
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cell. Infect. Microbiol., 17 June 2022
Sec. Clinical Microbiology
Volume 12 - 2022 | https://doi.org/10.3389/fcimb.2022.907314
This article is part of the Research TopicRekindling of a Masterful Precedent: BacteriophageView all 5 articles
 Lucile Plumet1
Lucile Plumet1 Nour Ahmad-Mansour1
Nour Ahmad-Mansour1 Catherine Dunyach-Remy2
Catherine Dunyach-Remy2 Karima Kissa1
Karima Kissa1 Albert Sotto3
Albert Sotto3 Jean-Philippe Lavigne2
Jean-Philippe Lavigne2 Denis Costechareyre1,4
Denis Costechareyre1,4 Virginie Molle1*
Virginie Molle1*Staphylococcus aureus (S. aureus) is a common and virulent human pathogen causing several serious illnesses including skin abscesses, wound infections, endocarditis, osteomyelitis, pneumonia, and toxic shock syndrome. Antibiotics were first introduced in the 1940s, leading to the belief that bacterial illnesses would be eradicated. However, microorganisms, including S. aureus, began to develop antibiotic resistance from the increased use and abuse of antibiotics. Antibiotic resistance is now one of the most serious threats to global public health. Bacteria like methicillin-resistant Staphylococcus aureus (MRSA) remain a major problem despite several efforts to find new antibiotics. New treatment approaches are required, with bacteriophage treatment, a non-antibiotic strategy to treat bacterial infections, showing particular promise. The ability of S. aureus to resist a wide range of antibiotics makes it an ideal candidate for phage therapy studies. Bacteriophages have a relatively restricted range of action, enabling them to target pathogenic bacteria. Their usage, usually in the form of a cocktail of bacteriophages, allows for more focused treatment while also overcoming the emergence of resistance. However, many obstacles remain, particularly in terms of their effects in vivo, necessitating the development of animal models to assess the bacteriophage efficiency. Here, we provide a review of the animal models, the various clinical case treatments, and clinical trials for S. aureus phage therapy.
More than a century ago, bacteriophages were offered as an alternate therapy for bacterial diseases. However, the discovery of antibiotics led to phage treatment being mostly ignored, with the exception of some Eastern European nations (Chanishvili, 2012). The research and development of novel antibiotics has been largely abandoned by the majority of pharmaceutical companies (Projan, 2003; Projan and Shlaes, 2004). This has resulted in a 90 percent decrease in new systemic antibiotic approvals by the United States Food and Drug Administration (FDA) over the last 30 years (Spellberg et al., 2008; Shlaes et al., 2013). The World Health Organization (WHO) estimates that antibiotic-resistant infections account for around 700,000 deaths per year worldwide, and that this figure might rise to 10 million fatalities by 2050, accounting for more deaths than cancer (O’Neill, 2016). Therefore, the WHO has urged researchers to design innovative antibacterial approaches for treating priority antibiotic-resistant infections (Asokan et al., 2019). The use of specialized and individualized phage mixtures has shown to be an interesting alternative in the fight against multi-drug resistant bacteria (Kortright et al., 2019; AL-Ishaq et al., 2021). Phage therapy, a non-antibiotic technique for treating bacterial infections, has recently regained popularity. Phages are lytic viruses that infect bacteria from a variety of habitats, including soil, wastewater, and aquatic environments (Principi et al., 2019). Because of their specificity, the use of phages as a therapeutic option seems to be highly advantageous. Lytic phages are an acceptable option for human infection treatments as they kill their bacterial host quickly and they can be used by mixing several, minimizing the likelihood of bacteria acquiring phage resistance. Moreover, these organisms only infect their target bacteria and have no effect on the human host microbiota, in contrast to antibiotics, which can induce intestinal microbial dysbiosis (Febvre et al., 2019). Many Gram-negative and Gram-positive bacteria, especially S. aureus, have been effectively treated using phage treatment, although this is not yet a routine therapeutic method (Kortright et al., 2019; Luong et al., 2020). S. aureus is a common pathogen that causes hospital- and community-acquired infections worldwide. It is remarkably adaptable, capable of causing a wide range of illnesses varying in severity from minor skin and soft-tissue infections to lethal bloodstream infections in humans and animals (Lowy, 1998). In this review, we focus on animal models, the various clinical case treatments, and clinical trials for S. aureus phage therapy.
A number of animal models of the most prevalent and important human bacterial illnesses have been used to evaluate newly identified phages and their efficiency in combating bacterial infections in vivo (Melo et al., 2020). These studies have assessed the safety and efficacy of medications to translate to human therapy (Brix et al., 2020; Melo et al., 2020). Vertebrate and invertebrate animal models improve understanding of the processes of phage therapy on a living organism, including the immune response, the gastrointestinal microbiota, infected tissue, the level of security, toxicity, and potential side effects (Brix et al., 2020). Interestingly, for most of the S. aureus-related infections an animal model was developped, excepted to date for urinary tract infections (Luong et al., 2020). In Table 1, we summarized the animal model findings regarding the development of S. aureus phage therapy.
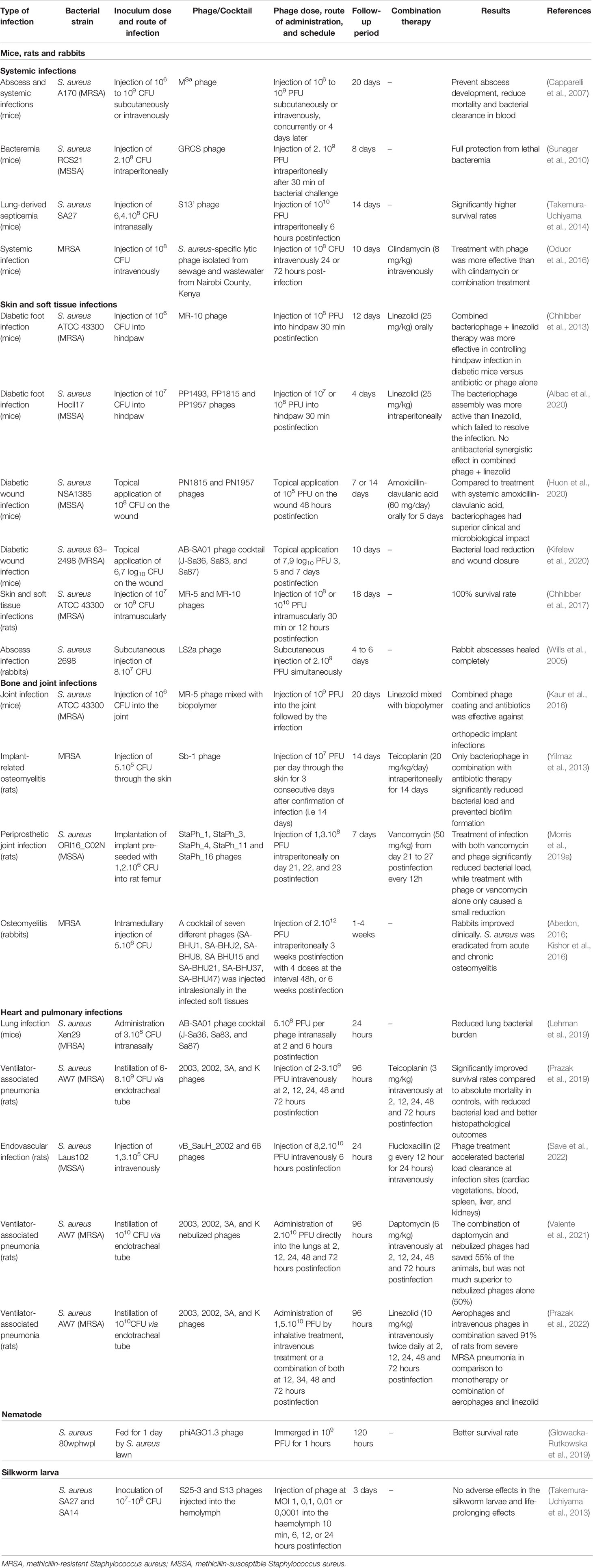
Table 1 Animal models for the development of S. aureus phage therapy.
Mouse (Mus musculus), rat (Rattus norvegicus) and rabbit (Oryctolagus cuniculus) models have been reported for S. aureus phage therapy. Testing novel medicinal compounds in vertebrates is often preferred due to their genetic similarity to humans (Brix et al., 2020; Cieślik et al., 2021).
Murine models are the most common for investigating S. aureus phage treatment in diverse pathologies as detailed below and summarized in Table 1. The genetic and physiological similarities between the murine and human species allow to investigate the efficacy of phage treatment developped for human medecine. Animals such as mice may only tolerate the injection of low amounts of liquid, particularly when delivered intravenously or intranasally; phages must thus be concentrated in order to accommodate the required inoculum (Penziner et al., 2021).
Systemic infections are those that result in bacteremia and/or propagation to several organs. Capparelli et al. described the isolation of a phage active against local and systemic infections of S. aureus in mice, demonstrating the decrease in bacterial load following phage treatment (Capparelli et al., 2007). A single dose of phage treatment injected intravenously four days after the infection challenge showed a 100-fold decrease in the bacterial counts, while repeated doses resulted in a 10,000-fold decrease. Phage-treated animals were free of bacteria in their kidneys, spleens, blood, and hearts at 20 days post-therapy, while the control mouse’s organs and blood remained contaminated. They also emphasized that phage therapy administered simultaneously with bacteria inhibited the development of methicillin-resistant S. aureus (MRSA)-related abscesses (Capparelli et al., 2007).
Sunagar et al. (2010) developed phage therapy as an alternative treatment for fatal S. aureus bacteremia in diabetic and non-diabetic mouse models (Sunagar et al., 2010). In both diabetic and non-diabetic septicemic mice, a single intraperitoneal dose of the GRCS phage was significantly more beneficial than oxacillin antibiotic alone. Noteworthy, diabetic and nondiabetic mice were both given the fourth injection in a series of weekly injections of the phage GRCS. After the fourth injection, the titers of IgG and IgM antibodies against the phage rose above the background by 2500 fold and 100-fold, respectively, in both groups. Though, despite this augmentation, no allergic responses, changes in core body temperature, or other adverse effects were noted in any of the two groups (Sunagar et al., 2010). Another mouse model of bacteremia is the staphylococcal lung-derived fatal septicemia developed and tested by Takemura-Uchiyama et al., where the therapeutic benefits of phage S13′ were investigated (Takemura-Uchiyama et al., 2014). The intraperitoneal phage treatment at six hours post-infection lowered the severity of the symptoms and saved the affected mice. In addition, Oduor et al. (2016) demonstrated that a S. aureus-specific lytic phage found in waste and sewage water in Nairobi County could be used for MRSA bacterial infections (Oduor et al., 2016). Their mouse model provided evidence that phage treatment could be used to tackle the increasing antimicrobial resistance in sub-Saharan Africa (Lord et al., 2021).
