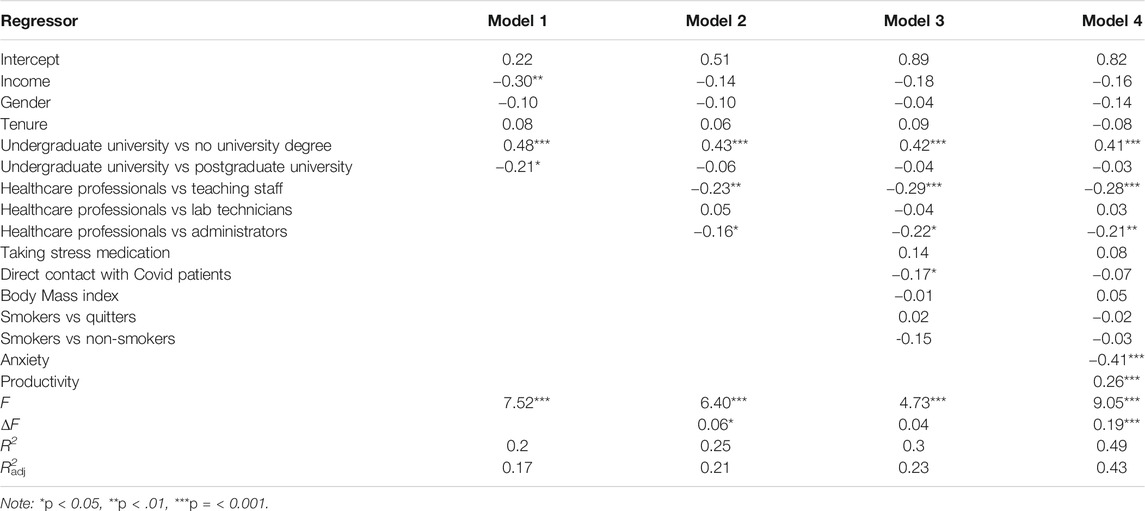
TABLE 3. Regression Model for compliance.
Furthermore, a hierarchical multiple regression with productivity as the dependent variable was formed (Table 4), and showed that at stage one, income, gender, tenure, and dummy variables for education, did not contribute significantly to the regression model, [F (5, 154) = 1.65, p = 0.149]. Introducing the dummy variable of profession to the second model improved it significantly: [F (8, 151) = 3.67, p < 0.001] and accounted for 11.8% of the variation in productivity. This change in R2 was significant, [F (3, 151) = 6.71, p < 0.001]. Introducing the BMI, dummy variables for smoking condition, taking stress medication, and COVID-contact variables explained an additional 21.8% of the variation in normal compliance, and this change in R2 was significant [F (5, 146) = 10.25, <0.001]. Thus, this model was retained for analysis purposes. When all 13 independent variables were included in stage three of the regression model, only tenure, profession, performance, education, and job were significant predictors of compliance. Together, the 13 independent variables accounted for 38% of the variance in compliance.
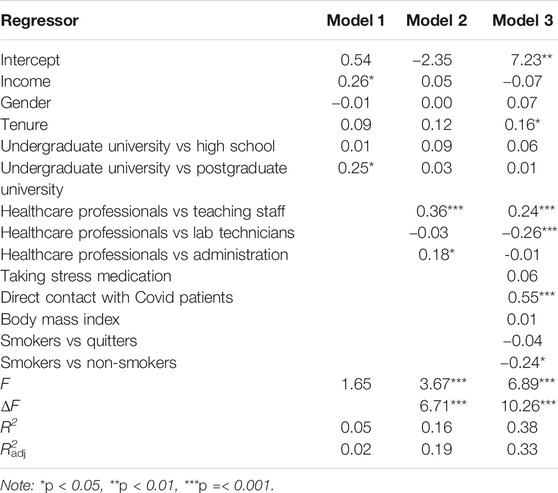
TABLE 4. Regression model for productivity.
