 Antonia Huhndt1
Antonia Huhndt1 Yanbing Chen2
Yanbing Chen2 Shane O’Donnell3
Shane O’Donnell3 Drew Cooper1
Drew Cooper1 Hanne Ballhausen1,4,5
Hanne Ballhausen1,4,5 Katarzyna A. Gajewska5,6
Katarzyna A. Gajewska5,6 Timothée Froment5
Timothée Froment5 Mandy Wäldchen3
Mandy Wäldchen3 Dana M. Lewis7Klemens Raile1
Dana M. Lewis7Klemens Raile1 Timothy C. Skinner8,9,10
Timothy C. Skinner8,9,10 Katarina Braune1,4,11*
Katarina Braune1,4,11*- 1Department of Paediatric Endocrinology and Diabetes, Charité—Universitätsmedizin Berlin, Berlin, Germany
- 2School of Public Health, Physiotherapy & Sports Science, University College Dublin, Belfield, Ireland
- 3School of Sociology, University College Dublin, Belfield, Ireland
- 4Berlin Institute of Health (BIH), Berlin, Germany
- 5#dedoc° Diabetes Online Community, Dedoc Labs GmbH, Berlin, Germany
- 6Population Health Sciences, Royal College of Surgeons in Ireland, Dublin, Ireland
- 7OpenAPS, Seattle, WA, United States
- 8Department of Psychology, University of Copenhagen, Copenhagen, Denmark
- 9Australian Centre for Behavioural Research in Diabetes, Melbourne, Australia
- 10La Trobe University, Bendigo, Australia
- 11Institute of Medical Informatics, Charité—Universitätsmedizin Berlin, Berlin, Germany
Background: As a treatment option for people living with diabetes, automated insulin delivery (AID) systems are becoming increasingly popular. The #WeAreNotWaiting community plays a crucial role in the provision and distribution of open-source AID technology. However, while a large percentage of children were early adopters of open-source AID, there are regional differences in adoption, which has prompted an investigation into the barriers perceived by caregivers of children with diabetes to creating open-source systems.
Methods: This is a retrospective, cross-sectional and multinational study conducted with caregivers of children and adolescents with diabetes, distributed across the online #WeAreNotWaiting online peer-support groups. Participants—specifically caregivers of children not using AID—responded to a web-based questionnaire concerning their perceived barriers to building and maintaining an open-source AID system.
Results: 56 caregivers of children with diabetes, who were not using open-source AID at the time of data collection responded to the questionnaire. Respondents indicated that their major perceived barriers to building an open-source AID system were their limited technical skills (50%), a lack of support by medical professionals (39%), and therefore the concern with not being able to maintain an AID system (43%). However, barriers relating to confidence in open-source technologies/unapproved products and fear of digital technology taking control of diabetes were not perceived as significant enough to prevent non-users from initiating the use of an open-source AID system.
Conclusions: The results of this study elucidate some of the perceived barriers to uptake of open-source AID experienced by caregivers of children with diabetes. Reducing these barriers may improve the uptake of open-source AID technology for children and adolescents with diabetes. With the continuous development and wider dissemination of educational resources and guidance—for both aspiring users and their healthcare professionals—the adoption of open-source AID systems could be improved.
Introduction
There are about 1.2 million children and adolescents <20 years of age worldwide who live with type 1 diabetes (1). To reduce their risks of acute and long-term complications, therapeutic guidelines recommend target hemoglobin A1c levels of <7,0% (2, 3). However, not all children and adolescents achieve these glycemic targets. Methods for treating diabetes vary widely (4, 5). Technology is evolving rapidly and continuously, which is significant in improving health conditions. Medical devices, mobile technology, cloud computing, and social media make it possible—especially for patients—to improve, co-design, and co-develop new treatments (6). This possibility is particularly important for children and adolescents living with diabetes, as well as their caregivers and families (7).
Automated Insulin Delivery (AID) systems represent an important advance in diabetes therapy. Given the limitations in access to this technology, the #WeAreNotWaiting community has created so-called “Do-It-Yourself Artificial Pancreas Systems” (DIYAPS) or ‘open-source AID’ systems and made the resources needed to build them available via open-source platforms (7–10). These systems are not approved by regulatory bodies and thus are used by people with diabetes at their own risk. However, devices that are approved and commercially available are needed as components (e.g. insulin pumps and continuous glucose monitoring (CGM) systems). There are several types of open-source AID systems each with multiple different branches. While OpenAPS runs the algorithm on a Linux-based minicomputer, AndroidAPS, Loop, and FreeAPS are smartphone applications. Depending on the setup, additional hardware (e.g. OpenAPS rig, Riley-, Orange- or EmaLink) and software components (e.g. xDrip+, Nightscout) may also be required (11, 12). The algorithms for automated insulin delivery adjust insulin dosing according to the user’s glycemic levels. Previous studies have shown that open-source AID systems have the potential to improve clinical outcomes in users of several age groups (e.g. better HbA1c-level and time in range (TIR)) (13–23). Moreover, they reduce the individual burden of living with diabetes, such as improving quality of life and sleep quality (14, 24–28). A profound understanding of pump therapy and CGM systems, but also technical literacy are needed to successfully build and use open-source AID (25, 29–32). The questions that arise include who is actually able to use and even create this technology and who would benefit from it (33, 34).
