 Drifa Frostadottir
Drifa Frostadottir Lisa Wasserstrom
Lisa Wasserstrom Karolin Lundén1,2
Karolin Lundén1,2 Lars B. Dahlin
Lars B. Dahlin- 1Department of Translational Medicine – Hand Surgery, Lund University, Malmö, Sweden
- 2Department of Hand Surgery, Skåne University Hospital, Malmö, Sweden
- 3Clinical Microbiology, Laboratory Medicine Skåne, Lund, Sweden
- 4ESCMID Study Group for Legionella Infections (ESGLI), Basel, Switzerland
- 5Department of Biomedical and Clinical Sciences, Linköping University, Linköping, Sweden
Extrapulmonary manifestations of infection with Legionella species, of which 24 may cause disease in humans, are very rare. Here, we describe a case of a 61-year-old woman with no history of immunosuppression presenting with pain and swelling of her index finger after a prick by rose thorns during gardening. Clinical examination showed fusiform swelling of the finger with mild redness, warmth, and fever. The blood sample revealed a normal white blood cell count and a slight increase in C-reactive protein. Intraoperative observation showed extensive infectious destruction of the tendon sheath, while the flexor tendons were spared. Conventional cultures were negative, while 16S rRNA PCR analysis identified Legionella longbeachae that also could be isolated on buffered charcoal yeast extract media. The patient was treated with oral levofloxacin for 13 days, and the infection healed quickly. The present case report, with a review of the literature, indicates that Legionella species wound infections may be underdiagnosed due to the requirement for specific media and diagnostic methods. It emphasizes the need for heightened awareness of these infections during history taking and clinical examination of patients presenting with cutaneous infections.
Introduction
Legionella species (spp.) are gram-negative rod bacteria and present primarily in aqueous environments and soil, where they are adapted to survive and replicate intracellularly in protozoa. The intracellular mechanism behind Legionella infections is well described for Legionella pneumophila in mammalian tissue culture models, mainly using macrophage-like tissue, but also epithelial cells, where the primary mechanism of infection after internalization in these cell types is similar. Both L. pneumophila and Legionella longbeachae replicate inside the host by forming a Legionella-containing vacuole (LCV) that fuses with mitochondria and associates with the endoplasmic reticulum (ER) exit vesicle. By mimicking the host’s own ER vesicles, the bacteria can evade intracellular defenses, such as phagocytosis (Newton et al., 2010). The LCV delivers virulence-associated proteins by a Dot/Icm type 4B secretion system that modulates many different host signaling pathways, including anti-apoptotic effectors to prevent cell death during replication and proapoptotic effectors to promote exit of the bacteria at the end of the infection cycle (Mondino et al., 2020). Little is still known about the virulence of L. longbeachae, but studies have shown that mice are more susceptible to L. longbeachae than L. pneumophila, possibly due to the absence of flagella, which has a role in triggering cell death. Also, the presence of a capsule might protect L. longbeachae against phagocytosis (Cazalet et al., 2010).
There are over 60 Legionella species reported of which 24 may cause an infection in humans (Bell et al., 2021; Girolamini et al., 2022). The clinical manifestations of legionellosis vary from an acute, febrile illness (i.e., Pontiac fever) to potentially fatal pneumonia (i.e., Legionnaires’ disease). The mortality rate of Legionnaires’ disease varies and depends on the underlying status of the patient as well as the promptness of diagnosis and treatment. In Europe, L. pneumophila is the predominant pathogenic species causing 95% of Legionnaires’ disease. It spreads via amoeba present in man-made water systems, such as fountains, bubble baths, and cooling towers (Fields et al., 2002). Out of the remaining 5%, several other species can cause the disease with L. longbeachae, first isolated in 1980 in a patient with pneumonia in Long Beach, CA, USA (Whiley H, 2011), being the most common (Whiley H, 2011). However, due to a diagnostic shortage in detecting non-pneumophila species, these species are most likely underdiagnosed. Interestingly, in Australia and New Zealand, Legionnaires’ disease caused by L. longbeachae is as common as L. pneumophila, and since spreading has only been associated with compost and potting soil, commercially bagged soiled is marked with health warning symbols in these countries (Montanaro-Punzengruber et al., 1999). Extrapulmonary manifestations of Legionella spp. are extremely rare, but reported sites include brain (Charles et al., 2013), septic arthritis (Bemer et al., 2002; Linscott et al., 2004; Naito et al., 2007; Flendrie et al., 2011; Just et al., 2012; Thurneysen and Boggian, 2014; Banderet et al., 2017), pericarditis (Svendsen et al., 1987), and cutaneous infections (Table 1). Here, we describe a case of soft tissue infection by L. longbeachae in the index finger, pricked by rose thorns during gardening, in an immunocompetent person. We also review the available literature on these rare soft tissue infections caused by different Legionella spp.
