
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Cell. Infect. Microbiol., 27 April 2023
Sec. Fungal Pathogenesis
Volume 13 - 2023 | https://doi.org/10.3389/fcimb.2023.1165236
This article is part of the Research TopicUpdate on diagnostics, treatment, and prognosis on invasive fungal infectionsView all 7 articles
 Alexander Rombauts1*†
Alexander Rombauts1*† Marta Bodro2†Victor Daniel Gumucio3Irene Carbonell2
Marta Bodro2†Victor Daniel Gumucio3Irene Carbonell2 Àlex Favà4†Laura Lladó5†José González-Costello6†
Àlex Favà4†Laura Lladó5†José González-Costello6† Federico Oppenheimer7†
Federico Oppenheimer7† María Ángeles Castel-Lavilla8Oscar Len9,10,11†Ester Marquez-Algaba9,10†
María Ángeles Castel-Lavilla8Oscar Len9,10,11†Ester Marquez-Algaba9,10† Xavier Nuvials-Casals12†Daniel Martínez González12Judith Sacanell Lacasa12
Xavier Nuvials-Casals12†Daniel Martínez González12Judith Sacanell Lacasa12 Jordi Carratalà1,11,13†Nuría Sabé1,11†
Jordi Carratalà1,11,13†Nuría Sabé1,11†COVID-19-associated pulmonary aspergillosis (CAPA) has emerged as a frequent complication in the intensive care unit (ICU). However, little is known about this life-threatening fungal superinfection in solid organ transplant recipients (SOTRs), including whether targeted anti-mold prophylaxis might be justified in this immunosuppressed population. We performed a multicentric observational retrospective study of all consecutive ICU-admitted COVID-19 SOTRs between August 1, 2020 and December 31, 2021. SOTRs receiving antifungal prophylaxis with nebulized amphotericin-B were compared with those without prophylaxis. CAPA was defined according the ECMM/ISHAM criteria. Sixty-four SOTRs were admitted to ICU for COVID-19 during the study period. One patient received antifungal prophylaxis with isavuconazole and was excluded from the analysis. Of the remaining 63 SOTRs, nineteen (30.2%) received anti-mold prophylaxis with nebulized amphotericin-B. Ten SOTRs who did not receive prophylaxis developed pulmonary mold infections (nine CAPA and one mucormycosis) compared with one who received nebulized amphotericin-B (22.7% vs 5.3%; risk ratio 0.23; 95%CI 0.032-1.68), but with no differences in survival. No severe adverse events related to nebulized amphotericin-B were recorded. SOTRs admitted to ICU with COVID-19 are at high risk for CAPA. However, nebulized amphotericin-B is safe and might reduce the incidence of CAPA in this high-risk population. A randomized clinical trial to confirm these findings is warranted.
Several studies have shown an association between invasive pulmonary aspergillosis and viral infections, such as cytomegalovirus disease (Singh and Husain, 2009; Kuo et al., 2022) and influenza (Schauwvlieghe et al., 2018; Verweij et al., 2020). Worryingly, recent large cohort studies of COVID-19-associated pulmonary aspergillosis (CAPA) in patients admitted to the intensive care unit (ICU) have raised concerns about this superinfection. Indeed, this life-threatening secondary infection appears to develop in approximately 18-19% of patients with critical COVID-19 and significantly increases mortality (Bartoletti et al., 2021; Dupont et al., 2021; Xu et al., 2021; Gangneux et al., 2022; Prattes et al., 2022).
Solid organ transplant recipients (SOTRs) are at increased risk of severe COVID-19 (Trapani et al., 2021; Maggiore et al., 2022), and ICU admission than the general population (Gatti et al., 2022). Because of baseline immunosuppression, CAPA is likely to be more frequent in SOTRs than in the general population admitted to ICU for severe COVID-19. Unfortunately, data about CAPA in SOTRs is extremely scarce. Indeed, when combining data from three of the largest studies published to date, only 44 of the 1209 included patients were SOTRs (Bartoletti et al., 2021; Gangneux et al., 2022; Prattes et al., 2022). Of concern, however, a staggering 31,8% (14 out of 44) had CAPA (Bartoletti et al., 2021; Gangneux et al., 2022; Prattes et al., 2022).
