
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Clin. Diabetes Healthc., 16 August 2022
Sec. Diabetes Inequalities
Volume 3 - 2022 | https://doi.org/10.3389/fcdhc.2022.947552
 Marianna S. Wetherill1,2*
Marianna S. Wetherill1,2* Casey Bakhsh3
Casey Bakhsh3 Lacey Caywood1
Lacey Caywood1 Mary B. Williams2,4
Mary B. Williams2,4 Micah L. Hartwell5Denna L. Wheeler6Randolph D. Hubach7
Micah L. Hartwell5Denna L. Wheeler6Randolph D. Hubach7 T. Kent Teague8,9,10Gerwald Köhler10James R. Hebert11Sheri D. Weiser12
T. Kent Teague8,9,10Gerwald Köhler10James R. Hebert11Sheri D. Weiser12Background: Over the past four decades, advances in HIV treatment have contributed to a longer life expectancy for people living with HIV (PLWH). With these gains, the prevention and management of chronic co-morbidities, such as diabetes, are now central medical care goals for this population. In the United States, food insecurity disproportionately impacts PLWH and may play a role in the development of insulin resistance through direct and indirect pathways. The Nutrition to Optimize, Understand, and Restore Insulin Sensitivity in HIV for Oklahoma (NOURISH-OK) will use a novel, multi-level, integrated framework to explore how food insecurity contributes to insulin resistance among PLWH. Specifically, it will explore how food insecurity may operate as an intermediary risk factor for insulin resistance, including potential linkages between upstream determinants of health and downstream consequences of poor diet, other behavioral risk factors, and chronic inflammation.
Methods/design: This paper summarizes the protocol for the first aim of the NOURISH-OK study, which involves purposeful cross-sectional sampling of PLWH (n=500) across four levels of food insecurity to test our conceptual framework. Developed in collaboration with community stakeholders, this initial phase involves the collection of anthropometrics, fasting blood samples, non-blood biomarkers, 24-hour food recall to estimate the Dietary Inflammatory Index (DII®) score, and survey data. A 1-month, prospective observational sub-study (total n=100; n=25 for each food security group) involves weekly 24-hour food recalls and stool samples to identify temporal associations between food insecurity, diet, and gut microbiome composition. Using structural equation modeling, we will explore how upstream risk factors, including early life events, current discrimination, and community food access, may influence food insecurity and its potential downstream impacts, including diet, other lifestyle risk behaviors, and chronic inflammation, with insulin resistance as the ultimate outcome variable. Findings from these analyses of observational data will inform the subsequent study aims, which involve qualitative exploration of significant pathways, followed by development and testing of a low-DII® food as medicine intervention to reverse insulin resistance among PLWH (ClinicalTrials.gov Identifier: NCT05208671).
Discussion: The NOURISH-OK study will address important research gaps to inform the development of food as medicine interventions to support healthy aging for PLWH.
The fourth decade of the HIV epidemic marks many milestones in the treatment and management of HIV as a chronic disease. These medical advances have paved the way for new questions about how to optimize the health span for people living with HIV (PLWH), including chronic co-morbidity risk reduction and management. PLWH experience higher rates of diabetes compared to the general US population (1), with one in ten PLWH having diabetes (1) and another three in ten PLWH having prediabetes (2). The underlying insulin resistance that leads to diabetes is also associated with other co-morbidities of concern for PLWH, such as non-alcoholic fatty liver disease (3) and cognitive decline (4). Insulin resistance occurs when a person’s tissues become resistant to insulin-induced glucose uptake (5) and its causes among PLWH are likely multifactorial (5). Non-modifiable risk factors include age and family history, as well as factors specific to HIV, such as certain antiretroviral medications (6, 7) and possibly HIV infection itself (1). Modifiable risk factors for insulin resistance include central adiposity, physical inactivity, and poor diet. Although intervention data are lacking for PLWH, insulin resistance can often be reversed in the general population through healthy eating and other lifestyle behavior changes (6).
While identification of modifiable risk behaviors for insulin resistance among PLWH is an important clinical question, it is unlikely to result in risk reduction unless the context of these behaviors is elucidated and addressed through additional resources and supports. Among PLWH, those with limited financial resources are disproportionately insulin resistant (8). Food insecurity, the uncertain or limited household availability of a healthy food supply, may provide insightful context for understanding predisposition to insulin resistance among low-income PLWH. Food insecurity disproportionately affects PLWH and is a well-established predictor of HIV risk, transmission, and treatment outcomes that operates through nutritional and non-nutritional pathways (9). In the general population, food insecurity is associated with insulin resistance and diabetes, as well as modifiable risk factors for insulin resistance, including inflammatory diets (10), inadequate sleep (11), and physical inactivity (12).
Since food insecurity is a multidimensional, graded phenomenon of increasing severity, each dimension may have distinct influence on health behaviors and outcomes. Therefore, its influence may be understood best when the construct is treated as an ordinal or continuous variable rather than a dichotomous one. For example, marginal and low food security may contribute to insulin resistance via overnutrition through the consumption of a pro-inflammatory diet, consisting of low-cost, energy-dense foods with low fiber and micronutrient content (10, 13). In contrast, very low food security can result in undernutrition due to physical hunger and unintentional weight loss. Very low food security may contribute to insulin resistance through other changes in body composition, such as loss of lean muscle mass and possibly functional and morphologic changes in the intestine including intestinal inflammation and gut microbiome alterations (14, 15). Periods of binge eating when food becomes available may contribute to obesity (16, 17). The psychological worry that accompanies food insecurity may influence other behavioral risk factors for insulin resistance, such as tobacco use (18), inadequate sleep (11), and chronic stress (19), while inadequate food intake can limit energy available to engage in physical activity (12) and may encourage tobacco use as a strategy to cope with hunger pangs. Thus, interventions to support long-term food security for PLWH may substantially reduce risk for insulin resistance through many behavioral pathways other than nutrition.
Moving further upstream, food insecurity can be viewed as a symptom of broader structural forces that indirectly predispose PLWH towards insulin resistance. Unpacking these determinants can enhance the value of social policies, housing programs, and integrated mental health care efforts as necessary investments for enhancing the metabolic health of PLWH. These forces may include community factors (e.g., residential area deprivation and the local food environment), as well as life course events (e.g., early childhood adversity and trauma related to HIV diagnosis), which may each serve as important effect moderators for food insecurity, health risk behaviors, and biologic pathways. For example, adverse childhood experiences (ACEs) (20), such as physical neglect, are important determinants of food insecurity risk in adulthood (21, 22) and disproportionately reported by PLWH (23). ACEs are associated with epigenetic changes (24) as well as many health risk behaviors (25), which can result in biologic consequences, including chronic inflammation (26), insulin resistance (24), and diabetes risk (27, 28) in the general adult population. Therefore, the influence of these upstream risk factors as potential root causes of chronic co-morbidity risk among PLWH are undoubtedly complex, and their impact likely profound (Figure 1).
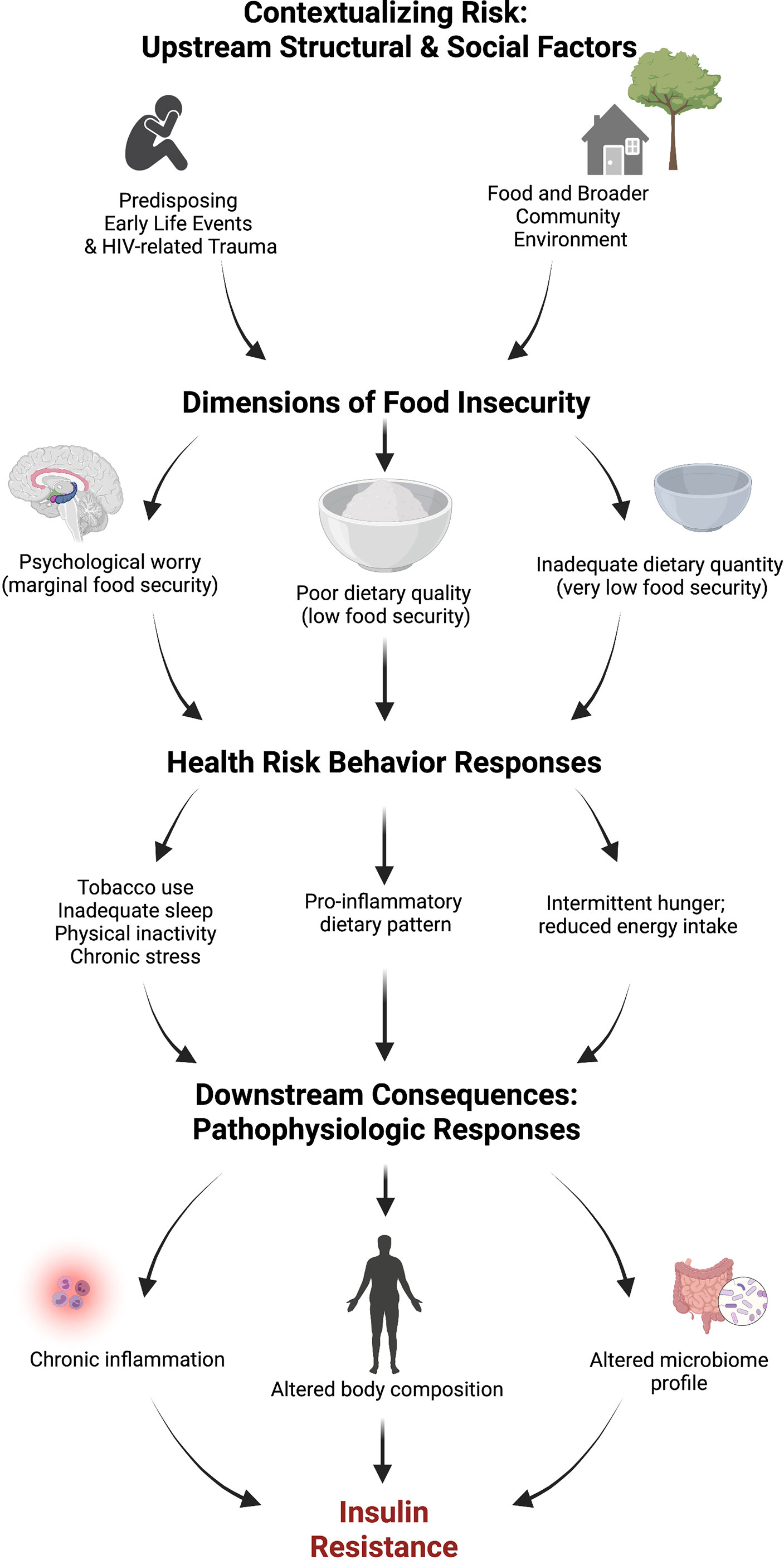
Figure 1 Conceptual framework for food insecurity and insulin resistance. Created with BioRender.com.
At a physiologic, downstream level, additional questions exist for how food insecurity gets “under the skin” to produce pathophysiologic responses associated with insulin resistance. One plausible biological pathway linking upstream forces, food insecurity, and its associated risk behaviors to insulin resistance may be through chronic inflammation. Elevated systemic levels of the inflammatory marker C-reactive protein (CRP) have been linked to food insecurity in the general population (29). Chronic inflammation may be an important contributor to dysglycemia (30), diabetes incidence (31, 32), and other chronic co-morbidities (33) among PLWH, who have higher levels of CRP than the general population (33). Measures of body composition, including body fat and muscle mass, are important biological variable predictors of chronic inflammation (34, 35) and insulin resistance (6, 7, 36, 37). Furthermore, HIV lipodystrophy, body composition changes that are characterized by loss of peripheral fat and deposition of visceral abdominal fat, is also linked to higher fasting insulin levels (38). Central adiposity (independent of BMI) (37) and lipodystrophy (38) in PLWH may directly cause insulin resistance due to accumulation of macrophages in adipose tissue, which secrete proinflammatory mediators (e.g., CRP) that impair glucose uptake into cells (39). Among men with HIV, the residual systematic inflammation that remains after viral suppression may be related to ongoing macrophage activation (40). Among women with HIV, food insecurity has been linked to elevated markers of chronic inflammation, even when controlling for viral suppression and CD4+ T cell count (41).
