
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cell. Infect. Microbiol. , 04 July 2024
Sec. Intestinal Microbiome
Volume 14 - 2024 | https://doi.org/10.3389/fcimb.2024.1367998
 Ana Mendes-Frias1,2†
Ana Mendes-Frias1,2† Marta Moreira3†
Marta Moreira3† Maria C. Vieira1,2
Maria C. Vieira1,2 Joana Gaifem4
Joana Gaifem4 Patrício Costa1,2
Patrício Costa1,2 Luís Lopes1,2,3
Luís Lopes1,2,3 Ricardo Silvestre1,2*
Ricardo Silvestre1,2*Introduction: Ulcerative colitis is an inflammatory disorder characterized by chronic inflammation in the gastrointestinal tract, mainly in the colon and rectum. Although the precise etiology of ulcerative colitis remains unclear, recent research has underscored the significant role of the microbiome in its development and progression.
Methods: The aim of this study was to establish a relationship between the levels of specific gut bacterial species and disease relapse in ulcerative colitis. For this study, we recruited 105 ulcerative colitis patients in remission and collected clinical data, blood, and stool samples. Akkermansia muciniphila and Parabacteroides distasonis levels were quantified in the stool samples of ulcerative colitis patients. Binary logistic regression was applied to collected data to predict disease remission.
Results: The median time in remission in this cohort was four years. A predictive model incorporating demographic information, clinical data, and the levels of Akkermansia muciniphila and Parabacteroides distasonis was developed to understand remission patterns.
Discussion: Our findings revealed a negative correlation between the levels of these two microorganisms and the duration of remission. These findings highlight the importance of the gut microbiota in ulcerative colitis for disease prognosis and for personalized treatments based on microbiome interventions.
Ulcerative Colitis (UC) is a chronic inflammatory disease that affects the colon and rectum, with a complex and multifactorial pathophysiology that involves environmental factors, immune system disorders and microbiome interactions in genetically susceptible individuals (Shen et al., 2018). UC has emerged as a global health challenge, owing to its elevated occurrence in developed countries and the progressively rising incidence in developing regions (Kobayashi et al., 2020). This increased incidence is justified by the adoption of a more westernized lifestyle, associated with increased consumption of highly processed and animal-based food (Wang et al., 2023). According to European Crohn´s and Colitis Organization (ECCO) guidelines, the current goal is to promote clinical remission defined as cessation of rectal bleeding and normal stool frequency, supported by increase of hemoglobin (Hb) and reduction of specific inflammatory markers (fecal calprotectin, erythrocyte sedimentation rate (ESR) and C reactive protein (CRP) (Travis et al., 2011; Raine et al., 2022). Ulcerative Colitis Symptoms Questionnaire (UC-SQ) is used to standardize symptoms characterization among clinical studies, allowing assessment of disease remission (Panes et al., 2023). After analysis, this scale was validated to evaluate responsiveness to treatment, and after modifications to a 15-point scale (excluding the joint pain and constipation) achieved an area under the curve (AUC) of 0.79 to estimate remission if the patient revealed 14 or less points in the questionnaire (Panes et al., 2023). Endoscopic and histological remission are determined based on colonoscopy with biopsies, through evaluation of the Mayo endoscopic sub-score (indicating remission if the score is 0–1) and mucosal lesions, respectively (Travis et al., 2011). Since the precise etiology of UC is not well-established, treatment strategies focus on achieving disease remission. The initial therapeutic approach involves the administration of aminosalicylates, while corticosteroids are used in relapse situations to mitigate the inflammatory response and tissue damage, thereby promoting restoration of homeostasis (Cai et al., 2021; Segal et al., 2021). Patients unresponsive to initial treatment require the administration of systemic immunomodulators such as biological agents. These agents consist of antibodies targeting key players of inflammatory response, primarily focusing on TNFα, α4β7-integrin and, more recently, IL-12/IL-23 (Raine, 2014; Genaro et al., 2021; Keam, 2023). Considering that all the therapies are administered to mitigate inflammation rather than provide a cure, and that these are only effective to a subset of patients, more research is needed to unravel specific targets to effectively manage UC.
Growing evidence has shown a significant contribution of microbiome to the development and maintenance of UC (Schirmer et al., 2018, 2024; Lloyd-Price et al., 2019; Jiang et al., 2024; Wu et al., 2024). Indeed, microbial species regulate immune function in the gut, inhibit proliferation and invasion of pathogenic agents, along with the production of metabolites with an important impact in intestinal homeostasis (Hu et al., 2022). Therefore, UC is characterized by a significant alteration in the composition of the microbiota (dysbiosis), with overgrowth of certain pathogenic bacteria and reduction of species with mucosal protective effects. These changes induce inflammation of the intestinal mucosa, compromising its barrier function, leading to an increased bacterial translocation, and promoting an exacerbated inflammatory response (Glassner et al., 2020). Previous work from our research group revealed a protective effect of Akkermansia muciniphila and Parabacteroides distasonis in murine models of chemically-induced colitis (Gaifem et al., 2024). The anti-inflammatory properties of A. muciniphila have been reported in both murine models and UC patients (Abbasi et al., 2023). However, the use of this strain as a probiotic requires further investigation since the beneficial impact of A. muciniphila depends on the strain used and, on the amount, administrated (Qu et al., 2023) (Liu et al., 2021). In addition, quantification of A. muciniphila have been reported in different cohorts, both adult and pediatric patients, reveling contradictory results (Chiantera et al., 2023; Zheng et al., 2023). Altogether, these studies revealed that the levels of A. muciniphila are altered by different factors, for instance diet and age, demonstrating that the use of A. muciniphila as a marker must be critically considered. P. distasonis was described to have a dichotomic effect in colitis, with reports revealing both anti and pro-inflammatory effect of this species (Ezeji et al., 2021). In addition, several reports revealed decreased levels of P. distasonis in UC patients during active disease (do Nascimento et al., 2020; Okahara et al., 2020; Nomura et al., 2021). However, the interaction between these two species is still under scrutiny.
In this work, we propose to evaluate the role of A. muciniphila and P. distasonis in UC relapse. A binary logistic regression that combines the clinical information of patients and the levels of A. muciniphila and P. distasonis was established to predict the interval of time for patients’ remission. We demonstrate an interaction between A. muciniphila and P. distasonis that is linked to a shorter time since relapse in patients experiencing remission.
This is a single-center prospective cohort study performed in collaboration between Life and Health Sciences Research Institute (ICVS) and Hospital de Santa Luzia [Local Health Unit of Alto Minho (ULSAM)], a Portuguese Hospital in Viana do Castelo affiliated with University of Minho summarized in Figure 1. From December 2021 to March 2023, all patients diagnosed with UC attending the Inflammatory Bowel Disease (IBD) outpatient clinic were invited to participate in this study. The study was approved by the local Ethic Committee of ULSAM with the reference 19/2020. Volunteer participants were informed about the aims of the study and signed an informed consent to participate. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee. All patients with histologically confirmed UC followed at ULSAM with more than 18 years old were included. The exclusion criteria were patients who underwent colon resection surgery, had irregular follow-up appointments, had follow-up of less than one year or had taken antibiotics in the three months preceding sample collection.