Efficacy is often shown in studies to be dependent on the time of phage delivery. Capparelli et al. (2007) demonstrated that therapy may be postponed significantly in the case of a more chronic infection, and that the severity of the infection was dependent on the phage dosage administered. The research carried out by Caparelly and colleagues gives support to prior remarks on the limitations imposed by some experimental infection designs (Bull et al., 2002). Furthermore, in all of the publications analysed, the phages were supplied either intraperitoneally or intravenously, which are the ways via which drugs are frequently provided in medical practise. More research, however, is needed to evaluate other treatment options such as oral administration. As a result, the success for phage therapy in the treatment of systemic S. aureus infections is dependent on a number of parameters that must be extensively investigated before phage therapy can be widely used in the treatment of sepsis in humans.
Chhibber et al., showed that phage treatment had comparable effectiveness to linezolid antibiotic cure in halting hindpaw infection in diabetic mice with a single dose of the lytic phage, MR-10 (Chhibber et al., 2013). However, combining the treatments significantly increased the arrest of entire infection process. More recently, the same group presented a promising approach for improving phage treatment by using liposomes and transfersomes to deliver the phage to the patient (Chhibber et al., 2017; Malik et al., 2017). These vesicles disperse the substance throughout the body, avoiding fast breakdown, and increasing cellular absorption (Singh et al., 2015; Abu Lila and Ishida, 2017). In a rat model of S. aureus skin and soft tissue infection (SSTI), Chhibber et al.. demonstrated that transfersomes-entrapped phages injected intramuscularly generated a quicker recovery than free phages upon S. aureus SSTI (Chhibber et al., 2017). This novel approach demonstrates the advantages of a novel strategy to treat SSTI caused by MRSA, combining vectorization and phage delivery.
DFI are usually polymicrobial, yet, S. aureus is the most commonly found pathogen (Lipsky et al., 2020; Pouget et al., 2021). Recent research by Albac et al. evaluated the in vivo effectiveness of a cocktail of three phages (PP1493, PP1815 and PP1957) in comparison to linezolid in diabetic and non-diabetic mouse models of methicillin-susceptible S. aureus (MSSA) foot infection (Albac et al., 2020). In all cases, a single dose of phages into the hindpaw demonstrated considerable antistaphylococcal activity. Linezolid was as efficient as phages in non-diabetic mice but was ineffective in diabetic mice. The bacteriophages were found in high quantity in all examined organs two hours after the intravenous administration, according to the results of the pharmacokinetic data, and were still detected in the spleen 72 hours after infection, but they quickly declined in the blood, liver, and kidney, to be undetected after 48 hours (Albac et al., 2020). Moreover, during the pharmacokinetic research, no clinical symptoms of toxicity (mortality, weight loss, or decreased activity) were found in the participants overall. These results indicate that a single dose of three mixed phages at the sites of infection was about as efficient as a single dose of linezolid intravenously in lowering the bacterial load in the hindpaw of non-diabetic mice. These promising, preliminary data imply that phages may be a viable therapy option for S. aureus DFI that are very severe and difficult to treat. Moreover, this phage cocktail has progressed to clinical testing.
The AB-SA01 phage cocktail was applied topically to diabetic mice, where the antimicrobial activity was evaluated for its ability to heal wounds infected by MRSA clinical strains (Kifelew et al., 2020). A week after AB-SA01 treatment, a significant decrease in bacterial burdens was observed, while the non-treated group remained infected. AB-SA01 therapy may have higher or equal effectiveness to vancomycin, which is the standard first-line antibiotic for treating severe MRSA DFI. These examples of phage cocktails rather than single phage solution have the benefit of enhancing the host range of therapeutic phage compositions, and decreasing the development of phage resistant strains (Chan et al., 2013). In addition, Huon et al. (2020) used an infected diabetic wound model in mice to evaluate topical administration of phages delivered alone or in conjunction with oral amoxicillin-clavulanic acid. Clinical recovery was enhanced with phage therapy, with a decrease in local bacterial load at 7 and 14 days post-treatment (Huon et al., 2020). In comparison to antibiotic therapy, the phage medication did not have an effect on the gut microbiota. In conclusion, these latest studies demonstrate that local application of phages to cure DFI is a realistic complementary strategy when combined with oral antibiotic therapy.
Similarly to humans but in contrast to mice, rabbits are naturally susceptible to S. aureus infections, making them an excellent animal model for studying the development of staphylococcal diseases. A rabbit model of S. aureus wound infection has been designed (Wills et al., 2005) using subcutaneous injections, resulting in the formation of abscesses. Phages were given either concurrently with the bacteria or soon after at the infected region. Four to six days after infection, the phage treatment showed to be effective in preventing abscess development when the phages were administered simultaneously with S. aureus (Wills et al., 2005).
The studies most clearly demonstrate the safety of phage treatment when applied topically like for diabetic foot ulcer, or injected intramuscularly or in the hindpaw of mice. It is noteworthy that the majority of the studies evaluated models for phage treatment against infected diabetic foot ulcers, so proving the efficiency of such models for treating these types of infections.
Heart and pneumonia models of phage treatment were first underrepresented in comparison to other models of infection, but they have recently gained prominence in the scientific literature as detailed below. Lehman et al. (2019) described the design of AB-SA01, a phage cocktail targeting S. aureus. In vitro, AB-SA01 was effective against 94.5% of 401 clinical S. aureus strains, including MRSA. Intranasal administration of AB-SA01 decreased lung S. aureus bacterial load to the same extent as vancomycin, in both neutropenic and immunocompetent mice models of acute pneumonia (Lehman et al., 2019). Prazak et al. (2019) investigated the effectiveness of intravenous phage therapy in ventilator-associated pneumonia (VAP) caused by MRSA (Prazak et al., 2019). In a fatal rat model of staphylococcal pneumonia, phage treatment considerably decreased mortality compared to placebo. However, there was no difference for rats treated with a combination of phages and teicoplanin. In addition, the fact that non-infected animals treated with phage showed a slight elevation in IL-1β production raises concerns regarding the use of phage treatment in the absence of a diagnosis or a strong suspicion of VAP. This effect has been reported in other investigations, which have used a variety of different experimental conditions and phages, highlighting the need for a comprehensive reconsideration of the precise influence of induced inflammation during the clinical course of infection (Van Belleghem et al., 2017). One measure that would be required would be the use of highly purified, toxin-free phage solutions that would be generated in accordance with the Good Manufacturing Practices (GMP). In a recent study by Valente et al. (2021) they determine the effects of systemic daptomycin in combination with nebulized bacteriophages in the treatment of experimental pneumonia caused by methicillin-resistant S. aureus (Valente et al., 2021). A rat animal model of VAP caused by MRSA was used to determine whether the simultaneous application of intravenous daptomycin and nebulised phages was superior to aerophage therapy alone in terms of improving animal survival (55 percent vs. 50%) or reducing bacterial burdens in either the lungs or an organ known to be affected by the infection. As a result, it does not seem that this combination is beneficial when used in individuals with MRSA pneumonia. However, it is still uncertain which technique of phage delivery is most effective in the setting of VAP. Therefore, Prazak et al. (2022) investigated the efficacy of aerosolized phages (aerophages) in the treatment of experimental MRSA pneumonia. Single treatment either by either aerophages or intravenous phages (IV) were able to save fifty percent of the animals who were suffering from severe MRSA pneumonia. Interestingly, aerophages and phages together saved 91% of the animals, which was a significantly larger percentage than using either treatment alone (Prazak et al., 2022). In addition, antibiotic treatment with the standard drug linezolid was successful in saving 38% of the animals, while synergy between linezolid and aerophages was not seen. However, this model exhibited significant shortcomings as it is rapidly lethal for animals and then required therapy quickly after inoculation which is not a true representation of what happens in clinical settings. The establishment of a repeatable infection also depends on a significant quantity of bacteria as well as high phage loads to produce a therapeutic effect that was satisfactory. Consequently, additional studies are required for its potential extrapolation for human treatment. Save et al. (2022) recently demonstrated the efficiency of a phage cocktail against MRSA strains tested in vitro and in vivo in a rat model of endocarditis (Save et al., 2022). Interestingly, in most studies reviewed treatment with staphylococcal phages was most effective when used in conjunction with antibiotics, confirming that this phage therapy is a promising alternative treatment.
There are a few animal studies on bacteriophage treatment for bone and joint infections, but most were conducted in murine models (Genevière et al., 2021; Gibb and Hadjiargyrou, 2021). As detailed in the case reports sections, implant-related staphylococcal infections resistant to most antibiotics represent a serious problem in orthopedic surgery. Yilmaz et al. (2013) investigated the effect of local application of bacteriophages against bacterial biofilms. Rats were implanted with an intravenous catheter containing a pre-generated biofilm in the tibial medullary canal and examined for implant-related osteomyelitis. The findings revealed a synergistic effect of teicoplanin and the phages in eradicating MRSA biofilms (Yilmaz et al., 2013). A similar approach was undertaken by Kaur et al. (2016), who investigated the effects of naked wire, hydroxypropylmethylcellulose (HPMC)-coated wire, or K-wire coated with phage and/or linezolid (Kaur et al., 2016). The wires were surgically inserted into the intramedullary canals of mice femora and inoculated with MRSA. The mice transplanted with K-wire coated with a combination of phage and linezolid had the greatest benefits, which included reduced inflammation of the joint and decreased bacterial adhesion to the adjacent joint tissue, as well as better recovery of limb locomotion and functional ability. Therefore, the use of dual coated implants including both linezolid and a specific MRSA lytic phage represents a novel, attractive and effective strategy in the prevention and treatment of implant-associated MRSA infections. In addition, Morris et al. (2018) previously demonstrated in in vitro experiments the ability of a lytic phage cocktail to lower the amount of S. aureus bacteria in growing biofilms on custom 3D-printed, miniaturized porous titanium implants, a material that is frequently used during for orthopedic implants (Morris et al., 2018). The same group developed a new rat model of S. aureus biofilm-associated prosthetic joint infection using the same titanium implants and other biomaterials used in total knee arthroplasty procedures (Morris et al., 2019b). They revealed that the combined effect of phages and vancomycin provided a considerably greater therapeutic value than separate therapy, although phage therapy alone decreased bacterial load within joint tissue and on the titanium implant of the infected knee in the first week of therapy. Furthermore, no detrimental systemic or local damage was detected after multiple doses of lytic phages containing high quantities of phages (Morris et al., 2019a). Moreover, there were no important variations in IL-6, IL-1ß, and IL-4 levels in plasma of vancomycin-treated and phage plus vancomycin-treated animals at day 28 post-surgery in comparison to treated controls.