Additionally, the dietary patterns and periods of prolonged fasting caused by food insecurity may influence the gut microbiome (14), which is increasingly recognized for its role in systemic inflammation and insulin resistance within the general population (42, 43). Thus, food insecurity may exacerbate the consequences of HIV, since infection already disrupts gut homeostasis by reducing CD4+ Th17 and Treg cells in gut-associated lymphoid tissue, which increases intestinal permeability and microbial translocation (44), and drives immune activation and inflammation (45). AIDS history may be particularly detrimental to gut health (44), inflammation (33), and insulin resistance (33). HIV-related alterations in gut microbiome composition, dysbiosis, includes increases in pro-inflammatory Prevotella strains, and decreases in anti-inflammatory Bacteroides (33). A recent study linked a specific gut microbiome signature with metabolic dysfunction in PLWH, but lacked dietary data (46). Of the few studies that explore the influence of food insecurity or malnutrition on the gut microbiome and its metabolites (14, 47), none have included PLWH.
Malnutrition played a significant role in HIV morbidity and mortality risk in the pre-ART era (48). Community responses to address malnutrition during the early HIV epidemic resulted in the formation of home-delivered meals, other grocery assistance programs, and medical nutrition therapy that typically emphasized intake of high-calorie foods. Over time, many of these programs and services have become institutionalized cornerstones of HIV care across the US. For example, the Ryan White program serves >500,000 unduplicated PLWH nationally (49) and food assistance is an authorized expenditure for Ryan White HIV/AIDS Part A (medical) and Part B (social service) Programs (50).
In contrast with the well-recognized role of food in the prevention and treatment of malnutrition, less is known about how food may be used to reduce chronic co-morbidity risks among PLWH in the modern ART era. Anti-inflammatory dietary patterns may be particularly beneficial for several reasons. Specifically, the Dietary Inflammatory Index (DII®), a dietary quality measure that quantifies the inflammatory potential of diet (51), is a useful predictor of chronic inflammation (52), insulin resistance (53–55), and metabolic syndrome (53). Additionally, a high-DII® dietary pattern is associated with food insecurity among lower-income adults in the general population (10). A low-DII dietary pattern is achieved through consumption of wide variety of colorful plant-based foods (fruits, vegetables, nuts, seeds, whole grains, and beans), herbs and spices, and other minimally processed foods. The relationships between food insecurity, inflammatory potential of diet, and insulin resistance among PLWH are yet to be established. An aging cohort of long-term survivors, along with younger generations of more recently diagnosed PLWH, can benefit from HIV-specific nutrition guidance for the prevention of diabetes and related co-morbidities. Research exploring the role of dietary patterns in insulin resistance among PLWH may also be of interest to federal, state, and community stakeholders responsible for management of food assistance programs.
The Nutrition to Optimize, Understand, and Restore Insulin Sensitivity in HIV for Oklahoma (NOURISH-OK) study will result in an integrated, multi-level understanding of how food insecurity contributes to insulin resistance, which is central to the pathogenesis of many chronic co-morbidities in HIV. Its objectives are to: 1) identify the upstream determinants and downstream impacts of food insecurity on pathophysiological processes that may shorten the health span of PLWH, and 2) develop and test a community-driven, science-informed food as medicine intervention to reduce chronic co-morbidity risk among PLWH by addressing key mechanisms in the causal pathway of insulin resistance. We hypothesize that food insecurity will be significantly associated with insulin resistance and that this relationship will be partly mediated by nutritional and non-nutritional health behaviors that increase risk for chronic inflammation. We further hypothesize that these behavioral and inflammatory mediators will significantly differ across all four levels of foods security.
The NOURISH-OK study is being conducted in Oklahoma, a state that ranks among the highest in the nation for adverse childhood experiences (ACEs) (56) and where 54 of its 77 counties are classified as food deserts with all but one county having areas of low food access (57). Among its general adult population, the food insecurity rate (15.6%) exceeds the US rate (11.7%) (58). Its rates of tobacco use, poor diet, and physical inactivity are higher than the national average (59) and the state ranks 2nd highest for obesity, 6th highest for premature mortality (59), and 7th highest for diabetes (59). A recent federal report recognized Oklahoma as being among the top seven states experiencing a high rural HIV burden (60).
The NOURISH-OK study is a 5-year community-based participatory research project that is comprised of three aims. The first aim, initiated in June 2021 with an anticipated enrollment timeline of 18 months, involves a cross-sectional study (n=500) of objective and survey measures to test and refine our conceptual framework of food insecurity and insulin resistance among PLWH. Findings from these analyses will inform the second and third aims of the study, which involve qualitative exploration of significant pathways identified in Aim 1, followed by development and testing of a “food as medicine” intervention to reverse insulin resistance among PLWH that has been prospectively registered (ClinicalTrials.gov Identifier: NCT05208671). Here, we describe the protocol for the first aim of NOURISH-OK.
We developed the NOURISH-OK study using a community-based participatory research (CBPR) approach. This orientation helps to ensure the perspectives and priorities of the study population and other stakeholders are represented throughout the study design, execution, data analysis, and findings dissemination (61). The study’s main community partner, Tulsa CARES, is the state’s largest HIV social services provider and the only dedicated provider of nutrition services for PLWH in northeastern Oklahoma. Founded in 1991, Tulsa CARES is one of four state recipients of Ryan White funding and serves nearly 800 PLWH annually residing in 7 urban counties and 16 rural counties of northeastern Oklahoma.
Prior to the study’s enrollment launch, the main principal investigator (MSW) and community site principal investigator (CB) conducted a series of individual and small group interviews with HIV community stakeholders (n=18) between September 2020-January 2021. Stakeholders included PLWH and those representing public health, rural health, research, Ryan White medical and social services, advocacy, prevention, and outreach sectors. Interviews yielded information on perceived food needs as they relate to well-being for PLWH and community interest in research collaboration to study and address food insecurity. Additionally, the community site principal investigator recruited the initial members of the study’s participant advisory committee (PAC) in January 2021. PAC members provided input on the study logo, frequently asked questions for the study website, recruitment strategies, structure of study incentives, survey items, and enrollment procedures. Finally, Tulsa CARES staff participated in beta testing of participant surveys to provide additional feedback on survey item clarity and flow in March 2021. The University of Oklahoma Health Sciences Center Institutional Review Board (IRB) provided human subjects research approval for all methods described in this protocol. Additional safety protocols pertaining to collection, handling, and processing of saliva, blood, and stool specimens were approved by the University of Oklahoma Health Sciences Center Institutional Biosafety Committee.
The target population for the NOURISH-OK study is PLWH who are eligible for Ryan White-funded programs and reside in Oklahoma. An estimated 3,000 PLWH access one or more Ryan White-funded programs annually (49) and represent the study’s known recruitment pool. Nearly half (47%) of these individuals identify as a racial or ethnic minority, including 23.8% Black, 5.8% American Indian, and 10.1% Hispanic (49). An estimated 79.7% are male with most Ryan White clients aged 25-44 (42.7%) and 45-64 years (49.2%) (49). Study eligibility criteria require participants be HIV-positive residents of Oklahoma, financially eligible for Ryan White services (i.e., household income <400% federal poverty level), prescribed antiretroviral therapy (ART) for at least the past 6 months, and ability to provide a 10-hour fasting blood sample. Study exclusion criteria includes receiving treatment for cancer or end-stage renal disease.
A preliminary food needs study among Oklahoma Ryan White clients in 2012 found a high prevalence of very low (47.6%) and low (19.5%) food security in this population (62). To test our theoretical model of food insecurity as a central mediator linking upstream and downstream determinants of insulin resistance, representation at each level of food security status is needed. Therefore, selection criteria will be based on a food security pre-screening using the 10-item US Adult Food Security Survey Measure (63). Enrollment goals are based on food security status to ensure equal representation across four categories of food security: high (n=125), marginal (n=125), low (n=125), and very low (n=125) (Figure 2).
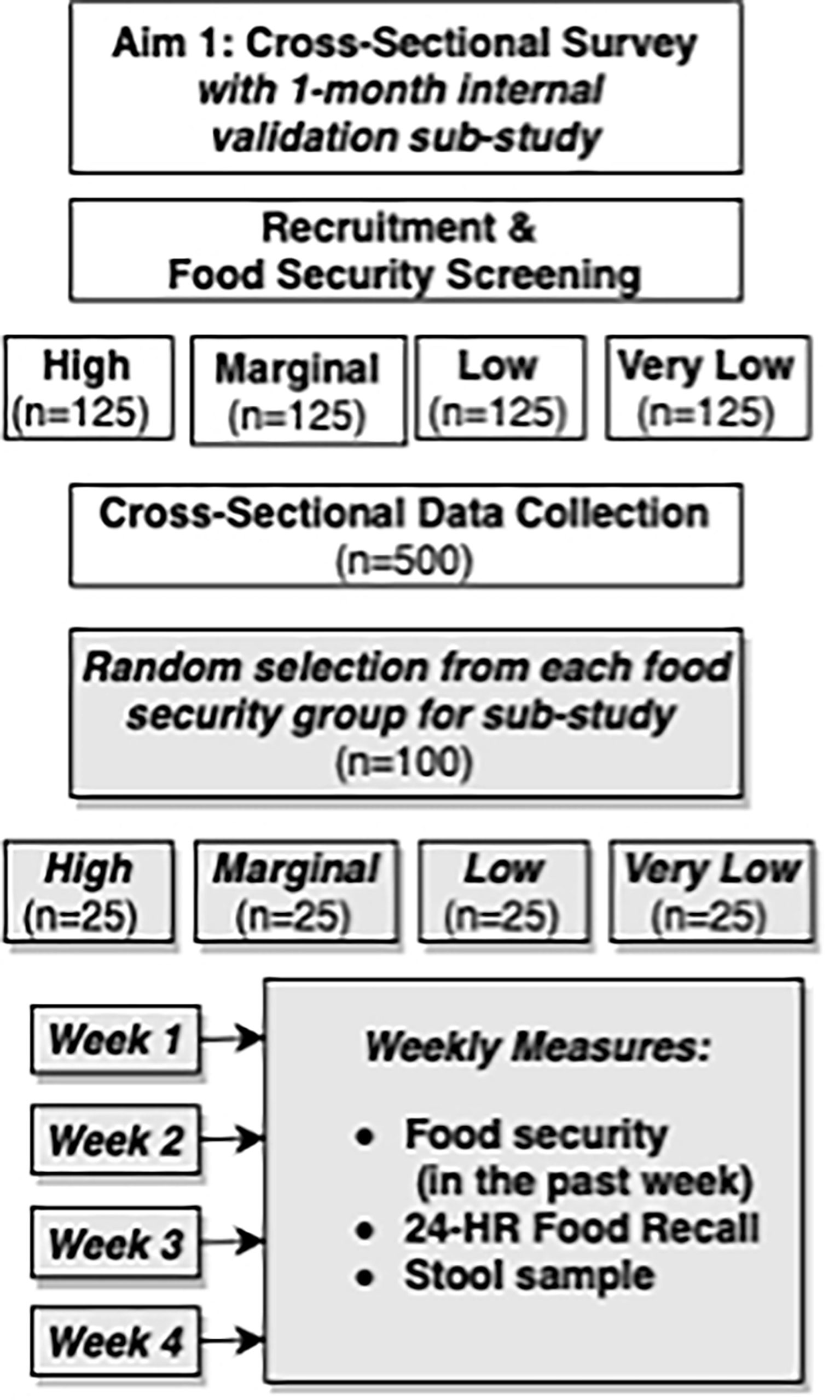
Figure 2 Study design overview for NOURISH-OK Aim 1, which includes a cross-sectional main study and prospective, observational sub-study.