Few studies have examined the perceived barriers to adopting open-source AID solutions. Schipp et al. looked at the perceived challenges of adults during the set-up of their AID system (25). However, this work and most other research reports almost exclusively focus on the experiences and emotions of people with diabetes who have already successfully built and are using an open-source system. Among members of online support groups such as “Looped” on Facebook (N=28,323), there are a number of people with diabetes and caregivers of children who have not yet built and used open-source AID. O’Donnell et al. previously identified barriers perceived by adult non-users (35), but evidence is currently lacking concerning children and adolescents with diabetes and their caregivers. Therefore, it might be possible that the barriers to building and using open-source AID are not completely identified yet. To fill such an evidence gap, this paper refers to the caregivers of children living with diabetes. One of the challenges to addressing this gap is that to respond to questions about the barriers to using open-source AID systems, it is necessary to recruit caregivers who know about these systems and have some understanding of what it entails to build and maintain them. Therefore, this study aimed to recruit caregivers from the #WeAreNotWaiting community who meet these criteria. Clearly, with members of this well-informed and pro-active community, it is to be expected that there are biases with this sample. Hence, our results will not include the barrier of not knowing about the systems.
The overall aim of this study is to 1) investigate the barriers to scale-up open-source AID systems in caregivers of children and adolescents in the #WeAreNotWaiting community who are non-users of open-source AID and 2) analyze the participants’ socioeconomic status in relation to the perceived barriers.
Methods
Study Design
This survey was part of a large retrospective, multinational, web-based cross-sectional study conducted from September to November 2020 with users and non-users of open-source AID within the #WeAreNotWaiting community. Two questionnaires, titled “Your Thoughts about DIYAPS” (DIWHYnot) and “About you and your child” (socioeconomic factors) were distributed to caregivers of children with diabetes who were still non-users of open-source AID.
Survey Tool
Questionnaires were designed by an interdisciplinary team of researchers living with type 1 diabetes and were both users and non-users of open-source AID (35); some researchers had used open-source AID for several years, some were in the process of uptaking systems, and others were not interested in using open-source AID. TF—a non-user—provided statements about challenges regarding the set-up, which were reviewed and completed by users (SO, DL, KB, MW) and non-users (KAG) to generate a final list of items. The ‘DIWHYnot’ questionnaire comprised of a combination of check-box items with comments, and questions on a 5-point Likert scale (“Strongly Agree”, “Agree”, “Neither Agree or Disagree’’, “Disagree” and “Strongly Disagree”); respondents were able to choose “Other”, “I don’t know” or “I’d rather not say” in response to the questions (Appendix A). The questionnaire applied branching logic to address progressively more specific questions. “About you and your child” used mostly check-box items and open-field inputs to collect information on socio-economic factors; respondents were again capable of answering “I’d rather not say”, “Other”, “None of the above’’ or “I don’t know”, allowing each participant to be included in the statistics (Appendix B).
Participants and Recruitment
Caregivers (e.g. a parent, family member, or legal guardian) of children and adolescents under the age of 18 who are living with diabetes were eligible for participation. The participants were recruited via Facebook groups including the multinational “Looped” groups, “AndroidAPS users”, “CGM in the Cloud” and “Nightscout Germany”; through the OPEN website; and social media accounts such as “Diabetes Daily”. The survey was conducted using the REDCap electronic data capture tool hosted by Charité – Universitätsmedizin Berlin. Ethical approval for the survey—including all questionnaires—was granted by the Life Sciences Human Research Ethics Committee at University College Dublin (LS-20-37).
Data Analysis
After data cleaning, analyses were conducted using IBM SPSS Statistics 27 (International Business Machines Corporation, Armonk, NY, United States) and Microsoft Office (Microsoft Corporation, Redmond, WA, United States). Validity and internal consistency (e.g. factor analysis, Cronbach’s alpha) tests of specific survey items were performed followed by descriptive and inferential analyses (e.g. Levene’s test, independent samples t-test).
Results
Participant Characteristics
Of the 1052 total participants of the OPEN study, 56 were caregivers of children with diabetes who were not using open-source AID at the time of data collection (Supplementary Figure 1). Responses from 49 participants were included in the analysis of socioeconomic factors (of children and caregivers). Overall, 59.2% of the children were male with a mean age of 11 years (range: 1-18 years, SD: 3 years). The participants were from 13 different countries of which 67.3% were from Germany (n=12), Denmark (n=11), the United Kingdom (n=5), and the United States (n=5). Of the participants, 87.8% described the ethnicity of the children as “White”. 63.3% of the caregivers were employed either full- or part-time, mostly in the science sector (32.6%), most commonly with educational qualifications of a Master’s (34.7%) or Bachelor’s degree (30.6%). The majority reported annual household income ranged from 100 000 to 199 999 US dollars (32.7%) and 50 000 to 99 999 US dollars (20.4%). Supplementary Table 1 summarizes the demographic data in detail. Most participants (84.6%; n=22/26) expressed they wanted to learn more about open-source AID, especially regarding the support they would get if they decided to build a system. More than half of them (64.3%; n=18/28) have not yet created a system but could imagine doing so under certain conditions. Among those who could imagine building an open-source AID system, most (30.4%; n=17/56) were interested in “Loop” (app for Apple iPhones). While 61.5% (n=16/26) were convinced and wanted to create a system, a smaller group (21.4%; n=6/28) were already in the process of setting up a system but had not yet used it. 28.6% (n=16/56) did not report out-of-pocket expenses for the required diabetes equipment, while the remaining participants pay up to 50 USD per month (7.1%; n=4/56), rarely more. Expenses for insulin were reported most often (14.3%; n=8/56), followed by CGM sensors (10.7%; n=6/56). When asked how the participants had heard about open-source AID, the majority responded “I have heard of it through social media” (48.2%; n=27/56).