Antifungal prophylaxis might be justified for high-risk groups due to the incidence and mortality of CAPA in ICUs. Unfortunately, antifungal prophylaxis in SOTRs is not without challenges. Drug-drug interactions exist between triazoles and the most common immunosuppressants (calcineurin inhibitors and mammalian target of rapamycin [mTOR] inhibitors) (Lempers et al., 2015). Echinocandins have poor activity against molds with higher rates of breakthrough infections (Gomes et al., 2014; Lionakis et al., 2018), while the use of intravenous amphotericin-B is limited by the risk of renal injury and the potential for drug-drug interactions (Trejtnar et al., 2014). In this scenario, nebulized amphotericin-B, ensuring high alveolar concentrations (Fauvel et al., 2012) with limited systemic exposure, seems an attractive choice. Clinical studies among lung (Peghin et al., 2016; Huggins et al., 2022) and cardiac transplant recipients (Paniagua Martin et al., 2010), plus neutropenic hematological patients (Rijnders et al., 2008), show that this approach has high efficacy and causes few adverse events.
In this retrospective study, we aimed to evaluate the impact of antifungal prophylaxis with nebulized amphotericin-B in SOTRs admitted to ICU for COVID-19.
We conducted a multicenter, real-world, retrospective cohort study among adult (age ≥ 18 years) SOTRs admitted with COVID-19 to ICUs in Barcelona between August 1, 2020 and December 31, 2021. Three university hospitals with transplant programs took part (Hospital Universitari de Bellvitge, Hospital Clínic de Barcelona and Hospital Universitari Vall d’Hebron) and collected the following data from the electronic health record during hospitalization: demographic, comorbidities, symptoms, oxygen requirements, radiological features, treatments, microbiological and analytic parameters, and clinical courses. COVID-19 associated aspergillosis was defined according to the European Confederation of Medical Mycology (ECMM)/International Society for Human and Animal Mycoses (ISHAM) criteria (Koehler et al., 2021). None of the studies sites reported environmental issues which might influence the development of aspergillosis.
All three centers employed the same antifungal prophylaxis regimen, giving a 24 mg dose of nebulized liposomal amphotericin-B three times a week. Mechanically ventilated patients received 6 mg of nebulized amphotericin-B desoxycholate every 8 hours. See Supplementary Material for more detail. We excluded participants if they received a different antifungal prophylaxis and patients of the first wave of the COVID-19 pandemic to limit heterogeneity. After witnessing several CAPA cases in COVID-19 ICU admitted SOTRs in the first year of the pandemic, the infectious diseases consultants encouraged the use of prophylaxis with nebulized amphotericin-B, although the final decision on initiating prophylaxis remained with the treating intensivist.
Descriptive statistical analysis was performed for all study variables. Data are reported as means and standard deviations or as the percentage of patients with data available for a given variable. We then compared patients who did and did not receive nebulized amphotericin-B. To identify risk factors, we also compared patients with and without CAPA. Chi-squared tests were used to assess categorical variables and student t-tests or Mann–Whitney U tests were used to assess quantitative variables.
The study protocol was approved by the Clinical Research Ethics Committee of the Bellvitge University Hospital (EOM039/21) and the procedures were conducted in accordance with the ethical standards of the Helsinki Declaration. The need for informed consent was waived because of the retrospective observational nature of the study and the use of de-identified anonymous clinical data.
During the study period, 64 SOTRs were admitted to ICUs with COVID-19 pneumonia. Of the 20 patients, (31.3%) who received antifungal prophylaxis, 19 received nebulized amphotericin-B, while one patient receiving isavuconazole prophylaxis was excluded from the analysis.
The analyzed sample included 63 SOTRs (mean age, 62.1 ± 11.7 years), 49 renal, 6 lung, 4 heart, 3 liver, and 1 pancreas/kidney recipients, of which 16 (25.4%) had undergone transplantation in the 6 months before ICU admission. Maintenance immunosuppression typically included tacrolimus (90.5%) with mycophenolate (85.7%), whereas the acute treatment of COVID-19 included corticosteroids (96.8%), tocilizumab (25.4%), and remdesivir (9.5%), with 77.7% requiring invasive mechanical ventilation. The in-hospital mortality rate was 57.1%.