Our multi-method recruitment strategy will include direct recruitment of Tulsa CARES clients (anticipated reach n=800) through a combination of dear client letters, direct phone calls, and in-person recruitment during Tulsa CARES appointments and sponsored events. Additional dear client letters will be directly mailed by the Oklahoma State Department of Health to individuals participating in the HIV Drug Assistance Program. Indirect recruitment strategies to the broader community of eligible PLWH will include recruitment flyers and business cards at community-based providers, medical clinics serving PLWH, study information booths at community events, and select pharmacies that dispense higher volumes of HIV prescriptions throughout northeastern Oklahoma.
Individuals expressing interest in the study will undergo a telephone or in-person screening interview to confirm eligibility and to discuss study requirements and procedures. Participants will be referred to the study website and encouraged to review its “frequently asked questions” section and informed consent paperwork before their scheduled enrollment appointment. Participants can elect to receive customized appointment reminder texts via the HIPAA-compliant Apptoto messaging service and/or phone calls the day before and the day of their scheduled appointment.
The first portion of the appointment will be dedicated to participant completion of study enrollment forms including written informed consent, authorization for use of protected health information in research, and the option to biobank blood samples for use in future studies.
Study compensation was informed through input from PAC stakeholders and will include a $50 gift card from a select list of stores (e.g., Amazon, Wal-Mart, Target), a personalized nutrition assessment results report, and choice of a non-monetary gift valued at $10 (e.g., portable phone battery charger, adult coloring book, paper towel and toilet paper pack). A $15 transportation voucher will additionally be provided to participants living outside of the enrollment site’s county (Tulsa County).
Study measures will be collected through a combination of interviewer and self-administered surveys, a nutrition and vital signs assessment, and a fasting blood sample. Participants will be encouraged to collect all study measures in a single 2-hour visit. If two sessions are needed, the self-administered survey portion can be completed at a separate appointment within 5 days from the blood sample and nutrition and vital signs assessment. Study measures are summarized in Tables 1, 2.
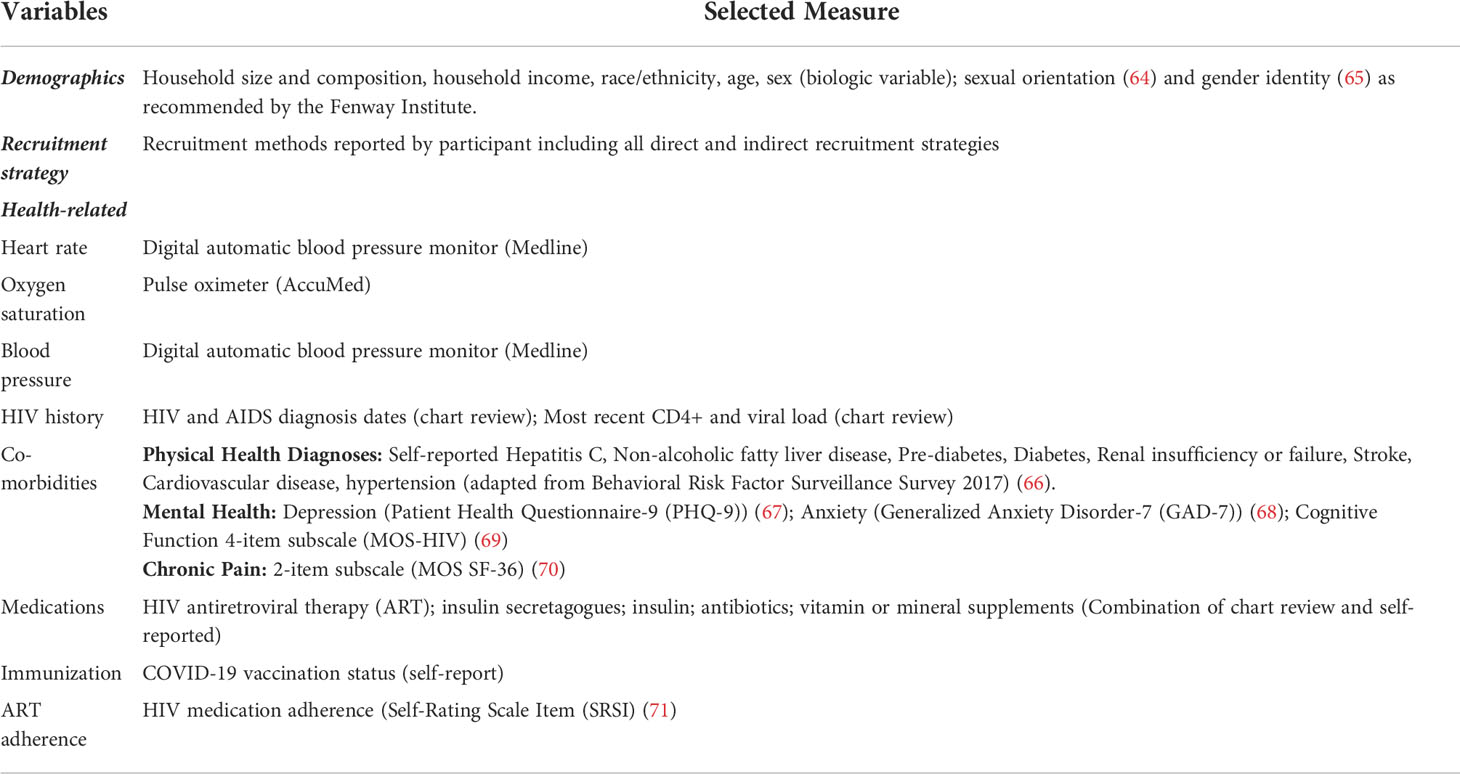
Table 1 NOURISH-OK Aim 1 Study Demographics, Recruitment, and Health Measures.
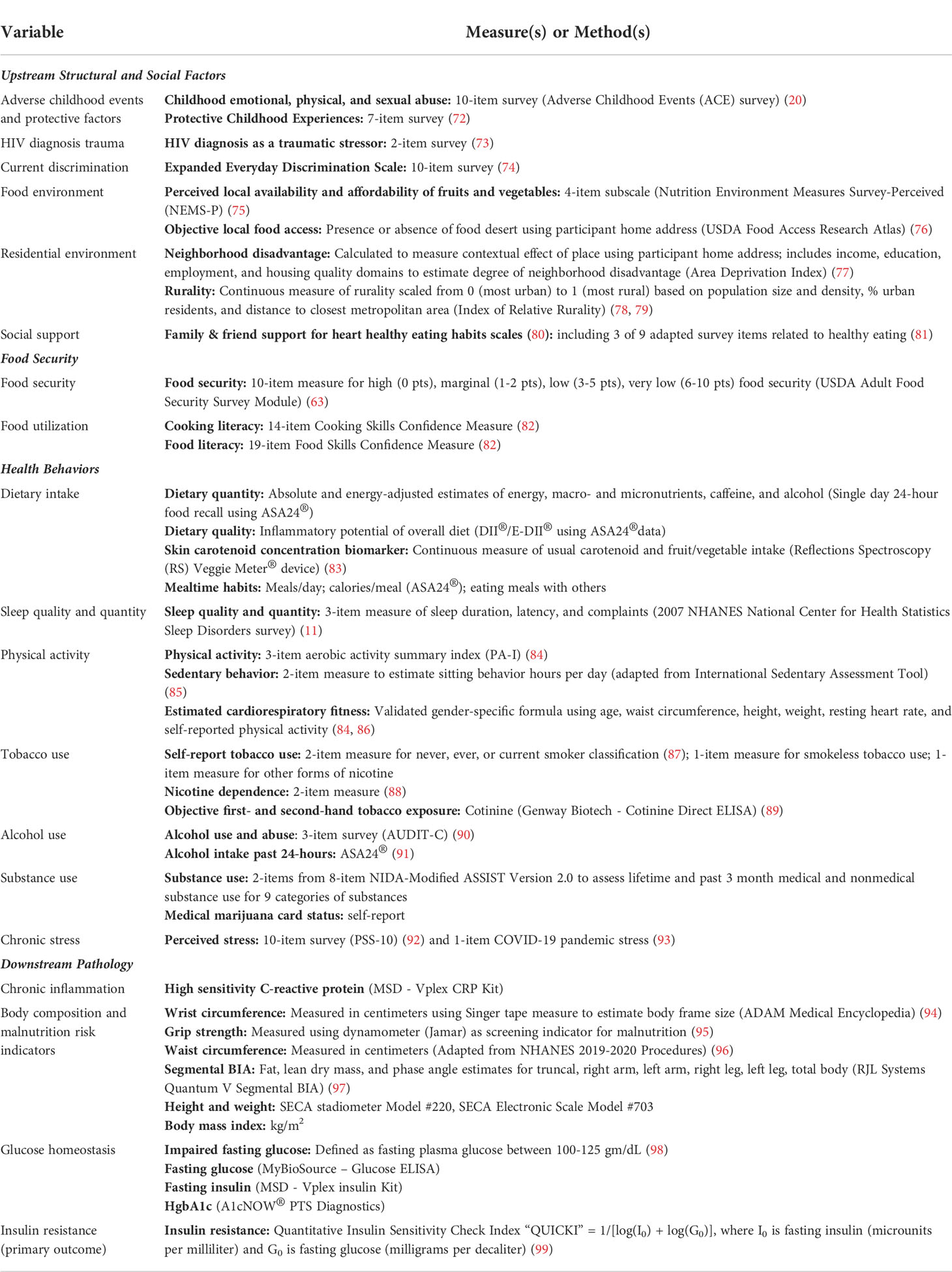
Table 2 NOURISH-OK Study Measures.
Before blood samples are collected, research staff will confirm each participant has fasted a minimum of 10 hours by asking the last time the participant ate or drank anything besides water. Venous blood samples will be collected by a trained phlebotomist using one BD Vacutainer serum tube, one BD Vacutainer EDTA plasma tube, one BD Vacutainer Heparin tube, one BD Vacutainer P800 plasma tube, and one BD Vacutainer CPT tube for peripheral blood mononuclear cells (PBMC). Samples will be transported to the designated study lab and processed within 2 hours of draw according to manufacturer’s instructions. Plasma and serum aliquots will be stored at −80°C until analysis. Peripheral blood mononuclear cells aliquots will be stored for less than 75 hours at −80°C and then transferred to liquid nitrogen vapor phase for cryopreservation until analysis. Laboratory measures, including serum insulin, blood glucose, c-reactive protein, hemoglobin A1c, and blood cotinine, are summarized in Table 2.
Trained research assistants will then conduct a nutrition assessment including height, weight, waist circumference, wrist circumference, grip strength, and a segmental bioelectrical impedance analysis test. Additional vital signs will include resting heart rate, blood oxygen level, and blood pressure. Resting heart rate, waist circumference, gender, and age will be used to estimate cardiorespiratory fitness (84, 86). We will collect one 24-hr food recall using the Automated Self-Administered 24-hour (ASA24®) Dietary Assessment Tool as our primary measure of dietary intake from all subjects (91). We will additionally measure skin carotenoid concentration using Reflections Spectroscopy (RS) (83). This will serve as a concentration biomarker to adjust for measurement error in estimated carotenoid and total fruit and vegetable intake from the ASA24®-generated dietary intake estimates.
We will measure height and weight (without shoes) to calculate body mass index (BMI) using a medical grade stadiometer and scale. We will measure central adiposity using waist circumference adapted from NHANES guidelines (96). To minimize participant discomfort, participants will identify body landmarks for self-measure in front of a mirror with assistance from staff. We will conduct segmental bioelectrical impedance analysis (BIA) using the Quantum V Segmental BIA (RJL Systems). Participants who may be pregnant or who have implanted electronic devices will be excluded from this measure. Participants with metal surgical implants present on one side of the body will complete a one-sided measure using the side of the body without the implant. Segmental body fat readings (right arm, left arm, right leg, left leg, and torso) will be used to further identify body type pattern associated with insulin resistance (97). We will minimize BIA measurement error associated with dehydration by providing 16 oz. of water 30 minutes prior to measurement. Collectively, these measures will be used to estimate nutritional and functional status.