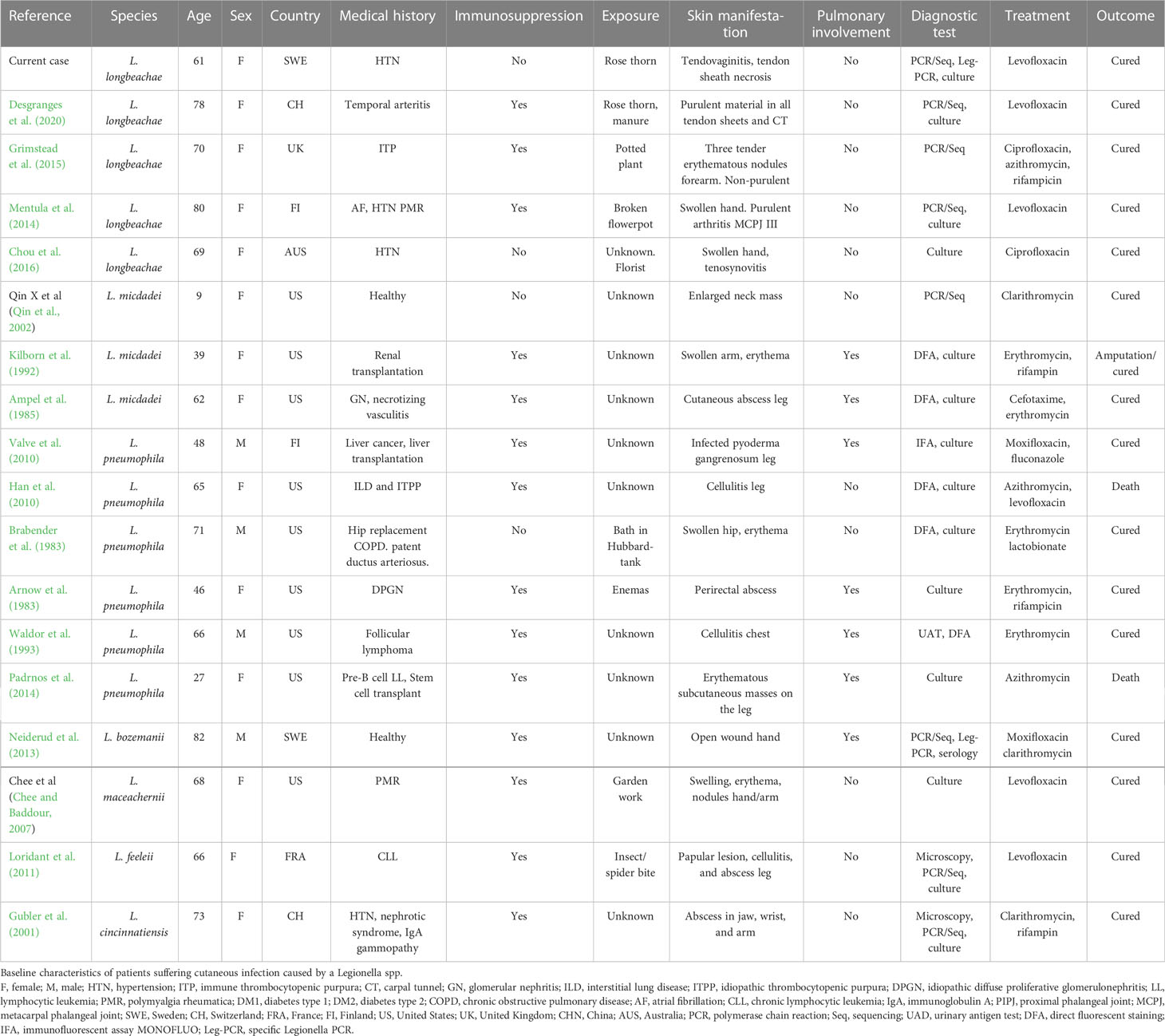
Table 1 Patient group characteristics.
Case report
A 61-year-old woman, without any history of immunosuppression or severe underlying disease, but treated for hypertension and hyperlipidemia, presented at our hospital with a 1-day history of fever and a painful swollen right index finger, which had started in the tip of the finger. The symptoms had spread to the base of the index finger, also involving her thumb and long finger upon arrival at the hospital. Two days earlier, she had been working in her garden, planting roses with locally purchased bagged soil and groundcover bark. Despite wearing gardening gloves, she had pricked her finger on the rose thorns.
On examination, she reported extreme pain on palpation along the volar aspect of the finger and on attempting extension and flexion of the finger. The index finger showed fusiform swelling with mild redness and warmth as well as some swelling of the thumb and long finger without pain. She had a fever (39.5°C) and chills, while other hemodynamic parameters were stable. She had no respiratory symptoms. White blood cell count was normal, 7.7 × 109 cells/L (normal range 4.3–10.8), and C-reactive protein was 23 mg/L (normal < 5 mg/L).
