 Marie-Céline Zanella1,2*
Marie-Céline Zanella1,2* Abdessalam Cherkaoui1
Abdessalam Cherkaoui1 Vladimira Hinic3
Vladimira Hinic3 Gesuele Renzi1
Gesuele Renzi1 Daniel Goldenberger3
Daniel Goldenberger3 Adrian Egli3,4
Adrian Egli3,4 Jacques Schrenzel1,2,5
Jacques Schrenzel1,2,5- 1Laboratory of Bacteriology, Division of Laboratory Medicine and Division of Infectious Diseases, University of Geneva Hospitals, Geneva, Switzerland
- 2Division of Infectious Diseases, University of Geneva Hospitals, Geneva, Switzerland
- 3Division of Clinical Bacteriology and Mycology, University Hospital Basel, Basel, Switzerland
- 4Applied Microbiology Research, Department of Biomedicine, University of Basel, Basel, Switzerland
- 5University of Geneva Medical School, Geneva, Switzerland
False-positive results in the diagnostic of meningitis and encephalitis pose important challenges. This study aimed to determine false-positive rates for Haemophilus influenzae in cerebrospinal fluids evaluated by the BioFire FilmArray® Meningitis/Encephalitis Panel. We conducted a retrospective study of all H. influenzae-positive FilmArray®. Meningitis/Encephalitis Panel results from June 2016 to October 2019 in two Swiss university hospitals. Cases were classified as true positive, likely true-positive, and likely false-positive results according to cerebrospinal fluid culture, H. influenzae-specific quantitative real-time PCR (qPCR), and Gram staining, as well as culture of other materials. We performed 3,082 panels corresponding to 2,895 patients: 0.6% of the samples (18/3,082) were positive for H. influenzae. Culture and H. influenzae-specific qPCR were performed on 17/18 (94.4%) and 3/18 (16.7%) cerebrospinal fluid samples, respectively; qPCR was negative in all cases. Among 17 samples sent for culture, 10 concerned patients were not treated with antibiotics prior to lumbar puncture. Only 1/17 revealed growth of H. influenzae and was classified as a true positive. We further classified 3/18 (16.7%) cases with the identification of Gram-negative rods in the cerebrospinal fluid or positive blood cultures for H. influenzae as likely true-positive and 14/18 (77.8%) cases as likely false-positive. Diagnostic results should always be interpreted together with the clinical presentation, cerebrospinal fluid analysis, and other available microbiological results. All H. influenzae-positive results should be viewed with special caution and a H. influenzae-specific qPCR should be systematically considered.
Introduction
Central nervous system (CNS) infections are commonly caused by diverse pathogens, mostly viruses and bacteria, and molecular multiplex panels have been developed to simultaneously diagnose multiple pathogens in cerebrospinal fluid (CSF) samples. These molecular rapid diagnostic tests are increasingly used in routine diagnostic laboratories for the diagnosis of CNS infections, including meningitis and meningoencephalitis, with the advantages of being easy to use and having short turn-around times. Nevertheless, these syndromic panels lack extensive analytical and clinical validation and concerns have been raised regarding their suboptimal performances (Vetter et al., 2020). Several cases of false-positive results for some targeted pathogens, more specifically for Haemophilus influenzae, have been reported with the BioFire FilmArray® Meningitis/Encephalitis (ME) Panel (bioMérieux, Lyon, France) (Naccache et al., 2018; Boudet et al., 2019). False-positive results could lead to additional investigations and inappropriate antibiotic prescriptions.
H. influenzae is associated with upper and lower respiratory tract infections, but also with invasive infections including meningitis (Agrawal and Murphy, 2011). The broad use of the Haemophilus influenzae type b (Hib) conjugate vaccine led to a dramatic reduction of Hib infections in various countries including Switzerland, where the incidence in 2019 was 1.43 of confirmed cases per 100,000 population (Federal Office of Public Health, Division of Communicable Diseases, [[NoYear]]; Agrawal and Murphy, 2011). In Switzerland, the reported vaccination coverage for children is 89% for the 2014–2016 period (Federal Office of Public Health, Division of Communicable Diseases, 2018).
After implementation of the FilmArray® ME Panel, the bacteriology laboratories of Geneva and Basel university hospitals witnessed an unexpectedly high number of positive cases of H. influenzae, raising suspicion of false-positive cases. In this context, the aim of this retrospective study was to analyze all reports of H. influenzae and to determine the proportion of false-positive cases on all CSF samples analyzed in these two laboratories starting from the introduction of the FilmArray® ME Panel.