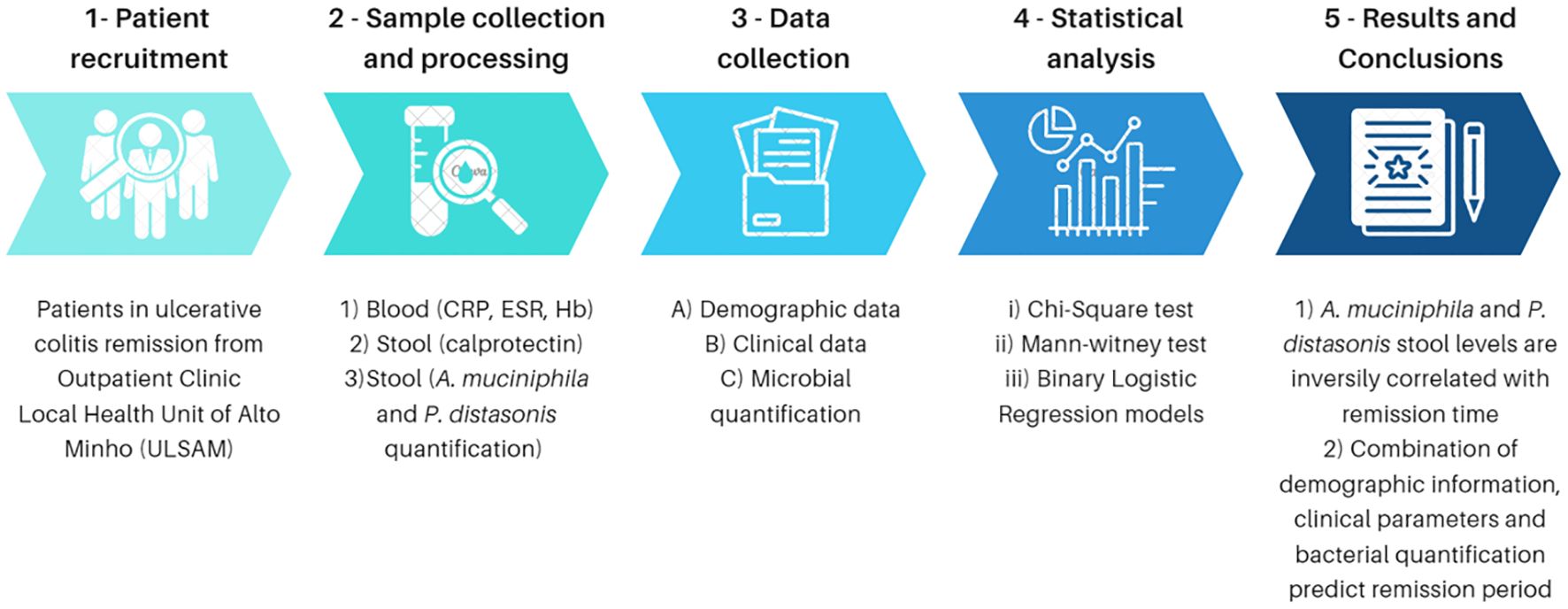
Figure 1 Study design.
From all the 105 participants, clinical data was collected using the UC-SQ to evaluate relevant symptoms that patients failed to report spontaneously, along with disease extension, time since last relapse, gender, age, age at onset, treatment, and use of antibiotics in the last three months. UC-SQ includes 17 different symptoms (frequency of bowel movements, passing of gases, abdominal pain, rectal pain, cramping, tiredness, loss of appetite, joint pain, difficulty sleeping, bloating, diarrhea, blood in stool, mucus in stool, constipation, false urge to defecate and defecatory urgency) rated from never to always regarding the 7 days prior to the questionnaire. During appointment, blood samples were collected to quantify inflammatory markers commonly used to follow UC patients: Hb, CRP and ESR. Finally, two sets of stool samples were collected; one to quantify fecal calprotectin and the other was immediately frozen until DNA extraction for quantification of the species of interest for this study. Samples added in multiple model 2 were longitudinal samples from the same patients already included, 6 months after the first sample.
The categorization of active disease or remission was determined through a medical evaluation that considered a combination of symptoms, analytical data, and colonoscopy findings. Symptoms were analysed using the UC-SQ relative to the seven days preceding the visit. Laboratory data collected during outpatient visits were defined as normal under the following criteria: Hb >12g/dL, CRP <1mg/dL, ESR <20mm/h, and fecal calprotectin <250μg/g. Remission was defined according to symptoms, biomarkers and latest endoscopy. However, in cases when these three parameters were not aligned, a rectosigmoidoscopy was performed to confirm remission. Only patients in disease remission were included in this study.
DNA from stool samples was extracted using Genomic DNA Kit (GK03.0100, Grisp) according to manufacturer’s instruction. A suggested protocol for DNA purification for stool samples was applied, using a lysozyme buffer (Lysozyme Buffer: 20mg/ml Lysozyme in 20mM Tris-HCl, 2mM EDTA, 1% Triton X-100) to efficiently lysate bacteria. Briefly, samples were homogenized using the lysozyme buffer and incubated with proteinase K (1mg/mL) and, then, RNase A (µg/mL) (both included in the kit). Samples were centrifuged at 16000g for 5minutes to remove insoluble components. DNA was isolated using a column included in the kit. After extraction, DNA was quantified using NanoDrop 1000 (Thermofisher).
Specific primers for A. muciniphila (CAGCACGTGAAGGTGGGGAC (forward) and CCTTGCGGTTGGCTTCAGAT (reverse)) and for P. distasonis (TGCCTATCAGAGGGGGATAAC (forward) and GCAAATATTCCCATGCGGGAT (reverse)) were used to obtain a specific sequence to each bacterium (Collado et al., 2007; Tong et al., 2011). This sequence was cloned in a vector using CloneJET PCR Cloning Kit (Thermo Scientific) to obtain a DNA template to each bacterium. A standard curve was obtained by qPCR using 10-fold dilutions of the template created. The bacterial abundance was determined by quantifying bacterial copy number in the DNA of stool samples using specific primers and the standard curve previously mentioned. Quantification results were normalized as number of copies per picograms of DNA.
Qualitative variables were summarized using absolute and relative frequencies. The quantitative variables were summarized using the median and interquartile range, considering the small sample size and the non-normality observed in our variables, confirmed by normality tests (Kolmogorov-Smirnov and Shapiro-Wilk test) and histogram distribution.
The chi-square test was performed for categorical variables to assess the interdependence between variables. A Mann-Whitney test was employed to compare the study groups. For each statistical test we calculated the adequate effect size measure (r for the Mann-Whitney test and the V-Cramer/Phi for the chi-square test) and its interpretation followed the Cohen’s effect size cut-off values (Cohen, 2013). Binary logistic regressions models were employed and Odds Ratio (OR) and p-value were reported for each variable. Statistical analysis was performed using SPSS version 28 software (IBM, New York, USA).
Out of all the patients attending the appointments, 105 individuals diagnosed with UC and confirmed to be in a state of clinical disease remission as defined above were enrolled in this study. The demographic characterization of the cohort is presented in Table 1. Our gender-balanced cohort (48.6% males and 51.4% females) effectively invalidates gender-related influence in the subsequent analysis. Regarding endoscopic disease severity, patients included in this study exhibited endoscopic remission, indicated by a Mayo endoscopic sub-score of 0 and managed their symptoms with aminosalicylates (69.1% and 75.2%, respectively). Interestingly, laboratory parameters also indicated disease remission in our cohort comparing the median values with reference ranges, described in the Methods section. The median disease extension of our cohort is 12 years. The median time since relapse is 48 months (equivalent to 4 years). Consequently, we will consider the time since relapse as a categorical variable with two levels: exceeding 4 years and less than 4 years.