The patient was promptly taken to operation due to strong suspicion of an aggressive infection. An incision at the level of A1 pulley of the tendon sheath at the base of the index finger showed destruction of the tendon sheath that had dissolved, leaving only brown jellylike remains. The subcutaneous tissue was very swollen and distended from the wound. The incision was extended to the tip of the finger, revealing the same destruction in the rest of the tendon sheath from the A1 to the A5 pulleys. Interestingly, the flexor tendons seemed unaffected as well as the dermis and epidermis, which showed no discoloration. The surgical wound was washed extensively with sterile saline after retrieving tissue culture from the destructed tendon sheath. The tissue was divided into two ESwab tubes (Copan, Brescia, Italy) for microbiological cultivation and 16S rRNA PCR analysis due to the unusual presentation and sent for analysis at the Regional Clinical Microbiology Laboratory in Lund, Sweden. The patient was treated with benzylpenicillin 3 g and clindamycin 600 mg intravenously three times daily. Postoperatively, the patient’s health status remained stable, and her fever dropped, but with remaining subcutaneous swelling distending from the wound and with extensive transparent yellowish secretion (Figure 1A). Aerobic standard cultivation was performed with the first sample on blood agar plates (Neogen, Lansing, MI, USA), hematin agar plates (Oxoid Ltd., Basingstoke, UK), Gc-D Agar plates (Difco GC agar base, BD, Franklin Lakes, USA, supplemented with Vitox, Oxoid Ltd., Basingstoke, UK) in 5% CO2, and anaerobic cultivation on FAA agar plates and FAA broth (Neogen, Lansing, MI, USA). From the second sample, nucleic acid was extracted and analyzed with 16S rRNA PCR and Sanger sequencing, using forward primer (P5f) 5′-TGC CAG CMG CCG CGG TWA-3′ and reverse primer (P1067r) 5′-AAC ATY TCA CRA CAC GAG CT-3′ (Eurofins Genomics, Ebersberg, Germany) adapted from Relman et al. (1993). The sequencing results from the forward and reverse strands were aligned using BioNumerics software (Applied Maths NV (bioMérieux), Sint-Martens-Latem, Belgium) and analyzed using BLASTn (Bethesda, 2004) that identified L. longbeachae with 99% identity (552/553 bases) on postoperative day 3. Based on the PCR results, the treatment regime was changed to levofloxacin 500 mg twice daily with prolonged treatment with benzylpenicillin while waiting on the standard cultures. The L. longbeachae result could be confirmed (Cq of 25) using a newly established in-house multiplex real-time PCR method, modified from Cross et al. (2016), that targets the 23S–5S rRNA spacer region common to all L. spp. and identifies L. longbeachae, L. micdadei, L. bozemanii, and L. anisa using species-specific probes (Eurofins Genomics, Ebersberg, Germany). To confirm the PCR result, cultivation was performed with a small amount of remaining sample on buffered charcoal yeast extract agar containing Legionella BCYE Growth Supplement (BCYE agar) and BCYE agar containing Legionella BMPA Growth Supplement (BMPA agar) (Oxoid Ltd., Basingstoke, UK) and incubated at 35°C and 5% CO2. Postoperatively at day 7, a total of five colonies had appeared (Figure 2) that could be identified as L. longbeachae using matrix-assisted laser desorption/ionization–time of flight (MALDI-TOF) (Vitek MS; bioMérieux, France). The standard cultures showed no bacterial growth. The patient improved by treatment with levofloxacin and was dismissed from the hospital on postoperative day 11. Two weeks after surgery, the patient started physical therapy. The patient stopped levofloxacin treatment after a total of 13 days. The wound then healed, and the swelling improved (Figures 1B, C), but the patient developed a painful Achilles tendonitis bilateral as well as generalized muscle pain, which is a well-known side effect of levofloxacin. Treatment with levofloxacin was stopped, even though no previous experience of fewer than 3 weeks of antibiotic treatment has been described among patients with Legionella wound infection. The patient started physical therapy and regained full range of motion without bowstringing and normal sensation 2 months postoperatively (Figure 1D).

Figure 1 (A) Patients’ right hand and index finger at day 1 postoperatively, (B) at day 10 postoperatively, (C) at day 13 postoperatively, and (D) at 2 months postoperatively.
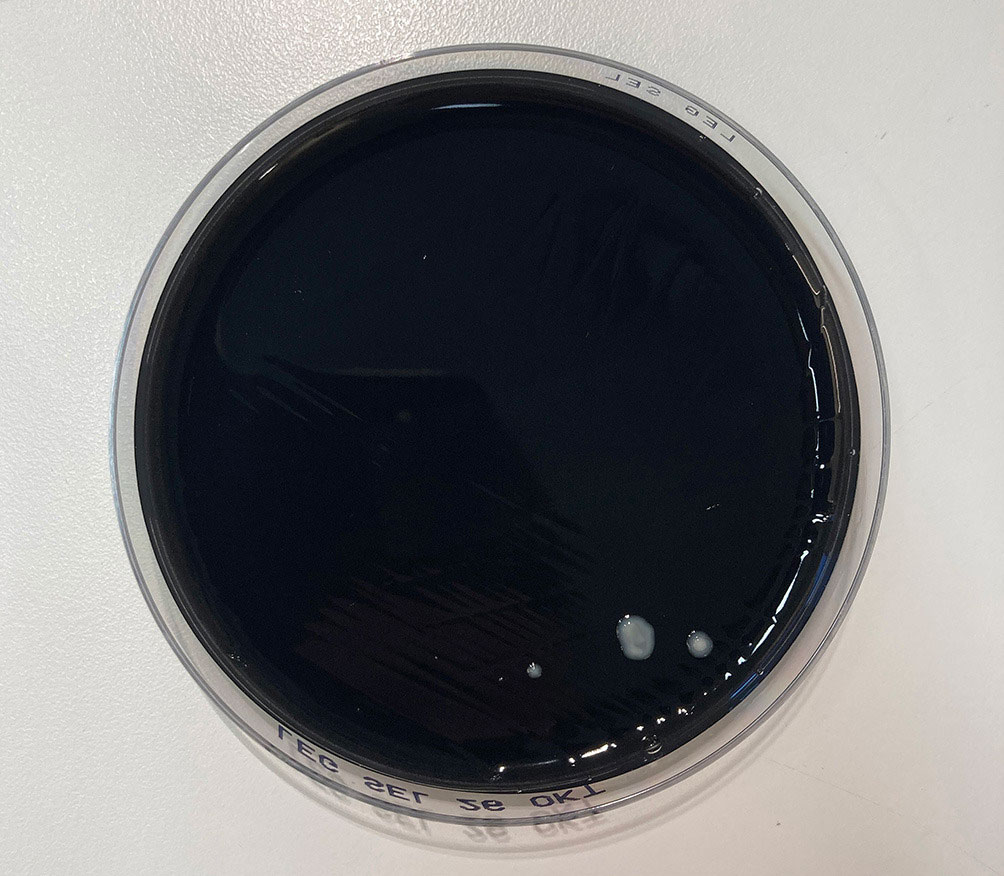
Figure 2 A total of five colonies of Legionella longbeachae colonies grew on buffered charcoal yeast extract agar (BCYE).