Types of Barriers
Only a few respondents (11.1%; n=3/27) perceived the necessary components were too expensive. 33.3% (n=9/27) were interested in building an open-source AID but did not know where to source some of the components, especially additional components, such as the RileyLink and OpenAPS rig (77.8%; n=7/9) and loopable pumps (66.7%; n=6/9).
Overall, the result of the internal consistency analysis was acceptable (Cronbach’s alpha=0.741). 18 out of 20 items questioned all perceived barriers except for the procurement and the costs of necessary components to use open-source AID (Cronbach’s alpha=0.730). The reliability of the remaining 18 items was improved by deleting several statements, with Cronbach’s alpha increasing to 0.807. Following the elimination of the items “insufficient expertise of diabetes teams”, the “missing knowledge about pump therapy” and the “imagination to carry the required equipment”, a good internal consistency was achieved. The remaining 15 items were examined through exploratory factor analysis using principal component analysis and the Varimax rotation method, which indicated the point of inflection on the screen plot was at three factors and this generated a simple solution (factors only loading > 0.4 on one factor (Table 1). As the results suggested, the 15 items can be reduced to three components (cumulative proportion=60.71%): Dimension 1 “building and maintenance” of a system, Dimension 2 “therapy knowledge and trust in technology” and Dimension 3 “support and liability”. The item “My child is currently using commercial automated delivery systems.” (loading<0.4) did not fit into any of the dimensions. Thus, our final scale was best represented by the remaining 14 items in Table 1.
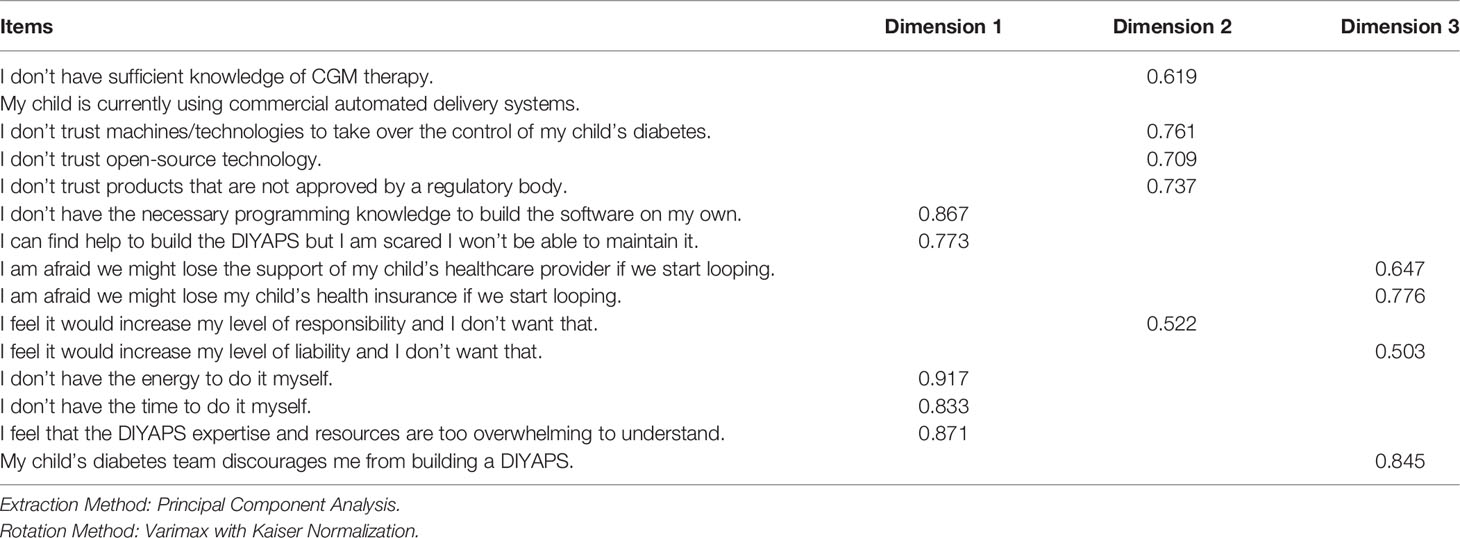
Table 1 Item Factor Loadings > 0.4 for Final 14 Items in the Barriers to Uptake Questionnaire.
Regarding “building and maintenance” of the open-source AID system, half of the participants reported (n=14/28) that they did not perceive having the skills needed to build it. 42.9% (n=12/28) knew they could find help to set it up, but were not sure if they would be able to maintain the system. Lack of time (33.3%; n=9/27) and too little energy (32.1%; n=9/28) were concerns, in addition to that resources are too overwhelming to understand (35.7%; n=10/28). In terms of “therapy knowledge and trust in technology”, respondents were most likely to fear having to take on additional responsibility (21.4%; n=6/28). Insufficient knowledge about CGM was reported by 14.3% (n=4/28). Only a minority of the respondents (7.1%; n=2/28) reported a lack of trust in machines and technologies to take over the control of diabetes in general. Similarly, only one respondent reported a lack of trust in products that have not been approved by a regulatory body. As for “support and liability”, by far the biggest concern was a potential loss of support by the healthcare provider (39.3%; n=11/28), followed by discouraging the uptake of an open-source AID by the diabetes team (25%; n=7/28). There was less agreement on both the fear of losing health insurance if they start looping and the worry that liability would increase (10.7%; n=3/28). Additionally, it is important to mention that 44.4% (n=12/27) reported no available support from healthcare professionals (HCP) of the diabetes care team due to their limited expertise in diabetes technology in general (Figure 1).
