
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Cell. Infect. Microbiol. , 14 October 2021
Sec. Parasite and Host
Volume 11 - 2021 | https://doi.org/10.3389/fcimb.2021.744163
This article is part of the Research Topic Revisiting the Life Cycle of Parasitic Protozoa View all 10 articles
 Daniel Holanda Barroso1,2,3
Daniel Holanda Barroso1,2,3 Otávio de Toledo Nóbrega1,4
Otávio de Toledo Nóbrega1,4 Carla Nunes de Araújo1
Carla Nunes de Araújo1 Gustavo Subtil Magalhães Freire2
Gustavo Subtil Magalhães Freire2 Sofia Sales Martins2,4
Sofia Sales Martins2,4 Bruna Côrtes Rodrigues1,2
Bruna Côrtes Rodrigues1,2 Ciro Martins Gomes1,2,3,5*†
Ciro Martins Gomes1,2,3,5*† Raimunda Nonata Ribeiro Sampaio1,2,3,4†
Raimunda Nonata Ribeiro Sampaio1,2,3,4†Leishmania braziliensis is the most important causal agent of American tegumentary leishmaniasis (ATL), and 3 to 5% of patients develop mucosal lesions. The mechanisms related to parasite and host immune interactions and the parasite life cycle that lead to dissemination to the mucosa are poorly understood. We aimed to detect L. braziliensis DNA in the nasal mucosa of cutaneous leishmaniasis (CL) patients with early mucous dissemination and to relate those findings to specific inflammatory responses. Nasal swabs were collected from patients with the cutaneous form of ATL. L. braziliensis DNA was investigated using TaqMan-based real-time PCR. The levels of serum cytokines (IL-12, IL-6, TNF-α, IL-10, IL-1β and IL-8) were measured by a multiplex cytometric array. A Poisson regression model was used to test prevalence ratios (PRs) and multivariate interactions of clinical and laboratory characteristics. Of the 79 CL patients, 24 (30%) had L. braziliensis DNA in the nasal mucosa. In the multivariate model, parasite DNA presence in mucosa was associated with a reduction in IL-12 levels (PR = 0.440; p=0.034), increased IL-6 levels (PR = 1.001; p=0.002) and a higher number of affected body segments (PR = 1.65; p<0.001). In this study, we observed a higher rate of early dissemination to the nasal mucosa than what was previously described. We suggest that an enhanced Th1 profile characterized by higher IL-12 is important for preventing dissemination of L. braziliensis to the mucosa. Further evaluation of parasite-related interactions with the host immunological response is necessary to elucidate the dissemination mechanisms of Leishmania.
Tegumentary leishmaniasis is a vector-borne disease with an incidence of approximately 0.7 to 1.2 million cases each year (World Health organization, 2021). The disease burden measured in disability-adjusted life years is higher than that of diseases such as leprosy, dengue fever and Chagas disease (Hotez et al., 2004). One of the main factors related to the negative impact of the disease is the possibility of sequelae related to the compromise of the nasal mucosa (Costa et al., 1987; Strazzulla et al., 2013). The presence of mucosal lesions is characteristic of American tegumentary leishmaniasis (ATL); it is estimated to occur in 3% to 5% of all patients with the disease in the Americas and is primarily caused by Leishmania braziliensis (Lessa et al., 2007).
Mucosal leishmaniasis (ML) is an outcome of ATL resulting from parasite dissemination from uncontained cutaneous leishmaniasis (CL) (Marsden et al., 1984; Amato et al., 2009). The presence of the parasite in the mucosa triggers an intense immune response dependent on macrophage activation (Da-Cruz et al., 2002; Carvalho et al., 2007; Conceição-Silva et al., 2018). This intense cellular reaction is responsible for the development of granulomatous lesions in the nasal septum and oropharyngeal structures (Conceição-Silva et al., 2018), reducing the quantity of parasites in late stages and diminishing the sensitivity of parasitological and molecular biology methods for diagnosis (Gomes et al., 2014). The natural history of ML shows that a possible paradox related to immunology exists. Although the presence of Leishmania in the mucosa over time stimulates an intense granulomatous response, earlier in disease progression, the parasite escapes from the host immunological response during dissemination periods to the mucosa (de Magalhães et al., 1986; Ávila et al., 2018; Martínez-López et al., 2018).
Early in the disease course, ML can coexist with active cutaneous lesions (Figueroa et al., 2009), but due to delayed access to healthcare, patients are normally diagnosed when the effects of destructive lesions, such as nasal septal perforation or destruction of facial architecture, have already occurred (Sampaio et al., 2019). The process begins with the dissemination of the parasite to the nasal mucosa, leading to microscopic and finally macroscopic changes (Amato et al., 2009). At first, lesions are oligosymptomatic and are not easily observed by the patient, which contributes to the delayed diagnosis (Boaventura et al., 2006). Later steps of disease development have been the focus of research in the field, limiting our understanding of the initial physio-pathogenic stages, including dissemination (Maretti-Mira et al., 2012; Ávila et al., 2018). L. braziliensis can be demonstrated in the nasal mucosa of patients with active cutaneous lesions (Figueroa et al., 2009; Romero et al., 2010; Canário et al., 2019), making these patients an interesting model to study early steps of disease development.
Here, we aimed to detect L. braziliensis DNA in the mucosa of ATL patients with active CL and to relate those findings with clinical and systemic immunological mediators related to the early dissemination (ED) of the parasite to the nasal mucosa.
We performed a cross-sectional study with patients attending from February 2017 to December 2020 the Leishmaniasis Clinic at the University Hospital of Brasilia, a referral service for leishmaniasis diagnosis and treatment in the Brazilian mid-western region. Initially, patients with active cutaneous lesions suggestive of leishmaniasis were screened for inclusion, and clinical and laboratory data were collected. After initial investigation, patients under immunosuppressive therapy or without a confirmed diagnosis of CL were excluded, and only patients with cutaneous lesions confirmed to be ATL were included. All CL cases were defined according to a reference standard based on the results of clinical evaluation, indirect immunofluorescense, direct skin exam, culture of skin aspirates in Novy-MacNeal-Nicolle medium and polymerase chain reactions of skin fragments as described elsewhere (Gomes et al., 2014; Gomes et al., 2014).