The mean time to CAPA diagnosis after ICU admission was 6.8 ± 5.8 days, with intensivists diagnosing 1 possible and 9 probable cases of aspergillosis, together with 1 case of pulmonary mucormycosis (17.4%). The ECMM/ISHAM criteria used to establish pulmonary aspergillosis can be found in the Supplementary Material (Table S1). The characteristics of patients with and without aspergillosis can be found in the Supplementary Material (Table S2). Univariate analysis revealed that SARS-CoV-2 vaccination (41.5% vs 80%; p=0.025) was associated with CAPA and a trend for higher CAPA risk among SOTRs treated with tocilizumab (50%) compared to those not treated with tocilizumab (50% vs 20.8%; p=0.051). Patients with and without CAPA did not differ by ICU length of stay, duration of invasive mechanical ventilation, or in-hospital mortality.
The characteristics of patients with and without prophylaxis are shown in Table 1. The mean duration of prophylaxis was of 21.1 days (SD 15.2). Of note, 10 patients (22.7%) in the non-prophylaxis group developed a pulmonary fungal infection (9 CAPA, 1 mucormycosis) compared to 1 patient (5.3%) in the prophylaxis group (risk ratio 0.23; 95%CI 0.032–1.68).
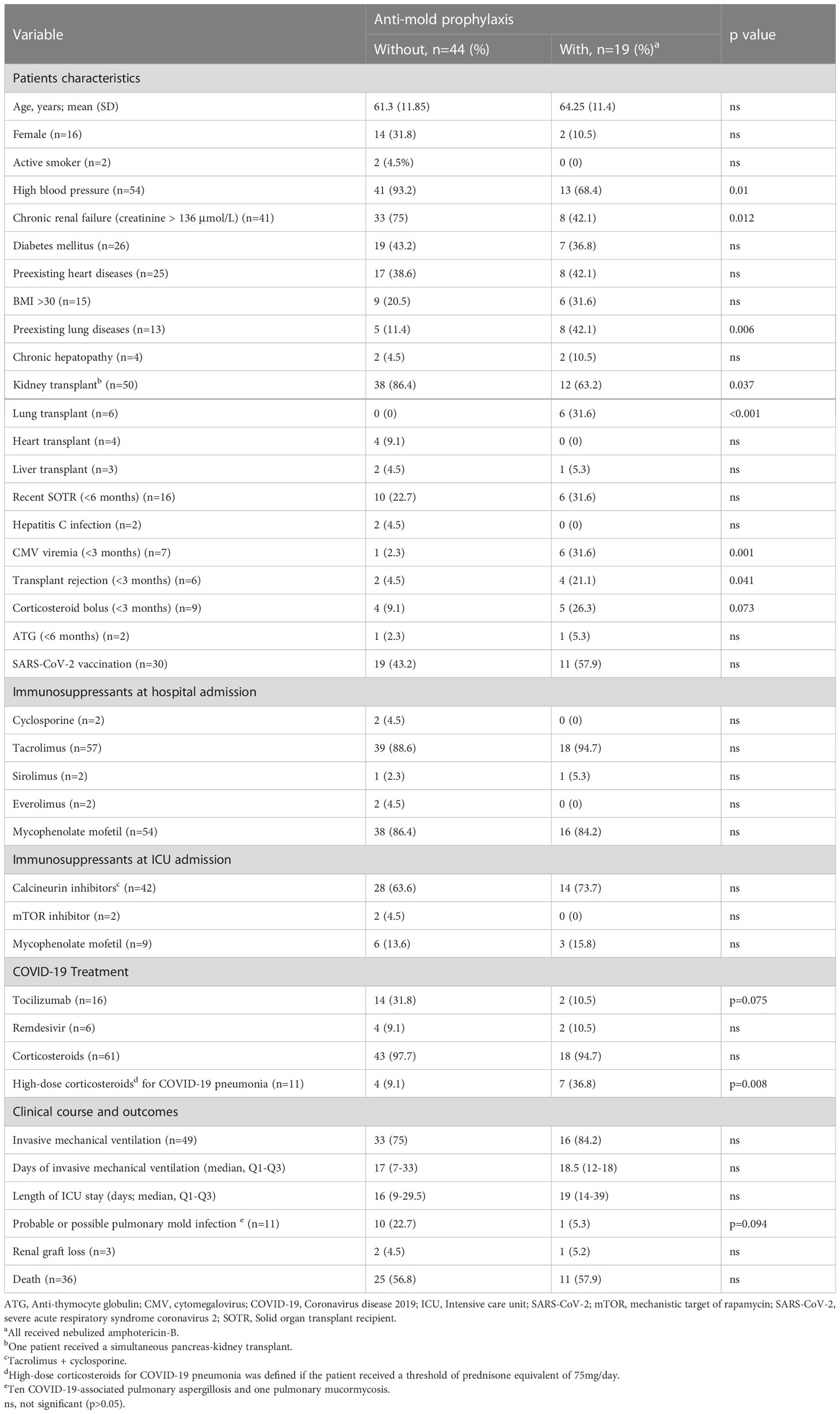
Table 1 Comparison between SOTRs with and without anti-mold prophylaxis at ICU admission for COVID-19.
