 Chengwei Wang
Chengwei Wang Rongrong Xue
Rongrong Xue Xinru Wang
Xinru Wang Li Xiao
Li Xiao Jianchun Xian
Jianchun Xian
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Cell. Infect. Microbiol. , 16 May 2023
Sec. Virus and Host
Volume 13 - 2023 | https://doi.org/10.3389/fcimb.2023.1186877
This article is part of the Research Topic Viruses, Innate Immunity, and Antiviral Strategies: from Basic Research to Clinical Applications. View all 6 articles
Occult hepatitis B virus (HBV) infection (OBI) is a condition in which replication-competent viral DNA is detected in the liver (with detectable or undetectable HBV DNA in serum) of individual testing negative for HBV surface antigen (HBsAg). It is a risk factor for transfusion or transplant transmission, reactivation after immunosuppression or chemotherapy, and progression of chronic liver disease and hepatocarcinogenesis. The long-term stable presence of covalently closed circular DNA (cccDNA), which is fully replicative in the nucleus of infected hepatocytes is the molecular basis for the formation of OBI. HBV genome in liver tissue, HBV DNA and anti-HBc test in serum are the gold standard, common method and alternative markers for OBI diagnosis, respectively. Due to the stability of covalently closed circular DNA (cccDNA) and the long half-life of hepatocytes, the existence of OBI is extensive and prolonged. The low and/or intermittent replication of HBV in OBI patients, the limitations of the sensitivity of serological tests, and the non-standardized and invasive nature of liver histology render the “commonly used” serological tests are unreliable and the “gold standard” liver histology is impractical, thus the findings from studies on the formation, diagnosis and transplantation or transfusion transmission of HBV in OBI strongly suggest that the “alternative” marker, the anti-HBc test, may be the most reliable and practical approach for OBI diagnosis.
Occult hepatitis B virus (HBV) infection (OBI) is generally defined as the presence of replication-competent HBV DNA (i.e., HBV covalent closed circular DNA [cccDNA]) in the liver and/or HBV DNA in the blood of individuals who test negative for hepatitis B surface antigen (HBsAg) according to currently available assays. According to the HBV-specific antibody profile, OBI can be divided into seropositive OBI with positive hepatitis B core antibody (anti-HBc) and/or hepatitis B surface antibody (anti-HBs) and seronegative OBI with negative anti-HBc and anti-HBs. Among them, seronegative OBI accounts for about 1% to 20% of all OBI cases (Raimondo et al., 2019). OBI is a risk factor for transfusion or transplant transmission, reactivation after immunosuppression or chemotherapy, chronic liver disease progression and hepatocarcinogenesis (Saitta et al., 2022). Due to the stability of covalently closed circular DNA (cccDNA) and the long half-life of hepatocytes, the existence of OBI is extensive and prolonged, while the low and/or intermittent replication of HBV in patients with OBI (Morales-Romero et al., 2014; Saitta et al., 2022), the limitations of the sensitivity of serological tests, and the non-standardized and invasive nature of liver histology determine that the “commonly used” serological tests are unreliable and the “gold standard” liver histology is impractical. The practical results of research on the formation mechanism, diagnosis and transplantation or transfusion transmission of OBI strongly suggest that although there is a certain proportion of seronegative OBI, as long as anti-HBc is positive, then there is a high possibility of the presence of OBI, and the “alternative” marker anti-HBc test is the most reliable and practical method for the diagnosis of OBI. In this article, we explore the above issues in terms of the definition of OBI, the mechanism of covalently closed circular DNA (cccDNA) clearance, the limitations of diagnostic methods and the practical findings of transplantation/transfusion HBV transmission.
