 Teresa Nascimento1*
Teresa Nascimento1* João Inácio2
João Inácio2 Daniela Guerreiro1
Daniela Guerreiro1 Priscila Diaz3
Priscila Diaz3 Patrícia Patrício4
Patrícia Patrício4 Luís Proença1
Luís Proença1 Cristina Toscano5
Cristina Toscano5 Helena Barroso1
Helena Barroso1- 1Microbiology, Egas Moniz Center for Interdisciplinary Research (CiiEM), Egas Moniz School of Health & Science, Almada, Portugal
- 2School of Applied Sciences, University of Brighton, Brighton, United Kingdom
- 3Intensive Care Unit, Hospital Prof. Doutor Fernando da Fonseca, Amadora, Portugal
- 4Intensive Care Unit, Hospital Beatriz Ângelo, Loures, Portugal
- 5Clinical Pathology, Centro Hospitalar Lisboa Ocidental Hospital Egas Moniz, Lisboa, Portugal
Introduction: Candida auris is an emerging pathogen that represents a worldwide health problem due to its global expansion, multidrug resistance, and difficult laboratory identification. Among the risk factors for colonization/infection by C. auris, a stay in an intensive care unit (ICU) stands out. This prospective multicenter study aimed to monitor the trend of the local epidemiology of Candida spp. and unveil the prevalence of C. auris.
Methods: From 2020 to 2022, axillar/inguinal swabs were collected from adult patients at three points: upon admission (D1) and on the fifth (D5) and eighth (D8) days of their ICU stay. We employed culture-based screening methods combined with molecular techniques to identify Candida spp. down to the species level. Specific screening for Candida auris was conducted using a real-time PCR assay in combination with an improved selective culture medium, mannitol salt agar auris (MSAA). To validate the effectiveness of MSAA, a collection of reference C. auris strains representing the four major geographical clades was used.
Results: We enrolled 675 patients, and 355 Candida isolates were retrieved from the 988 swab samples collected. From those, 185/355 (52.1%) were identified as C. albicans and 170/355 (47.9%) as non-albicans Candida (NAC). MSAA medium showed a specificity of 94.8%, albeit C. auris was not detected in this cohort. The dynamics of Candida spp. colonization by ICU were significant at the three collection points. Upon admission, C. albicans was associated with the Beatriz Ângelo Hospital ICU (p=0.003) and C. tropicalis with the general Hospital Professor Doutor Fernando Fonseca (FFH) ICU (p=0.006). C. parapsilosis and C. lusitaniae were associated with FFH ICUs, with the general ICU at D5 (p=0.047) and surgical ICU at D8 (p=0.012). The dynamics of NAC colonization by ICU were significantly different at D1 (p=0.011), D5 (p=0.047), and D8 (p=0.012).
Conclusion: We developed and implemented a screening protocol for C. auris while uncovering the colonization patterns of Candida in the ICU. Our findings contribute to the optimization of overall patient management, ensuring that ICU protocols are resilient and adaptive to emerging fungal threats.
1 Introduction
In the intensive care unit (ICU), patients are at heightened risk for healthcare-associated infections due to factors such as invasive procedures, weakened immune systems, and prolonged hospital stays (Thomas-Rüddel et al., 2022). Candida species, including the emerging multidrug-resistant Candida auris, are prominent pathogens that contribute to these infections through skin colonization (Soriano et al., 2023; Lass-Flörl et al., 2024).
Despite the predominant feature of colonization, C. auris candidemia usually follows colonization and presents mortality rates up to 70%, resulting in this species, together with C. albicans, being listed on the World Health Organization (WHO) critical priority group of fungal pathogens (WHO, 2022). Candida species are the third leading cause of nosocomial bloodstream infections and reducing their transmission is an important aspect of ICU care (Poissy et al., 2022).
Given the critical importance of accurately screening and identifying Candida strains, systematic surveillance in high-risk settings, particularly among ICU patients, is essential (Ahmad and Asadzadeh, 2023). Global surveillance efforts have been implemented to monitor the spread and characteristics of C. auris across all continents (Worth et al., 2020; Contreras and Morgan, 2022; Taori et al., 2022; Piatti et al., 2022; de Melo et al., 2023; Rowlands et al., 2023; Vinayagamoorthy et al., 2022). However, the lack of C. auris surveillance in countries with low prevalence presents significant challenges to global public health, as undetected introductions and potential outbreaks could occur, leading to delayed responses and increased transmission. In this context, several studies highlight the importance of screening high-risk patients upon ICU admission, particularly those with a history of healthcare exposure in foreign hospitals (Worth et al., 2020; Briano et al., 2022; Ahmad and Asadzadeh, 2023). The early identification of potential community-acquired cases is crucial in preventing C. auris colonization and minimizing the risk of subsequent infections (Lass-Flörl et al., 2024).
Current methods such as polymerase chain reaction (PCR), matrix-assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS), and DNA sequencing are not universally accessible, require specialized expertise, and are time-intensive (Keighley et al., 2021; Maldonado et al., 2018). C. auris poses significant laboratory challenges due to frequent misidentification by standard microbiology assays and automated systems (Jones et al., 2024; de Cássia Orlandi Sardi et al., 2018). Real-time PCR and DNA sequencing are typically required for reliable identification, with the sequencing of specific DNA regions like the D1/D2 of 28S rDNA or internal transcribed spacer (ITS) helping to differentiate C. auris clades (Lockhart et al., 2022). Given these challenges, it is crucial to encourage and support the establishment of C. auris surveillance programs in a cost-effective manner. This involves providing affordable diagnostic tools to ensure that emerging cases are detected and managed swiftly. To address this gap, we aimed to assess the pattern of Candida colonization in ICU patients and unveil the prevalence of C. auris.
2 Methods
2.1 Study design
This prospective multicenter study was conducted from January 2020 to December 2022, in suburban Lisbon, at two large tertiary hospitals belonging to the Portuguese National Public Health Service: Hospital Professor Doutor Fernando Fonseca (FFH), an 802-bed hospital with two ICUs (general and surgery), and Beatriz Ângelo Hospital (BAH), a 424-bed hospital with one general ICU. Participation in the study was voluntary and authorized by signing an informed consent form. All patients under the age of 18, pregnant women, and mentally disabled individuals were not included in the study. Collection was made in the context of a daily chlorhexidine gluconate (CHG) 2% and 4% (v/v) bathing routine infection control practice. All patients had at least one CHG bath prior to swab collection, with a daily bath for the first 5 days of stay.
The sampling from each patient was performed using a non-invasive bilateral axillary/inguinal combine swab. Collection was made upon the admission of patients to the ICU (D1) and continued during the ICU stay, one the fifth day (D5) and eighth day (D8), when applicable.
Swabs were collected in a 1 ml ∑-Transwab® system transport (Sigma Transwab-Liquid Amies) and processed within 48 h, using mycological cultural and molecular-based methods simultaneously.
2.2 The C. auris surveillance protocol with culture-based methods
Briefly, for cultural methods, 50 µl aliquots of the suspensions were spread directly onto appropriate culture media: Sabouraud Gentamicin Chloramphenicol 2 agar (SDA) (bioMérieux, Marcy l’Etoile, France) and a commercially available Candida chromogenic medium (CHROMagar ™ Candida, CHROMagar, Paris, France). The plates were incubated aerobically for 48 h, one set of plates at 25°C and a second set at 37°C (Figure 1).
