
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cell Dev. Biol., 23 July 2021
Sec. Stem Cell Research
Volume 9 - 2021 | https://doi.org/10.3389/fcell.2021.654210
This article is part of the Research TopicMesenchymal Stromal Cell Therapy for Regenerative MedicineView all 38 articles
 Trinidad Montero-Vilchez1,2
Trinidad Montero-Vilchez1,2 Álvaro Sierra-Sánchez2,3*
Álvaro Sierra-Sánchez2,3* Manuel Sanchez-Diaz1,2
Manuel Sanchez-Diaz1,2 Maria Isabel Quiñones-Vico2,3,4
Maria Isabel Quiñones-Vico2,3,4 Raquel Sanabria-de-la-Torre2,3,4
Raquel Sanabria-de-la-Torre2,3,4 Antonio Martinez-Lopez1,2
Antonio Martinez-Lopez1,2 Salvador Arias-Santiago1,2,3,4
Salvador Arias-Santiago1,2,3,4The skin is the largest organ of the human body, and its dysfunction is related to many diseases. There is a need to find new potential effective therapies for some skin conditions such as inflammatory diseases, wound healing, or hair restoration. Mesenchymal stromal cell (MSC)-conditioned medium (CM) provides a potential opportunity in the treatment of skin disease. Thus, the objective of this review is to evaluate the uses of MSC-CM for treating skin diseases in both animal and human models. A systematic review was conducted regarding the use of MSC-CM for treating skin conditions. One hundred one studies were analyzed. MSC-CM was evaluated in wound healing (55), hypertrophic scars (9), flap reperfusion (4), hair restoration (15), skin rejuvenation (15), and inflammatory skin diseases (3). MSC-CM was obtained from different MSC sources, mainly adipose tissue, bone marrow, and umbilical cord blood. MSC-CM was tested intravenously, intraperitoneally, subcutaneously, intradermally or intralesionally injected or topically applied. MSC-CM was used in both animals and humans. MSC-CM improved wound healing, hair restoration, skin rejuvenation, atopic dermatitis, and psoriasis in both animals and humans. MSC-CM also decreased hypertrophic scars and flap ischemia in animal models. In conclusion, MSC-CM is a promising therapy for skin conditions. Further studies are needed to corroborate safety and effectiveness and to standardize CM manufacturing.
Mesenchymal stromal cells (MSCs) are a type of multipotent adult stem cells that have the potential to proliferate, self-regenerate, and differentiate into multiple cell lineages (Dominici et al., 2006). They can be isolated from several sources such as bone marrow (BM-MSCs), adipose tissue (AT-MSCs), umbilical cord (UC-MSCs), amnion, placenta, or dental pulp (Bogatcheva and Coleman, 2019). MSCs are considered to be one of the most promising therapeutic options in cell therapy and tissue engineering, as they can be used for treating skin, cardiovascular, hematological, neurological, bone, and cartilage diseases (Wong et al., 2015; Kim et al., 2017; Hu et al., 2018; Martinez-Lopez et al., 2020).
It has been observed that the beneficial effects of MSCs are due not only to their multipotent ability but also to their secreted cytokines and growth factors (Caplan, 2017). Cell-free preparations have several advantages over cell therapy, as they can be obtained more easily and more economically and can be manufactured, packaged, and transported straightforwardly (Yang et al., 2021). Moreover, cell-free preparations do not have adverse events associated with cell administration such as rejection, tumorigenic, thrombogenic, ossification, or calcification risk (Bogatcheva and Coleman, 2019; Yang et al., 2021). The risk of malignant transformation of MSCs is a great concern, as MSCs therapy involves ex vivo production and expansion of cell lines, although the spontaneous malignant transformation of human MSCs has not been completely proved and there are many studies that have demonstrated that MSCs, even after physical and chemical stress, undergo senescence rather than become tumorigenic (Caplan et al., 2019). MSCs activate the host innate immune systems and the coagulation, increasing the expression of procoagulant tissue factor and demonstrating a procoagulant effect after MSC contact with blood in in vitro investigations. Infusion reactions and thromboembolism have been reported when using intravascular MSC products. A possible proposed solution to this problem is diluting or treating the MSCs with tissue factor pathway-blocking reagents. Moreover, hemocompatibility testing and optimal product delivery are important for designing safer MSC therapies. Other experimental intravascular therapies, such as islets, hepatocytes, and products derived from MSCs, could also improve MSC safety (Moll et al., 2019). The activation of the immune response could also lead to rejection. There are many investigations that focus on strategies to evade immune recognition, such as human leukocyte antigen (HLA)-matched cells or pharmaceutical immunosuppression (Moll et al., 2019, 2020). Cell-free preparation could help to reduce this risk of malignant transformation, thrombogenic risk, and rejection.
The molecules secreted by stromal cells are referred to the stromal cell secretome and include proteins, microRNA, growth factors, antioxidants, proteasomes, and exosomes (Maguire, 2013). The stromal cell culture media that comprise the secretome are known as the conditioned media (CM), and they are considered to be an abundant resource of paracrine factors (Pawitan, 2014; Mizukami and Yagihashi, 2016). The paracrine factors secreted in vitro include vascular endothelial growth factor (VEGF), hepatocyte growth factor (HGF), insulin-like growth factor-1 (IGF-1), IGF−2, and stromal cell-derived factor 1 (SDF−1) (Ratajczak et al., 2012; Deng et al., 2018). The administration of these factors to the site of an injured organ increases its metabolic activity and oxygen supply and remodels the extracellular matrix (Ratajczak et al., 2012).
The skin is the largest organ of the human body, and its dysfunction is linked to several diseases (Montero-Vilchez et al., 2021). MSCs provide a supply of new cells for epidermal homeostasis, hair cycling, and repairing injured tissue (Kim et al., 2017; Guo et al., 2020). MSCs-CM also provide a potential opportunity in the treatment of skin disease, and there is increased evidence justifying its use for the treatment of cutaneous conditions such as wound healing, hair growth, inflammatory skin diseases, or skin rejuvenation. Thus, the objective of this review is to evaluate the use of MSC-CM for treating skin diseases in both in animals and humans.
A literature search was performed using Medline, Scopus, Embase, and ClinicalTrials.gov from conception to October 2020, following PRISMA Guidelines (Supplementary Material). The following search terms were used: [(MSC) OR (Mesenchymal Stem Cell) OR (Mesenchymal Stromal Cell) OR (Multipotent Stem Cell) OR (Multipotent Stromal Cell) OR (Stem Cell)] AND [(Conditioned Medium) OR (Conditioned Culture Media)] AND [(skin) OR (dermatology)].
The search was limited to (i) human or animal data, (ii) in vivo studies, (iii) using MSC-CM for skin conditions, and (iv) articles written in English or Spanish.
All types of epidemiological studies (clinical trials, cohort studies, case–control studies, and cross-sectional studies) regarding MSC-CM use for skin conditions were included and analyzed. Reviews, guidelines, protocols, and conference abstracts were excluded.
Two researchers (TMV and AML) independently reviewed the titles and abstracts of the articles obtained in the first search to assess relevant studies. The full texts of all articles meeting the inclusion criteria were reviewed, and their bibliographic references were checked for additional sources. The articles considered relevant by both researchers were included in the analysis. Disagreements about inclusion or exclusion of articles were discussed until a consensus was reached. If no consensus was reached, resolution was achieved by discussion with a third researcher (SAS).
The variables assessed were MSC source, passage number and percentage of confluence, model tested, treatment group, route of administration, sample size, assessment, outcomes, and adverse events.
Our literature search identified 1,422 references, 757 after removing duplicates. After the title and abstract were screened, 197 records underwent full-text review. A total of 96 records were excluded because they did not investigate MSC-CM treatment in vivo skin conditions. Other reasons for exclusion along with the flowchart are shown in Figure 1. Ultimately, 101 studies met the eligible criteria.
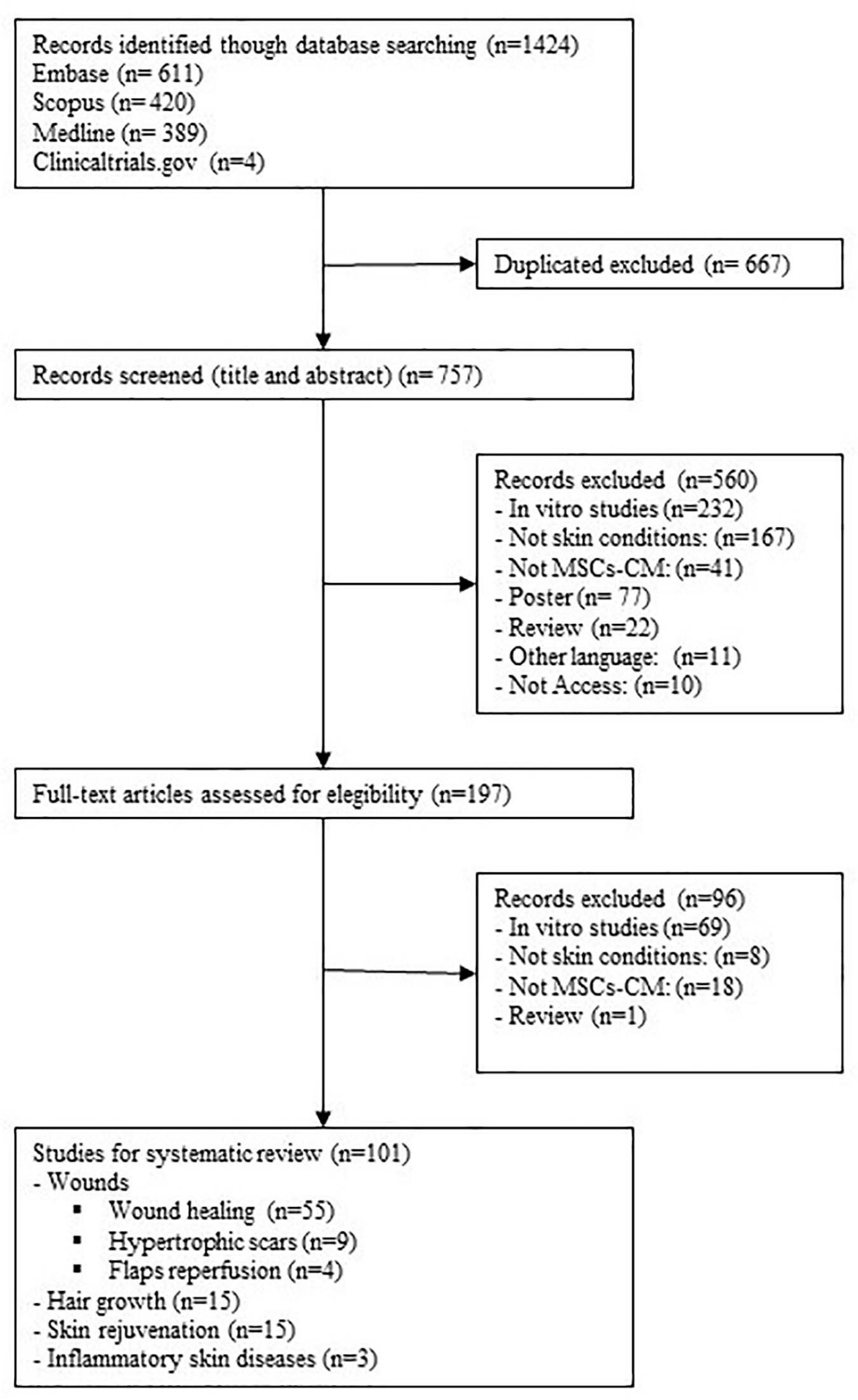
Figure 1. Flow diagram of the study selection process.
Mesenchymal stromal cell-CM has been tested in several skin conditions: wound healing, hypertrophic scars, flap and graft reperfusion, hair restoration, aesthetic applications, and cutaneous inflammatory diseases.
Fifty-three studies evaluated the effects of MSC-CM on wound healing, 58.49% (31/53) evaluated outcomes in non-diabetic wounds, and 35.85% (19/53) in diabetic wounds, including three studies that evaluated wound healing in both diabetic and non-diabetic animals (Fong et al., 2014; Tam et al., 2014; Raj et al., 2019). Moreover MSC-CM has also been tested on burn wounds (5.66%, 3/53), infected wounds (3.77%, 2/53), and radiation-induced wounds (1.89%, 1/53).
Thirty-one studies evaluated the potential of MSC-CM for treating non-diabetic wounds (Table 1). To obtain CM, cells were mainly isolated from human tissues (74.19%, 23/31): from adipose tissue (Cho et al., 2010; Heo et al., 2011; Deng et al., 2017; Yuan et al., 2018; Chen et al., 2021) (21.74%, 5/23), amnion (Yoon et al., 2010; Jun et al., 2014; Park et al., 2018; He et al., 2020) (17.34%, 4/23), umbilical cord blood (Lee et al., 2011; Dong et al., 2017; Raj et al., 2019; Rong et al., 2019) (17.34%, 4/23), bone marrow (Tamari et al., 2013; Chen et al., 2014; Ahangar et al., 2020) (13.04%, 3/23), and Wharton’s jelly (Fong et al., 2014; Tam et al., 2014; Sabzevari et al., 2020) (13.04%, 3/23). Human dental pulp (Zhou et al., 2020) and skin (Robert et al., 2019) were also used. Moreover, murine, swine, caprine, canine, deer, and rabbit tissues were also employed (Chen et al., 2008; Templin et al., 2009; Sun et al., 2014; Mehanna et al., 2015; Du et al., 2017; Payushina et al., 2018; Rong et al., 2019; Joseph et al., 2020). CM was collected from MSCs between passages 1 and 12 at 50–100% confluence. The most common model was murine (96.77%, 30/31), although a swine model was also used (Joseph et al., 2020). Regarding the route of administration, MSC-CM was mainly used topically (51.61%, 16/31), applied to the wounds or around them in cream, hydrogel, or membranes (Heo et al., 2011; Lee et al., 2011; Chen et al., 2014; Jun et al., 2014; Sun et al., 2014; Mehanna et al., 2015; Park et al., 2018; Joseph et al., 2020). MSC-CM was also injected (41.94%, 13/31), mainly subcutaneously (25.81%, 8/31) (Templin et al., 2009; Lee et al., 2011; Deng et al., 2017; He et al., 2020; Zhou et al., 2020) but also intradermally (Cho et al., 2010) and intraperitoneally (Fong et al., 2014). Subcutaneously injected and topically applied concomitant MSC-CM was also tested (Chen et al., 2008; Yoon et al., 2010). Topical application might be more effective than subcutaneous injections (Lee et al., 2011).
