 Tsung-Ta Chiang1
Tsung-Ta Chiang1 Tzu-Wen Huang2,3Jun-Ren Sun1,4
Tzu-Wen Huang2,3Jun-Ren Sun1,4 Shu-Chen Kuo5
Shu-Chen Kuo5 Aristine Cheng6,7Chang-Pan Liu8,9Yuag-Meng Liu10
Aristine Cheng6,7Chang-Pan Liu8,9Yuag-Meng Liu10 Ya-Sung Yang1
Ya-Sung Yang1 Te-Li Chen11
Te-Li Chen11 Yi-Tzu Lee12,13*†
Yi-Tzu Lee12,13*† Yung-Chih Wang1*†
Yung-Chih Wang1*†- 1Division of Infectious Diseases and Tropical Medicine, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan
- 2Department of Microbiology and Immunology, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan
- 3Graduate Institute of Medical Sciences, College of Medicine, Taipei Medical University, Taipei, Taiwan
- 4Institute of Preventive Medicine, National Defense Medical Center, Taipei, Taiwan
- 5National Institute of Infectious Diseases and Vaccinology, National Health Research Institute, Maoli County, Taiwan
- 6Department of Internal Medicine, National Taiwan University Hospital, Taipei, Taiwan
- 7College of Medicine, National Taiwan University, Taipei, Taiwan
- 8Division of Infectious Diseases, Department of Internal Medicine, Mackay Memorial Hospital, Taipei, Taiwan
- 9Department of Medical Research, Mackay Memorial Hospital, Taipei, Taiwan
- 10Division of Infectious Diseases, Department of Internal Medicine, Changhua Christian Hospital, Changhua, Taiwan
- 11Graduate Institute of Life Sciences, National Defense Medical Center, Taipei, Taiwan
- 12Department of Emergency Medicine, Taipei Veterans General Hospital, Taipei, Taiwan
- 13Faculty of Medicine, School of Medicine, National Yang-Ming University, Taipei, Taiwan
In the past decades, due to the high prevalence of the antibiotic-resistant isolates of Acinetobacter baumannii, it has emerged as one of the most troublesome pathogens threatening the global healthcare system. Furthermore, this pathogen has the ability to form biofilms, which is another effective mechanism by which it survives in the presence of antibiotics. However, the clinical impact of biofilm-forming A. baumannii isolates on patients with bacteremia is largely unknown. This retrospective study was conducted at five medical centers in Taiwan over a 9-year period. A total of 252 and 459 patients with bacteremia caused by biofilm- and non-biofilm-forming isolates of A. baumannii, respectively, were enrolled. The clinical demographics, antimicrobial susceptibility, biofilm-forming ability, and patient clinical outcomes were analyzed. The biofilm-forming ability of the isolates was assessed using a microtiter plate assay. Multivariate analysis revealed the higher APACHE II score, shock status, lack of appropriate antimicrobial therapy, and carbapenem resistance of the infected strain were independent risk factors of 28-day mortality in the patients with A. baumannii bacteremia. However, there was no significant difference between the 28-day survival and non-survival groups, in terms of the biofilm forming ability. Compared to the patients infected with non-biofilm-forming isolates, those infected with biofilm-forming isolates had a lower in-hospital mortality rate. Patients with either congestive heart failure, underlying hematological malignancy, or chemotherapy recipients were more likely to become infected with the biofilm-forming isolates. Multivariate analysis showed congestive heart failure was an independent risk factor of infection with biofilm-forming isolates, while those with arterial lines tended to be infected with non-biofilm-forming isolates. There were no significant differences in the sources of infection between the biofilm-forming and non-biofilm-forming isolate groups. Carbapenem susceptibility was also similar between these groups. In conclusion, the patients infected with the biofilm-forming isolates of the A. baumannii exhibited different clinical features than those infected with non-biofilm-forming isolates. The biofilm-forming ability of A. baumannii may also influence the antibiotic susceptibility of its isolates. However, it was not an independent risk factor for a 28-day mortality in the patients with bacteremia.
Introduction
Acinetobacter baumannii is an important pathogen responsible for various nosocomial infections and leads to high rates of mortality and morbidity in the infected patients (Cisneros et al., 1996; Dijkshoorn et al., 2007). Its emergence as a drug-resistant pathogen has made the treatment of infected patients difficult (Dijkshoorn et al., 2007; Peleg et al., 2008). Moreover, A. baumannii has been found to have the ability to form biofilms, which is another effective way for the bacteria to survive in the presence of antibiotics (Villegas and Hartstein, 2003; Martí et al., 2011). Biofilm, a three-dimensional structure constructed by the bacterial community, is encased in an extracellular polymeric matrix (Hall-Stoodley et al., 2004). Biofilms may act as a barrier against the penetration of antimicrobials, to alter their metabolism and effects, resulting in antimicrobial resistance (Harrison et al., 2007). However, some studies have shown that biofilm-forming isolates exhibit variations in drug resistance (Rodríguez-Baño et al., 2008; Qi et al., 2016; Donadu et al., 2021). These findings suggest that the biofilm-forming ability of bacterial isolates may contribute to differences in drug resistance. Moreover, biofilm- and non-biofilm-forming isolates could show different virulence.
A. baumannii can cause various biofilm-associated infections, such as chronic wound infections, ventilator-associated pneumonia, infective endocarditis, and catheter-related infections (Høiby et al., 2015; Gedefie et al., 2021). Although biofilm-associated infections are considered the cause of morbidity and mortality in patients, several studies have reported that infections caused by them are not associated with worse outcomes (Rodríguez-Baño et al., 2008; Barsoumian et al., 2015; Wang et al., 2018). Therefore, the clinical impact of the biofilm-forming ability of the pathogen remains elusive. In previous studies, we found that biofilm formation was not associated with worse outcomes in A. baumannii bacteremic pneumonia (Wang et al., 2018). However, different types of biofilm-associated infections may result in different clinical outcomes. Limited data are available regarding the clinical impacts of biofilm-forming ability of the isolates of A. baumannii. This study aimed to establish a correlation between the biofilm-forming ability of A. baumannii and the clinical outcomes in patients with A. baumannii bacteremia.
Materials and methods
Hospital setting and study population
This retrospective study was conducted from January 2010 to December 2019 at five medical centers in Taiwan, namely (alphabetically) Changhua Christian Hospital (CCH, 1676 beds) in Central Taiwan, Mackay Memorial Hospital (MMH, 2055 beds), National Taiwan University Hospital (NTUH, 2245 beds), Taipei Veterans General Hospital (TVGH, 2900 beds), and Tri-Service General Hospital (TSGH, 1712 beds) of National Defense Medical Center in Northern Taiwan. Patients who had at least one positive blood culture for A. baumannii and who simultaneously had symptoms and signs of infection were enrolled. In patients with two or more positive blood cultures, only the first blood culture was included. Patients under 20 years of age and with incomplete medical records were excluded. The study protocol was approved by the institutional review board (IRB) of each hospital (approval numbers: CCH: IRB No. 140514, MKH: IRB No. 14MMHIS125, NTU: IRB No. 201008047R, TSGH: IRB No. 1-103-05-100, and TVGH: IRB No. 2015-04-003C).