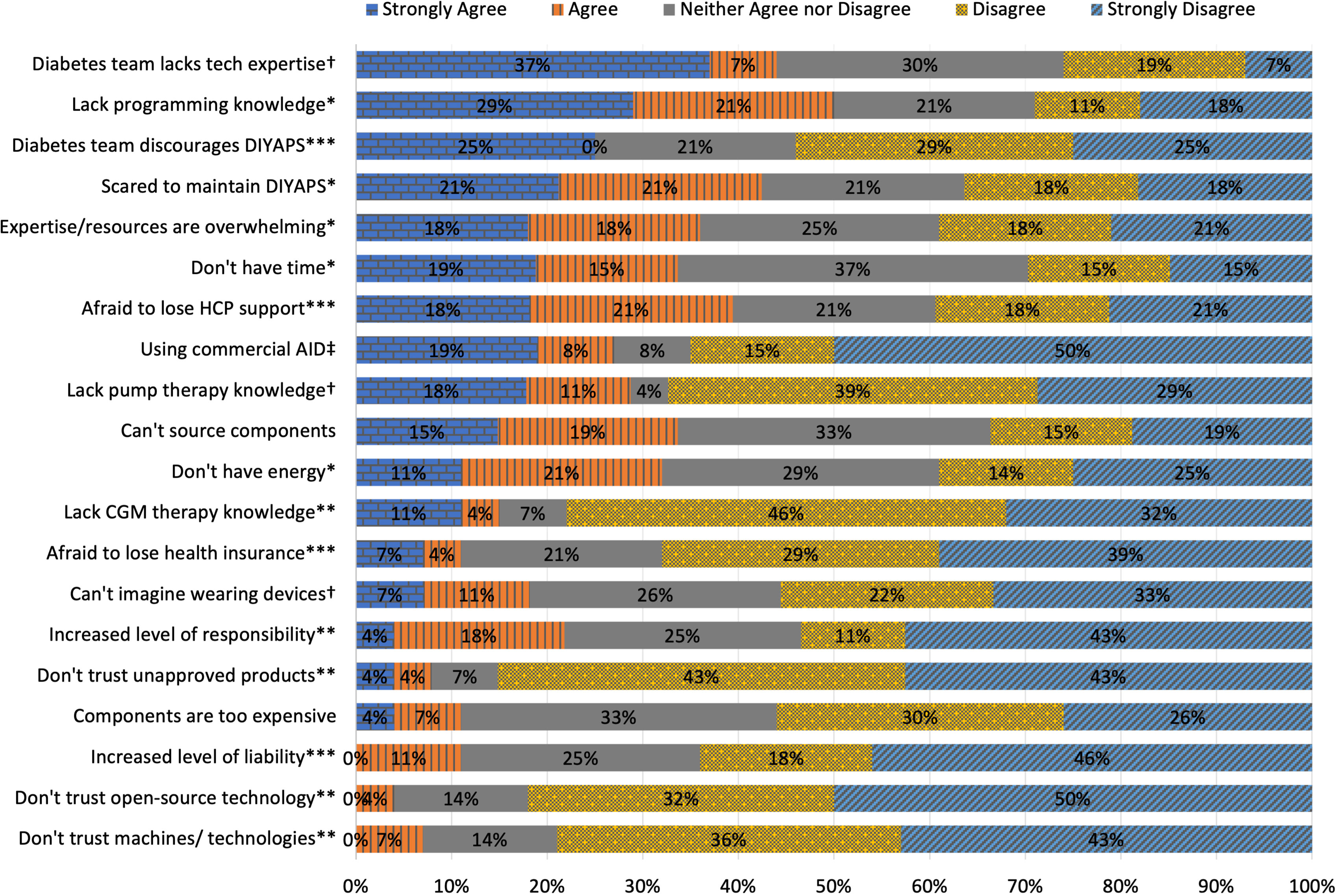
Figure 1 N=56; responses to statements regarding interest in building an open-source AID (“I would be interested in building a DIYAPS, but…”). Participants rated statements on a 5-point Likert scale (strongly agree, agree, neither agree nor disagree, disagree, strongly disagree). The responses were classified into three dimensions using principal component analysis and are labeled accordingly (*Building and Maintenance, **Knowledge and Trust in Technology, ***Support and Liability, † were excluded due to reduced reliability, ‡ was excluded after principal component analysis due to insufficient loading).
Encouragement
It is remarkable that many of the respondents would be encouraged to set up an AID system if their decision was officially supported. For example, 88.9% (n=24/27) confirmed “strongly agree” or “agree” that they would be motivated to start an open-source AID if their HCP recommended it. A similar number (80.8%; n=21/26) would be convinced if professional diabetes associations such as the International Diabetes Federation supported their use. Both the support of diabetes care teams (77.8%; n=21/27) and increased uptake in open-source AID in healthcare in general (74.1%; n=20/27) would encourage some caregivers to consider taking up a system. However, for slightly more than half of the participants (55.6%; n=15/27), it is also important that there is a company to provide warranty and support in case of technical errors.