This study investigated the effect of anxiety and productivity on organizational compliance of a medical science university in Iran during the outbreak of the COVID-19 infectious disease. Anxiety and stress are often experienced simultaneously, especially when facing significant uncertainties in life. When exposed to chronic stressors, individuals tend to engage in detrimental health behaviors such as drinking, smoking, binge eating, etc. (Rosenbaum and White, 2015). While previous studies have mostly focused on the impacts of anxiety and stress on individual health outcomes, the current study explored how anxiety and stress are linked to compliance behaviors. The findings of the study suggest that increased stress and anxiety led to fewer compliance behaviors. During COVID19, health compliance behaviors are unprecedentedly important as affected individuals can appear asymptomatic and still transmit the virus to others (Holshue et al., 2020). Whether or not to comply with the medical instructions is rooted in one’s moral reasoning and psychological state (Harper et al., 2020). Our study has confirmed that a poor psychological state can result in less health compliance behaviors, which in turn leads to decreased health outcomes in the community. This finding is in line with previous studies showing stress and anxiety deteriorate compliance (Gershon et al., 1999; Karvinen et al., 2013). The fear of COVID19 is unique as the virus can swiftly transmit across large populations. While fear may encourage a range of risk-reducing behaviors, it may also instill various negative emotions in people that lead to impaired health decisions (Harper et al., 2020). As evidenced in this study that stress leads to compromising compliance, government and health organizations are warranted to engage in effective communication that helps mitigate uncertainty and stress amidst the general population. The findings of this study contribute to our understanding of the Precede-Proceed model by focusing on health compliance, an individual health behavior that also has fatal consequences on others. As the world is becoming increasingly interdependent, future health studies/models need to pay more attention to behaviors and decision-making at a community-level.
This study also found that people with higher education backgrounds are more likely to comply with instructions. This positive relationship between education and health compliance is consistent with previous findings. Education is positively associated with the perception of self-efficacy and perceived benefits of health-promoting behavior, and those with higher education are more likely to comply with medical instructions (Garcia-Pena et al., 2001; Hacihasanoğlu and Gözüm, 2011). Future studies are warranted to continue control for education when studying individual health behaviors.
Furthermore, this study showed a significant difference in compliance among the employees of the various organizational sections. Medical science university teachers and administrators showed a higher level of compliance. Previous studies also showed that profession could affect compliance (Gershon et al., 1999). The effect of profession could be related to the more stressful nature of tasks among the healthcare professionals and lab technicians who are more involved in diagnosing and treating the patients compared to the policymaking, educational, and supporting role of the other employees in the healthcare organizations.
The positive effect of productivity on compliance is also a significant finding of this study. Majorly, the previous organizational studies have approached productivity as an outcome, while this research showed that once employees perceive themselves as more efficient at work, they are more likely to comply with the organizational regulations. Previous research showed that productivity is positively associated with participative activity in organization (Rosenberg and Rosenstein, 1980). Also, productivity is positively associated with different forms of psychological and mental abilities such as organizational involvement, organizational commitment, and perceived self-efficacy (Bandura, 2000; Eastin and LaRose, 2000; Wolf and Zwick, 2008; Phipps et al., 2013). Organizational commitment could be related to the psychological attachment with the organization to be more productive and reduce the intention to leave. Previous studies also indicated the association of compliance and increasing organizational commitment (Fritz, Arnett, and Conkel, 1999). The impact of productivity on compliance is related to the satisfaction employees perceive due to their work efficiency, increasing their attachment to the organization, and boosting their compliance. Especially, being efficient during the Covid-19 crisis entails both organizational and social satisfaction. During the crisis, healthcare employees worldwide were greatly appreciated for their extraordinary commitment and service. The feeling of being useful in battling the COVID-19 could have resulted in a higher self-efficacy and commitment, and compliance. This finding is in line with the previous study that indicated motivation as a necessary element of compliance (DiMatteo et al., 2012).
Further related to productivity, the study showed that healthcare professionals and lab technicians are more productive than the university teaching staff and administrators. Furthermore, the study showed that direct contact with COVID-19 patients increases workplace productivity. Both healthcare professionals (i.e. doctors and nurses) and lab technicians are highly involved with the COVID-19 patients, and their task entails an excessive level of care and commitment, associated with higher productivity, as mentioned before. Interestingly, the healthcare professional showed higher productivity and lowered compliance, while the total sample showed that productivity increased compliance. One explanation is that although working in a crisis circumstance has entailed higher workplace efficiency, healthcare professionals used more non-complying ways to go around the organizational regulations and accomplish their tasks more efficiently. Future studies should investigate the relationship between compliance and creativity during crises.
Furthermore, the study showed that tenure increases productivity among employees. The longer-tenured employees may have a better perception of their tasks to deal with the crisis. However, it is also essential to consider the effect of age. Further research is needed to investigate the independent effect of tenure on productivity. The study’s finding concerning tenure is in line with previous research showing tenure increased creativity and in-role performance and decreased self-rated counterproductive behavior in the organizations (Ng and Feldman, 2010).