After receiving authorization from participants through the informed consent process, research staff will conduct a medical chart review to obtain participant’s most recent CD4+ T cell and viral load measures and HIV and AIDS diagnosis dates. Alternatively, participants will be required to provide proof of HIV positivity and a copy of their most recent lab work in the past 6-12 months if this information is not accessible via chart review. On the day of study enrollment, participants will also be asked to confirm their residential address, demographics, and medication lists from their existing chart records before this information is added to the study database. Residential address will be used to create objective measures of the community environment, including food desert status (100) and residential area socioeconomic deprivation (77).
A 233-item self-administered survey will collect remaining study measures. These measures include early life events, trauma related to HIV diagnosis, perceived availability of food in the participant’s home and neighborhood, nutrition and health behaviors, food and cooking literacy, social support, and emotional, mental, and physical health history.
At the end of their study visit, each participant will receive an information packet that includes a list of community resources, including food assistance and mental health services, contact information for study staff, and several study business cards to share with others who may be eligible for the study. Any participant who reported suicidal ideations while completing the PHQ-9 will be connected on-site with a licensed clinical social worker for further evaluation and follow up at this time. Several days after the study appointment, a designated member of the research team will attempt to contact participants via phone to collect qualitative feedback for quality improvement purposes. Feedback areas include satisfaction and opportunities for improvement with research staff, study procedures, incentives, and other general feedback.
Upon completion of the cross-sectional study, participants will be randomly selected within their food security group for an invitation to participate in a 4-week observational sub-study. Elucidating the influence of food insecurity on dietary intake presents an important methodologic challenge because intake estimates from those with low and/or very low food security may potentially have higher error as compared to those with high or marginal food security. These differences in error may be due to wider fluctuations in food access throughout each month (101) and seasonally (102) for food insecure groups. Therefore, the primary purpose of the sub-study is to collect replicate dietary recalls to obtain a more precise estimate of usual dietary intake for each food security group, in addition to exploring how food security fluctuates from week-to-week. Trained interviewers will collect replicate dietary recalls and food security surveys via phone. At sub-study enrollment, subjects will receive a printed guide illustrating standard food units of measure for reference during phone calls to improve reporting accuracy.
Sub-study participants will also be asked to provide a single saliva sample and 4 weekly stool samples for exploratory analyses of microbiome profiles and variables of interest. At the time of sub-study enrollment, participants will provide their saliva sample using a self-sampling saliva test kit (OMNIgene*ORAL, OM-501; DNA Genotek, Ottawa, Ontario, Canada) that allows for DNA stability at room temperature for up to 1 year. Participants will receive four stool collection kits (OMNIgene*Gut, OMR-200.100; DNA Genotek) that will be marked with unique identifiers for self-collection at home. Research staff will instruct study subjects on how to use the kits and store stool samples, which can be kept for up to 60 days at room temperature.
On a randomly-selected day each week, participants will receive a text or phone call notification from research staff requesting to complete their weekly phone survey which includes a 24-hour dietary recall followed by collection of a sample from their next stool. Participants will have the option to return kits by mail or by hand to the enrollment site. Participants will receive up to a $100 gift card upon completion of the sub-study ($25 for each week dietary recall is completed and stool sample is collected).
Upon arrival to the research lab, handling and storage of the saliva and stool samples will follow the manufacturer’s recommendations. For precautionary measures, sample processing and DNA isolation procedures will be under Biosafety Level 2 (BSL-2) containment. Samples will be stored under suitable conditions (long-term storage at -80°C) until processing for DNA isolation. A commercial DNA isolation kit (e.g., Zymo Research ZymoBIOMICS DNA Miniprep Kit) will be used to isolate DNA from saliva and fecal sample aliquots. Isolated DNAs will be quality controlled using spectrophotometry for measurement of DNA concentration and purity (260nm/280nm, 260nm/230nm ratios) as well as agarose gel electrophoresis for determination of DNA integrity. If indicated, isolations will be repeated.
Salivary and fecal DNAs will be processed for 16S ribosomal RNA gene-based analyses of the respective microbiotas. We will target the hypervariable region V4 of 16S rRNA genes using dual-indexed, paired-end amplicon sequencing with an Illumina MiSeq system (Illumina, Inc., San Diego, CA) as described by Kozich et al. (103). The resulting sequence reads will be analyzed following state-of-the-art bioinformatics pipelines for quality control, taxonomic profiling, and differential abundance analyses of microbial communities. Sub-study measures are summarized in Table 3.
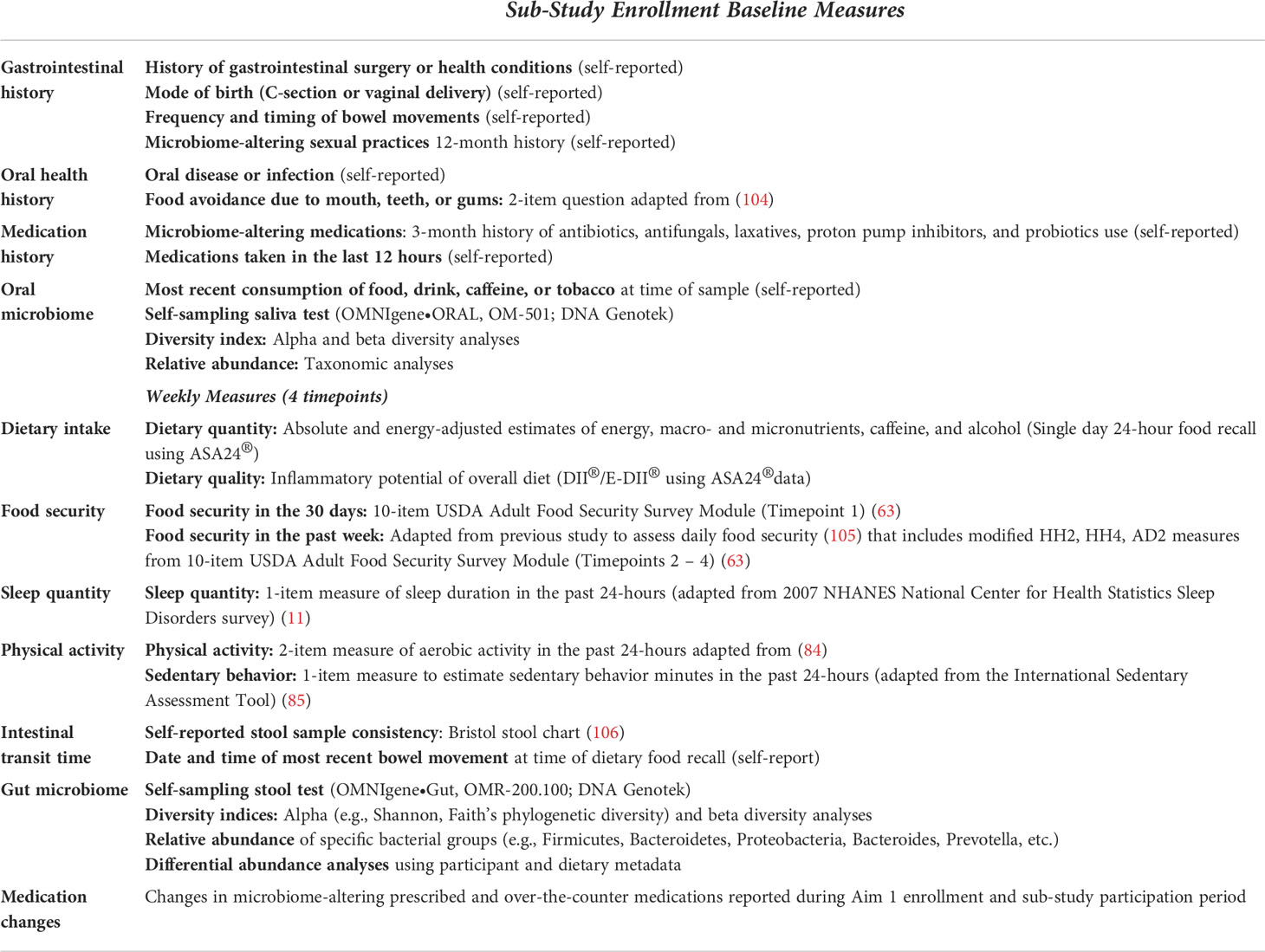
Table 3 NOURISH-OK Aim 1 Sub-study Observational Measures.
To protect confidentiality, each participant will be assigned a unique study identifier that will be used to link study datasets. Identifying information, including participant name, contact information, and the unique study identifier will be stored in a separate database not to be included in the data analysis. Survey data will be collected and managed using REDCap electronic data capture tools (107, 108) that are hosted on a secure server at the University of Oklahoma Health Sciences Center. Biomarker and body composition data will be manually entered into the REDCap database by research staff. De-identified microbiome sample data will be stored and analyzed at Oklahoma State University Center for Health Sciences. Analytic output files (dietary recall data) will be directed downloaded from the ASA24® website and saved on a secure server at the University of Oklahoma Health Sciences Center. Before analysis, these dietary data will be reviewed for missing nutrient data, portion outliers, and nutrient outliers in accordance with the general guidelines from the National Cancer Institute (NCI) regarding how to review and edit ASA24 data.
We will first examine associations between continuous measures, such as food insecurity on the 10-point scale, DII® scores, CRP level, and various measures of glucose homeostasis, using linear regression. We will compare means using t-tests for categorical variables with 2-levels and ANOVA for variables with 3 or more levels, such as the 4-level food security categorical variable (high, marginal, low, very low food secure).
We will use fasting glucose and insulin measures to calculate the quantitative insulin sensitivity check index (QUICKI) as the primary outcome measure for our analyses where a lower value indicates greater insulin resistance (99). Due to its reliability, reproducibility, accuracy, and positive predictive value across a wide range of co-morbidities, the QUICKI is a widely-accepted surrogate index measure of insulin sensitivity that is recommended for larger, community-based research studies when the laborious, clinic-based hyperinsulinemic-euglycemic clamp technique is not feasible (107). The QUICKI uses the empirically-derived equation QUICKI = 1/[log(I0) + log(G0)], where I0 is fasting insulin (μU/ml), and G0 is fasting glucose (mg/dl) (99). The QUICKI has been shown to perform equally to or slightly better than the homeostasis model assessment of insulin resistance (HOMA-IR) across the insulin sensitivity-resistance spectrum (108, 109). Additionally, it offers a slight advantage for measuring changes in insulin sensitivity over time (107, 110), which in consideration of our third aim (examining the effects of a food is medicine intervention on insulin resistance), the QUICKI was selected as the most appropriate outcome measure for the NOURISH-OK study.
We will calculate DII® scores (crude and energy-adjusted) developed by Hebert and colleagues (51) for the full sample with measurement error correction using information from the sub-study. The DII® and the energy-adjusted DII (E-DII™) scores are calculated based on dietary intake of food parameters (i.e., a combination of whole foods and nutrients associated with inflammation). Scores can range from a theoretical low of around -9 to a theoretical high of +8; however, scores are rarely outside the range of -6 to +6. Negative scores represent an anti-inflammatory dietary pattern, while positive scores represent a pro-inflammatory dietary pattern. We hypothesize that DII® score will be positively associated with insulin resistance. We will conduct sensitivity analyses of the relationship between DII® scores and insulin resistance at each level of food security. We hypothesize that DII® scores will be more strongly associated with insulin resistance for food insecure groups than food secure groups (111). These analyses will inform a list of candidate intervention foods for further evaluation in Aim 2. Dietary fiber has been inversely associated with BMI in PLWH (112) and is a source of sustenance for beneficial gut bacteria (113), thus we will also compare the impact of dietary fiber on insulin resistance. We will further explore dietary component factor loadings contributing most strongly to the DII® scores and use discriminant analysis to understand the relationship between DII® score and reported patterns of intake.