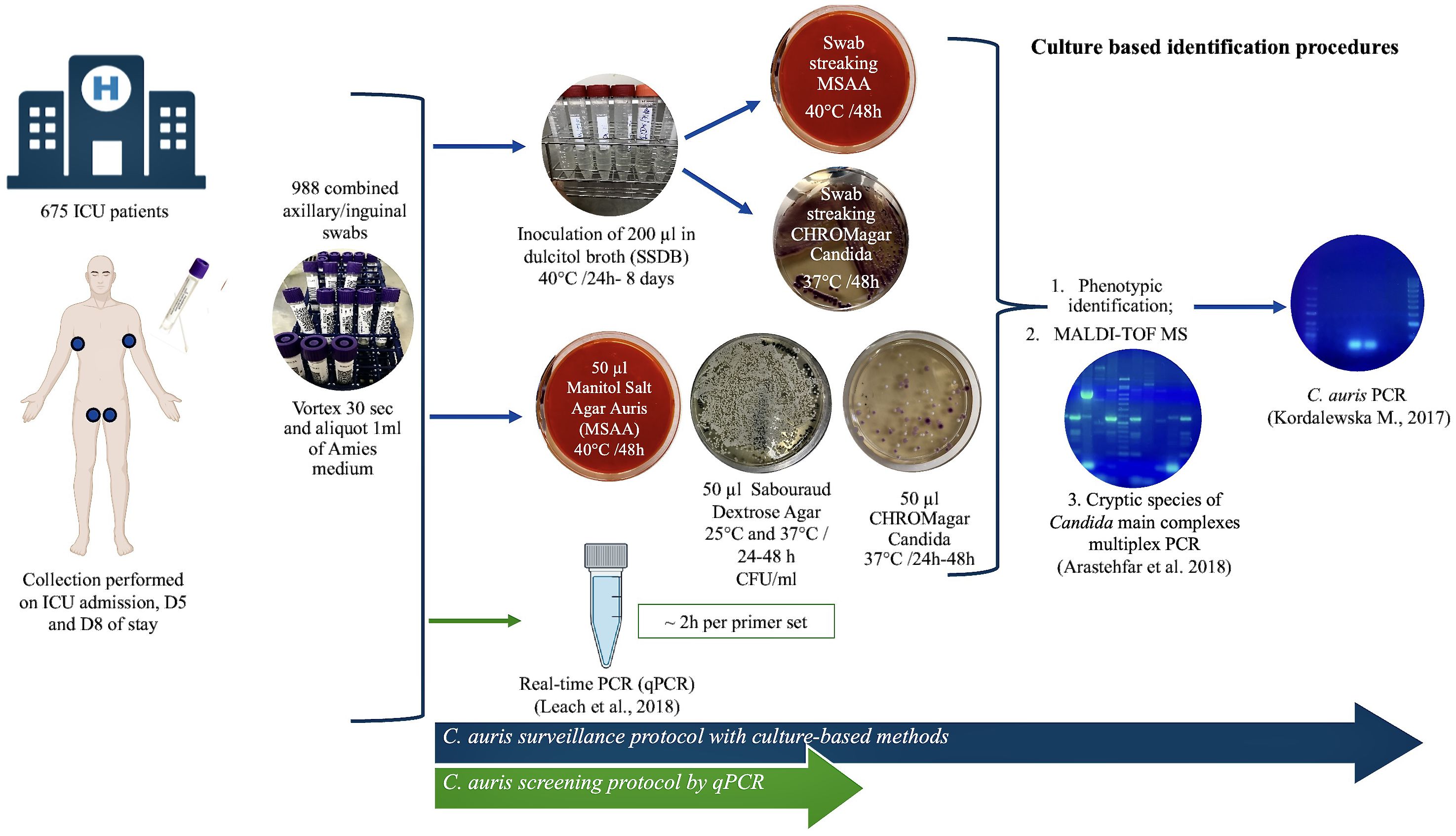
Figure 1. Scheme of the mycological algorithm used to screen Candida auris. The algorithm for the molecular identification of C. auris from clinical isolates (blue arrow). C. auris screening from surveillance samples using a specific real-time PCR (green arrow).
2.2.1 Species identification
The presumptive identification of isolates was based on standard criteria of macroscopic and microscopic morphology, growth temperature, the biochemical profile of aerobic sugar assimilation, and the appearance on chromogenic agar (Figure 1). All isolates were further processed for analysis with MALDI-TOF MS—VITEK MS (bioMérieux, Marcy l’Etoile, France) using VITEK MS v3.2 software (Sarvestani et al., 2022). All identifications displaying a single result with a confidence value of 99.9% were considered acceptable (Figure 1).
Molecular methods were employed to analyze the three Candida species complexes (C. albicans, C. glabrata, and C. parapsilosis) most linked to human infections. The protocol, optimized from the one developed by Arastehfar et al., was designed to simultaneously identify cryptic species within the C. albicans, C. glabrata, and C. parapsilosis complexes (Arastehfar et al., 2018). Additionally, all Candida isolates were subjected to a PCR assay specific for C. auris (Kordalewska et al., 2017). For this purpose, total DNA was extracted from the isolates using an NZYMicrobial gDNA Isolation Kit® (Nzytech, Lisboa, Portugal), following the manufacturer’s instructions. The PCRs were performed using a T100 thermal cycler (Bio-Rad Laboratories, Hercules, CA, USA). The amplified products were analyzed on 2% agarose gels stained with GreenSafe (NZYtech, Lisboa, Portugal) and visualized using a UV transilluminator (Figure 1).
2.2.2 C. auris screening with mannitol salt agar auris
Aliquots of 50 μl of the swab suspensions were spread directly on an in-house selective medium for C. auris (MSAA) (Figure 1) adapted from the enrichment broth developed by Welsh et al (Welsh et al., 2017). The base of the MSAA medium was SDA supplemented with gentamicin and chloramphenicol to a 50 mg/l final concentration, to which 10% NaCl (wt./vol), 2% mannitol (wt./vol), and phenol red indicator solution, adjusted to pH 5.9, were added (Nascimento et al., 2021). A positive test result was defined as the presence of visible colony growth (yellow colonies) after 24–48 h of incubation at 40°C. A C. auris DSM 105987 suspension was used as positive control, prepared from a 48 h SDA culture to a concentration of 1.0 McFarland. Additionally, 200-μl aliquots of the swab suspensions were inoculated into Salt Sabouraud Dulcitol Broth (SSDB) containing dulcitol, supplemented with chloramphenicol, gentamycin, and 10% of sodium chloride for 24 h to 8 days at 40°C with shaking at 250 rpm and observed daily for turbidity. In this study, the enrichment broth was reproduced based on the description published by the Centers for Disease Control and Prevention (CDC, 2022). All the SSDB tubes after the maximum incubation time were re-inoculated (swab streaked) onto CHROMagar Candida® and MSAA for 48 h at 37°C and 40°C, respectively. The results were recorded considering any colony growth on the plates and colony color (Figure 1).
2.2.2.1 Validation of MSAA medium
A panel of C. auris strains representative of the four major geographical clades were obtained from the Deutsche Sammlung von Mikroorganismen (DSMZ; Braunschweig, Germany): C. auris DSMZ 21987, representative of South Asia Clade (I); DSMZ 105986, for the East Asia Clade (II); DSMZ 105988, for the South Africa Clade (III); and DSMZ 105990, for the South America Clade (IV). Other yeasts used to validate the MSAA medium were Candida albicans ATCC 60193, Candida tropicalis ATCC 1369, Nakaseomyces glabrata (formerly known as Candida glabrata) ATCC 15126, Candida parapsilosis ATCC 22019, Pichia kudriavzevii (formerly known as Candida krusei) ATCC 6258, Candida haemulonii DSMZ 70624, Candida duobushaemulonii CBS 7798, Cutaneotrichosporon mucoides (Trichosporon mucoides) ATCC 204094, and clinical isolates of Clavispora lusitaniae (formerly known as Candida lusitaniae) and Saccharomyces cerevisiae. All cultures were streaked onto MSAA medium using as inoculum yeast suspensions in 0.85% (v/v) saline solution adjusted to 1–5 × 106 cells/ml (OD530nm: 0.128; 0.5 McFarland standard). The MSAA medium was also inoculated with all the surveillance swab sample suspensions, with and without pre-enrichment in SSDB (Figure 1), to evaluate its specificity to differentiate C. auris from other species often found as commensal organisms on the skin.
The sensitivity of the MSAA medium to detect C. auris at low concentration levels was assessed using serial dilutions of all the C. auris reference strains and other culture collection yeast strains listed above. Yeast suspensions adjusted to 1–5 × 105 cells/mL (OD530nm: 0.020; 0.1 McFarland standard) were prepared and spotted in a grid fashion onto MSAA medium. The plates were incubated for 48 h at 40°C, and the appearance of the colonies was recorded after 24 and 48 h. All suspensions were also spotted onto SDA plates, which were incubated for 48 h at 30°C, as a positive control for organism viability.
2.3 C. auris screening by qPCR
In addition to the culture-based workflow for C. auris screening, 100-µl aliquots of the vortexed swab samples were processed with a highly accurate real-time PCR (qPCR) protocol as described previously by Leach et al. (Figure 1) (Leach et al., 2018). Briefly, genomic DNA was extracted from bilateral axilla and inguinal swab suspensions using an NZY Soil gDNA Isolation kit® (Nzytech, Lisbon, Portugal) according to the manufacturer’s instructions. Each PCR run on the Qiagen Rotor-Gene Q included a positive extraction (C. auris DSM105986; 103 CFU/50 μl) and positive amplification (C. auris DSM105990; 0.02 pg/l) controls, as well as negative extraction (reagents only) and negative amplification (sterilized nuclease-free water) controls.
2.4 Statistical analysis
Data analysis was carried out through descriptive and inferential methodologies using the IBM SPSS Statistics v. 29.0 (IBM Corp., Armonk, NY, USA) software. A p-value < 0.05 was considered statistically significant for all the above inferential analyses.
3 Results
3.1 Surveillance samples
A total of 675 patients were enrolled in the study: in 2020, 64 and 71 patients, respectively, from the general and surgical FFH ICU, and in 2021–2022, 540 patients from the BAH ICU. For 203 and 110 patients, samples were collected, respectively, within 5 (D5) and 8 (D8) days after admission to the ICU. Overall, 988 swab samples were collected from the cohort: 217 in 2020, 231 in 2021, and 532 in 2022.
3.2 Candida auris screening and the identification of isolates
C. auris screening by qPCR assay and culture-based methods was negative for the 988 samples. However, 371 yeast isolates were obtained from 329 culture positive samples, of which 355 corresponded to Candida species.