An episode of A. baumannii bacteremia was defined as the isolation of A. baumannii from a blood culture on one or more occasions. The onset of bacteremia was defined as the day when the blood culture that eventually yielded A. baumannii was obtained. Bacteremia episodes in the intensive care unit (ICU) were defined as having occurred within 48 h of ICU admission. A previous stay in the ICU was defined as admission to the ICU within 30 days prior to the bacteremia onset. Previous use of antimicrobials was defined as the use of antimicrobials, 30 days preceding the date of bacteremia onset. Those who received immunosuppressant agents within 2 weeks or corticosteroids at a dosage equivalent to or higher than 15 mg of prednisolone daily for 1 week within 4 weeks prior to the bacteremia onset were considered to have received immunosuppressant therapy. Chemotherapy use was defined as the administration of cytotoxic agents within 6 weeks prior to the onset of bacteremia. Recent surgery was defined as a surgery performed within 4 weeks prior to the onset of bacteremia. The source of bacteremia was determined according to the US Centers for Disease Control and Prevention definitions (Garner et al., 1988). The Acute Physiology and Chronic Health Evaluation (APACHE) II score within 24 h prior to the bacteremia onset was used to assess the severity of the disease. The all-cause 28-day mortality was defined as death occurring within 28 days of the onset of bacteremia and was set as the endpoint. The survival status of those who were discharged before the 28-day period was determined by contacting the patient or reviewing their medical records. None of the patients in this group were lost to follow-up.
Bacterial identification and antimicrobial susceptibility testing
Presumptive identification of the isolates at the A. baumannii complex (Abc) level was performed using the Vitek 2 system (bioMérieux, Marcy l’Etoile, France). The multiplex polymerase chain reaction was carried out to identify A. baumannii at the level of genomic species (Chen et al., 2007). The minimum inhibitory concentrations (MICs) of antimicrobial agents were determined by broth microdilution (Wayne and CLSI., 2006) and interpreted according to the standards given by the Clinical and Laboratory Standards Institute (CLSI) standards (Wayne and CLSI., 2020).
Biofilm cultivation and measurement
Biofilm-forming capability was quantitatively estimated using the crystal violet staining method (O’Toole et al., 1999; Wang et al., 2016). However, minor modifications in the procedure were made. Briefly, the bacterial strains were cultured at 37°C for 24 h in 5 mL Luria-Bertani (LB) broth supplemented with 1% D–glucose (LBglu). The cultures were diluted in LBglu to achieve an optical density (OD) of 0.03 at a wavelength of 570 nm. Aliquots of 200 μL of the final solution were added to each well of a 96-well tissue culture polystyrene microtiter plate. After incubation with agitation for 48 h at 37°C, the suspensions were removed and the wells were washed with phosphate-buffered saline (PBS), followed by the addition of 200 μL of 0.1% crystal violet to stain the cells. The plates were then incubated for 20 min with gentle agitation and washed. The crystal violet of the stained biofilms were solubilized with 200 μL of 95% ethanol for 10 min with agitation. The amount of biofilm formed was quantified by measuring the optical density at 570 nm (OD570). All experiments were performed in triplicates and repeated on three separate occasions. The OD570 values of the well with un-inoculated LB medium were used as a negative control. Those with OD570 values at least twice that of the negative controls on at least two separate occasions were considered as biofilm formation positive (Rodríguez-Baño et al., 2008).
Statistical analyses
The data were analyzed using the statistical package PASW for the Windows version 26 (SPSS, Chicago, IL, USA). The χ2 test with Yate’s correction or Fisher’s exact test was used to compare the categorical differences. Continuous variables were analyzed using the Student’s t test and data were presented as median and interquartile range (IQR). The time to mortality, defined as the interval between bacteremia onset and death, was analyzed using Kaplan–Meier survival analysis, and log-rank test was used to compare the univariate survival distribution between different groups of patients. The logistic regression model was used to explore independent prognostic factors associated with the 28-day mortality. Univariate analyses were performed for each of the risk factors to ascertain the odds ratio (OR) and 95% confidence interval (CI). All biologically plausible variables with a P < 0.10 in the univariate analysis were considered for inclusion in the multivariate logistic regression model with a backward selection process. A P < 0.05 was considered statistically significant.
Results
Patients who had experienced at least one episode of the A. baumannii complex monomicrobial bacteremia during the 9-year period were enrolled for evaluation. Those with bacteremia caused by non-baumannii Acinectobacter spp. were excluded from the analysis. Ultimately, of 711 patients that were enrolled, 385 (54.15%) survived and 326 (45.85%) died within 28 days of the onset of A. baumannii bacteremia. The demographic and clinical features of the 28-days survivors and non-survivors are presented in Table 1. Multivariate logistic regression analysis was carried out (Table 2) to delineate the independent risk factors of 28-day mortality due to A. baumannii bacteremia. Previous exposure to fluoroquinolones (OR, 2.052; CI 1.182–3.564; P = 0.011), liver cirrhosis (OR, 2.395; CI, 1.196–4.796; P = 0.014), higher disease severity (APACHE II score) (OR, 1.147; CI, 1.116–1.178; P < 0.001), shock (OR, 1.863; CI, 1.179–2.944; P =0.008), receipt of a thoracic drain (OR, 5.502; CI, 1.889–16.021; P = 0.002), infection by carbapenem-resistant isolates (OR, 2.425; CI, 1.524–3.858; P < 0.001), and receipt of inappropriate antimicrobial therapy (OR, 1.670; CI, 1.051–2.655; P = 0.030) were independent risk factors of 28-day mortality. In contrast, those who had hypertension (OR, 0.523; CI, 0.336–0.815; P = 0.004), cerebrovascular disease (OR, 0.296; CI, 0.171–0.512; P < 0.001), underwent a surgery within the past 4 weeks (OR, 0.492; CI, 0.288–0.840; P = 0.009), and those who had developed bacteremia as a consequence of a urinary tract infection (OR, 0.381; CI, 0.161–0.904; P = 0.029) were more likely to survive the 28-days after developing bacteremia. The proportion of infection caused by biofilm formation isolates was not significant differed between survivors and non-survivors within 28 days. (38.4% vs. 31.9%, P = 0.071).
