 Sarah C. Stevens
Sarah C. Stevens Suruchi Sood
Suruchi Sood Nicole Mertz
Nicole Mertz Kelli Kostizak
Kelli Kostizak- Dornsife School of Public Health, Department of Community Health and Prevention, Drexel University, Philadelphia, PA, United States
In the Europe and Central Asia region, there are at least five million children diagnosed with some type of disability. These children are likely to be subjected to stigmatization and marginalization, which can lead to discrimination and reduction in access to social services. A pilot study was developed to examine factors affecting the treatment of children with disabilities from a holistic, systematic perspective. Stratified by the social ecological model, 450 respondents participated in a structured interview designed to measure knowledge, attitudes, norms, marginalization, and stigma. The results yielded four conclusions. First, it showed that professionals did not rate differently on the constructs of the conceptual model when compared to nonprofessionals. Second, norms are likely affecting the treatment of children with disabilities. Third, the study shows that there is not enough emphasis on educating and involving community members to improve the treatment and protect the rights of children with disabilities. Finally, the results emphasize the importance of approaching disability from a comprehensive social ecological perspective.
Introduction
Over five million of the children who reside in the Europe and Central Asia region are believed to have some sort of disability, with close to 3.6 million living in residential institutions (UNICEF, 2015). In recent decades, there have been many global initiatives to improve the lives of children with disabilities, such as the Convention on the Rights of the Child (CRC) and the Convention of the Rights of Persons with Disabilities (CRPD), which outline the responsibilities of the State to protect vulnerable individuals from health, social, economic, cultural, civic, and political discrimination (UN General Assembly, 1989, 2007). Despite such agreements, many children with disabilities face significant challenges and violations of their human rights. Children with disabilities are often deprived of medical access and education and are less likely to have proper nutrition (Byers et al., 2018; UNICEF, 2018). They are also at a higher risk for maltreatment, abuse, and violence (Hibbard and Desch, 2007; Hershkowitz et al., 2010). Girls with disabilities may face two-fold discrimination due to the intersection of their disability and gender (UNICEF, 2013). Further, stigma, prejudice, and ignorance due to the lack of capacity building and trainings related to children with disabilities often get in the way of positive change (UNICEF, 2013).
This study, therefore, seeks to better understand the social-environmental factors that are perpetuating discrimination against children with disabilities in Europe and Central Asia.
Defining Disability
It is important to begin with a common understanding of how disability is defined, as there are several ways in which it can be conceptualized. Perhaps most common, the medical model of disability considers persons with disabilities as having problems that need to be cured (Manago et al., 2017). The medical model implies that abnormality is inherent in disability and encourages the individual to adapt to society. Another model, the charity model, sees persons with disabilities as victims of their impairments in need of sympathy and charity to cope with their (perceived as) tragic situation (Hollenweger and Martinuzzi, 2015). A third, more holistic model, called the social model, began to develop in the 1960's. The social model posits that disability is a limitation in attitudes, institutions, and the environment that prevents full and equal participation of all individuals in society (World Health Organization (WHO) World Bank, 2011). By situating disability within a larger context, the social model allows for a systems level, rather than individualistic, approach to addressing disabilities.
The social model was approved by the WHO and published in the International Classification of Impairments, Disabilities and Handicaps in 1980 (Bickenbach et al., 1999). While progressive at the time, it grew to receive criticism, as the language was ambiguous and still seemed somewhat in line with the medical model [Bickenbach et al., 1999]. Therefore, in 2002, the International Classification of Functioning, Disability, and Health (ICF) described a more inclusive framework that combines the social and medical model, called the biopsychosocial model (World Health Organization (WHO), 2002). The ICF defines disability as “an umbrella term for impairments, activity limitations and participation restrictions” [World Health Organization (WHO), 2002, p. 2]. It is conceptualized by the interaction between health conditions due to diseases, disorders, and injuries and contextual factors. Contextual factors include environmental factors, such as social attitudes, and individual factors, such as education. These constructs influence how a person experiences disability [World Health Organization (WHO), 2002]. Whenever this paper mentions disability, it will employ this human-rights-based definition, drawing upon the biopsychosocial model.
Children With Disabilities in North Macedonia
Accurate data on the number of children living with a disability in North Macedonia is lacking. Estimates from 2010 and 2011 placed the number somewhere between 25,535 and 55,000 children, depending on the formula used [Velichkovski and Chichivalieva, 2010; World Health Organization (WHO) World Bank, 2011]. However, official figures from 2018 reported an estimate of 8,000 children (MLSP, 2018). While this figure includes 700 estimated children unregistered and not in contact with social services, it is still considerably less than external estimates. The discrepancy between official estimates and external estimates indicates that there may be many more unregistered children with disabilities who are being hidden away at home and not receiving any official services.
Even children who are registered may not receive the support to which they are entitled. Despite ratifying the CRPD in 2011 and accepting by succession the CRC in 1993, national policies are often poorly implemented (United Nations, 2020). North Macedonia's federal provisions for children with disabilities are mainly handled by the health, education, and social sectors, but a 2015 assessment of the capacity of these sectors found that there was little integration between them and no shared vision to comprehensively meet the needs of children with disabilities (Hollenweger, 2015). Further, the current public funding schemes seem to promote exclusion of children with disabilities by privileging specialized institutions over inclusion (Hollenweger, 2015).
Many organizations beyond the federal government provide support for children with disabilities and their families; a mapping in 2014 identified 136 associations, foundations, and informal civic initiatives involved in the field of inclusion of and support for children with disabilities (Open the Windows, 2014). However, these organizations are not evenly distributed, and the capital city is the only place in which persons with all types of disabilities are supported (Open the Windows, 2014). Similar to the federal sectors, there is little communication or cooperation among non-governmental organizations or with the public sector.
The effectiveness of the systems and organizations is likely further affected by the knowledge, attitudes, and practices (KAP) of those working in them. While there is little information on the specific perspectives of professionals in North Macedonia about children with disabilities, it may be possible to generalize the KAP of professionals from the views of the general population. A 2014 KAP study in North Macedonia found that 69% of the population views disability through either the medical or the charity model and that over half of participants reported having no or low awareness of children with disabilities (UNICEF, 2014). Additionally, only 4% of the population was in support of inclusive education, with 48% saying children with disabilities should be in separate schools (UNICEF, 2014). The level of rejection for children with disabilities also seems to vary depending on the nature of the relationship being explored. For example, depending on the type of disability, between 63 and 79% of respondents found it acceptable for a child with a disability to live in the same settlement or street with their own child; comparatively, only 2–6% found it acceptable for a child with a disability to marry their child (as adults) (UNICEF, 2014).
Conceptualizing Discrimination
The CRPD describes discrimination as “any distinction, exclusion, or restriction on the basis of disability which has the purpose or effect of impairing or nullifying the recognition, enjoyment or exercise, on an equal basis with others, of all human rights and fundamental freedoms in the political, economic, social, cultural, civil, or any other field” (UN General Assembly, 2007, Article 2). However, knowing the definition of discrimination is not sufficient for eliminating it. To reduce discrimination against children with disabilities, it is imperative to determine the factors that lead to such behaviors. The conceptual model in Figure 1 is based on a systematic review of behavior change theories, disability, and discrimination conducted by the authors in 2017 (Sood et al., 2020).
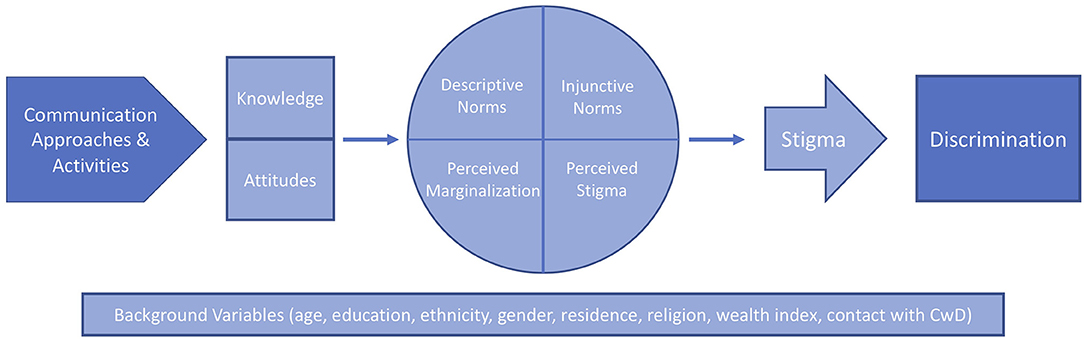
Figure 1. Conceptual model connecting communication approaches and activities to discrimination.