A sufficient and necessary condition for the diagnosis of OBI is the detection of replication-competent HBV DNA in the liver and/or HBV DNA in blood of HBsAg-negative individuals. Among them, the “gold standard” for diagnosis is the detection of HBV DNA in the liver tissue, the “commonly used” method is the detection of HBV DNA in the blood, and the anti-HBc test in blood is an “alternative” method for OBI diagnosis (Raimondo et al., 2019; Saitta et al., 2022) (Table 1). In the serological diagnosis of OBI, many experts and guidelines currently recommend a highly sensitive HBV DNA method with a lower limit of detection (10-20 IU/ml) (which should actually be the lower limit of quantification, author’s note), a wider linear range, and a higher specificity. However, due to the fact that HBV DNA in OBI patients is usually <200 IU/ml, of which 80%-90% is <20 IU/ml, with intermittent elevation/positive characteristics, along with the impact of test efficacy and method, serum/plasma extraction volume, sample volume, genotype coverage, internal standard setting and cost differences, facing shortcomings such as nucleic acid contamination, lack of industry regulation and standardization, thus the limitations of serum HBV DNA testing for OBI diagnosis are evident (Kang et al., 2014; Morales-Romero et al., 2014; Raimondo et al., 2019; Cai et al., 2022), the most prominent of which is the sensitivity of the assay.
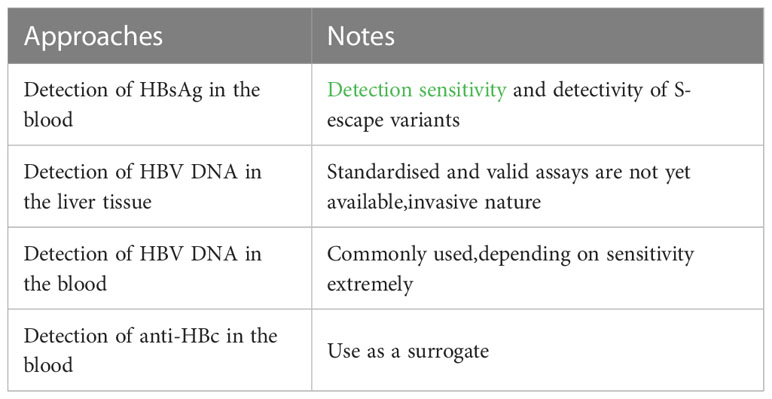
Table 1 Diagnosis of OBI.
Altunay et al. (2010) revealed that the rate of OBI detection among isolated anti-HBc positive individuals by serological methods was only 0.091% (Table 2). Cai et al. (2022) showed that the positive rate of HBV DNA detection in the serum of HBsAg(-)/anti-HBc(+) patients was 5.4% (108/2013)(see more details in Table 2). The detection rate may vary depending on the pattern of HBV serologic markers, with the highest detection rate in anti-HBe(+)/anti-HBc(+) status (15.61%, 32/205), followed by anti-HBs(+)/anti-HBe(+)/anti-HBc(+) (6.27%, 53/845), anti-HBc(+) (3.73%, 10/268), and anti-HBs(+)/anti-HBc(+) (1.87%,13/695) (Table 3). It is evident that anti-HBs is negatively correlated with the detection rate of OBI serologically, while anti-HBe is positively correlated with the detection rate of OBI serologically, which is also consistent with the role of anti-HBs and anti-HBe, since anti-HBs is a protective antibody, whereas anti-HBe is a sign that the body has a strong immune response and is still in the immune clearance or recovery phase (de Almeida Pondé, 2021). Candotti et al. (2019) showed that HBsAg, HBV DNA-negative donors were still at risk of transfusion-transmitted HBV even after 3 repeated tests using the most sensitive serologic method [lower limit of detection (LOD): 3.4 IU/mL], and reducing transfusion volume and receptor anti-HBs positivity contributed to prevention. The intermittent positivity of serum HBV DNA in patients with OBI shown in the evaluation of longitudinal studies also suggests that serum HBV DNA negativity does not exclude the existence of OBI even using the most sensitive serological methods. The sensitivity of quantitative serum HBV DNA testing for the diagnosis of OBI is not satisfactory, i.e., serologic methods, although commonly used, are not reliable.

Table 2 Summary of case reports.