For dietary intake estimates, we will conduct an internal regression calibration study using the sub-sample of 100 subjects with four additional dietary recalls to estimate and adjust for measurement error in the remaining sample with single-day recalls (114). We will use the methods of triads to combine dietary recall data with dermal carotenoid scores to more precisely estimate true carotenoid and total fruit and vegetable intake (115, 116). Since chronic inflammation and smoking are both independently associated with lower beta-carotene concentrations (116), we will control for these confounders, if needed. Additionally, we will explore whether measurement error varies by food security status using sensitivity analysis to estimate and adjust for measurement error at each food security level. We will estimate variance in SAS using the Restricted Maximum Likelihood Estimation method and variance ratios as the error variance/variance across individuals. The within- (CVw=Sw/mean of each nutrient) and between-individual (CVb = Sb/mean of each nutrient) coefficient of variation (CV) will be estimated using Beaton’s formula (117). The CVw will then be used to estimate the number of 24-hr food recall days needed to estimate accurate dietary intakes among PLWH, and whether the number of recall days differ by food security status (117). Findings will be applied to modify the number of dietary recalls collected to evaluate the impact of the NOURISH-OK intervention (Aim 3).
As described in our conceptual framework, food insecurity may influence risk factors beyond dietary intake, such as tobacco use and stress. Therefore, we will validate self-report tobacco use with serum cotinine, which is recognized by the Centers for Disease Control and Prevention as the preferred biomarker for tobacco use (89). Additionally, we will use regression to assess variance explained in the stress biomarker CRP values by PSS scores. Results from these validation studies will inform selection of appropriate measures to evaluate the impact of the NOURISH-OK intervention on additional health risk behaviors.
Finally, we will test our conceptual model using structural equation modeling, a method that allows simultaneous measurement of the strength and significance of predictor variables via direct and indirect pathways on a single outcome established a priori by theory (118). The theoretical framework draws from existing conceptual models (16, 119) that position physical and social community environments as risk regulators (119) for household food insecurity and its resulting individual nutritional and non-nutritional risk behaviors (16), which become embodied through pathophysiologic responses (119) (Figure 1). Sample size recommendations vary widely for studies that employ structural equation modeling, with lower estimates citing 200 cases for SEM models (118). We have selected a conservative sample size of 500, which exceeds more recent recommendations for up to 460 cases for multi-factor, multi-indicator models (120).
The SEM will simultaneously estimate direct and indirect effects of continuous exposure variables in the directional pathway of food insecurity and insulin resistance (Figure 3). Specifically, we will test the influence of upstream and social factors on food insecurity, and whether food utilization skills modify the association between community food access and food security. As an intermediate variable in the SEM, food security status will be used to predict insulin resistance using behavioral and pathophysiologic mediators with AIDS diagnosis as a potential effect modifier. We will use similar methods developed in our past research (121), including quasi-maximum likelihood estimation with Satorra-Bentler correction to measure direct and indirect paths between all variables. We will use Chi-square, Root Mean Square Error of Approximation (RMSEA), and Comparative Fit Index (CFI) to assess model fit. We will conduct invariance testing using AIDS status to compare model differences between those with and without AIDS diagnosis history. We will re-specify the model, if needed, using a theory-informed approach. Analyses will be conducted using R, Version 4.0.2.
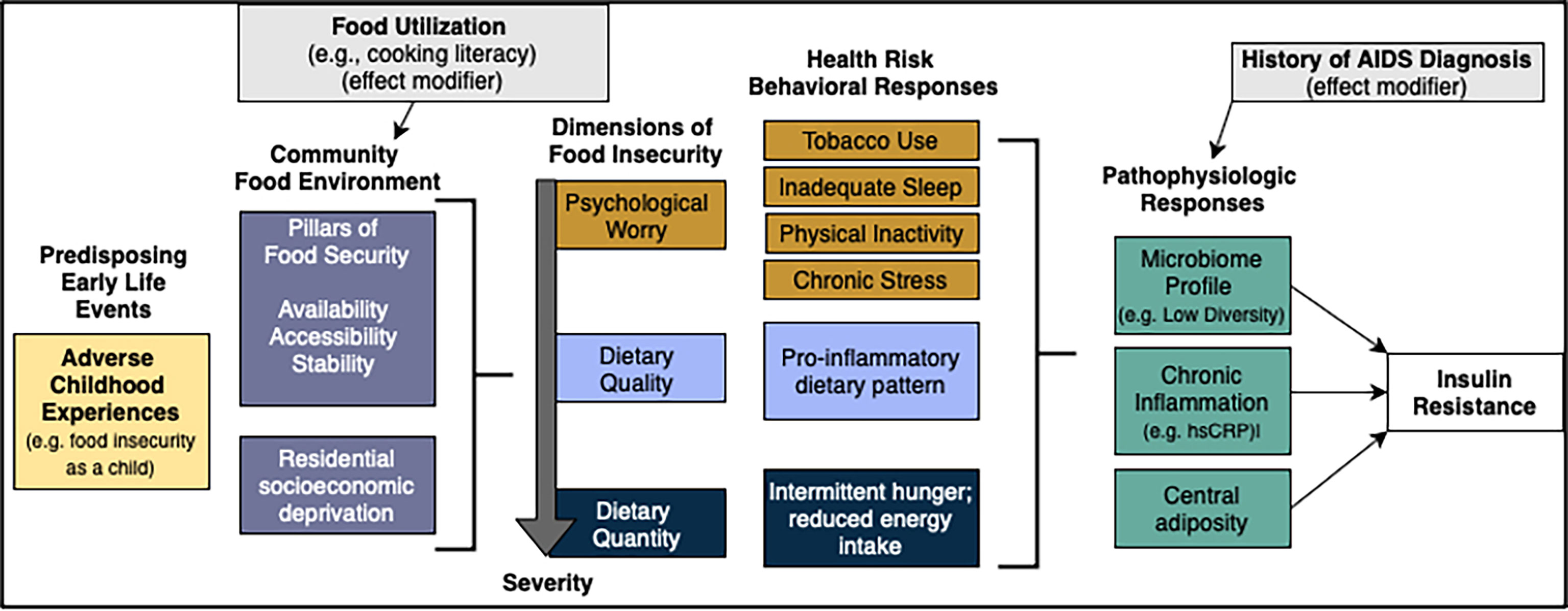
Figure 3 Structural equation model of food insecurity and insulin resistance. Additional co-variate demographics not depicted. Created with draw.io.
The highly complex nature of microbiome data has led to a continuing evolution of analyses methods. We will use the next-generation microbiome bioinformatics platform QIIME 2 (122) as the standard analysis package from raw sequences to statistical evaluation of the cross-sectional saliva and the longitudinal (time series) stool microbiota study results. Additional methods such as LEfSe (Linear discriminant analysis Effect Size) (123) will be included in our analysis pipeline.
The compositional and zero-inflated nature of microbial community profiling data requires specialized, preferably non-parametric approaches for statistical analyses of associations with clinical or dietary variables. Due to high rates of periodontal disease in people with FI (124, 125) and PLWH (126, 127), we will explore correlations between oral microbiota profiles (composition and diversity) and insulin resistance, and whether self-reported measures of poor oral health, food insecurity, and chronic inflammation mediate these relationships. Additionally, we will explore whether GMB qualities (i.e., overall GMB diversity index; specific biomarker components, such as Prevotella, Bacteroides (128)) mediate the association between dietary intake (i.e., DII®; individual constituents such as fiber) and insulin resistance. The variance estimates and intraclass correlation coefficients from repeated measures of GMB and dietary recall data will be used to refine data collection and statistical analysis methods for the NOURISH-OK intervention (Aim 3).
The NOURISH-OK study is a novel exploration of how the distinct psychological, dietary quality, and dietary quantity components of food insecurity may influence health risk behaviors and insulin resistance among PLWH. It challenges prevailing food insecurity research paradigms that traditionally emphasize one level of understanding (e.g., behavioral vs. molecular) by simultaneously considering environmental, psychosocial, behavioral, and biological factors in the pathogenesis of insulin resistance, and how food insecurity may amplify or dampen these pathways. Further, its conceptual framework incorporates the role of traumatic events as potential underlying contributors to food insecurity and its associated outcomes. Collectively, the first aim of the NOURISH-OK study is designed to provide HIV researchers, clinicians, and other stakeholders with key leverage point opportunities for building nutrition equity among PLWH, including development of evidence-informed food as medicine programs that address dimension(s) of underlying need.
In addition to elucidating the various potential mechanisms by which food insecurity shapes health risks, the NOURISH-OK study will support validation of dietary assessment measures in PLWH. These measures include dermal carotenoids as a biomarker for total carotenoid and total fruit/vegetable intake and construct validity of the DII® as a predictor of inflammation in PLWH. Because carotenoids, fruits, and vegetables correlate with other nutrients that comprise the DII® score and inflammatory markers, dermal carotenoids may be a useful non-invasive alternative to intensive dietary collection methods in future PLWH studies, including measures of intake and dietary intervention adherence. Although tested extensively in diverse populations (129, 130), this surrogate biomarker has not been studied among PLWH. The NOURISH-OK sub-study will further address methodologic gaps by exploring whether there are differences in dietary intake measurement error based on food insecurity status. If food security status is found to be related to measurement error, it will be paramount that future research investigating the role of food insecurity on dietary intake incorporate methods to adjust for this error. Furthermore, the sub-study’s oral and gut microbiome analyses will answer important questions about whether food insecurity is associated with distinct microbiome profiles and whether these profiles are attributable to diet and insulin resistance among PLWH. Finally, the NOURISH-OK study addresses additional methodologic gaps in health behavior research by including additional validation studies of other lifestyle behaviors among PLWH beyond diet, including self-reported tobacco (validated with serum cotinine) and perceived stress (validated with CRP).
An important limitation of the NOURISH-OK study’s first aim is the inability to establish temporal linkages among variables within the conceptual framework due to its cross-sectional design. Since the relationships between food insecurity and HIV-related outcomes may operate bidirectionally (9), additional research will be necessary to elicit a deeper understanding of complex relationships within the framework and to refine proposed mechanisms. The study’s second aim, comprised of qualitative inquiry with PLWH who experience food insecurity, will help to address this limitation by allowing the research team to triangulate data pertaining to potential directionality and context of significant pathways identified in Aim 1.
In closing, the NOURISH-OK promotes structural equity in HIV research by operating through a community-academic research partnership that directly involves PLWH at the decision-making table (131). These contextual factors will help to ensure current study activities incorporate community concerns and priorities, while simultaneously building capacity to plan and engage in future research that responds to evolving community needs.
The studies involving human participants were reviewed and approved by University of Oklahoma Health Sciences Center Institutional Review Board (study #12509). The patients/participants provided their written informed consent to participate in this study.
MSW, conceptualized and obtained funding the NOURISH-OK study, designed the conceptual framework depicted in Figure 1, led development of the methods, and wrote the original manuscript draft; CB, contributed to the overall study design and recruitment strategies, led participant advisory board activities; LC, led project administration activities pertaining to database development, writing of research protocol, participant enrollment, data collection, and monitoring; MBW, led data curation activities pertaining to data management, cleaning and integrity and supervised statistical support staff; MLH led methods for structural equation modeling; RH, advised on recruitment methods for rural Oklahomans living with HIV; RDW, advised on rural sampling and classification methods; TKT, led selection of blood and serum laboratory measures and supervision of laboratory personnel; GK, contributed to the literature review, advised on microbiome sub-study design and oversaw analysis of oral and gut microbiome samples; JDH, co-developed the Dietary Inflammatory Index® and advised on nutrition epidemiologic methods; SDW, advised on study design, participant safety protocols, and survey measures as an HIV food insecurity content expert. All authors reviewed, edited, and approved the final version of the manuscript.