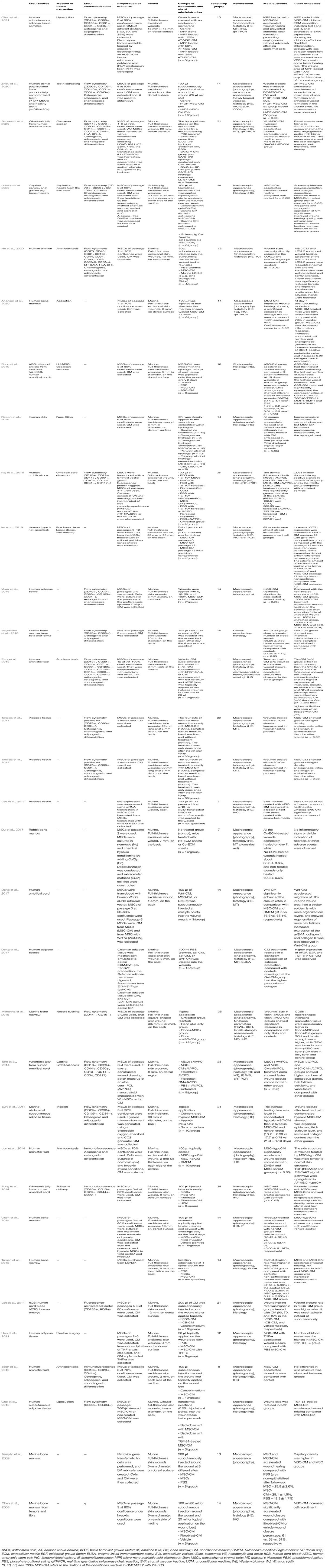
Table 1. Studies regarding mesenchymal stromal cell-conditioned medium for treating wounds in animal models.
MSC-CM was tested for treating wounds in 421 animals. The mean wound size was 11.65 mm (from 2 to 35 mm), and the mean follow-up was 16.48 days (from 5 to 35 days). Wounds were assessed mainly by macroscopic appearance, histology, immunohistochemistry, and qRT-PCR. Outcomes showed that MSC-CM had better results in terms of wound closure, re-epithelialization, and vascularization than non-treated groups or other treatment groups (phosphate-buffered saline (PBS), hydrogel without cells, Dulbecco’s modified Eagle medium (DMEM), and unconditioned medium). Moreover, some research compared the effects between MSCs and MSC-CM with similar results. Topically applied MSCs and their CM via fibrin vehicle showed similar wound healing rates (Mehanna et al., 2015). Healing rates, vascularity, and cellular density were similar between MSCs and MSC-CM injected intraperitoneally (Fong et al., 2014). Injections of MSCs or MSC-CM around the wound showed similar results in wound healing (Templin et al., 2009; Tamari et al., 2013) (non-epithelialized area after 14 days’ follow-up: 25.9 ± 2.6% in MSCs and 25.1 ± 1.5% in the MSC-CM group).
Different MSC sources and CM delivery were also compared. Allogeneic MSC-CM showed better healing rate than xenogeneic MSC-CM treatment (Joseph et al., 2020). The wound closure rate was higher in animals treated with carrageenan-embedded CM than mice treated with polyvinyl alcohol-embedded CM (Robert et al., 2019). Moreover, CM supplemented with selenium and basic fibroblast growth factor (bFGF) showed better results in wound healing than CM alone or CM only supplemented with bFGF or selenium, as complete wound closure after 11 days’ follow-up was only observed in CM supplemented with both growth factors (Park et al., 2018). Hypoxic conditions also improved wound healing, accelerating wound closure (Chen et al., 2014; Jun et al., 2014; Sun et al., 2014; Du et al., 2017). TNF-α- and TFG-β1-implemented CM also accelerated wound healing as compared with non-supplemented MSC-CM (Cho et al., 2010; Heo et al., 2011). CM derived from Wnt7a-transduced MSCs also showed higher closures rates than did the MSC-CM group (Dong et al., 2017). No adverse events were reported in these studies.
Nineteen studies evaluated the effects of MSC-CM for treating diabetic wounds (Table 2). To obtain CM, cells were mainly isolated from human tissues (89.47%, 17/19): from umbilical cord blood (Kim et al., 2010; Kusindarta et al., 2016; Chen Z. et al., 2018; Raj et al., 2019; Zhang S. et al., 2020) (29.41%, 5/17), bone marrow (Pouriran et al., 2016; Amini et al., 2018; Bagheri et al., 2018; Saheli et al., 2020) (23.53%, 4/17), adipose tissue (Deng et al., 2019; De Gregorio et al., 2020) (11.76%, 2/17), and Wharton’s jelly (Fong et al., 2014; Tam et al., 2014) (11.76%, 2/17). Human hair follicles (Ma et al., 2015), menstrual blood (Dalirfardouei et al., 2019), and urine (Chen C. Y. et al., 2018) were also used. Moreover, murine (Li T. et al., 2019) and swine (Irons et al., 2018) adipose tissues were employed. CM was collected from MSCs between passages 1 and 12 at 50–100% confluence. The most common model was murine (94.12%, 16/17), although a swine model was also used (Irons et al., 2018). Regarding the route of administration, MSC-CM was injected (78.95%, 15/19) mainly intraperitoneally (26.31%, 5/19) (Fong et al., 2014; Pouriran et al., 2016; Amini et al., 2018; Bagheri et al., 2018; Saheli et al., 2020), subcutaneously (15.79%, 3/19) (Chen C. Y. et al., 2018; Li T. et al., 2019; Zhang S. et al., 2020), intradermally (15.79%, 3/19) (Kim et al., 2010; Dalirfardouei et al., 2019; Deng et al., 2019), or intravenously (5.26%, 1/19) (De Gregorio et al., 2020). MSC-CM was also applied topically (21.05%, 4/19) to the wounds or around them in creams, hydrogels, or membranes (Kusindarta et al., 2016; Chen Z. et al., 2018; Irons et al., 2018).

Table 2. Studies regarding mesenchymal stromal cell-conditioned medium for treating diabetic wounds in animal models.
MSC-CM has been tested on 256 animals with diabetic wounds. The mean wound size was 13.47 mm (from 3.5 to 50 mm), and the mean follow-up was 18.83 days (from 9 to 28 days). Wounds were assessed mainly by macroscopic appearance, histology, immunohistochemistry, and qRT-PCR. MSC-CM had better results in terms of wound closure, re-epithelialization, and vessel formation than non-treated groups or other treatment groups (PBS, hydrogel without cells, DMEM, unconditioned medium, or povidone iodine). Moreover, some studies compared the effect between cells and its CM with similar results (Kim et al., 2010; Fong et al., 2014; Tam et al., 2014; Irons et al., 2018; Dalirfardouei et al., 2019; Zhang S. et al., 2020). MSC-CM was also used to heal wounds in combination with laser therapy, showing that the combined treatment enhanced wound healing compared with laser or MSC-CM alone (Pouriran et al., 2016; Amini et al., 2018; Bagheri et al., 2018).
Different ways of CM implementation have been also evaluated. CM supplemented with deferoxamine, a hypoxic mimetic agent, had a more potent effect on recovering skin vasculatures than non-supplemented CM (De Gregorio et al., 2020). DMBT1 expression also improves wound healing (Chen C. Y. et al., 2018). Moreover, CM cultured on polydopamine-modified three-dimensional-printed bioceramic (DOPA-BC) scaffolds showed a higher healing rate than CM cultured on tissue culture plates (TCPs) or pure three-dimensional-printed bioceramic (pure BC) (Li T. et al., 2019). After 14 days’ follow-up, the remaining wound area was 7.1 ± 3.4% in the DOPA-BC-CM group, 15.2 ± 6.6% in the BC-CM group, and 21.2 ± 11.3% in TCP-CM group (Li T. et al., 2019).
MSC-CM was also evaluated in second- and third-degree burn wounds (Aryan et al., 2019; Li J. Y. et al., 2019; Zhou et al., 2019), radiation-induced wounds (Sun et al., 2019), and infected wounds (Fridoni et al., 2019; Kouhkheil et al., 2019; Table 3). Cells were isolated from human tissues: bone marrow (Aryan et al., 2019; Fridoni et al., 2019; Kouhkheil et al., 2019), umbilical cord (Zhou et al., 2019), Wharton’s jelly (Sun et al., 2019), and placenta (Li J. Y. et al., 2019). MSCs from passages 3 to 8 at 60–80% confluence were used. All tested models were murine.
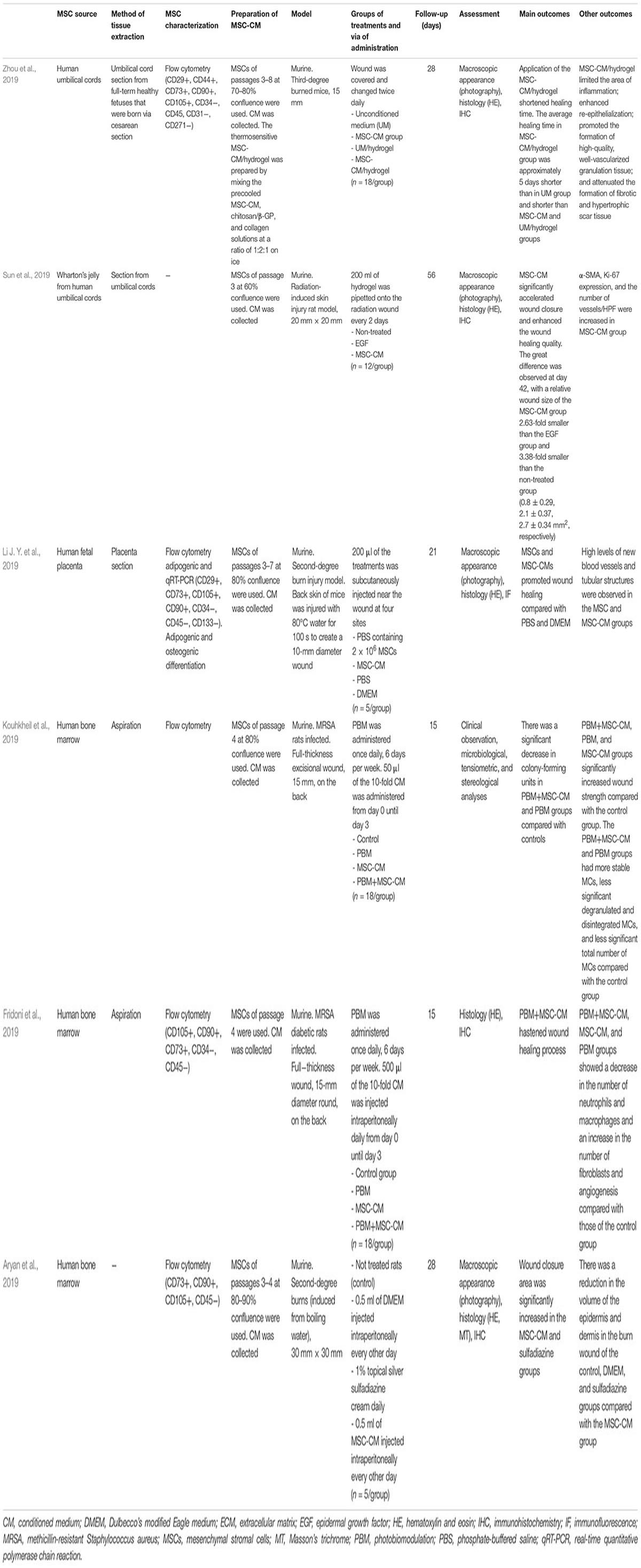
Table 3. Studies regarding mesenchymal stromal cell-conditioned medium for treating other types of wounds in animal models.
Twenty-eight mice with burn wounds were treated with MSC-CM with a mean follow-up of 25.67 days (from 21 to 28 days). MSC-CM was tested using subcutaneous (Li J. Y. et al., 2019) or intraperitoneal (Aryan et al., 2019) injections or topically applied (Zhou et al., 2019). In burn wounds, MSC-CM showed faster wound healing, increased re-epithelialization, and vascularization compared with controls (unconditioned medium, PBS, or DMEM).
Moreover, 72 mice infected with methicillin-resistant Staphylococcus aureus were treated with MSC-CM or MSC-CM plus photobiomodulation (PBM). MSC-CM plus PBM decreased colony-forming units and the number of inflammatory cells (Fridoni et al., 2019; Kouhkheil et al., 2019).
Twelve mice with radiation-induced skin injuries were also treated with MSC-CM. Topical application of MSC-CM in hydrogel accelerated wound closure and enhanced the wound healing quality (Sun et al., 2019).
Five studies evaluated the effects of MSC-CM combined with PBM or pulsed wave low-level laser therapy (PWLLLT) for treating diabetic wounds and infected wounds (Pouriran et al., 2016; Amini et al., 2018; Bagheri et al., 2018; Fridoni et al., 2019; Kouhkheil et al., 2019) (Supplementary Table 1). Regarding diabetic wounds, the results are controversial (Pouriran et al., 2016; Amini et al., 2018; Bagheri et al., 2018). Two studies showed that MSC-CM, PBM, and the combined therapy improved wound healing as compared with control group (Pouriran et al., 2016; Bagheri et al., 2018). Moreover, it was found that the extent of healing was significantly greater in the MSC-CM+PBM group (Amini et al., 2018). On the other hand, it was showed that PWLLLT and MSC-CM, alone or in combination, improved biomechanical parameters in the wound but that PWLLLT was more effective compared with MSC-CM (Pouriran et al., 2016). Concerning infected wounds, it was observed that both PBM+MSC-CM and PBM groups decreased colony-forming units and hastened wound healing process as compared with controls, while it did not happen when using MSC-CM alone (Fridoni et al., 2019; Kouhkheil et al., 2019).
Only one clinical study evaluated the effects of MSC-CM on wound healing (Table 4). This research assessed the use of MSC-CM derived from human amniotic membrane for treating chronic plantar ulcers in leprosy. The mean age of the patients was 52.12 ± 1.33 years, the mean ulcer duration was 1.41 ± 0.36 years, and the mean ulcer size at baseline was 2.64 ± 0.5 cm2 with a depth lower than 0.5 cm. Sixty-six patients were divided into groups to receive MSC-CM, MSC-CM+vitamin C, or MSC-CM+vitamin E topically applied every 3 days for 8 weeks. All groups improved wound healing, with MSC-CM+vitamin E being the most effective treatment. Wound size was reduced by 1.7 ± 1.05 vs. 2.01 ± 1.19 vs. 2.84 ± 1.67 cm2; and depth was decreased by 0.35 ± 0.14 vs. 0.25 ± 0.11 vs. 0.27 ± 0.15 cm in MSC-CM, MSC-CM+vitamin C, and MSC-CM+vitamin E groups, respectively. No adverse events were reported (Prakoeswa et al., 2018).