The overall results showed that Candida albicans remains the most frequently isolated species, representing 185 out of 355 isolates (52.1%), indicating a nearly equal distribution between C. albicans and non-albicans Candida (NAC) species. Among the NAC species, C. parapsilosis complex ranked second (30.7%), followed by C. glabrata in third (10.1%) (Table 1).
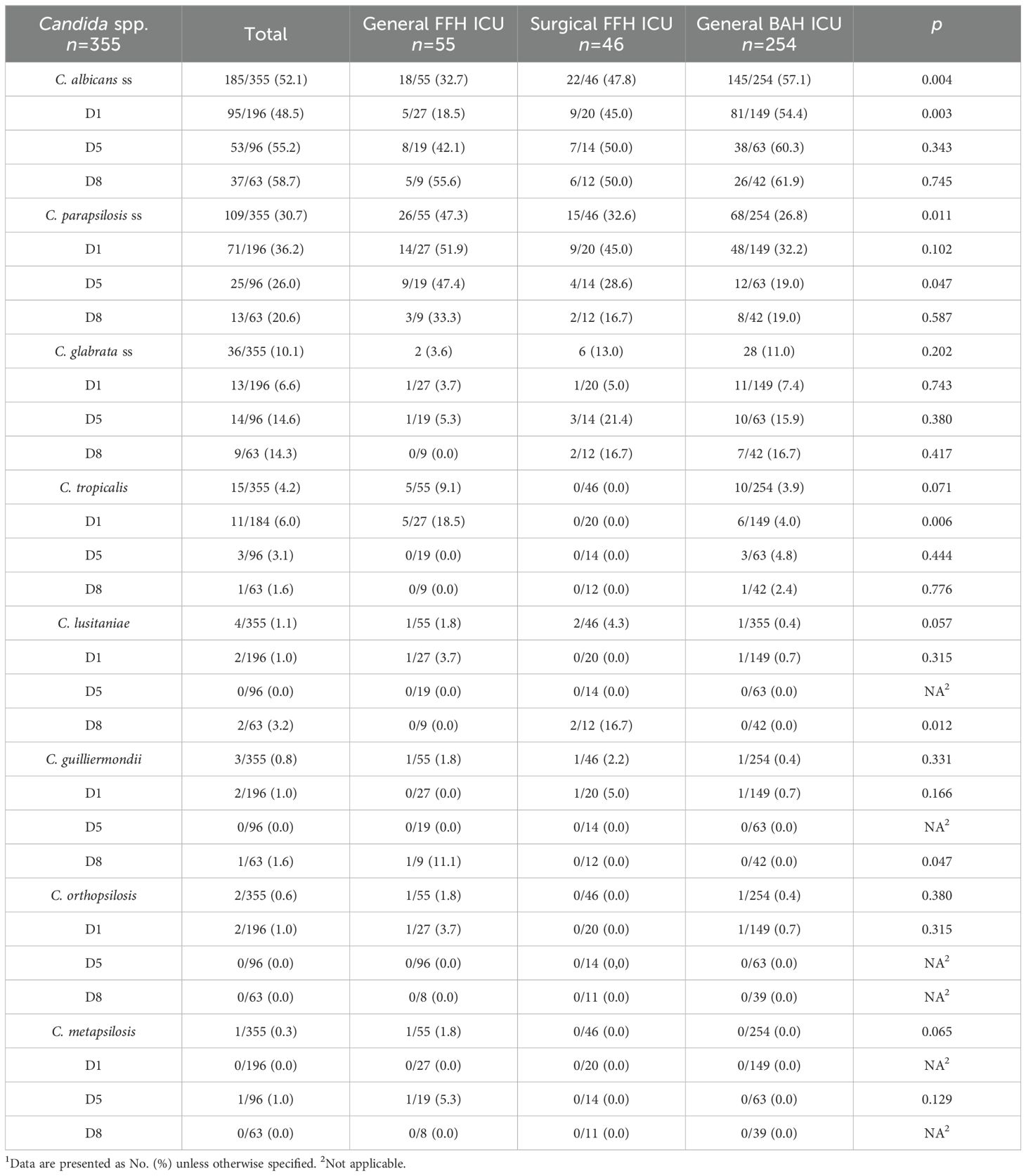
Table 1. Candida spp. isolates distribution by collection day and ICU1.
If we particularize by hospital unit, 61 out of 101 isolates (60.4%) in the FFH ICUs were NAC species, compared with 109 out of 254 isolates (42.9%) in the BAH ICU. In terms of the distribution of C. albicans versus NAC species during the first week of hospitalization, there was a slight increase in C. albicans isolates across all ICUs, rising from 48.5% on day 1 to 55.2% on day 5, and 58.7% by day 8 (Table 1).
When analyzing the distribution of Candida species by ICU and hospital unit, species diversity was lower in the surgical FFH ICU. In contrast, both the general BAH and FFH ICUs exhibited the presence of all identified Candida species, although the percentage distribution of each species varied significantly (Figure 2).
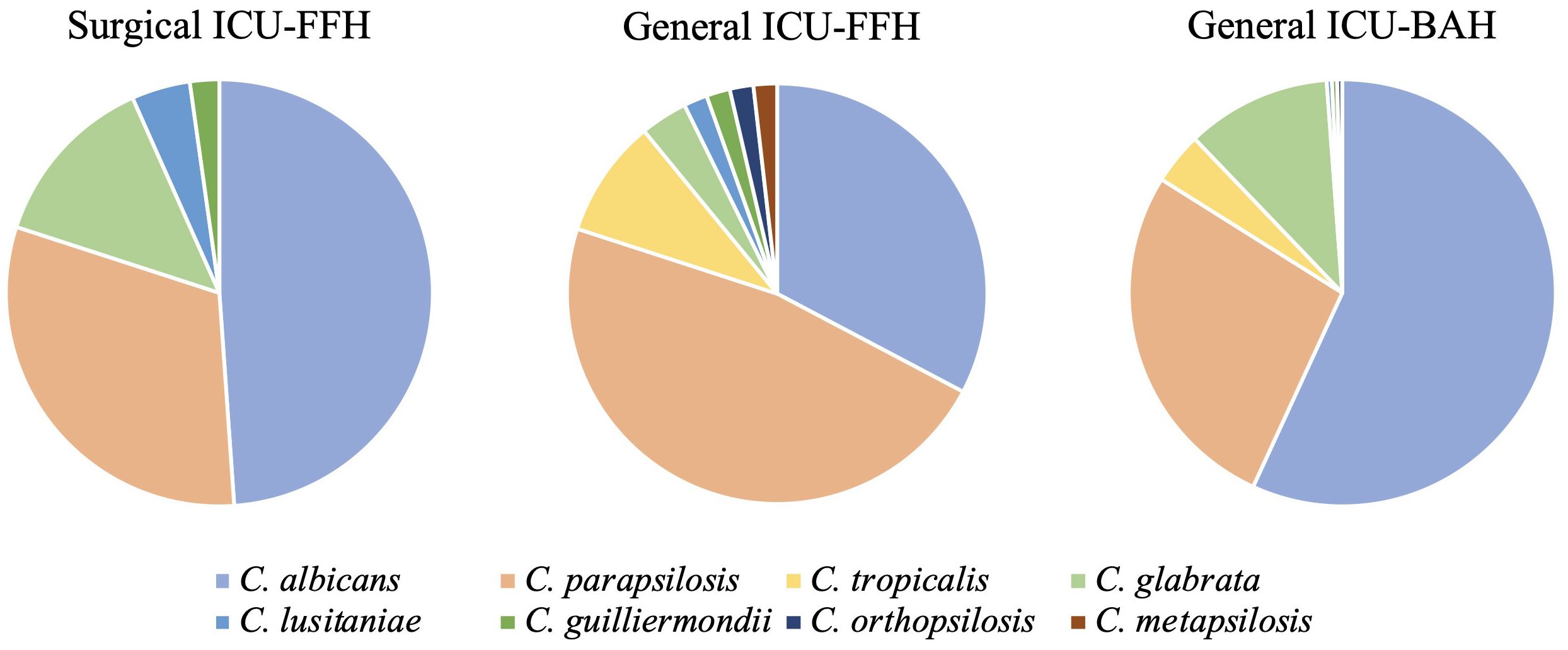
Figure 2. Distribution of Candida spp. isolates by ICU (general and surgical FFH and General BAH).
The dynamics of Candida spp. colonization by ICU were significant at the three-point collections. Upon admission, C. albicans was associated with the BAH ICU (p=0.003). C. parapsilosis ranked second overall, except in the general ICU of the FFH, where it became the most prevalent species, representing 47.3% of isolates (p=0.011). Cryptic isolates from the C. parapsilosis complex were detected exclusively in the general ICUs of both the FFH and BAH, although this finding lacked statistical significance (Table 1). Interestingly, C. tropicalis was absent from all collection points in the surgical ICU of FFH. Despite the low number of C. tropicalis isolates overall, its distribution was significantly associated with the general ICU of FFH upon admission (p=0.006) (Table 1). Additionally, C. parapsilosis and C. lusitaniae were associated with specific collection points in the FFH ICUs. C. parapsilosis showed a significant association with the general ICU on day 5 (p=0.047), whereas C. lusitaniae was significantly linked to the surgical ICU on day 8 (p=0.012) (Table 1).