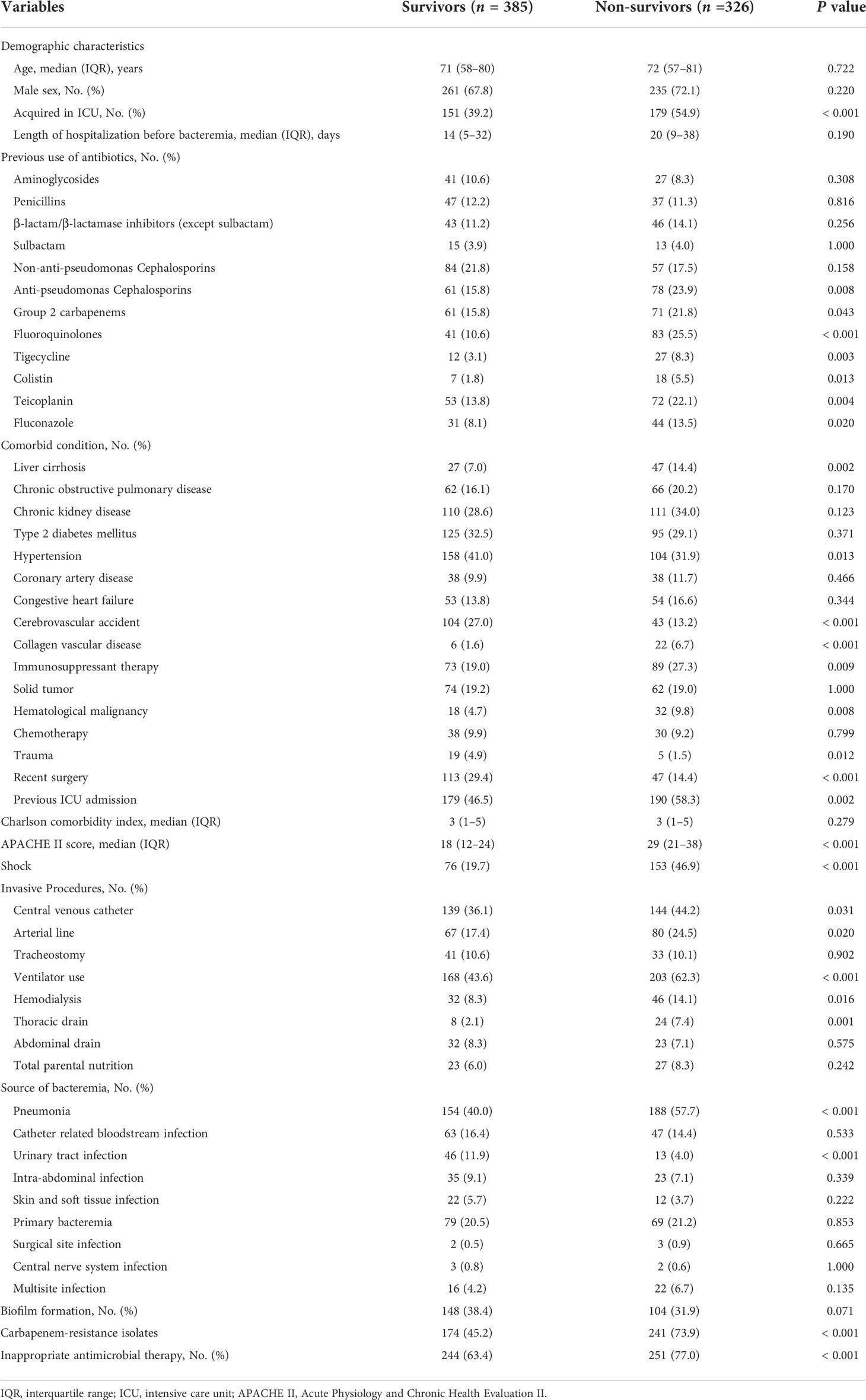
Table 1 Clinical characteristics and outcomes of patients with Acinetobacter baumannii bloodstream infections who survived or died within 28 days of bacteremia onset.
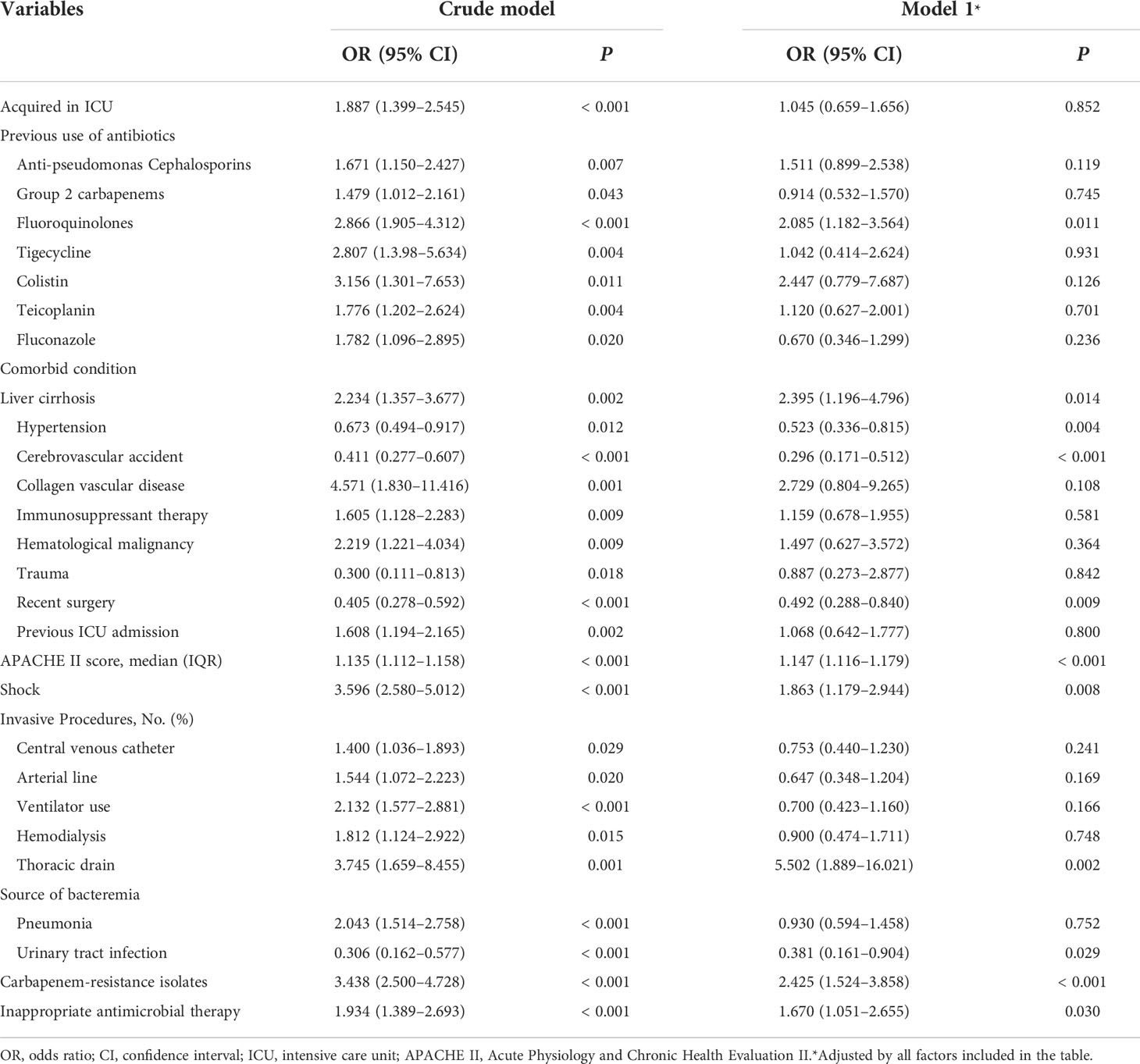
Table 2 Logistic regression analysis for the risk of 28-day mortality in patients with Acinetobacter baumannii bloodstream infections.