The first constructs of the model are knowledge and attitudes, as they are precursors to behavior; they are the important steps that lead to the intention to practice (or to not practice) a behavior (Ajzen, 1991). The connection between knowledge, attitudes, and behavior has been extensively studied and is generally accepted. However, knowledge and attitudes alone are not always sufficient to predict behavior; social norms may also be a key component. Social norms are the behaviors that a group of people believe to be typical or appropriate. They are the unwritten rules that guide behavior (Bicchieri et al., 2018). Social norms do not always align with personal attitudes. Someone may approve of a behavior but choose not to practice it because of their beliefs about the approval and behavior of others. Social norms are generally divided into two components; although the terminology differs throughout the literature, this paper will refer to descriptive and injunctive norms. Descriptive norms are beliefs about what other people are doing, while injunctive norms are beliefs about what other people think people should do (Mackie et al., 2015). It is important to measure both descriptive and injunctive norms to understand normative influences on a behavior.
Taken together, knowledge, attitudes, and social norms can start to affect stigma. Stigma was considered integral to the model because discrimination is often conceptualized as the behavioral reaction to the negative prejudices of stigma (Link and Phelan, 2001; Corrigan and Watson, 2002; Major and O'Brien, 2005; Van Brakel, 2007; Van Brakel et al., 2012). The World Health Organization defines stigma as “a mark of shame, disgrace or disapproval which results in an individual being rejected, discriminated against, and excluded from participating in a number of different areas of society” [World Health Organization (WHO), 2001, p. 17]. Stigma has been conceived as a compound of multiple components: labeling, stereotyping, separation, and status loss and discrimination (Link and Phelan, 2001). Stigma includes recognizing socially salient differences, assigning negative attributes to those differences, and creating a sense of “otherness” by reacting to those differences (Green et al., 2005). This study also considers perceived stigma (beliefs about the amount of stigmatization perpetrated by others) and perceived marginalization (beliefs about the amount of marginalization perpetrated by others), as these can affect stigmatization from a normative approach.
Stigma ultimately leads to discrimination through avoidance, withholding help, segregation, and coercive treatment (Van Brakel, 2007; Social Exclusion Knowledge Network, 2008). Stigma can reduce access to treatment and services, as well as increase social exclusion (US DHHS, 1999; Green et al., 2005; Stuber et al., 2008). Unequal power dynamics caused by these practices continue the cycle of exclusion, which can result in health inequities (Krieger, 2000; Social Exclusion Knowledge Network, 2008). In this case, we are looking at experiences of marginalization on the basis of a person's disability.
In the conceptual model, communication interventions and activities are placed at the beginning, to emphasize their important role in reducing discrimination against children with disabilities. Communication that takes an evidence- and rights-based approach and emphasizes participation from all stakeholders can be used in behavior and social change interventions. These approaches are especially effective when they empower communities to take an active role in the decisions that affect their lives (UNICEF, 2019).
Therefore, the conceptual model shows that communication approaches and activities can promote positive changes in attitudes and knowledge about children with disabilities, which can affect social norms, perceived marginalization, and perceived stigma. These can lead to a reduction in stigma, which contributes to decreasing discrimination against children with disabilities. Sociodemographic variables, like age, sex, and education, are placed across the entire model, as they can also affect how people think and how they behave.
Measuring Discrimination
In order to assess discrimination against children with disabilities, and to be able to track changes in the amount of discrimination they face, it is necessary to have valid and reliable tools for measurement. However, current research on the conceptualization and practice around children with disabilities vary in quality. A systematic review by the authors of 44 studies on discriminatory attitudes and social norms related to children with disabilities revealed that such research generally lacks tools to accurately measure attitudes or social norms, clear definitions of key concepts, involvement of children, mixed-methods approaches, participatory methods, and a focus on social norms (Sood et al., 2020). Furthermore, the review found that most studies and programs do not approach research on discrimination against children with disabilities holistically or systematically. Of the 44 articles, only 25 used a theoretical framework, and only five of those used the Social Ecological Model (SEM) (Sood et al., 2020). The SEM stresses the importance of the multifaceted interactions between social and environmental factors and how they impact behavior (UNICEF, 2016). Given the understanding of disability through the biopsychosocial model, it is especially important to take such a multilevel approach to disability research. Research using the SEM as its guiding framework would seek to gain the perspectives from stakeholders at every level: individual, family, community, and policy/systems. While children with disabilities, children without disabilities, parents, and professionals were all represented in the different peer-reviewed studies, only two of the 44 examined more than one type of audience (Sood et al., 2020). Additionally, the studies focused predominantly on knowledge, attitudes, and practice, with social norms being noticeably absent. If norms perpetuate discrimination at the social level, then they must be clearly defined, and tools must exist to measure the normative constructs.
Other systematic reviews on attitudes, beliefs, and prejudice against people with disabilities found similar gaps. For example, a systematic review of 20 studies on the relationship between students' attitudes and the social participation of peers with disabilities found that studies were using inconsistent measures of attitudes (De Boer et al., 2012). Furthermore, of the 20 studies, only three presented empirical data on the connection between attitudes and discrimination and social exclusion of children with disabilities (De Boer et al., 2012). Through a systematic review of nurses' attitudes toward children with disabilities, Cervasio (2010) concluded that “scant” research exists on the connection between health professionals' attitudes and the treatment children with disabilities receive. Scior (2011) reviewed 75 articles on public awareness, attitudes, and beliefs about intellectual disability and found mainly descriptive accounts of attitudes and a lack of high-quality evaluations. The author concluded that “there is a need for research that considers the complex processes involved in the formation of stigma, prejudices and discrimination that can negatively affect the opportunities available to people with intellectual disabilities and their social inclusion” (Scior, 2011, p. 2179).
The Present Study
The current study attempts to address the aforementioned gaps in research by creating a set of validated measures for the constructs of the conceptual model. It investigates the relationships between social-environmental factors and discrimination by measuring key stakeholders' knowledge, attitudes, social norms, and stigma toward children with disabilities and their families. The study aims to determine the importance of a holistic and systematic approach for realizing the rights of children with disabilities.
Materials and Methods
Materials
A quantitative questionnaire was developed by adapting pre-existing measures and creating new ones where necessary. The questionnaire was designed to capture knowledge, attitudes, normative beliefs, perceived marginalization, perceived stigma, and personal stigmatization of children with disabilities. As this was a pilot study, more questions were included than typical, so as to assess the best way to measure the constructs of the conceptual model. The draft tools were then reviewed by multiple experts in disability and researchers with experience in interviewing children. After revisions, the tools were translated into Macedonian and pretested in the field with the help of a local research agency to ensure comprehension and cultural appropriateness. Pretesting the tools for all children, specifically children with disabilities, was given greater emphasis to ensure that the instructions for the activities and the questions were simple to understand. The tool was finalized for pilot testing based on the results of the pretest.
Study Sample
Fifteen different stakeholder groups spanning the SEM were identified as important to the treatment of children with disabilities in North Macedonia (Figure 2). These included children with disabilities (ages 12–18 years) at the individual level; caregivers of children with disabilities (three groups corresponding to the child's age: 0–3, 3–6, and 6–11 years) at the family level; children without disabilities (ages 12–18 years) and caregivers of children without disabilities (three groups corresponding to the child's age: 0–3, 3–6, and 6–11 years) at the community level; and academic professionals (both teachers and administrators), health professionals (for both maternity and school-aged children), social workers, civil society professionals and government officials at the policy level.