Infection with L. longbeachae is a notifiable disease according to Swedish law. Samples were taken from the patient’s garden and water, but Legionella cultures were negative. Samples from the patient’s garden gloves were also analyzed with Legionella 23S-5S real-time PCR, which showed weak amplification of Legionella species at Cq > 35, but no Legionella colonies could be cultivated on BCYE agar (i.e., 2 months after the infection).
Review of reported cases
Methods
A literature search on PubMed from start through December 2022 using the terms “Legionella”, “Legionella” combined with “longbeachae”, “pneumophila”, “bozemanii”, and “micdadei” with an additional search of combined “soft tissue”, “skin”, “cutaneous manifestation”, “infection”, and “wound”. The retrieved articles were reviewed to identify additional cases of Legionella skin and soft tissue infection. The inclusion criteria were cutaneous legionellosis confirmed with PCR or culture positive for L. longbeachae, L. pneumophila, L. bozemanii, L. feeleii, L. micdadei, or L. cincinnatiensis. Exclusion criteria were postoperative infection, septic arthritis, suspected blood-borne infection, or pulmonary involvement preceding the cutaneous infection.
Results
Baseline characteristics
Our review included 18 cases of confirmed Legionella spp. cutaneous infections. Of those, 5/18 were L. longbeachae, 6/18 were L. pneumophila, 3/18 were L. micdadei, 1/18 was L. bozemanii, 1/18 was L. maceachernii, 1/18 was L. feeleii, and 1/18 was L. cincinnatiensis.
Women suffered more commonly a cutaneous infection with Legionella spp. than men (14/18, 78%), where the median age was 66 [48–71 interquartile range] (Table 1). Country of origin was most commonly the United States (9/18) followed by Finland (2/18), Sweden (2/18), Switzerland (2/18), France (1/18), United Kingdom (1/18), and Australia (1/18).
Medical history and immunosuppression
Of the patients diagnosed with a cutaneous infection caused by a Legionella spp., 14/18 (78%) were treated with immunosuppressive medication for underlying conditions. These conditions included temporal arteritis, immune thrombocytopenic purpura, polymyalgia rheumatica (PMR), glomerulonephritis, renal transplantation, liver transplantation, interstitial lung disease, lymphoma, and leukemia.
Exposure and cutaneous manifestation
All the L. longbeachae cutaneous infections manifested after garden work with flowers or flowerpots. This also included the infection related to L. maceachernii. For the rest of the infections, the exposure was either unknown or unclear.
Diagnostic studies
The most common test to first yield Legionella spp. was general 16S rRNA PCR and Sanger sequencing 8/18 (44%) (depicted as PCR/Seq in Table 1) followed by culturing on BCYE agar. In addition to 16S rRNA PCR, two of the articles performed a confirmatory Legionella-specific PCR that identified L. bozemanii (Neiderud et al., 2013) and L. longbeachae (current case). Other methods used to detect Legionella included direct fluorescent antibody (DFA) assays (Brabender et al., 1983; Ampel et al., 1985; Kilborn et al., 1992; Waldor et al., 1993; Han et al., 2010), immunofluorescent assay MONOFLUO (IFA) (Valve et al., 2010), and cultivation on chocolate agar (Arnow et al., 1983). Urinary Legionella Antigen Test (UAT) was used in two of the cases, but both yielded negative results (Padrnos et al., 2014; Grimstead et al., 2015).