To further explore the risk of the infection by biofilm-forming isolates, we divided the patients into two groups according to the biofilm-forming ability of the bacterial isolates. The demographic and clinical characteristics of patients with A. baumannii bacteremia caused by the biofilm-forming (n = 252, 35.44%) and non-biofilm-forming (n = 459, 64.56%) isolates are listed in Table 3. Those who became infected with biofilm-forming isolates were less likely to contract the infection in the ICU (40.1% vs. 49.9%, P = 0.015), more likely to have congestive heart failure (19.0% vs. 12.9%, P = 0.029), less likely to be exposed previously to penicillin (8.3% vs. 13.7%, P= 0.039), more likely to have hematological malignancy (10.3% vs. 5.2%, P = 0.014), more likely to receive chemotherapy (12.7% vs. 7.8%, P = 0.045), less likely to receive a central venous catheter insertion (28.2% vs. 46.2%, P < 0.001), less likely to receive an arterial line insertion (9.5% vs. 26.8%, P < 0.001), less likely to be on a ventilator (44% vs. 56.6%, P = 0.002), and less likely to receive a thoracic drain insertion (2% vs. 5.9%, P = 0.022). The resistance rates to carbapenems were similar for both biofilm-forming and non-biofilm-forming isolates (56.7% vs. 59.3%, P = 0.525). Furthermore, there was no significant difference in their 14-day and 28-day mortality rates (Figure 1). The overall mortality rate was higher in the non-biofilm-forming group by a borderline statistical difference, compared with the biofilm-forming group (58.4% vs. 50.4%, P = 0.048). Logistic regression analysis was performed to delineate the independent risk factors for the infection by the biofilm-forming isolates. As shown in Table 4, congestive heart failure was a risk factor of infection with biofilm-forming isolates (OR, 1.918; CI, 1.221–3.012; P = 0.005). However, those who received an arterial line were less likely to be infected with biofilm-forming isolates (OR, 0.416; CI, 0.240–0.721; P = 0.002).
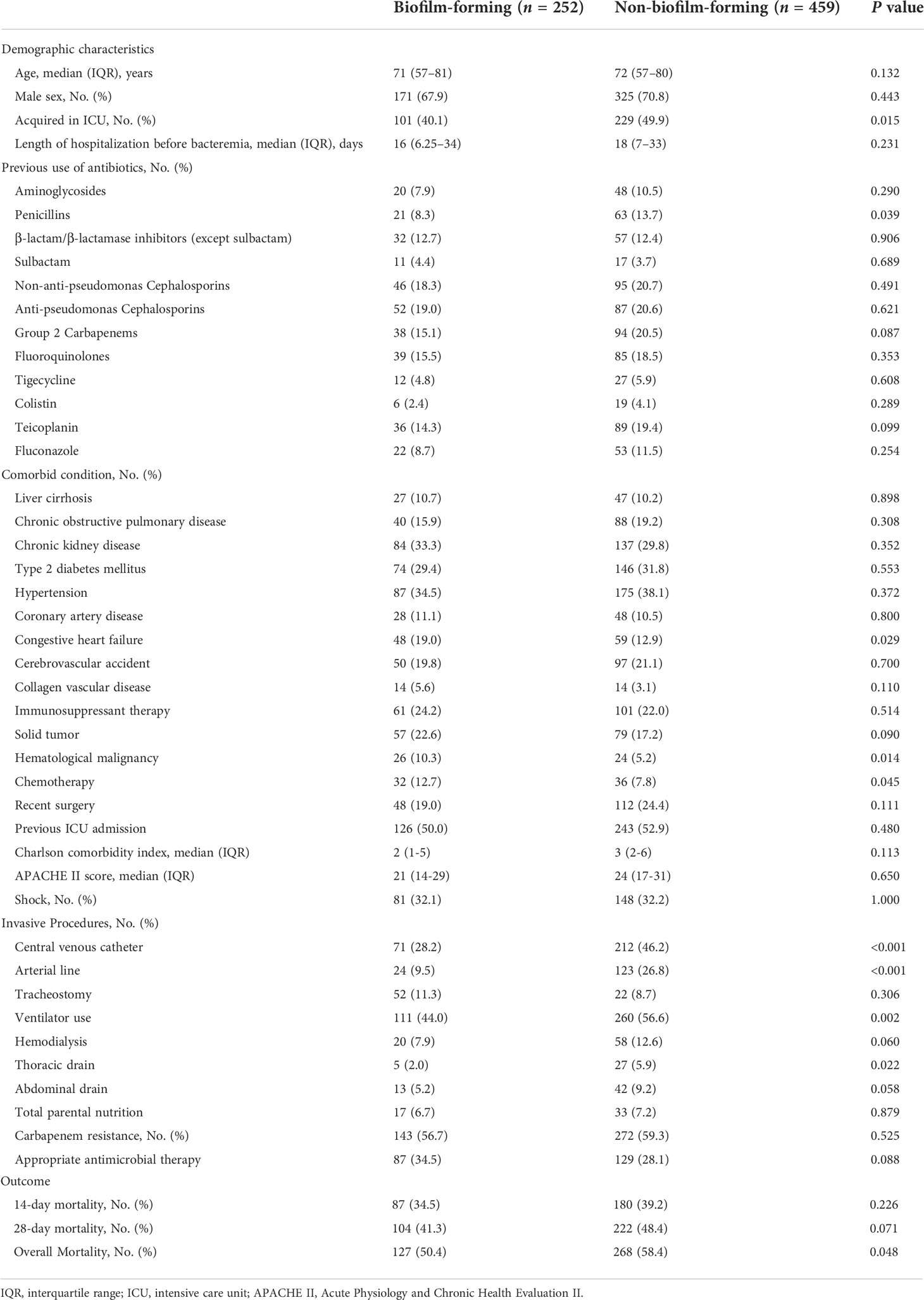
Table 3 Clinical characteristics of patients and clinical isolates with biofilm-forming and non-biofilm-forming Acinetobacter baumannii blood stream infections.