Another study in the rabbit model found that phage treatment was successful in a MRSA osteomyelitis infection model, although others disputed the conclusions of this study (Abedon, 2016; Kishor et al., 2016). Although the viability of phage treatment was established, the rabbit model differed from the patient’s condition, in which the infection was persistent and phage medication was performed after traditional techniques had failed. This case illustrated the difficulty in developing suitable chronic models of infection. This is a recurrent issue in bacteriophage therapy as animal models are used to study acute infections, which may not be the best equivalent for phage treatment in humans, where it is used to treat chronic conditions (Kortright et al., 2019).
The use of a non-mammalian model avoids the ethical issues that come with researches with in mammals. For instance, the nematode (Caenorhabditis elegans), common fruit fly (Drosophila melanogaster), wax moth (Galleria mellonella), silkworm (Bombyx mori) and zebrafish (Danio rerio), are among the most common invertebrate or lower vertebrate models for phage therapy (Brix et al., 2020). However only the nematode and silk worm larva models have been used for S. aureus studies (Takemura-Uchiyama et al., 2013; Glowacka-Rutkowska et al., 2019).
C. elegans is a small worm of 1 mm in length that may be readily infected by bacteria, fungi, and virus, resulting in deadly or non-lethal infection depending on the pathogen (Cohen and Troemel, 2015). C. elegans may be used for large-scale screening experiments since the pathways causing mortality in nematodes are conserved in mammals as while bypassing professional immune cells, the response against pathogens in C. elegans is conducted by epithelial cells that stimulate autophagy and the immune system via the synthesis of antimicrobial proteins, peptides (AMPs), and p38 pathway activation (Ewbank and Zugasti, 2011). As nematodes eat bacteria as their primary food source, infections may be accomplished quickly and simply. Phages can be supplied using the same mode of administration. C. elegans models for S. aureus infections and the use of phage treatment were developed recently by Glowacka-Rutkowska et al., and showed a significant decrease of mortality for larvae treated following S. aureus infection (Glowacka-Rutkowska et al., 2019). The staphylococcal lytic podovirus phiAGO1.3 presented a wide strain spectrum, thus demonstrating the promising potential of this phage in a clinical setting. Furthermore, they showed that phiAGO1.3 and its S. aureus host strains may co-exist over time, thus contributing to the emergence of phage-resistant strains but with reduced virulence (Glowacka-Rutkowska et al., 2019).
The findings of this research suggested that C. elegans may be used as an animal model, despite the fact that mortality was used as the only measure for analysing phage efficacy and effects.
As an animal model for infection, silkworm larvae offer a number of benefits, including the ability to reproduce in a short amount of time, the ability to be readily cultured in laboratories. The size of silkworm larvae is also adequate for handling during syringe injection of pathogens and therapeutics, which is a practical challenge with small-sized species such as Drosophila melanogaster and Caenorhabditis elegans. The silkworm larva has been used to test pharmacodynamics, pharmacokinetics, pathogenicity and toxicity of novel antimicrobial compounds (Kaito et al., 2002; Kaito and Sekimizu, 2007; Kurokawa et al., 2007; Fujiyuki et al., 2010). Takemura-Uchiyama et al. (2013) selected S. aureus phages with a wide host range from wastewater (Takemura-Uchiyama et al., 2013), isolating two staphylococcal phages, S25-3 and S13′. Administration of these phages alone had no negative impact on the silkworm larvae but had significant protective effects in silkworm larvae infected with S. aureus. This model was validated by comparison in an acute septic mice infection model, where the findings were comparable. Despite the distinct circulatory and immunity, the silkworm larval infection model seems relevant to test antibiotics and phage treatments upon S. aureus infections (Takemura-Uchiyama et al., 2013).
Bacteriophage treatments have been infrequently described for different infections in case studies (Table 2).
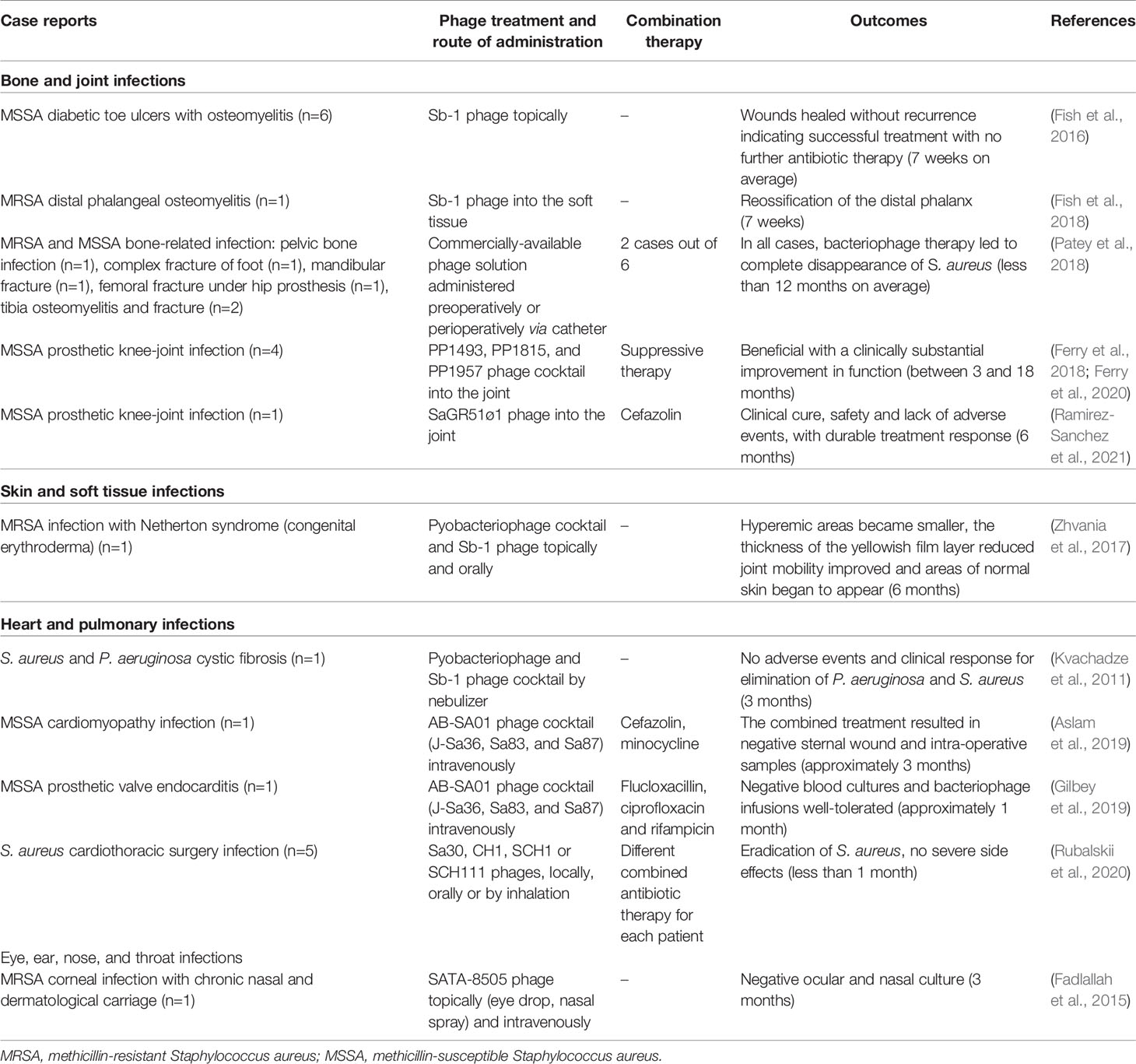
Table 2 Summary of recent published clinical reports of phage therapy in humans.
The rising number of patients with bone and join infections requiring extended antibiotic medication increases the risk of multidrug-resistant organism infection (Osmon et al., 2013; Schmitt, 2017). 10 to 20% of patients with periprosthetic joint infections and fracture-related infections experience treatment failure, and an even higher complication rate of 28% has been recorded for patients with foot osteomyelitis (Senneville et al., 2011; Barshes et al., 2016). However, there are limited therapeutic alternatives in treatment failure, and amputation is relatively frequent. S. aureus (33 to 43%), Staphylococcus epidermidis (18 to 40%), and Enterococcus species (2.5 to 15%) are the most prevalent causes of these infections (Genevière et al., 2021; Gibb and Hadjiargyrou, 2021).
A commercially available solution of Staphylococcal phage Sb-1 was used in nine patients with diabetic toe ulcers presenting S. aureus-bone and soft tissue infections unresponsive to antibiotic treatment, two of whom had osteomyelitis (Fish et al., 2016). These non-healing wounds with persistent osteomyelitis resolved in around 6 weeks, and a unique application of the Staphylococcal phage solution was shown to be both effective and safe in comparison to existing treatments. Osteomyelitis and cellulitis symptoms recovered promptly, and the ulcers closed without recurrence (Fish et al., 2016).
A subsequent study by the same investigators reported a MSSA diabetic ulcer and a distal phalangeal osteomyelitis in a 63-year-old female (Fish et al., 2018). The bacteriophages were applied once weekly for six weeks, with increasing radiographic reossification of the distal phalanx and reduced erythema and edema that continued to heal after the injection therapy was stopped. Therefore, such phage treatment may be beneficial in treating diabetic foot osteomyelitis (Fish et al., 2018).