Regarding the prevalence of Candida species, no significant month-to-month variations were observed during the collection period within the same hospital (Figures 3A, B). This suggests a consistent presence of Candida spp. throughout the year, without notable fluctuations in colonization rates across different months.
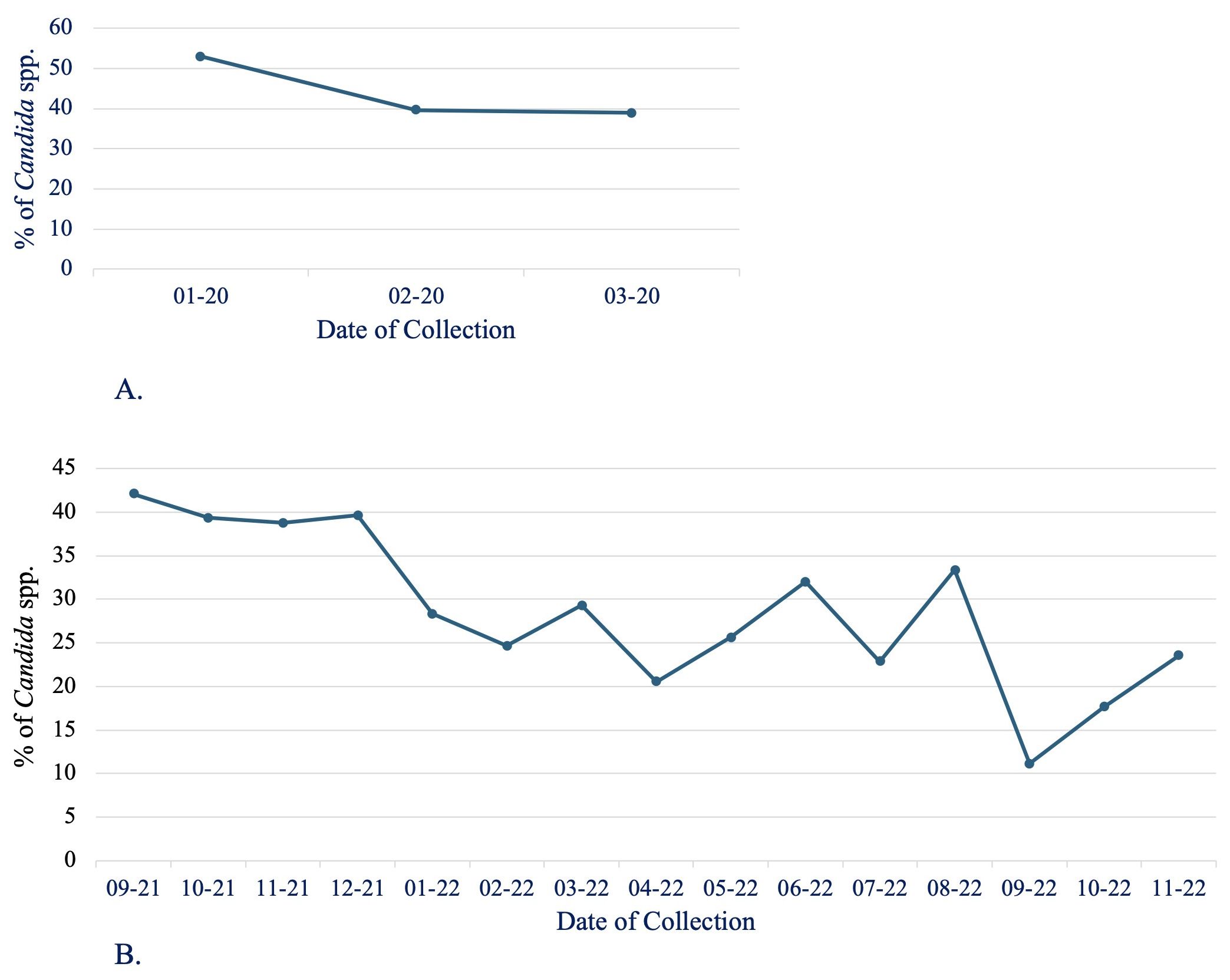
Figure 3. Distribution of Candida spp. isolates by month and hospital ICU. (A) General and surgical FFH and (B) General BAH.
However, a broader analysis over a 3-year period revealed a noticeable decrease in the percentage of Candida-positive samples, dropping from 44.7% in 2020 to 40.2% in 2021, and further down to 25.6% in 2022. Although this downward trend was evident, it did not reach statistical significance, implying that although there may be a reduction in Candida prevalence, the change is not robust enough to rule out the possibility of random variation.
3.3 Specificity and sensitivity of the MSAA medium
Regarding the evaluation of the MSAA medium for the selective and differential isolation of C. auris control strains, after 48 h of incubation at 40°C, small yellow colonies were observed for the strains representing the major phylogeographic clades of C. auris (Clade I, II, III, and IV), whereas none of the remaining yeast species could grow on the same medium (Figure 4A). It is worth mentioning that C. auris DSM 105986 (East Asia: Japan, clade II) was the slowest growing strain. All strains grew on SDA plates and CHROMagar Candida, evidenced by the formation of white to cream and pink colonies, respectively, assuring the viability of all cultures (Figure 4B). Phylogenetically related species, such as C. haemulonii and C. duobushaemulonii, did not grow on the MSAA medium (Figures 4A.1, A.2). Similarly, the remaining 10 reference strains of other yeast species showed no growth on this selective medium at 40°C during the same incubation period.
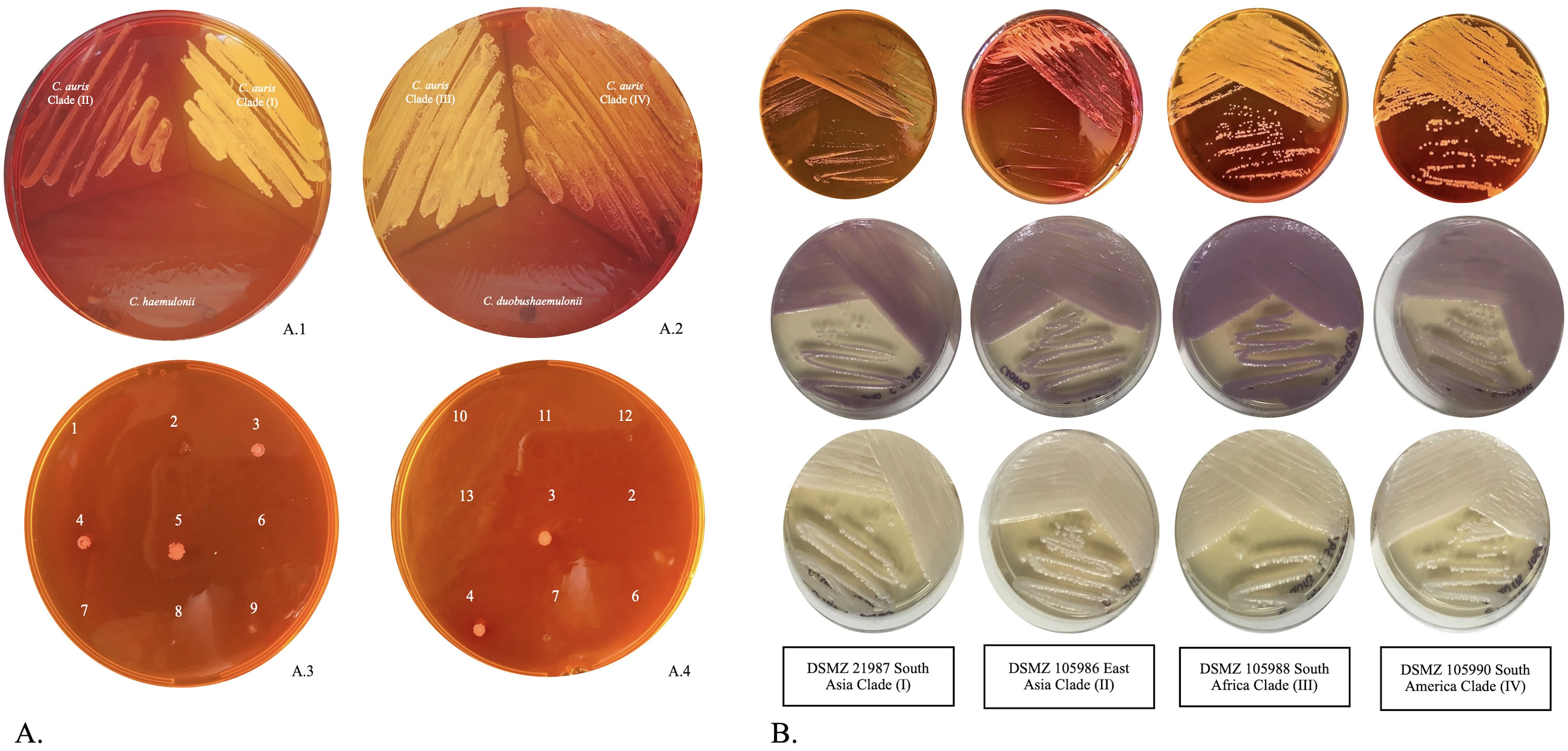
Figure 4. (A, A.1) MSAA plate inoculated with C. auris DSMZ 105986 (Clade II) and DSMZ 105987 (Clade I), and Candida haemulonii DSMZ 70624); (A.2) MSAA plate inoculated with C. auris DSMZ 105988 (Clade III) and DSMZ 105990 (Clade IV), and Candida duobushaemulonii CBS 7798. The MSAA plates were incubated for 48 h at 40°C; (A.3, A.4) MSAA sensitivity, growth at 0.1 McFarland. The Candida spp. tested were: 1 = Candida albicans; 2 = Candida duobushaemulonii; 3 = C. auris DSMZ 105990 (Clade IV); 4 = C. auris DSMZ 105987 (Clade I); 5 = C. auris DSMZ 105988 (Clade III); 6 = Candida haemulonii DSMZ 70624; 7 = Candida glabrata; 8 = Candida parapsilosis; 9 = C. auris DSMZ 105986 (Clade II); 10 = Candida krusei; 11= Candida tropicalis; 12 = Trichosporon mucoides; and 13 = Saccharomyces cerevisiae. (B) Macroscopic observation of C. auris clades I, II, III, and IV after 48 h of incubation at 37°C. MSAA plates inoculated by streaking from suspensions with 106 CFU/ml of the control strains (top row). In CHROMagar Candida, C. auris cultures usually develop an appearance of various shades of pink (center row). On Sabouraud Dextrose Agar (SDA), the colonies generally remain white and creamy (bottom row).