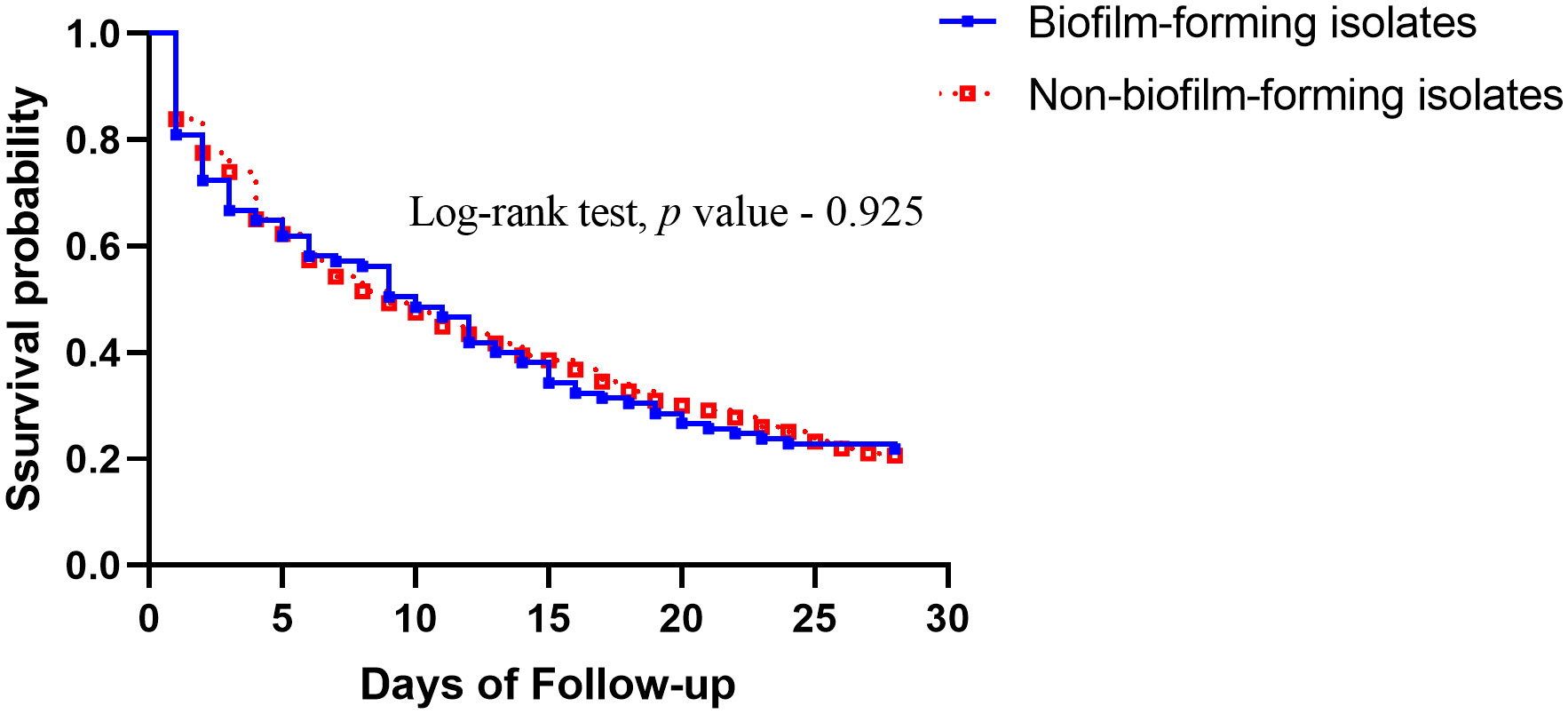
Figure 1 Comparison of Kaplan–Meier survival curves, at 28 days, between patients with Acinetobacter baumannii bacteremia caused by biofilm-forming isolates and non-biofilm-forming isolates.

Table 4 Logistic regression analysis of predictors for patients infected with biofilm-forming Acinetobacter baumannii.
We further stratified the strains according to the infection foci that resulted in bacteremia (Table 5). Pneumonia was the most common source of infection, followed by primary bacteremia and catheter-related bloodstream infections. There were no significant difference in the sources of bacteremia between the biofilm-forming and non-biofilm-forming isolates.
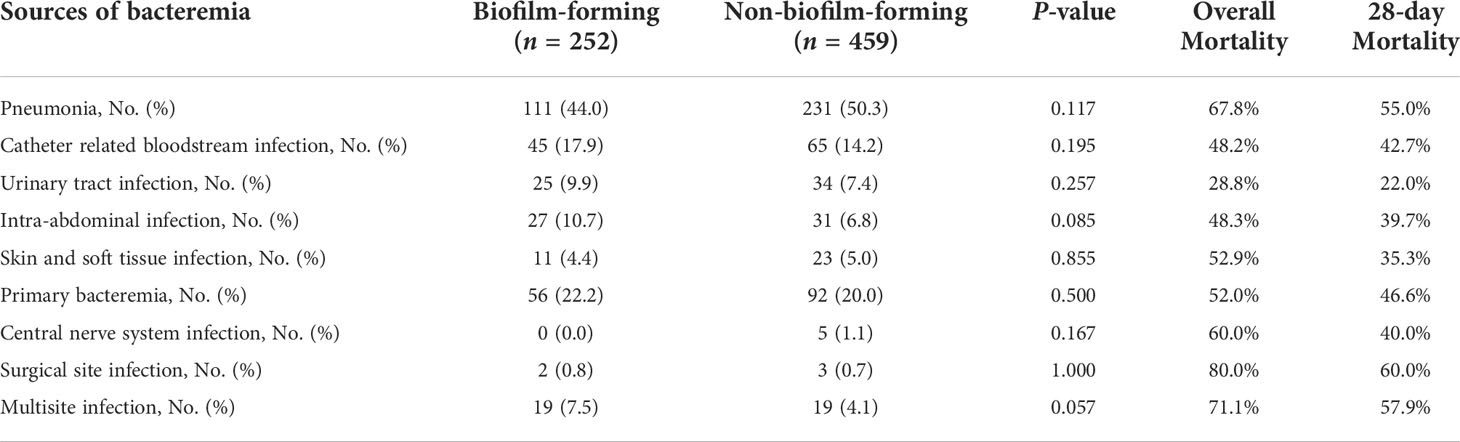
Table 5 Types of infections caused by biofilm-forming and non-biofilm-forming isolates of Acinetobacter baumannii.