Research reported in this publication was supported by National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health under Award Number R01DK127464 and by the National Institute of General Medical Sciences of the National Institutes of Health under Award Number U54GM104938. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
The authors thank members of the participant advisory committee for their valuable contributions to the NOURISH-OK study methods. The authors also acknowledge the contributions of Brenda Davis and Ashlee Rempel from the laboratory of T. Kent Teague at the University of Oklahoma Integrative Immunology Center for their assistance with details of the study protocol involving sampling, processing, and handling of all blood samples. The authors thank Victoria Thomas, MD, MPH, Raegan Tremblay, BGS, and Jacqueline Dukes, BS, for their assistance with the preliminary development of the NOURISH-OK study procedures manual as well as Donna Fesler, MS, RN, CNEcl, and Kia Beverly for their training and consultation in phlebotomy procedures. We acknowledge the Harold Hamm Diabetes Center for its supportive consultation throughout the development of the NOURISH-OK study.
Unrelated to the present work, MSW previously served as an advisor for Food and Society at the Aspen Institute’s Food is Medicine Initiative and is a consultant for the Sunflower Foundation’s Food is Medicine Initiative.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
ACEs, Adverse childhood experiences; BMI, Body mass index; CRP, C-reactive protein; DII®, Dietary Inflammatory Index; LEfSe, Linear discriminant analysis Effect Size; NOURISH-OK, Nutrition to Optimize, Understand and Restore Insulin Sensitivity in HIV for Oklahoma; PLWH, People living with HIV; PSS, Perceived stress scale; QUICKI, quantitative insulin sensitivity check index; SEM, Structural equation modeling.
1. Hernandez-Romieu AC, Garg S, Rosenberg ES, Thompson-Paul AM, Skarbinski J. Is diabetes prevalence higher among HIV-infected individuals compared with the general population? evidence from MMP and NHANES 2009-2010. BMJ Open Diabetes Res. Care (2017) 5(1):e000304–e000304. doi: 10.1136/bmjdrc-2016-000304
2. Arafath S, Campbell T, Yusuff J, Sharma R. Prevalence of and risk factors for prediabetes in patients infected with HIV. Diabetes Spectr. (2018) 31(2):139. doi: 10.2337/ds17-0009
3. Price JC, Seaberg EC, Latanich R, Budoff MJ, Kingsley LA, Palella FJ Jr, et al. Risk factors for fatty liver in the multicenter AIDS cohort study. Am. J. Gastroenterol. (2014) 109(5):695–704. doi: 10.1038/ajg.2014.32
4. Khuder SS, Chen S, Letendre S, Marcotte T, Grant I, Franklin D, et al. Impaired insulin sensitivity is associated with worsening cognition in HIV-infected patients. Neurology (2019) 92(12):e1344–53. doi: 10.1212/WNL.0000000000007125
5. Pedro MN, Rocha GZ, Guadagnini D, Santos A, Magro DO, Assalin HB, et al. Insulin resistance in HIV-patients: Causes and consequences. Front. Endocrinol. (Lausanne) (2018) 9:514. doi: 10.3389/fendo.2018.00514
6. The National Institute of Diabetes and Digestive and Kidney Diseases Health Information Center. Insulin resistance & prediabetes (2018). Available at: https://www.niddk.nih.gov/health-information/diabetes/overview/what-is-diabetes/prediabetes-insulin-resistance#develop.
7. Hulgan T. Factors associated with insulin resistance in adults with HIV receiving contemporary antiretroviral therapy: a brief update. Curr. HIV/AIDS Rep. (2018) 15(3):223–32. doi: 10.1007/s11904-018-0399-7
8. Hessol NA, Ameli N, Cohen MH, Urwin S, Weber KM, Tien PC. The association between diet and physical activity on insulin resistance in the women's interagency HIV study. journal of acquired immune deficiency syndromes. (2013) 62(1):74–80. doi: 10.1097/QAI.0b013e318275d6a4
9. Weiser SD, Young SL, Cohen CR, Kushel MB, Tsai AC, Tien PC, et al. Conceptual framework for understanding the bidirectional links between food insecurity and HIV/AIDS. Am. J. Clin. Nutr. (2011) 94(6):1729S–39S. doi: 10.3945/ajcn.111.012070
10. Bergmans RS, Palta M, Robert SA, Berger LM, Ehrenthal DB, Malecki KM. Associations between food security status and dietary inflammatory potential within lower-income adults from the united states national health and nutrition examination survey, cycles 2007 to 2014. J. Acad. Nutr. Diet (2018) 118(6):994–1005. doi: 10.1016/j.jand.2017.12.003
11. Ding M, Keiley MK, Garza KB, Duffy PA, Zizza CA. Food insecurity is associated with poor sleep outcomes among US adults. J. Nutr. (2015) 145(3):615–21. doi: 10.3945/jn.114.199919
12. To QG, Frongillo EA, Gallegos D, Moore JB. Household food insecurity is associated with less physical activity among children and adults in the U.S. population. J. Nutr. (2014) 144(11):1797–802. doi: 10.3945/jn.114.198184
13. Muhammad JN, Fernandez JR, Clay OJ, Saag MS, Overton ET, Willig AL. Associations of food insecurity and psychosocial measures with diet quality in adults aging with HIV. AIDS Care (2019) 31(5):554–62. doi: 10.1080/09540121.2018.1554239
14. Attia S, Feenstra M, Swain N, Cuesta M, Bandsma RHJ. Starved guts: Morphologic and functional intestinal changes in malnutrition. J. Pediatr. Gastroenterol. Nutr. (2017) 65(5):491–5. doi: 10.1097/MPG.0000000000001629
15. Ecklu-Mensah G, Gilbert J, Devkota S. Dietary selection pressures and their impact on the gut microbiome. Cell. Mol. Gastroenterol. Hepatol. (2022) 13(1):7–18. doi: 10.1016/j.jcmgh.2021.07.009
16. Seligman HK, Schillinger D. Hunger and socioeconomic disparities in chronic disease. New Engl. J. Med. (2010) 363(1):6–9. doi: 10.1056/NEJMp1000072
17. Sirotin N, Hoover DR, Shi Q, Anastos K, Weiser SD. Food insecurity with hunger is associated with obesity among HIV-infected and at risk women in Bronx, NY. PloS One [Electronic Resource] (2014) 9(8):e105957. doi: 10.1371/journal.pone.0105957
18. Kim-Mozeleski JE, Tsoh JY, Ramirez-Forcier J, Andrews B, Weiser SD, Carrico AW. Smoking predicts food insecurity severity among persons living with HIV. AIDS Behav. (2018) 22(9):2861–7. doi: 10.1007/s10461-018-2069-6
19. El Zein A, Shelnutt KP, Colby S, Vilaro MJ, Zhou W, Greene G, et al. Prevalence and correlates of food insecurity among U.S. college students: a multi-institutional study. BMC Public Health (2019) 19(1):660. doi: 10.1186/s12889-019-6943-6
20. Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. Am. J. Prev. Med. (1998) 14(4):245–58. doi: 10.1016/S0749-3797(98)00017-8
21. Chilton M, Knowles M, Bloom SL. The intergenerational circumstances of household food insecurity and adversity. J. Hunger Environ. Nutr. (2017) 12(2):269–97. doi: 10.1080/19320248.2016.1146195
22. Chilton M, Knowles M, Rabinowich J, Arnold KT. The relationship between childhood adversity and food insecurity: 'It's like a bird nesting in your head'. Public Health Nutr. (2015) 18(14):2643–53. doi: 10.1017/S1368980014003036
23. Campbell JA, Walker RJ, Egede LE. Associations between adverse childhood experiences, high-risk behaviors, and morbidity in adulthood. Am. J. Prev. Med. (2016) 50(3):344–52. doi: 10.1016/j.amepre.2015.07.022
24. Berens AE, Jensen SKG, Nelson CA. Biological embedding of childhood adversity: from physiological mechanisms to clinical implications. BMC Med. (2017) 15(1):135. doi: 10.1186/s12916-017-0895-4
25. Chen M, Lacey RE. Adverse childhood experiences and adult inflammation: Findings from the 1958 British birth cohort. Brain Behav. Immun. (2018) 69:582–90. doi: 10.1016/j.bbi.2018.02.007
26. Baumeister D, Akhtar R, Ciufolini S, Pariante CM, Mondelli V. Childhood trauma and adulthood inflammation: a meta-analysis of peripheral c-reactive protein, interleukin-6 and tumour necrosis factor-alpha. Mol. Psychiatry (2016) 21(5):642–9. doi: 10.1038/mp.2015.67
27. Campbell JA, Mosley-Johnson E, Garacci E, Walker RJ, Egede LE. The co-occurrence of diabetes and adverse childhood experiences and its impact on mortality in US adults. J. Affect. Disord. (2019) 249:20–5. doi: 10.1016/j.amepre.2015.07.022
28. Huang H, Yan P, Shan Z, Chen S, Li M, Luo C, et al. Adverse childhood experiences and risk of type 2 diabetes: A systematic review and meta-analysis. Metabolism (2015) 64(11):1408–18. doi: 10.1016/j.metabol.2015.08.019
29. Gowda C, Hadley C, Aiello AE. The association between food insecurity and inflammation in the US adult population. Am. J. Public Health (2012) 102(8):1579–86. doi: 10.2105/AJPH.2011.300551
30. Nkinda L, Patel K, Njuguna B, Ngangali JP, Memiah P, Bwire GM, et al. C - reactive protein and interleukin - 6 levels among human immunodeficiency virus -infected patients with dysglycemia in Tanzania. BMC Endocrine Disord. (2019) 19(1):77–7. doi: 10.1186/s12902-019-0407-y
31. Galescu O, Bhangoo A, Ten S. Insulin resistance, lipodystrophy and cardiometabolic syndrome in HIV/AIDS. Rev. Endocr. Metab. Disord. (2013) 14(2):133–40. doi: 10.1007/s11154-013-9247-7
32. Brown TT, Tassiopoulos K, Bosch RJ, Shikuma C, McComsey GA. Association between systemic inflammation and incident diabetes in HIV-infected patients after initiation of antiretroviral therapy. Diabetes Care (2010) 33(10):2244–9. doi: 10.2337/dc10-0633
33. Zicari S, Sessa L, Cotugno N, Ruggiero A, Morrocchi E, Concato C, et al. Immune activation, inflammation, and non-AIDS Co-morbidities in HIV-infected patients under long-term ART. Viruses (2019) 11(3):200. doi: 10.3390/v11030200
34. Festa A, D'Agostino R Jr., Williams K, Karter AJ, Mayer-Davis EJ, Tracy RP, et al. The relation of body fat mass and distribution to markers of chronic inflammation. Int. J. Obes. Relat. Metab. Disord. (2001) 25(10):1407–15. doi: 10.1038/sj.ijo.0801792
35. Pérez-Baos S, Prieto-Potin I, Román-Blas JA, Sánchez-Pernaute O, Largo R, Herrero-Beaumont G. Mediators and patterns of muscle loss in chronic systemic inflammation. Front. Physiol. (2018) 9:409–9. doi: 10.3389/fphys.2018.00409
36. Lake JE. The fat of the matter: Obesity and visceral adiposity in treated HIV infection. Curr. HIV/AIDS Rep. (2017) 14(6):211–9. doi: 10.1007/s11904-017-0368-6
37. Grunfeld C, Rimland D, Gibert CL, Powderly WG, Sidney S, Shlipak MG, et al. Association of upper trunk and visceral adipose tissue volume with insulin resistance in control and HIV-infected subjects in the FRAM study. J. Acquir Immune Defic Syndromes (1999) (2007) 46(3):283–90. doi: 10.1097/QAI.0b013e31814b94e2
38. Hadigan C, Meigs JB, Corcoran C, Rietschel P, Piecuch S, Basgoz N, et al. Metabolic abnormalities and cardiovascular disease risk factors in adults with human immunodeficiency virus infection and lipodystrophy. Clin. Infect. Dis. (2001) 32(1):130–9. doi: 10.1086/317541
39. Apovian CM, Bigornia S, Mott M, Meyers MR, Ulloor J, Gagua M, et al. Adipose macrophage infiltration is associated with insulin resistance and vascular endothelial dysfunction in obese subjects. Arterioscler. Thromb. Vasc. Biol. (2008) 28(9):1654–9. doi: 10.1161/ATVBAHA.108.170316
40. Wada NI, Jacobson LP, Margolick JB, Breen EC, Macatangay B, Penugonda S, et al. The effect of HAART-induced HIV suppression on circulating markers of inflammation and immune activation. AIDS (London England) (2015) 29(4):463–71. doi: 10.1097/QAD.0000000000000545
41. Leddy AM, Roque A, Sheira LA, Frongillo EA, Landay AL, Adedimeji AA, et al. Food insecurity is associated with inflammation among women living with HIV. J. Infect. Dis. (2019) 219(3):429–36. doi: 10.1093/infdis/jiy511
42. Canfora EE, Meex RCR, Venema K, Blaak EE. Gut microbial metabolites in obesity, NAFLD and T2DM. Nat. Rev. Endocrinol. (2019) 15(5):261–73. doi: 10.1038/s41574-019-0156-z
43. Zheng D, Liwinski T, Elinav E. Interaction between microbiota and immunity in health and disease. Cell Res. (2020) 30(6):492–506. doi: 10.1038/s41422-020-0332-7
44. Li SX, Armstrong A, Neff CP, Shaffer M, Lozupone CA, Palmer BE. Complexities of gut microbiome dysbiosis in the context of HIV infection and antiretroviral therapy. Clin. Pharmacol. Ther. (2016) 99(6):600–11. doi: 10.1002/cpt.363
45. Dillon SM, Frank DN, Wilson CC. The gut microbiome and HIV-1 pathogenesis: a two-way street. AIDS (London England) (2016) 30(18):2737–51. doi: 10.1097/QAD.0000000000001289
46. Gelpi M, Vestad B, Hansen SH, Holm K, Drivsholm N, Goetz A, et al. Impact of HIV-related gut microbiota alterations on metabolic comorbidities. Clin. Infect. Dis. (2020) 71(8):e359-e67. doi: 10.1093/cid/ciz1235
47. Benjamin-Neelon S, Differding M, Mueller N. Infants from food insecure households have altered gut microbiota (OR01-03-19). Curr. Develop Nutr. (2019) 3(Supplement_1). doi: 10.1093/cdn/nzz040.OR01-03-19
48. Guenter P, Muurahainen N, Simons G, Kosok A, Cohan GR, Rudenstein R, et al. Relationships among nutritional status, disease progression, and survival in HIV infection. J. Acquir. Immune Defic. Syndr. (1988) (1993) 6(10):1130–8.