Materials and Methods
Ethics Statement
The study was approved by the Geneva and Basel cantonal ethics commissions (Geneva #2020-00215; Basel #2020-01724).
Clinical Specimens
We included all samples from pediatric and adult patients for whom a FilmArray® ME Panel PCR (bioMérieux, Lyon, France) was ordered for CSF microbiology testing at the bacteriology laboratories of Geneva and Basel university hospitals from 1 June 2016 (Geneva) and 17 May 2016 (Basel) to 31 December 2019 and reported to be positive for H. influenzae. Multiple specimens from single patients were not excluded.
Routine, FilmArray® ME Panel, and Confirmatory Testing
Both laboratories are accredited (ISO/IEC17025) and regularly participate in external quality control surveys. In both hospitals, all patients with suspected CNS infection benefit from clinical evaluation, prompt administration of antimicrobials, cerebral radiological exams when needed, and lumbar puncture for CSF analysis, according to published guidelines (van de Beek et al., 2016). When sufficient CSF sample volume is available, the following analyses are performed: CSF cellular count and chemistry, and direct examination with Gram stain, culture, and the FilmArray® ME Panel. Further microbiological investigations can be performed according to the clinical presentation and suspected pathogen, local epidemiology, in accordance with published guidelines (van de Beek et al., 2016). H. influenzae positive results with the FilmArray® ME panel are confirmed with a specific quantitative real-time PCR (qPCR) as previously reported (Price et al., 2015) when enough CSF sample is available.
The FilmArray® ME Panel was performed on CSF samples in accordance with the manufacturer’s instructions, including laboratory precautions and good microbiological practice to prevent contamination. Briefly, 200 µl of CSF specimen is subjected to panel testing. The FilmArray® ME Panel test consists of automated nucleic acid extraction, reverse transcription, two multiplex nucleic acid PCR amplifications, and detection using DNA melting temperature analysis of 14 of the most common bacterial, viral, and fungal pathogens associated with CNS infections (seven viruses, six bacteria and Cryptococcus neformans/gatii) (Leber et al., 2016); results are available within approximately 1 h.
Data Collection
Chart review was conducted to collect the characteristics of the included patients and data regarding their clinical management. During clinical management, the diagnosis of CNS infection was based on the integration of the pre-test probability, clinical presentation, radiological examinations and CSF analysis results. Patients received antimicrobial treatment according to published guidelines (van de Beek et al., 2016). A review of laboratory data was conducted to collect CSF cell counts, as well as protein and chemistry values of the included CSF samples. Results of culture and other molecular assays were obtained for the included CSF samples and additional clinical samples collected within 48 h around the time of CSF sampling. Medical charts were also reviewed for adverse events attributed to antibiotic treatment and Clostridioides difficile infection during a maximum of 2 months in-hospital follow-up.
Data Analysis
Positive results for H. influenzae with the FilmArray® ME Panel and further laboratory tests were classified as follows:
- True-positive result: confirmed by CSF culture and/or positive H. influenzae-specific qPCR on the same CSF sample.
- Likely true-positive result: not confirmed by CSF culture or H. influenzae- specific qPCR when performed. CSF cellularity, chemistry analysis, CSF Gram stain results and the culture results of other clinical samples (e.g. blood cultures) suggest that the result was likely to be a true positive.
- Likely false-positive result: not confirmed by CSF culture or H. influenzae-specific qPCR when performed. CSF cellularity, chemistry analysis, CSF Gram stain results and the culture results of other clinical samples (e.g. blood cultures) suggest that the result was likely to be a false-positive.
Results
We performed a total of 3,082 FilmArray® ME Panels corresponding to 2,895 patients (2,252 adult; 643 pediatric patients). Results for H. influenzae were negative in 99.4% (3,064/3,082; 95% CI 99.1–99.6%) cases and positive in 0.6% (18/3082; 95% CI 0.4–0.9%) CSF samples, corresponding to 12 adult and six pediatric patients. Clinical characteristics and laboratory data of the 18 cases with positive H. influenzae FilmArray® ME Panel results are detailed in Table 1. Among the 18 cases, five cases (patients #1, #2, #3, #5, and #6, Table 1) and 13 cases had CSF specimens collected and analyzed in Basel and Geneva University Hospital Laboratory, respectively.