The results of this study should be interpreted in light of some considerations. First, the possibility of self-bias in the report of compliance is a common limitation in the self-report measurement of compliance studies (De Bono et al., 2014). The same consideration is relevant to how people assess their productivity in the workplace. Second, despite the efforts, the respondent participation and small sample size impose restrictions on the generalizability of the finding. Further studies with higher sample sizes are warranted to measure the effect of various constructs on organizational compliance in healthcare organizations. Especially due to the cultural aspects of compliance, investigating this construct in diverse cultural contexts is crucial. Third, the disproportional sizes of some variables could have possibly affected some results.
The purpose of this study was to investigate the effect of anxiety, productivity, and various individual factors on healthcare organization employee compliance with organizational regulations during the COVID-19 outbreak. A significant theoretical contribution of this study is the sizable impact of anxiety on organizational compliance. This finding indicates the significance of caring for the employees’ mental health, especially during crises. The study also contributed to the current knowledge by showing that working under pressure and higher perceived risks can increase organizational productivity, which could lead to higher compliance, but the deteriorating effect of anxiety on compliance is much higher. The study also showed that education has a crucial role in increasing organizational compliance, and investing in employee education can benefit organizations by increasing employee compliance.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Dr Mohammad Jamalian, director of research ethics committee, Arak University of Medical Science . The patients/participants provided their written informed consent to participate in this study.
FV: Data Collection, Introduction (Anxiety) CZ: Introduction, Data analysis, Discussion, Theoretical framework AG: Method, Data analysis. proof-reading DR: Data collection, Introduction, compliance, productivity, individual risk factors, analysis, discussion, theoretical and method design.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Adeniyi, O. V., Ajayi, A. I., Ter Goon, D., Owolabi, E. O., Eboh, A., and Lambert, J. (2018). Factors affecting adherence to antiretroviral therapy among pregnant women in the Eastern Cape, South Africa. BMC Infect. Dis. 18 (1), 175. doi:10.1186/s12879-018-3087-8
Andersen, B. L., Kiecolt-Glaser, J. K., and Glaser, R. (1994). A biobehavioral model of cancer stress and disease course. Am. Psychol. 49 (5), 389–404. doi:10.1037//0003-066x.49.5.389
Arab-Mazar, Z., Sah, R., Rabaan, A. A., Dhama, K., and Rodriguez-Morales, A. J. (2020). Mapping the incidence of the COVID-19 hotspot in Iran - implications for travellers. Trav. Med. Infect. Dis. 34, 101630. doi:10.1016/j.tmaid.2020.101630
Bandura, A. (2000). “Cultivate self-efficacy for personal and organizational effectiveness,” in Handbook of principles of organization behavior. Editor E. Locke (Sussex, United Kingdom: Wiley), Vol. 2, 179–200.
Bandura, A. (1994). “Self-efficacy,” in Encyclopedia of human behaviour. Editor V. S. Ramachaudran (San Diego, CA: Academic Press), Vol. 4, 71–81.
Barlow, D. H. (1991). “The nature of anxiety: anxiety, depression, and emotional disorders,” in Chronic anxiety: generalized anxiety disorder and mixed anxiety-depression. Editors R. M. Rapee, and D. H. Barlow (New York, NY: Guilford Press), 1–28.