A subgroup analysis was conducted to assess the risk factors of 28-day mortality in the patients infected with biofilm-forming isolates (Supplementary Table S1). Those who had developed bacteremia in the ICU, had previous exposure to fluoroquinolones, had collagen vascular disease, were recipients of immunosuppressant therapy, had hematological malignancy, had previous ICU admission history, were recipients of ventilator support, were infected with carbapenem-resistant isolates, had presented with shock, had higher APACHE II score, had bacteremia secondary to pneumonia, or had a multisite infection, were associated with a higher 28-day mortality rate. In contrast, those who underwent surgery within 4 weeks prior to the onset of bacteremia, those who had received appropriate antimicrobial therapy, those who had bacteremia secondary to urinary tract infection were associated with lower 28-day mortality rates. In the logistic regression analysis, those who had hematological malignancy (OR, 3.636; CI, 1.011–13.072; P = 0.048), infected with carbapenem-resistant isolates (OR, 2.945; CI, 1.344–6.453; P = 0.007), and had higher APACHE II score (OR, 1.151; CI, 1.098–1.206; P < 0.001) were independently associated with the 28-day mortality rates (Supplementary Table S2).
Discussion
This study revealed that there were no significant differences in the 14-day and 28-day mortality rates between patients infected with the biofilm-forming and non-biofilm-forming isolates of A. baumannii. Previous exposure to fluoroquinolones, liver cirrhosis, higher APACHE II score, shock status, infection with carbapenem-resistant isolates, and receipt of inappropriate antimicrobial therapy were independent risk factors of 28-day mortality in patients with A. baumannii bacteremia. Congestive heart failure was an independent risk factor of infection with biofilm-forming isolates, while the patients with an arterial line were more likely to be infected with non-biofilm-forming isolates.
It is not surprising that shock status, higher APACHE II score, infection with carbapenem-resistant A. baumannii, and inappropriate treatment were independent risk factors for mortality, which is consistent with previous findings (Peleg et al., 2008; Lee et al., 2012; Wong et al., 2017). Those with liver cirrhosis had a higher 28-day mortality in this study. Our previous study also demonstrated a higher 30-day mortality rate in patients with liver cirrhosis compared to those without cirrhosis;, however, there was no significant difference (Liu et al., 2019). That study investigated all Acinetobacter species and enrolled a relatively small number of patients with A. baumannii bacteremia. The relatively small population of patients with A. baumannii bacteremia in that study may have contributed to the insignificance.
Patients with a previous exposure to fluoroquinolones had worse clinical outcomes. Although there is limited research regarding the correlation between fluoroquinolone exposure and outcomes in patients with A. baumannii bacteremia, one study concluded that exposure to fluoroquinolones is an independent risk factor for the development of carbapenem-resistant A. baumannii bacteremia (Kopterides et al., 2007). This may explain the risk of mortality in patients with A. baumannii bacteremia in our study.
The components of biofilms and their unique environment overpower most antimicrobials used for treating biofilm-associated infections (Høiby et al., 2010; Del Pozo, 2018; Law and Tan, 2022). The biofilm-associated infections can subsequently induce chronic infections, resulting in a considerable burden on the global healthcare system (Hall-Stoodley et al., 2004; Høiby et al., 2015). However, there is limited research regarding the clinical implications of biofilm formation. A previous study demonstrated that those infected with biofilm-forming isolates of A. baumannii had a probable history of ICU admission, use of antibiotics, and lesser severity of disease (Zhang et al., 2016). The study did not demonstrate an influence of biofilm formation on the clinical outcomes in the patients. A single-institute study documented that the mortality during an initial infection was significantly more common in patients with the biofilm-forming isolates, compared with those with the non-biofilm-forming isolates (Barsoumian et al., 2015). However, the low attributable mortality (7.1%) among the study population made it difficult to draw any conclusions regarding the clinical outcomes of biofilm formation ability of A. baumannii (Barsoumian et al., 2015). Recently, in a cohort study involving 273 patients, we found that biofilm formation was not associated with worse outcomes in patients with A. baumannii bacteremic pneumonia (Wang et al., 2018). As A. baumannii contributes to a variety of biofilm-associated infections, we included all types of infections to delineate the effects of biofilm formation on the clinical outcomes in this study. We found that biofilm formation capability was not an independent risk factor of 14-day and 28-day mortality in patients with A. baumannii bacteremia.
Bacterial cells embedded in the biofilms are known to be resistant to antimicrobials through several mechanisms, including limited penetration of the antimicrobials, slow growth rate of the bacterial cells in biofilms, physiological heterogeneity of the biofilms, and the expression of some resistance genes (Lewis, 2001; Mah and O’Toole, 2001; Harrison et al., 2007; Olsen, 2015). These conditions make biofilms difficult to eradicate and therefore, the correlation between resistance to individual antibiotics and biofilm formation remains elusive. While some studies have shown a positive correlation between resistance to individual antibiotics and biofilm formation (Rao et al., 2008; Badave and Kulkarni, 2015), others have found a negative correlation between the biofilm formation ability and carbapenem resistance (Rodríguez-Baño et al., 2008; Qi et al., 2016; Wang et al., 2018). Our previous studies have also demonstrated that most carbapenem-resistant A. baumannii transformants exhibit reduced biofilm-forming abilities (Wang et al., 2018). Our current study has shown similar findings, as the biofilm-forming isolates exhibited lower rates of carbapenem-resistance than the non-biofilm-forming isolates (56.7% vs. 59.3%). These findings suggest that the complexity of biofilm composition, and not of the bacteria themselves in the biofilms, may contribute to the antibiotic resistance of the biofilms (Lewis, 2001; Mah and O’Toole, 2001; Harrison et al., 2007; Olsen, 2015). Further studies are needed to elucidate the detailed mechanisms of antimicrobial resistance in the biofilms.
A major strength of this study was the larger sample size of patients who were enrolled from multiple medical centers. In order to exclude colonized isolates, all the bacterial strains collected in this study were isolated from blood samples. We enrolled patients with A. baumannii bacteremia caused by different sources of infection to represent the real-world clinical situations. Another strength was the use of multivariate analysis to delineate the risk factors for mortality in patients with bacteremia caused by biofilm-forming isolates of A. baumannii.
This retrospective study had several limitations, including selection bias and inconsistencies in patient care among the different hospitals. Another key limitation is that the in vitro formation of biofilms does not represent the actual in vivo conditions. Although there are several methods for the detecting in vitro biofilm formation, there is currently no gold-standard protocol for its quantification. Furthermore, it is challenging to assess the biofilm formation inside the human body. In addition, the in vitro conditions may be quite different from those of the human environment.