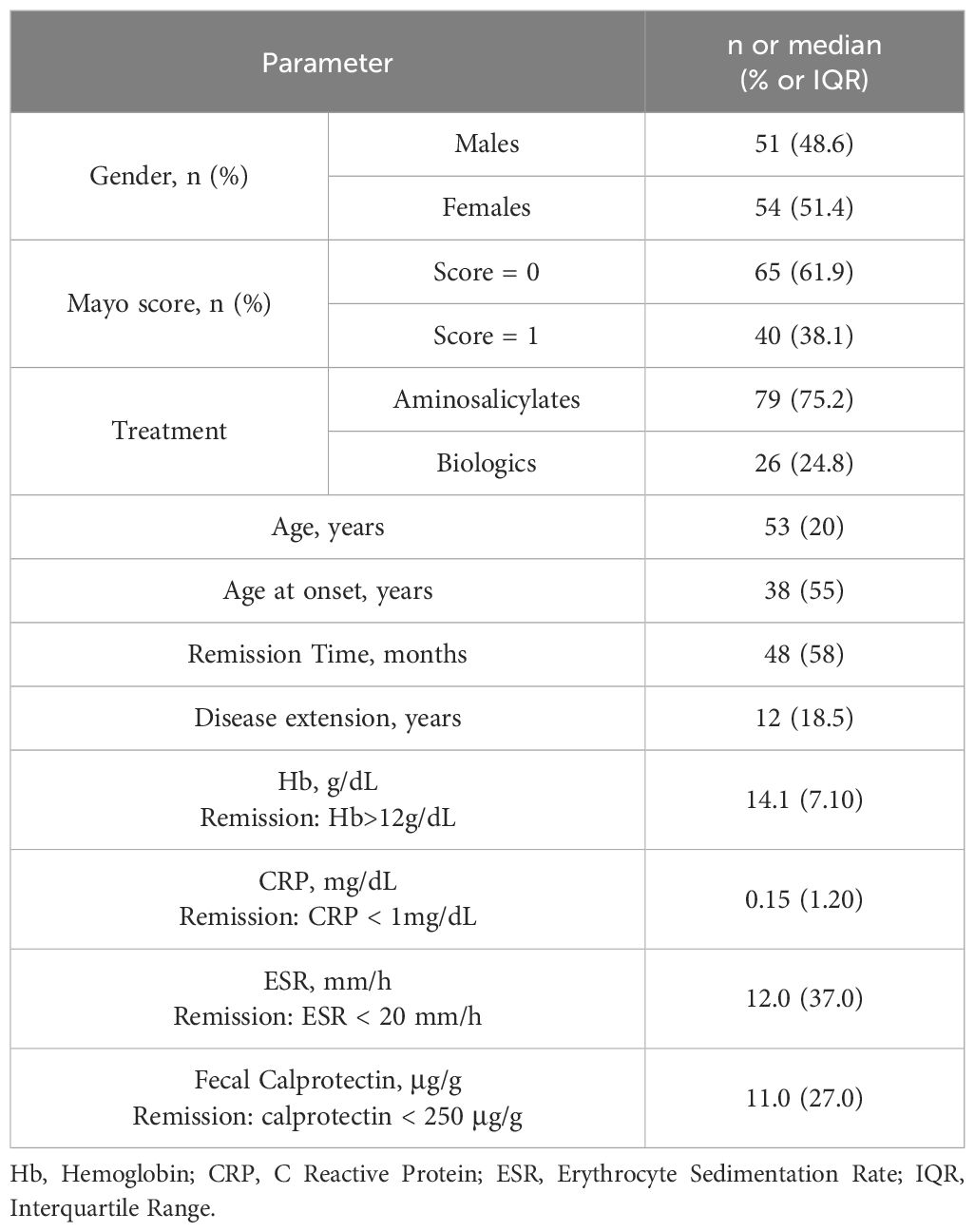
Table 1 Demographic and clinical characterization of the UC patients’ cohort (n=105).
Disease severity is often determined based on treatment, whereby patients unresponsive to the initial line of therapy (aminosalicylates) received biologics as a step-up approach (Cai et al., 2021). Following this criterion, patients are categorized as mild to moderate if treated with aminosalicylates, and as severe if they require biologics. To explore the potential impact of treatment on both clinical parameters and the levels of A. muciniphila and P. distasonis, this variable was employed as a grouping factor for comprehensive analysis (Table 2). No association was found between treatment and variables such as gender, age, time since relapse, Mayo score, disease extension and clinical parameters (Hb, ESR and fecal calprotectin) (p>0.05). However, when comparing patients on biologics to those taking aminosalicylates, the CRP levels were found significantly higher in the former group (p=0.022). Predominantly, the levels of A. muciniphila were undetectable in most patients (75%), aligning with existing literature indicating diminished abundance of this species in UC patients. Thus, the absolute abundance and the binary presence/absence of detection for A. muciniphila were considered. A similar approach was adopted for P. distasonis, although this species was quantified in most samples (83%). Ultimately, the analysis did not establish an association between the presence or combination of these species, according to the type of treatment, and subsequently, disease severity.
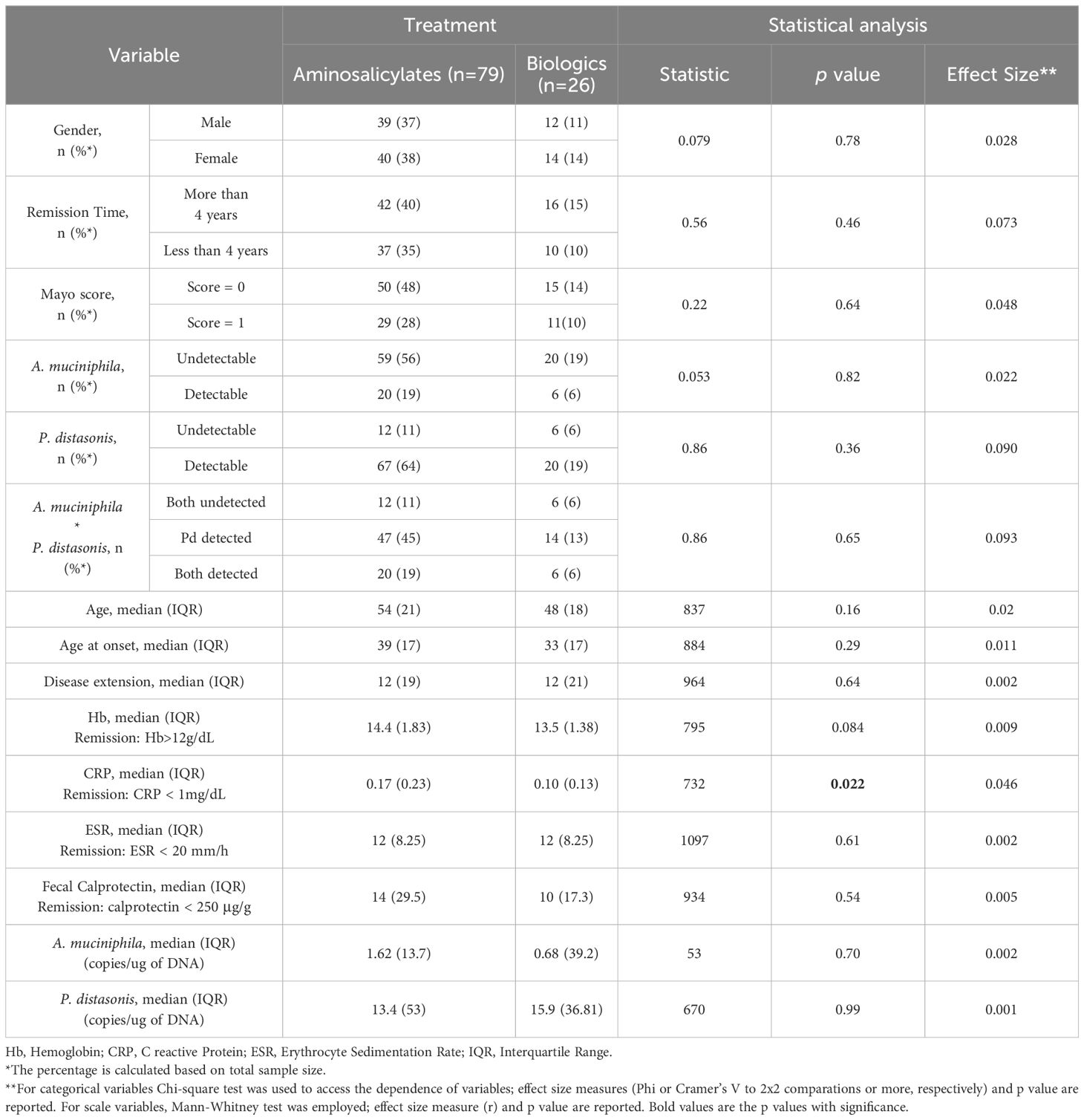
Table 2 Characterization of the different variables according to treatment (n=105).