Patients with ATL early dissemination (CL-ED) were defined as active CL patients with the presence of L. braziliensis DNA in the nasal mucosa. Patients with negative testing were considered controls (CL-ED-Neg). In our study, all CL patients were examined by an assistant dermatologist with anterior rhinoscopy and oroscopy and were referenced for endoscopic examination of the ear, nose, and throat by an expert otorhinolaryngologist. Dermatological clinical examination also included measurement of cutaneous lesions using an adhesive ORC-9752 scale (Orc forensics, Oregon City, USA). In any patient with CL in whom an active mucous lesion was concomitantly identified, we applied Lessa’s classification as previously described: I, nodulation without ulcerations; II, superficial ulcerations; III, deep ulcerations; IV, septum perforation; and V, destruction of nasal architecture and altered facial structure (Lessa et al., 2012).
Anterior nasal swabs (Absorve™ sterile Sample collection swab, São Paulo, Brazil) were collected from all included patients. The swabs were rotated five times in each nasal fossa at the anterior septum and inferior turbinate head. DNA extraction from the nasal swab samples was performed using the PureLink Genomic DNA Kit (Invitrogen, Carlsbad, USA) according to the manufacturer’s protocol. Real-time polymerase chain reactions (RT-PCR) were performed with a TaqMan-specific probe for L. braziliensis detection (forward 5’-TGCTATAAAATCGTACCACCCGACA-3’, reverse 5’-GAACGGGGTTTCTGTATGCCATTT-3’), a probe for FAM (6-carboxyfluorescein; TTGCAGAACGCCCCTACCCAGAGGC), and TAMRA (6-carboxytetramethylrhodamine) on a QuantStudio 1 (Thermo Fisher Scientific, Waltham, USA), as described by Gomes et al. (2017). To evaluate circulating cytokine levels, plasma from each patient was isolated, and tumour necrosis factor (TNF)-α, interleukin (IL)-10, IL-1β, IL-8, IL-6 and IL-12p70 levels were measured using the Human Inflammatory Cytokine Cytometric Bead Array (Becton Dickinson, Franklin Lakes, USA) with a FACSVerse flow cytometer (Becton Dickinson).
For sample size calculation, we aimed at a power of 0.9 and an alpha of 0.05. The calculation was performed based on the expected levels of TNF-α extrapolated from a study by Da-Cruz et al (Da-Cruz et al., 1996), considering that the levels of this cytokine in subjects with ED would be similar to those observed in ML patients (231.4 ± 76.3 pg/ml) and that patients without ED would have a cytokine level comparable to that in CL patients (43.5 ± 8.2 pg/ml). We considered that approximately 11% (Gomes, 2014) of the CL patients would have ED and that 50% of the initially screened subjects would have CL confirmed after investigation. With these assumptions, we included 91 patients to have the desired power and alpha.
Regression imputation using the dependent variable and significant covariates was used to estimate three missing values of the total area of the lesions. The association between ED and clinical variables (sex, age, lesion evolution time, total area of the lesions, number of lesions, number of affected body segments, presence of mucosal symptoms and location of the lesions - hip or legs, arms, face or neck, and chest or abdomen) and cytokine levels was tested using two samples T tests for the parametrical variable “age” and Wilcoxon rank sum tests for all the other variables that were shown to be non-parametrical. All the variables associated with ED having p<0.25 were included in the multivariate model. Multivariate analysis was performed with Poisson regression with robust variance (Zou, 2004), and variables were chosen using the stepwise backward selection strategy. At each step, model improvement was evaluated by the Bayesian information criterion. Multicollinearity was also evaluated using the variance inflation factor (VIF). All statistical analyses were performed with Stata Statistical Software Release 16 (StataCorp LLC, College Station, USA). This study was approved by the institutional review board of the University of Brasilia (1.521.691), and subjects signed an informed consent form before inclusion.
We recruited 93 patients, 14 of whom were excluded, nine for not having a leishmaniasis diagnosis and five for having an alternative diagnosis. The remaining 79 patients constituted our sample, with L. braziliensis DNA being identified in the nasal mucosa of 24 (30.3%) (Figure 1). The typical patient of our population was 41 years old, with a single lesion being approximately two months old on average. After otorhinolaryngological endoscopic examination, as expected, clinically active mucous lesions were found in only five patients in the CL-ED group (Table 1). In these patients, the lesions were early, not surpassing grade II in Lessa’s classification (Lessa et al., 2012) (Table 1). All patients were treated according to the national CL treatment protocol with meglumine antimoniate at a daily dose of 20 mg Sb5+/kg for 20 days.