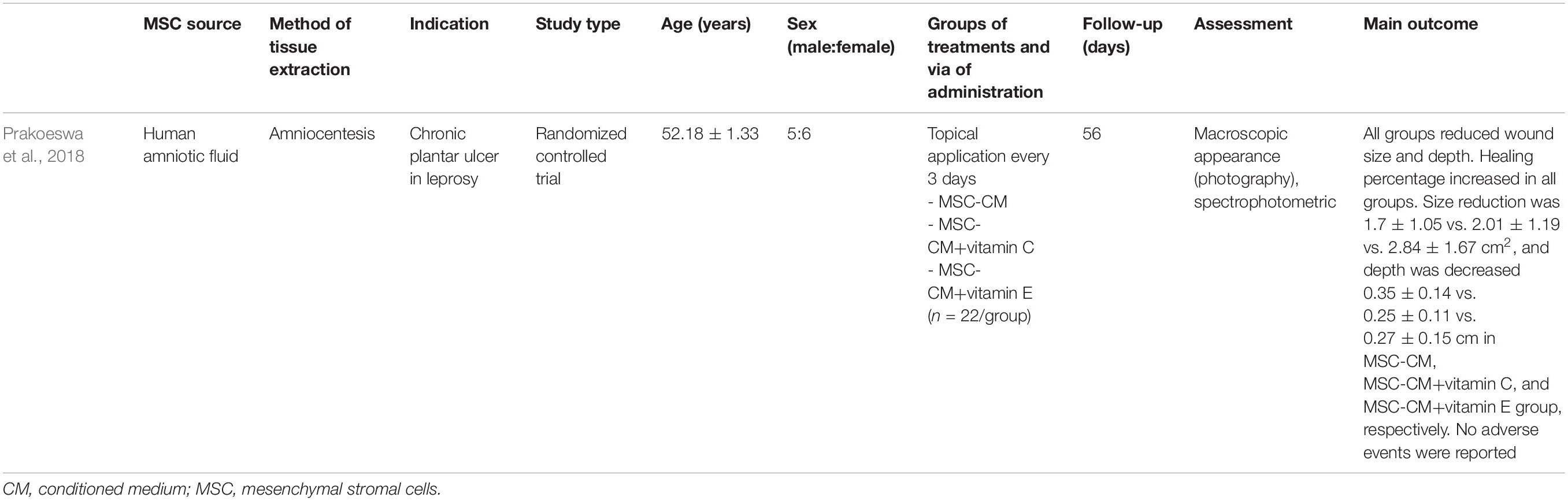
Table 4. Studies regarding mesenchymal stromal cell-conditioned medium for treating wounds in human.
Nine studies evaluated the potential of MSC-CM in the treatment of hypertrophic scars or avoiding scar formation (Wu et al., 2015; Zhang et al., 2015; Du et al., 2016a, b; Li et al., 2016; Choi et al., 2017; Liu et al., 2018; Arjunan et al., 2020; Hu et al., 2020; Table 5). To obtain CM, MSCs were mainly isolated from human tissues: adipose tissue (Li et al., 2016; Choi et al., 2017; Liu et al., 2018) (33.33%, 3/9), umbilical cord blood (Arjunan et al., 2020), placenta (Du et al., 2016a), and bone marrow (Wu et al., 2015). Murine bone marrow (Hu et al., 2020), murine placenta (Du et al., 2016b), and rabbit adipose tissue (Zhang et al., 2015) were also used. CM was collected from MSCs between passages 3 and 13 at 70–90% confluence. The most common model was murine (88.89%, 8/9), although a rabbit model was also used (Zhang et al., 2015). CM was used mainly by subcutaneous injection (66.66%, 6/9) (Wu et al., 2015; Du et al., 2016a, b; Li et al., 2016; Liu et al., 2018; Hu et al., 2020). Intralesional (Zhang et al., 2015; Arjunan et al., 2020) and intravenous (Choi et al., 2017) injections were also used. MSC-CM was tested in 97 animals for treating hypertrophic scar and keloids or preventing scar formation. The mean follow-up time was 23 days. Scars were assessed mainly by macroscopic appearance, histology, immunohistochemistry, and qRT-PCR.
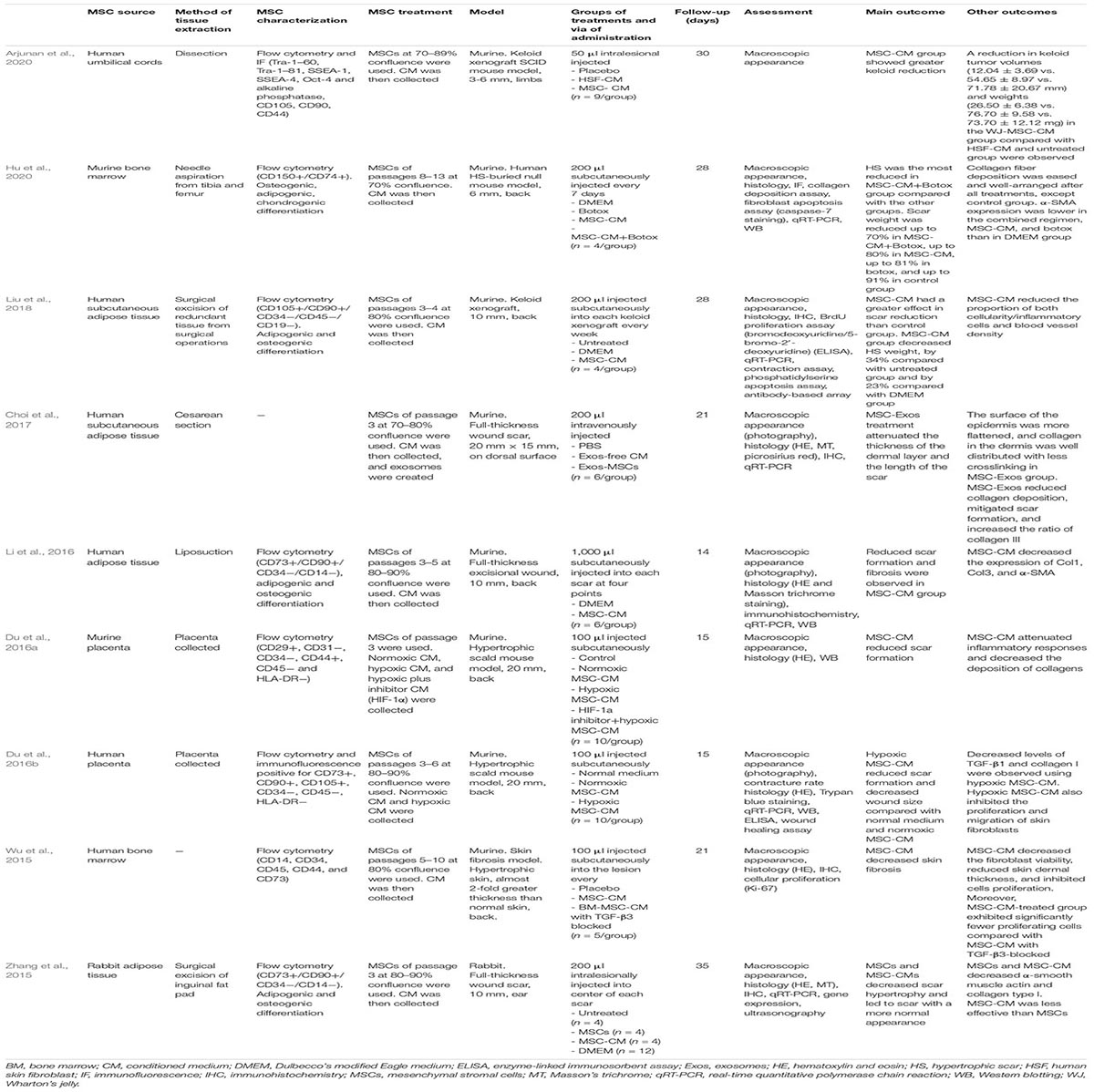
Table 5. Studies regarding mesenchymal stromal cell-conditioned medium for treating hypertrophic scars in animal models.
Mesenchymal stromal cell-CM had better results than non-treated groups or other treatments groups (PBS, DMEM, and unconditioned medium) in terms of tumor volumes, tumor weight, collagen fiber deposition, and skin fibrosis. CM derived from MSCs cultured in hypoxic conditions showed greater effects on scar formation than cultured in normoxic conditions (Du et al., 2016a, b). Moreover, the MSC-CM-treated group exhibited significantly fewer proliferating cells than did MSC-CM with TGF-β3 blocked, showing that TGF-β3 may be responsible for parts of the antifibrotic effect of the MSC-CM (Wu et al., 2015). The combination of MSC-CM and botulinum toxin type A (botox) had a greater effect when treating human hypertrophic scars than did botox alone, MSC-CM alone, or DMEM. Scar weight was reduced by 21, 11, or 10% more compared with DMEM, MSC-CM, or botox, respectively (Hu et al., 2020). Although both MSCs and MSC-CMs reduced hypertrophic scars, MSC-CM might be more effective than MSCs (Zhang et al., 2015). The Scar Elevation Index was reduced in both MSC- and MSC-CM-treated groups compared with internal controls (44.04 and 32.48%, p < 0.01, respectively), and it was significantly lower in the MSC-treated group than in the MSC-CM-treated group (p < 0.01) (Zhang et al., 2015).
No clinical study specifically evaluated the effects of MSC-CM on hypertrophic scar formation. Nevertheless, the effect of MSC-CM has been tested on acne scars in combination with laser therapy, showing that combined therapy had a greater effect on reducing acne scars than laser alone (Zhou et al., 2016; Abdel-Maguid et al., 2019; El-Domyati et al., 2019; Park C. S. et al., 2019). These studies are further developed in the Skin Rejuvenation section.
Four studies evaluated the effects of MSC-CM for treating ischemic wounds or flaps (Mirabella et al., 2012; Lee S. M. et al., 2014; Cooper et al., 2018; Pu et al., 2019; Table 6). MSCs were isolated from human adipose tissue (Lee S. M. et al., 2014; Cooper et al., 2018; Pu et al., 2019) or human amniotic fluid (Mirabella et al., 2012). CM was collected from MSCs between passages 3 and 8 at 70–90% confluence. All the models employed were murine.

Table 6. Studies regarding mesenchymal stromal cell-conditioned medium for improving flaps reperfusion in animal models.
Two studies tested MSC-CM in ischemia/reperfusion flap models by clamping the flap and then releasing it. Pu et al. evaluated the effects of MSC-CM applied to the subcutaneous layer between the flap and its bed and at the proximal, middle, and distal parts as compared with saline (n = 6/group) (Pu et al., 2019). A porcine skin-derived gelatine membrane soaked in either MSC-CM or saline was also tested (n = 5/group) (Mirabella et al., 2012). Both studies observed that the MSC-CM treatment group enhanced skin flap recovery, attenuated the necrotic area, increased hair growth, and stimulated angiogenesis as compared with controls (Mirabella et al., 2012; Pu et al., 2019).
MSC-CM were also applied topically on flap ischemic wounds in six mice. It was observed that MSC-CM accelerated the closure of flap ischemic wounds by 50% as compared with controls (Cooper et al., 2018). MSC-CM was also tested on skin allografts, intravenously injected, and compared with placebo and MSCs. MSCs and MSC-CMs increased skin allograft survival as compared with the control (23.9 ± 2.0, 19.6 ± 2.4, and 9.3 ± 1.4 days, respectively), without any differences between MSCs and MSC-CMs (Lee S. M. et al., 2014).
There are no studies at the clinical level.
Ten studies evaluated the effect of MSC-CM on hair growth at the preclinical level (Park et al., 2010; Won et al., 2010, 2015; Dong et al., 2014; Shim, 2015; Choi et al., 2019; Gunawardena et al., 2019a; Park J. et al., 2019; Ou et al., 2020; Xiao et al., 2020; Table 7). MSCs were isolated mainly from human hair follicles (Won et al., 2010; Won et al., 2015; Gunawardena et al., 2019a; Ou et al., 2020) (40%, 4/10) and human adipose tissue (Park et al., 2010; Choi et al., 2019; Xiao et al., 2020) (30%, 3/10). Other tissues used were human amniotic fluid (Park J. et al., 2019), human deciduous teeth (Gunawardena et al., 2019a), human dermal cells (Shim, 2015), and murine bone marrow (Dong et al., 2014). CM was collected from MSCs between passages 2 and 6 at 50–100% confluence. All studies employed murine models.
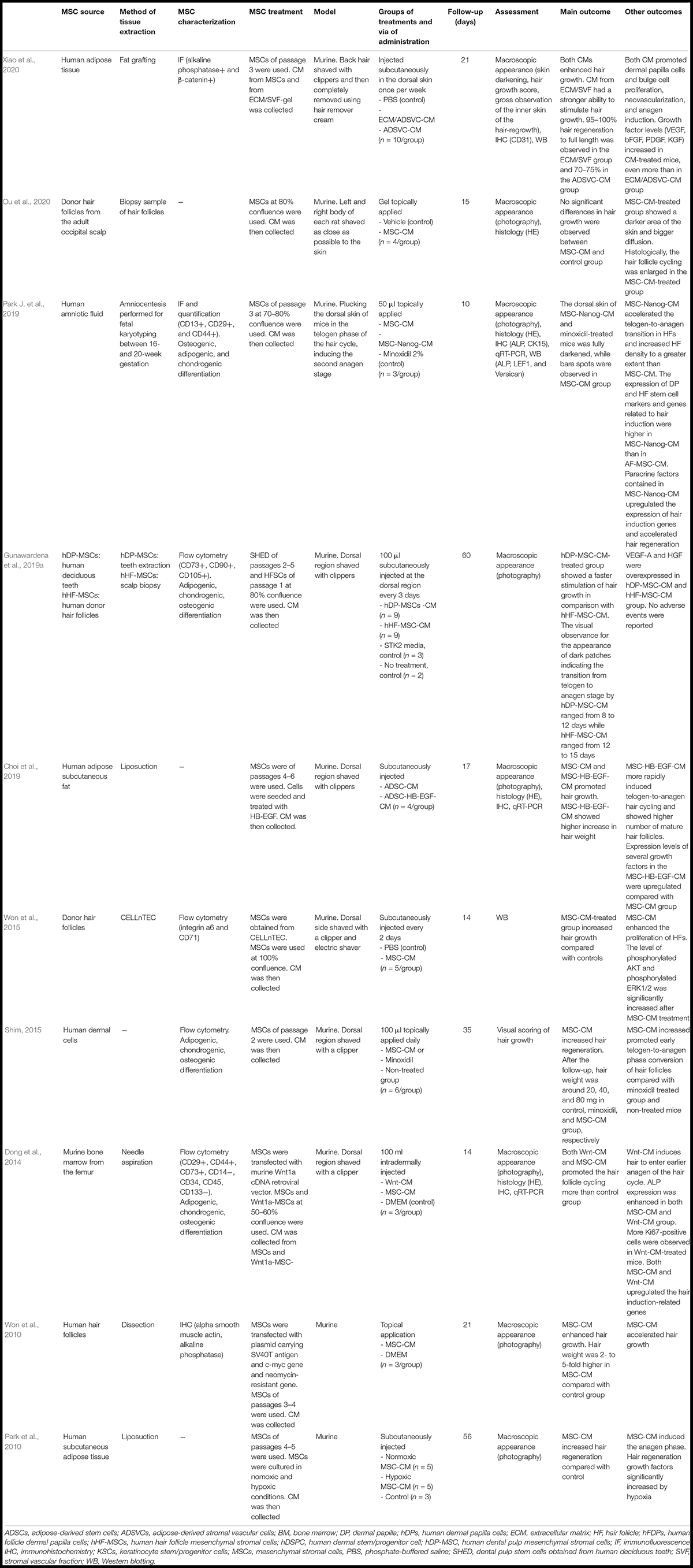
Table 7. Studies regarding mesenchymal stromal cell-conditioned medium for hair restoration in animal models.