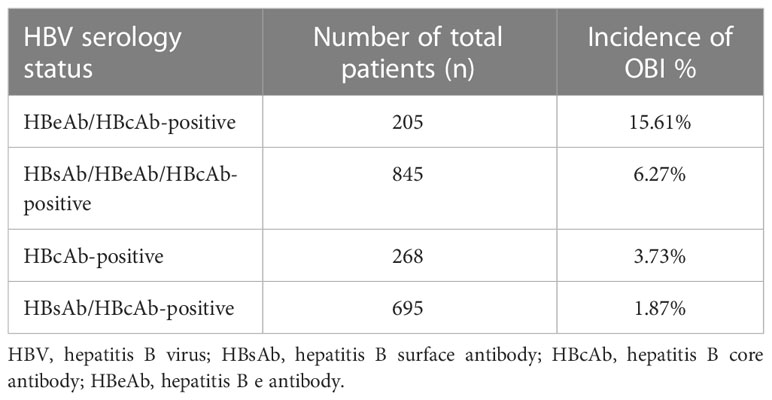
Table 3 OBI incidence depending on HBV serology makers.
The long-term stable presence of fully replicative cccDNA in the nucleus of hepatocytes is the main molecular basis of OBI (Zoulim, 2005). It is generally accepted that there are two balances in infection of HBV in human body, one between viral replication in hepatocytes and viral decline in circulation and the other between replenishment and decline of the cccDNA pool (Zeuzem et al., 1997; Murray et al., 2006; Dandri et al., 2008). The host immune function and drug interventions can affect the first balance, but hardly the second (Zeuzem et al., 1997; Murray et al., 2006; Dandri et al., 2008). Due to different clinical settings or host immune status, the half-life of cccDNA can range from 1 month to 26.2 months (Zeuzem et al., 1997; Murray et al., 2006; Dandri et al., 2008), and the half-life of HBV-infected hepatocytes can range from 10 to 100 days (Nowak et al., 1996). The incompleteness and lack of long-term effectiveness of host immune control and current antiviral drug treatment determine that virus DNA synthesis in hepatocytes can still not be completely blocked even with highly effective antiviral drug treatment. HBV DNA can still be detected in the liver even 30 years after HBsAg clearance or seroconversion (Zeuzem et al., 1997; Bläckberg and Kidd-Ljunggren, 2000; Murray et al., 2006; Dandri et al., 2008; Bes et al., 2012; Boyd et al., 2016), so once HBV infection is established, the cccDNA in liver or OBI status can persist for a long time or even for life.
A study from Japan showed that in a follow-up of 14 cases of acute self-limiting HBV infection with a median time of 4.2 years (range 1.8 to 9.5 years) after recovery, the serum positivity rate was 21.43% (3/14) by real-time polymerase chain reaction (PCR) detection (detection limit of 10 copies/ml). HBV cccDNA was detected in biopsy liver tissues (100%) in all 9 patients. However, only 2 out of 9 patients with positive HBV DNA in their liver tissues had positive serum results (2/9, 22.22%) (Yuki et al., 2003) (Table 2). Another study from Japan showed that in a follow-up of 15 patients with chronic hepatitis B after HBsAg seroclearance with a median follow-up time of 4.4 years (range 0.9 to 15.3 years), the serum occult hepatitis B infection (OBI) detection rate was 13.33% (2/15) by real-time PCR detection (quantitative lower limit of 200 copies/ml). However, HBV DNA was detected in all liver tissues of the patients examined (100%) (Komori et al., 2001) (Table 2). A review from Paris, France showed that the positivity rates of viral genome in serum and liver were 28% and 94%, respectively (Bréchot et al., 2001) (Table 2). A study from Italy showed that among 100 HBsAg-negative and anti-HBc-positive liver transplant donors (mean age 68.2 years, 64 males, 36 females), nested PCR detection of HBV DNA in liver tissue revealed that 52% (52/100) of the individuals had occult hepatitis B infection (OBI) (defined as positive for nested PCR in at least 2 different HBV genome regions). Among the 52 individuals who tested positive for nested PCR in liver tissue, digital droplet PCR (ddPCR) was used to detect cccDNA in liver cells, and the positivity rate was 52% (27/52). Using real-time PCR, only 22.2% (6/27) of individuals who tested positive for cccDNA by ddPCR had positive HBV DNA in their blood (all <20 IU/ml) (Caviglia et al., 2018), indicating that the sensitivity of serological methods for diagnosing OBI is significantly lower than that of ddPCR and nested PCR techniques in liver tissue (Table 2). Knöll A et al. (Knöll et al., 2006). (Table 2) examined serologic HBV DNA in 545 patients with isolated anti-HBc(+) and liver tissue HBV DNA in 37 patients with negative serum HBV DNA but isolated anti-HBc(+). The results showed a serology positivity rate of 8.1% (44/545) with a detection limit of 50-100 copies/ml. The highest positivity rate was observed in the age group of 1-30 years (4/27; 14.8%), while the lowest was observed in the age group of >80 years (1/21; 4.8%), but with a non-linear relationship between age and positivity rate. Among the 37 patients with HBV DNA negative serology, 15 (40.54%) were found to be HBV DNA positive in liver tissue samples, indicating that even in cases where the serological detection rate is 0, the liver tissue positivity rate can reach 40% as long as the serum anti-HBc is positive. These findings suggest that the serology method has a lower positivity rate (8.1-28%) compared to the liver histology positivity rate (50-100%).