Treatment and outcome
All the patients were treated with fluoroquinolones and/or macrolides in single or combination therapy after diagnosis of a Legionella spp. Single therapy was prescribed in 9/18 cases (50%). Of those, 6/18 (33%) received fluoroquinolones [levofloxacin 5/6 (83%) (Chee and Baddour, 2007; Loridant et al., 2011; Mentula et al., 2014; Desgranges et al., 2020) and ciprofloxacin 1/6 (17%) (Chou et al., 2016)], and 3/18 (15%) received macrolides [clarithromycin 1/3 (33%) (Qin et al., 2002), erythromycin 1/3 (33%) (Waldor et al., 1993), and azithromycin 1/3 (33%) (Padrnos et al., 2014)]. Combination therapy of fluoroquinolones and macrolides was prescribed in 3/18 (15%) (Han et al., 2010; Neiderud et al., 2013; Grimstead et al., 2015). Of the remaining cases, 5/18 (28%) were treated with macrolides in combination with other antibiotics (Arnow et al., 1983; Brabender et al., 1983; Ampel et al., 1985; Kilborn et al., 1992; Gubler et al., 2001), and 1/18 was treated with fluoroquinolones combined with fluconazole (Valve et al., 2010).
The recommendation for the treatment of Legionnaires’ disease is azithromycin or levofloxacin since they are highly effective and have fewer side effects than erythromycin (Phin et al., 2014). To the best of our knowledge, no specific recommendations exist for cutaneous Legionella infections.
Discussion
Cutaneous infections caused by Legionella spp. are rare, and to this date, there are only 18 published cases (including the current case), reporting a diagnostically verified infection. In our case, L. longbeachae seemed to selectively attack the tendon sheath, causing it to dissolve into brown discolored remains while sparing the tendon. We found only a few descriptions of intraoperative findings in the literature with no similar description as our findings. This leads us to the conclusion that there is a clear need for a more detailed description of intraoperative findings on cases of legionella wound infections for clinical suspicion of Legionella spp. to rise early in the treatment process. Interestingly, Jäger et al. (2014), while studying the effect of L. pneumophila infection on the lung tissue, showed that L. pneumophila adheres to the alveolar lining and primarily infects alveolar macrophages, causing damage to the alveolar septa. Nevertheless, we found no connection in the literature between the selectiveness of L. longbeachae to the tendon sheath and its destruction.
After less than 2 weeks of treatment, the present patient experienced quite severe side effects from the levofloxacin in the form of muscle, joint, and tendon pain. This is a well-known side effect where the risk increases with age over 60 years, concomitant corticosteroid therapy, renal dysfunction, and a history of organ transplantation (Bidell and Lodise, 2016). The present patient had therefore a relatively short levofloxacin treatment compared to other published cases yet regained full recovery. This might help in determining treatment lengths for future patients experiencing similar side effects.
In our review, 78% of the patients were women with a median age of 66 years. This is an interesting finding since epidemiological studies have shown that women are at less risk than men when it comes to developing most infectious diseases. The sex hormone estradiol appears to confer protective immunity, a hormone that is reduced after menopause. This could yet explain the high percentage of women found to suffer from L. longbeachae wound infection since the larger part of the women included in our review can be assumed to have been postmenopausal (Gay et al., 2021). Another factor is occupation and lifestyle activities that can play a major role in exposure to pathogens. Still, the authors found no published studies indicating that gardening was more common among women than men. Of the 18 included patients in our review, 78% were treated with immunosuppressive medication for underlying conditions. Nevertheless, in our case, the patients did not have any history of immunosuppression. In otherwise healthy patients, it is uncommon to have complex rare skin infections, which might play a role in the choice of microbial analyses. To enable the detection of Legionella, the clinician must specifically ask for that analysis since Legionella requires specific growth conditions, or the use of 16S rRNA analysis was the most common test to first yield Legionella spp. in the reviewed cases including the present case. In our clinic, it is not standard to order a wide range of microbial cultures when an otherwise healthy patient presents with septic tenosynovitis. Again, a culture-negative infection that is hard to treat with broad-spectrum antibiotics appears, needing repeated surgery with surgical debridement and washing before the infection subsides without a clear diagnosis. One might wonder if the number of immunosuppressed patients in these cases is perhaps not representative of the total population but rather the population that is prescribed the right cultures due to a higher risk for complicated infections. This means that the number of true cases is hard to estimate. In our region, we are only aware of three additional cutaneous infections identified by 16S rRNA analysis, two of which could be cultivated (L. sainthelensis and L. pneumophila).
An obstacle to suggesting that one expands the prescribed microbial analysis per patient is most certainly the cost, but also time. An additional 16S rRNA PCR is time-consuming and expensive and, most importantly requires a sample collected from a normally sterile location. Otherwise, it is impossible to interpret the result correctly since the PCR will amplify all the bacteria present in the sample. Therefore, a clear protocol is needed to guide physicians and surgeons in their choice of microbial analyses.