Mesenchymal stromal cell-CM was used subcutaneously (Park et al., 2010; Won et al., 2015; Choi et al., 2019; Gunawardena et al., 2019a; Xiao et al., 2020) (50%, 5/10) or intradermally (Dong et al., 2014) injected or topically applied (Won et al., 2010; Shim, 2015; Park J. et al., 2019; Ou et al., 2020) (40%, 4/10). MSC-CM was tested on 86 animals with shaved regions. The mean follow-up time was 26.3 days (from 10 to 60 days). Hair growth improvement was assessed mainly by macroscopic appearance (skin darkening and hair weight) or histology. It was found that MSCs enhanced hair growth compared with control group (PBS, minoxidil, or DMEM). Hair weight in the MSC-CM group increased by 40 mg as compared with that in the non-treated groups and by 20 mg as compared with that in the minoxidil group (Shim, 2015). MSC-CM stimulated hair growth by promoting dermal papilla cell proliferation, accelerating telogen-to-anagen transition, and promoting neovascularization.
The overexpression of a reprogramming factor in the CM, Nanog, improved hair induction even more than MSC-CM without Nanog (Park J. et al., 2019). Moreover, it was observed that CM collected from human deciduous teeth accelerated hair growth more than CM derived from hair follicle cells. The transition from telogen to anagen stage for teeth-MSC-CM was between 8 and 12 days, while that at hair follicle-MSC-CM ranged from 12 to 15 days (Gunawardena et al., 2019a). CM enrichment with heparin binding-epidermal growth factor-like growth factor (HB-EGF) showed a greater effect in promoting hair growth compared with non-supplemented CM (Choi et al., 2019). Furthermore, CM collected from MSCs cultured in hypoxic conditions increased hair regeneration growth factors (Park et al., 2010). No adverse events were reported when using MSC-CM in hair restoration.
Four clinical studies evaluated the effects of MSC-CM on hair growth (Shin et al., 2015; Lee et al., 2020; Narita et al., 2020; Oh et al., 2020; Table 8). To obtain CM, cells were isolated from human adipose tissue (Shin et al., 2015; Lee et al., 2020; Narita et al., 2020) (75%) and human umbilical cord blood (Oh et al., 2020) (25%). All studies evaluated the effect of MSC-CM in androgenetic alopecia (AGA). MSC-CM was tested on 100 patients, both men and women, with an age range of 23–74 years. Two observational studies used intradermal injections of human AT-MSC-CM and observed that hair density increased by 17.3 hairs/cm2 and hair thickness increased by 6.5 μm as compared with baseline (Shin et al., 2015; Narita et al., 2020). A clinical trial also evaluated the effects of human UC-MSC-CM enriched with TGF-1 and LiCl applied topically twice daily for 112 days. It was observed that MSC-CM increased hair density by 14.24%, hair thickness by 28.19%, and hair growth by 19.54% as compared with a placebo (Oh et al., 2020). Moreover, MSC-CM treatment was also evaluated in patients who underwent non-ablative fractional laser treatment for AGA. It was found that concomitant treatment (MSC-CM+laser) had a greater effect than laser treatment only. The MSC-CM group had greater hair density (102.1 ± 4.09 vs. 89.3 ± 3.79/cm2) and gross hair volume (2 ± 0.13 vs. 1.2 ± 0.19, evaluated by a 7-point global improvement score) than the placebo group after 12 weeks of treatment administration (Lee et al., 2020). No serious adverse events were reported in these studies.
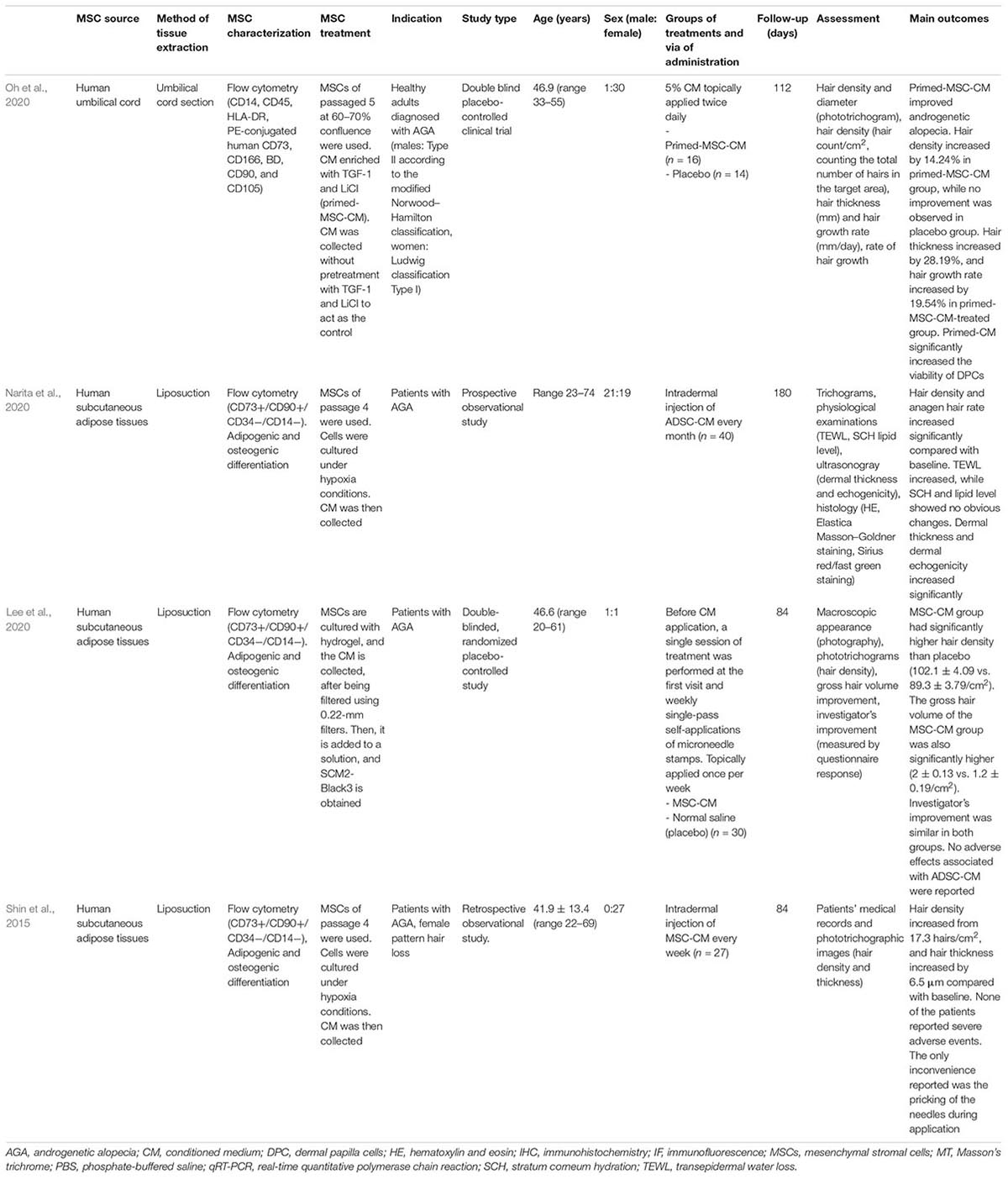
Table 8. Studies regarding mesenchymal stromal cell-conditioned medium for hair restoration in humans.
Three studies evaluated the effect of MSC-CM in 36 UV-induced photoaged mice (Ueda and Nishino, 2010; Kwon et al., 2016; Zhang K. et al., 2020; Table 9). MSCs were isolated from human umbilical cord (33.33%, 1/3) (Zhang K. et al., 2020), human bone marrow (33.33%, 1/3) (Kwon et al., 2016), and human dental pulp (33.33%, 1/3) (Ueda and Nishino, 2010). The mean follow-up was 35 days (from 14 to 35). MSC-CM reduced the level of wrinkles, improved transepidermal water loss (TEWL) and stratum corneum hydration (SCH) values, and increased collagen fibers than did vehicle or PBS. Nevertheless, the effect of MSC-CM on improving wrinkles was lower than that of MSCs (Ueda and Nishino, 2010).
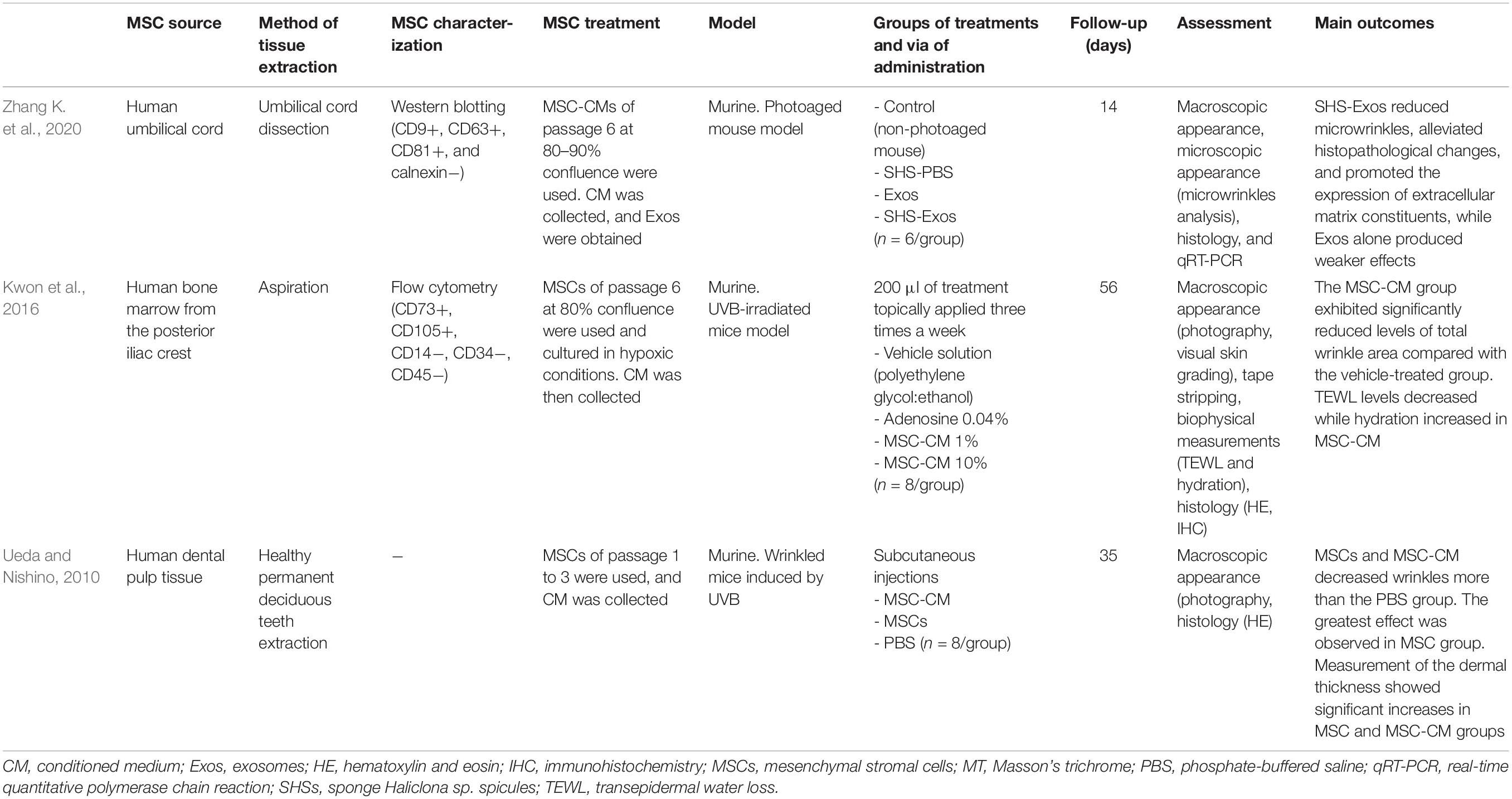
Table 9. Studies regarding mesenchymal stromal cell-conditioned medium for skin rejuvenation in animal models.
Twelve studies evaluated the effect of MSC-CM on skin wrinkles (Seo et al., 2013; Zhou et al., 2013; Lee S. M. et al., 2014; Xu et al., 2016; Kim et al., 2018; Prakoeswa et al., 2019; El-Domyati et al., 2020; Kim J. et al., 2020) and acne scars (Zhou et al., 2016; Abdel-Maguid et al., 2019; El-Domyati et al., 2019; Park C. S. et al., 2019; Table 10). MSCs were isolated from human tissues: adipose tissue (Zhou et al., 2013, 2016; Xu et al., 2016; Park C. S. et al., 2019) (30.77%, 4/13), amniotic fluid (Abdel-Maguid et al., 2019; El-Domyati et al., 2019, 2020; Prakoeswa et al., 2019) (30.77%, 4/13), umbilical cord blood (Kim et al., 2018; Kim J. et al., 2020) (15.38%, 2/13), human embryos (Seo et al., 2013; Lee S. M. et al., 2014) (15.38%, 2/13), and the placenta (Xu et al., 2016).
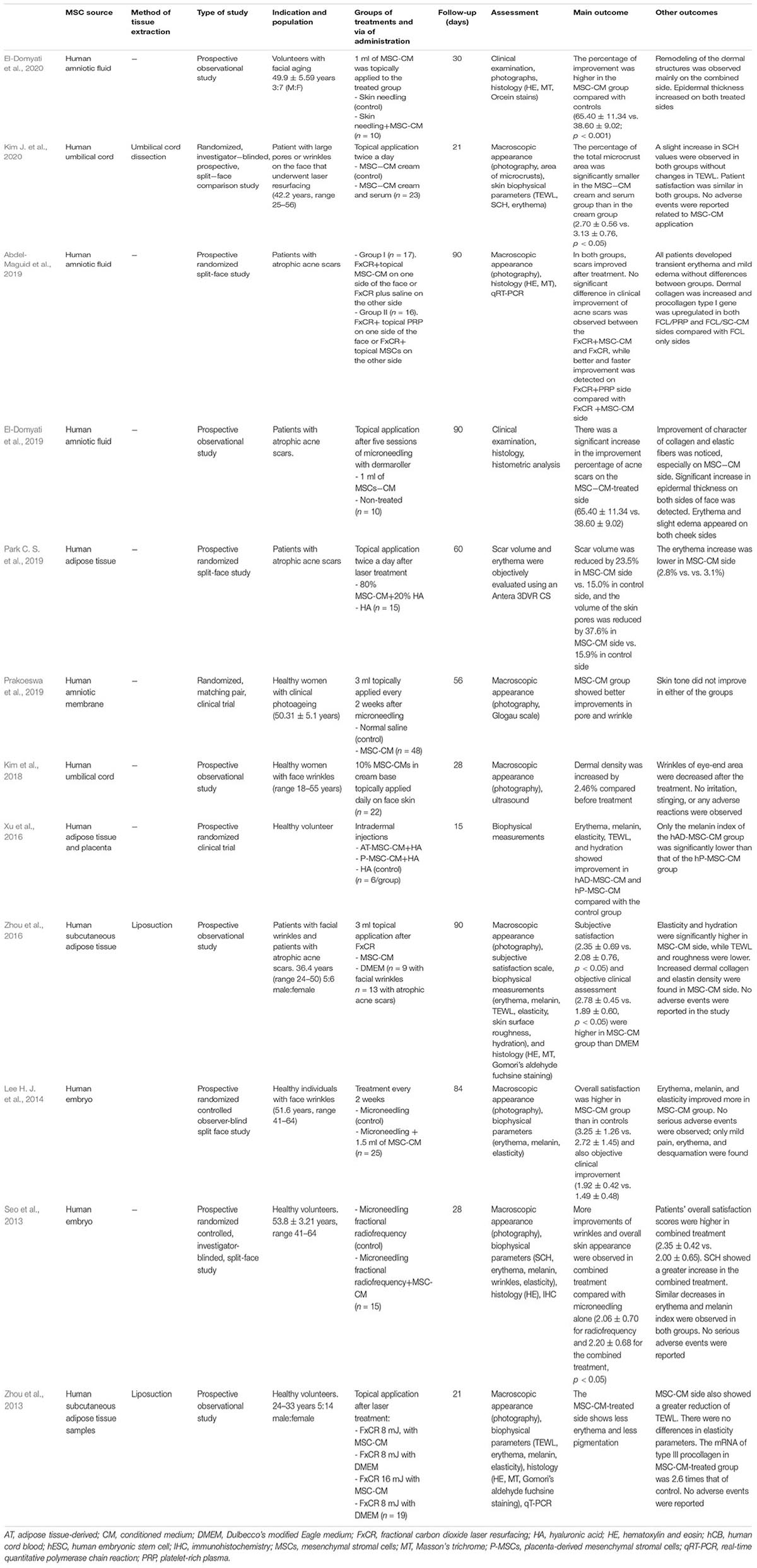
Table 10. Studies regarding mesenchymal stromal cell-conditioned medium for skin rejuvenation in humans.