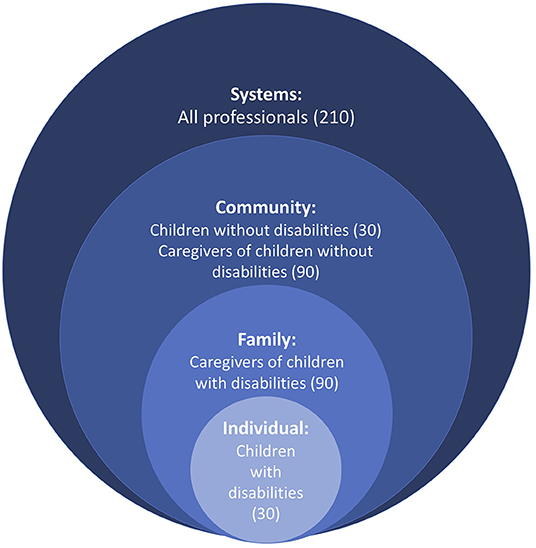
Figure 2. Respondent groups distributed by the social ecological model.
When identifying participants, the CRPD definition of disability was used: a “long-term physical, mental, intellectual, or sensory impairment which in interaction with various barriers may hinder their full and effective participation in society on an equal basis with others” (CRPD, Article 1, 2006). The study aimed to look at discrimination against children with disabilities as a whole, therefore no specific disability was sampled for.
The three age groups for children were identified in conjunction with local experts as representing three critical phases in children with disabilities' lives: their first interaction with the healthcare system and the period during which institutionalization is most likely, their first interaction with the education system, and their expanding connection with, and understanding of and by, peers. While it is understood that the experiences of children with disabilities vary across their lifetime, the scope of the study limited the number of age groups that could be assessed. The age groups not assessed in this study offer opportunities for further study.
Pretesting of the tools was unsuccessful with children with disabilities under the age of 12. Based on the recommendation made by local disability experts, children with disabilities ages 12–18 were interviewed instead, while still interviewing parents that corresponded to the three age groups of interest. These decisions were then mirrored for children without disabilities and caregivers of children without disabilities for comparability of data.
The convention of using 30 individuals per group is common for pilot studies and thus was used in the present study (Johanson and Brooks, 2010). A list of children with disabilities and their parents was collected from government records and consultations with health and social service NGO's who work with children with disabilities and their parents. The government and non-governmental health and social workers assisted with sample selection by informing individuals of the study and providing them with a phone number to call, if they wished to participate. The children without disabilities and their parents were purposively selected, to the extent possible, from the same residential location or school as their counterparts. The professional sample was purposively selected from a list of Disability Persons Organizations, to cover different professional ranks and job responsibilities.
For the purposes of analysis of this study, the fifteen stakeholder groups were condensed into four aggregate groups corresponding to each SEM level. At the individual level were children with disabilities themselves (30 individuals). The three groups of caregivers of children with disabilities were categorized together as the family level (90 individuals). Both children without disabilities and their caregivers were considered community members (120 individuals). Finally, all professionals were combined to represent the policy/systems level (210 individuals).
Variables
The quantitative questionnaire asked questions to measure the variables of interest, as identified in the conceptual model: knowledge, attitudes, normative beliefs, perceived marginalization, perceived stigma, and personal stigmatization of children with disabilities. As this was a pilot study, it was first necessary to analyze the questions themselves. This was done by looking at the percentage of “don't know” or “refused to respond” answers to each question, along with qualitative input from data collectors and statistical tests, such as factor analyses and Cronbach's alpha. Factor analysis was performed on the scales for attitudes, perceived marginalization, perceived public stigma, and personal stigmatization of children with disabilities. Table 1 lists the eigenvalues and Cronbach's α associated with these factor analyses.
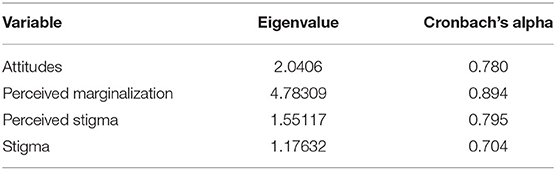
Table 1. Factor analysis results for scale creation.
Sixteen knowledge questions were asked to all respondents, conceptualized as the ability to identify types of disabilities and impairments, with response options of no, maybe, or yes. For knowledge, four questions with high proportions of refused to respond and don't know were removed and the remaining 12 were evenly split into knowledge of intellectual disabilities and knowledge of physical disabilities.
All respondents were then asked attitudinal questions, in which they rated their agreement with a series of 15 statements, e.g., “children with disabilities can do lots of things for themselves,” using a five-point Likert scale from strongly disagree to strongly agree. After statistical analysis, the final scale for attitudes included five items from the original 12 (α = 0.78).
Normative questions were based on vignettes. The vignettes described a child with a disability and combinations of age group (0–3, 3–6, 6–11), type of impairment (physical or intellectual), and key behavior of interest (deinstitutionalization, inclusive education, or general human rights). After being read the vignette, respondents were asked questions to assess descriptive and injunctive norms. First, they were asked what they would do, e.g., “Where is the best place for this child to live? At home, with a foster family, or at an institution?” This was followed by asking what they thought their family, community, and society would approve of, e.g., “Would your family members approve of keeping the child at home, placing her in a foster family, or putting her in an institution?” Next, they were asked to rate the extent to which [from not at all (1) to completely (5)] their decision from the first question would be affected by what their family/community/society expects them to do. Each adult respondent was asked the series of questions about two vignettes, one about a physical impairment and one about an intellectual impairment.
Twelve questions were asked to all respondents to assess perceived marginalization. Participants stated how often they thought the event happened to children with disabilities or their families, from never (1) to multiple times per day (6). The questions included events such as “they receive poorer service than other people in restaurants or stores.” The final scale for marginalization included nine items from the original 12 (α = 0.89).
Because of the likelihood that people would not admit to directly committing discriminating actions against children with disabilities, due to social desirability bias, this study looked at personal stigmatization of children with disabilities as the outcome measure. Personal stigmatization was operationalized as a set of eight questions designed to capture the components of labeling, stereotyping, and separation when taken together, with answers ranging from strongly disagree (1) to strongly agree (1). To capture perceived stigma, all respondents were asked to rate other's agreement with those same eight questions. The final scales for perceived stigma and personal stigmatization both included three items from the original eight (α = 0.795 and α = 0.704, respectively).
Ethical Considerations
The study received ethical approval from Drexel University, as well as independent approval from Health Media Lab. All adult participants gave informed consent before the start of the study. Child participants gave assent to participate, with their parent or guardian also consenting for their participation. Children were interviewed using specially trained local social workers that have experience in working with and researching children with and without disabilities.
Data Analysis
Statistical analysis was performed on STATA 15 with results from completed structured interviews. Questionnaires were considered complete if at least 80% of the questions were answered.
To create the indicators, all Likert scales were recoded to start at 0 instead of 1 and any dichotomous questions were recoded as 0/1. All questions that were worded in an opposite way of the rest of the scale were reverse coded. Responses that included “don't know” and “refused to answer” were recoded as missing data. The final indicators for attitudes, perceived marginalization, perceived stigma, and personal stigmatization were created by adding across the final scale items. Because the distribution of these additive variables proved to be skewed, dichotomous variables were created for each. Respondent scores were coded as low or high (for knowledge, marginalization, and stigma) or as negative or positive (for attitudes).
Descriptive analyses were completed for demographic information, with significance testing (t-test for means, chi-squared for all others) to see if the sample varied by the background characteristics. Frequencies and percentages were calculated for all construct indicators. Then, chi-squared tests were conducted to look for significant differences in any of the construct indicators by SEM level. Subsequently, bivariate analysis was done through logistical regression, followed by a multiple logistic regression that included all variables in the model.
Results
Description of the Sample
The sample contained statistically significantly more females (75.1%) than males (24.9%) (p = 0.000). For children with disabilities, the mean age was 16.6 years (sd = 1.9); for caregivers of children with disabilities, it was 37.1 years (sd = 5.7); for the community level, 30.0 years (sd = 10.7), and for professionals, 44.4 years (sd = 11.3). Most (56.9%) of the participants were at least college-educated, whereas 35.6% had only completed secondary school and 7.6% had only completed primary school. Table 2 summarizes sociodemographic characteristics for the entire sample, by SEM level.