Adopting a similar approach as for treatment type, we examined the association between the time since relapse, categorized in two intervals as previously mentioned (Table 3). No association was found between the demographic and clinical parameters and the time since relapse (p>0.05). However, in concordance with the literature, patients experiencing a relapse within the last 4 years were significantly younger than those who had not relapsed (p=0.011) (Jang et al., 2009; Nakov and Nakov, 2021). No significant differences emerged among the groups in the absolute levels of both A. muciniphila and P. distasonis. Interestingly, concerning the presence or absence of these bacteria, while the detection of A. muciniphila is not associated with the time since relapse, the presence of P. distasonis is significantly associated with decreased remission time (p=0.035), but with a small effect size (0.21). Remarkably, even when considering the detection of both species simultaneously, an association persisted between the presence of these bacteria and diminished duration of remission time (p=0.049).
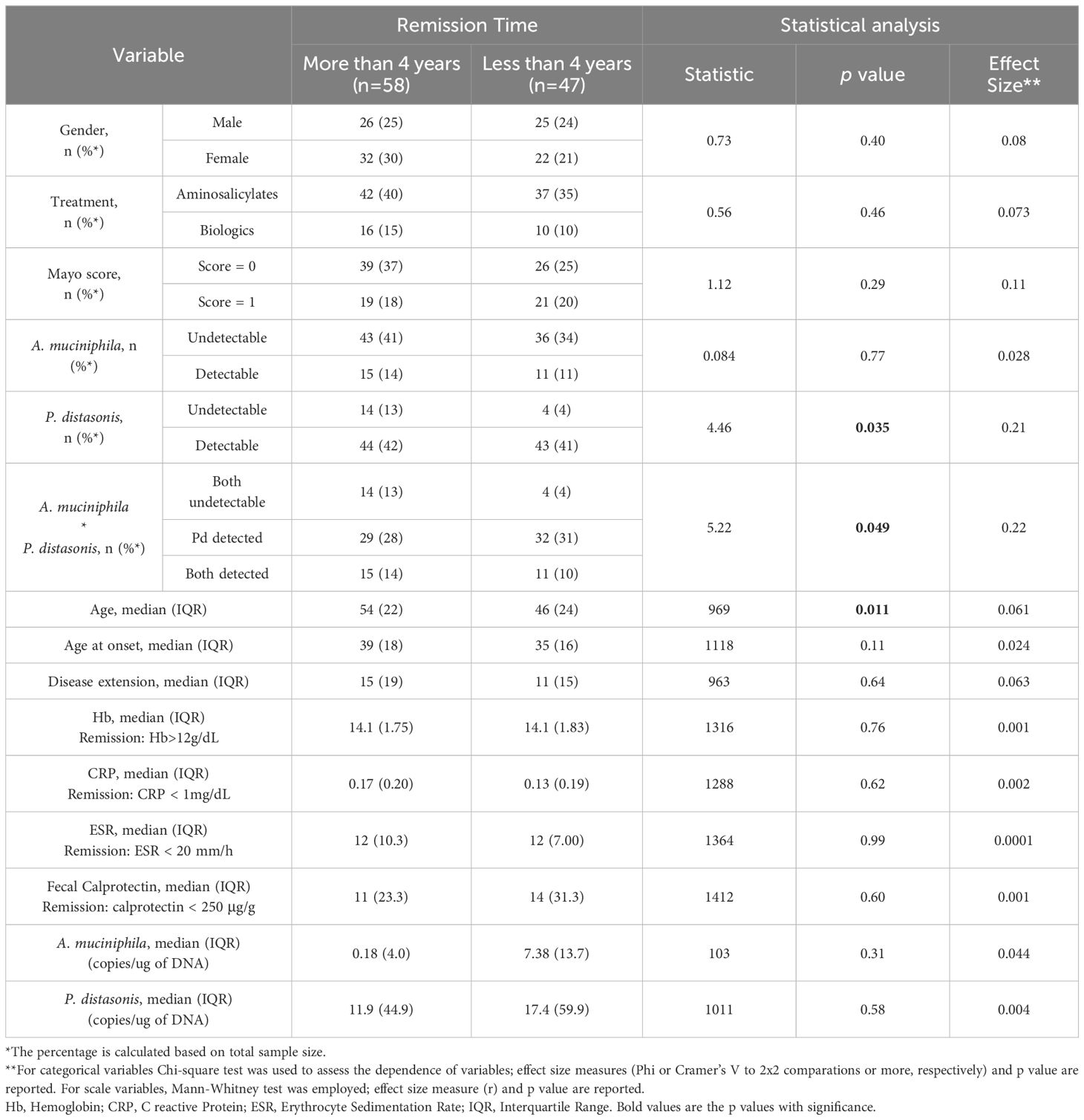
Table 3 Characterization of the different variables according to time since relapse (n=105).
Predicting remission time in UC patients poses a significant challenge due to its dependency on many factors, including diet, daily habits (such as smoking and exercise) and microbiome composition. Given the observed relationship between the detection of A. muciniphila and P. distasonis and the time since relapse, we hypothesize that these two parameters might offer utility to predict the remission duration of UC patients. A binary logistic regression model was applied to all the variables as a single model to assess this. As presented in Table 4, in addition to age, which has already been pointed out as an important factor in disease remission, no other variable significantly impacted the time since relapse. Subsequently, an array of mixed models was assessed, encompassing a comprehensive spectrum of variables including clinical information and bacterial levels (absolute and detectable/undetectable). A significant and robust model (p=0.035 and R2 = 0.53) was identified, including the following variables: gender, age, Hb, ESR, fecal calprotectin, the absolute levels of A. muciniphila and P. distasonis and the interaction between these latter two variables. However, only ESR revealed a significant contribution to the model (p=0.036). Subsequently, additional samples from the same patients at different time points were incorporated into the model to investigate whether the lack of significance was due to sample size constraints. Remarkably, with the inclusion of these supplementary samples, the model gained strength and significance (R2 = 0.57 and p=0.001). Thus, the levels of the two species under analysis and their interaction began to influence the prediction of the remission time significantly. This concerned not only individual species but also the combination of both (p=0.026 to A. muciniphila, p=0.046 to P. distasonis and p=0.026 for the interaction). Of note, in both models, the adjusted ORs for A. muciniphila, P. distasonis and their interaction remained consistent (OR=1.58, 1.01 and 0.99 to A. muciniphila, P. distasonis and their interaction, respectively, in the first model and OR=1.87, 1.01 and 0.99, respectively, in the second model), meaning that the contribution of each variable is the same in both models. A receiver operating characteristic (ROC) curve was created to each mixed model (Figure 2). An area under the curve (AUC) = 0.86 (CI 95%: 0.74;0.99, p<0.0001) and AUC = 0.846 (CI:0.71;0.98, p=0.001) was obtained to model 1 and model 2, respectively. Consequently, it can be concluded that the levels of A. muciniphila and P. distasonis indeed contribute to determining the time since relapse in UC patients.