Two hundred six healthy volunteers were treated with MSC-CM for anti-aging therapies (Seo et al., 2013; Zhou et al., 2013; Lee S. M. et al., 2014; Xu et al., 2016; Kim et al., 2018; Prakoeswa et al., 2019; El-Domyati et al., 2020; Kim J. et al., 2020). This research included women between 24 and 64 years. The studies evaluated the effects of microneedling, radiofrequency, or laser therapy alone compared with combined treatment with MSC-CM. They observed that combined therapy showed better improvement in macroscopic appearance (less pores and wrinkles), biophysical parameters (increased SCH and decreased TEWL, erythema, and melanin), and histology (increased dermal density) and had higher patient satisfaction scores. Similar results were found for the application of CM derived from human adipose tissue and human placenta, showing only a greater decrease in melanin index in the AT-MSC-CM group (Xu et al., 2016). The application of human UC-MSC-CM containing serum and cream on patients who underwent fractional laser therapy showed less microcrusts than the application of UC-MSC-CM only containing cream (Kim J. et al., 2020). No serious adverse events were observed in these reports.
Moreover, MSC-CM was also tested on acne scars (Zhou et al., 2016; Abdel-Maguid et al., 2019; El-Domyati et al., 2019; Park C. S. et al., 2019), suggesting that combined therapy (laser+MSC-CM) may increase the regenerative effects of fractional laser. Four studies evaluated the therapeutic potential in 71 patients with a mean follow-up of 82.5 days (range 60–90). After laser treatment, topical application of MSC-CM showed greater scar volume reduction than did with the control, by 23.5% on the MSC-CM side vs. 15.0% on the control side (Park C. S. et al., 2019). Furthermore, the MSC-CM-treated side improved subjective satisfaction and clinical assessment, showing better TEWL, SCH, elasticity, roughness, and collagen density than did the controls (laser alone or DMEM). Nevertheless, laser therapy+MSC-CM showed lower clinical improvement in acne scars than the combination of laser+platelet-rich plasma (Abdel-Maguid et al., 2019). Adverse events reported were erythema and edema, linked more to laser therapy than MSC-CM treatment.
One study evaluated the effect of CM derived from murine adipose tissue for treating atopic dermatitis (AD) (Park H. S. et al., 2019; Table 11). Mice were followed up 33 days after AD lesions had developed and treated with subcutaneous injections every 3 days with saline, MSC, MSC-CM, or 2.5% cortisone lotion (n = 6/group). A higher AD severity index decrease was observed in groups treated with MSC, MSC-CM, or cortisone, as compared with the saline group. Moreover, the severity index (assessed by SCORAD) was lower in the MSC-CM group treated with MSCs or cortisone. Skin thickness decreases were similar between MSC-CM, MSC, and cortisone, and all greater than in the saline group. Likewise, mast cell infiltration was reduced in MSC-CM, MSC, and cortisone groups. Th2 expression, measured in optical densities, was lower in the MSC-CM groups than in the MSC, cortisone, or saline group (1.58 ± 1.84 vs. 3.79 ± 2.08 vs. 4.10 ± 3.32 vs. 19.19 ± 5.54). Ig E levels were slightly reduced in mice that were treated with MSC, MSC-CM, or cortisone. IL-4 was also reduced in the group treated with MSC-CM (Park H. S. et al., 2019).
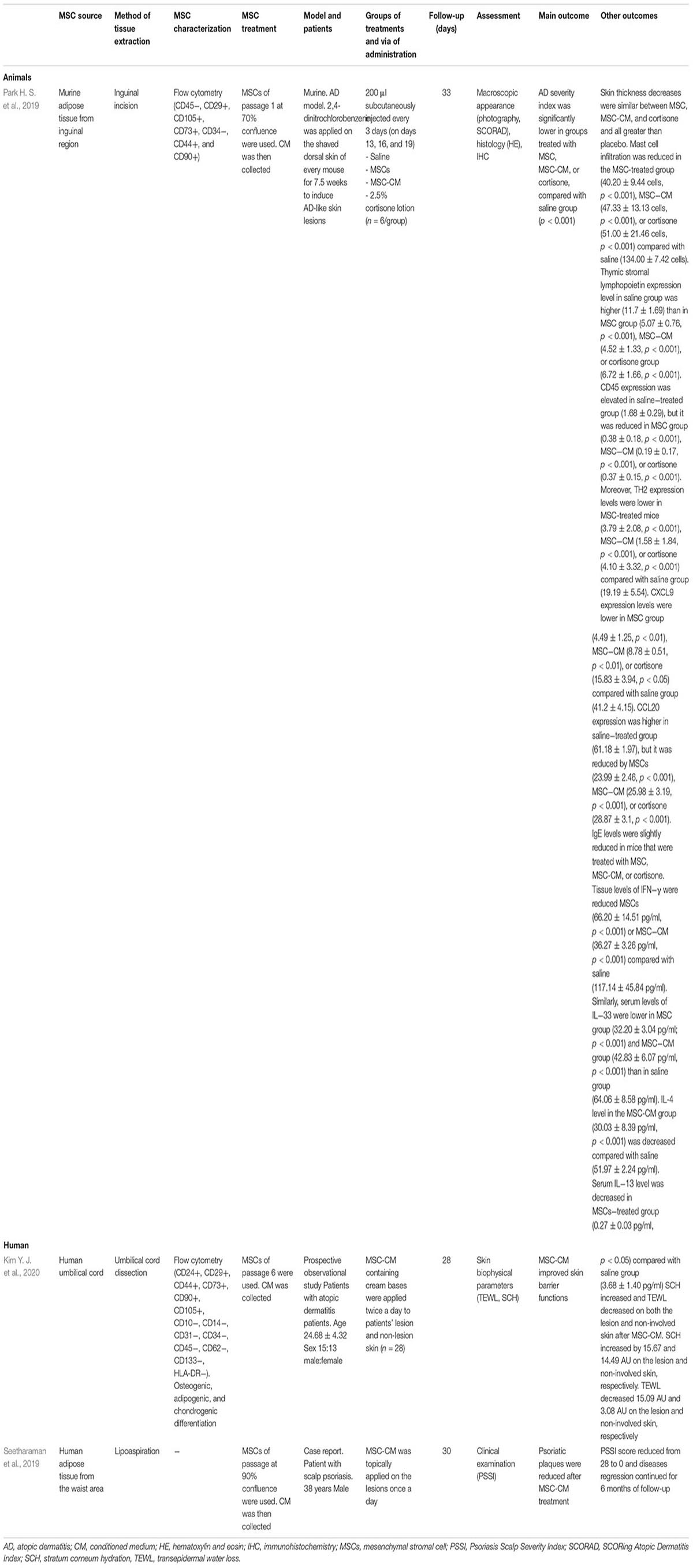
Table 11. Studies regarding mesenchymal stromal cell- conditioned medium for treating inflammatory skin diseases.
One study evaluated the effects of MSC-CM for treating AD (Kim Y. J. et al., 2020), and one case report showed the outcomes in a patient with scalp psoriasis treated with MSC-CM (Seetharaman et al., 2019; Table 11).
Twenty-eight patients (15 males and 13 females; mean age 24.68 ± 4.32 years) were treated with human UC-MSC-CM in cream bases for 4 weeks. MSC-CM was applied on both eczematous lesions and non-involved skin twice a day. After treatment, SCH increased by 15.67 arbitrary units (AU), a relative unit of measurement to show the ratio of amount of some quantities to a predetermined reference measurement, on eczematous lesions and 14.49 AU on non-involved skin. Moreover, TEWL decreased by 15.09 g⋅m−2⋅h−1 AU on eczematous lesions and 3.08 g⋅m−2⋅h−1 on non-involved skin (Kim Y. J. et al., 2020). In agreement with preclinical studies, these data showed that cosmetics that contained MSC-CM improved the skin barrier function and could be an effective treatment for AD patients.
One study also evaluated the clinical efficacy of MSC-CM derived from human adipose tissue for treating psoriasis scalp. A 38-year-old male was treated topically with MSC-CM on the lesions once a day. After 1-month follow-up, the number of psoriatic plaques was reduced and Psoriasis Scalp Severity Index (PSSI) changed from 28 to 0. Moreover, no relapse or adverse events were observed after 6 months’ follow-up (Seetharaman et al., 2019).
MSC-CM may be an alternative, safe, and easily delivered therapy for several skin conditions, but evidence in clinical studies is limited. They have been mainly tested in hair restoration (Shin et al., 2015; Lee et al., 2020; Narita et al., 2020; Oh et al., 2020) and skin rejuvenation (Abdel-Maguid et al., 2019; El-Domyati et al., 2019; Kim J. et al., 2020), with promising results. Preclinical studies are mainly focused on wound healing (Shin et al., 2015; Lee et al., 2020; Narita et al., 2020; Oh et al., 2020), showing high rates in wound closure. MSC-CM may also be an effective treatment for decreasing hypertrophic scars (Arjunan et al., 2020; Hu et al., 2020), improving flap reperfusion (Mirabella et al., 2012; Lee S. M. et al., 2014; Cooper et al., 2018; Pu et al., 2019), and treating psoriasis (Seetharaman et al., 2019) and AD (Park H. S. et al., 2019; Kim Y. J. et al., 2020). Nevertheless, there was significant variability between studies in the cell source, cell treatment, method of delivery, disease model used to assess efficacy, ways of assessment, and outcome evaluation. This review provides a useful summary regarding the use of MSC-CM for skin conditions and highlights the need to standardize manufacturing processes and characterize CM. The main findings of this review are summarized in Figure 2.
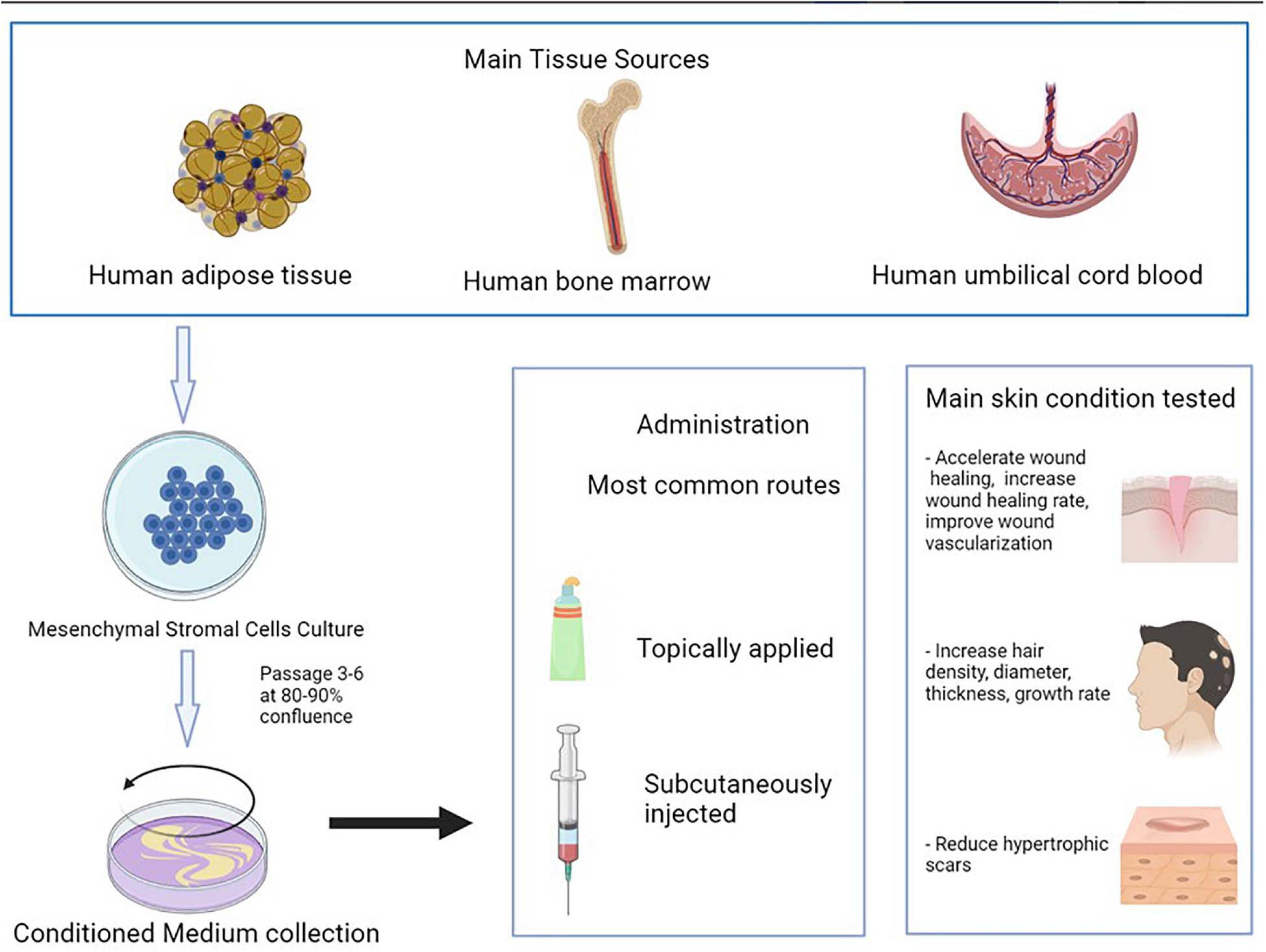
Figure 2. Iconographic summary of this review’s main findings.