Beck, A. T., Epstein, N., Brown, G., and Steer, R. A. (1988). An inventory for measuring clinical anxiety: psychometric properties. J. Consult. Clin. Psychol. 56 (6), 893–897. doi:10.1037/0022-006X.56.6.893
Birnbaum, H. G., Ben-Hamadi, R., Kelley, D., Hsieh, M., Seal, B., Kantor, E., et al. (2010). Assessing the relationship between compliance with antidepressant therapy and employer costs among employees in the United States. J. Occup. Environ. Med. 52 (2), 115. doi:10.1097/JOM.0b013e3181cb5b10
Burton, W. N., Chen, C. Y., Li, X., and Schultz, A. B. (2017). Association between employee dental claims, health risks, workplace productivity, and preventive services compliance. J. Occup. Environ. Med. 59 (8), 721–726. doi:10.1097/JOM.0000000000001069
Carthey, J., Walker, S., Deelchand, V., Vincent, C., and Griffiths, W. H. (2011). Breaking the rules: understanding non-compliance with policies and guidelines. BMJ 343, d5283. doi:10.1136/bmj.d5283
Chiang, L. C., Huang, J. L., Yeh, K. W., and Lu, C. M. (2004). Effects of a self-management asthma educational program in Taiwan based on PRECEDE-PROCEED model for parents with asthmatic children. J. Asthma 41 (2), 205–215. doi:10.1081/jas-120026078
Ciorlia, L. A., and Zanetta, D. M. (2005). Hepatitis B in healthcare workers: prevalence, vaccination and relation to occupational factors. Braz. J. Infect. Dis. 9 (5), 384–389. doi:10.1590/S1413-86702005000500005
De Bono, S., Heling, G., and Borg, M. A. (2014). Organizational culture and its implications for infection prevention and control in healthcare institutions. J. Hosp. Infect. 86 (1), 1–6. doi:10.1016/j.jhin.2013.10.007
DiMatteo, M. R., Haskard-Zolnierek, K. B., and Martin, L. R. (2012). Improving patient adherence: a three-factor model to guide practice. Health Psychol. Rev. 6 (1), 74–91. doi:10.1080/17437199.2010.537592
Drewnowski, A. (2019). Impact of nutrition interventions and dietary nutrient density on productivity in the workplace. Nutr. Rev. 78 (3), 215–224. doi:10.1093/nutrit/nuz088
Eastin, M. S., and LaRose, R. (2000). Internet self-efficacy and the psychology of the digital divide. J. Computer-Mediated Commun. 6 (1). doi:10.1111/j.1083-6101.2000.tb00110.x
Farzianpour, F., Abbasi, M., Foruoshani, A. R., and Pooyan, E. J. (2016). The relationship between Hofstede organizational culture and employees job burnout in hospitals of Tehran University of Medical Sciences 2014-2015. Mater Sociomed. 28 (1), 26–31. doi:10.5455/msm.2016.28.26-31
Flodgren, G., O'Brien, M. A., Parmelli, E., and Grimshaw, J. M. (2019). Local opinion leaders: effects on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 6 (6), CD000125. doi:10.1002/14651858.CD000125.pub5
Foorthuis, R., and Bos, R. (2011). A framework for organizational compliance management tactics. Berlin, Heidelberg: Paper presented at the Advanced Information Systems Engineering Workshops.
Fritz, J. M. H., Arnett, R. C., and Conkel, M. (1999). Organizational ethical standards and organizational commitment. J. Bus. Ethics 20 (4), 289–299. doi:10.1023/A:1005939325707
Fuller, C., Michie, S., Savage, J., McAteer, J., Besser, S., Charlett, A., et al. 2012). The Feedback Intervention Trial (FIT)--improving hand-hygiene compliance in United Kingdom healthcare workers: a stepped wedge cluster randomised controlled trial. PloS One 7 (10), e41617. doi:10.1371/journal.pone.0041617
Garcia-Peña, C., Thorogood, M., Armstrong, B., Reyes-Frausto, S., and Muñoz, O. (2001). Pragmatic randomized trial of home visits by a nurse to elderly people with hypertension in Mexico. Int. J. Epidemiol. 30, 1485–1491. doi:10.1093/ije/30.6.1485
Gates, D. M., Succop, P., Brehm, B. J., Gillespie, G. L., and Sommers, B. D. (2008). Obesity and presenteeism: the impact of body mass index on workplace productivity. J. Occup. Environ. Med. 50 (1), 39. doi:10.1097/JOM.0b013e31815d8db2
Gershon, R. R., Karkashian, C. D., Vlahov, D., Kummer, L., Kasting, C., Green-McKenzie, J., et al. (1999). Compliance with universal precautions in correctional health care facilities. J. Occup. Environ. Med. 41 (3), 181–189. doi:10.1097/00043764-199903000-00007
Gershon, R. R., Vlahov, D., Felknor, S. A., Vesley, D., Johnson, P. C., Delclos, G. L., et al. (1995). Compliance with universal precautions among health care workers at three regional hospitals. Am. J. Infect. Contr. 23 (4), 225–236. doi:10.1016/0196-6553(95)90067-5
Gielen, A. C., and McDonald, E. M. (1997). “The precede-proceed planning model,” in Health behavior and education. Editors K. Glanz, F. M Lewis, and B. K. Rimmer (San Francisco, CA: Jossey-Bass Publishers), 359–383.
Green, L. W., and Kreuter, M. W. (1991). Health promotion planning: an educational and environmental approach. 2nd Edn. Mountain View, CA: Mayfield Publishers.