Patey et al. (2018) reported multiple cases of phage-treated bone infections. These bone infections ranged from pelvic bone infection, complex foot fracture, jaw fracture, osteosynthesis and fistulized infection, femoral fracture under hip prosthesis, knee prosthesis infection, osteomyelitis of the tibia and operated tibia. Interestingly, phage treatment cured these diseases, and the researchers found that applying bacteriophages locally was safe (Patey et al., 2018).
Ferry et al. described the case of an 80-year-old patient with acute postoperative MSSA infection that was unsuccessfully treated with debridement and antibiotics. An implant retention procedure involving debridement and antibiotics was carried out, followed by injection of a cocktail of Pseudomonas aeruginosa and S. aureus phages into the joint cavity. No clinical evidence of chronic infection was seen 18 months later (Ferry et al., 2018). More recently, Ferry et al. reported a phage therapy during a debridement and implant retention procedure followed by antibiotic treatment on three patients with relapsing S. aureus prosthetic knee infections for whom removal of the implant was not possible (Ferry et al., 2020). After this surgery procedure and joint closure, the surgeon injected a phage cocktail directly into the joint. There was a statistically significant and clinically noteworthy increase in knee function, implying that this technique contributed to the clinical outcomes.
In 2021, Ramirez-Sanchez et al. reported the case of a 61-year-old woman treated with phages to cure a persistent MSSA prosthetic knee-joint infection. The authors noted the safety and effectiveness of their phage therapy administered intravenously and intra-articularly, as well as success using a single lytic phage (Ramirez-Sanchez et al., 2021).
Therefore, considering the bacteriophage antimicrobial efficacy and reports of its successful usage in the treatment of bone and joint infections, the possibility of using phages to develop antibacterial treatments seems promising.
Infection of the epidermis, dermis, subcutaneous tissue, superficial fascia, or muscles may cause skin and soft tissue infections (SSTIs), which can have a broad variety of symptoms, causative agents, and severity (Ki and Rotstein, 2008). SSTIs have been further complicated due to the emergence of MRSA strains, necessitating the reevaluation of phage therapy.
Zhvania et al. (2017) reported the case of a 16-year-old boy with classic Netherton syndrome, an autosomal recessive illness including congenital ichthyosiform erythroderma, trichorrhexis invaginatus, and atopic diathesis, often associated with bacterial infections (Altman and Stroud, 1969; Zhvania et al., 2017). The patient presented atopic diathesis and recurring major staphylococcal infections as well as allergy to several medications. All treatments had been exhausted (Zhvania et al., 2017). Within 7 days of therapy with pyobacteriophage and Sb-1 phage cocktail solutions applied externally, in both liquid and cream forms, or as oral medication, this patient experienced considerable health improvement. After 6 months of therapy, his quality of life was greatly improved, and he continued the use phage at home (Zhvania et al., 2017). Therefore, phage therapy could be an effective therapeutic option for treating chronic infection for patients with recurrent infections.
Patients who have had cardiothoracic surgery are at high risk of life-threatening infections, and deaths after surgery are significantly influenced by surgical site infections. Implant-associated infections frequently become chronic because bacteria on implant surfaces tend to develop biofilms that are extremely resistant to antibiotics. S. aureus is one of the most common pathogens associated with infective endocarditis and its frequency has been growing in recent years (Asgeirsson et al., 2018).
Aslam et al. (2019), used phage therapy for the first time as an adjuvant to antibiotics to treat left ventricular assist device infection (Aslam et al., 2019). S. aureus device infection in a 65-year-old male patient with nonischemic cardiomyopathy led to numerous hospitalizations, surgical debridements, and long-term injectable antibiotics. This patient’s continuing recurrent infections disqualified him for heart transplant. Anti-staphylococcal phage cocktail AB-SA01 was administered intravenously every 12h for 28 days, along with cefazolin every 8h and minocycline twice daily orally. The patient’s condition improved, and his sternal cultures were negative for MSSA at the end of the first week and throughout the rest of the treatment. This approach resulted in less purulence and healthier granulation tissue in the wound. Therefore, this patient could be transplanted and 7 months later was in good health with no return of infection.
Gilbey et al. (2019) recently reported the success of the first intravenous use of the staphylococcal phage cocktail ABSA01 for treating severe staphylococcal sepsis with prosthetic valve endocarditis (Gilbey et al., 2019). S. aureus-induced infectious endocarditis has a high mortality rate (Asgeirsson et al., 2018). A 65-year-old man with a mechanical aortic valve suffered from persistent MSSA infection on his implant. The patient recovered with AB-SA01 phage cocktail injection intravenously twice a day for 14 days in combination with antibiotics. After receiving bacteriophage infusions, no fever, tachycardia, hypotension, or rashes were seen, and no adverse sequelae were associated with the treatment.
Rubalskii et al. (2020) described a series of cases in which multi-drug-resistant or persistent infections linked with implants or transplants were effectively treated with different bacteriophages (Rubalskii et al., 2020). They developed a novel technique of individualized phage therapy in conjunction with fibrin glue composed of fibrinogen and thrombin and used a hemostat, sealant, and tissue adhesive. Phage suspension was used as a nontoxic matrix and surgically administered, allowing infected areas to receive phages for an extended period of time. Infections were completely eradicated in 7/8 patients, and there were no serious adverse side effects reported. Therefore, this innovative phage treatment method, when combined with standard antibiotic therapy, may successfully cure S. aureus or other bacterial infections associated with cardiothoracic surgery when conventional antibiotic therapy fails.
Lung infections are particularly difficult to treat in cystic fibrosis patients, where S. aureus colonizes the lungs, and despite treatment with antibiotics results in recurrent and relapsing infections (Goerke and Wolz, 2010). Phage administered by nebulizer to a 7-year-old girl with cystic fibrosis demonstrated favorable clinical outcome (Kvachadze et al., 2011). She had a long-term lung infection with P. aeruginosa and S. aureus, and had taken broad spectrum antibiotics for many years, with little impact on the bacterial invasion. The phage therapy was given nine times by nebulizer with a 4- to 6-weeks interval between each phage treatment. The proportion of P. aeruginosa fell dramatically after the first phage treatment, but the S. aureus load was not influenced. Therefore, Sb-1 was added, a well-studied staphylococcal phage with strong in vitro lytic efficacy against the patient’s colonizing bacterial strains. Following the application of this mix, the quantity of S. aureus was significantly reduced, remained low, without adverse effects. Notably, after several months of treatment, the bacterial level remained below the detection threshold, and antibiotics were reduced.
S. aureus is a primary pathogen in bacterial keratitis, a condition that may cause permanent visual impairment (Schaefer et al., 2001). Fadlallah et al. (2015) described the case of a 65-year-old woman with a corneal ulcer with interstitial keratitis in her left eye (Fadlallah et al., 2015). The patient accepted phage therapy at the Phage Therapy Center (Tbilisi, Georgia) using the S. aureus bacteriophage SATA-8505 after having experienced persistent nasal, dermatological, and ocular vancomycin-intermediate S. aureus (VISA) infection for 11 years. The patient received topical (eye drops and nasal spray) and systemic (intravenous) phage therapy treatment for 4 weeks. After 3 months, normal ocular and nasal cultures were verified, indicating eradication of the infection. Therefore, this case suggests that phage eye-drops combined to systemic phage administration may be an interesting therapeutic option for the treatment of infectious keratitis related to antibiotic-resistant S. aureus infections.
Beyond compassionate circumstances, the major obstacle to phage treatment is the lack of laws and policies around therapeutic application and deployment. Furthermore, the lack of clinical trials hampers the development of phage. Clinical trial methodology for phage treatment is similar to classical medication clinical trial design (Payne and Jansen, 2003). Only a few past and on-going clinical trials involving monotherapy or combination therapy approaches towards S. aureus-related infections have been described, as detailed in Table 3.

Table 3 Clinical trials of S. aureus phage therapy.
The first small phase I clinical trial was of a phage cocktail (WPP-201) in patients with venous leg ulcers (VLUs) with or without current symptoms of infection (Rhoads et al., 2009). The cocktail of bacteriophages tested was designed to selectively target particular members of the wound bacterial population, corresponding to P. aeruginosa, S. aureus, and E. coli, to enhance wound healing. Of the 42 patients with VLUs included, 39 completed the study successfully, while 3 dropped out. The ulcers were treated for 12 weeks with either saline or phages solution, with follow-up until 24 weeks. There were no serious side effects linked to the trial, and no statistical difference between the test and control groups for the number of side effects, the pace or frequency of healing. Therefore, the use of this phage cocktail therapy was found to be successful and safe. This cocktail now needs to be tested in phase II efficacy research with a larger sample size.
Infections with S. aureus are linked with persistent chronic rhinosinusitis (CRS). In a phase 1 trial, Ooi et al. (2019) studied the effectiveness and safety of an increasing dosage of the phage cocktail AB-SA01 administered intranasally to nine patients with CRS testing positive for S. aureus (Ooi et al., 2019). Three groups (with three patients per dose) were treated with AB-SA01 twice a day. The intranasal phage therapy was well tolerated, with no fatalities recorded in any of the groups. Eradication of infection was observed in two of nine patients indicating that the treatment was effective. This study confirmed that phage therapy might be used as a substitute to antibiotics in the treatment of people suffering from CRS. However, further research must be conducted to discover the appropriate dose and verify the effectiveness of AB-SA01 in a randomized trial.
Other phage trials are on-going, as detailed in Table 3. These studies include testing the effectiveness of phage treatment in preventing operation in individuals with hip/knee prosthetic joint infections; or tolerability of phage cocktail SPK as an adjuvant to conventional therapy for the management and cure of burns. Another study aims to evaluate the effectiveness of conventional therapy combined with a topical anti-staphylococcal phage cocktail to usual care in the treatment of acute and chronic ulcers infected by MRSA or MSSA.