The above comparison study of serology and liver histology suggests that the positivity rate of serology for diagnosing occult hepatitis B infection (OBI) is only about 10%-20% of that of liver histology. Additionally, the age of the host and the mode of prior HBV infection are also related to the detection rate of OBI.
A study in Spain retrospectively reviewed 25 cases of liver transplant recipients with negative HBV markers between 1995 and 1998 who received liver from donors positive for HBsAg (-)/anti-HBc (+). The results showed that 15 cases (60%, 15/25) developed hepatitis B (confirmed by detection of HBsAg in two consecutive serum samples) (Prieto et al., 2001) (Table 4). In the study by Uemoto et al (Uemoto et al., 1998), 16 cases of anti-HBc (+)/anti-HBs (+) (14 cases also positive for anti-HBe) donor livers were transplanted to recipients who were negative for anti-HBs and lacking prophylaxis. Among the recipients, 15 cases (93.75%) showed positive HBsAg in their serum (Table 4). In 50%-73% of anti-HBc (+) liver donors, HBV DNA was detected in liver, but all donors had negative HBV DNA in their serum. Anti-HBc (+) is a risk marker for HBV transmission and reactivation after liver transplantation (Uemoto et al., 1998). The risk of HBV transmission from the anti-HBc(+) liver donors to the recipients ranged from 25% - 95%, and the presence of anti-HBs from the donors did not appear to provide good protection against HBV transmission to the recipients (Uemoto et al., 1998; Prieto et al., 2001; Muñoz, 2002). The information provided by these studies strongly suggests that the absence of serum HBV DNA in anti-HBc (+) donors does not rule out the possibility of HBV transmission to the recipient. In addition, the synthesis of cccDNA and HBcAg is closely related to the production of anti-HBc (Moretto et al., 2020). Therefore, the detection of anti-HBc in blood can be used as an alternative biomarker for OBI, and as a more reliable marker for the diagnosis of OBI. This may also be a key reason why the 2017 EASL (European Association for the Study of the Liver et al., 2017) and Pollicino et al (Pollicino and Caminiti, 2021). consider HBsAg-negative/anti-HBc-positive status as an OBI phase in the natural history of HBV infection.

Table 4 HBsAg(-)/anti-HBc(+) liver donor transmitting HBV.
In summary, the detection rate of “commonly used” serological methods for OBI diagnosis using highly sensitive HBV DNA tests is mostly below 20%, while the “gold standard” of liver histology has a higher detection rate up to 50% or more. However, liver histology is an invasive examination and is currently not standardized. This indicates that the “common” methods are unreliable for the diagnosis of OBI, while the reliable “gold standard” method is not practical. The mechanism of difficulty in cccDNA clearance, as well as the results of research on the formation, diagnosis, and transmission of HBV through transplantation or transfusion strongly suggest that the possibility of OBI in anti-HBc positive individuals can reach over 90%. Therefore, the “alternative” anti-HBc test is the most reliable and practical marker for OBI diagnosis.
RX and XW contributed to the initial manuscript writing and literature search. CW, LX, and JX participated in scientific discussions and contributed to the writing of some sections. JX proposed the writing ideas, provided guidance, revised the manuscript, and finalized the paper. All authors contributed to the article and approved the submitted version.