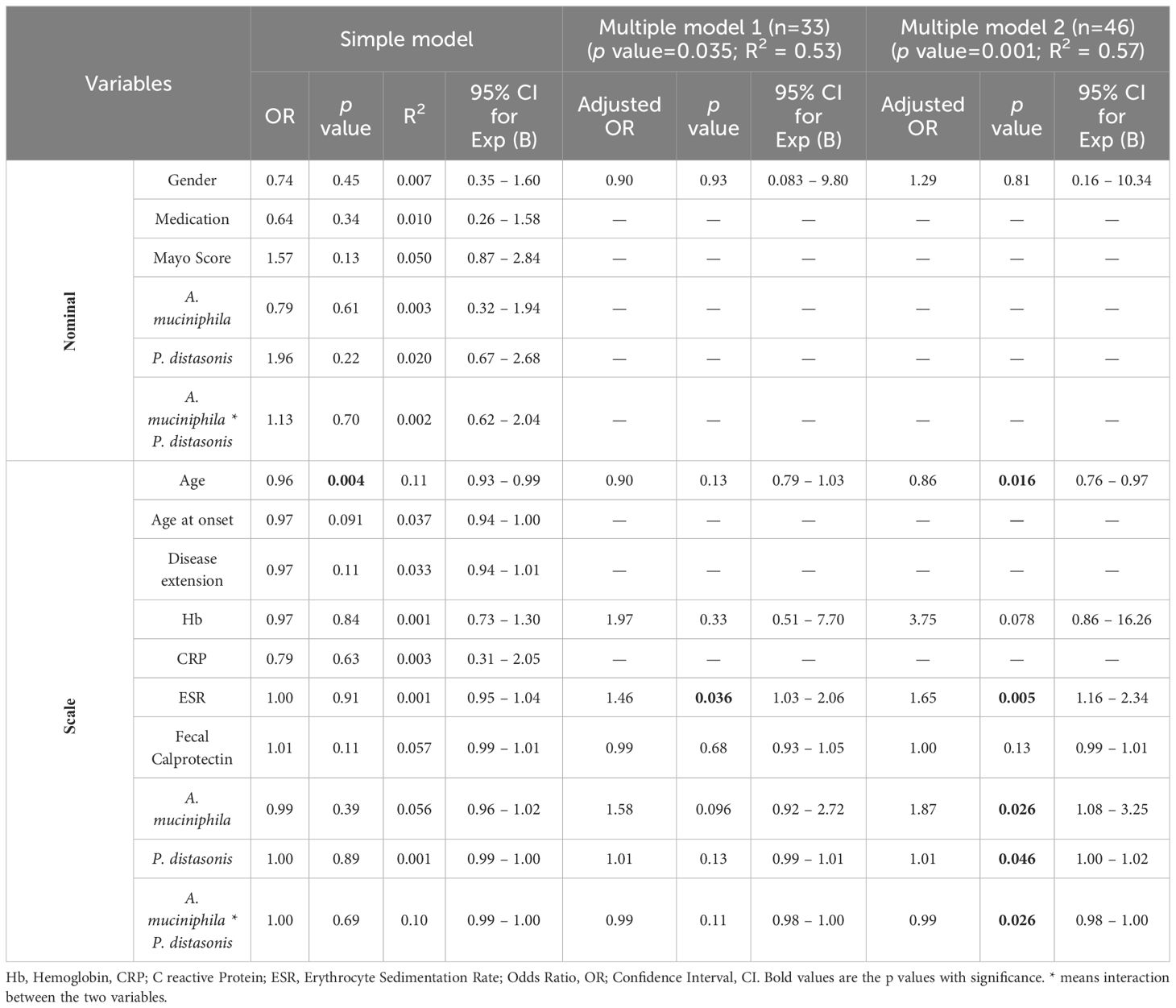
Table 4 Binary logistic regression to predict remission time.
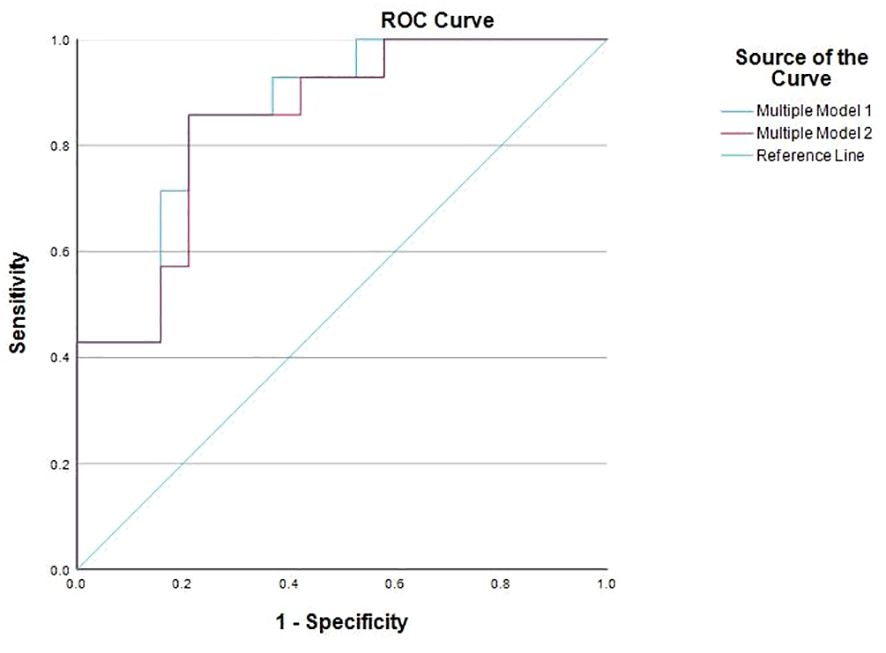
Figure 2 Receiver operating characteristic (ROC) curves of multiple model 1 and multiple model 2.
UC has emerged as a global burden, affecting millions worldwide, with an increasing incidence over the last few years (Wang et al., 2023). While the precise etiology of the disease remains elusive, significant efforts have been made to define accurate diagnostic and monitoring markers (Feuerstein et al., 2019). The intestinal microbiome plays a crucial role in the gut homeostasis and the development and progression of UC. Given the consistent alterations in the microbiome composition in UC patients, identifying microbial markers may be pivotal for a more effective clinical management of the disease (Glassner et al., 2020). The quantification of these microbial markers or even the microorganisms themselves, is valuable for enhancing diagnosis, improving patient follow-up as a prognostic marker, and predicting treatment response and disease recurrence in a non-invasive manner (Guo et al., 2022).
The patient cohort evaluated in this study was balanced for age and gender, in which all patients were classified as being in remission state of the disease. Regarding treatment, in our cohort 75% of patients maintain disease remission only with aminosalicylates therapy (mesalazine), while 25% of patients require biologic agents (infliximab, adalimumab, ustekinumab or vedolizumab) to achieve remission. These percentages are consistent with European studies, particularly with a Spanish cohort that reported a remission maintenance rate of 72% among UC patients treated with aminosalicylates (Marti-Aguado et al., 2019).
Clinical parameters have been used as follow-up measures for disease activity in UC (Sakurai and Saruta, 2023). Reduced levels of fecal calprotectin have been identified as a predictive indicator for mucosal healing and colitis remission, establishing it as a non-invasive marker of remission (Malvão et al., 2021; Kawashima et al., 2023). However, our study did not find statistically significant differences in fecal calprotectin levels between the two remission groups. Notably, a median of 11 μg/g was observed for patients in remission for over 4 years, in contrast to a median of 14 μg/g for patients with a remission period lower than 4 years. Also, the predictive value of fecal calprotectin was not evident in our study, either alone (p = 0.11) or in combination with the other markers (p = 0.68 to the first model and p = 0.13). While most studies compare remission and active disease, our study establish a four-year remission cut-off, indicating fecal calprotectin’s limitations in discriminating based on the duration of remission. In contrast, our study unveiled a significant association between ESR levels and the prediction of remission period. ESR, a classic inflammatory marker widely used for diagnosis and follow-up in UC patients, despite its elevation in various inflammatory conditions (Sakurai and Saruta, 2023), ESR has been suggested by other studies as predictor of recurrence in UC, comparing active disease with remission (Liverani et al., 2016). Our findings indicate that ESR serves as a complementary marker for predicting the remission period. When used alone in a binary logistic model, ESR did not show predictive value; however, its significance emerged when combined with several markers in predicting disease remission.
In this work, we propose two microbial targets, A. muciniphila and P. distasonis, as specific markers for disease remission. Both bacteria have been associated with reports of both beneficial and pathogenic effects on human health (Ezeji et al., 2021; Abbasi et al., 2023). Additionally, recently published data from our research group suggests an interaction between these two species associated with a protective phenotype in mouse models of UC (Gaifem et al., 2024). Our findings suggest an inverse correlation between the levels of these species and remission time. Indeed, we have established a robust and significant model that combines the levels of these two microorganisms with clinical parameters to predict the remission time. Additionally, our data suggest an interaction between the levels of A. muciniphila and P. distasonis and that these two species directly impact remission period in UC patients.