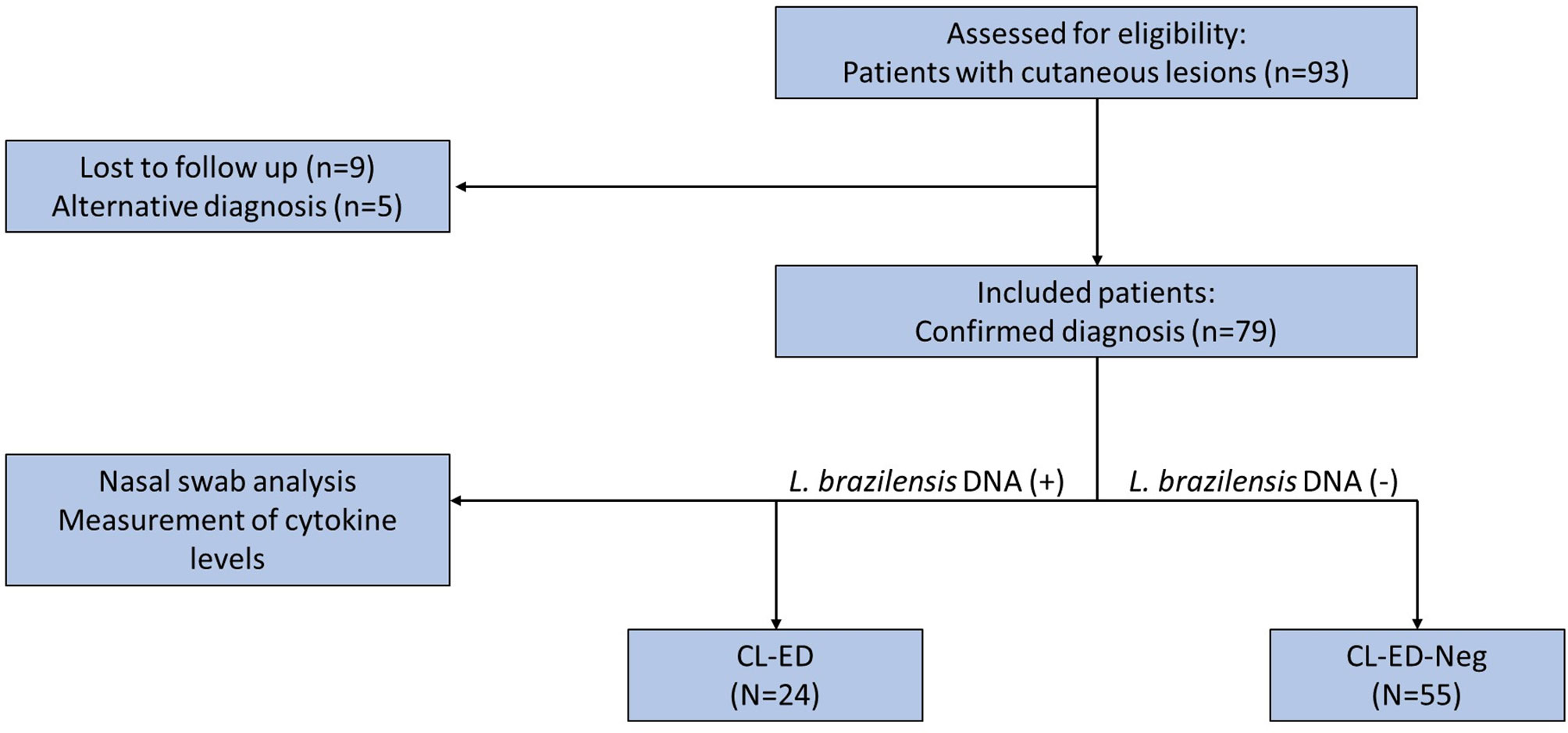
Figure 1 Flow chart showing eligible and included patients as well as the final group configuration. n, number of patients; CL-ED, cutaneous leishmaniasis with early dissemination to mucosa; CL-ED-Neg, cutaneous leishmaniasis without early dissemination to mucosa.

Table 1 Description of early mucosal lesions of five patients with cutaneous leishmaniasis with concomitant mucous lesions and a positive result for Leishmania braziliensis DNA from nasal swabs.
Cytokine levels are disclosed in Table 2 and were apparently similar between groups in the univariate analysis. In the univariate model, ED was significantly associated with a higher number of affected body segments (p=0.005) and a higher number of lesions (p= 0.003) (Table 2). Important variables in the univariate analysis were initially entered into the model (Table 2). High multicollinearity was found, and the TNF-α level was dropped from the model based on its VIF of 14.06 and its higher p value in the univariate model. After the selection of variables, the only variables that remained significant and thus were included in the model were IL-12 level (prevalence ratio (PR) =0.44; 95% confidence interval (CI): 0.21-0.94; p=0.034), IL-6 level (PR=1.001; 95%CI: 1.0005-1.002; p=0.002) and number of affected body segments (PR= 1.65; 95%CI: 1.36-2.01; p<0.001).
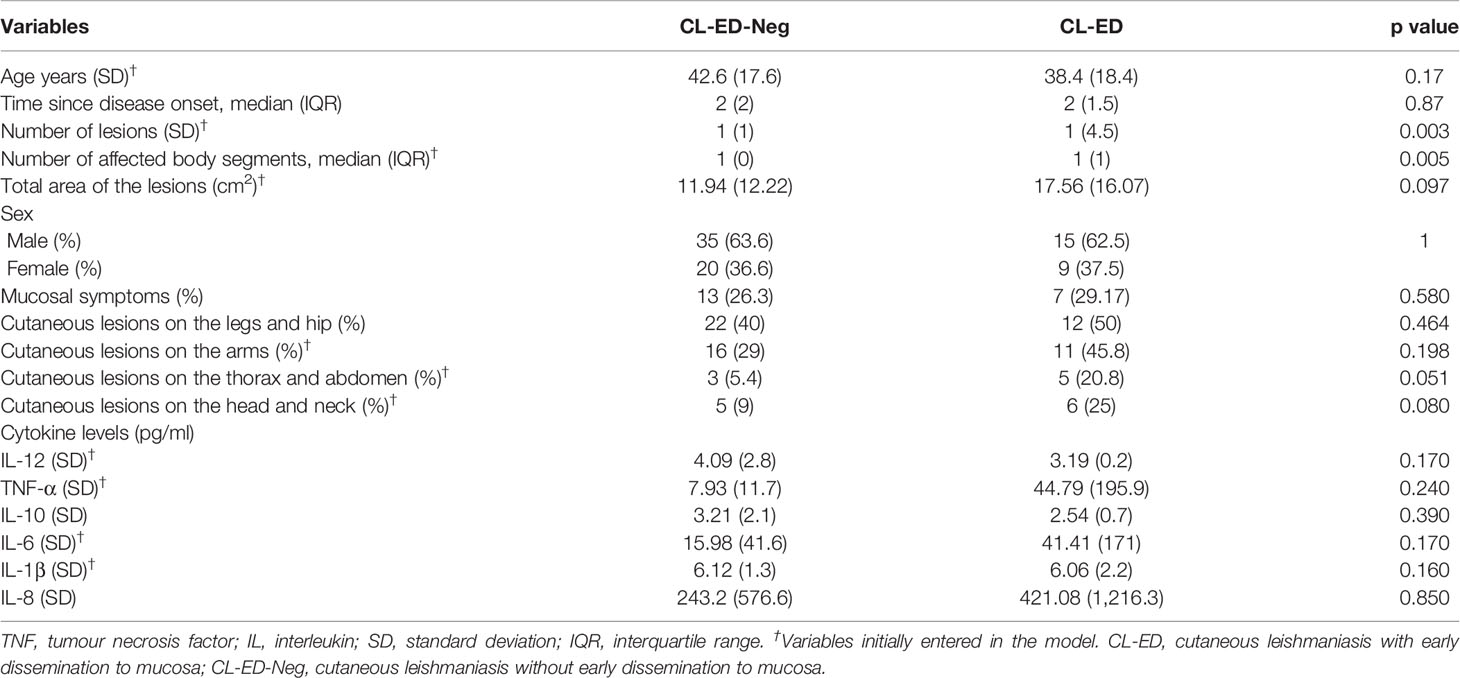
Table 2 Univariate analysis of possible risk factors for early dissemination of Leishmania braziliensis to the nasal mucosa.