This study was supported by Taizhou Science and Technology Support Program (Social Development) Project (TS201813).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Altunay, H., Kosan, E., Birinci, I., Aksoy, A., Kirali, K., Saribas, S., et al. (2010). Are isolated anti-HBc blood donors in high risk group? the detection of HBV DNA in isolated anti-HBc cases with nucleic acid amplification test (NAT) based on transcription-mediated amplification (TMA) and HBV discrimination. Transfusion Apheresis Sci. 43 (3), 265–268. doi: 10.1016/j.transci.2010.09.012
Bes, M., Vargas, V., Piron, M., Casamitjana, N., Esteban, J. I., Vilanova, N., et al. (2012). T Cell responses and viral variability in blood donation candidates with occult hepatitis b infection. J. Hepatol. 56 (4), 765–774. doi: 10.1016/j.jhep.2011.11.011
Bläckberg, J., Kidd-Ljunggren, K. (2000). Occult hepatitis b virus after acute self-limited infection persisting for 30 years without sequence variation. J. Hepatol. 33 (6), 992–997. doi: 10.1016/S0168-8278(00)80134-8
Boyd, A., Lacombe, K., Lavocat, F., Maylin, S., Miailhes, P., Lascoux-Combe, C., et al. (2016). Decay of ccc-DNA marks persistence of intrahepatic viral DNA synthesis under tenofovir in HIV-HBV co-infected patients. J. Hepatol. 65 (4), 683–691. doi: 10.1016/j.jhep.2016.05.014
Bréchot, C., Thiers, V., Kremsdorf, D., Nalpas, B., Pol, S., Paterlini-Bréchot, P. (2001). Persistent hepatitis b virus infection in subjects without hepatitis b surface antigen: clinically significant or purely “occult”? Hepatology 34 (1), 194–203. doi: 10.1053/jhep.2001.25172
Cai, J., Wu, W., Wu, J., Chen, Z., Wu, Z., Tang, Y., et al. (2022). Prevalence and clinical characteristics of hepatitis b surface antigen-negative/hepatitis b core antibody-positive patients with detectable serum hepatitis b virus DNA. Ann. Trans. Med. 10 (1). doi: 10.21037/atm-21-6272
Candotti, D., Assennato, S. M., Laperche, S., Allain, J. P., Levicnik-Stezinar, S. (2019). Multiple HBV transfusion transmissions from undetected occult infections: revising the minimal infectious dose. Gut 68 (2), 313–321. doi: 10.1136/gutjnl-2018-316490
Caviglia, G. P., Abate, M. L., Tandoi, F., Ciancio, A., Amoroso, A., Salizzoni, M., et al. (2018). Quantitation of HBV cccDNA in anti-HBc-positive liver donors by droplet digital PCR: a new tool to detect occult infection. J. Hepatol. 69 (2), 301–307. doi: 10.1016/j.jhep.2018.03.021
Dandri, M., Murray, J. M., Lutgehetmann, M., Volz, T., Lohse, A. W., Petersen, J. (2008). Virion half-life in chronic hepatitis b infection is strongly correlated with levels of viremia. Hepatology 48 (4), 1079–1086. doi: 10.1002/hep.22469
de Almeida Pondé, R. A. (2021). Dynamic profile of the HBeAg-anti-HBe system in acute and chronic hepatitis b virus infection: a clinical-laboratory approach. Mol. Biol. Rep. 48 (1), 843–854. doi: 10.1007/s11033-020-06056-4
European Association for the Study of the Liver, Electronic Address EEE, European Association for the Study of The L (2017). EASL 2017 clinical practice guidelines on the management of hepatitis b virus infection. J. Hepatol. 67 (2), 370–398. doi: 10.1016/j.jhep.2017.03.021
Kang, S. Y., Kim, M. H., Lee, W. I. (2014). Occult hepatitis b virus infection in Korean patients with isolated anti-HBc. Arch. Virol. 159, 227–233. doi: 10.1007/s00705-013-1810-8
Knöll, A., Hartmann, A., Hamoshi, H., Weislmaier, K., Jilg, W. (2006). Serological pattern “anti-HBc alone”: characterization of 552 individuals and clinical significance. World J. Gastroenterol: WJG 12 (8), 1255.