It is important to characterize the composition of CM, but there is a lack of evidence in this aspect. Some studies showed that CM contained high concentrations of growth factors and cytokines associated with angiogenesis and endothelial cell migration such as EGF, tissue inhibitors of metalloproteinase-1, or IGF-binding protein-7 (De Gregorio et al., 2020; Kim Y. J. et al., 2020). The properties of MSC-CM vary depending on the cell source (Sagaradze et al., 2019). More than 10 sources of MSCs were used to treat skin conditions. MSCs were mainly isolated from human adipose tissue, human bone marrow, and human umbilical cord blood. Another important aspect is the timing of the collection of CM from the cells and concentration steps carried out for obtaining CM (Im et al., 2019). Most studies used cells from passages 3 to 6 at 80–90% confluence. The secretome of cells may also vary depending on the age of the cells (Maguire, 2013). Furthermore, the same type of cells is reported to secrete different levels of paracrine factors depending on the culture condition (Park et al., 2010) (hypoxic vs. normoxic) and the scaffold type (Li T. et al., 2019) (monolayer vs. 3D cultures). Hypoxic treatment is one of the most frequently used ways to improve CM, as hypoxic stress reduces oxygen and improves cellular functions (Du et al., 2017). CM collected from MSCs cultured under hypoxic conditions improved the cells’ capacities of proliferation and self-renewal (Chen et al., 2014; Jun et al., 2014; Du et al., 2016a, 2017). Determining the levels of paracrine factors secreted by MSCs at different passages with different conditions may also provide knowledge about the best stromal cell growth stage for obtaining a specific group of paracrine factors. Furthermore, MSC-CM should be considered both an alternative therapy and a synergic therapy for improving skin conditions, as MSC-CM combined with the conventional therapy has been proved to have better results than MSC-CM or the conventional therapy alone (Pouriran et al., 2016; Amini et al., 2018; Bagheri et al., 2018; Fridoni et al., 2019; Kouhkheil et al., 2019). In fact, some studies regarding wound healing in diabetic and infected wounds showed that PBM+MSC-CM application accelerated the process of wound healing, while it did not happen when using MSC-CM alone (Pouriran et al., 2016; Fridoni et al., 2019; Kouhkheil et al., 2019).
Several routes of administration have been also tested. Topical application and subcutaneous injection of CM were the most common routes of administration, and they are also the least invasive ways, appearing as promising routes for future research on MSC-CM.
No adverse events were reported to be related to MSC-CM in either preclinical or clinical trials. This is one of the main advantages of using MSC-CM instead of CM, as adverse events related to cells such as hyperimmunogenicity or tumorigenicity can be avoided (Gunawardena et al., 2019b). Only three studies evaluated differences between MSCs and MSC-CM, showing similar results between them (Tamari et al., 2013; Park H. S. et al., 2019; Zhang S. et al., 2020). Similar effectiveness was observed between UC-MSCs and UC-MSC-CM for accelerating wound healing rate. The wound area of UC-MSC and UC-MSC-CM was ≈15% reduced as compared with controls without differences in UC-MSC and UC-MSC-CM (Park H. S. et al., 2019; Zhang S. et al., 2020). Other research also showed similar epithelialization rate when using MSC or MSC-CM (Tamari et al., 2013). Moreover, it was observed that the effect of autologous AT-MSCs and AT-MSC-CM was similar for treating AD in mouse and higher than in the control group (Park H. S. et al., 2019).
It is also important to differentiate MSC-CM from culture media only. MSC-CM is the one in which MSCs have been grown for a period of time and with some requirements, and the culture media only is the media in which we grow the MSC-CM but has not been exposed to the cells. The culture media were used as control in some studies to prove the effectiveness of MSC-CM in wound healing (Jun et al., 2014; Deng et al., 2019; Rong et al., 2019). Higher wound healing rates and faster healing were observed with MSC-CM treatment than DMEM. Moreover, it was observed that hypertrophic scar reduction was higher using MSC-CM than DMEM (Zhang et al., 2015; Liu et al., 2018; Hu et al., 2020). It was also found that the topical application of MSC-CM after laser treatment showed less erythema and less pigmentation than the application of DMEM (Zhou et al., 2013, 2016). This might mean that the effect observed of MSC-CM in these diseases is due to the secretome and is not being caused by the culture media alone.
One of the limitations of MSC-CM is that, to translate its use to patients, it is necessary to know the exact composition of each CM and that its use validation should be conducted for every disease it is to be used for. Moreover, CM needs to be given more frequently than MSC, as the half-lives of cytokines and growth factors are mostly shorter than those of stromal cells, which may survive for rather long periods (Pawitan, 2014). Further research is needed to determine the components of MSC-CM that improves skin diseases. Moreover, regulatory requirements for manufacturing, standardization, and quality control of MSC-CM regarding MSC origin, isolation methods, and culture conditions are necessary to establish the safety and efficacy profiles of these products (Park H. S. et al., 2019).
Although there are some reviews regarding MSC-CM (Pawitan, 2014; Mizukami and Yagihashi, 2016; Bogatcheva and Coleman, 2019), they include little information about cutaneous disease. Pawitan et al. included some studies where MSC-CM was used for skin repair and alopecia. Bogatcheva and Coleman only included two articles where MSC-CM was used for skin diseases, one on treating dermatitis and the other on burns. Mizukami and Yagihashi reviewed the status of preclinical studies on stromal cell therapy for diabetic polyneuropathy, but they focused on MSCs and did not include information on other diseases. As far as we know, here, we review the use of MSC-CM in all skin conditions reported in the literature for the first time.
In conclusion, MSC-CM is a promising therapy for skin conditions. Studies on animals showed important rates of wound closure after MSC-CM treatment and clinical studies showed good results for skin rejuvenation. Further studies are needed to corroborate safety and effectiveness and to standardize CM manufacturing.
TM-V and SA-S contributed to conceptualization, formal analysis, investigation, and writing – original draft preparation. TM-V, ÁS-S, and SA-S contributed to methodology. AM-L contributed to software. TM-V, AM-L, and SA-S contributed to validation and visualization. MQ-V contributed to resources. TM-V, ÁS-S, MS-D, and MQ-V contributed to data curation. TM-V, SA-S, ÁS-S, and AM-L contributed to writing – review and editing. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcell.2021.654210/full#supplementary-material
AD, atopic dermatitis; AGA, androgenetic alopecia; AT, adipose tissue; BM, bone marrow; Botox, botulinum toxin type A; CM, conditioned medium; DMEM, Dulbecco’s modified Eagle medium; ECM, extracellular matrix; EV, extracellular vesicles; Exos, exosomes; HB-EGF, heparin binding-epidermal growth factor-like growth factor; HDFs, human dermal fibroblasts; HGF, hepatocyte growth factor; IGF, insulin-like growth factor; IL, interleukin; Men, menstrual blood; MSCs, mesenchymal stromal cells; PBS, phosphate-buffered saline; PSSI, Psoriasis Scalp Severity Index; qRT-PCR, real-time quantitative polymerase chain reaction; SCH, stratum corneum hydration (SCH); SCORAD, SCORing Atopic Dermatitis Index; SHSs, Haliclona sp. spicules; SDF − 1, stromal cell-derived factor 1; TEWL, transepidermal water loss; TGF- β, transforming growth factor β; Th2, lymphocyte T helper type 2; TNF- α, tumor necrosis factor α; UC, umbilical cord; VEGF, vascular endothelial growth factor.
Abdel-Maguid, E. M., Awad, S. M., Hassan, Y. S., El-Mokhtar, M. A., El-Deek, H. E., and Mekkawy, M. M. (2019). Efficacy of stem cell-conditioned medium vs. platelet-rich plasma as an adjuvant to ablative fractional CO2 laser resurfacing for atrophic post-acne scars: a split-face clinical trial. J. Dermatolog. Treat. 32, 242–249. doi: 10.1080/09546634.2019.1630701
Ahangar, P., Mills, S. J., Smith, L. E., Strudwick, X. L., Ting, A. E., Vaes, B., et al. (2020). Human multipotent adult progenitor cell-conditioned medium improves wound healing through modulating inflammation and angiogenesis in mice. Stem Cell Res. Ther. 11:299. doi: 10.1186/s13287-020-01819-z
Amini, A., Pouriran, R., Abdollahifar, M. A., Abbaszadeh, H. A., Ghoreishi, S. K., Chien, S., et al. (2018). Stereological and molecular studies on the combined effects of photobiomodulation and human bone marrow mesenchymal stem cell conditioned medium on wound healing in diabetic rats. J. Photochem. Photobiol. B 182, 42–51. doi: 10.1016/j.jphotobiol.2018.03.010
Arjunan, S., Gan, S. U., Choolani, M., Raj, V., Lim, J., Biswas, A., et al. (2020). Inhibition of growth of Asian keloid cells with human umbilical cord Wharton’s jelly stem cell-conditioned medium. Stem Cell Res. Ther. 11:78. doi: 10.1186/s13287-020-01609-7
Aryan, A., Bayat, M., Bonakdar, S., Taheri, S., Haghparast, N., Bagheri, M., et al. (2019). Human bone marrow mesenchymal stem cell conditioned medium promotes wound healing in deep second-degree burns in male rats. Cells Tissues Organs. 206, 317–329. doi: 10.1159/000501651
Bagheri, M., Amini, A., Abdollahifar, M. A., Ghoreishi, S. K., Piryaei, A., Pouriran, R., et al. (2018). Effects of photobiomodulation on degranulation and number of mast cells and wound strength in skin wound healing of streptozotocin-induced diabetic rats. Photomed Laser Surg. 36, 415–423. doi: 10.1089/pho.2018.4453
Bian, X., Li, B., Yang, J., Ma, K., Sun, M., Zhang, C., et al. (2020). Regenerative and protective effects of dMSC-sEVs on high-glucose-induced senescent fibroblasts by suppressing RAGE pathway and activating Smad pathway. Stem Cell Res. Ther. 11:166. doi: 10.1186/s13287-020-01681-z
Bogatcheva, N. V., and Coleman, M. E. (2019). Conditioned medium of mesenchymal stromal cells: a new class of therapeutics. Biochemistry (Mosc) 84, 1375–1389. doi: 10.1134/S0006297919110129
Caplan, A. I. (2017). Mesenchymal stem cells: time to change the name! Stem Cells Transl. Med. 6, 1445–1451. doi: 10.1002/sctm.17-0051
Caplan, H., Olson, S. D., Kumar, A., George, M., Prabhakara, K. S., Wenzel, P., et al. (2019). Mesenchymal stromal cell therapeutic delivery: translational challenges to clinical application. Front. Immunol. 10:1645. doi: 10.3389/fimmu.2019.01645
Chen, C. Y., Rao, S. S., Ren, L., Hu, X. K., Tan, Y. J., Hu, Y., et al. (2018). Exosomal DMBT1 from human urine-derived stem cells facilitates diabetic wound repair by promoting angiogenesis. Theranostics 8, 1607–1623. doi: 10.7150/thno.22958
Chen, L., Cheng, L., Wang, Z., Zhang, J., Mao, X., Liu, Z., et al. (2021). Conditioned medium-electrospun fiber biomaterials for skin regeneration. Bioact Mater. 6, 361–374. doi: 10.1016/j.bioactmat.2020.08.022
Chen, L., Tredget, E. E., Wu, P. Y., and Wu, Y. (2008). Paracrine factors of mesenchymal stem cells recruit macrophages and endothelial lineage cells and enhance wound healing. PLoS One 3:e1886. doi: 10.1371/journal.pone.0001886
Chen, L., Xu, Y., Zhao, J., Zhang, Z., Yang, R., Xie, J., et al. (2014). Conditioned medium from hypoxic bone marrow-derived mesenchymal stem cells enhances wound healing in mice. PLoS One 9:e96161. doi: 10.1371/journal.pone.0096161
Chen, Z., Pan, D., Hu, S., Yang, J., Zhou, L., and Shen, J. (2018). The combination of exosomes derived from umbilical cord mesenchymal stem cells and Pluronic F-127 promotes the proliferation and migration of vascular endothelial cells. Diabetes Metabolism Res. Rev. 34, 24–25. doi: 10.1002/dmrr.3079
Cho, J. W., Kang, M. C., and Lee, K. S. (2010). TGF-β1-treated ADSCs-CM promotes expression of type I collagen and MMP-1, migration of human skin fibroblasts, and wound healing in vitro and in vivo. Int. J. Mol. Med. 26, 901–906. doi: 10.3892/ijmm_00000540
Choi, N., Kim, W. S., Oh, S. H., and Sung, J. H. (2019). HB-EGF improves the hair regenerative potential of adipose-derived stem cells via ROS Generation and Hck Phosphorylation. Int. J. Mol. Sci. 21:122. doi: 10.3390/ijms21010122
Choi, Y. J., Lee, K. S., Yeom, S. H., and Cho, Y. W. (2017). Exosomes secreted by human adipose-derived stem cells regulate the expression of collagen synthesis-related genes in human dermal fibroblasts. J. Extracell. Vesicles 6:141. doi: 10.1080/20013078.2017.1310414
Cooper, D. R., Wang, C., Patel, R., Trujillo, A., Patel, N. A., Prather, J., et al. (2018). Human adipose-derived stem cell conditioned media and exosomes containing MALAT1 promote human dermal fibroblast migration and ischemic wound healing. Adv. Wound Care 7, 299–308. doi: 10.1089/wound.2017.0775
Dalirfardouei, R., Jamialahmadi, K., Jafarian, A. H., and Mahdipour, E. (2019). Promising effects of exosomes isolated from menstrual blood-derived mesenchymal stem cell on wound-healing process in diabetic mouse model. J. Tissue Eng. Regener. Med. 13, 555–568. doi: 10.1002/term.2799