All the reviewed L. longbeachae cutaneous infections (5/18) manifested after garden work with flowers or flowerpots. A recent study on the frequency of L. longbeachae on gardening gloves using a L. longbeachae-specific PCR showed the presence of the bacterium on 14% of the gloves (11/76), postulating that gloves could be a vector and contribute to Legionella infections (Chambers et al., 2021). In our case, 23S–5S rRNA Legionella-specific real-time PCR on a swab sample taken from the patients’ gloves, stored for 2 months since the debut of infection in a dry place, gave a low amplification for PAN-Legionella but not specifically for L. longbeachae. Cultivation on BCYE and BMPA media did not result in Legionella growth, whereby the source of the bacteria could not be determined. To identify the source of the Legionella spp. causing the infection is time-consuming work involving sampling and cultivation of many environmental samples followed by molecular typing to determine if there is an epidemiological match to the patient strain. For various types of water reservoirs, the sampling methods are rather well established, and the presence of Legionella spp. has been well studied (Kanarek et al., 2022). For soil, it is more problematic and varies depending on the country. In a soil survey conducted in Australia in 1989–1990, 73% of potting soil samples tested positive for Legionella, and 75% of these contained L. longbeachae. In a study conducted in Switzerland in 2009, 21/46 (46%) of potting soils contained Legionella spp (Steele et al., 1990; Casati et al., 2009). The discrepancies between countries might be explained by a variety of factors, including climate, the composition of the soil in the bags, and the methods used in production. During a L. longbeachae outbreak in Sweden in 2018, Löf et al. (2021) tried to identify the disease-causing strains by sequencing isolated patient and environmental strains. They could determine a higher risk for L. longbeachae infection if the patient had been handling bagged compost and/or soil, but a direct connection to the patient isolates could not be established by next-generation sequencing (NGS) since the soil isolates were polyclonal, thus containing several L. longbeachae strains (Löf et al., 2021).
Conclusion
To the best of our knowledge, this is the largest review of cutaneous Legionella cases, and our case adds information to the limited existing literature on similar patients. Legionella spp. may be an underdiagnosed source of extrapulmonary infections due to the requirement for specific media and diagnostic methods. These infections can go undetected for a long time and cause serious infections. We believe special attention and heightened awareness of these infections during history taking and clinical examination of patients presenting with atypical cutaneous infections is therefore important.
Ethics statement
Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.”
Author contributions
All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors are grateful to Yuk Ting Siu at the Department of Clinical Microbiology, Infection Control and Prevention, Skåne University Hospital, Lund, for her involvement in improving Legionella spp. diagnostic method.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Ampel, N. M., Ruben, F. L., Norden, C. W. (1985). Cutaneous abscess caused by legionella micdadei in an immunosuppressed patient. Ann. Intern. Med. 102 (5), 630–632. doi: 10.7326/0003-4819-102-5-630
Arnow, P. M., Boyko, E. J., Friedman, E. L. (1983). Perirectal abscess caused by legionella pneumophila and mixed anaerobic bacteria. Ann. Intern. Med. 98 (2), 184–185. doi: 10.7326/0003-4819-98-2-184
Banderet, F., Blaich, A., Soleman, E., Gaia, V., Osthoff, M. (2017). Septic arthritis due to legionella cincinnatiensis: case report and review of the literature. Infection 45 (4), 551–555. doi: 10.1007/s15010-016-0964-1
Bell, H., Chintalapati, S., Patel, P., Halim, A., Kithas, A., Schmalzle, S. A. (2021). Legionella longbeachae pneumonia: case report and review of reported cases in non-endemic countries. IDCases 23, e01050. doi: 10.1016/j.idcr.2021.e01050
Bemer, P., Leautez, S., Ninin, E., Jarraud, S., Raffi, F., Drugeon, H. (2002). Legionella pneumophila arthritis: use of medium specific for mycobacteria for isolation of l. pneumophila in culture of articular fluid specimens. Clin. Infect. Dis. 35 (1), E6–E7. doi: 10.1086/340713
Bethesda (2004). Blastn (National library of Madicine (US), National Center for Biotechnology Information). (2004-2021-11-21). Available at: https://blast.ncbi.nlm.nih.gov/Blast.cgi.
Bidell, M. R., Lodise, T. P. (2016). Fluoroquinolone-associated tendinopathy: does levofloxacin pose the greatest risk? Pharmacotherapy 36 (6), 679–693. doi: 10.1002/phar.1761
Brabender, W., Hinthorn, D. R., Asher, M., Lindsey, N. J., Liu, C. (1983). Legionella pneumophila wound infection. JAMA 250 (22), 3091–3092. doi: 10.1001/jama.1983.03340220059036
Casati, S., Gioria-Martinoni, A., Gaia, V. (2009). Commercial potting soils as an alternative infection source of legionella pneumophila and other legionella species in Switzerland. Clin. Microbiol. Infect. 15 (6), 571–575. doi: 10.1111/j.1469-0691.2009.02742.x
Cazalet, C., Gomez-Valero, L., Rusniok, C., Lomma, M., Dervins-Ravault, D., Newton, H. J., et al. (2010). Analysis of the legionella longbeachae genome and transcriptome uncovers unique strategies to cause legionnaires' disease. PloS Genet. 6 (2), e1000851. doi: 10.1371/journal.pgen.1000851
Chambers, S. T., Withers, A., Dawson, K., Anderson, T., Williman, J., Murdoch, D., et al. (2021). How safe are gloves and masks used for protection against legionella longbeachae infection when gardening? Lett. Appl. Microbiol. 73 (5), 616–622. doi: 10.1111/lam.13546
Charles, M., Johnson, E., Macyk-Davey, A., Henry, M., Nilsson, J. E., Miedzinski, L., et al. (2013). Legionella micdadei brain abscess. J. Clin. Microbiol. 51 (2), 701–704. doi: 10.1128/JCM.02160-12
Chee, C. E., Baddour, L. M. (2007). Legionella maceachernii soft tissue infection. Am. J. Med. Sci. 334 (5), 410–413. doi: 10.1097/MAJ.0b013e318068b5c2
Chou, L., Day, J., Ciciriello, S. (2016). An unexpected cause of tenosynovitis. J. Rheumatol. 43 (2), 461–462. doi: 10.3899/jrheum.150968
Cross, K. E., Mercante, J. W., Benitez, A. J., Brown, E. W., Diaz, M. H., Winchell, J. M., et al (2016). Simultaneous detection of Legionella species and L. anisa, L. bozemanii, L. longbeachae and L. micdadei using conserved primers and multiple probes in a multiplex real-time PCR assay. Diagn. Microbiol. Infect. Dis. 850 (3), 295–301.