Regarding sensitivity, the examination of MSAA plates with grid inoculation revealed consistent results even at low dilutions (standard suspension of 0.1 McFarland). For various Candida species, as well as S. cerevisiae and T. mucoides, MSAA revealed no growth for any of the isolates after 24 h of incubation, including C. auris. However, after 48 h of incubation, strains representing the geographical clades of C. auris exhibited growth, with the appearance of yellow colonies [Figures 4A.3, A.4, (compare inoculation points 1–13)]. The SDA plates used as controls to verify the viability of the isolates displayed creamy white colonies for all the reference strains, thereby validating the reliability of the MSAA medium results (Figure 4B). Based on these findings, the sensitivity of the MSAA medium for the presumptive detection of C. auris was determined after a 48-h incubation period, yielding a sensitivity of 100%.
3.4 The detection of presumptive C. auris isolates with culture-based methods
SSDB and MSAA media showed growth after inoculation with 51 and 21 surveillance swab samples, respectively. All MSAA-positive plates also evidenced turbidity in the enrichment broth. However, the SSDB yielded positive results for an additional 30 samples (Table 2).
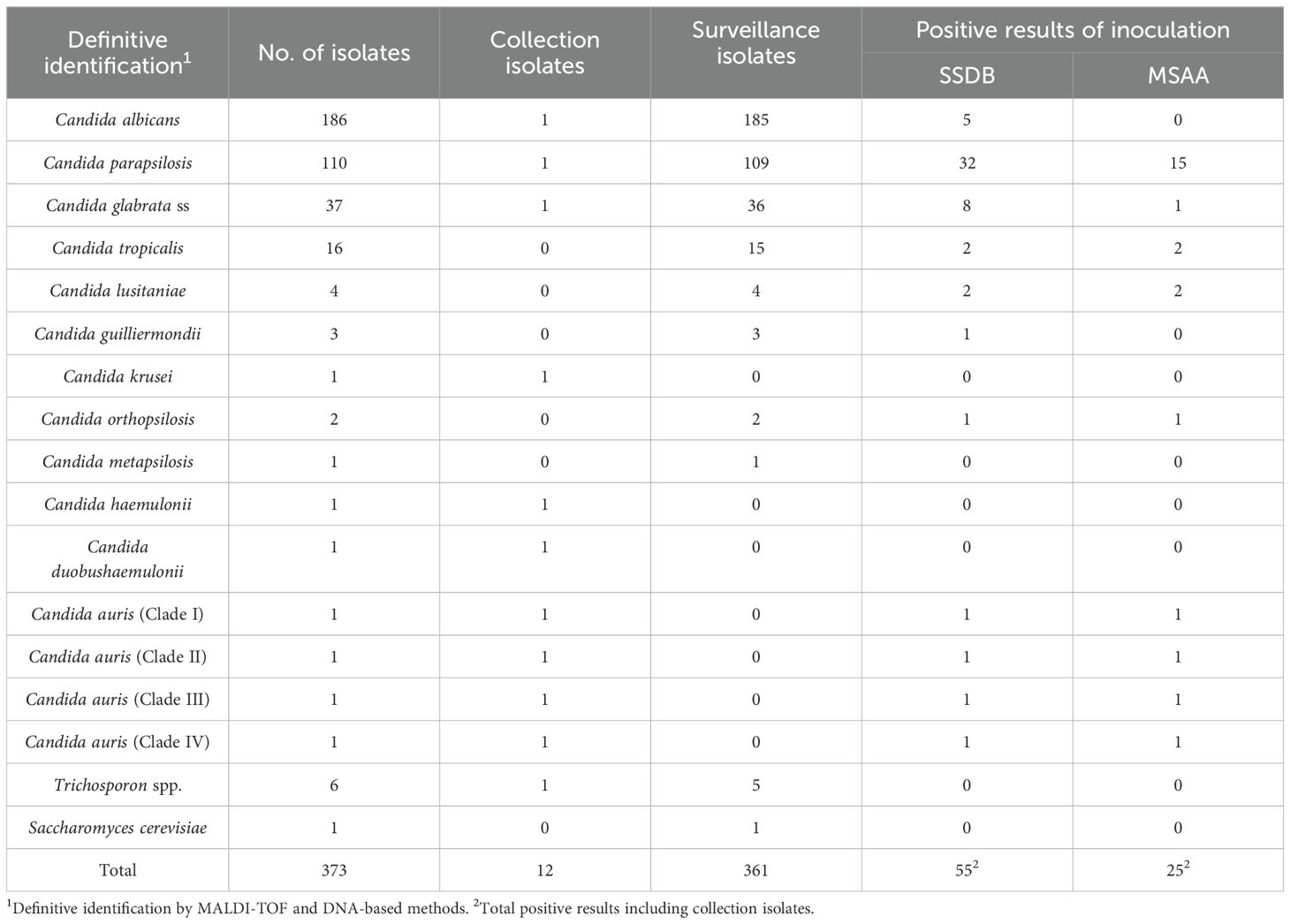
Table 2. Presumptive identification results obtained with culture media (SSDB and MSAA) used to screen for C. auris vs. definitive identification.
The isolates retrieved from these two media were identified by MALDI-TOF MS as C. glabrata, C. tropicalis, C. lusitaniae, C. guilliermondii, C. parapsilosis, and C. orthopsilosis. The definitive identification of the isolates of C. glabrata and C. parapsilosis complexes was obtained using multiplex PCR. This identification was identical to that obtained from the primary isolation media used in the fungal colonization screening protocol. However, 16 samples were considered positive only after being cultured in the enrichment broth. Among the isolates from these samples, two of C. lusitaniae, five of C. glabrata, and nine of C. parapsilosis were retrieved. From these 16 samples, after transferring from dulcitol broth to CHROMagar Candida and MSAA, growth was observed only in MSAA for two samples, which were identified as C. lusitaniae.
The results of the cultural and molecular examination of combined axillary/inguinal mucosa swabs are summarized in Table 2. No sample with growth on either MSAA or SSDB was confirmed as positive for C. auris by MALDI-TOF or PCR. Based on these results, the specificities of SSDB and MSAA culture alone for the presumptive detection of C. auris from swab samples were 88.5% and 94.8%, respectively.
4 Discussion
Our results highlight the variability of Candida species frequency depending on the local hospital epidemiology, and our study evidenced the importance of the ICU type (surgery vs. general), as already mentioned by other authors (Guinea et al., 2014). Findings from this work are in line with previous studies (carriage/infection) worldwide, showing that C. albicans still ranks as the main yeast colonizer on ICU patients but, in the last decade, a change in favor of NAC has been observed in the ICU (Sasso et al., 2017; Boattini et al., 2023).