Differences by Education Level and Household Income
To determine whether perceptions of different barriers are related to educational attainment, participants with Bachelor’s and Master’s degrees, as well as different household income groups were compared (Table 2).
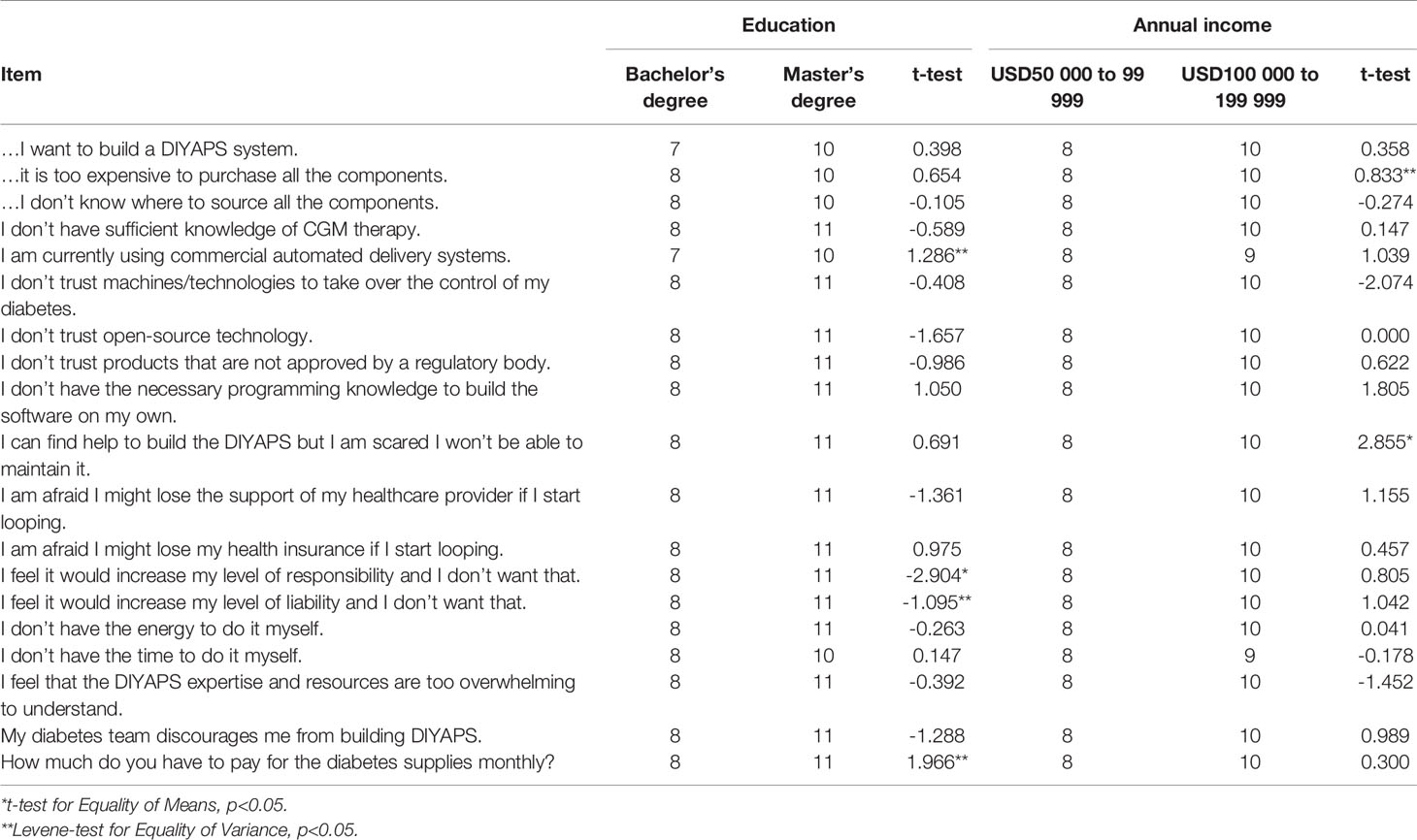
Table 2 Comparison of education and annual household income level of caregivers of children and adolescents who are non-users of open-source AID.
The worry about having to take on additional responsibility when using open-source AID differed significantly between caregivers with a Bachelor’s and a Master’s degree (T-test, T=-2.904, df=17, p=0.01), with participants with a Master’s degree being more aware. No significant differences were found regarding the caregivers’ motivation to build open-source AID (T-test, T=0.398, df=15, p=0.69) or concerns about sourcing components (T-test, T=-0.105, df=16, p=0.92). Differences were also found between the income groups of USD 50 000 to 99 999 and USD 100 000 to 199 999 per year. The worry of not being able to regularly maintain the open-source AID system once they have successfully built it was perceived as more significant for caregivers with a higher income (T-test, T=2.855, df=16, p=0.01). Non-significant differences were found for insufficient programming skills (T-test, T=1.805, df=16, p=0.09) and fear of losing support from the healthcare provider (T-test, T=1.155, df=16, p=0.27).