In this study, we observed that 30.3% of patients with active cutaneous ulcers had molecular evidence of the presence of L. braziliensis in the nasal mucosa. In another study from an L. braziliensis endemic area, Canário et al. found parasite DNA in the mucosa of 7.8% CL subjects with clinically healthy nasal mucosa (Canário et al., 2019). This difference may be partially explained by the distinct inclusion criteria of the studies, since we did not exclude patients with CL if they were shown to have simultaneous early mucosal lesions.
In addition, all mucosal lesions found were early, not surpassing grade II of V in Lessa’s classification (Lessa et al., 2012). Conversely, other studies have shown that by the time of diagnosis, approximately 60% of active ML cases are classified as grade III or greater (Lessa et al., 2012; de Lima et al., 2021). Thus, the early diagnosis of mucosal lesions in this study was associated with shorter disease duration, three months on average, and consequently less severe disease. Our data thus support the proposition by Boaventura et al. that earlier diagnosis may be made if patients with cutaneous lesions are subjected to systematic otorhinolaryngological examination (Boaventura et al., 2006). On the other hand, the proportion of patients with evidence of ED to the nasal mucosa in our study was lower than those found in Colombia (45%-58%) (Figueroa et al., 2009; Martínez-Valencia et al., 2017). It is possible that this difference between studies is partially explained by the Leishmania species responsible, since in Colombia, most of the isolates are from Leishmania panamensis (Martínez-Valencia et al., 2017), and most mucosal lesions (61%) due to this species occur simultaneously with the active ulcer (Osorio et al., 1998).
Clinical lesions on the mucosa can be difficult to access, and early lesions can lead to only discolouration of mucosa long before the beginning of mucous-specific symptoms (Nishino et al., 1986; Oliveira et al., 1995; Silveira, 2019). Consequently, these lesions can sometimes only be found by expert examiners with the use of special equipment and magnification. Once ML requires longer courses of treatment, the recognition of early mucous lesions is paramount for achieving satisfactory cure (Ministério da Saúde do Brasil SDVES and Departamento de Vigilância Epidemiológica, 2017).
Dissemination of the parasite from an initial cutaneous lesion is assumed to be the main mechanism of ML development (Marsden et al., 1984; Amato et al., 2009). Although conceivable, multiple infections are unlikely to be the culprit for this form. Parasite similarity occurs between cutaneous and mucosal lesions of the same patient, with the parasite genetic variability in these patient lesions being less prominent than the variability between different patients, as shown in an L. braziliensis kDNA signature study (Oliveira et al., 2013). Another possibility is that the parasite disseminates later in the disease process. It has been suggested that amastigotes from ML patients have a decreased ability to be internalized and grow more slowly than those from CL patients (Gomes et al., 2016) and that stationary phase promastigotes from ML are more resistant to nitric oxide (Ávila et al., 2018). These findings suggest that ML parasites are transmitted by vectors as promastigotes that are initially more resistant and more likely to disseminate (Ávila et al., 2018). Additionally, the protective immune responses against L. braziliensis are weaker in the early disease process (Unger et al., 2009). Thus, parasite and host immune factors make it more likely that early dissemination is the essential step leading to the development of ML in most cases.
In line with the pool of evidence found in the literature, our univariate analysis showed that the number of lesions and the number of affected body segments were associated with ED of L. braziliensis to the nasal mucosa. A greater number of lesions was also found to be associated with ED in another study (Maretti-Mira et al., 2012). Interestingly, the clinical risk factors we found were the same as those found in previous studies (Marsden et al., 1984; Cuentas et al., 1984; Turetz et al., 2002), suggesting a predictive relationship between ED and the possible development of ML. The confirmation of this relationship, however, would require a study with long-term follow-up, since many patients commonly have cutaneous lesions a long time before the development of ML (with 37.1% having lesions more than 5 years earlier and 5.7% having lesions more than 15 years earlier according to one classical study (Marsden et al., 1984).