In conclusion, this is the first large sample size study on the clinical outcomes of patients with A. baumannii bacteremia. Our results demonstrated that the biofilm-forming ability was not an independent risk factor for mortality in patients with A. baumannii bacteremia. Patients with A. baumannii bacteremia with a greater severity of disease, who were infected with carbapenem-resistant isolates, or had received an inappropriate antimicrobial therapy had worse outcomes. Patients with congestive heart failure were more likely to be infected with biofilm-forming isolates, while those with an arterial line were less likely to be infected with them. Among the patients infected with biofilm-forming isolates, those with hematological malignancies, infected with carbapenem-resistant isolates, and those with greater severity of disease (higher APACHE II scores) were associated with worse clinical outcomes. Further studies are required to establish the optimal treatment for bacteremia caused by the biofilm-forming isolates of A. baumannii.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving human participants were reviewed and approved by Changhua Christian Hospital (140514) Mackay Memorial Hospital (14MMHIS125) National Taiwan University Hospital (201008047R) Taipei Veterans General Hospital (2015-04-003C) Tri-Service General Hospital (1-103-05-100). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
Conceptualization, T-TC, Y-TL, and Y-CW; Data curation, AC, C-PL, Y-ML, and Y-SY; Formal analysis, T-TC, T-WH, and J-RS; Funding acquisition, Y-TL and Y-CW; Investigation, S-CK, AC, and C-PL; Methodology, T-TC, Y-TL, and Y-CW; Project administration, Y-TL, and Y-CW; Resources, Y-ML, Y-SY, and T-LC; Software, T-WH, J-RS, and S-CK; Supervision, T-LC, Y-TL, and Y-CW; Validation, T-LC, Y-TL, and Y-CW; Visualization, C-PL, Y-ML, and Y-SY; Writing – original draft, T-TC, Y-TL, and Y-CW; Writing – review and editing, T-TC, Y-TL, and Y-CW. All authors contributed to the article and approved the submitted version.
Funding
This work was supported by grants from Taipei Veterans General Hospital [V108C-012, VTA108-T-2-3, VTA109-T-3-2, VTA110-V4-5-2, VTA111-T-3-3], Tri-Service General Hospital [TSGH-E-109237, TSGH-E-110205, TSGH-E-111245], and the Ministry of Science and Technology [MOST-108-2314-B-016 -029, MOST-109-2314-B-016 -056, MOST-110-2314-B-016-063, MOST-110-2314-B-075-072, MOST 108-2314-B-075-034-MY3, MOST 107-2314-B-075-066-MY3].
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcimb.2022.964539/full#supplementary-material
References
Badave, G. K., Kulkarni, D. (2015). Biofilm producing multidrug resistant acinetobacter baumannii: An emerging challenge. J. Clin. Diagn. Res. 9, DC08–DC10. doi: 10.7860/JCDR/2015/11014.5398
Barsoumian, A. E., Mende, K., Sanchez, C. J., Jr., Beckius, M. L., Wenke, J. C., Murray, C. K., et al. (2015). Clinical infectious outcomes associated with biofilm-related bacterial infections: a retrospective chart review. BMC Infect. Dis. 15, 223. doi: 10.1186/s12879-015-0972-2
Chen, T.-L., Sin, L.-K., Wu, R. C.-C., Shaio, M.-F., Huang, L.-Y., Fung, C.-P., et al. (2007). Comparison of one-tube multiplex PCR, automated ribotyping and intergenic spacer (ITS) sequencing for rapid identification of Acinetobacter baumannii. clin. Microbiol. Infect. 13, 801–806. doi: 10.1111/j.1469-0691.2007.01744.x
Cisneros, J. M., Reyes, M. J., Pachón, J., Becerril, B., Caballero, F. J., García-Garmendía, J. L., et al. (1996). Bacteremia due to acinetobacter baumannii: epidemiology, clinical findings, and prognostic features. Clin. Infect. Dis. 22, 1026–1032. doi: 10.1093/clinids/22.6.1026
CLSI (2006). Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically: Approved standard M7-A7. Wayne, PA: Clinical and Laboratory Standards Institute.
CLSI (2020). Performance Standards for Antimicrobial Susceptibility Testing. 30th Ed. CLSI Supplement M100. Wayne, PA: Clinical and Laboratory Standards Institute.
Del Pozo, J. L. (2018). Biofilm-related disease. Expert Rev. Anti-Infect Ther. 16, 51–65. doi: 10.1080/14787210.2018.1417036
Dijkshoorn, L., Nemec, A., Seifert, H. (2007). An increasing threat in hospitals: multidrug-resistant acinetobacter baumannii. Nat. Rev. Microbiol. 5, 939–951. doi: 10.1038/nrmicro1789
Donadu, M. G., Mazzarello, V., Cappuccinelli, P., Zanetti, S., Madléna, M., Nagy, ÁL., et al. (2021). Relationship between the biofilm-forming capacity and antimicrobial resistance in clinical acinetobacter baumannii isolates: results from a laboratory-based in vitro study. Microorganisms 9(11):2384. doi: 10.3390/microorganisms9112384
Garner, J. S., Jarvis, W. R., Emori, T. G., Horan, T. C., Hughes, J. M. (1988). CDC Definitions for nosocomial infections, 1988. Am. J. Infect. Control. 16, 128–140. doi: 10.1016/0196-6553(88)90053-3
Gedefie, A., Demsis, W., Ashagrie, M., Kassa, Y., Tesfaye, M., Tilahun, M., et al. (2021). Acinetobacter baumannii biofilm formation and its role in disease pathogenesis: A review. Infect. Drug Resist. 14, 3711–3719. doi: 10.2147/IDR.S332051
Høiby, N., Bjarnsholt, T., Givskov, M., Molin, S., Ciofu, O. (2010). Antibiotic resistance of bacterial biofilms. Int. J. Antimicrob. Agents. 35, 322–332. doi: 10.1016/j.ijantimicag.2009.12.011
Høiby, N., Bjarnsholt, T., Moser, C., Bassi, G. L., Coenye, T., Donelli, G., et al. (2015). ESCMID guideline for the diagnosis and treatment of biofilm infections 2014. Clin. Microbiol. Infect. 21 Suppl 1, S1–25. doi: 10.1016/j.cmi.2014.10.024