Grupe, D. W., and Nitschke, J. B. (2013). Uncertainty and anticipation in anxiety: an integrated neurobiological and psychological perspective. Nat. Rev. Neurosci. 14 (7), 488–501. doi:10.1038/nrn3524
Hacihasanoğlu, R., and Gözüm, S. (2011). The effect of patient education and home monitoring on medication compliance, hypertension management, healthy lifestyle behaviours and BMI in a primary health care setting. J. Clin. Nurs. 20, 692–705. doi:10.1111/j.1365-2702.2010.03534.x
Hair, J. F., Black, W. C., Babin, B. J., and Anderson, R. E. (2014). Multivariate data analysis. 7th Edn. Upper Saddle River, NJ: Prentice Hall.
Harper, C. A., Satchell, L. P., Fido, D., and Latzman, R. D. (2020). Functional fear predicts public health compliance in the COVID-19 pandemic. Int. J. Ment. Health Addiction 1, 1. doi:10.1007/s11469-020-00281-5
Holshue, M. L., DeBolt, C., Lindquist, S., Lofy, K. H., Wiesman, J., Bruce, H., et al. (2020). First case of 2019 novel coronavirus in the United States. N. Engl. J. Med. 382, 929–936. doi:10.1056/NEJMoa2001191
Hu, L. T., and Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct. Equ. Model.: A Multidisciplinary Journal 6, 1–55. doi:10.1080/10705519909540118
Hu, Q., Dinev, T., Hart, P., and Cooke, D. (2012). Managing employee compliance with information security policies: the critical role of top management and organizational culture*. Decis. Sci. J. 43 (4), 615–660. doi:10.1111/j.1540-5915.2012.00361.x
Huttunen, R., and Syrjänen, J. (2014). Healthcare workers as vectors of infectious diseases. Eur. J. Clin. Microbiol. Infect. Dis. 33 (9), 1477–1488. doi:10.1007/s10096-014-2119-6
Jahanshahi, A. A., Dinani, M. M., Madavani, A. N., Li, J., and Zhang, S. X. (2020). The distress of Iranian adults during the Covid-19 pandemic-more distressed than the Chinese and with different predictors. Brain Behav. Immun. 87, 124–125. doi:10.1016/j.bbi.2020.04.081
Joshi, A. V., Madhavan, S. S., Ambegaonkar, A., Smith, M., Scott, V., and Dedhia, H. (2006). Association of medication adherence with workplace productivity and health-related quality of life in patients with Asthma. J. Asthma 43 (7), 521–526. doi:10.1080/02770900600857010
Karvinen, K. H., Murray, N. P., Arastu, H., and Allison, R. R. (2013). Stress reactivity, health behaviors, and compliance to medical care in breast cancer survivors. Oncol. Nurs. Forum 40 (2), 149–156. doi:10.1188/13.ONF.149-156
Lancet, T. (2020). COVID-19: protecting healthcare workers. Lancet 395 (10228), 922. doi:10.1016/S0140-6736(20)30644-9
Liu, S., Volčič, Z., and Gallois, C. (2019). Introducing intercultural communication: global cultures and contexts. 3rd Edn. Thousand Oaks, CA: Sage.
Lofland, J. H., Pizzi, L., and Frick, K. D. (2004). A review of health-related workplace productivity loss instruments. Pharmacoeconomics 22 (3), 165–184. doi:10.2165/00019053-200422030-00003
Martin, L. R. (2014). “Barriers and keys to treatment adherence and health behavior change,” in The oxford handbook of health communication, behavior change and treatment adherence. Editors L. R. Martin, and M. R. DiMatteo (New York, NY: Oxford University Press), 9–20.