De Gregorio, C., Contador, D., Diáz, D., Cárcamo, C., Santapau, D., Lobos-Gonzalez, L., et al. (2020). Human adipose-derived mesenchymal stem cell-conditioned medium ameliorates polyneuropathy and foot ulceration in diabetic BKS db/db mice. Stem Cell Res. Ther. 11:168. doi: 10.1186/s13287-020-01680-0
Deng, C., He, Y., Feng, J., Dong, Z., Yao, Y., and Lu, F. (2019). Conditioned medium from 3D culture system of stromal vascular fraction cells accelerates wound healing in diabetic rats. Regen. Med. 14, 925–937. doi: 10.2217/rme-2018-0083
Deng, C., He, Y., Feng, J., Dong, Z., Yao, Y., Mok, H., et al. (2017). Extracellular matrix/stromal vascular fraction gel conditioned medium accelerates wound healing in a murine model. Wound Repair Regen. 25, 923–932. doi: 10.1111/wrr.12602
Deng, H., Sun, C., Sun, Y., Li, H., Yang, L., Wu, D., et al. (2018). Lipid, Protein, and MicroRNA composition within mesenchymal stem cell-derived exosomes. Cell Reprogram 20, 178–186. doi: 10.1089/cell.2017.0047
Dominici, M., Le Blanc, K., Mueller, I., Slaper-Cortenbach, I., Marini, F., Krause, D., et al. (2006). Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy 8, 315–317. doi: 10.1080/14653240600855905
Dong, L., Hao, H., Liu, J., Ti, D., Tong, C., Hou, Q., et al. (2017). A conditioned medium of umbilical cord mesenchymal stem cells overexpressing Wnt7a promotes wound repair and regeneration of hair follicles in mice. Stem Cells Int. 2017:3738071. doi: 10.1155/2017/3738071
Dong, L., Hao, H., Xia, L., Liu, J., Ti, D., Tong, C., et al. (2014). Treatment of MSCs with Wnt1a-conditioned medium activates DP cells and promotes hair follicle regrowth. Sci. Rep. 4:5432. doi: 10.1038/srep05432
Du, H. C., Jiang, L., Geng, W. X., Li, J., Zhang, R., Dang, J. G., et al. (2017). Growth Factor-Reinforced ECM fabricated from chemically hypoxic msc sheet with improved in vivo wound repair activity. Biomed. Res. Int. 2017:2578017. doi: 10.1155/2017/2578017
Du, L., Lv, R., Yang, X., Cheng, S., Ma, T., and Xu, J. (2016a). Hypoxic conditioned medium of placenta-derived mesenchymal stem cells protects against scar formation. Life Sci. 149, 51–57. doi: 10.1016/j.lfs.2016.02.050
Du, L., Lv, R., Yang, X., Cheng, S., Xu, J., and Ma, T. (2016b). Hypoxia enhances the protective effects of placenta-derived mesenchymal stem cells against scar formation through hypoxia-inducible factor-1α. Biotechnol. Lett. 38, 931–939. doi: 10.1007/s10529-016-2067-6
El-Domyati, M., Moftah, N. H., Nasif, G. A., Ameen, S. W., Ibrahim, M. R., and Ragaie, M. H. (2020). Facial rejuvenation using stem cell conditioned media combined with skin needling: a split-face comparative study. J. Cosmetic Dermatol. 19, 2404–2410. doi: 10.1111/jocd.13594
El-Domyati, M., Moftah, N. H., Nasif, G. A., Ragaie, M. H., Ibrahim, M. R., and Ameen, S. W. (2019). Amniotic fluid-derived mesenchymal stem cell products combined with microneedling for acne scars: a split-face clinical, histological, and histometric study. J. Cosmetic Dermatol. 18, 1300–1306. doi: 10.1111/jocd.13039
Fong, C. Y., Tam, K., Cheyyatraivendran, S., Gan, S. U., Gauthaman, K., Armugam, A., et al. (2014). Human Wharton’s jelly stem cells and its conditioned medium enhance healing of excisional and diabetic wounds. J. Cell Biochem. 115, 290–302. doi: 10.1002/jcb.24661
Fridoni, M., Kouhkheil, R., Abdollhifar, M. A., Amini, A., Ghatrehsamani, M., Ghoreishi, S. K., et al. (2019). Improvement in infected wound healing in type 1 diabetic rat by the synergistic effect of photobiomodulation therapy and conditioned medium. J. Cell Biochem. 120, 9906–9916. doi: 10.1002/jcb.28273
Gunawardena, T. N. A., Masoudian, Z., Rahman, M. T., Ramasamy, T. S., Ramanathan, A., and Abu Kasim, N. H. (2019a). Dental derived stem cell conditioned media for hair growth stimulation. PLoS One 14:e0216003. doi: 10.1371/journal.pone.0216003
Gunawardena, T. N. A., Rahman, M. T., Abdullah, B. J. J., and Abu Kasim, N. H. (2019b). Conditioned media derived from mesenchymal stem cell cultures: the next generation for regenerative medicine. J. Tissue Eng. Regen. Med. 13, 569–586. doi: 10.1002/term.2806
Guo, S., Wang, T., Zhang, S., Chen, P., Cao, Z., Lian, W., et al. (2020). Adipose-derived stem cell-conditioned medium protects fibroblasts at different senescent degrees from UVB irradiation damages. Mol. Cell Biochem. 463, 67–78. doi: 10.1007/s11010-019-03630-8
He, D., Zhao, F., Jiang, H., Kang, Y., Song, Y., Lin, X., et al. (2020). LOXL2 from human amniotic mesenchymal stem cells accelerates wound epithelialization by promoting differentiation and migration of keratinocytes. Aging (Albany NY) 12, 12960–12986. doi: 10.18632/aging.103384
Heo, S. C., Jeon, E. S. I, Lee, H., Kim, H. S., Kim, M. B., and Kim, J. H. (2011). Tumor necrosis factor-α-activated human adipose tissue-derived mesenchymal stem cells accelerate cutaneous wound healing through paracrine mechanisms. J. Invest. Dermatol. 131, 1559–1567. doi: 10.1038/jid.2011.64
Hu, C. H., Tseng, Y. W., Lee, C. W., Chiou, C. Y., Chuang, S. S., Yang, J. Y., et al. (2020). Combination of mesenchymal stem cell-conditioned medium and botulinum toxin type A for treating human hypertrophic scars. J. Plast Reconstr. Aesthet Surg. 73, 516–527. doi: 10.1016/j.bjps.2019.07.010
Hu, L., Yin, C., Zhao, F., Ali, A., Ma, J., and Qian, A. (2018). Mesenchymal stem cells: cell fate decision to osteoblast or adipocyte and application in osteoporosis treatment. Int. J. Mol. Sci. 19:360. doi: 10.3390/ijms19020360
Im, G. B., Kim, Y. H., Kim, Y. J., Kim, S. W., Jung, E., Jeong, G. J., et al. (2019). Enhancing the wound healing effect of conditioned medium collected from mesenchymal stem cells with high passage number using bioreducible nanoparticles. Int. J. Mol. Sci. 20:4835. doi: 10.3390/ijms20194835
Irons, R. F., Cahill, K. W., Rattigan, D. A., Marcotte, J. H., Fromer, M. W., Chang, S., et al. (2018). Acceleration of diabetic wound healing with adipose-derived stem cells, endothelial-differentiated stem cells, and topical conditioned medium therapy in a swine model. J. Vasc. Surg. 68, 115s–125s. doi: 10.1016/j.jvs.2018.01.065
Joseph, A., Baiju, I., Bhat, I. A., Pandey, S., Bharti, M., Verma, M., et al. (2020). Mesenchymal stem cell-conditioned media: a novel alternative of stem cell therapy for quality wound healing. J. Cell. Physiol. 235, 5555–5569. doi: 10.1002/jcp.29486
Jun, E. K., Zhang, Q., Yoon, B. S., Moon, J. H., Lee, G., Park, G., et al. (2014). Hypoxic conditioned medium from human amniotic fluid-derived mesenchymal stem cells accelerates skin wound healing through TGF-β/SMAD2 and PI3K/Akt pathways. Int. J. Mol Sci. 15, 605–628. doi: 10.3390/ijms15010605
Kim, J., Kim, B., Kim, S., Lee, Y. I., Kim, J., and Lee, J. H. (2020). The effect of human umbilical cord blood–derived mesenchymal stem cell media containing serum on recovery after laser treatment: a double-blinded, randomized, split-face controlled study. J. Cosmetic Dermatol. 19, 651–656. doi: 10.1111/jocd.13063
Kim, J. Y., Song, S. H., Kim, K. L., Ko, J. J., Im, J. E., Yie, S. W., et al. (2010). Human cord blood-derived endothelial progenitor cells and their conditioned media exhibit therapeutic equivalence for diabetic wound healing. Cell Transplant. 19, 1635–1644. doi: 10.3727/096368910X516637
Kim, K. H., Blasco-Morente, G., Cuende, N., and Arias-Santiago, S. (2017). Mesenchymal stromal cells: properties and role in management of cutaneous diseases. J. Eur. Acad Dermatol. Venereol. 31, 414–423. doi: 10.1111/jdv.13934
Kim, Y. J., Ahn, H. J., Lee, S. H., Lee, M. H., and Kang, K. S. (2020). Effects of conditioned media from human umbilical cord blood-derived mesenchymal stem cells in the skin immune response. Biomed. Pharmacother. 118:109131. doi: 10.1016/j.biopha.2020.110789
Kim, Y. J., Seo, D. H., Lee, S. H., Lee, S. H., An, G. H., Ahn, H. J., et al. (2018). Conditioned media from human umbilical cord blood-derived mesenchymal stem cells stimulate rejuvenation function in human skin. Biochem. Biophys. Rep. 16, 96–102. doi: 10.1016/j.bbrep.2018.10.007
Kouhkheil, R., Fridoni, M., Abdollhifar, M. A., Amini, A., Bayat, S., Ghoreishi, S. K., et al. (2019). Impact of photobiomodulation and condition medium on mast cell counts, degranulation, and wound strength in infected skin wound healing of diabetic rats. Photobiomodul Photomed Laser Surg. 37, 706–714. doi: 10.1089/photob.2019.4691
Kusindarta, D. L., Wihadmadyatami, H., Fibrianto, Y. H., Nugroho, W. S., Susetya, H., Musana, D. K., et al. (2016). Human umbilical mesenchymal stem cells conditioned medium promote primary wound healing regeneration. Vet. World 9, 605–610. doi: 10.14202/vetworld.2016.605-610
Kwon, T. R., Oh, C. T., Choi, E. J., Kim, S. R., Jang, Y. J., Ko, E. J., et al. (2016). Conditioned medium from human bone marrow-derived mesenchymal stem cells promotes skin moisturization and effacement of wrinkles in UVB-irradiated SKH-1 hairless mice. Photodermatol. Photoimmunol. Photomed 32, 120–128. doi: 10.1111/phpp.12224
Lee, H. J., Lee, E. G., Kang, S., Sung, J. H., Chung, H. M., and Kim, D. H. (2014). Efficacy of microneedling plus human stem cell conditioned medium for skin rejuvenation: a randomized, controlled, blinded split-face study. Ann. Dermatol. 26, 584–591. doi: 10.5021/ad.2014.26.5.584
Lee, J. Y., Oh, N., and Park, K. S. (2017). Ell3 modulates the wound healing activity of conditioned medium of adipose-derived stem cells. Dev. Reprod. 21, 335–342. doi: 10.12717/dr.2017.21.3.335
Lee, M. J., Kim, J., Lee, K. I., Shin, J. M., Chae, J. I., and Chung, H. M. (2011). Enhancement of wound healing by secretory factors of endothelial precursor cells derived from human embryonic stem cells. Cytotherapy 13, 165–178. doi: 10.3109/14653249.2010.512632
Lee, S. M., Lee, S. C., and Kim, S. J. (2014). Contribution of human adipose tissue-derived stem cells and the secretome to the skin allograft survival in mice. J. Surg. Res. 188, 280–289. doi: 10.1016/j.jss.2013.10.063
Lee, Y. I., Kim, J., Kim, J., Park, S., and Lee, J. H. (2020). The effect of conditioned media from human adipocyte-derived mesenchymal stem cells on androgenetic alopecia after nonablative fractional laser treatment. Dermatol. Surg. 46, 1698–1704. doi: 10.1097/DSS.0000000000002518
Li, J. Y., Ren, K. K., Zhang, W. J., Xiao, L., Wu, H. Y., Liu, Q. Y., et al. (2019). Human amniotic mesenchymal stem cells and their paracrine factors promote wound healing by inhibiting heat stress-induced skin cell apoptosis and enhancing their proliferation through activating PI3K/AKT signaling pathway. Stem Cell Res. Ther. 10:247. doi: 10.1186/s13287-019-1366-y
Li, T., Ma, H., Ma, H., Ma, Z., Qiang, L., Yang, Z., et al. (2019). Mussel-Inspired nanostructures potentiate the immunomodulatory properties and angiogenesis of mesenchymal stem cells. ACS Appl. Mater. Interfaces 11, 17134–17146. doi: 10.1021/acsami.8b22017
Li, Y., Zhang, W., Gao, J., Liu, J., Wang, H., Li, J., et al. (2016). Adipose tissue-derived stem cells suppress hypertrophic scar fibrosis via the p38/MAPK signaling pathway. Stem Cell Res. Ther. 7:102. doi: 10.1186/s13287-016-0356-6
Liu, J., Ren, J., Su, L., Cheng, S., Zhou, J., Ye, X., et al. (2018). Human adipose tissue-derived stem cells inhibit the activity of keloid fibroblasts and fibrosis in a keloid model by paracrine signaling. Burns 44, 370–385. doi: 10.1016/j.burns.2017.08.017
Ma, D., Kua, J. E. H., Lim, W. K., Lee, S. T., and Chua, A. W. C. (2015). In vitro characterization of human hair follicle dermal sheath mesenchymal stromal cells and their potential in enhancing diabetic wound healing. Cytotherapy 17, 1036–1051. doi: 10.1016/j.jcyt.2015.04.001
Maguire, G. (2013). Stem cell therapy without the cells. Commun. Integr. Biol. 6:e26631. doi: 10.4161/cib.26631
Martinez-Lopez, A., Montero-Vilchez, T., Sierra-Sanchez, A., Molina-Leyva, A., and Arias-Santiago, S. (2020). Advanced medical therapies in the management of non-scarring alopecia: areata and androgenic alopecia. Int. J. Mol. Sci. 21:8390. doi: 10.3390/ijms21218390
Mehanna, R. A., Nabil, I., Attia, N., Bary, A. A., Razek, K. A., Ahmed, T. A., et al. (2015). The effect of bone marrow-derived mesenchymal stem cells and their conditioned media topically delivered in fibrin glue on chronic wound healing in rats. Biomed. Res. Int. 2015:846062. doi: 10.1155/2015/846062
Mirabella, T., Hartinger, J., Lorandi, C., Gentili, C., van Griensven, M., and Cancedda, R. (2012). Proangiogenic soluble factors from amniotic fluid stem cells mediate the recruitment of endothelial progenitors in a model of ischemic fasciocutaneous flap. Stem Cells Dev. 21, 2179–2188. doi: 10.1089/scd.2011.0639
Mizukami, H., and Yagihashi, S. (2016). Is stem cell transplantation ready for prime time in diabetic polyneuropathy? Curr. Diab. Rep. 16:86. doi: 10.1007/s11892-016-0776-9
Moll, G., Ankrum, J. A., Kamhieh-Milz, J., Bieback, K., Ringden, O., Volk, H. D., et al. (2019). Intravascular mesenchymal stromal/stem cell therapy product diversification: time for new clinical guidelines. Trends Mol. Med. 25, 149–163. doi: 10.1016/j.molmed.2018.12.006
Moll, G., Hoogduijn, M. J., and Ankrum, J. A. (2020). Editorial: safety, efficacy and mechanisms of action of mesenchymal stem cell therapies. Front. Immunol. 11:243. doi: 10.3389/fimmu.2020.00243
Montero-Vilchez, T., Segura-Fernandez-Nogueras, M. V., Perez-Rodriguez, I., Soler-Gongora, M., Martinez-Lopez, A., Fernandez-Gonzalez, A., et al. (2021). Skin barrier function in psoriasis and atopic dermatitis: transepidermal water loss and temperature as useful tools to assess disease severity. J. Clin. Med. 10:359. doi: 10.3390/jcm10020359