49. Health Resources and Services Administration (HRSA). Ryan White HIV/AIDS program. In: RSR client characteristics in Oklahoma in 2018. HIV/AIDS Bureau. (2019). Available at: https://hab.hrsa.gov/stateprofiles2018/#/profile. Accessed January 14, 2022.
50. Health Resources and Services Administration (HRSA). Ryan White HIV/AIDS program services: Eligible individuals & allowable uses of funds, in policy clarification notice (PCN) #16-02. (2018).
51. Hebert JR, Shivappa N, Wirth MD, Hussey JR, Hurley TG. Perspective: The dietary inflammatory index (DII)-lessons learned, improvements made, and future directions. Adv. Nutr. (2019) 10(2):185–95. doi: 10.1093/advances/nmy071
52. Shivappa N, Bonaccio M, Hebert JR, Di Castelnuovo A, Costanzo S, Ruggiero E, et al. Association of proinflammatory diet with low-grade inflammation: results from the moli-sani study. Nutrition (2018) 54:182–8. doi: 10.1016/j.nut.2018.04.004
53. Phillips CM, Shivappa N, Hebert JR, Perry IJ. Dietary inflammatory index and biomarkers of lipoprotein metabolism, inflammation and glucose homeostasis in adults. Nutrients (2018) 10(8):1033. doi: 10.3390/nu10081033
54. Mtintsilana A, Micklesfield LK, Chorell E, Olsson T, Shivappa N, Hebert JR, et al. Adiposity mediates the association between the dietary inflammatory index and markers of type 2 diabetes risk in middle-aged black south African women. Nutrients (2019) 11(6):1246. doi: 10.3390/nu11061246
55. Moslehi N, Ehsani B, Mirmiran P, Shivappa N, Tohidi M, Hebert JR, et al. Inflammatory properties of diet and glucose-insulin homeostasis in a cohort of Iranian adults. Nutrients (2016) 8(11):735. doi: 10.3390/nu8110735
56. Data Resource Center for Child and Adolescent Health. America's health rankings analysis of U.S. HHS, HRSA, maternal and child health bureau (MCHB), child and adolescent health measurement initiative (CAHMI), national survey of children's health indicator data set (2020). Available at: https://www.americashealthrankings.org/explore/health-of-women-and-children/measure/ACEs/state/U.S.
57. LaVarnway J, Craven E. An overview of food deserts in Oklahoma: June 2017. (2017). Regional Food Bank of Oklahoma, Oklahoma City, OK
58. Coleman-Jensen A, Rabbitt MP, Gregory CA, Singh A. Household food security in the united states in 2018. Washington, DC: United States Department of Agriculture (2019).
60. Health Resources and Services Administration (HRSA). Ending the HIV epidemic: a plan for America. (2019). Available at: https://files.hiv.gov/s3fs-public/Ending-the-HIV-Epidemic-Counties-and-Territories.pdf
61. Mercer SL GL, Cargo M, Potter MA, Daniel M, Olds S, Reed-Gross E. Appendix c: Reliability-tested guidelines for assessing participatory research projects. In: Community-based participatory research for health: From process to outcomes. San Francisco: Jossey-Bass (2008). p. 407–18.
62. Wetherill M, John R, Wheeler D. Estimating food insecurity and its association with HIV-related health outcomes using self-administered surveys: A community-based research approach. London: SAGE Publications, Ltd (2017). Available from: https://methods.sagepub.com/case/food-insecurity-hiv-outcomes-self-administered-surveys-community-based.
63. USDA Economic Research Service. U.S. adult food security survey module: Three-stage design, with screeners. U.S: Department of Agriculture (2012).
64. Evans L, Lawler K, Sass S. Gathering sexual orientation data on statewise behavioral risk factor surveillance surveys: a call to action for states. Cahill S, editor. Boston, MA: The Fenway Institute (2014).
65. Bauer GR, Braimoh J, Scheim AI, Dharma C. Transgender-inclusive measures of sex/gender for population surveys: Mixed-methods evaluation and recommendations. PloS One (2017) 12(5):e0178043–e0178043. doi: 10.1371/journal.pone.0178043
66. Centers for Disease Control and Prevention. 2017 behavioral risk factor surveillance system questionnaire (2016). Available at: https://www.cdc.gov/brfss/questionnaires/pdf-ques/2017_BRFSS_Pub_Ques_508_tagged.pdf.
67. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. (2001) 16(9):606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
68. Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch. Intern. Med. (2006) 166(10):1092–7. doi: 10.1001/archinte.166.10.1092
69. Wu AW, Revicki DA, Jacobson D, Malitz FE. Evidence for reliability, validity and usefulness of the medical outcomes study HIV health survey (MOS-HIV). Qual Life Res. (1997) 6(6):481–93. doi: 10.1023/A:1018451930750
70. Ware JE Jr., Sherbourne CD. The MOS 36-item short-form health survey (SF-36). i. conceptual framework and item selection. Med. Care (1992) 30(6):473–83.
71. Feldman BJ, Fredericksen RJ, Crane PK, Safren SA, Mugavero MJ, Willig JH, et al. Evaluation of the single-item self-rating adherence scale for use in routine clinical care of people living with HIV. AIDS Behav. (2013) 17(1):307–18. doi: 10.1007/s10461-012-0326-7
72. Bethell C, Jones J, Gombojav N, Linkenbach J, Sege R. Positive childhood experiences and adult mental and relational health in a statewide sample: Associations across adverse childhood experiences levels. JAMA Pediatr. (2019) 173(11):e193007–e193007. doi: 10.1001/jamapediatrics.2019.3007
73. Nightingale VR, Sher TG, Mattson M, Thilges S, Hansen NB. The effects of traumatic stressors and HIV-related trauma symptoms on health and health related quality of life. AIDS Behav. (2011) 15(8):1870–8. doi: 10.1007/s10461-011-9980-4
74. Krieger N, Smith K, Naishadham D, Hartman C, Barbeau EM. Experiences of discrimination: validity and reliability of a self-report measure for population health research on racism and health. Soc. Sci. Med. (2005) 61(7):1576–96. doi: 10.1016/j.socscimed.2005.03.006
75. Green SH, Glanz K. Development of the perceived nutrition environment measures survey. Am. J. Prev. Med. (2015) 49(1):50–61. doi: 10.1016/j.amepre.2015.02.004
76. USDA. Food access research atlas. Available at: https://www.ers.usda.gov/data-products/food-access-research-atlas/.
77. University of Wisconsin School of Medicine Public Health. 2015 area deprivation index v2.0 (2020). Available at: https://www.neighborhoodatlas.medicine.wisc.edu/.
78. Waldorf BS. A continuous multi-dimensional measure of rurality: Moving beyond threshold measures. In: 2006 annual meeting. Long Beach, CA: American Agricultural Economics Association (2006).
79. Waldorf BS. What is rural and what is urban in Indiana? West Lafayette, IN: Purdue Center for Regional Development (2007).
80. Sallis JF, Grossman RM, Pinski RB, Patterson TL, Nader PR. The development of scales to measure social support for diet and exercise behaviors. Prev. Med. (1987) 16(6):825–36. doi: 10.1016/0091-7435(87)90022-3
81. Ball K, Crawford D. An investigation of psychological, social and environmental correlates of obesity and weight gain in young women. Int. J. Obes. (2006) 30(8):1240–9. doi: 10.1038/sj.ijo.0803267
82. Lavelle F, McGowan L, Hollywood L, Surgenor D, McCloat A, Mooney E, et al. The development and validation of measures to assess cooking skills and food skills. Int. J. Behav. Nutr. Phys. Act (2017) 14(1):118. doi: 10.1186/s12966-017-0575-y
83. Jahns L, Johnson LK, Mayne ST, Cartmel B, Picklo MJ Sr., Ermakov IV, et al. Skin and plasma carotenoid response to a provided intervention diet high in vegetables and fruit: uptake and depletion kinetics. Am. J. Clin. Nutr. (2014) 100(3):930–7. doi: 10.3945/ajcn.114.086900
84. Nes BM, Janszky I, Vatten LJ, Nilsen TIL, Aspenes St Wisløff U. Estimating V˙O2peak from a nonexercise prediction model: The HUNT study, Norway. Med. Sci. Sports Exercise (2011) 43(11):2024–30. doi: 10.1249/MSS.0b013e31821d3f6f
85. Prince SA, LeBlanc AG, Colley RC, Saunders TJ. Measurement of sedentary behaviour in population health surveys: a review and recommendations. PeerJ (2017) 5:e4130–0. doi: 10.7717/peerj.4130
86. Nes BM, Vatten LJ, Nauman J, Janszky I, Wisløff U. A simple nonexercise model of cardiorespiratory fitness predicts long-term mortality. Med. Sci. Sports Exercise (2014) 46(6):1159–65. doi: 10.1249/MSS.0000000000000219
87. Centers for Disease Control and Prevention. 2020 behavioral risk factor surveillance system questionnaire (2021). Available at: https://www.cdc.gov/brfss/questionnaires/pdf-ques/2020-BRFSS-Questionnaire-508.pdf.
88. Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO. The fagerström test for nicotine dependence: a revision of the fagerström tolerance questionnaire. Br. J. Addict. (1991) 86(9):1119–27. doi: 10.1111/j.1360-0443.1991.tb01879.x
89. Centers for Disease Control and Prevention. Biomonitoring summary: Cotinine (2017). Available at: https://www.cdc.gov/biomonitoring/Cotinine_BiomonitoringSummary.html.
90. Bush K, Kivlahan DR, McDonell MB, Fihn SD, Bradley KA, for the Ambulatory Care Quality Improvement P. The audit alcohol consumption questions (AUDIT-c): An effective brief screening test for problem drinking. Arch. Internal Med. (1998) 158(16):1789–95. doi: 10.1001/archinte.158.16.1789
91. National Cancer Institute. Automated self-administered 24-hour (ASA24®) dietary assessment tool. In: Division of cancer control and population sciences (2017). Available at: https://epi.grants.cancer.gov/asa24.
92. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J. Health Soc. Behav. (1983) 24(4):385–96. doi: 10.2307/2136404
93. John-Henderson NA, Ginty AT. Historical trauma and social support as predictors of psychological stress responses in American Indian adults during the COVID-19 pandemic. J. Psychos Res. (2020) 139:110263. doi: 10.1016/j.jpsychores.2020.110263
94. MedlinePlus. Calculating body frame size (2020). Available at: https://medlineplus.gov/ency/imagepages/17182.htm.
95. White JV, Guenter P, Jensen G, Malone A, Schofield M. Consensus statement: Academy of nutrition and dietetics and American society for parenteral and enteral nutrition: characteristics recommended for the identification and documentation of adult malnutrition (undernutrition). JPEN J. Parenter Enteral Nutr. (2012) 36(3):275–83. doi: 10.1177/0148607112440285
96. Centers for Disease Control and Prevention. National health and nutrition examination survey (NHANES): Anthropometry procedures manual. Atlanta, GA: CDC (2020). Availbale at: https://wwwn.cdc.gov/nchs/data/nhanes/2019-2020/manuals/2020-Anthropometry-Procedures-Manual-508.pdf
97. Azuma K, Heilbronn LK, Albu JB, Smith SR, Ravussin E, Kelley DE, et al. Adipose tissue distribution in relation to insulin resistance in type 2 diabetes mellitus. Am. J. Physiol. Endocrinol. Metab. (2007) 293(1):E435–42. doi: 10.1152/ajpendo.00394.2006
98. Rao SS, Disraeli P, McGregor T. Impaired glucose tolerance and impaired fasting glucose. Am. Fam Phys (2004) 69(8):1961–8.
99. Katz A, Nambi SS, Mather K, Baron AD, Follmann DA, Sullivan G, et al. Quantitative insulin sensitivity check index: a simple, accurate method for assessing insulin sensitivity in humans. J. Clin. Endocrinol. Metab. (2000) 85(7):2402–10. doi: 10.1210/jcem.85.7.6661
100. FAO. Declaration of the world food summit on food security. Rome: Food and Agriculture Organization of the United Nations (2009).
101. Tarasuk V, McIntyre L, Li J. Low-income women's dietary intakes are sensitive to the depletion of household resources in one month. J. Nutr. (2007) 137(8):1980–7. doi: 10.1093/jn/137.8.1980
102. Nyambose J, Koski KG, Tucker KL. High intra/interindividual variance ratios for energy and nutrient intakes of pregnant women in rural Malawi show that many days are required to estimate usual intake. J. Nutr. (2002) 132(6):1313–8. doi: 10.1093/jn/132.6.1313
103. Kozich JJ, Westcott SL, Baxter NT, Highlander SK, Schloss PD. Development of a dual-index sequencing strategy and curation pipeline for analyzing amplicon sequence data on the MiSeq illumina sequencing platform. Appl. Environ. Microbiol. (2013) 79(17):5112–20. doi: 10.1128/AEM.01043-13
104. Slade GD, Spencer AJ. Development and evaluation of the oral health impact profile. Community Dent. Health (1994) 11(1):3–11.
105. Gassman-Pines A, Schenck-Fontaine A. Daily food insufficiency and worry among economically disadvantaged families with young children. J. Marriage Family (2019) 81(5):1269–84. doi: 10.1111/jomf.12593
106. Lewis SJ, Heaton KW. Stool form scale as a useful guide to intestinal transit time. Scand. J. Gastroenterol. (1997) 32(9):920–4. doi: 10.3109/00365529709011203
107. Muniyappa R, Madan R, Varghese RT. Assessing insulin sensitivity and resistance in humans. In: Feingold KR, et al, editors. Endotext. South Dartmouth (MA: MDText.com, Inc (2000). MDText.com, Inc. Copyright © 2000-2022.
108. Mather KJ, Hunt AE, Steinberg HO, Paradisi G, Hook G, Katz A, et al. Repeatability characteristics of simple indices of insulin resistance: implications for research applications. J. Clin. Endocrinol. Metab. (2001) 86(11):5457–64. doi: 10.1210/jcem.86.11.7880
109. Chen H, Sullivan G, Quon MJ. Assessing the predictive accuracy of QUICKI as a surrogate index for insulin sensitivity using a calibration model. Diabetes (2005) 54(7):1914–25. doi: 10.2337/diabetes.54.7.1914
110. Katsuki A, Sumida Y, Gabazza EC, Murashima S, Urakawa H, Morioka K, et al. QUICKI is useful for following improvements in insulin sensitivity after therapy in patients with type 2 diabetes mellitus. J. Clin. Endocrinol. Metab. (2002) 87(6):2906–8. doi: 10.1210/jcem.87.6.8592
111. Berkowitz SA, Gao X, Tucker KL. Food-insecure dietary patterns are associated with poor longitudinal glycemic control in diabetes: results from the Boston Puerto Rican health study. Diabetes Care (2014) 37(9):2587–92. doi: 10.2337/dc14-0753
112. Hendricks KM, Willis K, Houser R, Jones CY. Obesity in HIV-infection: dietary correlates. J. Am. Coll. Nutr. (2006) 25(4):321–31. doi: 10.1080/07315724.2006.10719542
113. Makki K, Deehan EC, Walter J, Backhed F. The impact of dietary fiber on gut microbiota in host health and disease. Cell Host Microbe (2018) 23(6):705–15. doi: 10.1016/j.chom.2018.05.012
114. Willett WC. Correction for the effects of measurement error. In: Nutritional epidemiology. New York: Oxford University Press (2013).
115. Fowke JH, Hebert JR, Fahey JW. Urinary excretion of dithiocarbamates and self-reported cruciferous vegetable intake: application of the 'method of triads' to a food-specific biomarker. Public Health Nutr. (2002) 5(6):791–9. doi: 10.1079/PHN2002345
116. Van Dam RM, Hunter D. Biochemical indicators of dietary intake. In: Willett WC, editor. Nutritional epidemiology. New York: Oxford University Press (2013).
117. Beaton GH, Milner J, Corey P, McGuire V, Cousins M, Stewart E, et al. Sources of variance in 24-hour dietary recall data: implications for nutrition study design and interpretation. Am. J. Clin. Nutr. (1979) 32(12):2546–59. doi: 10.1093/ajcn/32.12.2546
118. Kline RB. Principles and practice of structural equation modeling. Little TD, editor. New York: Guilford Press (2005).
119. Glass TA, McAtee MJ. Behavioral science at the crossroads in public health: extending horizons, envisioning the future. Soc. Sci. Med. (2006) 62(7):1650–71. doi: 10.1016/j.socscimed.2005.08.044
120. Wolf EJ, Harrington KM, Clark SL, Miller MW. Sample size requirements for structural equation models: An evaluation of power, bias, and solution propriety. Educ. psychol. Measure (2013) 76(6):913–34. doi: 10.1177/0013164413495237
121. Hartwell ML, Khojasteh J, Wetherill MS, Croff JM, Wheeler D. Using structural equation modeling to examine the influence of social, behavioral, and nutritional variables on health outcomes based on NHANES data: Addressing complex design, nonnormally distributed variables, and missing information. Curr. Develop Nutr. (2019) 3(5). doi: 10.1093/cdn/nzz010
122. Bolyen E, Rideout JR, Dillon MR, Bokulich NA, Abnet CC, Al-Ghalith GA, et al. Reproducible, interactive, scalable and extensible microbiome data science using QIIME 2. Nat. Biotechnol. (2019) 37(8):852–7. doi: 10.1038/s41587-019-0209-9
123. Segata N, Izard J, Waldron L, Gevers D, Miropolsky L, Garrett WS, et al. Metagenomic biomarker discovery and explanation. Genome Biol. (2011) 12(6):R60–0. doi: 10.1186/gb-2011-12-6-r60
124. Freeland-Graves J, Babaei M, Sachdev P. Food insecurity and periodontal disease in low-income women (P04-043-19). Curr. Develop Nutr. (2019) 3(Supplement_1). doi: 10.1093/cdn/nzz051.P04-043-19
125. Santin GC, Martins CC, Pordeus IA, Ferreira FM. Food insecurity and oral health: A systematic review. Pesquisa Bras. em Odontopediatria e Clin Integrada (2014) 144):335–246. doi: 10.4034/PBOCI.2014.144.08
126. Mataftsi M, Skoura L, Sakellari D. HIV Infection and periodontal diseases: an overview of the post-HAART era. Oral. Dis. (2011) 17(1):13–25. doi: 10.1111/j.1601-0825.2010.01727.x
127. Valentine J, Saladyanant T, Ramsey K, Blake J, Morelli T, Southerland J, et al. Impact of periodontal intervention on local inflammation, periodontitis, and HIV outcomes. Oral. Dis. (2016) 22 Suppl 1:87–97. doi: 10.1111/odi.12419
128. Gorvitovskaia A, Holmes SP, Huse SM. Interpreting prevotella and bacteroides as biomarkers of diet and lifestyle. Microbiome (2016) 4(1):15. doi: 10.1186/s40168-016-0160-7
129. Most MM. Estimated phytochemical content of the dietary approaches to stop hypertension (DASH) diet is higher than in the control study diet. J. Am. Diet Assoc. (2004) 104(11):1725–7. doi: 10.1016/j.jada.2004.08.001
130. Jahns L, Whigham L, Johnson L, Mayne S, Cartmel B, Ermakov I, et al. Dermal carotenoids as measured by resonance raman spectroscopy as a biomarker of response to a Fruit/Vegetable intervention study. FASEB J. (2012) 26(1_supplement):131.3–3. doi: 10.1096/fasebj.26.1_supplement.131.3
Keywords: food insecurity, food access, insulin resistance, HIV- human immunodeficiency virus, inflammation, microbiome, community-based participatory research (CBPR), structural equation modeling
Citation: Wetherill MS, Bakhsh C, Caywood L, Williams MB, Hartwell ML, Wheeler DL, Hubach RD, Teague TK, Köhler G, Hebert JR and Weiser SD (2022) Unpacking determinants and consequences of food insecurity for insulin resistance among people living with HIV: Conceptual framework and protocol for the NOURISH-OK study. Front. Clin. Diabetes Healthc. 3:947552. doi: 10.3389/fcdhc.2022.947552
Received: 18 May 2022; Accepted: 01 July 2022;
Published: 16 August 2022.
Edited by:
Elena Succurro, University of Magna Graecia, ItalyReviewed by:
Ceren Gezer, Eastern Mediterranean University, TurkeyCopyright © 2022 Wetherill, Bakhsh, Caywood, Williams, Hartwell, Wheeler, Hubach, Teague, Köhler, Hebert and Weiser. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marianna S. Wetherill, bWFyaWFubmEtd2V0aGVyaWxsQG91aHNjLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.