A. muciniphila, a gram-negative anaerobe, resides in the mucus layer and degrades mucin to produce metabolites (short-chain fatty acids) that benefit the intestinal epithelial barrier (Derrien et al., 2004). Indeed, an increased abundance of these bacteria has been reported in healthy individuals, while decreased levels were found in UC patients (Derrien et al., 2008). In recent years, the beneficial properties of this species have been extensively explored in mouse models of UC, suggesting A. muciniphila as a potential candidate for probiotic use as an adjuvant to therapy (Abbasi et al., 2023; Zheng et al., 2023). However, excessive colonization of A. muciniphila promotes increased degradation of mucins from the mucus layer, leading to the concomitant destruction of the epithelial barrier structure and inflammation in the gut (Qu et al., 2023). Indeed, the effect of A. muciniphila in a DSS-induced colitis mouse model was demonstrated to depend on the administered strain (Liu et al., 2021). In our cohort, no significant association was found between the levels of A. muciniphila and remission time. Herrera-deGuise and colleagues found a positive correlation between the levels of this microorganism and remission time (Herrera-deGuise et al., 2023). These variations may be attributed to the different analysis performed in both studies. In our study, only samples above the detection limit were included in the analysis, which reduced considerably the sample size (A. muciniphila was only detectable in 25% of all samples). To overcome this limitation, we created a dichotomic variable referring to the presence or absence of both species, so that all samples could be included. The Spanish study used a method in which values below the detection limit were treated by imputing them as the lowest abundance in the data set divided by 2. While this approach offers the advantage of incorporating all data points into subsequent analyses, it’s crucial to note that this imputation was applied in a relevant number of cases, leading to a reduction in the dispersion of the variable distribution. Thus, the discrepancy in results could be explained by this increase in the number of patients with low levels of A. muciniphila.
P. distasonis, a gram negative aerotolerant bacterium, colonizes the gastrointestinal tract and exhibit a dichotomous effect on the host, with both pathogenic and beneficial effects (Ezeji et al., 2021). On one hand, P. distasonis administration alleviates obesity, metabolic dysfunctions, and experimental colitis, in both DSS and TNBS mouse models (Kverka et al., 2011; Wang et al., 2019; Cuffaro et al., 2020). On the other hand, the abundance of this microorganism has been found to increase in acute and chronic DSS-induced colitis model, promoting inflammation in mouse models by degrading the mucosal barrier, potentially contributing to the development of intestinal inflammation (Okayasu et al., 1990; González-Páez et al., 2019). Additionally, a dichotomous effect of this microorganism has been observed in the context of diabetes: while Cai and colleagues demonstrate the anti-inflammatory properties of P. distasonis that could prevent diabetes by decreasing insulin resistance, Hasain and colleagues found an enrichment of this species in gestational diabetes mellitus (Cai et al., 2020; Hasain et al., 2020). Also, the levels of this microorganism are also inversely correlated with the presence of intestinal tumors, emphasizing that the influence of P. distasonis levels in disease varies in a context-dependent manner (Kverka et al., 2011; Wang et al., 2019; Cuffaro et al., 2020; Gu et al., 2021). Our work found an association between the levels of P. distasonis and disease remission, with an increased level of this microorganism in individuals with a remission time lower than four years. Overall, these data suggest that P. distasonis may contribute for the immunopathological events underlying remission of UC. However, more research is needed to understand the mechanisms underlying this impact.
In this study, we integrated patient demographic, clinical and microbial data to create a predictive model for remission time. Our model reveals that higher levels of A. muciniphila and P. distasonis and their interaction are associated with decreased remission time. This is the first association between these two microorganisms in the context of UC, specifically within a patient cohort. Despite the small sample size and the challenges to quantify A. muciniphila, our model is an important clinical tool for predicting UC patients’ remission time due to its lower levels in UC patients. Given the evident influence of sample size on p-values, it is advisable to closely monitor and discuss the effect size measures, namely OR in this case. Although we did not initially obtain statistically significant results for these two microorganisms (and their interaction), the calculated OR values suggest that even a modest increase in our sample size could potentially yield significant results. Additionally, a R2 greater than 0.5 reflects that this is a robust model for predicting remission time, according to Cohen’s cut-off values (Cohen, 2013). Thus, the extension of our cohort could increase statistical power of the tested models. Also, the integration of Crohn’s patients in our cohort could benefit the knowledge about the different forms of IBD and the influence of the microbiome in both diseases. Nevertheless, this study demonstrates a novel promising model that can provide relevant information for UC clinical management, since it can be used to infer relapses in patients that show higher risk for remission. The evaluation of specific bacterial species (in this case, A. muciniphila and P. distasonis), in combination with demographic parameters and biochemical markers can constitute an important tool to predict remission, as previously defined by other research groups (Hosseini et al., 2015; Pang et al., 2023).
In conclusion, our results have enhanced the understanding of microbial changes in the Portuguese population during UC remission. Considering that the microbiome varies significantly across populations due to differences in diet and lifestyle, these cohort studies are crucial to characterize populations fully and should take into account the changes in diet between individuals, that were not considered in this work. Smoking habits have also been described to shape the microbiome and to affect UC onset (Papoutsopoulou et al., 2020; Gui et al., 2021; Nicolaides et al., 2021). However, the smoking habits of the participants were not available. Nevertheless, understanding which and how different microbial players interact with these two species may allow the improvement of microbiota-targeted therapies, tailored to different subsets of patients. This ultimately will contribute towards a more personalized healthcare approach and an improved quality of life for UC patients.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The study was approved by the local Ethic Committee of Local Health Unit of Alto Minho (ULSAM) with the reference 19/2020. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