This review emphasized the importance of phage therapy in the treatment of S. aureus-related infections and detailed the studies already performed, ranging from case reports to clinical trials, as well as the development of various animal models. Antibiotic resistance in S. aureus is increasing at an alarming rate, necessitating alternative therapies. Phages possess the necessary features for human therapeutic procedures, and progress has been made in testing them in clinical trials and compassionate research investigations. The versatility of phage therapy makes it an excellent choice for integration in complex and multifaceted measures to overcome staphylococcal infections. A high effectiveness level towards different strains of S. aureus, including MRSA, was shown in many of the studies. They were safe, as evidenced by the lack of adverse effects in most investigations. Despite the fact that numerous doses, phage delivery methods, and infection models were used in the trials, no negative side results were noted. Interestingly, these investigations showed that the antibacterial effect may be increased by improving phage administration, the use of phage cocktails, or combining them with antibiotics, as well as, using them in preventive treatments. Moreover, it is also necessary to have reglemented phage production processes, whether they are single or phage cocktails, in order to ensure their safe clinical use as the effectiveness of phage therapy is dependent in large part on maintaining phage stability and reducing immune reaction from the manufacturing process to the administration. The development of the purification procedures for the delivered phages will improve their safety, so minimising side effects and immune response. Interestingly, it is possible to prepare phage cocktails and utilise them in succession in the event of phage resistance. However, the notion of phage cocktail has been questioned, notably by the Phagoburn clinical trial on P. aeruginosa burn-related infections (Jault et al., 2019). Although, the use of a preassembled cocktail was required for PhagoBurn, stability issues associated with such a complex product caused differing opinions among industry experts and active regulatory agencies (ANSM, AFMPS, European Medicines Agency, and the United States Food and Drug Administration). Another clinical trial intended to illustrate the potentials of a novel kind of treatment for paediatric diarrhoea, which is a significant cause of morbidity and fatalities in Bangladesh and other poor countries (Sarker et al., 2016). The purpose of this randomised, double-blind, placebo-controlled study was to assess the efficacy of orally delivered E. coli phage in children between the ages of 4 and 60 months old who have been clinically diagnosed with enterohemorrhagic diarrhoea. Oral coliphages demonstrated a safe gut transit in children, but they were unable to improve diarrhoea outcomes (Sarker et al., 2016). Another randomised controlled trial after a pilot phase was conducted, where the purpose was to assess the effectiveness of intravesical bacteriophage therapy to normalise urine culture in comparison to intravesical placebo or conventional antibiotic treatment. In terms of effectiveness and safety, intravenous bacteriophage therapy was not inferior to the standard-of-care antibiotic treatment for the treatment of urinary tract infections (UTIs), though it was not superior to the placebo bladder irrigation treatment (Leitner et al., 2021).
The emergence of bacterial resistance to bacteriophages is a possibility, since bacteria already possess or have the capacity to evolve a variety of mechanisms for preventing viral infections (Seed, 2015). For instance, the S. aureus protein A located on the bacterial surface inhibits the adsorption of bacteriophages (Nordström and Forsgren, 1974). Antibiotic association with bacteriophages, the use of phage cocktails, or the delivery of a higher initial phage inoculum, may help to minimise the development of bacterial resistance to bacteriophages. If bacteriophages kill pathogens more quickly than they can reproduce, the used of a large inoculum is associated with less risk of the emergence of phage-resistant bacteria. Therefore, when selecting therapeutic phages, consideration should be given to the capacity of each phage to create bacterial resistance as well as estimating the dose required to prevent the formation of bacterial resistance.
Moreover, the immunogenicity of phages, which is the ability of phages to trigger particular immune responses that result in the generation of specific antibodies against phage antigens, is another crucial factor to consider. Phage immunogenicity in humans is a subject on which there are limited and conflicting opinions. Importantly, certain clinical findings suggest that the immunogenicity of phages varies greatly depending on the phage type, dosage, mode of administration, as well as the immunological condition of the host. In general, there was no clear relationship between the effectiveness of phage therapy and the presence of antiphage antibodies (Bruttin and Brüssow, 2005; Łusiak-Szelachowska et al., 2014; Żaczek et al., 2016; Łusiak-Szelachowska et al., 2017). More specifically to S. aureus, the dynamics of phage immunogenicity was investigated in a mouse model in which phages remained in the blood flow for 21–25 days and, despite the existence of antibodies against phages, these antibodies were unable to neutralise the phage-antibacterial activity (Capparelli et al., 2007).
Because this area of research is quickly progressing, some concerns need to be resolved, and research in animals represents one of the solutions. The animal research reviewed here suggested that phage treatment can be effective in a variety of S. aureus infection models, and established their safety. However, the development of animal models remains necessary. Therapy effectiveness can be established in invertebrate and vertebrate models less expensively, and more quickly than human trials and are ethically acceptable. Novel models could be considered for the future, such as the zebrafish, which is gaining popularity for studying host-pathogen interactions (Torraca and Mostowy, 2018; Rasheed et al., 2021). In addition to a mature innate immune system, zebrafish embryos are genetically similar to human, and their transparency make them ideal for investigating characteristics of infection mechanisms unreachable in standard animal models. Very recently, several zebrafish studies have been published for evaluating phage treatment upon bacterial infections, though none have studied S. aureus (Easwaran et al., 2017; Johansen et al., 2021; Sundaramoorthy et al., 2021). Bacteria can be injected into the embryo’s bloodstream alongside phages, and this treatment was effective with a better survival of the infected zebrafish embryos. Therefore, the use of lower vertebrates like zebrafish presents numerous benefits, including cheaper costs and shorter experiments.
Another important issue about S. aureus phage treatment is the lack of real clinical trials for S. aureus infections. More particularly, no randomized double-blind trials have been performed. The known treatments rely essentially on case reports or small clinical trial series. Moreover, despite our understanding of phages’ antimicrobial properties in vitro, we have limited data about their activities in vivo, particularly though clinical trials, and more data are required for their use in healthcare situations. Two recent reviews evaluating phage therapy against multidrug-resistant bacteria, including S. aureus, highlighted the importance of policies and regulations, as well as standardisation, at the national level, that would facilitate the incorporation of phages into clinical practises in the future (Cafora et al., 2019; El Haddad et al., 2019; AL-Ishaq et al., 2021; Al-Zubidi et al., 2019; Assafiri et al., 2021).
Furthermore, future studies are needed to evaluate if phages should be used alone, in cocktail, or in combination with antibiotics. Due to the possible synergistic impact of combination treatment demonstrated in some studies, it has the potential to be employed in clinical settings to effectively treat and prevent or minimise the development of bacterial resistance. We reviewed nine papers that determined the effects of combination antibiotics and phage treatment on a variety of different outcomes (Table 1). For the most part, the therapeutic result of combination therapy for S. aureus infections was synergistic, with a substantial increase in survival or a decrease in bacterial load concentration being seen in the majority of investigations. This demonstrates that the method of delivery, the dose, and even the antibiotic used may all have an impact on the effectiveness of a treatment. Together, these data support the notion that bacteriophage treatment does not intend to supplant antibiotics, but rather that it may be very effective when used in conjunction with antibiotics to treat S. aureus infections. However, there are only a few publications available, and further studies are needed to completely understand the treatment dynamics in combination therapy to be effectively employed in clinical practise.
In addition, the dose and mode of administration of bacteriophage treatment are the most important factors in achieving a satisfactory outcome. It is noteworthy to mention that phages were supplied by a variety of methods in the studies reviewed above, including subcutaneously, intraperitoneally, intravenously, intranasally, injection into the hindpaw or the joint, local topical application, and intramuscularly. As a result, choosing the most suitable course of administration method is dependent on the model and type of infection as well as the place of infection. Although there has been some progress, there is still a significant gap in knowledge about the application, feasibility, and safety of the various administration routes in humans.
Bacteriophage treatment is regarded as a highly individualised method, with each patient’s infections being targeted specifically. As a result, phages are a personalised therapeutic product that is tailored to the specific needs of each individual patient rather than a universal medical treatment. Therefore, the phagogram for each patient will become indispensable for a better personalised phage treatment, which must be feasible and interpretable like an antibiogram. Also, understanding of phage pharmacology is required for its use in healthcare situations. It is possible that the pharmacokinetics of the phage (uptake and delivery within the body) and the pharmacodynamics of the phage (toxic effects, adverse reactions, reduction of bacterial growth) will impact the outcome of phage therapy and that these aspects should be investigated further for phages that are destined to clinical usages (Payne and Jansen, 2003). To date, no such investigations were reported in the publications reviewed and will need to be addressed.
As a result of the growing issue of S. aureus antibiotic resistance around the globe, phage treatment seems to be an effective and safe therapy for fighting bacterial resistance. Some limits, on the other hand, may be identified. First and foremost, there is a lack of research that would thoroughly analyse the safety and effectiveness of phage treatment. A further limitation of the current literature is the absence of an established and regulated protocol for phage extraction and purification that leads to differences in the outcomes of the different studies reported. Finally, further research to characterize the host immune response dynamics upon treatment is required to assure that phage therapy is successful.
In conclusion, phage treatment has the potential to be important for protecting people from S. aureus infections in the future if a systemic strategy towards effectiveness and safety is developed in order to stimulate phage therapy development and acceptability as a treatment alternative.
LP and VM: conceptualization, writing. LP, NA-M, DC and VM: data curation. LP, NA-M, J-PL, DC and VM: writing – original draft preparation. LP, NA-M, CD-R, AS, J-PL, DC and VM: writing – review and editing. DC, J-PL and VM: supervision, resources, and funding acquisition. All authors contributed to the article and approved the submitted version.
This study was supported by the University Hospital of Nîmes, and the Greenphage SAS.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank Sarah Kabani for her editing assistance.