Concerning adverse effects, only 1 of the 19 patients receiving nebulized amphotericin-B prophylaxis developed mild-to-moderate bronchospasm, and this did not require the interruption of prophylaxis. Finally, in-hospital mortality was comparable between groups.
In this multicenter observational study, antifungal prophylaxis with nebulized amphotericin-B among SOTRs admitted to ICU with COVID-19 showed a trend to lower the incidence of CAPA: 1 of 19 patients (5.3%) using this prophylaxis compared with 9 of 44 (20.5%) without prophylaxis. These results suggest that nebulized amphotericin-B might be effective in preventing CAPA in SOTRs. Our results are in line with two previous observational studies that showed a reduction in CAPA diagnosis in ICU-admitted COVID-19 patients with posaconazole (Hatzl et al., 2021) and nebulized amphotericin-B (Van Ackerbroeck et al., 2021) prophylaxis. However, while CAPA is associated with a higher mortality in other observational studies (Bartoletti et al., 2021; Dupont et al., 2021; Hatzl et al., 2021; Xu et al., 2021; Gangneux et al., 2022; Prattes et al., 2022), we found no differences in mortality nor length of ICU stay. Similar to a study of how antifungal prophylaxis affected CAPA, we also observed no survival benefit with inhaled amphotericin-B (Hatzl et al., 2021). The small sample size and number of CAPA events precludes the detection of meaningful clinical outcomes.
Our study has several limitations. Adverse events were not recorded prospectively in a standardized format and intolerance may therefore be underreported. Nonetheless, no discontinuation of prophylaxis due to side effects was recorded. Antifungal prophylaxis assignment was not randomized, meaning that baseline characteristics were not completely balanced between the two study groups. However, most known risk factors for aspergillosis were more common in the prophylaxis group (e.g., prior cytomegalovirus viremia, high-dose corticosteroids for COVID-19 and preexisting lung disease). In addition, none of the CAPA cases could be classified as proven, underlying the difficulties in diagnosing CAPA in ICU admitted patients. Despite the multicenter study design, the study population is small and included few CAPA events, and this limits both the reproducibility and the generalizability of the results of the study itself. However, the observed CAPA prevalence in this study might have been underestimated in the absence of standardized screening. Given that the range of CAPA prevalence is wide in other studies, it may not be possible to extrapolate our results to other geographic regions.
Despite the limitations of our research, targeted antifungal prophylaxis with nebulized amphotericin-B may still be justified for SOTRs admitted to ICU with COVID-19. First, patients admitted to ICU with COVID-19 have an estimated prevalence of 18%–19% for CAPA (Bartoletti et al., 2021; Dupont et al., 2021; Xu et al., 2021; Gangneux et al., 2022; Prattes et al., 2022), which could be higher in SOTRs given their baseline immunosuppression. Second, not only do the radiological features of pulmonary aspergillosis overlap with those of COVID-19 (Koehler et al., 2021) but also most diagnostic methods have lower sensitivities in non-hematological patients (Ullmann et al., 2018). Third, Aspergillus spp. treatment increases the risk of drug-drug interactions and toxicity among SOTRs (Luong et al., 2012; Lempers et al., 2015).