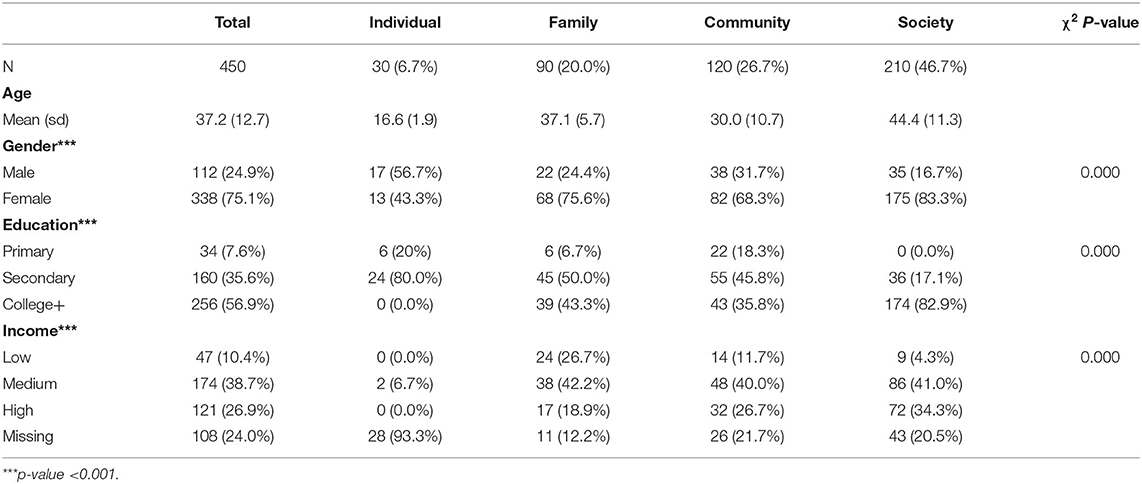
Table 2. Demographics overall and by social ecological model level.
Frequency Results
More (58.4%) of the sample had high knowledge of physical disabilities as compared to low levels (41.6%). On the other hand, slightly less than half (48.0%) of the sample had high knowledge of intellectual disabilities. The respondents mainly had positive attitudes toward children with disabilities (76.9% compared to 23.1% negative), yet most (58.4%) respondents perceived high amounts of public stigma and high amounts of marginalization (78.0%). When considering norms, perceptions of approval of the desired behavior decreased with social distance from the respondent. Of adult participants, 35.6% of participants said they themselves approved of the desired behavior, while 32.8% thought that their family approves of the desired behavior, 25.9% thought their community does, and only 17.4% thought society does. Similarly, the effect of others' expectations on the behavior of the adult respondents decreased with social distance from the individual. Sixty nine percent of respondents are affected by their family's expectations, while only 62.3 and 51.3% said they are affected by their community and society's expectations, respectively. Ultimately 58.4% (n = 263) reported high levels of personal stigmatization of children with disabilities. Table 3 presents the frequency results overall and by SEM level (see next section).
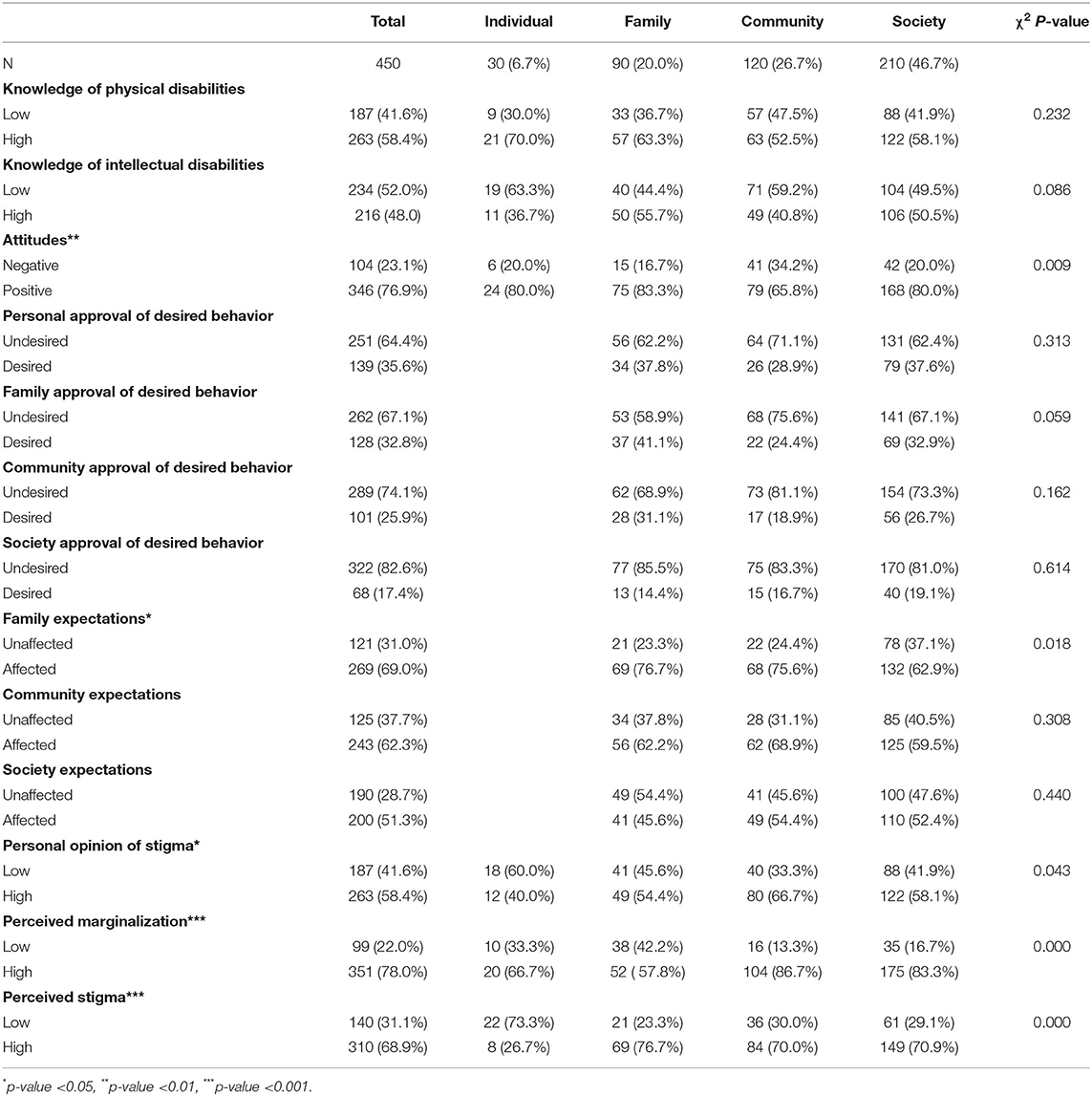
Table 3. Frequency results for all constructs in the conceptual model, by total and by social ecological model level.
Comparison by SEM
When the variables for each construct were analyzed by SEM level—individual, family, community, and society—many were not statistically significant. However, attitudes, family expectations, perceived stigma, perceived marginalization, and personal stigmatization all had statistically significant differences by SEM level.
Although not statistically significant, it is interesting to note that only 58.1% of professionals had high levels of knowledge of physical disabilities, which was less than both children with disabilities (70.0%) and their caregivers (63.3%). Similarly, fewer professionals had high levels of knowledge of intellectual disabilities than did caregivers of children with disabilities (50.5 vs. 55.7%, respectively).
There were statistically significant differences in proportions of SEM level with positive attitudes (p = 0.009). Community members had the lowest proportion of positive attitudes toward children with disabilities (65.8%), while caregivers of children with disabilities had the highest (83.3%). Eighty percent of professionals had positive attitudes, the same proportion as children with disabilities themselves.
Rates for approval of the desired behavior in the norms questions were similar across SEM levels for self, family, community, and society approval variables. Caregivers of children without disabilities had the lowest rates of approval of the desired behaviors for three of the approval variables: 28.9% for self-approval, 24.4% for family approval, and 18.9% for community. For belief that society approves of the desired behavior, caregivers of children with disabilities had the lowest proportion (14.4%).