Abedon, S. T. (2016). Commentary: Phage Therapy of Staphylococcal Chronic Osteomyelitis in Experimental Animal Model. Front. Microbiol. 7. doi: 10.3389/fmicb.2016.01251
Abu Lila, A. S., Ishida, T. (2017). Liposomal Delivery Systems: Design Optimization and Current Applications. Biol. Pharm. Bull. 40, 1–10. doi: 10.1248/bpb.b16-00624
Albac, S., Medina, M., Labrousse, D., Hayez, D., Bonnot, D., Anzala, N., et al. (2020). Efficacy of Bacteriophages in a Staphylococcus aureus Nondiabetic or Diabetic Foot Infection Murine Model. Antimicrob. Agents Chemother. 64, e01870–e01819. doi: 10.1128/AAC.01870-19
AL-Ishaq, R. K., Skariah, S., Büsselberg, D. (2021). Bacteriophage Treatment: Critical Evaluation of Its Application on World Health Organization Priority Pathogens. Viruses 13, 51. doi: 10.3390/v13010051
Altman, J., Stroud, J. (1969). Neterton’s Syndrome and Ichthyosis Linearis Circumflexa. Arch. Dermatol. 100, 550–558. doi: 10.1001/archderm.1969.01610290034007
Al-Zubidi, M., Widziolek, M., Court, E. K., Gains, A. F., Smith, R. E., Ansbro, K., et al. (2019). Identification of Novel Bacteriophages With Therapeutic Potential That Target Enterococcus faecalis. Infect. Immun. 87, e00512–e00519. doi: 10.1128/IAI.00512-19
Asgeirsson, H., Thalme, A., Weiland, O. (2018). Staphylococcus aureus Bacteraemia and Endocarditis - Epidemiology and Outcome: A Review. Infect. Dis. (Lond) 50, 175–192. doi: 10.1080/23744235.2017.1392039
Aslam, S., Pretorius, V., Lehman, S. M., Morales, S., Schooley, R. T. (2019). Novel Bacteriophage Therapy for Treatment of Left Ventricular Assist Device Infection. J. Heart Lung Transplant. 38, 475–476. doi: 10.1016/j.healun.2019.01.001
Asokan, G. V., Ramadhan, T., Ahmed, E., Sanad, H. (2019). WHO Global Priority Pathogens List: A Bibliometric Analysis of Medline-PubMed for Knowledge Mobilization to Infection Prevention and Control Practices in Bahrain. Oman Med. J. 34, 184–193. doi: 10.5001/omj.2019.37
Assafiri, O., Song, A. A.-L., Tan, G. H., Hanish, I., Hashim, A. M., Yusoff, K. (2021). Klebsiella Virus UPM2146 Lyses Multiple Drug-Resistant Klebsiella pneumoniae In Vitro and In Vivo. PloS One 16, e0245354. doi: 10.1371/journal.pone.0245354
Barshes, N. R., Mindru, C., Ashong, C., Rodriguez-Barradas, M., Trautner, B. W. (2016). Treatment Failure and Leg Amputation Among Patients With Foot Osteomyelitis. Int. J. Low Extrem. Wounds 15, 303–312. doi: 10.1177/1534734616661058
Brix, A., Cafora, M., Aureli, M., Pistocchi, A. (2020). Animal Models to Translate Phage Therapy to Human Medicine. Int. J. Mol. Sci. 21, 3715. doi: 10.3390/ijms21103715
Bruttin, A., Brüssow, H. (2005). Human Volunteers Receiving Escherichia Coli Phage T4 Orally: A Safety Test of Phage Therapy. Antimicrob. Agents Chemother. 49, 2874–2878. doi: 10.1128/AAC.49.7.2874-2878.2005
Bull, J. J., Levin, B. R., DeRouin, T., Walker, N., Bloch, C. A. (2002). Dynamics of Success and Failure in Phage and Antibiotic Therapy in Experimental Infections. BMC Microbiol. 2, 35. doi: 10.1186/1471-2180-2-35
Cafora, M., Deflorian, G., Forti, F., Ferrari, L., Binelli, G., Briani, F., et al. (2019). Phage Therapy Against Pseudomonas aeruginosa Infections in a Cystic Fibrosis Zebrafish Model. Sci. Rep. 9, 1527. doi: 10.1038/s41598-018-37636-x
Capparelli, R., Parlato, M., Borriello, G., Salvatore, P., Iannelli, D. (2007). Experimental Phage Therapy Against Staphylococcus aureus in Mice. Antimicrobial. Agents Chemother 51, 2765–2773. doi: 10.1128/AAC.01513-06
Chan, B. K., Abedon, S. T., Loc-Carrillo, C. (2013). Phage Cocktails and the Future of Phage Therapy. Future Microbiol. 8, 769–783. doi: 10.2217/fmb.13.47
Chanishvili, N. (2012). Phage Therapy–History From Twort and D’Herelle Through Soviet Experience to Current Approaches. Adv. Virus Res. 83, 3–40. doi: 10.1016/B978-0-12-394438-2.00001-3
Chhibber, S., Kaur, T., Kaur, S. (2013). Co-Therapy Using Lytic Bacteriophage and Linezolid: Effective Treatment in Eliminating Methicillin Resistant Staphylococcus aureus (MRSA) From Diabetic Foot Infections. PloS One 8, e56022. doi: 10.1371/journal.pone.0056022
Chhibber, S., Shukla, A., Kaur, S. (2017). Transfersomal Phage Cocktail Is an Effective Treatment Against Methicillin-Resistant Staphylococcus aureus-Mediated Skin and Soft Tissue Infections. Antimicrob. Agents Chemother. 61. doi: 10.1128/AAC.02146-16
Cieślik, M., Bagińska, N., Górski, A., Jończyk-Matysiak, E. (2021). Animal Models in the Evaluation of the Effectiveness of Phage Therapy for Infections Caused by Gram-Negative Bacteria From the ESKAPE Group and the Reliability of Its Use in Humans. Microorganisms 9, 206. doi: 10.3390/microorganisms9020206
Cohen, L. B., Troemel, E. R. (2015). Microbial Pathogenesis and Host Defense in the Nematode C. Elegans. Curr. Opin. Microbiol. 23, 94–101. doi: 10.1016/j.mib.2014.11.009
Easwaran, M., Dananjaya, S. H. S., Park, S. C., Lee, J., Shin, H.-J., De Zoysa, M. (2017). Characterization of Bacteriophage pAh-1 and Its Protective Effects on Experimental Infection of Aeromonas Hydrophila in Zebrafish (Danio Rerio). J. Fish Dis. 40, 841–846. doi: 10.1111/jfd.12536
El Haddad, L., Harb, C. P., Gebara, M. A., Stibich, M. A., Chemaly, R. F. (2019). A Systematic and Critical Review of Bacteriophage Therapy Against Multidrug-Resistant ESKAPE Organisms in Humans. Clin. Infect. Dis. 69, 167–178. doi: 10.1093/cid/ciy947
Ewbank, J. J., Zugasti, O. (2011). C. Elegans: Model Host and Tool for Antimicrobial Drug Discovery. Dis. Model. Mech. 4, 300–304. doi: 10.1242/dmm.006684
Fadlallah, A., Chelala, E., Legeais, J.-M. (2015). Corneal Infection Therapy With Topical Bacteriophage Administration. TOOPHTJ 9, 167–168. doi: 10.2174/1874364101509010167
Febvre, H. P., Rao, S., Gindin, M., Goodwin, N. D. M., Finer, E., Vivanco, J. S., et al. (2019). PHAGE Study: Effects of Supplemental Bacteriophage Intake on Inflammation and Gut Microbiota in Healthy Adults. Nutrients 11, E666. doi: 10.3390/nu11030666
Ferry, T., Kolenda, C., Batailler, C., Gustave, C.-A., Lustig, S., Malatray, M., et al. (2020). Phage Therapy as Adjuvant to Conservative Surgery and Antibiotics to Salvage Patients With Relapsing S. aureus Prosthetic Knee Infection. Front. Med. (Lausanne) 7. doi: 10.3389/fmed.2020.570572
Ferry, T., Leboucher, G., Fevre, C., Herry, Y., Conrad, A., Josse, J., et al. (2018). Salvage Debridement, Antibiotics and Implant Retention (“DAIR”) With Local Injection of a Selected Cocktail of Bacteriophages: Is It an Option for an Elderly Patient With Relapsing Staphylococcus aureus Prosthetic-Joint Infection? Open Forum Infect. Dis. 5, ofy269. doi: 10.1093/ofid/ofy269
Fish, R., Kutter, E., Bryan, D., Wheat, G., Kuhl, S. (2018). Resolving Digital Staphylococcal Osteomyelitis Using Bacteriophage-A Case Report. Antibiot. (Basel) 7, E87. doi: 10.3390/antibiotics7040087
Fish, R., Kutter, E., Wheat, G., Blasdel, B., Kutateladze, M., Kuhl, S. (2016). Bacteriophage Treatment of Intransigent Diabetic Toe Ulcers: A Case Series. J. Wound Care 25, 7. doi: 10.12968/jowc.2016.25.Sup7.S27
Fujiyuki, T., Imamura, K., Hamamoto, H., Sekimizu, K. (2010). Evaluation of Therapeutic Effects and Pharmacokinetics of Antibacterial Chromogenic Agents in a Silkworm Model of Staphylococcus aureus Infection. Drug Discovery Ther. 4, 349–354.