ML is characterized by a marked inflammatory infiltrate that is responsible for maintaining autoaggression in the presence of few or no parasites (de Magalhães et al., 1986). The inflammatory process is driven by excess proinflammatory mediators such as TNF-α and IFN-γ that are unchecked by regulatory cytokines such as IL-10 and TGF-β (Bacellar et al., 2002; Campos et al., 2018). TNF-α is the most studied mediator (Castes et al., 1993; Cabrera et al., 1995; Da-Cruz et al., 1996; Ribeiro-de-Jesus et al., 1998), but other inflammatory cytokines, such as IL-6 (Castellucci et al., 2006), IL-1β (Moreira et al., 2017) and IL-8 (Vargas-Inchaustegui et al., 2009), may also play a role. In the classical paradigm framework, the development of ML is related to a Th1 phenotype characterized by CD4+ T lymphocytes expressing IFN-γ. In this context, IL-12 is an inducer, and IL-10 is an opposing cytokine (Ribeiro-de-Jesus et al., 1998; Silveira, 2019). However, the same inflammatory mediators linked to protection also play a role in tissue destruction associated with ML (Hartley et al., 2014). Some authors have suggested that this apparent paradox may be associated with the dynamics of inflammatory cytokine expression in relation to disease evolution (Ribeiro-de-Jesus et al., 1998; Unger et al., 2009), with early diminished IFN-γ and TNF-α expression being associated with worse prognosis (Unger et al., 2009). We investigated the association of key cytokines with the ED of L. braziliensis to the nasal mucosa to better understand the role of the early immune response in the development of ML. To account for possible confounding clinical variables, we opted to use statistical multivariate modelling to assess the association between cytokine levels and the outcome. Higher IL-6 levels were significantly associated with ED in our final multivariate model (PR=1.001; p=0.002). Although IL-6 has been implicated in the development of mucosal disease (Castellucci et al., 2006), in our study, the effect size (PR=1.001; p=0.002) was too low for the result to be considered of physio-pathological significance, especially considering the effect sizes of the other independent variables included in the model.
IL-12 was a protective mediator against ED of L. braziliensis to the nasal mucosa (PR=0.44; p=0.034; 95%CI: 0.21-0.94) in our final multivariate model. IL-12 is a cytokine classically associated with the development of the Th1 cytokine response (O'Garra and Vieira, 2007) and is in the proinflammatory cytokine milieu associated with the development of ML (Ribeiro-de-Jesus et al., 1998; Silveira, 2019). This protective role of IL-12 seems contradictory since most studies have linked the development of ML with the proinflammatory Th1 response (Castes et al., 1993; Da-Cruz et al., 2002; Bacellar et al., 2002). However, this finding may be explained by the scarcity of studies that address the early immunopathological steps leading to ML development. In a transcriptomic study with ten patients with CL, five of whom later developed ML, Maretti-Mira et al. suggested that patients prone to mucosal disease have an insufficient or delayed development of immune response (Maretti-Mira et al., 2012). In another study by Gomes et al, IFN-γ knockout (KO) mice were infected with amastigotes from patients with ML and CL. Interestingly, in mice infected with ML-derived amastigotes, cutaneous lesions appeared later, but a greater number of parasites were observed in the spleen (Gomes et al., 2016). The same group later showed that the stationary-phase promastigotes derived from ML are more resistant to killing by nitric oxide (NO) and reactive oxygen species than are the CL-derived promastigotes. On the other hand, a lower resistance of ML amastigotes to NO was observed. Altogether, the findings of these two studies suggest that earlier in infection, ML parasites have a weaker capacity to stimulate the immune response at the site of infection but a greater ability to disseminate (Ávila et al., 2018). The delayed development of a protective immune response may facilitate parasite dissemination, and chronic systemic exposure to Leishmania antigens could in turn lead to the exacerbated inflammatory immune response associated with mucosal disease. This idea is in accordance with the finding that in cured ML patients, the duration of active disease is positively associated with antigen-induced production of IFN-γ but negatively associated with IL-10 production (Nogueira et al., 2014).
It is important to state that although this study represents the evaluation of a representative population the presence of untested confounders is always a limitation of clinical observational studies. This is especially true for the study of host-parasite immunological interaction. The present results show that future experiments are feasible and paramount for the study of dissemination mechanisms present in ML cases. The use of more complex laboratory methods, the search for a wider panel of mediators, a wider profile of clinical characteristics and the investigation of Leishmania RNA virus associations are important factors that must be searched in future protocols and that may significantly influence the clinical presentation of CL and ML.
Our study shows that the Th1 response, characterized by higher IL-12 levels, possibly helps limit the disease to the cutaneous site of infection, preventing dissemination to the nasal mucosa. We hypothesize that during the cutaneous phase of the disease, an insufficient rather than exacerbated immune response is responsible for the dissemination of the parasite and later development of mucous disease. These findings are, however, of exploratory nature and deserve to be more thoroughly investigated in other studies. Our study also highlights the importance of a detailed search for mucous commitment in CL to avoid insufficient treatment.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comitê de Ética em Pesquisa da Faculdade de Medicina da Universidade de Brasília - UnB. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
DB: conception, design, data acquisition, analysis, interpretation of data, drafting, final approval. OT: data acquisition, analysis, interpretation of data. CA: data acquisition, analysis, interpretation of data. GF: data acquisition, analysis and interpretation. SS: data acquisition and analysis. BR: data acquisition and analysis. CG: conception, design, data acquisition, analysis, interpretation of data, drafting, final approval, supervision. RS: conception, design, data acquisition, analysis, interpretation of data, drafting, final approval, supervision. All authors contributed to the article and approved the submitted version.
This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001. This work was also supported by grants - 16854.78.40785.2604/2017 and 0193.001447/2016- from Fundação de Apoio à Pesquisa do Distrito Federal (FAP-DF), and from Brazilian Society of Dermatology through FUNADERM.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We thank all the laboratory and clinical staff related to patient care at Hospital Universitário de Brasília.