Professionals (62.9%) were less affected by their family's expectations than caregivers of children with disabilities (76.7%) and caregivers of children without disabilities (75.6%) (p = 0.018). However, there were no statistically significant differences in the proportions affected by community and society expectations.
Community members (86.7%) and professionals (83.3%) perceived more marginalization than children with disabilities (66.7%) and their caregivers (57.8%) did (p = 0.000). There were also statistically significant differences in perceived stigma by SEM (p = 0.000). Only 26.7% of children with disabilities perceived high stigma, compared to 76.7% of caregivers of children with disabilities. About 70% of both community members and professionals perceived high levels of stigmatization of children with disabilities.
Bivariate Results
There were no statistically significant differences in personal stigmatization of children with disabilities by education, gender, or age. The odds of stigmatization increased with increasing income. Also compared to other respondents, children with disabilities were significantly less likely to display stigma toward other children with disabilities (OR = 0.45, p = 0.38). On the other hand, community members were at 1.61 times the odds of highly stigmatizing children with disabilities, as compared to all other respondents (p = 0.034).
When looking at the key constructs, knowledge of physical disabilities, attitudes, being affected by society's expectations, and perceived stigma were all significantly related to levels of personal stigmatization of children with disabilities. Counter to expectations, those with high levels of knowledge of physical disabilities were at higher odds of personally stigmatizing children with disabilities (OR = 1.78, p = 0.003). However, having positive attitudes toward children with disabilities was protective against highly stigmatizing children with disabilities (OR = 0.36, p = 0.000). Additionally, those who reported being highly affected by society's expectations were at almost twice the odds of highly stigmatizing children with disabilities (OR = 1.95, p = 0.001). Finally, those with high levels of perceived public stigmatization of children with disabilities were 7.49 times more likely of themselves highly stigmatizing children with disabilities (p = 0.000). Table 4 details the bivariate logistic regression results.
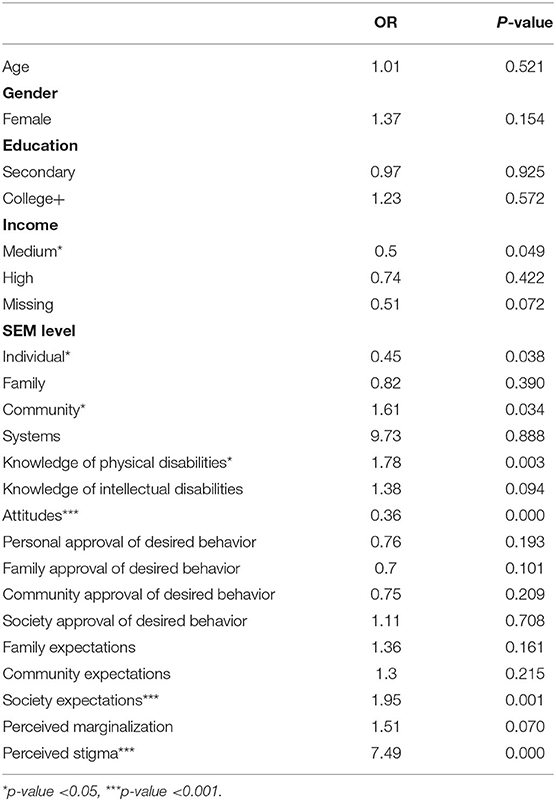
Table 4. Bivariate logistic regression results with stigma as the dependent variable.
Multivariate Results
Similar to the bivariate logistic regressions, the multivariate logistic regression showed significant differences in personal stigmatization of children with disabilities by correct knowledge of physical disabilities, attitudes, being affected by society's expectations, and perceived stigmatization of children with disabilities. When adjusting for all the variables in the model (age, gender, socioeconomic status, education, knowledge of physical disabilities, knowledge of intellectual disabilities, attitudes, descriptive norms, injunctive norms, perceived marginalization, and perceived stigma), those with high levels of knowledge of physical disabilities were at twice the adjusted odds of high levels of personal stigmatization of children with disabilities (AOR = 2.04, p = 0.011). Being affected by society's expectations and perceiving high levels of stigmatization of children with disabilities also led to increased adjusted odds of highly stigmatizing children with disabilities (AOR = 2.61, p = 0.004; AOR = 9.83, p = 0.000, respectively). On the other hand, those with positive attitudes had significantly lower adjusted odds of highly stigmatizing children with disabilities (AOR = 0.33, p = 0.002). The multivariate logistic regression results are shared in Table 5.
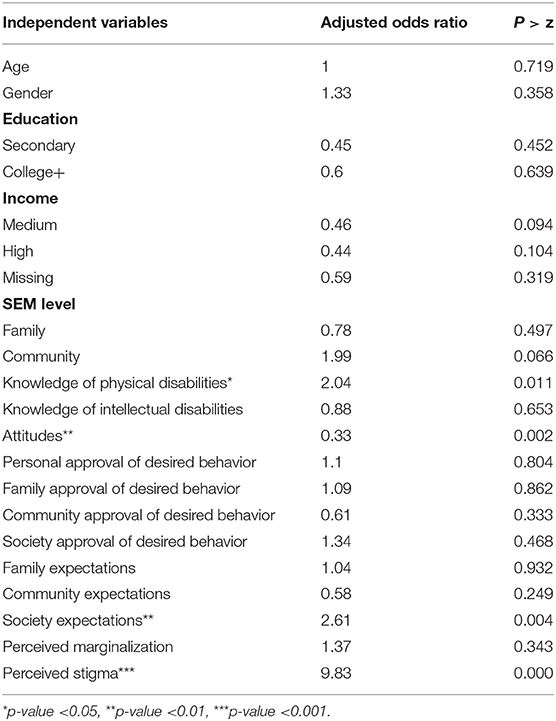
Table 5. Multivariate logistic regression results with stigma as the dependent variable.
Discussion
Four main conclusions can be drawn from the results of this study, all related to conceptualizing and addressing the treatment of children with disabilities from a systematic perspective. These include the comparison of professionals to nonprofessionals, the role of social norms in discrimination against children with disabilities, the ratings of community members across variables in the model, and the importance of addressing discrimination through multilevel approaches.
The first inference is that professionals concerned with children with disabilities, those highly educated and trained to work on issues to improve the treatment and protect the rights of children with disabilities, did not rate differently on the constructs of the model when compared to nonprofessionals. The professionals included in this study included health workers, teachers, school administrators, social workers, employees of civil society organizations, and government officials. One would anticipate, or at least hope, that more of these professionals would have high levels of knowledge of both physical and intellectual disabilities, that more would have positive attitudes, and that fewer would be affected by others' expectations when it comes to doing the “right” thing for children with disabilities. However, there were no notable differences in these variables when comparing the professionals to respondents in other levels of the SEM. In fact, though not statistically significant, fewer professionals had high levels of knowledge of physical disabilities than did children with disabilities and their caregivers; similarly, fewer professionals had high levels of knowledge of intellectual disabilities than did caregivers of children with disabilities. The undesired results for professionals are underscored by looking at the outcome variable: almost 60% of the professionals fell into the high personal stigmatization of children with disabilities category.
This finding, supported by the preexisting research that showed a lack of capacity of the professionals involved in supporting children with disabilities in North Macedonia, indicates a need for social and behavior change interventions targeting the systems level (Hollenweger, 2015). Training on technical aspects alone is not sufficient, though; if discrimination against children with disabilities is to be reduced, any interventions for professionals will need to be accompanied with communication messages that encourage destigmatizing. At the policy level, advocacy approaches, such as coalition-building, community mobilization, and communication of evidence-based justifications for programs, are often effective (Servaes and Malikhao, 2017). Advocacy approaches can offer an opportunity for the voices of children with disabilities themselves to be heard by centering their stories and experiences; such participation is a vital component of human-rights-based advocacy approaches (Callus and Camilleri Zahra, 2017). Social mobilization focused on uniting partners at the national and community levels for a common purpose would be especially beneficial, given that professionals in North Macedonia are often described as not collaborating (Hollenweger, 2015). However, since not all of the professionals work directly with policy, advocacy approaches should be combined with more targeted messaging to the individual professions, along with communication interventions for the general public. For example, teachers and administrators should be targeted with communication messages on inclusive education, while social and health workers involved in disability identification and registration could be targeted with messages about de-institutionalization.