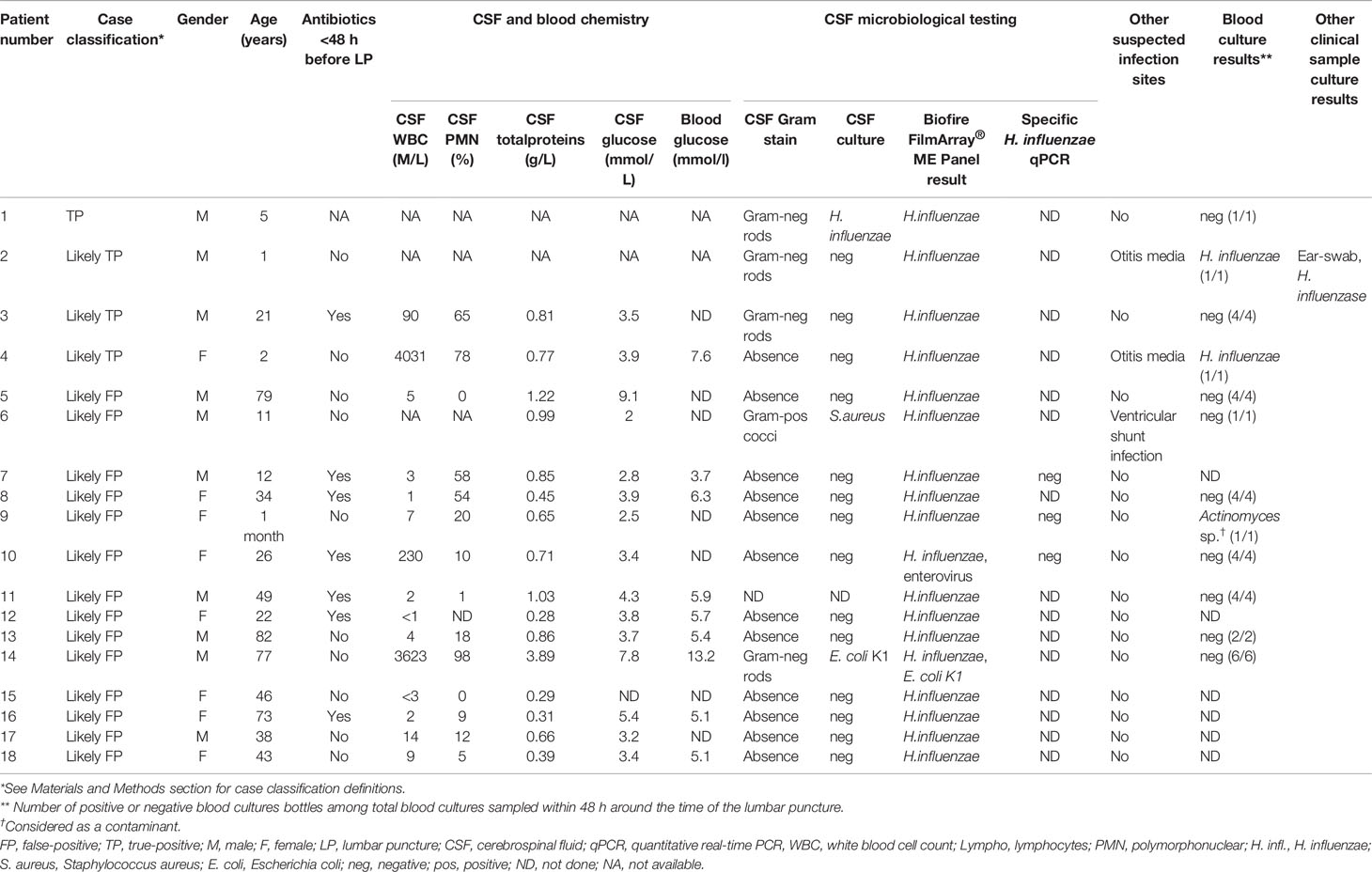
Table 1 Case classification, patient characteristics and laboratory data of patients with positive H. influenzae BioFire FilmArray® ME Panel results (n = 18).
Culture and H. influenzae-specific qPCR were performed on 17/18 (94.4%) and 3/18 (16.7%) CSF samples, respectively. H. influenzae-specific qPCR assay was performed in three samples only due to the limited CSF sample volume available for further testing; qPCR was negative in three cases. Among 17 samples sent for culture, 10 concerned patients were not treated with antibiotics prior to lumbar puncture and only one revealed the growth of H. influenzae. This case (patient #1, Table 1) was classified as a true positive. We classified three (16.7%) cases as likely true-positive, with the identification of Gram-negative rods on CSF gram stain in two cases (patients #2 and #3, Table 1) and positive blood cultures for H. influenzae in two cases (patients #2 and #4, Table 1). Of note, patients #2 and #4 were diagnosed with H. influenzae otitis media. The remaining 14 (77.8%) cases were classified as likely false-positive cases (Table 1).