Amato, V. S., Tuon, F. F., Imamura, R., Abegao de Camargo, R., Duarte, M. I., Neto, V. A. (2009). Mucosal Leishmaniasis: Description of Case Management Approaches and Analysis of Risk Factors for Treatment Failure in a Cohort of 140 Patients in Brazil. J. Eur. Acad. Dermatol. Venereol. 23 (9), 1026–1034. doi: 10.1111/j.1468-3083.2009.03238.x
Ávila, L. R., Gomes, C. M., Oliveira, P. G., Gomes, R. S., Vinaud, M. C., Dorta, M. L., et al. (2018). Promastigote Parasites Cultured From the Lesions of Patients With Mucosal Leishmaniasis Are More Resistant to Oxidative Stress Than Promastigotes From a Cutaneous Lesion. Free Radical Biol. Med. 129, 35–45. doi: 10.1016/j.freeradbiomed.2018.09.005
Bacellar, O., Lessa, H., Schriefer, A., Machado, P., de Jesus, A. R., Dutra, W. O., et al. (2002). Up-Regulation of Th1-Type Responses in Mucosal Leishmaniasis Patients. Infect. Immun. 70 (12), 6734–6740. doi: 10.1128/IAI.70.12.6734-6740.2002
Boaventura, V. S., Cafe, V., Costa, J., Oliveira, F., Bafica, A., Rosato, A., et al. (2006). Concomitant Early Mucosal and Cutaneous Leishmaniasis in Brazil. Am. J. Trop. Med. Hyg. 75 (2), 267–269. doi: 10.4269/ajtmh.2006.75.267
Cabrera, M., Shaw, M.-A., Sharples, C., Williams, H., Castes, M., Convit, J., et al. (1995). Polymorphism in Tumor Necrosis Factor Genes Associated With Mucocutaneous Leishmaniasis. J. Exp. Med. 182 (5), 1259–1264. doi: 10.1084/jem.182.5.1259
Campos, M. B., Lima, L. V. D. R., de Lima, A. C. S., Vasconcelos dos Santos, T., Ramos, P. K. S., Gomes, C. M. D. C., et al. (2018). Toll-Like Receptors 2, 4, and 9 Expressions Over the Entire Clinical and Immunopathological Spectrum of American Cutaneous Leishmaniasis Due to Leishmania (V.) Braziliensis and Leishmania (L.) Amazonensis. PloS One 13 (3), e0194383. doi: 10.1371/journal.pone.0194383
Canário, A., Queiroz, M., Cunha, G., Cavalcante, T., Riesz, V., Sharma, R., et al. (2019). Presence of Parasite DNA in Clinically Unaffected Nasal Mucosa During Cutaneous Leishmaniasis Caused by Leishmania (Viannia) Braziliensis. Clin. Microbiol. Infect. 25 (4), e5–e7, 515. doi: 10.1016/j.cmi.2018.12.027
Carvalho, L., Passos, S., Bacellar, O., Lessa, M., Almeida, R. P. D., Magalhaes, A., et al. (2007). Differential Immune Regulation of Activated T Cells Between Cutaneous and Mucosal Leishmaniasis as a Model for Pathogenesis. Parasite Immunol. 29 (5), 251–258. doi: 10.1111/j.1365-3024.2007.00940.x
Castellucci, L., Menezes, E., Oliveira, J., Magalhaes, A., Guimaraes, L. H., Lessa, M., et al. (2006). IL6– 174 G/C Promoter Polymorphism Influences Susceptibility to Mucosal But Not Localized Cutaneous Leishmaniasis in Brazil. J. Infect. Dis. 194 (4), 519–527. doi: 10.1086/505504
Castes, M., Trujillo, D., Rojas, M. E., Fernandez, C. T., Araya, L., Cabrera, M., et al. (1993). Serum Levels of Tumor Necrosis Factor in Patients With American Cutaneous Leishmaniasis. Biol. Res. 26 (1-2), 233–238.
Conceição-Silva, F., Leite-Silva, J., Morgado, F. N. (2018). The Binomial Parasite-Host Immunity in the Healing Process and in Reactivation of Human Tegumentary Leishmaniasis. Front. Microbiol. 9, 1308. doi: 10.3389/fmicb.2018.01308
Costa, J. M. L., Vale, K. C., Cecílio, I. N., Osaki, N. K., Netto, E. M., Tada, M. S., et al. (1987). Aspectos Psicossociais E Estigmatizantes Da Leishmaniose Cutâneo-Mucosa. Rev. da Sociedade Bras. Medicina Trop. 20 (2), 77–82. doi: 10.1590/S0037-86821987000200003
Cuentas, E. L., Marsden, P., Cuba, C., Barreto, A., Campos, M. (1984). Possible Risk Factors in Development of Mucosal Lesions in Leishmaniasis. Lancet 324 (8397), 295. doi: 10.1016/S0140-6736(84)90346-5
Da-Cruz, A. M., Bittar, R., Mattos, M., Oliveira-Neto, M. P., Nogueira, R., Pinho-Ribeiro, V., et al. (2002). T-Cell-Mediated Immune Responses in Patients With Cutaneous or Mucosal Leishmaniasis: Long-Term Evaluation After Therapy. Clin. Diagn. Lab. Immunol. 9 (2), 251–256. doi: 10.1128/CDLI.9.2.251-256.2002
Da-Cruz, A. M., de Oliveira, M. P., De Luca, P. M., Mendonca, S. C., Coutinho, S. G. (1996). Tumor Necrosis Factor-Alpha in Human American Tegumentary Leishmaniasis. Mem. Inst. Oswaldo Cruz 91 (2), 225–229. doi: 10.1590/S0074-02761996000200019
de Lima, C. M. F., Magalhães, A. S., Costa, R., Barreto, C. C., Machado, P. R. L., Carvalho, E. M., et al. (2021). High Anti-Leishmania IgG Antibody Levels Are Associated With Severity of Mucosal Leishmaniasis. Front. Cell. Infect. Microbiol. 11, 652956 (258). doi: 10.3389/fcimb.2021.652956
de Magalhães, A. V., Moraes, M. A., Raick, A. N., Llanos-Cuentas, A., Costa, J. M., Cuba, C. C., et al. (1986). Histopathology of Mucocutaneous Leishmaniasis Caused by Leishmania Braziliensis Brasiliensis. 3. Cell. Reaction. Rev. Do Instituto Medicina Trop. São Paulo 28 (5), 300–311. doi: 10.1590/S0036-46651986000500004
Figueroa, R. A., Lozano, L. E., Romero, I. C., Cardona, M. T., Prager, M., Pacheco, R., et al. (2009). Detection of Leishmania in Unaffected Mucosal Tissues of Patients With Cutaneous Leishmaniasis Caused by Leishmania (Viannia) Species. J. Infect. Dis. 200 (4), 638–646. doi: 10.1086/600109
Gomes, C. M. (2014). Acurácia Da Reação Em Cadeia Da Polimerase Em Amostras De Saliva, Swab Nasal E Papel Filtro Oral No Diagnóstico Da Leishmaniose Tegumentar Americana: Estudo Clínico, Revisão Sistemática Da Literatura E Meta-Análise. [master’s thesis]. [Brasília (DF), Brazil]:Universidade de Brasília.