Secondly, the results demonstrate that social norms associated with expectations of others are likely affecting the treatment of children with disabilities. Social scientists have wrestled with the concept of social norms for quite some time, specifically what they are, how they shape behavior, and how individuals and groups are influenced by norms. While sociologists tend to emphasize the role of norms in defining society and in dictating social behaviors, social psychologists have focused more on why individuals follow social norms (Marcus and Harper, 2015). It is not surprising that there is great diversity in how social norms have been conceptualized and continue to be understood.
Broadly speaking, social norms are the unwritten rules that guide human behavior; they are in other words, what we do, what we believe others do, and what we believe others think we should do [World Health Organization (WHO), 2010]. Social norms inherently require a reference group, i.e., a network of people to whom we identify and compare ourselves (Lapinski and Rimal, 2005). This reference group determines norms because identity with a specific group influences whether or not a behavior is considered normative within the group and, in turn, may predict whether or not a new behavior will be adopted (Goldstein et al., 2008).
Insofar as social norms are considered an inherent characteristic of individuals embedded within a larger social system, norms are rules or expectations held by social groups that guide behaviors (Mackie et al., 2015). Members of a group expect and are expected to follow and are motivated to follow norms because of expectations of sanctions for non-adherence and rewards for adherence. Two conditions have to be satisfied for a social norm to exist. First, individuals have to be aware of the norm and that it applies to them, and second, individuals conform to the norm if both of the following conditions are satisfied: they expect a majority of their social network to conform to the norm and they believe that a sufficiently large part of their social network think that they ought to conform to the norm and may sanction them if they do not. It is these expectations that keep people from “cheating” out of concern about what others will think of them and may do to them. In this definition of social norms, reciprocal expectations (norm of reciprocity) in which rewards and benefits received should also be returned, establishes an interdependence impacting the behavior of individuals within a social system.
One example of the existence of social norms within the study results is illustrated by examining the responses of community members for the descriptive and injunctive norms variables. Overall, fewer community members believed that their social networks approved of the desired behavior and more community members expressed being affected by their social networks. Coupled with the fact that community members were least likely to choose the desired behavior themselves, it is likely that discriminatory social norms are at least somewhat dictating how community members view and subsequently treat children with disabilities. In other words, the community members, specifically caregivers of children without disabilities, believe other people don't make the desired choice and believe that other people expect them to not make the desired choice, and subsequently are more likely to not make the desired choice.
Communication approaches in this context can address discriminatory norms toward children with disabilities by working at the community level to promote participatory deliberation on social justice for children with disabilities, the end result being that deliberations about the treatment of children with disabilities can lead to collective decisions and public commitments to improve systemic stigma. The underlying philosophy is that people need to see each other committing to change in order for change to occur.
The argument for normative influence in the treatment of children with disabilities is also supported by the trend of decreasing proportions of perceived approval of the desired behavior as the social distance from the individual increases (self > family > community > society). What this demonstrates is that people have their own opinions and are likely to be familiar with the opinions of those close to them. However, as one broadens the field and examines perceptions of people and institutions at the outer systems and policy levels of the SEM, individuals are less likely to know the “truth” and more likely to make assumptions about what these distant others think, feel, and do. In the absence of interpersonal communication, these false assumptions sustain themselves, making norms essentially a communication phenomenon (Berkowitz, 2004; Yanovitzky and Rimal, 2006). Therefore, one way to overcome this is through communicating to individuals that their beliefs are congruent with the larger majority. If norms are indeed a factor affecting levels of stigma, then communication activities are an essential component of programming to improve the treatment of children with disabilities.
The results also suggest that not enough emphasis has been placed on educating and involving community members to improve the treatment and protect the rights of children with disabilities. The respondents in this SEM level, both children without disabilities and their caregivers, had the lowest proportions of high levels of knowledge of physical and of intellectual disabilities, positive attitudes, and approval of the “desired” behavior in the norm's vignettes, as compared to all other SEM levels. While such results are to be expected—as, according to Intergroup Contact Theory, those without regular direct contact with children with disabilities are less likely to have positive attitudes and beliefs—they are not preferred (Pettigrew, 1998). Improving general community awareness and beliefs is especially important since community members as a whole are an integral part of the creation of the norms that continue to violate the human rights of children with disabilities.
Communication approaches have been successfully used by many organizations to raise communities' awareness and affect communities' attitudes (Johnson et al., 2005; Limani et al., 2018). Social change communications strategies at this level would need to emphasize dialogue and interpersonal communication. Some methods include the use of theater, animation, media, partnering with organizations to create education workshops, and empowering youth (UNICEF, 2016).
Finally, the results emphasize the importance of approaching disability from a comprehensive perspective. Even with the small sample size, there were statistically significant differences in level of personal stigmatization of children with disabilities in one indicator of every construct: knowledge of physical disabilities, attitudes, injunctive norms, and perceived stigma. If all constructs affect stigma, and thus affect discrimination and the violation of the basic rights of children with disabilities, then all are important when designing programs and interventions. This is especially important if norms are conceptualized as part of a larger equation of behavior and social change. In this theorizing, norms are considered to be an intermediate step that have to change in order to accomplish positive outcomes. The use of a broader social-ecological perspective in this type of theorizing situates individuals within their broader environment (inter-personal, community, institutional, societal etc.) and allows for analysis at different levels of influence and the development of strategies to impact them. A human rights-based approach to communication programming, is therefore grounded within larger social, political and cultural systems. Equally, it is important to monitor and evaluate all constructs in order to track the improvement in the realization of the fundamental rights of children with disabilities.
Limitations
As with every study, this study was not without limitations. Perhaps most significantly, the sample size was small. Although there were 450 participants in total, each of the specific 15 respondent types only had 30 participants. Even with combining respondents into aggregate SEM level groups, the children with disabilities level still only contained 30 people. Therefore, the small—and disproportionate among SEM levels—sample sizes could affect the ability to obtain statistically significant results. Further, the sample wasn't randomly selected and all of the participants were selected from within or adjacent to the capital city, meaning no rural participants were included. These methods of participant selection, along with the small sample sizes, make it likely that the sample is not representative of the population of North Macedonia. Additional larger studies are required to improve the generalizability of the results of this study, both to North Macedonia as a whole and to external contexts.
The small sample size also prevented data from being disaggregated in important ways. While some questions were asked about both intellectual and physical disabilities separately, some were asked about disability as a whole. There is much evidence that the constructs of this model would vary by specific type of disability, even beyond the broad categorization of physical and intellectual impairments. For example, a study by Snyder et al. (2010) found workers with non-physical disabilities reported significantly greater levels of procedural injustice and subtle discrimination. Future studies would benefit from having enough participants to look at knowledge, attitudes, norms, marginalization, and stigma separately by physical and intellectual impairments at a minimum. The ability to examine the intersectionality of social norms with gender, age, and education would also provide important insights. Specific programs would want to further expand their sample and disaggregate by the specific disabilities of most relevance to them. The ability to analyze and report data by specific type of professional would also be beneficial and allow for better understanding of the specific communication intervention needs of the different stakeholders: heath workers who are often responsible for diagnosing disability, teachers who are charged with including children with disabilities into their classrooms, civil society organizations that provide much needed social services, and government representatives who are responsible for establishing child friendly policies.
This study is also limited in that it relies on self-reported data, which was not externally validated. Self-reported data cannot be independently verified, which means the responses to the questions must be taken at face value. This type of data collection is subject to bias, as participants might feel the need to respond in a socially acceptable way or participants may provide answers without fully understanding the questions. Respondents might also not be able to recall their experiences accurately. To improve data validity, an observation component could be added to verify treatment of children with disabilities.