CSF white blood cell count was determined in 13 samples (median 7 M/L [range 1–4,031 M/L]). Among patients with an elevated CSF white blood cell count, two cases were classified as likely true-positive H. influenzae results (patients #3 and #4, Table 1), and two as likely false-positive with another retained cause of CNS infection (patient #10 with enterovirus-associated meningitis and patient #14 with Escherichia coli-associated meningitis, Tables 1 and 2).
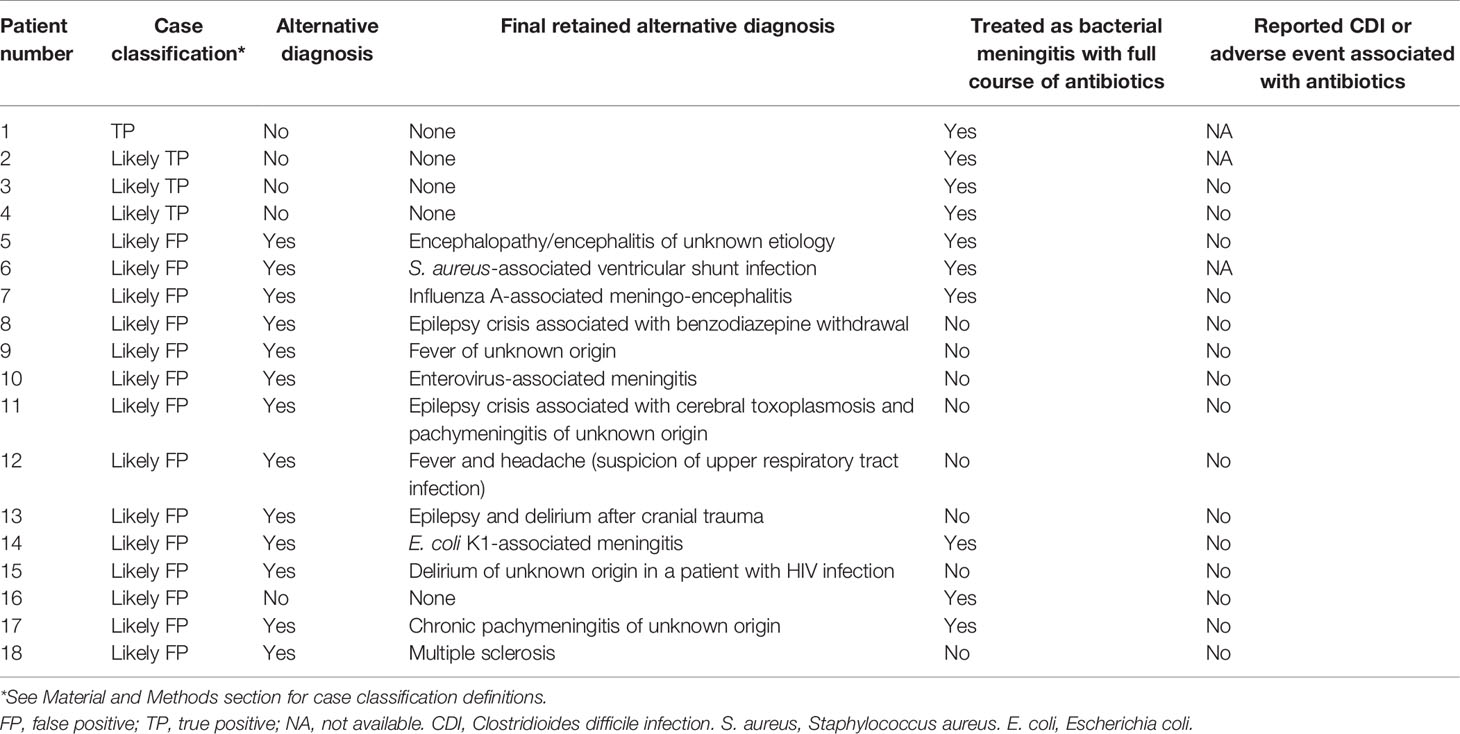
Table 2 Alternative diagnosis, clinical management, and reported adverse effects of antibiotic treatment based on the retrospective review of medical charts of patients with positive H. influenzae BioFire FilmArray® ME Panel results (n = 18).