Discussion
Non-users of open-source AID reported several structural and individual barriers to the adoption of open-source AID. Structural barriers concerned the sourcing of compatible insulin pumps and additional components. Major individual barriers were limited perceived technical skills such as programming knowledge, limited support by medical professionals, and therefore the concerns of not being able to build and maintain the AID system by themselves. However, it was neither the confidence in the open-source technologies and lack of their regulatory approval nor the fear of digital technologies taking over the control of diabetes management that prevented non-users from creating and using an open-source AID system. Except for the two significant characteristics of annual household income and highest educational degree, socioeconomic status did not have a significant impact on the perceived barriers.
The structural problem of obtaining suitable insulin pumps could best be explained by the fact that not all compatible models are available via prescription. A compatible insulin pump refers to one that can interoperate with the algorithm and receive commands to adjust insulin delivery. Although the number of compatible insulin pump models has increased in recent years, some “loopable” pumps are only available on prescription in select countries, insurances often set time limits when a prescription can be renewed, and the availability of older out-of-warranty pump models, e.g. traded second-hand via online platforms, is limited. A previous study on barriers to the adoption of insulin pumps in Ireland has identified some people with diabetes having difficulties in orienting and understanding the health systems and their reimbursement principles (36). In terms of individual challenges, the self-perceived insufficient programming skills emerged as very relevant.
Finally, non-users were concerned about their ability to maintain and service the system on their own. Previous studies describing the experiences of those who have successfully set up open-source AID have shown that peer-support can help overcome this barrier (25, 37) with the support of experienced or technically versed community members. Their fears and worries could be alleviated and their self-confidence and determination could be strengthened through the achievement of successfully setting up an AID system. Therefore, connecting with other members of the #WeAreNotWaiting community online or in-person, as well as utilizing the available resources (e.g., online documentation and tutorials) could help close pre-existing knowledge gaps.
Similarly, respondents reported not receiving the desired support from their diabetes care teams, e.g., as they have limited necessary expertise in diabetes technology in general and open-source AID in particular. Medical professionals are important gatekeepers when it comes to access to open-source AID and, in fact, all diabetes technology. Many families with children with diabetes experience difficulties in access to AID systems, i.e., because these are not yet approved in their countries, are not approved for children of a particular age or are not reimbursed. It may take many years until AID technology is fully affordable and accessible for everyone. Until such time, open-source AID will continue to “fill the gap” for some people with diabetes in accessing this life-enhancing technology and therefore merits the support of medical professionals as well as other stakeholders in the diabetes community. Previous work has highlighted that HCPs are caught in a dilemma between the uncertainty regarding liability, the lack of regulatory approval of open-source AID, and supporting the choice and best interest of their patients (12, 33, 38). Meanwhile, individuals with diabetes may also face an associated dilemma between the advantages of using an AID system and the risk of losing support from HCPs. It seems that the open-source innovations have gained more acceptance among some HCPs, but not the majority of them. Due to the trend, more knowledge about the technology is available and can be used for supporting patients who are interested in applying an AID system (39). Therefore, changing medical guidelines to support open-source AID could help to reduce concerns of people with diabetes and remove the two barriers “insufficient expertise of diabetes teams” and the associated “lack of support”. This point of view has already been supported by other authors who looked at the perspectives of HCPs (34, 39–42). A recently published international consensus statement provided practical guidance to HCPs and specifically addressed professional educational aspects but also ethical and legal issues (12). For children and adolescents specifically, the consensus group recommended that the child’s welfare should always be considered by HCPs and caregivers who are setting up open-source AID for children, with the child’s assent and engagement (12). Further research should investigate the experiences and thoughts of HCPs and particularly address the challenges of procuring necessary devices (insulin pumps, CGM) via prescription (12, 39, 43–47).
To the best of the authors’ knowledge, this is the first study that is determining the perceived challenges in detail that are seen by caregivers of children and adolescents with diabetes when setting up an open-source AID. Previous studies have specifically examined the experiences of adult users (less so children) with open-source AID (14, 17, 25, 37, 48, 49). The fact that most of the involved researchers have personal experience with open-source AID as active users in addition to their professional roles, as well as the involvement of non-users in the study design underlines the public and patient engagement as a strength of this paper. Of further strength is the multinational character of this study. Nevertheless, several limitations apply as the sample size of 56 participants is relatively small compared to other sub-cohorts that participated in the OPEN survey. Furthermore, the participants identified predominantly as “White”, based in North America and Europe, and mostly had a high socioeconomic status. The number of participants with an educational level lower than a Bachelor’s degree was too small to be included in the factor analysis. Therefore, the sample is not representative of all caregivers of children with diabetes who are not using an open-source AID system, and the results may not reflect the non-user population of developing and emerging countries (50). Finally, based on the results of the reliability and validity tests, the items of the questionnaires could be adapted and improved for further surveys. Given the smaller sample size and socioeconomic background of this specific population, it would be of interest to investigate barriers in non-users outside the #WeAreNotWaiting community. Previous studies described motivations, enablers, and sources of support in open-source AID users (adults and caregivers of children) (14, 25, 27). While this paper describes barriers that prevent non-users from building open-source AID, it may be equally important to investigate what might encourage them to do so.
Lastly, as commercially developed AID systems have recently become available in select countries and can be made available via prescription, it would be of interest to investigate barriers to uptake with respect to commercial AID systems and outside the context of the #WeAreNotWaiting community as well.