AF: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal analysis, Investigation, Methodology. MM: Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. MV: Formal analysis, Investigation, Methodology, Writing – review & editing. JG: Conceptualization, Data curation, Writing – review & editing. PC: Data curation, Formal analysis, Writing – review & editing, Methodology. LL: Project administration, Resources, Supervision, Validation, Writing – review & editing. RS: Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Validation, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work has been funded by National funds, through the Foundation for Science and Technology (FCT) - project UIDB/50026/2020 (DOI 10.54499/UIDB/50026/2020), UIDP/50026/2020 (DOI 10.54499/UIDP/50026/2020) and LA/P/0050/2020 (DOI 10.54499/LA/P/0050/2020) and by the project NORTE-01-0145-FEDER-000039, supported by Norte Portugal Regional Operational Programme (NORTE 2020), under the PORTUGAL 2020 Partnership Agreement, through the European Regional Development Fund (ERDF). The FCT contracts 2021.07836.BD to AF, CEECIND/00185/2020 to RS and 2020.00088.CEECIND to JG.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbasi, A., Bazzaz, S., Da Cruz, A. G., Khorshidian, N., Saadat, Y. R., Sabahi, S., et al. (2023). A critical review on akkermansia muciniphila: functional mechanisms, technological challenges, and safety issues. Probiotics Antimicrob. Proteins. 1. doi: 10.1007/s12602-023-10118-x
Cai, W., Xu, J., Li, G., Liu, T., Guo, X., Wang, H., et al. (2020). Ethanol extract of propolis prevents high-fat diet-induced insulin resistance and obesity in association with modulation of gut microbiota in mice. Food Res. Int. 130, 108939. doi: 10.1016/j.foodres.2019.108939
Cai, Z., Wang, S., Li, J. (2021). Treatment of inflammatory bowel disease: A comprehensive review. Front. Med. 8. doi: 10.3389/fmed.2021.765474
Chiantera, V., Laganà, A. S., Basciani, S., Nordio, M., Bizzarri, M. (2023). A critical perspective on the supplementation of akkermansia muciniphila: benefits and harms. Life 13, 1247. doi: 10.3390/life13061247
Cohen, J. (2013). Statistical power analysis for the behavioral sciences (Cambridge, Academic Press: Routledge). doi: 10.4324/9780203771587
Collado, M. C., Derrien, M., Isolauri, E., de Vos, W. M., Salminen, S. (2007). Intestinal integrity and akkermansia muciniphila, a mucin-degrading member of the intestinal microbiota present in infants, adults, and the elderly. Appl. Environ. Microbiol. 73, 7767–7770. doi: 10.1128/AEM.01477-07
Cuffaro, B., Assohoun, A. L. W., Boutillier, D., Súkeníková, L., Desramaut, J., Boudebbouze, S., et al. (2020). In vitro characterization of gut microbiota-derived commensal strains: selection of parabacteroides distasonis strains alleviating TNBS-induced colitis in mice. Cells 9, 2104. doi: 10.3390/cells9092104
Derrien, M., Collado, M. C., Ben-Amor, K., Salminen, S., de Vos, W. M. (2008). The mucin degrader akkermansia muciniphila is an abundant resident of the human intestinal tract. Appl. Environ. Microbiol. 74, 1646–1648. doi: 10.1128/AEM.01226-07
Derrien, M., Vaughan, E. E., Plugge, C. M., de Vos, W. M. (2004). Akkermansia muciniphila gen. nov., sp. nov., a human intestinal mucin-degrading bacterium. Int. J. Syst. Evol. Microbiol. 54, 1469–1476. doi: 10.1099/ijs.0.02873-0
do Nascimento, R.de P., MaChado, A.P.da F., Galvez, J., Cazarin, C. B. B., Maróstica Junior, M. R. (2020). Ulcerative colitis: Gut microbiota, immunopathogenesis and application of natural products in animal models. Life Sci. 258, 1–22. doi: 10.1016/j.lfs.2020.118129
Ezeji, J. C., Sarikonda, D. K., Hopperton, A., Erkkila, H. L., Cohen, D. E., Martinez, S. P., et al. (2021). Parabacteroides distasonis: intriguing aerotolerant gut anaerobe with emerging antimicrobial resistance and pathogenic and probiotic roles in human health. Gut Microbes 13, 1–27. doi: 10.1080/19490976.2021.1922241
Feuerstein, J. D., Moss, A. C., Farraye, F. A. (2019). Ulcerative colitis. Mayo Clin. Proc. 94, 1357–1373. doi: 10.1016/j.mayocp.2019.01.018
Gaifem, J., Mendes-Frias, A., Wolter, M., Steimle, A., Garzón, M. J., Ubeda, C., et al. (2024). Akkermansia muciniphila and Parabacteroides distasonis synergistically protect from colitis by promoting ILC3 in the gut. mBio. 15. doi: 10.1128/mbio.00078-24
Genaro, L. M., Gomes, L. E. M., Franceschini, A. P. M., de, F., Ceccato, H. D., de Jesus, R. N., et al. (2021). Anti-TNF therapy and immunogenicity in inflammatory bowel diseases: a translational approach. Am. J. Transl. Res. 13, 13916–13930.
Glassner, K. L., Abraham, B. P., Quigley, E. M. M. (2020). The microbiome and inflammatory bowel disease. J. Allergy Clin. Immunol. 145, 16–27. doi: 10.1016/j.jaci.2019.11.003
González-Páez, G. E., Roncase, E. J., Wolan, D. W. (2019). X-ray structure of an inactive zymogen clostripain-like protease from Parabacteroides distasonis. Acta Crystallogr. D Struct. Biol. 75, 325–332. doi: 10.1107/S2059798319000809
Gu, Z.-Y., Pei, W.-L., Zhang, Y., Zhu, J., Li, L., Zhang, Z. (2021). Akkermansia muciniphila in inflammatory bowel disease and colorectal cancer. Chin. Med. J. (Engl) 134, 2841–2843. doi: 10.1097/CM9.0000000000001829
Gui, X., Yang, Z., Li, M. D. (2021). Effect of cigarette smoke on gut microbiota: state of knowledge. Front. Physiol. 12. doi: 10.3389/fphys.2021.673341
Guo, X., Huang, C., Xu, J., Xu, H., Liu, L., Zhao, H., et al. (2022). Gut microbiota is a potential biomarker in inflammatory bowel disease. Front. Nutr. 8. doi: 10.3389/fnut.2021.818902
Hasain, Z., Mokhtar, N. M., Kamaruddin, N. A., Mohamed Ismail, N. A., Razalli, N. H., Gnanou, J. V., et al. (2020). Gut microbiota and gestational diabetes mellitus: A review of host-gut microbiota interactions and their therapeutic potential. Front. Cell Infect. Microbiol. 10. doi: 10.3389/fcimb.2020.00188
Herrera-deGuise, C., Varela, E., Sarrabayrouse, G., Pozuelo del Río, M., Alonso, V. R., Sainz, N. B., et al. (2023). Gut microbiota composition in long-remission ulcerative colitis is close to a healthy gut microbiota. Inflammation Bowel Dis. 29, 1362–1369. doi: 10.1093/ibd/izad058
Hosseini, S. V., Safarpour, A. R., Taghavi, S. A. (2015). Developing a novel risk-scoring system for predicting relapse in patients with ulcerative colitis: A prospective cohort study. Pak J. Med. Sci. 31, 1511–1516. doi: 10.12669/pjms.316.8811
Hu, Y., Chen, Z., Xu, C., Kan, S., Chen, D. (2022). Disturbances of the gut microbiota and microbiota-derived metabolites in inflammatory bowel disease. Nutrients 14, 5140. doi: 10.3390/nu14235140
Jang, E. S., Lee, D. H., Kim, J., Yang, H.-J., Lee, S. H., Park, Y. S., et al. (2009). Age as a clinical predictor of relapse after induction therapy in ulcerative colitis. Hepatogastroenterology 56, 1304–1309.