In conclusion, SOTRs admitted to ICU with respiratory failure due to SARS-CoV-2 infection have an elevated risk of CAPA. Nebulized amphotericin B represents an attractive choice for the prevention of CAPA in this high-risk population, benefiting from being effective and safe, while lacking drug-drug interactions (Rijnders et al., 2008; Paniagua Martin et al., 2010; Peghin et al., 2016; Van Ackerbroeck et al., 2021; Huggins et al., 2022). A randomized clinical trial to confirm these findings is warranted.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Clinical Research Ethics Committee of the Bellvitge University Hospital. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
AR, MB, NS, JC conceived of the presented idea, AR, MB, VD-G, IC, AF, LL, JG-C, FO, MC-L, OL, EM-A, XN-C, DMG, JL participated in the data collection, AR, NS performed the data analysis and interpretation, AR, JC and NS drafted the article, MB, OL, JC and NS provided critical revision. All authors contributed to the article and approved the submitted version.
AR received a predoctoral research grant from the Instituto de Salud Carlos III, Spanish Ministry of Science, Innovation and Universities, (PFIS grant FI18/00183). This work was supported by the Instituto de Salud Carlos III, Subdirección General de Redes y Centros de Investigación Cooperativa, Ministerio de Economía, Industria y Competitividad, Centro de Investigación Biomédica en Red de Enfermedades Infecciosas (CIBERINFEC), Madrid, Spain. We thank CERCA Programme/Generalitat de Catalunya for institutional support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcimb.2023.1165236/full#supplementary-material
CAPA, COVID-19-associated pulmonary aspergillosis; COVID-19, coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SOTRs, solid organ transplant recipients; ICU, intensive care unit.
Bartoletti, M., Pascale, R., Cricca, M., Rinaldi, M., Maccaro, A., Bussini, L., et al. (2021). Epidemiology of invasive pulmonary aspergillosis among intubated patients with COVID-19: a prospective study. Clin. Infect. Dis. 73 (11), E3606–E3614. doi: 10.1093/CID/CIAA1065
Dupont, D., Menotti, J., Turc, J., Miossec, C., Wallet, F., Richard, J. C., et al. (2021). Pulmonary aspergillosis in critically ill patients with coronavirus disease 2019 (COVID-19). Med. Mycol. 59 (1), 110–114. doi: 10.1093/MMY/MYAA078
Fauvel, M., Farrugia, C., Tsapis, N., Gueutin, C., Cabaret, O., Bories, C., et al. (2012). Aerosolized liposomal amphotericin b: prediction of lung deposition. Vitro uptake cytotoxicity Int. J. Pharm. 436 (1-2), 106–110. doi: 10.1016/J.IJPHARM.2012.07.012
Gangneux, J. P., Dannaoui, E., Fekkar, A., Luyt, C. E., Botterel, F., De Prost, N., et al. (2022). Fungal infections in mechanically ventilated patients with COVID-19 during the first wave: the French multicentre MYCOVID study. Lancet Respir. Med. 10 (2), 180–190. doi: 10.1016/S2213-2600(21)00442-2
Gatti, M., Rinaldi, M., Bussini, L., Bonazzetti, C., Pascale, R., Pasquini, Z., et al. (2022). Clinical outcome in solid organ transplant recipients affected by COVID-19 compared to general population: a systematic review and meta-analysis. Clin. Microbiol. Infect. 28 (8), 1057–1065. doi: 10.1016/J.CMI.2022.02.039
Gomes, M. Z. R., Jiang, Y., Mulanovich, V. E., Lewis, R. E., Kontoyiannis, D. P. (2014). Effectiveness of primary anti-aspergillus prophylaxis during remission induction chemotherapy of acute myeloid leukemia. Antimicrob. Agents Chemother. 58 (5), 2775–2780. doi: 10.1128/AAC.01527-13