As part of a retrospective, multinational, web-based cross-sectional study of the #WeAreNotWaiting community, this work has identified caregivers’ challenges for uptaking an open-source AID system. In order to increase the distribution of open-source AID, using online resources and community peer-support could be useful and complement support from medical professionals. Sharing problems that occurred during the build and use of open-source AID, and how these were encountered, could be insightful to aspiring users. The current open-source AID documentation already includes a comprehensive list of build errors and solution strategies. The findings of this study could help the #WeAreNotWaiting community to further extend these resources to better meet the needs of current non-users. In addition, providing educational resources to HCPs, such as the recently published consensus statement, could also help care teams to understand and better support current and future open-source AID users. Finally, regional differences and limitations in the availability of insulin pumps and CGM systems as AID components should be addressed by manufacturers, regulators, and policymakers. If access to diabetes technology would be more equal, many more people with diabetes would be able to benefit from digital innovations.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving human participants were reviewed and approved by Life Sciences Human Research Ethics Committee at University College Dublin. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
TF, KG, SO’D, DL, MW and KB created the survey design. Ethics approval was sought by SO’D. AH, YC, DC, SO’D, HB and KB processed and analyzed the data. AH and KB wrote the initial draft of the manuscript. All co-authors had access to the full data set, and have critically reviewed and revised the manuscript, approved the final version of the manuscript and can confirm the integrity of the study.
Funding
The authors declare that this study received funding from European Commission's Horizon 2020 Research and Innovation Program under the Marie-Sklodowska-Curie Action Research and Innovation Staff Exchange (RISE) grant agreement number 823902, the DFG-funded Digital Clinician Scientist Program of the Berlin Institute of Health (BIH), and the SPOKES Wellcome Trust Translational Partnership Program. The funders was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of Interest
Authors HB, KG and TF were employed by company Dedoc Labs GmbH.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank the members of the #WeAreNotWaiting community and their families for their collaboration and support in co-creating and disseminating this study.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcdhc.2022.876511/full#supplementary-material
References
1. Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF Diabetes Atlas: Global, Regional and Country-Level Diabetes Prevalence Estimates for 2021 and Projections for 2045. Diabetes Res. Clin. Pract. (2022) 183:109119. doi: 10.1016/j.diabres.2021.109119
2. DiMeglio LA, Acerini CL, Codner E, Craig ME, Hofer SE, Pillay K, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Glycemic Control Targets and Glucose Monitoring for Children, Adolescents, and Young Adults With Diabetes. Pediatr. Diabetes (2018) 19 Suppl 27:105–14. doi: 10.1111/pedi.12737
3. American Diabetes Association Professional Practice Committee, American Diabetes Association Professional Practice Committee, Draznin B, Aroda VR, Bakris G, Benson G, et al. 6. Glycemic Targets: Standards of Medical Care in Diabetes-2022. Diabetes Care (2022) 45:S83–96. doi: 10.2337/dc22-S006
4. Sherr JL, Tauschmann M, Battelino T, de Bock M, Forlenza G, Roman R, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Diabetes Technologies. Pediatr. Diabetes (2018) 19 Suppl 27:302–25. doi: 10.1111/pedi.12731
5. Danne T, Phillip M, Buckingham BA, Jarosz-Chobot P, Saboo B, Urakami T, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Insulin Treatment in Children and Adolescents With Diabetes. Pediatr. Diabetes (2018) 19 Suppl 27:115–35. doi: 10.1111/pedi.12718
6. Lee JM, Hirschfeld E, Wedding J. A Patient-Designed Do-It-Yourself Mobile Technology System for Diabetes: Promise and Challenges for a New Era in Medicine. JAMA (2016) 315:1447–8. doi: 10.1001/jama.2016.1903
7. LoopDocs. Available at: https://loopkit.github.io/loopdocs/ (Accessed February 7, 2022).
8. Welcome to the AndroidAPS Documentation — AndroidAPS 3.0 Documentation. Available at: https://androidaps.readthedocs.io/ (Accessed February 7, 2022).
9. Welcome to Openaps’s Documentation! — OpenAPS 0.0.0 Documentation. Available at: https://openaps.readthedocs.io/ (Accessed February 7, 2022).