Missing data also affects the study. Most notably, neither children with disabilities nor children without disabilities were asked the norms questions. The questionnaire was long, because it was testing many ways of measuring the constructs, and pretesting showed a great need to shorten the tool to accommodate the needs of children. Given the complexity of the norm's questions, and the struggle of the children to understand them during pretesting, this set of questions was removed from the children's questionnaire. As a result, we are not able to discuss the normative factors from the children's perspectives, which has two implications. First, it reduces the already small sample size for analysis of norms and discrimination, limiting generalizability. Secondly, it diminishes the ability to center the voices of those impacted, which as previously stated, is critical in research with marginalized populations. It is imperative that a simplified way of measuring norms, of which children are capable of comprehending, is developed.
Finally, this research is able to make broad recommendations on the value of multi-level communication interventions that cut across the SEM to address stigma and discrimination among children with disabilities. However, it is not designed to make claims about types of interventions that may be more effective than others, except to point to the relevance of including children with disabilities themselves and addressing knowledge, attitudes, and normative factors that impact the behaviors of professionals charged with protecting these vulnerable children.
Conclusion
Global conversations around disability are improving the ideological framework that guides national policy and legislation to protect the rights of children with disabilities. However, North Macedonia, like many countries, has focused too much on creating systems to deal with inequities faced by children with disabilities and their families, without adequately addressing the knowledge, attitudes, norms, and practices of those who make the systems run. Future work needs to take a more holistic perspective, with attention paid to stakeholders at all levels of the SEM. With improved, more systematic research and employing comprehensive communication strategies, it is likely that the rights of children with disabilities can be respected and their treatment improved.
Data Availability Statement
The datasets generated for this study will not be made publicly available. The consent and assent forms indicated that the data would not be shared publicly.
Ethics Statement
The studies involving human participants were reviewed and approved by the Drexel University Institutional Review Board and Health Media Lab. Written informed consent to participate in this study was provided by all adult participants. Child participants gave verbal assent to participate, with written consent provided by their legal guardian/next of kin.
Author Contributions
SCS, SS, and KK contributed to conception and the design of the study, trained and oversaw the local research agency, and provided technical assistance throughout data collection. SCS and SS organized the database. SCS, SS, and NM performed the statistical analysis. SCS and NM wrote the first draft of the manuscript. All authors contributed to manuscript revision and read and approved the submitted version.
Funding
This research was funded by the UNICEF Europe and Central Asia Regional Office through an Institutional/Corporate Contract with Drexel University (Contract No. 43240294). The contract was issued under the Global Communication for Development Long-Term Arrangement for Services mechanisms, Category 1: Research and Analysis (LTAS No. 42104841).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to acknowledge and sincerely thank the research team at Indago for their crucial contributions to this research, by adapting the tools to the local context and facilitating the pretesting and data collection process. The Indago team includes, but is not limited to: Boge Bozinovski, Mevlija Grbovic, Ljupco Efremov, Diana Milenkovska, and Maja Milosevsk. The authors would also like to acknowledge and thank the UNICEF Europe and Central Asia Regional Office and the UNICEF North Macedonia Country Office for their overall support and technical guidance throughout the research process, especially Mario Mosquera, Sergio Tomsa, Lori Bell, Nora Shabani, Elspeth Erikson, Suzie Pappas-Capovska, and Marija Makrova. Finally, the authors would like to thank the disability and measurement experts who reviewed the tools for appropriateness and relevance, including Randall Sell, Paula Frederica Hunt, Judith Hollenweger Haskell, and Sheena Bell.
References
Ajzen, I. (1991). The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 50, 179–211. doi: 10.1016/0749-5978(91)90020-T
Berkowitz, A. (2004). The Social Norms Approach: Theory, Research, and Annotated Bibliography. Available online at: http://www.alanberkowitz.com/articles/social_norms.pdf (accessed March 9, 2020).
Bicchieri, C., Muldoon, R., and Sontuoso, A. (2018). Social Norms. Available online at: https://plato.stanford.edu/entries/social-norms/#Bib (accessed March 9, 2020).
Bickenbach, J. E., Chatterji, S., Badley, E. M., and Üstün, T. B. (1999). Models of disablement, universalism and the international classification of impairments, disabilities and handicaps. Soc. Sci. Med. 48, 1173–1187. doi: 10.1016/S0277-9536(98)00441-9
Byers, E., Valliere, F. R., and Houtrow, A. J. (2018). “Conceptualizing childhood disabilities,” in Opportunities for Improving Programs and Services for Children With Disabilities. Washington, DC: National Academies Press. Available online at: https://www.ncbi.nlm.nih.gov/books/NBK518922/ (accessed March 9, 2020).
Callus, A.-M., and Camilleri Zahra, A,. (2017). Nothing About Us Without Us': Disabled People Determining Their Human Rights Through the UNCRPD. Mediterranean Review of Human Rights. Available online at: https://www.researchgate.net/publication/321825985_Nothing_about_us_without_us'_disabled_people_determining_their_human_rights_through_the_UNCRPD (accessed March 9, 2020).
Cervasio, K. (2010). Systematic literature review of nursing students attitudes towards children with disabilities. J. Health Sci. Pract. 1, 1–16.
Corrigan, P., and Watson, A. (2002). Understanding the impact of stigma on people with mental illness. World Psychiatry 1, 16–20.
De Boer, A., Pijl, J., and Minnaert, A. (2012). Students' attitudes towards peers with disabilities: a review of the literature. Int. J. Disabi. Dev. Educ. 59, 379–392. doi: 10.1080/1034912X.2012.723944
Goldstein, N. J., Cialdini, R. B., and Griskevicius, V. (2008). A room with a viewpoint: using social norms to motivate environmental conservation in Hotels. J. Consum. Res. 35, 472–482. doi: 10.1086/586910
Green, S., Davis, C., Karshmer, E., Marsh, P., and Straight, B. (2005). Living stigma: the impact of label, stereotyping, separation, status loss, and discrimination in the lives of individuals with disabilities and their families. Sociol. Inq. 75, 197–215. doi: 10.1111/j.1475-682X.2005.00119.x
Hershkowitz, I., Lamb, M. E., and Horowitz, D. (2010). Victimization of children with disabilities. Am. J. Orthopyschiatry 77, 629–835. doi: 10.1037/0002-9432.77.4.629
Hibbard, R. A., and Desch, L. W. (2007). The Committee on Child Abuse and Neglect (CCAN), and Council on Children with Disabilities (CCWD). Maltreatment of children with disabilities. Pediatrics 119, 1018–1025. doi: 10.1542/peds.2007-0565
Hollenweger, J. (2015). Assessment of Capacity of Services Provided by Health, Education and Social Sectors for Inclusion of Children with Disabilities. UNICEF. Available online at: https://www.unicef.org/northmacedonia/reports/capacities-services-inclusion-children-disabilities (accessed March 9, 2020).
Hollenweger, J., and Martinuzzi, A. (2015). Towards a Cross-Sectoral Approach to Inclusion of Children with Disabilities: Policy Brief . UNICEF. Available online at: https://www.unicef.org/northmacedonia/reports/towards-cross-sectoral-approach-inclusion-children-disabilities (accessed March 9, 2020).
Johanson, G. A., and Brooks, G. P. (2010). Initial scale development: sample size for pilot studies. Educ. Psychol. Meas. 70, 394–400. doi: 10.1177/0013164409355692
Johnson, B. T., Maio, G. R., and Smith-McLallen, A. (2005). “Communication and attitude change: causes, processes, and effects,” in The Handbook of Attitudes, eds D. Albarracín, B. T. Johnson, and M. P. Zanna (Mahwah, NJ: Lawrence Erlbaum), 617–670.
Krieger, N. (2000). “Discrimination and health,” in Social Epidemiology, eds L. F. Berkman and I. Kawachi (Oxford: Oxford University Press, Inc), 36–75.
Lapinski, M. K., and Rimal, R. N. (2005). An explication of social norms. Commun. Theory 15, 127–147. doi: 10.1111/j.1468-2885.2005.tb00329.x
Limani, M., Cuizon, D., and Zeqiri, D. (2018). The Effectiveness of Social Behavior Change Communications (SBCC) in Changing Social Attitudes on Equal Rights to Property for Women—The Case of Kosovo. Prepared for 2018 World Bank Conference on Land and Poverty. Available online at: https://www.researchgate.net/profile/Driton_Zeqiri/publication/323358096_PAPER_FOR_WORLD_BANK_CONFERENCE_ON_LAND_AND_POVERTY_2018/links/5ae02fc2aca272fdaf8b7a1e/PAPER-FOR-WORLD-BANK-CONFERENCE-ON-LAND-AND-POVERTY-2018.pdf (accessed March 9, 2020).