Gomes, C. M., Avila, L. R., Santos, J. C., Oliveira, P. G., Tome, F. D., Pereira, L. I., et al. (2016). Leishmania (Viannia) Braziliensis Amastigotes From Patients With Mucosal Leishmaniasis Have Increased Ability to Disseminate and Are Controlled by Nitric Oxide at the Early Stage of Murine Infection. Pathog. Dis. 74 (4), ftw023. doi: 10.1093/femspd/ftw023
Gomes, C. M., Cesetti, M. V., de Paula, N. A., Vernal, S., Gupta, G., Sampaio, R. N., et al. (2017). Field Validation of SYBR Green- and TaqMan-Based Real-Time PCR Using Biopsy and Swab Samples To Diagnose American Tegumentary Leishmaniasis in an Area Where Leishmania (Viannia) Braziliensis Is Endemic. J. Clin. Microbiol. 55 (2), 526–534. doi: 10.1128/JCM.01954-16
Gomes, C. M., de Paula, N. A., Cesetti, M. V., Roselino, A. M., Sampaio, R. N. (2014). Mucocutaneous Leishmaniasis: Accuracy and Molecular Validation of Noninvasive Procedures in a L. (V.) Braziliensis-Endemic Area. Diagn. Microbiol. Infect. Dis. 79 (4), 413–418. doi: 10.1016/j.diagmicrobio.2014.05.002
Gomes, C. M., Paula, N. A., Morais, O. O., Soares, K. A., Roselino, A. M., Sampaio, R. N. (2014). Complementary Exams in the Diagnosis of American Tegumentary Leishmaniasis. An Bras Dermatol. 89 (5), 701–709. doi: 10.1590/abd1806-4841.20142389
Hartley, M.-A., Drexler, S., Ronet, C., Beverley, S. M., Fasel, N. (2014). The Immunological, Environmental, and Phylogenetic Perpetrators of Metastatic Leishmaniasis. Trends Parasitol. 30 (8), 412–422. doi: 10.1016/j.pt.2014.05.006
Hotez, P. J., Remme, J. H., Buss, P., George, G., Morel, C., Breman, J. G. (2004). Combating Tropical Infectious Diseases: Report of the Disease Control Priorities in Developing Countries Project. Clin. Infect. Dis. 38 (6), 871–878. doi: 10.1086/382077
Lessa, M. M., Lessa, H. A., Castro, T. W., Oliveira, A., Scherifer, A., Machado, P. R. L., et al. (2007). Leishmaniose Mucosa: Aspectos Clínicos E Epidemiológicos. Rev. Bras. Otorrinolaringol 73(6), 843–847. doi: 10.1590/S0034-72992007000600016
Lessa, H. A., Lessa, M. M., Guimaraes, L. H., Lima, C. M., Arruda, S., Machado, P. R., et al. (2012). A Proposed New Clinical Staging System for Patients With Mucosal Leishmaniasis. Trans. R Soc. Trop. Med. Hyg. 106 (6), 376–381. doi: 10.1016/j.trstmh.2012.03.007
Maretti-Mira, A. C., Bittner, J., Oliveira-Neto, M. P., Liu, M., Kang, D., Li, H., et al. (2012). Transcriptome Patterns From Primary Cutaneous Leishmania Braziliensis Infections Associate With Eventual Development of Mucosal Disease in Humans. PloS Negl. Trop. Dis. 6 (9), e1816. doi: 10.1371/journal.pntd.0001816
Marsden, P. D., Llanos-Cuentas, E. A., Lago, E. L., Cuba, C. C., Barreto, A. C., Costa, J. M., et al. (1984). Human Mucocutaneous Leishmaniasis in Três Braços, Bahia-Brazil. An Area of Leishmania Braziliensis Braziliensis Transmission. III-Mucosal Disease Presentation and Initial Evolution. Rev. Soc. Bras. Med. Trop. 17 (4), 179–186. doi: 10.1590/S0037-86821984000400004
Martínez-López, M., Soto, M., Iborra, S., Sancho, D. (2018). Leishmania Hijacks Myeloid Cells for Immune Escape. Front. Microbiol. 9, 883 (883). doi: 10.3389/fmicb.2018.00883
Martínez-Valencia, A. J., Daza-Rivera, C. F., Rosales-Chilama, M., Cossio, A., Rincón, E. J. C., Desai, M. M., et al. (2017). Clinical and Parasitological Factors in Parasite Persistence After Treatment and Clinical Cure of Cutaneous Leishmaniasis. PloS Neglect. Trop. Dis. 11 (7), e0005713. doi: 10.1371/journal.pntd.0005713
Ministério da Saúde do Brasil SDVES, Departamento de Vigilância Epidemiológica (2017). Manual De Vigilância E Controle Da Leishmaniose Tegumentar Americana Atualizada, Editora MS. 1(1):1–189
Moreira, R. B., Pirmez, C., Oliveira-Neto, D., Paes, M., De Souza Aguiar, L., Da Silva Gonçalves, A. J., et al. (2017). AIM2 Inflammasome Is Associated to Disease Severity in Tegumentary Leishmaniasis Caused by Leishmania (V.) Braziliensis. Parasite Immunol. 39 (7), 1–7. doi: 10.1111/pim.12435
Nishino, L., Ragiotta, A. R., Almeida, N. A., Santamaria, J. R. (1986). Leishmaniose Em Crianças. An Bras Dermatol. 61 (1), 23–28.