Komori, M., Yuki, N., Nagaoka, T., Yamashiro, M., Mochizuki, K., Kaneko, A., et al. (2001). Long-term clinical impact of occult hepatitis b virus infection in chronic hepatitis b patients. J. Hepatol. 35 (6), 798–804. doi: 10.1016/S0168-8278(01)00214-8
Morales-Romero, J., Vargas, G., García-Román, R. (2014). Occult HBV infection: a faceless enemy in liver cancer development. Viruses 6 (4), 1590–1611. doi: 10.3390/v6041590
Moretto, F., Catherine, F. X., Esteve, C., Blot, M., Piroth, L. (2020). Isolated anti-HBc: significance and management. J. Clin. Med. 9 (1), 202. doi: 10.3390/jcm9010202
Muñoz, S. J. (2002). Use of hepatitis b core antibody–positive donors for liver transplantation. Liver Transplant. 8 (10), S82–S87.
Murray, J. M., Purcell, R. H., Wieland, S. F. (2006). The half-life of hepatitis b virions. Hepatology 44 (5), 1117–1121. doi: 10.1002/hep.21364
Nowak, M. A., Bonhoeffer, S., Hill, A. M., Boehme, R., Thomas, H. C., McDade, H. (1996). Viral dynamics in hepatitis b virus infection. Proc. Natl. Acad. Sci. 93 (9), 4398–4402. doi: 10.1073/pnas.93.9.4398
Pollicino, T., Caminiti, G. (2021). HBV-integration studies in the clinic: role in the natural history of infection. Viruses 13 (3), 368. doi: 10.3390/v13030368
Prieto, M., Gómez, M. D., Berenguer, M., Córdoba, J., Rayón, J. M., Pastor, M., et al. (2001). De novo hepatitis b after liver transplantation from hepatitis b core antibody–positive donors in an area with high prevalence of anti-HBc positivity in the donor population. Liver Transplant. 7 (1), 51–58. doi: 10.1053/jlts.2001.20786
Raimondo, G., Locarnini, S., Pollicino, T., Levrero, M., Zoulim, F., Lok, A. S. (2019). Taormina workshop on occult HBV infection faculty members. update of the statements on biology and clinical impact of occult hepatitis b virus infection. J. Hepatol. 71 (2), 397–408.
Saitta, C., Pollicino, T., Raimondo, G. (2022). Occult hepatitis b virus infection: an update. Viruses 14 (7), 1504. doi: 10.3390/v14071504
Uemoto, S., Sugiyama, K., Marusawa, H., Inomata, Y., Asonuma, K., Egawa, H., et al. (1998). Transmission of hepatitis b virus from hepatitis b core antibody-positive donors in living related liver transplants. Transplantation 65 (4), 494–499. doi: 10.1097/00007890-199802270-00007
Yuki, N., Nagaoka, T., Yamashiro, M., Mochizuki, K., Kaneko, A., Yamamoto, K., et al. (2003). Long-term histologic and virologic outcomes of acute self-limited hepatitis b. Hepatology 37 (5), 1172–1179. doi: 10.1053/jhep.2003.50171
Zeuzem, S., Robert, A., Honkoop, P., Roth, W. K., Schalm, S. W., Schmidt, J. M. (1997). Dynamics of hepatitis b virus infection in vivo. J. Hepatol. 27 (3), 431–436. doi: 10.1016/S0168-8278(97)80345-5
Keywords: hepatitis B virus, high-sensitivity HBV DNA test, occult HBV infection (OBI), hepatocellular carcinoma, cirrhosis
Citation: Wang C, Xue R, Wang X, Xiao L and Xian J (2023) High-sensitivity HBV DNA test for the diagnosis of occult HBV infection: commonly used but not reliable. Front. Cell. Infect. Microbiol. 13:1186877. doi: 10.3389/fcimb.2023.1186877
Received: 15 March 2023; Accepted: 25 April 2023;
Published: 16 May 2023.
Edited by:
Elisa Fanunza, University of Cagliari, ItalyReviewed by:
Salma Aktar, The University of Texas Health Science Center at San Antonio, United StatesCopyright © 2023 Wang, Xue, Wang, Xiao and Xian. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianchun Xian, eGlhbmpjMDlAMTYzLmNvbQ==
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.