Genevière, J., McCallin, S., Huttner, A., Pham, T.-T., Suva, D. (2021). A Systematic Review of Phage Therapy Applied to Bone and Joint Infections: An Analysis of Success Rates, Treatment Modalities and Safety. EFORT Open Rev. 6, 1148–1156. doi: 10.1302/2058-5241.6.210073
Gibb, B. P., Hadjiargyrou, M. (2021). Bacteriophage Therapy for Bone and Joint Infections. Bone Joint J. 103-B, 234–244. doi: 10.1302/0301-620X.103B2.BJJ-2020-0452.R2
Gilbey, T., Ho, J., Cooley, L. A., Petrovic Fabijan, A., Iredell, J. R. (2019). Adjunctive Bacteriophage Therapy for Prosthetic Valve Endocarditis Due to Staphylococcus aureus. Med. J. Aust. 211, 142–143.e1. doi: 10.5694/mja2.50274
Glowacka-Rutkowska, A., Gozdek, A., Empel, J., Gawor, J., Żuchniewicz, K., Kozińska, A., et al. (2019). The Ability of Lytic Staphylococcal Podovirus Vb_SauP_phiAGO1.3 to Coexist in Equilibrium With Its Host Facilitates the Selection of Host Mutants of Attenuated Virulence But Does Not Preclude the Phage Antistaphylococcal Activity in a Nematode Infection Model. Front. Microbiol. 9. doi: 10.3389/fmicb.2018.03227
Goerke, C., Wolz, C. (2010). Adaptation of Staphylococcus aureus to the Cystic Fibrosis Lung. Int. J. Med. Microbiol. 300, 520–525. doi: 10.1016/j.ijmm.2010.08.003
Huon, J.-F., Montassier, E., Leroy, A.-G., Grégoire, M., Vibet, M.-A., Caillon, J., et al. (2020). Phages Versus Antibiotics To Treat Infected Diabetic Wounds in a Mouse Model: A Microbiological and Microbiotic Evaluation. mSystems 5, e00542–20. doi: 10.1128/mSystems.00542-20
Jault, P., Leclerc, T., Jennes, S., Pirnay, J. P., Que, Y.-A., Resch, G., et al. (2019). Efficacy and Tolerability of a Cocktail of Bacteriophages to Treat Burn Wounds Infected by Pseudomonas aeruginosa (PhagoBurn): A Randomised, Controlled, Double-Blind Phase 1/2 Trial. Lancet Infect. Dis. 19, 35–45. doi: 10.1016/S1473-3099(18)30482-1
Johansen, M. D., Alcaraz, M., Dedrick, R. M., Roquet-Banères, F., Hamela, C., Hatfull, G. F., et al. (2021). Mycobacteriophage–antibiotic Therapy Promotes Enhanced Clearance of Drug-Resistant Mycobacterium abscessus. Dis. Models Mech. 14, dmm049159. doi: 10.1242/dmm.049159
Kaito, C., Akimitsu, N., Watanabe, H., Sekimizu, K. (2002). Silkworm Larvae as an Animal Model of Bacterial Infection Pathogenic to Humans. Microb. Pathog. 32, 183–190. doi: 10.1006/mpat.2002.0494
Kaito, C., Sekimizu, K. (2007). A Silkworm Model of Pathogenic Bacterial Infection. Drug Discov. Ther. 1, 89–93.
Kaur, S., Harjai, K., Chhibber, S. (2016). In Vivo Assessment of Phage and Linezolid Based Implant Coatings for Treatment of Methicillin Resistant S. aureus (MRSA) Mediated Orthopaedic Device Related Infections. PloS One 11, e0157626. doi: 10.1371/journal.pone.0157626
Kifelew, L. G., Warner, M. S., Morales, S., Vaughan, L., Woodman, R., Fitridge, R., et al. (2020). Efficacy of Phage Cocktail AB-SA01 Therapy in Diabetic Mouse Wound Infections Caused by Multidrug-Resistant Staphylococcus aureus. BMC Microbiol. 20, 204. doi: 10.1186/s12866-020-01891-8
Ki, V., Rotstein, C. (2008). Bacterial Skin and Soft Tissue Infections in Adults: A Review of Their Epidemiology, Pathogenesis, Diagnosis, Treatment and Site Of Care. Can. J. Infect. Dis. Med. Microbiol. 19, 173–184. doi: 10.1155/2008/846453
Kishor, C., Mishra, R. R., Saraf, S. K., Kumar, M., Srivastav, A. K., Nath, G. (2016). Phage Therapy of Staphylococcal Chronic Osteomyelitis in Experimental Animal Model. Indian J. Med. Res. 143, 87–94. doi: 10.4103/0971-5916.178615
Kortright, K. E., Chan, B. K., Koff, J. L., Turner, P. E. (2019). Phage Therapy: A Renewed Approach to Combat Antibiotic-Resistant Bacteria. Cell Host Microbe 25, 219–232. doi: 10.1016/j.chom.2019.01.014
Kurokawa, K., Kaito, C., Sekimizu, K. (2007). Two-Component Signaling in the Virulence of Staphylococcus aureus: A Silkworm Larvae-Pathogenic Agent Infection Model of Virulence. Methods Enzymol. 422, 233–244. doi: 10.1016/S0076-6879(06)22011-1
Kvachadze, L., Balarjishvili, N., Meskhi, T., Tevdoradze, E., Skhirtladze, N., Pataridze, T., et al. (2011). Evaluation of Lytic Activity of Staphylococcal Bacteriophage Sb-1 Against Freshly Isolated Clinical Pathogens: Staphylococcal Bacteriophages Sb-1. Microbial. Biotechnol. 4, 643–650. doi: 10.1111/j.1751-7915.2011.00259.x
Lehman, S. M., Mearns, G., Rankin, D., Cole, R. A., Smrekar, F., Branston, S. D., et al. (2019). Design and Preclinical Development of a Phage Product for the Treatment of Antibiotic-Resistant Staphylococcus aureus Infections. Viruses 11, 88. doi: 10.3390/v11010088
Leitner, L., Ujmajuridze, A., Chanishvili, N., Goderdzishvili, M., Chkonia, I., Rigvava, S., et al. (2021). Intravesical Bacteriophages for Treating Urinary Tract Infections in Patients Undergoing Transurethral Resection of the Prostate: A Randomised, Placebo-Controlled, Double-Blind Clinical Trial. Lancet Infect. Dis. 21, 427–436. doi: 10.1016/S1473-3099(20)30330-3
Lipsky, B. A., Senneville, É., Abbas, Z. G., Aragón-Sánchez, J., Diggle, M., Embil, J. M., et al. (2020). Guidelines on the Diagnosis and Treatment of Foot Infection in Persons With Diabetes (IWGDF 2019 Update). Diabetes Metab. Res. Rev. 36 Suppl 1, e3280. doi: 10.1002/dmrr.3280
Lord, J., Gikonyo, A., Miwa, A., Odoi, A. (2021). Antimicrobial Resistance Among Enterobacteriaceae, Staphylococcus aureus, and Pseudomonas Spp. Isolates From Clinical Specimens From a Hospital in Nairobi, Kenya. PeerJ 9, e11958. doi: 10.7717/peerj.11958
Lowy, F. D. (1998). Staphylococcus aureus Infections. N. Engl. J. Med. 339, 520–532. doi: 10.1056/NEJM199808203390806
Luong, T., Salabarria, A.-C., Roach, D. R. (2020). Phage Therapy in the Resistance Era: Where Do We Stand and Where Are We Going? Clin. Ther. 42, 1659–1680. doi: 10.1016/j.clinthera.2020.07.014
Łusiak-Szelachowska, M., Żaczek, M., Weber-Dąbrowska, B., Międzybrodzki, R., Kłak, M., Fortuna, W., et al. (2014). Phage Neutralization by Sera of Patients Receiving Phage Therapy. Viral Immunol. 27, 295–304. doi: 10.1089/vim.2013.0128
Łusiak-Szelachowska, M., Żaczek, M., Weber-Dąbrowska, B., Międzybrodzki, R., Letkiewicz, S., Fortuna, W., et al. (2017). Antiphage Activity of Sera During Phage Therapy in Relation to Its Outcome. Future Microbiol. 12, 109–117. doi: 10.2217/fmb-2016-0156
Malik, D. J., Sokolov, I. J., Vinner, G. K., Mancuso, F., Cinquerrui, S., Vladisavljevic, G. T., et al. (2017). Formulation, Stabilisation and Encapsulation of Bacteriophage for Phage Therapy. Adv. Colloid. Interface Sci. 249, 100–133. doi: 10.1016/j.cis.2017.05.014
Melo, L. D. R., Oliveira, H., Pires, D. P., Dabrowska, K., Azeredo, J. (2020). Phage Therapy Efficacy: A Review of the Last 10 Years of Preclinical Studies. Crit. Rev. Microbiol. 46, 78–99. doi: 10.1080/1040841X.2020.1729695
Morris, J., Kelly, N., Elliott, L., Grant, A., Wilkinson, M., Hazratwala, K., et al. (2018). Evaluation of Bacteriophage Anti-Biofilm Activity for Potential Control of Orthopedic Implant-Related Infections Caused by Staphylococcus aureus. Surg. Infect. (Larchmt) 20, 16–24. doi: 10.1089/sur.2018.135
Morris, J. L., Letson, H. L., Elliott, L., Grant, A. L., Wilkinson, M., Hazratwala, K., et al. (2019a). Evaluation of Bacteriophage as an Adjunct Therapy for Treatment of Peri-Prosthetic Joint Infection Caused by Staphylococcus aureus. PloS One 14, e0226574. doi: 10.1371/journal.pone.0226574
Morris, J. L., Letson, H. L., Grant, A., Wilkinson, M., Hazratwala, K., McEwen, P. (2019b). Experimental Model of Peri-Prosthetic Infection of the Knee Caused by Staphylococcus aureus Using Biomaterials Representative of Modern TKA. Biol. Open 8, bio045203. doi: 10.1242/bio.045203
Nordström, K., Forsgren, A. (1974). Effect of Protein A on Adsorption of Bacteriophages to Staphylococcus aureus. J. Virol. 14, 198–202. doi: 10.1128/jvi.14.2.198-202.1974
Oduor, J. M. O., Onkoba, N., Maloba, F., Arodi, W. O., Nyachieo, A. (2016). Efficacy of Lytic Staphylococcus aureus Bacteriophage Against Multidrug-Resistant Staphylococcus aureus in Mice. J. Infect. Dev. Ctries 10, 1208–1213. doi: 10.3855/jidc.7931
O’Neill, J. (2016) Tackling Drug-Resistant Infections Globally: Final Report and Recommendations. Available at: https://amr-review.org/sites/default/files/160518_Final%20paper_with%20cover.pdf (Accessed February 18, 2022).