Nogueira, R., Gomes-Silva, A., Bittar, R., Silva Mendonca, D., Amato, V., Silva Mattos, M., et al. (2014). Antigen-Triggered Interferon-γ and Interleukin-10 Pattern in Cured Mucosal Leishmaniasis Patients Is Shaped During the Active Phase of Disease. Clin. Exp. Immunol. 177 (3), 679–686. doi: 10.1111/cei.12364
O'Garra, A., Vieira, P. (2007). TH 1 Cells Control Themselves by Producing Interleukin-10. Nat. Rev. Immunol. 7 (6), 425–428. doi: 10.1038/nri2097
Oliveira, M. R. F. D., Macêdo, V. D. O., Carvalho, E. M. D., Barral, A., Marotti, J. G., Bittencourt, A., et al. (1995). Estudo Evolutivo Da Leishmaniose Mucosa (7 a 17 Anos De Seguimento) Causada Por Leishmania (Viannia) Braziliensis Em Três Braços, Bahia. Rev. da Sociedade Bras. Medicina Trop. 28 (4), 325–332. doi: 10.1590/S0037-86821995000400004
Oliveira, F. S., Valete-Rosalino, C. M., Pacheco, S. J., Costa, F. A. C., Schubach, A. O., Pacheco, R. S. (2013). American Tegumentary Leishmaniasis Caused by Leishmania (Viannia) Braziliensis: Assessment of Parasite Genetic Variability at Intra-and Inter-Patient Levels. Parasites & Vectors 6 (189), 1–8. doi: 10.1186/1756-3305-6-189
Osorio, L. E., Castillo, C. M., Ochoa, M. T. (1998). Mucosal Leishmaniasis Due to Leishmania (Viannia) Panamensis in Colombia: Clinical Characteristics. Am. J. Trop. Med. Hyg. 59 (1), 49–52. doi: 10.4269/ajtmh.1998.59.49
Ribeiro-de-Jesus, A., Almeida, R. P. D., Lessa, H., Bacellar, O., Carvalho, E. (1998). Cytokine Profile and Pathology in Human Leishmaniasis. Braz. J. Med. Biol. Res. 31 (1), 143–148. doi: 10.1590/S0100-879X1998000100020
Romero, I., Téllez, J., Suárez, Y., Cardona, M., Figueroa, R., Zelazny, A., et al. (2010). Viability and Burden of Leishmania in Extralesional Sites During Human Dermal Leishmaniasis. PloS Neglect. Trop. Dis. 4 (9), e819. doi: 10.1371/journal.pntd.0000819
Sampaio, R. N. R., Paula, C. D. R. D., Porto, C., Motta, JDOCD, Pereira, L. I. D. A., Martins, S. S., et al. (2019). A Randomized, Open-Label Clinical Trial Comparing the Long-Term Effects of Miltefosine and Meglumine Antimoniate for Mucosal Leishmaniasis. Rev. da Sociedade Bras. Medicina Trop. 52 e20180292, 1–8. doi: 10.1590/0037-8682-0292-2018
Silveira, F. T. (2019). What Makes Mucosal and Anergic Diffuse Cutaneous Leishmaniases So Clinically and Immunopathogically Different? A Review in Brazil. Trans. R. Soc. Trop. Med. Hyg. 113 (9), 505–516. doi: 10.1093/trstmh/trz037
Strazzulla, A., Cocuzza, S., Pinzone, M. R., Postorino, M. C., Cosentino, S., Serra, A., et al. (2013). Mucosal Leishmaniasis: An Underestimated Presentation of a Neglected Disease. BioMed. Res. Int. 2013, 805108. doi: 10.1155/2013/805108
Turetz, M. L., Machado, P. R., Ko, A. I., Alves, F., Bittencourt, A., Almeida, R. P., et al. (2002). Disseminated Leishmaniasis: A New and Emerging Form of Leishmaniasis Observed in Northeastern Brazil. J. Infect. Dis. 186 (12), 1829–1834. doi: 10.1086/345772
Unger, A., O’Neal, S., Machado, P. R., Guimarães, L. H., Morgan, D. J., Schriefer, A., et al. (2009). Association of Treatment of American Cutaneous Leishmaniasis Prior to Ulcer Development With High Rate of Failure in Northeastern Brazil. Am. J. Trop. Med. Hyg. 80 (4), 574–579. doi: 10.4269/ajtmh.2009.80.574
Vargas-Inchaustegui, D. A., Espinosa, D., Carlsen, E. D., Tulliano, G., Pacheco, R., Llanos-Cuentas, A., et al (2009). The Expression of Inflammatory Mediators and Its Association With the Susceptibility to Mucosal Leishmaniasis in Peru (136.6). Am. Assoc. Immnol. 182(1 Supplement), 136.6.
World Health Organization (2021) Leishmaniasis World Health Organization Webpage Newsroom: World Health Organization. Available at: https://www.who.int/news-room/fact-sheets/detail/leishmaniasis.
Keywords: leishmaniasis, immunology, multivariate analysis, mucocutaneous, flow cytometry
Citation: Barroso DH, Nóbrega OT, de Araújo CN, Freire GSM, Martins SS, Rodrigues BC, Gomes CM and Sampaio RNR (2021) The Presence of Leishmania braziliensis DNA in the Nasal Mucosa of Cutaneous Leishmaniasis Patients and the Search for Possible Clinical and Immunological Patterns of Disease Progression: A Cross Sectional Study. Front. Cell. Infect. Microbiol. 11:744163. doi: 10.3389/fcimb.2021.744163
Received: 19 July 2021; Accepted: 28 September 2021;
Published: 14 October 2021.
Edited by:
Claudia Masini d’Avila-Levy, Oswaldo Cruz Foundation (Fiocruz), BrazilReviewed by:
Danilo Ciccone Miguel, State University of Campinas, BrazilCopyright © 2021 Barroso, Nóbrega, de Araújo, Freire, Martins, Rodrigues, Gomes and Sampaio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ciro Martins Gomes, Y2lyb2dvbWVzQHVuYi5icg==
†These authors have contributed equally to this work and share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.