Sequential sampling to assess the dynamics of Candida species over time revealed stable results, with a tendency toward the prevalence of C. albicans over NAC species. This stability in colonization patterns aligns with previous longitudinal studies that used respiratory tract samples (Willger et al., 2014; Krause et al., 2016). Our results demonstrate that C. albicans consistently maintained colonization, reinforcing the established understanding of its virulence factors. C. albicans is known to possess the most extensive range of virulence traits among Candida species, enabling it to persist and maintain long-term viability within the host (Staniszewska, 2020). In contrast, NAC species were more often associated with transient colonization, with species turnover observed between ICU admission and collection after 1 week of hospitalization (day 8).
The observed decline in Candida spp. prevalence between 2020 and 2022 could be attributed to several factors, including improvements in infection control practices, shifts in patient demographics, or the impact of external influences such as the COVID-19 pandemic, which altered hospital admission patterns and antimicrobial usage. However, the lack of statistical significance in this trend indicates that further data collection and extended observation periods are needed to determine whether this decline is truly meaningful or simply part of natural variability. Understanding these trends is essential for guiding future surveillance efforts, optimizing infection control strategies, and anticipating potential changes in Candida prevalence within hospital settings.
The Candida parapsilosis complex was prevalent (31.5%) among NAC species, in agreement with previous studies that showed C. parapsilosis as the second most common species after C. albicans found at Southern European hospitals (Portugal, Spain, Italy, and Greece) (Castanheira et al., 2020; Boattini et al., 2023). It is worth noting that C. parapsilosis ranked first at admission for one ICU (p=0.011). This cohort of patients was enrolled in our study before the COVID-19 pandemic, and we may point to the reinforcement of infection control measures taken during the pandemic years, as the hands of healthcare professionals are recognized as a major vector for C. parapsilosis nosocomial acquisition.
Of the 36 isolates identified as C. glabrata, all strains were confirmed to be C. glabrata stricto sensu. These findings align with other studies that have investigated the presence of cryptic species within the glabrata complex and found no evidence of their existence (Kaan et al., 2021; Nasri et al., 2023). Only cryptic species of the C. parapsilosis complex were isolated. These results point to a stability in the distribution and emergence of cryptic species in the ICU setting in Portugal (Faria-Ramos et al., 2014).
C. tropicalis is typically derived from the gastrointestinal tract, which may account for its low prevalence of only 4.2% among the Candida isolates. Additionally, C. lusitaniae was identified in the cohort at a frequency of 1.1%, with a significant association found in the FFH surgical ICU (p=0.012). This pattern reflects similar findings reported in Portugal, where C. lusitaniae was present at a prevalence of 2.6% (Pinto-Magalhães et al., 2019).
Our screening to unveil C. auris in ICU patients relied on qPCR given the critical need for rapid identification to implement public health measures promptly. Nonetheless, MSAA medium showed a specificity of 94.8%, albeit C. auris was not detected in this cohort. Commercial culture media used to differentiate C. auris from other Candida species also presented misidentification issues. Although CHROMagar Candida Plus C. auris can identify all C. auris strains, other species were misidentified as C. auris, such as C. parapsilosis complex species (Taverna et al., 2023). Additional selective media were described for the isolation of C. auris (Ibrahim et al., 2021; Das et al., 2021). As for MSAA, these selective media are based on the yeast growth conditions: thermo-resistance and halo-tolerance (Jeffery-Smith et al., 2018). MSAA has less inhibitors (as we used a 40°C incubation temperature instead of 42°C and 10% of sodium chloride instead of 12.5%) and stable conservation (4°C) after medium preparation compared with medium described by Das et al., which requires fresh preparation (Das et al., 2021). All C. auris strains representing different major clades were able to grow on MSAA plates. However, as for the study by Das et al., the C. auris clade II strain showed limited growth even after 48 h of incubation time, due to its longer doubling time at 42°C (Das et al., 2021). Over the SCA described by Ibrahim et al., MSAA has the advantage of reading at 48 h instead of 72 h (Ibrahim et al., 2021).
In our study, MALDI-TOF MS-based identifications showed total agreement with molecular procedures, reinforcing other authors who stated that MALDI-TOF MS systems can correctly identify C. auris in most cases (Mahmoudi et al., 2019). Overall, our results show that when qPCR is not available, the MSAA medium can be used for the routine screening of C. auris. The MSAA medium can be easily prepared, is straightforward to use as it does not require mycological or molecular expertise, and provides a simple and cost-effective tool for the detection and presumptive identification of C. auris in the clinical microbiology laboratory. From these findings, the proposed workflow to identify C. auris based on culture-based methodologies associated with the molecular identification of the isolates is a good option and allows antifungal susceptibility tests to be performed.
To the best of our knowledge, this prospective study is the first surveillance study for C. auris colonization in Portuguese tertiary hospital ICUs. One major strength is that it is specifically designed to screen for C. auris in a cohort of patients from two large hospital centers in the suburban Lisbon region. For over 2 years, our findings showed that C. auris is not prevalent in Portuguese hospitals. Our findings align with other prospective screening studies, namely from the UK (Sharp et al., 2021), Egypt (Khairat et al., 2021), and Germany (Heindel et al., 2022), which also reported no C. auris colonization among ICU patients. Additionally, our results are consistent with observations from Europe and North America, where C. auris colonization and infection in ICUs are typically sporadic and often associated with nosocomial outbreaks (Pacilli et al., 2020; Worth et al., 2020; Eckbo et al., 2021; Piatti et al., 2022). However, the situation is markedly different in India, where C. auris has become the leading Candida species isolated from the blood of critically ill patients, with a notable increase in cases during the COVID-19 pandemic (Shastri et al., 2020; Sharma and Chakrabarti, 2023).
In Europe, new C. auris cases were mainly diagnosed during the COVID-19 pandemic, particularly in Spain (n=591), Italy (n=291), and Greece (n=71) (Kohlenberg et al., 2022). Nevertheless, several studies carried out all over Europe in recent years reported only isolated cases of C. auris in hospital units, such as with the first Portuguese clinical case (Kohlenberg et al., 2022; Henriques et al., 2023). Furthermore, a multicentric retrospective study including all candidemia case isolates from six Southern European tertiary hospitals did not find C. auris (Boattini et al., 2023). In a 2022 prospective screening study by Contreras et al., C. auris isolates were recovered from critically ill patients with complicated clinical conditions who had a history of medical care not only in intensive care units but also in long-term care facilities (Contreras and Morgan, 2022). Similarly, the CDC’s pilot study on C. auris screening in several healthcare facilities across New York City between 2017 and 2019 found that colonizing isolates were predominantly obtained from patients in long-term care facilities and senior residences (Rowlands et al., 2023).
As the patients in these two hospitals did not remain in the ICU for extended periods (e.g., a median of 5 days), they may not have been exposed to the cumulative risks that typically lead to C. auris colonization. A shorter stay reduces the likelihood of encountering contaminated environments, decreases the time exposed to other colonized patients, and limits the use of invasive devices that could serve as entry points for C. auris. The absence of C. auris colonization in the two hospitals could indeed be due to the relatively short duration of hospital stays among the participants. This aligns with existing literature that indicates a higher risk of C. auris colonization after prolonged hospital or ICU stays, typically at approximately or after 20 days (Corcione et al., 2022). Das et al. (2018) highlighted a critical observation that patients in ICU settings typically acquired C. auris infections after a period of 15 to 20 days (Das et al., 2018).
Another potential limitation of our study was the collection of samples from only two sites for C. auris screening in the ICU setting. This approach may have reduced detection effectiveness, as Rowlands et al. (2023) emphasized the importance of including nasal swabs alongside bilateral axillary/inguinal mucosal sampling for comprehensive screening (Rowlands et al., 2023). Additionally, the study collected fewer swabs than anticipated (988 instead of 1,350) due to its premature termination. This early conclusion was influenced by several factors, including logistical challenges and external events, which resulted in fewer patients being swabbed than initially planned. Specifically, in the two ICUs at FFH, the study was halted prematurely in March 2020 due to the onset of the COVID-19 pandemic. The pandemic disrupted hospital research activities, leading to an early end to the study. At BAH, from October 2022 onwards, staff shortages created significant difficulties in continuing the study, particularly in the collection of swabs. These staffing limitations ultimately forced an early end to the research. Understanding the specific reasons behind these premature terminations is crucial for planning and designing future research studies.
Although C. auris colonization currently appears to be uncommon in Portuguese hospitals, Portugal has seen a significant increase in the number of immigrants from areas endemic for C. auris. This trend raises concerns about the possibility of the fungus being introduced and spread in the country and suggests that Portuguese hospitals should consider the protocol presented for an active screening.
Considering the above findings, this study, along with the various studies cited in the Discussion, underscores the need to implement C. auris screening alongside existing protocols for nosocomial microorganisms such as methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus, and carbapenemase-producing Gram-negative bacteria. It is recommended that nasal and rectal swabs, in addition to axillary and inguinal swabs, be utilized for more comprehensive screening. Furthermore, screening should be systematically extended beyond the ICU to include palliative care units to enhance the early detection and management of C. auris.