Hatzl, S., Reisinger, A. C., Posch, F., Prattes, J., Stradner, M., Pilz, S., et al. (2021). Antifungal prophylaxis for prevention of COVID-19-associated pulmonary aspergillosis in critically ill patients: an observational study. Crit. Care 25 (1), 335. doi: 10.1186/S13054-021-03753-9
Huggins, J. P., Pease, R., Stanly, K., Workman, A., Reynolds, J., Alexander, B. D. (2022). Safety of inhaled amphotericin b lipid complex as antifungal prophylaxis in lung transplant recipients. Antimicrob. Agents Chemother. 66 (6), e0028322. doi: 10.1128/AAC.00283-22
Koehler, P., Bassetti, M., Chakrabarti, A., Chen, S. C. A., Colombo, A. L., Hoenigl, M., et al. (2021). Defining and managing COVID-19-associated pulmonary aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. Lancet Infect. Dis. 21 (6), e149–e162. doi: 10.1016/S1473-3099(20)30847-1
Kuo, C. W., Wang, S. Y., Tsai, H. P., Su, P. L., Cia, C. T., Lai, C. H., et al. (2022). Invasive pulmonary aspergillosis is associated with cytomegalovirus viremia in critically ill patients - a retrospective cohort study. J. Microbiol. Immunol. Infect. 55 (2), 291–299. doi: 10.1016/J.JMII.2021.03.005
Lempers, V. J., Martial, L. C., Schreuder, M. F., Blijlevens, N. M., Burger, D. M., Aarnoutse, R. E., et al. (2015). Drug-interactions of azole antifungals with selected immunosuppressants in transplant patients: strategies for optimal management in clinical practice. Curr. Opin. Pharmacol. 24, 38–44. doi: 10.1016/J.COPH.2015.07.002
Lionakis, M. S., Lewis, R. E., Kontoyiannis, D. P. (2018). Breakthrough invasive mold infections in the hematology patient: current concepts and future directions. Clin. Infect. Dis. 67 (10), 1621–1630. doi: 10.1093/CID/CIY473
Luong, M. L., Hosseini-Moghaddam, S. M., Singer, L. G., Chaparro, C., Azad, S., Lazar, N., et al. (2012). Risk factors for voriconazole hepatotoxicity at 12 weeks in lung transplant recipients. Am. J. Transplant 12 (7), 1929–1935. doi: 10.1111/J.1600-6143.2012.04042.X
Maggiore, U., Riella, L. V., Azzi, J., Cravedi, P. (2022). Mortality in solid organ transplant recipients with COVID-19: more than meets the eye. Am. J. Transplant 22 (5), 1496–1497. doi: 10.1111/AJT.16942
Paniagua Martin, M. J., Marzoa Rivas, R., Barge Caballero, E., Grille Cancela, Z., Fernandez, C. J., Solla, M., et al. (2010). Efficacy and tolerance of different types of prophylaxis for prevention of early aspergillosis after heart transplantation. Transplant. Proc. 42 (8), 3014–3016. doi: 10.1016/J.TRANSPROCEED.2010.08.013
Peghin, M., Monforte, V., Martin-Gomez, M. T., Ruiz-Camps, I., Berastegui, C., Saez, B., et al. (2016). 10 years of prophylaxis with nebulized liposomal amphotericin b and the changing epidemiology of aspergillus spp. infection Lung transplantation Transpl Int. 29 (1), 51–62. doi: 10.1111/TRI.12679
Prattes, J., Wauters, J., Giacobbe, D. R., Salmanton-García, J., Maertens, J., Bourgeois, M., et al. (2022). Risk factors and outcome of pulmonary aspergillosis in critically ill coronavirus disease 2019 patients-a multinational observational study by the European confederation of medical mycology. Clin. Microbiol. Infect. 28 (4), 580–587. doi: 10.1016/J.CMI.2021.08.014
Rijnders, B. J., Cornelissen, J. J., Slobbe, L., Becker, M. J., Doorduijn, J. K., Hop, W. C., et al. (2008). Aerosolized liposomal amphotericin b for the prevention of invasive pulmonary aspergillosis during prolonged neutropenia: a randomized, placebo-controlled trial. Clin. Infect. Dis. 46 (9), 1401–1408. doi: 10.1086/586739