Jiang, N., Liu, Z., Wang, H., Zhang, L., Li, M., Li, G., et al. (2024). Alterations in metabolome and microbiome: new clues on cathelicidin-related antimicrobial peptide alleviates acute ulcerative colitis. Front. Microbiol. 15. doi: 10.3389/fmicb.2024.1306068
Kawashima, K., Oshima, N., Kishimoto, K., Kataoka, M., Fukunaga, M., Kotani, S., et al. (2023). Low fecal calprotectin predicts histological healing in patients with ulcerative colitis with endoscopic remission and leads to prolonged clinical remission. Inflammation Bowel Dis. 29, 359–366. doi: 10.1093/ibd/izac095
Keam, S. J. (2023). Mirikizumab: first approval. Drugs 83, 1045–1052. doi: 10.1007/s40265-023-01909-1
Kobayashi, T., Siegmund, B., Le Berre, C., Wei, S. C., Ferrante, M., Shen, B., et al. (2020). Ulcerative colitis. Nat. Rev. Dis. Primers 6, 1–20. doi: 10.1038/s41572-020-0205-x
Kverka, M., Zakostelska, Z., Klimesova, K., Sokol, D., Hudcovic, T., Hrncir, T., et al. (2011). Oral administration of Parabacteroides distasonis antigens attenuates experimental murine colitis through modulation of immunity and microbiota composition. Clin. Exp. Immunol. 163, 250–259. doi: 10.1111/j.1365-2249.2010.04286.x
Liu, Q., Lu, W., Tian, F., Zhao, J., Zhang, H., Hong, K., et al. (2021). Akkermansia muciniphila exerts strain-specific effects on DSS-induced ulcerative colitis in mice. Front. Cell Infect. Microbiol. 11. doi: 10.3389/fcimb.2021.698914
Liverani, E., Scaioli, E., Digby, R. J., Bellanova, M., Belluzzi, A. (2016). How to predict clinical relapse in inflammatory bowel disease patients. World J. Gastroenterol. 22, 1017. doi: 10.3748/wjg.v22.i3.1017
Lloyd-Price, J., Arze, C., Ananthakrishnan, A. N., Schirmer, M., Avila-Pacheco, J., Poon, T. W., et al. (2019). Multi-omics of the gut microbial ecosystem in inflammatory bowel diseases. Nature 569, 655–662. doi: 10.1038/s41586-019-1237-9
Malvão, L., dos, R., Madi, K., Esberard, B. C., de Amorim, R. F., Silva, K. dos S., et al. (2021). Fecal calprotectin as a noninvasive test to predict deep remission in patients with ulcerative colitis. Medicine 100, e24058. doi: 10.1097/MD.0000000000024058
Marti-Aguado, D., Ballester, M. P., Tosca, J., Bosca-Watts, M. M., Navarro, P., Anton, R., et al. (2019). Long-term follow-up of patients treated with aminosalicylates for ulcerative colitis: Predictive factors of response: An observational case-control study. United Eur. Gastroenterol. J. 7, 1042–1050. doi: 10.1177/2050640619854277
Nakov, R., Nakov, V. (2021). Young age and short duration of the disease are associated with more frequent relapses in inflammatory bowel disease patients. Med. Pharm. Rep. 94, 43–47. doi: 10.15386/mpr-1510
Nicolaides, S., Vasudevan, A., Long, T., van Langenberg, D. (2021). The impact of tobacco smoking on treatment choice and efficacy in inflammatory bowel disease. Intest Res. 19, 158–170. doi: 10.5217/ir.2020.00008
Nomura, K., Ishikawa, D., Okahara, K., Ito, S., Haga, K., Takahashi, M., et al. (2021). Bacteroidetes species are correlated with disease activity in ulcerative colitis. J. Clin. Med. 10, 1749. doi: 10.3390/jcm10081749
Okahara, K., Ishikawa, D., Nomura, K., Ito, S., Haga, K., Takahashi, M., et al. (2020). Matching between donors and ulcerative colitis patients is important for long-term maintenance after fecal microbiota transplantation. J. Clin. Med. 9, 1650. doi: 10.3390/jcm9061650
Okayasu, I., Hatakeyama, S., Yamada, M., Ohkusa, T., Inagaki, Y., Nakaya, R. (1990). A novel method in the induction of reliable experimental acute and chronic ulcerative colitis in mice. Gastroenterology 98, 694–702. doi: 10.1016/0016-5085(90)90290-H
Panes, J., Otley, A., Sanchez Gonzalez, Y., Fitzgerald, K., Zhou, W., Ilo, D., et al. (2023). Ulcerative colitis-symptom questionnaire: valid for use in adults with moderately to severely active ulcerative colitis. Dig Dis. Sci. 68, 2318–2332. doi: 10.1007/s10620-022-07807-y
Pang, W., Zhang, B., Jin, L., Yao, Y., Han, Q., Zheng, X. (2023). Serological biomarker-based machine learning models for predicting the relapse of ulcerative colitis. J. Inflammation Res. Volume 16, 3531–3545. doi: 10.2147/JIR.S423086
Papoutsopoulou, S., Satsangi, J., Campbell, B. J., Probert, C. S. (2020). Review article: impact of cigarette smoking on intestinal inflammation—direct and indirect mechanisms. Aliment Pharmacol. Ther. 51, 1268–1285. doi: 10.1111/apt.15774
Qu, S., Zheng, Y., Huang, Y., Feng, Y., Xu, K., Zhang, W., et al. (2023). Excessive consumption of mucin by over-colonized Akkermansia muciniphila promotes intestinal barrier damage during Malignant intestinal environment. Front. Microbiol. 14. doi: 10.3389/fmicb.2023.1111911
Raine, T. (2014). Vedolizumab for inflammatory bowel disease: Changing the game, or more of the same? United Eur. Gastroenterol. J. 2, 333–344. doi: 10.1177/2050640614550672
Raine, T., Bonovas, S., Burisch, J., Kucharzik, T., Adamina, M., Annese, V., et al. (2022). ECCO guidelines on therapeutics in ulcerative colitis: medical treatment. J. Crohns Colitis 16, 2–17. doi: 10.1093/ecco-jcc/jjab178
Sakurai, T., Saruta, M. (2023). Positioning and usefulness of biomarkers in inflammatory bowel disease. Digestion 104, 30–41. doi: 10.1159/000527846
Schirmer, M., Franzosa, E. A., Lloyd-Price, J., McIver, L. J., Schwager, R., Poon, T. W., et al. (2018). Dynamics of metatranscription in the inflammatory bowel disease gut microbiome. Nat. Microbiol. 3, 337–346. doi: 10.1038/s41564-017-0089-z
Schirmer, M., Stražar, M., Avila-Pacheco, J., Rojas-Tapias, D. F., Brown, E. M., Temple, E., et al. (2024). Linking microbial genes to plasma and stool metabolites uncovers host-microbial interactions underlying ulcerative colitis disease course. Cell Host Microbe 32, 209–226. doi: 10.1016/j.chom.2023.12.013
Segal, J. P., Leblanc, J.-F., Hart, A. L. (2021). Ulcerative colitis: an update. Clin. Med. 21, 135–144. doi: 10.7861/clinmed.2021-0080
Shen, Z.-H., Zhu, C.-X., Quan, Y.-S., Yang, Z.-Y., Wu, S., Luo, W.-W., et al. (2018). Relationship between intestinal microbiota and ulcerative colitis: Mechanisms and clinical application of probiotics and fecal microbiota transplantation. World J. Gastroenterol. 24, 5–14. doi: 10.3748/wjg.v24.i1.5
Tong, J., Liu, C., Summanen, P., Xu, H., Finegold, S. M. (2011). Application of quantitative real-time PCR for rapid identification of Bacteroides fragilis group and related organisms in human wound samples. Anaerobe 17, 64–68. doi: 10.1016/j.anaerobe.2011.03.004
Travis, S. P. L., Higgins, P. D. R., Orchard, T., van der Woude, C. J., Panaccione, R., Bitton, A., et al. (2011). Review article: defining remission in ulcerative colitis. Aliment Pharmacol. Ther. 34, 113–124. doi: 10.1111/apt.2011.34.issue-2
Wang, R., Li, Z., Liu, S., Zhang, D. (2023). Global, regional and national burden of inflammatory bowel disease in 204 countries and territories from 1990 to 2019: A systematic analysis based on the Global Burden of Disease Study 2019. BMJ Open 13, 1–15. doi: 10.1136/bmjopen-2022-065186
Wang, K., Liao, M., Zhou, N., Bao, L., Ma, K., Zheng, Z., et al. (2019). Parabacteroides distasonis Alleviates Obesity and Metabolic Dysfunctions via Production of Succinate and Secondary Bile Acids. Cell Rep. 26, 222–235.e5. doi: 10.1016/j.celrep.2018.12.028
Wu, X., Zhang, T., Zhang, T., Park, S. (2024). The impact of gut microbiome enterotypes on ulcerative colitis: identifying key bacterial species and revealing species co-occurrence networks using machine learning. Gut Microbes 16, 1–20. doi: 10.1080/19490976.2023.2292254
Keywords: ulcerative colitis, Akkermansia muciniphila, Parabacteroides distasonis, disease relapse, inflammation
Citation: Mendes-Frias A, Moreira M, Vieira MC, Gaifem J, Costa P, Lopes L and Silvestre R (2024) Akkermansia muciniphila and Parabacteroides distasonis as prognostic markers for relapse in ulcerative colitis patients. Front. Cell. Infect. Microbiol. 14:1367998. doi: 10.3389/fcimb.2024.1367998
Received: 09 January 2024; Accepted: 10 June 2024;
Published: 04 July 2024.
Edited by:
Valeriy Poroyko, Laboratory Corporation of America Holdings (LabCorp), United StatesReviewed by:
Kathrin S. Michelsen, Cedars Sinai Medical Center, United StatesCopyright © 2024 Mendes-Frias, Moreira, Vieira, Gaifem, Costa, Lopes and Silvestre. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ricardo Silvestre, cmljYXJkb3NpbHZlc3RyZUBtZWQudW1pbmhvLnB0
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.