In conclusion, by integrating molecular technologies with traditional culture assays, a screening protocol for C. auris was developed and implemented. This protocol involves initial screening using MSAA to identify potential C. auris isolates, followed by confirmation using traditional PCR or MALDI-TOF MS. Through our study, we also uncovered the colonization pattern of Candida in the ICU and contributed to the optimization of overall patient management.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Institutional Ethics Committee of Hospital Prof. Doutor Fernando Fonseca (59/2019, 13/11/2019) 265 and the Institutional Ethics Committee of Hospital Beatriz Ângelo (3655/2021, 21/07/2021). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
TN: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. JI: Supervision, Writing – original draft, Writing – review & editing. DG: Investigation, Methodology, Writing – review & editing. PD: Investigation, Methodology, Writing – review & editing. PP: Investigation, Methodology, Writing – review & editing. LP: Formal analysis, Methodology, Supervision, Writing – review & editing. CT: Investigation, Methodology, Writing – review & editing. HB: Conceptualization, Formal analysis, Funding acquisition, Investigation, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The authors thank FCT/MCTES for the financial support to CiiEM (10.54499/UIDB/04585/2020) through national funds.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Ahmad, S., Asadzadeh, M. (2023). Strategies to prevent transmission of candida auris in healthcare settings. Curr. Fungal Infect. Rep. 17, 36–48. doi: 10.1007/s12281-023-00451-7
Arastehfar, A., Fang, W., Pan, W., Liao, W., Yan, L., Boekhout, T. (2018). Identification of nine cryptic species of Candida albicans, C. glabrata, and C. parapsilosis complexes using one-step multiplex PCR. BMC Infect. Dis. 18, 480. doi: 10.1186/s12879-018-3381-5
Boattini, M., Pinto, M. F., Christaki, E., Fasciana, T., Falces-Romero, I., Tofarides, A., et al. (2023). Multicentre surveillance of candida species from blood cultures during the SARS-CoV-2 pandemic in southern Europe (CANCoVEU project). Microorganisms 11, 560. doi: 10.3390/microorganisms11030560
Briano, F., Magnasco, L., Sepulcri, C., Dettori, S., Dentone, C., Mikulska, M., et al. (2022). Candida auris candidemia in critically ill, colonized patients: cumulative incidence and risk factors. Infect. Dis. Ther. 11, 1149–1160. doi: 10.1007/s40121-022-00625-9
Castanheira, M., Deshpande, L. M., Messer, S. A., Rhomberg, P. R., Pfaller, M. A. (2020). Analysis of global antifungal surveillance results reveals predominance of Erg11 Y132F alteration among azole-resistant Candida parapsilosis and Candida tropicalis and country-specific isolate dissemination. Int. J. Antimicrob. Agents 55, 105799. doi: 10.1016/j.ijantimicag.2019.09.003
CDC (2022).Centers for disease control and prevention. Available online at: https://www.cdc.gov/fungal/candida-auris/index.html (Accessed January 15, 2023).
Contreras, D. A., Morgan, M. A. (2022). Surveillance diagnostic algorithm using real-time PCR assay and strain typing method development to assist with the control of C. auris amid COVID-19 pandemic. Front. Cell Infect. Microbiol. 12, 887754. doi: 10.3389/fcimb.2022.887754
Corcione, S., Montrucchio, G., Shbaklo, N., De Benedetto, I., Sales, G., Cedrone, M., et al. (2022). First cases of candida auris in a referral intensive care unit in piedmont region, Italy. Microorganisms 10, 1521. doi: 10.3390/microorganisms10081521
Das, S., Singh, S., Tawde, Y., Chakrabarti, A., Rudramurthy, S. M., Kaur, H., et al. (2021). A selective medium for isolation and detection of candida auris, an emerging pathogen. J. Clin. Microbiol. 59, 10-1128. doi: 10.1128/JCM.00326-20
Das, S., Tigga, R., Rai, G., Singh, P. K., Datt, S., Tyagi, A., et al. (2018). Candida auris colonization in an immunocompetent patient: A new threat in medical ICU. Med. Mycol Case Rep. 21, 54–56. doi: 10.1016/j.mmcr.2018.05.004
de Cássia Orlandi Sardi, J., Silva, D. R., Soares Mendes-Giannini, M. J., Rosalen, P. L. (2018). Candida auris: Epidemiology, risk factors, virulence, resistance, and therapeutic options. Microb. Pathog. 125, 116–121. doi: 10.1016/j.micpath.2018.09.014
de Melo, C. C., de Sousa, B. R., da Costa, G. L., Oliveira, M. M. E., de Lima-Neto, R. G. (2023). Colonized patients by Candida auris: Third and largest outbreak in Brazil and impact of biofilm formation. Front. Cell Infect. Microbiol. 13, 1033707. doi: 10.3389/fcimb.2023.1033707
Eckbo, E. J., Wong, T., Bharat, A., Cameron-Lane, M., Hoang, L., Dawar, M., et al. (2021). First reported outbreak of the emerging pathogen Candida auris in Canada. Am. J. Infect. Control 49, 804–807. doi: 10.1016/j.ajic.2021.01.013
Faria-Ramos, I., Neves-Maia, J., Ricardo, E., Santos-Antunes, J., Silva, A. T., Costa-de-Oliveira, S., et al. (2014). Species distribution and in vitro antifungal susceptibility profiles of yeast isolates from invasive infections during a Portuguese multicenter survey. Eur. J. Clin. Microbiol. Infect. Dis. 33, 2241–2247. doi: 10.1007/s10096-014-2194-8
Guinea, J., Zaragoza, Ó., Escribano, P., Martín-Mazuelos, E., Pemán, J., Sánchez-Reus, F., et al. (2014). Molecular identification and antifungal susceptibility of yeast isolates causing fungemia collected in a population-based study in Spain in 2010 and 2011. Antimicrob. Agents Chemother. 58, 1529–1537. doi: 10.1128/AAC.02155-13
Heindel, J., Zweigner, J., Fuchs, F., Hamprecht, A. (2022). Usefulness of screening for Candida auris colonisation in international patients admitted to a large university hospital. Mycoses. 66, 138-143. doi: 10.1111/myc.13533
Henriques, J., Mixão, V., Cabrita, J., Duarte, T. I., Sequeira, T., Cardoso, S., et al. (2023). Candida auris in intensive care setting: the first case reported in Portugal. J. Fungi (Basel) 9, , 837. doi: 10.3390/jof9080837
Ibrahim, A., Peyclit, L., Abdallah, R., Khelaifia, S., Chamieh, A., Rolain, J. M., et al. (2021). SCA medium: A new culture medium for the isolation of all Candida auris clades. J. Fungi (Basel) 7, 433. doi: 10.3390/jof7060433
Jeffery-Smith, A., Taori, S. K., Schelenz, S., Jeffery, K., Johnson, E. M., Borman, A., et al. (2018). Candida auris: a review of the literature. Clin. Microbiol. Rev. 31, 10-1128. doi: 10.1128/CMR.00029-17
Jones, C. R., Neill, C., Borman, A. M., Budd, E. L., Cummins, M., Fry, C., et al. (2024). The laboratory investigation, management, and infection prevention and control of Candida auris: a narrative review to inform the 2024 national guidance update in England. J. Med. Microbiol. 73, 001820. doi: 10.1099/jmm.0.001820
Kaan, Ö., Koç, A. N., Atalay, M. A., Mutlu Sarigüzel, F. (2021). Molecular epidemiology, antifungal susceptibility and virulence factors of Candida glabrata complex strains in Kayseri/Turkey. Microb. Pathog. 154, 104870. doi: 10.1016/j.micpath.2021.104870
Keighley, C., Garnham, K., Harch, S. A. J., Robertson, M., Chaw, K., Teng, J. C., et al. (2021). Candida auris: diagnostic challenges and emerging opportunities for the clinical microbiology laboratory. Curr. Fungal Infect. Rep. 15, 116–126. doi: 10.1007/s12281-021-00420-y
Khairat, S. M., Anany, M. G., Ashmawy, M. M., Hussein, A. F. A. (2021). Setting a Protocol for Identi cation and Detecting the Prevalence of Candida auris in Tertiary Egyptian Hospitals Using the CDC Steps. Macedonian J. Med. Sci. 14, 397–402. doi: 10.3889/oamjms.2021.6095
Kohlenberg, A., Monnet, D. L., Plachouras, D., C. a. s. c. group & C. a. s. c. g. i. t. f. n. experts (2022). Increasing number of cases and outbreaks caused by Candida auris in the EU/EEA 2020 to 2021. Euro Surveill 27, 2200846. doi: 10.2807/1560-7917.ES.2022.27.46.2200846
Kordalewska, M., Zhao, Y., Lockhart, S. R., Chowdhary, A., Berrio, I., Perlin, D. S. (2017). Rapid and accurate molecular identification of the emerging multidrug-resistant pathogen Candida auris. J. Clin. Microbiol. 55, 2445–2452. doi: 10.1128/JCM.00630-17
Krause, R., Moissl-Eichinger, C., Halwachs, B., Gorkiewicz, G., Berg, G., Valentin, T., et al. (2016). Mycobiome in the lower respiratory tract - A clinical perspective. Front. Microbiol. 7, 2169. doi: 10.1371/journal.pone.0155033
Lass-Flörl, C., Kanj, S. S., Govender, N. P., Thompson, G. R., Ostrosky-Zeichner, L., Govrins, M. A. (2024). Invasive candidiasis. Nat. Rev. Dis. Primers 10, 20. doi: 10.1038/s41572-024-00503-3
Leach, L., Zhu, Y., Chaturvedi, S. (2018). Development and validation of a real-Time PCR assay for rapid detection of Candida auris from surveillance samples. J. Clin. Microbiol. 56, 10-1128. doi: 10.1128/JCM.01223-17
Lockhart, S. R., Lyman, M. M., Sexton, D. J. (2022). Tools for detecting a "Superbug": updates on Candida auris testing. J. Clin. Microbiol. 60, e0080821. doi: 10.1128/jcm.00808-21
Mahmoudi, S., Agha Kuchak Afshari, S., Aghaei Gharehbolagh, S., Mirhendi, H., Makimura, K. (2019). Methods for identification of Candida auris, the yeast of global public health concern: A review. J. Mycol Med. 29, 174–179. doi: 10.1016/j.mycmed.2019.04.004
Maldonado, I., Cataldi, S., Garbasz, C., Relloso, S., Striebeck, P., Guelfand, L., et al. (2018). Identification of Candida yeasts: Conventional methods and MALDI-TOF MS. Rev. Iberoam Micol 35, 151–154. Red de Micología de la Ciudad Autónoma de Buenos Aires (RMCABA) & R. d. M. d. l. C. A. d. B. Aires. doi: 10.1016/j.riam.2018.02.002
Nascimento, T., J., I., P., D., H., B. (2021). Mannitol salt agar auris: a useful medium for differentiating Candida auris. ESCMID eAcademy.