Desgranges, F., Coste, A. T., Wernly, D., Dufour, J., Opota, O., Meylan, S. (2020). Immunosuppressed gardener pricked by roses grows legionella longbeachae. Lancet 395 (10224), 604. doi: 10.1016/S0140-6736(20)30112-4
Fields, B. S., Benson, R. F., Besser, R. E. (2002). Legionella and legionnaires' disease: 25 years of investigation. Clin. Microbiol. Rev. 15 (3), 506–526. doi: 10.1128/CMR.15.3.506-526.2002
Flendrie, M., Jeurissen, M., Franssen, M., Kwa, D., Klaassen, C., Vos, F. (2011). Septic arthritis caused by legionella dumoffii in a patient with systemic lupus erythematosus-like disease. J. Clin. Microbiol. 49 (2), 746–749. doi: 10.1128/JCM.00606-10
Gay, L., Melenotte, C., Lakbar, I., Mezouar, S., Devaux, C., Raoult, D., et al. (2021). Sexual dimorphism and gender in infectious diseases. Front. Immunol. 12. doi: 10.3389/fimmu.2021.698121
Girolamini, L., Pascale, M. R., Salaris, S., Mazzotta, M., Orsini, M., Grottola, A., et al. (2022). Legionella bononiensis sp. nov., isolated from a hotel water distribution system in northern Italy. Int. J. Syst. Evolutionary Microbiol. 72 (9) doi: 10.1099/ijsem.0.005512
Grimstead, D., Tucker, D., Harris, K., Turner, D. (2015). Cutaneous legionella longbeachae infection in immunosuppressed woman, united kingdom. Emerg. Infect. Dis. 21 (8), 1426–1428. doi: 10.3201/eid2108.140828
Gubler, J. G., Schorr, M., Gaia, V., Zbinden, R., Altwegg, M. (2001). Recurrent soft tissue abscesses caused by legionella cincinnatiensis. J. Clin. Microbiol. 39 (12), 4568–4570. doi: 10.1128/JCM.39.12.4568-4570.2001
Han, J. H., Nguyen, J. C., Harada, S., Baddour, L. M., Edelstein, P. H. (2010). Relapsing legionella pneumophila cellulitis: a case report and review of the literature. J. Infect. Chemother. 16 (6), 439–442. doi: 10.1007/s10156-010-0072-6
Jäger, J., Marwitz, S., Tiefenau, J., Rasch, J., Shevchuk, O., Kugler, C., et al. (2014). Human lung tissue explants reveal novel interactions during legionella pneumophila infections. Infect. Immunity 82 (1), 275–285. doi: 10.1128/IAI.00703-13
Just, S. A., Knudsen, J. B., Uldum, S. A., Holt, H. M. (2012). Detection of legionella bozemanae, a new cause of septic arthritis, by PCR followed by specific culture. J. Clin. Microbiol. 50 (12), 4180–4182. doi: 10.1128/JCM.01899-12
Kanarek, P., Bogiel, T., Breza-Boruta, B. (2022). Legionellosis risk-an overview of legionella spp. habitats in Europe. Environ. Sci. pollut. Res. Int. 29 (51), 76532–76542. doi: 10.1007/s11356-022-22950-9
Kilborn, J. A., Manz, L. A., O'Brien, M., Douglass, M. C., Horst, H. M., Kupin, W., et al. (1992). Necrotizing cellulitis caused by legionella micdadei. Am. J. Med. 92 (1), 104–106. doi: 10.1016/0002-9343(92)90024-6
Linscott, A. J., Poulter, M. D., Ward, K., Bruckner, D. A. (2004). Legionella pneumophila serogroup 4 isolated from joint tissue. J. Clin. Microbiol. 42 (3), 1365–1366. doi: 10.1128/JCM.42.3.1365-1366.2004
Löf, E., Chereau, F., Jureen, P., Andersson, S., Rizzardi, K., Edquist, P., et al. (2021). An outbreak investigation of legionella non-pneumophila legionnaires' disease in Sweden, April to august 2018: gardening and use of commercial bagged soil associated with infections. Euro Surveill 26 (7). doi: 10.2807/1560-7917.ES.2021.26.7.1900702
Loridant, S., Lagier, J. C., La Scola, B. (2011). Identification of legionella feeleii cellulitis. Emerg. Infect. Dis. 17 (1), 145–146. doi: 10.3201/eid1701.101346
Mentula, S., Pentikainen, J., Perola, O., Ruotsalainen, E. (2014). Legionella longbeachae infection in a persistent hand-wound after a gardening accident. JMM Case Rep. 1 (4), e004374. doi: 10.1099/jmmcr.0.004374
Mondino, S., Schmidt, S., Rolando, M., Escoll, P., Gomez-Valero, L., Buchrieser, C. (2020). Legionnaires' disease: state of the art knowledge of pathogenesis mechanisms of legionella. Annu. Rev. Pathol. 15, 439–466. doi: 10.1146/annurev-pathmechdis-012419-032742