Regarding the clinical management, the review of medical charts identified that an alternative diagnosis was made for 13/18 (72.2%) patients (Table 2). All cases classified as likely true- positive were treated for H. influenzae meningitis (Table 2). Among cases classified as likely false-positive, only four were treated with antibiotics for bacterial meningitis (Table 2). No adverse event associated with antibiotic treatment or Clostridioides difficile infection was reported (Table 2).
Details of the amplification curve results of the initial and repeated FilmArray® ME Panels when performed are provided in Table S1. Only 1/18 (5.5%) samples revealed positive amplification curves on the two targets designed to detect H. influenzae (patient #4, Table S1). Among three patients for whom the FilmArray® ME Panel was repeated on the same CSF sample, results were positive in two patients and classified as likely true-positive cases (patients #2 and #4, Table S1).
Discussion
In this two-center retrospective study conducted over a period of 3 years, the proportion of CSF samples with H. influenzae FilmArray® ME Panel positive results was 0.6% (95% CI 0.4–0.9%). A review of the 18 H. influenzae positive results revealed that only one case (5.5%) could be considered as a true positive. Regarding H. influenzae culture-positive results from other clinical samples, Gram stain and CSF analysis, 16.7% of cases were classified as likely true-positive cases. At the time of clinical management, these patients have been treated accordingly. For a high proportion of cases (77.8%), CSF analysis and microbiological results suggested that H. influenzae FilmArray® ME positive results were likely false-positive. Among these, the review of medical charts suggested that H. influenzae-associated meningitis was finally retained in a few patients: an alternative diagnosis was made in 92.9% of patients and only 28.6% received a full course of antibiotics for bacterial meningitis. The fact that only a minority received antibiotics highlights that the result was not in concordance with the clinical picture and course of the patient. The impact of the false-positive results was therefore limited since panel results were interpreted together with clinical manifestations, CSF analysis, and other microbiological results. Importantly however, neither the validation studies performed before panel implementation nor the regular EQC is designed to detect that rate of false-positive results, thus prompting such reports by consortia of panel users.
In the context of a lack of extensive analytical and clinical validation studies, this study may contribute to the surveillance of the assay performance specifically regarding H. influenzae. Among the H. influenzae false-positive results reported in the literature (Naccache et al., 2018; Boudet et al., 2019), it remains unclear whether the false-positive results are due to pre-analytic issues, sample contamination or to an analytical artifact. However, in our study, sample contamination seems unlikely given the rigorous handling of the samples, the analyses performed in two different laboratories, and the absence of frequent false-positive results for Streptococcus pneumoniae for instance, which could be at least as frequent as an external contaminant; qPCR results revealed to be all negative, thus suggesting, at least in the tested samples, that the positive results of the H. influenzae FilmArray® ME Panel were likely false-positive. False-positive results highlight the precautions needed to perform rapid diagnostic tests to avoid cross-contamination from the environment and especially from the personnel in contact with the sample during the pre-analytical and analytical phases of testing.
Of note, there is also a lack of validation studies assessing the performance of the assay for each pathogen individually. Specifically regarding H. influenzae, the sensitivity of the FilmArray® ME Panel compared to culture may in fact confer an advantage for CNS infection diagnosis, as reported in a recent study (Nestor et al., 2019). Nevertheless, our study raises the issue of its potential lack of specificity for H. influenzae, as reported by others (Naccache et al., 2018; Boudet et al., 2019). Globally, the conclusions drawn on the basis of the performances of the assay based on the few validation studies available are notably limited by the low number of samples tested for each pathogen.
Our study has some limitations. Specific qPCR was not systematically performed in the context of an insufficient available CSF sample. Nevertheless, qPCR results revealed to be all negative, thus suggesting, at least in the samples tested, that the positive results of the H. influenzae FilmArray® ME Panel were likely false-positive. Some laboratory analyses were missing, precluding a rigorous classification of some cases. The retrospective review of clinical charts did not identify any antibiotic adverse events or C. difficile infections, although we cannot exclude information bias due to the lack of reporting or the occurrence of such events after hospitalization.