Narita, K., Fukuoka, H., Sekiyama, T., Suga, H., and Harii, K. (2020). Sequential scalp assessment in hair regeneration therapy using an adipose-derived stem cell-conditioned medium. Dermatol. Surg. 46, 819–825. doi: 10.1097/dss.0000000000002128
Oh, H. A., Kwak, J., Kim, B. J., Jin, H. J., Park, W. S., Choi, S. J., et al. (2020). Migration inhibitory factor in conditioned medium from human umbilical cord blood-derived mesenchymal stromal cells stimulates hair growth. Cells 9:1344. doi: 10.3390/cells9061344
Ou, K. L., Kuo, Y. W., Wu, C. Y., Huang, B. H., Pai, F. T., Chou, H. H., et al. (2020). The potential of a hair follicle mesenchymal stem cell-conditioned medium for wound healing and hair follicle regeneration. Appl. Sci. (Switzerland) 10:2646. doi: 10.3390/APP10082646
Park, B. S., Kim, W. S., Choi, J. S., Kim, H. K., Won, J. H., Ohkubo, F., et al. (2010). Hair growth stimulated by conditioned medium of adipose-derived stem cells is enhanced by hypoxia: evidence of increased growth factor secretion. Biomed. Res. 31, 27–34. doi: 10.2220/biomedres.31.27
Park, C. S., Park, J. H., Kim, C. R., and Lee, J. H. (2019). Objective analysis of volume restoration in atrophic acne scars and skin pores: a split study using human stem cell-conditioned media. J. Dermatol. Treat. 32, 73–77. doi: 10.1080/09546634.2019.1628915
Park, H. S., Son, H. Y., Choi, M. H., Son, Y., Kim, S., Hong, H. S., et al. (2019). Adipose-derived stem cells attenuate atopic dermatitis-like skin lesions in NC/Nga mice. Exp. Dermatol. 28, 300–307. doi: 10.1111/exd.13895
Park, J., Jun, E. K., Son, D., Hong, W., Jang, J., Yun, W., et al. (2019). Overexpression of Nanog in amniotic fluid-derived mesenchymal stem cells accelerates dermal papilla cell activity and promotes hair follicle regeneration. Exp. Mol. Med. 51:72. doi: 10.1038/s12276-019-0266-7
Park, J., Lee, J. H., Yoon, B. S., Jun, E. K., Lee, G. I., Kim, Y., et al. (2018). Additive effect of bFGF and selenium on expansion and paracrine action of human amniotic fluid-derived mesenchymal stem cells. Stem Cell Res. Ther. 9:293. doi: 10.1186/s13287-018-1058-z
Pawitan, J. A. (2014). Prospect of stem cell conditioned medium in regenerative medicine. Biomed. Res. Int. 2014:965849. doi: 10.1155/2014/965849
Payushina, O. V., Butorina, N. N., Sheveleva, O. N., and Domaratskaya, E. I. (2018). Effect of mesenchymal stromal cells and conditioned media on healing of skin wound. Bull. Exp. Biol. Med. 165, 572–575. doi: 10.1007/s10517-018-4215-6
Pouriran, R., Piryaei, A., Mostafavinia, A., Zandpazandi, S., Hendudari, F., Amini, A., et al. (2016). The effect of combined pulsed wave low-level laser therapy and human bone marrow mesenchymal stem cell-conditioned medium on open skin wound healing in diabetic rats. Photomed Laser Surg. 34, 345–354. doi: 10.1089/pho.2015.4020
Prakoeswa, C. R. S., Natallya, F. R., Harnindya, D., Thohiroh, A., Oktaviyanti, R. N., Pratiwi, K. D., et al. (2018). The efficacy of topical human amniotic membrane-mesenchymal stem cell-conditioned medium (hAMMSC-CM) and a mixture of topical hAMMSC-CM + vitamin C and hAMMSC-CM + vitamin E on chronic plantar ulcers in leprosy:a randomized control trial. J. Dermatol. Treat. 29, 835–840. doi: 10.1080/09546634.2018.1467541
Prakoeswa, C. R. S., Pratiwi, F. D., Herwanto, N., Citrashanty, I., Indramaya, D. M., Murtiastutik, D., et al. (2019). The effects of amniotic membrane stem cell-conditioned medium on photoaging. J. Dermatol. Treat. 30, 478–482. doi: 10.1080/09546634.2018.1530438
Pu, C. M., Chen, Y. C., Chen, Y. C., Lee, T. L., Peng, Y. S., Chen, S. H., et al. (2019). Interleukin-6 from adipose-derived stem cells promotes tissue repair by the increase of cell proliferation and hair follicles in ischemia/reperfusion-treated skin flaps. Mediators Inflamm. 2019:2343867. doi: 10.1155/2019/2343867
Raj, V., Claudine, S., Subramanian, A., Tam, K., Biswas, A., Bongso, A., et al. (2019). Histological, immunohistochemical, and genomic evaluation of excisional and diabetic wounds treated with human Wharton’s jelly stem cells with and without a nanocarrier. J. Cell. Biochem. 120, 11222–11240. doi: 10.1002/jcb.28398
Ratajczak, M. Z., Kucia, M., Jadczyk, T., Greco, N. J., Wojakowski, W., Tendera, M., et al. (2012). Pivotal role of paracrine effects in stem cell therapies in regenerative medicine: can we translate stem cell-secreted paracrine factors and microvesicles into better therapeutic strategies? Leukemia 26, 1166–1173. doi: 10.1038/leu.2011.389
Robert, A. W., Azevedo Gomes, F., Rode, M. P., Marques da Silva, M., Veleirinho, M., Maraschin, M., et al. (2019). The skin regeneration potential of a pro-angiogenic secretome from human skin-derived multipotent stromal cells. J. Tissue Eng. 10:2041731419833391. doi: 10.1177/2041731419833391
Rong, X., Chu, W., Zhang, H., Wang, Y., Qi, X., Zhang, G., et al. (2019). Antler stem cell-conditioned medium stimulates regenerative wound healing in rats. Stem Cell Res. Ther. 10:326. doi: 10.1186/s13287-019-1457-9
Sabzevari, R., Roushandeh, A. M., Mehdipour, A., Alini, M., and Roudkenar, M. H. (2020). SA/G hydrogel containing hCAP-18/LL-37-engineered WJ-MSCs-derived conditioned medium promoted wound healing in rat model of excision injury. Life Sci. 261:118381. doi: 10.1016/j.lfs.2020.118381
Sagaradze, G., Grigorieva, O., Nimiritsky, P., Basalova, N., Kalinina, N., Akopyan, Z., et al. (2019). Conditioned medium from human mesenchymal stromal cells: towards the clinical translation. Int. J. Mol. Sci. 20:1656. doi: 10.3390/ijms20071656
Saheli, M., Bayat, M., Ganji, R., Hendudari, F., Kheirjou, R., Pakzad, M., et al. (2020). Human mesenchymal stem cells-conditioned medium improves diabetic wound healing mainly through modulating fibroblast behaviors. Arch. Dermatol. Res. 312, 325–336. doi: 10.1007/s00403-019-02016-6
Seetharaman, R., Mahmood, A., Kshatriya, P., Patel, D., and Srivastava, A. (2019). Mesenchymal stem cell conditioned media ameliorate psoriasis vulgaris: a case study. Case Rep. Dermatol. Med. 2019:8309103. doi: 10.1155/2019/8309103
Seo, K. Y., Kim, D. H., Lee, S. E., Yoon, M. S., and Lee, H. J. (2013). Skin rejuvenation by microneedle fractional radiofrequency and a human stem cell conditioned medium in Asian skin: a randomized controlled investigator blinded split-face study. J. Cosmet Laser Ther. 15, 25–33. doi: 10.3109/14764172.2012.748201
Shim, J. H. (2015). Hair growth-promoting effect of human dermal stem/progenitor cell-derived conditioned medium. Tissue Eng. Regen. Med. 12, 268–275. doi: 10.1007/s13770-015-0012-8
Shin, H., Ryu, H. H., Kwon, O., Park, B. S., and Jo, S. J. (2015). Clinical use of conditioned media of adipose tissue-derived stem cells in female pattern hair loss: a retrospective case series study. Int. J. Dermatol. 54, 730–735. doi: 10.1111/ijd.12650
Sun, B., Guo, S., Xu, F., Wang, B., Liu, X., Zhang, Y., et al. (2014). Concentrated hypoxia-preconditioned adipose mesenchymal stem cell-conditioned medium improves wounds healing in full-thickness skin defect model. Int. Sch. Res. Notices 2014:652713. doi: 10.1155/2014/652713
Sun, J., Zhang, Y., Song, X., Zhu, J., and Zhu, Q. (2019). The healing effects of conditioned medium derived from mesenchymal stem cells on radiation-induced skin wounds in rats. Cell Transplant 28, 105–115. doi: 10.1177/0963689718807410
Tam, K., Cheyyatraviendran, S., Venugopal, J., Biswas, A., Choolani, M., Ramakrishna, S., et al. (2014). A nanoscaffold impregnated with human wharton’s jelly stem cells or its secretions improves healing of wounds. J. Cell. Biochem. 115, 794–803. doi: 10.1002/jcb.24723
Tamari, M., Nishino, Y., Yamamoto, N., and Ueda, M. (2013). Acceleration of wound healing with stem cell-derived growth factors. Int. J. Oral. Maxillofac. Implants 28, e369–e375. doi: 10.11607/jomi.te17
Tarcisia, T., Damayanti, L., Antarianto, R. D., Moenadjat, Y., and Pawitan, J. A. (2017). Adipose derived stem cell conditioned medium effect on proliferation phase of wound healing in sprague dawley rat. Med. J. Indonesia 26, 239–245. doi: 10.13181/mji.v26i4.1755
Templin, C., Grote, K., Schledzewski, K., Ghadri, J. R., Schnabel, S., Napp, L. C., et al. (2009). Ex vivo expanded haematopoietic progenitor cells improve dermal wound healing by paracrine mechanisms. Exp. Dermatol. 18, 445–453. doi: 10.1111/j.1600-0625.2008.00809.x
Ueda, M., and Nishino, Y. (2010). Cell-based cytokine therapy for skin rejuvenation. J. Craniofac. Surg. 21, 1861–1866. doi: 10.1097/SCS.0b013e3181f43f0a
Won, C. H., Choi, S. J., Kwon, O. S., Park, W. S., Kang, Y. J., Yoo, H. G., et al. (2010). The establishment and characterization of immortalized human dermal papilla cells and their hair growth promoting effects. J. Dermatol. Sci. 60, 196–198. doi: 10.1016/j.jdermsci.2010.08.015
Won, C. H., Jeong, Y. M., Kang, S., Koo, T. S., Park, S. H., Park, K. Y., et al. (2015). Hair-growth-promoting effect of conditioned medium of high integrin α6 and low CD 71 (α6bri/CD71dim) positive keratinocyte cells. Int. J. Mol. Sci. 16, 4379–4391. doi: 10.3390/ijms16034379
Wong, S. P., Rowley, J. E., Redpath, A. N., Tilman, J. D., Fellous, T. G., and Johnson, J. R. (2015). Pericytes, mesenchymal stem cells and their contributions to tissue repair. Pharmacol. Ther. 151, 107–120. doi: 10.1016/j.pharmthera.2015.03.006
Wu, Y., Peng, Y., Gao, D., Feng, C., Yuan, X., Li, H., et al. (2015). Mesenchymal stem cells suppress fibroblast proliferation and reduce skin fibrosis through a TGF-β3-dependent activation. Int. J. Lower Extremity Wounds 14, 50–62. doi: 10.1177/1534734614568373
Xiao, S., Deng, Y., Mo, X., Liu, Z., Wang, D., Deng, C., et al. (2020). Promotion of hair growth by conditioned medium from extracellular matrix/stromal vascular fraction gel in C57BL/6 Mice. Stem Cells Int. 2020:9054514. doi: 10.1155/2020/9054514
Xu, Y., Guo, S., Wei, C., Li, H., Chen, L., Yin, C., et al. (2016). The comparison of adipose stem cell and placental stem cell in secretion characteristics and in facial antiaging. Stem Cells Int. 2016:7315830. doi: 10.1155/2016/7315830
Yang, C. Y., Chang, P. Y., Chen, J. Y., Wu, B. S., Yang, A. H., and Lee, O. K. (2021). Adipose-derived mesenchymal stem cells attenuate dialysis-induced peritoneal fibrosis by modulating macrophage polarization via interleukin-6. Stem Cell Res. Ther. 12:193. doi: 10.1186/s13287-021-02270-4
Yoon, B. S., Moon, J. H., Jun, E. K., Kim, J., Maeng, I., Kim, J. S., et al. (2010). Secretory profiles and wound healing effects of human amniotic fluid-derived mesenchymal stem cells. Stem Cells Dev. 19, 887–902. doi: 10.1089/scd.2009.0138
Yuan, B., Broadbent, J. A., Huan, J., and Yang, H. (2018). The effects of adipose stem cell-conditioned media on fibrogenesis of dermal fibroblasts stimulated by transforming growth factor-β1. J. Burn Care Res. 39, 129–140. doi: 10.1097/bcr.0000000000000558
Zhang, K., Yu, L., Li, F. R., Li, X., Wang, Z., Zou, X., et al. (2020). Topical application of exosomes derived from human umbilical cord mesenchymal stem cells in combination with sponge spicules for treatment of photoaging. Int. J. Nanomed. 15, 2859–2872. doi: 10.2147/ijn.S249751
Zhang, Q., Liu, L. N., Yong, Q., Deng, J. C., and Cao, W. G. (2015). Intralesional injection of adipose-derived stem cells reduces hypertrophic scarring in a rabbit ear model. Stem Cell Res. Ther. 6:145. doi: 10.1186/s13287-015-0133-y
Zhang, S., Chen, L., Zhang, G., and Zhang, B. (2020). Umbilical cord-matrix stem cells induce the functional restoration of vascular endothelial cells and enhance skin wound healing in diabetic mice via the polarized macrophages. Stem Cell Res. Ther. 11:39. doi: 10.1186/s13287-020-1561-x
Zhou, B. R., Xu, Y., Guo, S. L., Xu, Y., Wang, Y., Zhu, F., et al. (2013). The effect of conditioned media of adipose-derived stem cells on wound healing after ablative fractional carbon dioxide laser resurfacing. Biomed Res. Int. 2013:519126. doi: 10.1155/2013/519126
Zhou, B. R., Zhang, T., Bin Jameel, A. A., Xu, Y., Xu, Y., Guo, S. L., et al. (2016). The efficacy of conditioned media of adipose-derived stem cells combined with ablative carbon dioxide fractional resurfacing for atrophic acne scars and skin rejuvenation. J. Cosmet Laser Ther. 18, 138–148. doi: 10.3109/14764172.2015.1114638
Zhou, H., Li, X., Yin, Y., He, X. T., An, Y., Tian, B. M., et al. (2020). The proangiogenic effects of extracellular vesicles secreted by dental pulp stem cells derived from periodontally compromised teeth. Stem Cell Res. Ther. 11:110. doi: 10.1186/s13287-020-01614-w
Keywords: advanced therapy, conditioned medium, dermatology, mesenchymal stem cells, stem cells
Citation: Montero-Vilchez T, Sierra-Sánchez Á, Sanchez-Diaz M, Quiñones-Vico MI, Sanabria-de-la-Torre R, Martinez-Lopez A and Arias-Santiago S (2021) Mesenchymal Stromal Cell-Conditioned Medium for Skin Diseases: A Systematic Review. Front. Cell Dev. Biol. 9:654210. doi: 10.3389/fcell.2021.654210
Received: 15 January 2021; Accepted: 21 June 2021;
Published: 23 July 2021.
Edited by:
Guido Moll, Charité – Universitätsmedizin Berlin, GermanyReviewed by:
Mohammad Bayat, Shahid Beheshti University of Medical Sciences, IranCopyright © 2021 Montero-Vilchez, Sierra-Sánchez, Sanchez-Diaz, Quiñones-Vico, Sanabria-de-la-Torre, Martinez-Lopez and Arias-Santiago. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Álvaro Sierra-Sánchez, YWx2YXJvc2lzYW5AZ21haWwuY29t; YWx2YXJvc2lzYW5AY29ycmVvLnVnci5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.