Schauwvlieghe, A. F. A. D., Rijnders, B. J. A., Philips, N., Verwijs, R., Vanderbeke, L., Van Tienen, C., et al. (2018). Invasive aspergillosis in patients admitted to the intensive care unit with severe influenza: a retrospective cohort study. Lancet Respir. Med. 6 (10), 782–792. doi: 10.1016/S2213-2600(18)30274-1
Singh, N., Husain, S. (2009). AST infectious diseases community of practice. Invasive aspergillosis solid Organ Transplant. recipients Am. J. Transplant 9 Suppl 4, S180–S191. doi: 10.1111/j.1600-6143.2009.02910.x
Trapani, S., Masiero, L., Puoti, F., Rota, M. C., Del Manso, M., Lombardini, L., et al. (2021). Incidence and outcome of SARS-CoV-2 infection on solid organ transplantation recipients: a nationwide population-based study. Am. J. Transplant 21 (7), 2509–2521. doi: 10.1111/AJT.16428
Trejtnar, F., Mandíková, J., Kočíncová, J., Volková, M. (2014). Renal handling of amphotericin b and amphotericin b-deoxycholate and potential renal drug-drug interactions with selected antivirals. Antimicrob. Agents Chemother. 58 (10), 5650–5657. doi: 10.1128/AAC.02829-14
Ullmann, A. J., Aguado, J. M., Arikan-Akdagli, S., Denning, D. W., Groll, A. H., Lagrou, K., et al. (2018). Diagnosis and management of aspergillus diseases: executive summary of the 2017 ESCMID-ECMM-ERS guideline. Clin. Microbiol. Infect. 24 Suppl 1, e1–e38. doi: 10.1016/j.cmi.2018.01.002
Van Ackerbroeck, S., Rutsaert, L., Roelant, E., Dillen, K., Wauters, J., Van Regenmortel, N. (2021). Inhaled liposomal amphotericin-b as a prophylactic treatment for COVID-19-associated pulmonary aspergillosis/aspergillus tracheobronchitis. Crit. Care 25 (1), 298. doi: 10.1186/S13054-021-03728-W
Verweij, P. E., Rijnders, B. J. A., Brüggemann, R. J. M., Azoulay, E., Bassetti, M., Blot, S., et al. (2020). Review of influenza-associated pulmonary aspergillosis in ICU patients and proposal for a case definition: an expert opinion. Intensive Care Med. 46 (8), 1524–1535. doi: 10.1007/S00134-020-06091-6
Keywords: COVID-19, SARS-CoV-2, solid-organ transplant recipients, amphotericin-B, prophylaxis, Aspergillus spp., CAPA, Aspergillosis
Citation: Rombauts A, Bodro M, Daniel Gumucio V, Carbonell I, Favà À, Lladó L, González-Costello J, Oppenheimer F, Castel-Lavilla MÁ, Len O, Marquez-Algaba E, Nuvials-Casals X, Martínez González D, Lacasa JS, Carratalà J and Sabé N (2023) Antifungal prophylaxis with nebulized amphotericin-B in solid-organ transplant recipients with severe COVID-19: a retrospective observational study. Front. Cell. Infect. Microbiol. 13:1165236. doi: 10.3389/fcimb.2023.1165236
Received: 13 February 2023; Accepted: 07 April 2023;
Published: 27 April 2023.
Edited by:
Jon Salmanton-Garcia, University Hospital of Cologne, GermanyReviewed by:
Maddalena Peghin, University of Insubria, ItalyCopyright © 2023 Rombauts, Bodro, Daniel Gumucio, Carbonell, Favà, Lladó, González-Costello, Oppenheimer, Castel-Lavilla, Len, Marquez-Algaba, Nuvials-Casals, Martínez González, Lacasa, Carratalà and Sabé. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexander Rombauts, YWxleGFuZGVyLnJvbWJhdXRzQGdtYWlsLmNvbQ==
†ORCID: Alexander Rombauts, orcid.org/0000-0003-0227-5916
Marta Bodro, orcid.org/0000-0002-0520-8279
Àlex Favà, orcid.org/0000-0003-1664-6001
Laura Lladó, orcid.org/0000-0002-3717-3306
José González-Costello, orcid.org/0000-0002-7437-3630
Federico Oppenheimer, orcid.org/0000-0002-1117-831X
Oscar Len, orcid.org/0000-0002-1819-3141
Ester Marquez-Algaba, orcid.org/0000-0002-9824-0138
Xavier Nuvials-Casals, orcid.org/0000-0002-6648-2394
Jordi Carratalà, orcid.org/0000-0003-3209-2563
Nuría Sabé, orcid.org/0000-0003-1697-4347
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.