In conclusion, this study highlights the need for caution for H. influenzae-positive results with the FilmArray® ME Panel. Meningoencephalitis syndromic panel results should always be interpreted together with clinical manifestations, CSF analysis, and other microbiological results. The use of a specific H. influenzae qPCR on CSF samples should be systematically considered as a confirmatory assay.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the Geneva and Basel cantonal ethics commissions. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
M-CZ, AE, and JS contributed to the conception of the work. M-CZ, VH, AC, and GR contributed to the data collection. M-CZ, AC, VH, DG, AE, and JS contributed to the data analysis and interpretation. M-CZ wrote the article. AE and JS contributed to the critical revision of the article. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to acknowledge Rosemary Sudan (Geneva University Hospitals, Switzerland) for editorial assistance.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcimb.2021.639658/full#supplementary-material
Supplementary Table 1 | Detailed results of the BioFire FilmArray® ME Panel for positive H. influenzae cerebrospinal fluid samples (n = 18).
References
Agrawal A., Murphy T. F. (2011). Haemophilus influenzae infections in the H. influenzae type b conjugate vaccine era. J. Clin. Microbiol. 49 (11), 3728–3732. doi: 10.1128/JCM.05476-11
Boudet A., Pantel A., Carles M. J., Bocle H., Charachon S., Enault C., et al. (2019). A review of a 13-month period of FilmArray Meningitis/Encephalitis panel implementation as a first-line diagnosis tool at a university hospital. PLoS One 14 (10), e0223887. doi: 10.1371/journal.pone.0223887
Federal Office of Public Health, Division of Communicable Diseases. Available at: www.bag.admin.ch/bag/en/home/krankheiten/krankheiten-im-ueberblick/hib.html. Haemophilus influenzae.
Federal Office of Public Health, Division of Communicable Diseases (2018) Couverture vaccinale des enfants âgés de 2, 8 et 16 ans en Suisse (2014-2016). Bull OFSP 2018, 24:13. Available at: www.bag.admin.ch/bag/en/home.html.
Leber A. L., Everhart K., Balada-Llasat J. M., Cullison J., Daly J., Holt S., et al. (2016). Multicenter Evaluation of BioFire FilmArray Meningitis/Encephalitis Panel for Detection of Bacteria, Viruses, and Yeast in Cerebrospinal Fluid Specimens. J. Clin. Microbiol. 54 (9), 2251–2261. doi: 10.1128/JCM.00730-16
Naccache S. N., Lustestica M., Fahit M., Mestas J., Dien Bard J. (2018). One Year in the Life of a Rapid Syndromic Panel for Meningitis/Encephalitis: a Pediatric Tertiary Care Facility’s Experience. J. Clin. Microbiol. 56 (5), e01940–17. doi: 10.1128/JCM.01940-17
Nestor D., Thulin Hedberg S., Lignell M., Skovbjerg S., Molling P., Sundqvist M. (2019). Evaluation of the FilmArray Meningitis/Encephalitis panel with focus on bacteria and Cryptococcus spp. J. Microbiol. Methods 157, 113–116. doi: 10.1016/j.mimet.2019.01.003
Price E. P., Sarovich D. S., Nosworthy E., Beissbarth J., Marsh R. L., Pickering J., et al. (2015). Haemophilus influenzae: using comparative genomics to accurately identify a highly recombinogenic human pathogen. BMC Genomics 16, 641. doi: 10.1186/s12864-015-1857-x
van de Beek D., Cabellos C., Dzupova O., Esposito S., Klein M., Kloek A. T., et al. (2016). ESCMID guideline: diagnosis and treatment of acute bacterial meningitis. Clin. Microbiol. Infect. 22 Suppl 3, S37–S62. doi: 10.1016/j.cmi.2016.01.007
Keywords: Haemophilus influenzae, false-positive, panel, diagnostics, meningitis, central nervous system infection
Citation: Zanella M-C, Cherkaoui A, Hinic V, Renzi G, Goldenberger D, Egli A and Schrenzel J (2021) Unexpectedly High False-Positive Rates for Haemophilus influenzae Using a Meningoencephalitis Syndromic PCR Panel in Two Tertiary Centers. Front. Cell. Infect. Microbiol. 11:639658. doi: 10.3389/fcimb.2021.639658
Received: 11 December 2020; Accepted: 04 February 2021;
Published: 08 March 2021.
Edited by:
Francois Vandenesch, Université de Lyon, FranceReviewed by:
Hege Vangstein Aamot, Akershus University Hospital, NorwayLiã Bárbara Arruda, University College London, United Kingdom
Copyright © 2021 Zanella, Cherkaoui, Hinic, Renzi, Goldenberger, Egli and Schrenzel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marie-Céline Zanella, bWFyaWUtY2VsaW5lLnphbmVsbGFAaGN1Z2UuY2g=