Nasri, E., Vaezi, A., Falahatinejad, M., Rizi, M. H., Sharifi, M., Sadeghi, S., et al. (2023). Species distribution and susceptibility profiles of oral candidiasis in hematological Malignancy and solid tumor patients. Braz. J. Microbiol. 54, 143–149. doi: 10.1007/s42770-022-00863-6
Pacilli, M., Kerins, J. L., Clegg, W. J., Walblay, K. A., Adil, H., Kemble, S. K., et al. (2020). Regional Emergence of Candida auris in Chicago and Lessons Learned From Intensive Follow-up at 1 Ventilator-Capable Skilled Nursing Facility. Clin. Infect. Dis. 71, e718–e725. doi: 10.1093/cid/ciaa435
Piatti, G., Sartini, M., Cusato, C., Schito, A. M. (2022). Colonization by Candida auris in critically ill patients: role of cutaneous and rectal localization during an outbreak. J. Hosp Infect. 120, 85–89. doi: 10.1016/j.jhin.2021.11.004
Pinto-Magalhães, S., Martins, A., Lacerda, S., Filipe, R., Prista-Leão, B., Pinheiro, D., et al. (2019). Candidemia in a Portuguese tertiary care hospital: Analysis of a 2-year period. J. Mycol Med. 29, 320–324. doi: 10.1016/j.mycmed.2019.08.002
Poissy, J., Rouzé, A., Cornu, M., Nseir, S., Sendid, B. (2022). The changing landscape of invasive fungal infections in ICUs: A need for risk stratification to better target antifungal drugs and the threat of resistance. J. Fungi (Basel) 8, 946. doi: 10.3390/jof8090946
Rowlands, J., Dufort, E., Chaturvedi, S., Zhu, Y., Quinn, M., Bucher, C., et al. (2023). Candida auris admission screening pilot in select units of New York City health care facilities 2017-2019. Am. J. Infect. Control 51, 866–870. doi: 10.1016/j.ajic.2023.01.012
Sarvestani, H. K., Ramandi, A., Getso, M. I., Razavyoon, T., Javidnia, J., Golrizi, M. B., et al. (2022). Mass spectrometry in research laboratories and clinical diagnostic: a new era in medical mycology. Braz. J. Microbiol. 53, 689–707. doi: 10.1007/s42770-022-00715-3
Sasso, M., Roger, C., Poujol, H., Barbar, S., Lefrant, J. Y., Lachaud, L. (2017). Changes in the distribution of colonising and infecting Candida spp. isolates, antifungal drug consumption and susceptibility in a French intensive care unit: A 10-year study. Mycoses 60, 770–780. doi: 10.1111/myc.2017.60.issue-12
Sharma, M., Chakrabarti, A. (2023). Candidiasis and other emerging yeasts. Curr. Fungal Infect. Rep. 17, 15-24. doi: 10.1007/s12281-023-00455-3
Sharp, A., Muller-Pebody, B., Charlett, A., Patel, B., Gorton, R., Lambourne, J., et al. (2021). Screening for Candida auris in patients admitted to eight intensive care units in England 2017 to 2018. Euro Surveill 26, 1900730. doi: 10.2807/1560-7917.ES.2021.26.8.1900730
Shastri, P. S., Shankarnarayan, S. A., Oberoi, J., Rudramurthy, S. M., Wattal, C., Chakrabarti, A. (2020). Candida auris candidaemia in an intensive care unit - Prospective observational study to evaluate epidemiology, risk factors, and outcome. J. Crit. Care 57, 42–48. doi: 10.1016/j.jcrc.2020.01.004
Soriano, A., Honore, P. M., Puerta-Alcalde, P., Garcia-Vidal, C., Pagotto, A., Gonçalves-Bradley, D. C., et al. (2023). Invasive candidiasis: current clinical challenges and unmet needs in adult populations. J. Antimicrob. Chemother. 78, 1569–1585. doi: 10.1093/jac/dkad139
Staniszewska, M. (2020). Virulence factors in Candida species. Curr. Protein Pept. Sci. 21, 313–323. doi: 10.2174/1389203720666190722152415
Taori, S. K., Rhodes, J., Khonyongwa, K., Szendroi, A., Smith, M., Borman, A. M., et al. (2022). First experience of implementing Candida auris real-time PCR for surveillance in the UK: detection of multiple introductions with two international clades and improved patient outcomes. J. Hosp Infect. 127, 111–120. doi: 10.1016/j.jhin.2022.06.009
Taverna, C. G., Vivot, M. E., Arias, B. A., Irazu, L., Canteros, C. E. (2023). Evaluation of the CHROMagar Candida Plus medium for presumptive identification of yeasts and MALDI-TOF MS identification. Mycoses 66, 977–983. doi: 10.1111/myc.v66.11
Thomas-Rüddel, D. O., Schlattmann, P., Pletz, M., Kurzai, O., Bloos, F. (2022). Risk factors for invasive Candida infection in critically ill patients: A systematic review and meta-analysis. Chest 161, 345–355. doi: 10.1016/j.chest.2021.08.081
Vinayagamoorthy, K., Pentapati, K. C., Prakash, H. (2022). Prevalence, risk factors, treatment and outcome of multidrug resistance Candida auris infections in Coronavirus disease (COVID-19) patients: A systematic review. Mycoses 65, 613–624. doi: 10.1111/myc.13447
Welsh, R. M., Bentz, M. L., Shams, A., Houston, H., Lyons, A., Rose, L. J., et al. (2017). Survival, persistence, and isolation of the emerging multidrug-resistant pathogenic yeast Candida auris on a plastic health care surface. J. Clin. Microbiol. 55, 2996–3005. doi: 10.1128/JCM.00921-17
WHO (2022). WHO fungal priority pathogens list to guide research, development and public health action (World Health Organization). Available online at: https://www.who.int/publications/i/item/9789240060241 (Accessed December 19, 2023).
Willger, S. D., Grim, S. L., Dolben, E. L., Shipunova, A., Hampton, T. H., Morrison, H. G., et al. (2014). Characterization and quantification of the fungal microbiome in serial samples from individuals with cystic fibrosis. Microbiome 2, 40. doi: 10.1186/2049-2618-2-40
Keywords: Candida spp., Candida auris, intensive care unit, surveillance, colonization, mannitol salt agar auris, prevalence
Citation: Nascimento T, Inácio J, Guerreiro D, Diaz P, Patrício P, Proença L, Toscano C and Barroso H (2024) Enhancing ICU Candida spp. surveillance: a cost-effective approach focused on Candida auris detection. Front. Cell. Infect. Microbiol. 14:1463456. doi: 10.3389/fcimb.2024.1463456
Received: 11 July 2024; Accepted: 24 September 2024;
Published: 01 November 2024.
Edited by:
Margie Morgan, Cedars Sinai Medical Center, United StatesReviewed by:
Andres Ceballos-Garzon, BIOASTER, FranceTinashe K. Nyazika, University of Wolverhampton, United Kingdom
Copyright © 2024 Nascimento, Inácio, Guerreiro, Diaz, Patrício, Proença, Toscano and Barroso. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Teresa Nascimento, dG5hc2NpbWVudG9AZWdhc21vbml6LmVkdS5wdA==