Ooi, M. L., Drilling, A. J., Morales, S., Fong, S., Moraitis, S., Macias-Valle, L., et al. (2019). Safety and Tolerability of Bacteriophage Therapy for Chronic Rhinosinusitis Due to Staphylococcus aureus. JAMA Otolaryngol.–Head Neck Surg. 145, 723–729. doi: 10.1001/jamaoto.2019.1191
Osmon, D. R., Berbari, E. F., Berendt, A. R., Lew, D., Zimmerli, W., Steckelberg, J. M., et al. (2013). Diagnosis and Management of Prosthetic Joint Infection: Clinical Practice Guidelines by the Infectious Diseases Society of America. Clin. Infect. Dis. 56, e1–e25. doi: 10.1093/cid/cis803
Patey, O., McCallin, S., Mazure, H., Liddle, M., Smithyman, A., Dublanchet, A. (2018). Clinical Indications and Compassionate Use of Phage Therapy: Personal Experience and Literature Review With a Focus on Osteoarticular Infections. Viruses 11, E18. doi: 10.3390/v11010018
Payne, R. J. H., Jansen, V. A. A. (2003). Pharmacokinetic Principles of Bacteriophage Therapy. Clin. Pharmacokinet. 42, 315–325. doi: 10.2165/00003088-200342040-00002
Penziner, S., Schooley, R. T., Pride, D. T. (2021). Animal Models of Phage Therapy. Front. Microbiol. 12. doi: 10.3389/fmicb.2021.631794
Pouget, C., Dunyach-Remy, C., Pantel, A., Boutet-Dubois, A., Schuldiner, S., Sotto, A., et al. (2021). Alternative Approaches for the Management of Diabetic Foot Ulcers. Front. Microbiol. 12. doi: 10.3389/fmicb.2021.747618
Prazak, J., Iten, M., Cameron, D. R., Save, J., Grandgirard, D., Resch, G., et al. (2019). Bacteriophages Improve Outcomes in Experimental Staphylococcus aureus Ventilator-Associated Pneumonia. Am. J. Respir. Crit. Care Med. 200, 1126–1133. doi: 10.1164/rccm.201812-2372OC
Prazak, J., Valente, L. G., Iten, M., Federer, L., Grandgirard, D., Soto, S., et al. (2022). Benefits of Aerosolized Phages for the Treatment of Pneumonia Due to Methicillin-Resistant Staphylococcus aureus: An Experimental Study in Rats. J. Infect. Dis. 225, 1452–1459. doi: 10.1093/infdis/jiab112
Principi, N., Silvestri, E., Esposito, S. (2019). Advantages and Limitations of Bacteriophages for the Treatment of Bacterial Infections. Front. Pharmacol. 10. doi: 10.3389/fphar.2019.00513
Projan, S. J. (2003). Why is Big Pharma Getting Out of Antibacterial Drug Discovery? Curr. Opin. Microbiol. 6, 427–430. doi: 10.1016/j.mib.2003.08.003
Projan, S. J., Shlaes, D. M. (2004). Antibacterial Drug Discovery: Is It All Downhill From Here? Clin. Microbiol. Infect. 10 Suppl 4, 18–22. doi: 10.1111/j.1465-0691.2004.1006.x
Ramirez-Sanchez, C., Gonzales, F., Buckley, M., Biswas, B., Henry, M., Deschenes, M. V., et al. (2021). Successful Treatment of Staphylococcus aureus Prosthetic Joint Infection With Bacteriophage Therapy. Viruses 13, 1182. doi: 10.3390/v13061182
Rasheed, S., Fries, F., Müller, R., Herrmann, J. (2021). Zebrafish: An Attractive Model to Study Staphylococcus aureus Infection and Its Use as a Drug Discovery Tool. Pharmaceuticals 14, 594. doi: 10.3390/ph14060594
Rhoads, D. D., Wolcott, R. D., Kuskowski, M. A., Wolcott, B. M., Ward, L. S., Sulakvelidze, A. (2009). Bacteriophage Therapy of Venous Leg Ulcers in Humans: Results of a Phase I Safety Trial. J. Wound Care 18, 237–243. doi: 10.12968/jowc.2009.18.6.42801
Rubalskii, E., Ruemke, S., Salmoukas, C., Boyle, E. C., Warnecke, G., Tudorache, I., et al. (2020). Bacteriophage Therapy for Critical Infections Related to Cardiothoracic Surgery. Antibiotics 9, 232. doi: 10.3390/antibiotics9050232
Sarker, S. A., Sultana, S., Reuteler, G., Moine, D., Descombes, P., Charton, F., et al. (2016). Oral Phage Therapy of Acute Bacterial Diarrhea With Two Coliphage Preparations: A Randomized Trial in Children From Bangladesh. EBioMedicine 4, 124–137. doi: 10.1016/j.ebiom.2015.12.023
Save, J., Que, Y., Entenza, J. M., Kolenda, C., Laurent, F., Resch, G. (2022). Bacteriophages Combined With Subtherapeutic Doses of Flucloxacillin Act Synergistically Against Staphylococcus aureus Experimental Infective Endocarditis. J. Am. Heart Assoc. 0, e023080. doi: 10.1161/JAHA.121.023080
Schaefer, F., Bruttin, O., Zografos, L., Guex-Crosier, Y. (2001). Bacterial Keratitis: A Prospective Clinical and Microbiological Study. Br. J. Ophthalmol. 85, 842–847. doi: 10.1136/bjo.85.7.842
Schmitt, S. K. (2017). Osteomyelitis. Infect. Dis. Clin. North Am. 31, 325–338. doi: 10.1016/j.idc.2017.01.010
Seed, K. D. (2015). Battling Phages: How Bacteria Defend Against Viral Attack. PloS Pathog. 11, e1004847. doi: 10.1371/journal.ppat.1004847
Senneville, E., Joulie, D., Legout, L., Valette, M., Dezèque, H., Beltrand, E., et al. (2011). Outcome and Predictors of Treatment Failure in Total Hip/Knee Prosthetic Joint Infections Due to Staphylococcus aureus. Clin. Infect. Dis. 53, 334–340. doi: 10.1093/cid/cir402
Shlaes, D. M., Sahm, D., Opiela, C., Spellberg, B. (2013). The FDA Reboot of Antibiotic Development. Antimicrob. Agents Chemother. 57, 4605–4607. doi: 10.1128/AAC.01277-13
Singh, D., Pradhan, M., Nag, M., Singh, M. R. (2015). Vesicular System: Versatile Carrier for Transdermal Delivery of Bioactives. Artif. Cells Nanomed. Biotechnol. 43, 282–290. doi: 10.3109/21691401.2014.883401
Spellberg, B., Guidos, R., Gilbert, D., Bradley, J., Boucher, H. W., Scheld, W. M., et al. (2008). The Epidemic of Antibiotic-Resistant Infections: A Call to Action for the Medical Community From the Infectious Diseases Society of America. Clin. Infect. Dis. 46, 155–164. doi: 10.1086/524891
Sunagar, R., Patil, S. A., Chandrakanth, R. K. (2010). Bacteriophage Therapy for Staphylococcus aureus Bacteremia in Streptozotocin-Induced Diabetic Mice. Res. Microbiol. 161, 854–860. doi: 10.1016/j.resmic.2010.09.011
Sundaramoorthy, N. S., Thothathri, S., Bhaskaran, M., GaneshPrasad, A., Nagarajan, S. (2021). Phages From Ganges River Curtail In Vitro Biofilms and Planktonic Growth of Drug Resistant Klebsiella pneumoniae in a Zebrafish Infection Model. AMB Express 11, 27. doi: 10.1186/s13568-021-01181-0
Takemura-Uchiyama, I., Uchiyama, J., Kato, S., Inoue, T., Ujihara, T., Ohara, N., et al. (2013). Evaluating Efficacy of Bacteriophage Therapy Against Staphylococcus aureus Infections Using a Silkworm Larval Infection Model. FEMS Microbiol. Lett. 347, 52–60. doi: 10.1111/1574-6968.12220
Takemura-Uchiyama, I., Uchiyama, J., Osanai, M., Morimoto, N., Asagiri, T., Ujihara, T., et al. (2014). Experimental Phage Therapy Against Lethal Lung-Derived Septicemia Caused by Staphylococcus aureus in Mice. Microbes Infect. 16, 512–517. doi: 10.1016/j.micinf.2014.02.011
Torraca, V., Mostowy, S. (2018). Zebrafish Infection: From Pathogenesis to Cell Biology. Trends Cell Biol. 28, 143–156. doi: 10.1016/j.tcb.2017.10.002
Valente, L. G., Federer, L., Iten, M., Grandgirard, D., Leib, S. L., Jakob, S. M., et al. (2021). Searching for Synergy: Combining Systemic Daptomycin Treatment With Localised Phage Therapy for the Treatment of Experimental Pneumonia Due to MRSA. BMC Res. Notes 14, 381. doi: 10.1186/s13104-021-05796-1
Van Belleghem, J. D., Clement, F., Merabishvili, M., Lavigne, R., Vaneechoutte, M. (2017). Pro- and Anti-Inflammatory Responses of Peripheral Blood Mononuclear Cells Induced by Staphylococcus aureus and Pseudomonas aeruginosa Phages. Sci. Rep. 7, 8004. doi: 10.1038/s41598-017-08336-9
Wills, Q. F., Kerrigan, C., Soothill, J. S. (2005). Experimental Bacteriophage Protection Against Staphylococcus aureus Abscesses in a Rabbit Model. Antimicrob. Agents Chemother. 49, 1220–1221. doi: 10.1128/AAC.49.3.1220-1221.2005
Yilmaz, C., Colak, M., Yilmaz, B. C., Ersoz, G., Kutateladze, M., Gozlugol, M. (2013). Bacteriophage Therapy in Implant-Related Infections: An Experimental Study. J. Bone Joint Surg. Am. Vol. 95, 117–125. doi: 10.2106/JBJS.K.01135
Zhvania, P., Hoyle, N. S., Nadareishvili, L., Nizharadze, D., Kutateladze, M. (2017). Phage Therapy in a 16-Year-Old Boy With Netherton Syndrome. Front. Med. 4. doi: 10.3389/fmed.2017.00094
Keywords: Staphylococcus aureus, bacteriophage therapy, case reports, clinical trials, animal models
Citation: Plumet L, Ahmad-Mansour N, Dunyach-Remy C, Kissa K, Sotto A, Lavigne J-P, Costechareyre D and Molle V (2022) Bacteriophage Therapy for Staphylococcus Aureus Infections: A Review of Animal Models, Treatments, and Clinical Trials. Front. Cell. Infect. Microbiol. 12:907314. doi: 10.3389/fcimb.2022.907314
Received: 29 March 2022; Accepted: 23 May 2022;
Published: 17 June 2022.
Edited by:
Ghadir Saied El Housseiny, Ain Shams University, EgyptReviewed by:
Mzia Kutateladze, George Eliava Institute of Bacteriophage, Microbiology and Virology, GeorgiaCopyright © 2022 Plumet, Ahmad-Mansour, Dunyach-Remy, Kissa, Sotto, Lavigne, Costechareyre and Molle. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Virginie Molle, dmlyZ2luaWUubW9sbGVAdW1vbnRwZWxsaWVyLmZy
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.