Link, B., and Phelan, J. (2001). Conceptualizing stigma. Ann. Rev. Sociol. 27, 363–385. doi: 10.1146/annurev.soc.27.1.363
Mackie, G., Moneti, F., Shakya, H., and Denny, E. (2015). What are Social Norms? How Are They Measured. UNICEF/University of California, San Diego, Center on Global Justice. Available online at: http://www.unicef.org/protection/files/4_09_30_Whole_What_are_Social_Norms.pdf (accessed March 9, 2020).
Major, B., and O'Brien, L. T. (2005). The social psychology of stigma. Ann. Rev. Psychol. 56, 393–421. doi: 10.1146/annurev.psych.56.091103.070137
Manago, B., Davis, J. L., and Goar, C. (2017). Discourse in action: parent's use of medical and social models to reists disability stigma. Soc. Sci. Med. 184, 169–177. doi: 10.1016/j.socscimed.2017.05.015
Marcus, R., and Harper, C. (2015). Social Norms, Gender Norms and Adolescent Girls: A Brief Guide. Knowledge to Action Resource Series: ODI. Avaialble online at: https://www.odi.org/sites/odi.org.uk/files/odi-assets/publications-opinion-files/9818.pdf (accessed March 9, 2020).
Ministry of Labour Social Policy (MLSP) (2018). National Deinstitutionalisation Strategy for the Republic of Macedonia 2018-2027. Republic of Macedonia. Avaialble online at: http://www.mtsp.gov.mk/content/pdf/2019pravilnici/23.4_National%20Deinstitutionalisation%20Strategy%20and%20Action%20plan.pdf (accessed March 9, 2020).
Open the Windows (2014). Mapping of Disability Persons Organisations. UNICEF. Avaialble online at: https://www.unicef.org/northmacedonia/reports/mapping-disability-persons-organisations-report (accessed March 9, 2020).
Pettigrew, T. (1998). Intergroup contact theory. Ann. Rev. Psychol. 49, 65–85. doi: 10.1146/annurev.psych.49.1.65
Scior, K. (2011). Public awareness, attitudes and beliefs regarding intellectual disability: a systematic review. Res. Dev. Disabil. 32, 2164–2182. doi: 10.1016/j.ridd.2011.07.005
Servaes, J., and Malikhao, P. (2017). Advocacy strategies for health communication. Public Relat. Rev. 36, 42–49. doi: 10.1016/j.pubrev.2009.08.017
Snyder, L. A., Carmichael, J. S., Blackwell, L., Cleveland, J. N., and Thorton, G. C. (2010). Perceptions of discrimination and justice among employees with disabilities. Employee Responsibilities Rights J. 22, 5–19. doi: 10.1007/s10672-009-9107-5
Social Exclusion Knowledge Network (2008). Understanding and Tackling Social Exclusion: Final Report to the Who Commission on Social Determinants of Health From the Social Exclusion Knowledge Network. Available online at: https://www.who.int/social_determinants/knowledge_networks/final_reports/sekn_final~report_042008.pdf?ua=1 (accessed March 9, 2020).
Sood, S., Kostizak, K., Stevens, S., Cronin, C., Ramaiya, A., and Padidam, P. (2020). Measurement and conceptualisation of attitudes and social norms related to discrimination against children with disabilities: a systematic review. Int. J. Disabil. Dev. Educ. doi: 10.1080/1034912X.2020.1786022
Stuber, J., Meyer, I., and Link, B. (2008). Stigma, prejudice, discrimination and health. Soc. Sci. Med. 67, 351–357. doi: 10.1016/j.socscimed,.2008.03.023
UN General Assembly (1989). Convention on the Rights of the Child. Treaty Series (1577), 3. Available online at: https://www.refworld.org/docid/3ae6b38f0.html (accessed March 9, 2020).
UN General Assembly (2007). Convention on the Rights of Persons with Disabilities. Available online at: https://www.refworld.org/docid/45f973632.html (accessed March 9, 2020).
UNICEF (2013). Children and Young People with Disabilities Fact Sheet. Available online at: https://www.unicef.org/disabilities/files/Fact_Sheet_Children_and_Young_People_with_Disabilities_-_2013.pdf (accessed March 9, 2020).
UNICEF (2014). Knowledge, Attitudes and Practices (Kap) Survey towards Inclusion of Children with Disabilities. Available online at: https://www.unicef.org/northmacedonia/media/3511/file/MK_KAP_BaselineStudy_2014_Report_ENG.pdf (accessed March 9, 2020).
UNICEF (2015). Focus on Children with Disabilities in Central and Eastern Europe and Central Asia. Available online at: https://www.unicef.org/ceecis/1_children_with_disabilities_LR_v.8.2_(1).pdf (accessed March 9, 2020).
UNICEF (2016). Behaviour and Social Change. Available online at: https://www.unicef.org/cbsc/index_65736.html (accessed March 9, 2020).
UNICEF (2018). Disabilities: Introduction. Available online at: https://www.unicef.org/disabilities/ (accessed March 9, 2020).
UNICEF (2019). Communication for Development at UNICEF. Available online at: https://www.unicef.org/cbsc/index_42328.html (accessed March 9, 2020).
United Nations (2020). Status of Treaties: 11. Convention on the Rights of the Child. Available online at: https://treaties.un.org/Pages/ViewDetails.aspx?src=TREATYandmtdsg_no=IV-11andchapter=4andclang=_en (accessed February 2, 2020).
US Department of Health and Human Services (US DHHS) (1999). Mental Health: A Report of the Surgeon General – Executive summary. Rockville, MD: Department of Health and Human Services, US Public Health Service.
Van Brakel, W. H. (2007). Measuring health-related stigma—a literature review. Psychol. Health Med. 11, 307–334. doi: 10.1080/13548500600595160
Van Brakel, W. H., Sihombing, B., Djarir, H., Beise, K., Kusumawardhani, L., Yulihane, R., et al. (2012). Disability in people affected by leprosy: the role of impairment, activity, social participation, stigma and discrimination. Glob. Health Action 5:18394. doi: 10.3402/gha.v5i0.18394
Velichkovski, R., and Chichivalieva, S. (2010). Children With Disabilities in the Republic of Macedonia. Skopje: SEEHN.
World Health Organization (WHO) (2001). World Health Report 2001 Mental Health: New Understanding, New Hope. Geneva: WHO.
World Health Organization (WHO) (2002). Towards a Common Language for Functioning, Disability and Health: ICF. Available online at: https://www.who.int/classifications/icf/icfbeginnersguide.pdf (accessed March 9, 2020).
World Health Organization (WHO) (2010). Violence Prevention: The Evidence. Available online at: http://www.who.int/violence_injury_prevention/violence/4th_milestones_meeting/evidence_briefings_all.pdf (accessed March 9, 2020).
World Health Organization (WHO) World Bank (2011). World Report on Disability. Available online at: http://www.who.int/disabilities/world_report/2011/report.pdf (accessed March 9, 2020).
Keywords: disabilities, children, social norms, discrimination, communication, measurement
Citation: Stevens SC, Sood S, Mertz N and Kostizak K (2020) Measuring Discriminatory Social Norms Against Children With Disabilities to Improve Communication-Based Programs. Front. Commun. 5:541901. doi: 10.3389/fcomm.2020.541901
Received: 10 March 2020; Accepted: 30 November 2020;
Published: 21 December 2020.
Edited by:
Elizabeth M. Glowacki, Northeastern University, United StatesReviewed by:
Cristina García-Ael, National University of Distance Education (UNED), SpainSandhya Vishwas Limaye, Tata Institute of Social Sciences, India
Copyright © 2020 Stevens, Sood, Mertz and Kostizak. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Suruchi Sood, c3MzNzI0QGRyZXhlbC5lZHU=