Høiby, N., Bjarnsholt, T., Moser, C., Bassi, G. L., Coenye, T., Donelli, G., et al. (2015). ESCMID guideline for the diagnosis and treatment of biofilm infections 2014. Clin. Microbiol. Infect. 21, S1–25. doi: 10.1016/j.cmi.2014.10.024
Hall-Stoodley, L., Costerton, J. W., Stoodley, P. (2004). Bacterial biofilms: from the natural environment to infectious diseases. Nat. Rev. Microbiol. 2, 95–108. doi: 10.1038/nrmicro821
Harrison, J. J., Ceri, H., Turner, R. J. (2007). Multimetal resistance and tolerance in microbial biofilms. Nat. Rev. Microbiol. 5, 928–938. doi: 10.1038/nrmicro1774
Kopterides, P., Koletsi, P. K., Michalopoulos, A., Falagas, M. E. (2007). Exposure to quinolones is associated with carbapenem resistance among colistin-susceptible acinetobacter baumannii blood isolates. Int. J. Antimicrob. Agents. 30, 409–414. doi: 10.1016/j.ijantimicag.2007.06.026
Law, S. K. K., Tan, H. S. (2022). The role of quorum sensing, biofilm formation, and iron acquisition as key virulence mechanisms in acinetobacter baumannii and the corresponding anti-virulence strategies. Microbiol. Res. 260, 127032. doi: 10.1016/j.micres.2022.127032
Lee, Y. T., Kuo, S. C., Yang, S. P., Lin, Y. T., Tseng, F. C., Chen, T. L., et al. (2012). Impact of appropriate antimicrobial therapy on mortality associated with acinetobacter baumannii bacteremia: Relation to severity of infection. Clin. Infect. Dis. 55, 209–215. doi: 10.1093/cid/cis385
Lewis, K. (2001). Riddle of biofilm resistance. Antimicrob. Agents Chemother. 45, 999–1007. doi: 10.1128/AAC.45.4.999-1007.2001
Liu, C. P., Chiang, T. T., Liu, Y. M., Kuo, S. C., Yang, Y. S., Lee, Y. T., et al. (2019). A multicenter study on clinical characteristics of acinetobacter bacteremia in patients with liver cirrhosis. J. Microbiol. Immunol. Infect. Wei mian yu gan ran za zhi. 52, 956–965. doi: 10.1016/j.jmii.2018.03.001
Mah, T. F., O’Toole, G. A. (2001). Mechanisms of biofilm resistance to antimicrobial agents. Trends Microbiol. 9, 34–39. doi: 10.1016/s0966-842x(00)01913-2
Martí, S., Rodríguez-Baño, J., Catel-Ferreira, M., Jouenne, T., Vila, J., Seifert, H., et al. (2011). Biofilm formation at the solid–liquid and air–liquid interfaces by acinetobacter species. BMC Res. Notes. 4, 5. doi: 10.1186/1756-0500-4-5
Olsen, I. (2015). Biofilm-specific antibiotic tolerance and resistance. Eur. J. Clin. Microbiol. Infect. Dis. 34, 877–886. doi: 10.1007/s10096-015-2323-z
O’Toole, G. A., Pratt, L. A., Watnick, P. I., Newman, D. K., Weaver, V. B., Kolter, R. (1999). Genetic approaches to study of biofilms. Methods Enzymol. 310, 91–109. doi: 10.1016/s0076-6879(99)10008-9
Peleg, A. Y., Seifert, H., Paterson, D. L. (2008). Acinetobacter baumannii: emergence of a successful pathogen. Clin. Microbiol. Rev. 21, 538–582. doi: 10.1128/CMR.00058-07
Qi, L., Li, H., Zhang, C., Liang, B., Li, J., Wang, L., et al. (2016). Relationship between antibiotic resistance, biofilm formation, and biofilm-specific resistance in acinetobacter baumannii. Front. Microbiol. 7. doi: 10.3389/fmicb.2016.00483
Rao, R. S., Karthika, R. U., Singh, S. P., Shashikala, P., Kanungo, R., Jayachandran, S., et al. (2008). Correlation between biofilm production and multiple drug resistance in imipenem resistant clinical isolates of acinetobacter baumannii. Indian J. Med. Microbiol. 26, 333–337. doi: 10.4103/0255-0857.43566
Rodríguez-Baño, J., Martí, S., Soto, S., Fernández-Cuenca, F., Cisneros, J. M., Pachón, J., et al. (2008). Biofilm formation in acinetobacter baumannii: Associated features and clinical implications. Clin. Microbiol. Infect. 14, 276–278. doi: 10.1111/j.1469-0691.2007.01916.x
Villegas, M. V., Hartstein, A. I. (2003). Acinetobacter outbreaks, 1977–2000. Infect. Control Hosp. Epidemiol. 24, 284–295. doi: 10.1086/502205
Wang, Y. C., Huang, T. W., Yang, Y. S., Kuo, S. C., Chen, C. T., Liu, C. P., et al. (2018). Biofilm formation is not associated with worse outcome in acinetobacter baumannii bacteraemic pneumonia. Sci. Rep. 8, 7289. doi: 10.1038/s41598-018-25661-9
Wang, Y. C., Kuo, S. C., Yang, Y. S., Lee, Y. T., Chiu, C. H., Chuang, M. F., et al. (2016). Individual or combined effects of meropenem, imipenem, sulbactam, colistin, and tigecycline on biofilm-embedded acinetobacter baumannii and biofilm architecture. Antimicrob. Agents Chemother. 60, 4670–4676. doi: 10.1128/AAC.00551-16
Wong, D., Nielsen, T. B., Bonomo, R. A., Pantapalangkoor, P., Luna, B., Spellberg, B. (2017). Clinical and pathophysiological overview of Acinetobacter infections: a century of challenges. Clin. Microbiol. Rev. 30, 409–447. doi: 10.1128/CMR.00058-16
Keywords: Acinetobacter baumannii, bacteremia, biofilm, carbapenem resistance, mortality
Citation: Chiang T-T, Huang T-W, Sun J-R, Kuo S-C, Cheng A, Liu C-P, Liu Y-M, Yang Y-S, Chen T-L, Lee Y-T and Wang Y-C (2022) Biofilm formation is not an independent risk factor for mortality in patients with Acinetobacter baumannii bacteremia. Front. Cell. Infect. Microbiol. 12:964539. doi: 10.3389/fcimb.2022.964539
Received: 08 June 2022; Accepted: 31 August 2022;
Published: 16 September 2022.
Edited by:
Milena Dropa, Faculty of Public Health, University of São Paulo, BrazilReviewed by:
Stefania Zanetti, University of Sassari, ItalyCarolina Silva Nodari, Institut Pasteur, France
Copyright © 2022 Chiang, Huang, Sun, Kuo, Cheng, Liu, Liu, Yang, Chen, Lee and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yung-Chih Wang, d3lzdHd5c3RAZ21haWwuY29t; Yi-Tzu Lee, czg1MTAwOUB5YWhvby5jb20udHc=
†These authors have contributed equally to this work