Montanaro-Punzengruber, J. C., Hicks, L., Meyer, W., Gilbert, G. L. (1999). Australian Isolates of legionella longbeachae are not a clonal population. J. Clin. Microbiol. 37 (10), 3249–3254. doi: 10.1128/JCM.37.10.3249-3254.1999
Naito, T., Suda, T., Saga, K., Horii, T., Chida, K. (2007). Reactive legionella pneumophila arthritis diagnosed by polymerase chain reaction. Rheumatol. Int. 27 (4), 415–416. doi: 10.1007/s00296-006-0223-3
Neiderud, C. J., Vidh, A. L., Salaneck, E. (2013). Soft tissue infection caused by legionella bozemanii in a patient with ongoing immunosuppressive treatment. Infect. Ecol. Epidemiol. 3. doi: 10.3402/iee.v3i0.20739
Newton, H. J., Ang, D. K., van Driel, I. R., Hartland, E. L. (2010). Molecular pathogenesis of infections caused by legionella pneumophila. Clin. Microbiol. Rev. 23 (2), 274–298. doi: 10.1128/CMR.00052-09
Padrnos, L. J., Blair, J. E., Kusne, S., DiCaudo, D. J., Mikhael, J. R. (2014). Cutaneous legionellosis: case report and review of the medical literature. Transpl. Infect. Dis. 16 (2), 307–314. doi: 10.1111/tid.12201
Phin, N., Parry-Ford, F., Harrison, T., Stagg, H. R., Zhang, N., Kumar, K., et al. (2014). Epidemiology and clinical management of legionnaires' disease. Lancet Infect. Dis. 14 (10), 1011–1021. doi: 10.1016/S1473-3099(14)70713-3
Qin, X., Abe, P. M., Weissman, S. J., Manning, S. C. (2002). Extrapulmonary legionella micdadei infection in a previously healthy child. Pediatr. Infect. Dis. J. 21 (12), 1174–1176. doi: 10.1097/00006454-200212000-00022
Relman, D. A., Persing, D. H., Smith, T. F., Tenover, F. C., White, T. J. (1993). “Universal bacterial 16S rRNA amplification and sequencing,” in Diagnostic molecular microbiology: principles and applications (Washington DC: ASM Press), 489–495.
Steele, T. W., Moore, C. V., Sangster, N. (1990). Distribution of legionella longbeachae serogroup 1 and other legionellae in potting soils in Australia. Appl. Environ. Microbiol. 56 (10), 2984–2988. doi: 10.1128/aem.56.10.2984-2988.1990
Svendsen, J. H., Jønsson, V., Niebuhr, U. (1987). Combined pericarditis and pneumonia caused by legionella infection. Br. Heart J. 58 (6), 663–664. doi: 10.1136/hrt.58.6.663
Thurneysen, C., Boggian, K. (2014). Legionella pneumophila serogroup 1 septic arthritis with probable endocarditis in an immunodeficient patient. J. Clin. Rheumatol. 20 (5), 297–298. doi: 10.1097/RHU.0000000000000128
Valve, K., Vaalasti, A., Anttila, V. J., Vuento, R. (2010). Disseminated legionella pneumophila infection in an immunocompromised patient treated with tigecycline. Scand. J. Infect. Dis. 42 (2), 152–155. doi: 10.3109/00365540903359895
Waldor, M. K., Wilson, B., Swartz, M. (1993). Cellulitis caused by legionella pneumophila. Clin. Infect. Dis. 16 (1), 51–53. doi: 10.1093/clinids/16.1.51
Keywords: legionella, bacteria, Legionella longbeachae, cutaneous, infection, extrapulmonary manifestation
Citation: Frostadottir D, Wasserstrom L, Lundén K and Dahlin LB (2023) Legionella longbeachae wound infection: case report and review of reported Legionella wound infections. Front. Cell. Infect. Microbiol. 13:1178130. doi: 10.3389/fcimb.2023.1178130
Received: 02 March 2023; Accepted: 04 April 2023;
Published: 26 April 2023.
Edited by:
Joseph B. McPhee, Ryerson University, CanadaReviewed by:
Dimosthenis Chochlakis, University of Crete, GreeceYuxin Mao, Cornell University, United States
Copyright © 2023 Frostadottir, Wasserstrom, Lundén and Dahlin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Drifa Frostadottir, ZHJpZmEuZnJvc3RhZG90dGlyQG1lZC5sdS5zZQ==
†These authors have contributed equally to this work and share first authorship