McCarthy, J. M., Trougakos, J. P., and Cheng, B. H. (2016). Are anxious workers less productive workers? It depends on the quality of social exchange. J. Appl. Psychol. 101 (2), 279. doi:10.1037/apl0000044
Moghanibashi-Mansourieh, A. (2020). Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian J. Psychi. 51, 102076. doi:10.1016/j.ajp.2020.102076
Moon, H., Quigley, N. R., and Marr, J. C. (2012). How interpersonal motives explain the influence of organizational culture on organizational productivity, creativity, and adaptation. Org. Psychology Rev. 2 (2), 109–128. doi:10.1177/2041386611433085
Ng, T. W. H., and Feldman, D. C. (2010). Organizational tenure and job performance. J. Manag. 36 (5), 1220–1250. doi:10.1177/0149206309359809
O’Reilly, C. A., and Chatman, J. (1986). Organizational commitment and psychological attachment: the effects of compliance, identification, and internalization on prosocial behavior. J. Appl. Psychol. 71 (3), 492–499. doi:10.1037/0021-9010.71.3.492
Paradis, G., O’Loughlin, J., Elliott, M., Masson, P., Renaud, L., Sacks-Silver, G., et al. (1995). Coeur en santé St-Henri--a heart health promotion programme in a low income, low education neighbourhood in Montreal, Canada: theoretical model and early field experience. J. Epidemiol. Community Health 49, 503–512. doi:10.1136/jech.49.5.503
Paulsen, R. (2016). Slipping into functional stupidity: the bifocality of organizational compliance. Hum. Relat. 70 (2), 185–210. doi:10.1177/0018726716649246
Phipps, S. T., Prieto, L. C., and Ndinguri, E. N.(2013). Understanding the impact of employee involvement on organizational productivity: the moderating role of organizational commitment.J. Organ. Cult. Commun. Conflict 17 (2), 107–120.
Rahmani, D. (2017). Minorities’ communication apprehension and conflict: An investigation of Kurds in Iran and Malays in Singapore. PhD thesis. Jyvaskyla (Finland): University of Jyvaskyla.
Ransdell, L. B. (2001). Using the precede-proceed model to increase productivity in health education faculty. Int. Electron. J. Health Educ. 4, 276–282.
Riedel, J. E., Lynch, W., Baase, C., Hymel, P., and Peterson, K. W. (2001). The effect of disease prevention and health promotion on workplace productivity: a literature review. Am. J. Health Promot. 15 (3), 167–191. doi:10.4278/0890-1171-15.3.167
Rosekind, M. R., Gregory, K. B., Mallis, M. M., Brandt, S. L., Seal, B., and Lerner, D. (2010). The cost of poor sleep: workplace productivity loss and associated costs. J. Occup. Environ. Med. 52 (1), 91. doi:10.1097/JOM.0b013e3181c78c30
Rosenbaum, D. L., and White, K. S. (2015). The relation of anxiety, depression, and stress to binge eating behavior. J. Health Psychol. 20 (6), 887–898. doi:10.1177/1359105315580212
Rosenberg, R. D., and Rosenstein, E. (1980). Participation and productivity: an empirical study. ILR Review 33 (3), 355–367. doi:10.1177/001979398003300306
Smith, L. E., D'Antoni, D., Jain, V., Pearce, J. M., Weinman, J., and Rubin, G. J. (2016). A systematic review of factors affecting intended and actual adherence with antiviral medication as treatment or prophylaxis in seasonal and pandemic flu. Influenza. Other Respir. Viruses 10 (6), 462–478. doi:10.1111/irv.12406
Weaver, G. R., and Treviño, L. K. (1999). Compliance and values oriented ethics programs: influenceson employees' attitudes and behavior. Bus. Ethics Q. 9 (2), 315–335. doi:10.2307/3857477
Welk, G. J. (1999). The youth physical activity promotion model: a conceptual bridge between theory and practice. Quest 51 (1), 5–23. doi:10.1080/00336297.1999.10484297
Wolf, E., and Zwick, T. (2008). Reassessing the productivity impact of employee involvement and financial incentives. Schmalenbach Bus. Rev. 60 (2), 160–181. doi:10.1007/BF03396764
Zhang, S. X., Liu, J., Afshar Jahanshahi, A., Nawaser, K., Yousefi, A., Li, J., et al. (2020). At the height of the storm: healthcare staff's health conditions and job satisfaction and their associated predictors during the epidemic peak of COVID-19. Brain Behav. Immun. 87, 144–146. doi:10.1016/j.bbi.2020.05.010
Keywords: organizational compliance, anxiety, productivity, COVID-19, regression, Iran
Citation: Rahmani D, Zeng C, Goodarzi AM and Vahid F (2021) Organizational Compliance During COVID-19: Investigating the Effects of Anxiety, Productivity, and Individual Risk Factors Among Iranian Healthcare Employees. Front. Commun. 6:560451. doi: 10.3389/fcomm.2021.560451
Received: 09 May 2020; Accepted: 07 January 2021;
Published: 08 February 2021.
Edited by:
Rukhsana Ahmed, University at Albany, United StatesReviewed by:
James Olumide Olufowote, University of Oklahoma, United StatesCopyright © 2021 Rahmani, Zeng, Goodarzi and Vahid. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Farhad Vahid, ZmFyaGFkdmFoaWRAb3V0bG9vay5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.