11. Project N. Welcome to Nightscout (2019). Available at: http://www.nightscout.info/.
12. Braune K, Lal RA, Petruželková L, Scheiner G, Winterdijk P, Schmidt S, et al. Open-Source Automated Insulin Delivery: International Consensus Statement and Practical Guidance for Health-Care Professionals. Lancet Diabetes Endocrinol (2022) 10:58–74. doi: 10.1016/S2213-8587(21)00267-9
13. Knoll C, Peacock S, Wäldchen M, Cooper D, Aulakh SK, Raile K, et al. Real-World Evidence on Clinical Outcomes of People With Type 1 Diabetes Using Open-Source and Commercial Automated Insulin Dosing Systems: A Systematic Review. Diabetes Med. (2021):e14741. doi: 10.1111/dme.14741
14. Braune K, Gajewska KA, Thieffry A, Lewis DM, Froment T, O’Donnell S, et al. Why #WeAreNotWaiting—Motivations and Self-Reported Outcomes Among Users of Open-Source Automated Insulin Delivery Systems: Multinational Survey. J. Med. Internet Res. (2021) 23:e25409. doi: 10.2196/25409
15. Braune K, O’Donnell S, Cleal B, Lewis D, Tappe A, Willaing I, et al. Real-World Use of Do-It-Yourself Artificial Pancreas Systems in Children and Adolescents With Type 1 Diabetes: Online Survey and Analysis of Self-Reported Clinical Outcomes. JMIR Mhealth Uhealth (2019) 7:e14087. doi: 10.2196/14087
16. Street TJ. Review of Self-Reported Data From UK Do-It-Yourself Artificial Pancreas System (DIYAPS) Users to Determine Whether Demographic of Population Affects Use or Outcomes. Diabetes Ther. (2021) 12:1839–48. doi: 10.1007/s13300-021-01071-5
17. Gawrecki A, Zozulinska-Ziolkiewicz D, Michalak MA, Adamska A, Michalak M, Frackowiak U, et al. Safety and Glycemic Outcomes of Do-It-Yourself AndroidAPS Hybrid Closed-Loop System in Adults With Type 1 Diabetes. PloS One (2021) 16:e0248965. doi: 10.1371/journal.pone.0248965
18. Petruzelkova L, Jiranova P, Soupal J, Kozak M, Plachy L, Neuman V, et al. Pre-School and School-Aged Children Benefit From the Switch From a Sensor-Augmented Pump to an AndroidAPS Hybrid Closed Loop: A Retrospective Analysis. Pediatr. Diabetes (2021). doi: 10.1111/pedi.13190
19. Kesavadev J, Srinivasan S, Saboo B, Krishna BM, Krishnan G. The Do-It-Yourself Artificial Pancreas: A Comprehensive Review. Diabetes Ther. (2020) 11:1217–35. doi: 10.1007/s13300-020-00823-z
20. Petruzelkova L, Soupal J, Plasova V, Jiranova P, Neuman V, Plachy L, et al. Excellent Glycemic Control Maintained by Open-Source Hybrid Closed-Loop AndroidAPS During and After Sustained Physical Activity. Diabetes Technol. Ther. (2018) 20:744–50. doi: 10.1089/dia.2018.0214
21. Patel R, Crabtree TSJ, Taylor N, Langeland L, Gazis AT, Mendis B, et al. Safety and Effectiveness of do-it-Yourself Artificial Pancreas System Compared With Continuous Subcutaneous Insulin Infusions in Combination With Free Style Libre in People With Type 1 Diabetes. Diabetes Med. (2022):e14793. doi: 10.1111/dme.14793
22. Lum J, Bailey R, Barnes-Lomen V, Naranjo D, Hood K, Lal RA, et al. A Real-World Prospective Study of the Safety and Effectiveness of the Loop Open Source Automated Insulin Delivery System. Diabetes Technol. Ther. (2020). doi: 10.1089/dia.2020.0535
23. Choi MS, Lee S, Kim J, Kim G, Park SM, Kim JH. Do-It-Yourself Open Artificial Pancreas System in Children and Adolescents With Type 1 Diabetes Mellitus: Real-World Data. Diabetes Metab. J. (2021). doi: 10.4093/dmj.2021.0011
24. Wu Z, Luo S, Zheng X, Bi Y, Xu W, Yan J, et al. Use of a do-it-Yourself Artificial Pancreas System Is Associated With Better Glucose Management and Higher Quality of Life Among Adults With Type 1 Diabetes. Ther. Adv. Endocrinol. Metab. (2020) 11:2042018820950146. doi: 10.1177/2042018820950146
25. Schipp J, Skinner T, Holloway E, Scibilia R, Langstrup H, Speight J, et al. How Adults With Type 1 Diabetes Are Navigating the Challenges of Open-Source Artificial Pancreas Systems: A Qualitative Study. Diabetes Technol. Ther. (2021). doi: 10.1089/dia.2020.0652
26. Suttiratana S, Wong J, Lanning MS, Dunlap AR, Hanes S, Hood K, et al. Qualitative Study of User Experiences With Loop, an Open-Source Automated Insulin Delivery (AID) System. Diabetes Technol. Ther. (2022). doi: 10.1089/dia.2021.0485
27. Braune K, Krug N, Knoll C, Ballhausen H, Thieffry A, Chen Y, et al. Emotional and Physical Health Impact in Children and Adolescents and Their Caregivers Using Open-Source Automated Insulin Delivery: Qualitative Analysis of Lived Experiences. (2021). doi: 10.2139/ssrn.3946995
28. Cleal B, Braune K, O’donnell S, Hauck B, Lewis DM, Skinner TC, et al. 78-LB: Detailing the Experiences of People With Diabetes Using Do-It-Yourself Artificial Pancreas Systems—Qualitative Analysis of Responses to Open-Ended Items in an International Survey. Diabetes (2019) 68. doi: 10.2337/db19-78-LB
29. Asarani NAM, Reynolds AN, Elbalshy M, Burnside M, de Bock M, Lewis DM, et al. Efficacy, Safety, and User Experience of DIY or Open-Source Artificial Pancreas Systems: A Systematic Review. Acta Diabetol. (2020). doi: 10.1007/s00592-020-01623-4
30. Lewis D. History and Perspective on DIY Closed Looping. J. Diabetes Sci. Technol. (2019) 13:790–3. doi: 10.1177/1932296818808307
31. Staszak W, Chromik J, Braune K, Arnrich B. Impact of Custom Features of Do-It-Yourself Artificial Pancreas Systems (DIYAPS) on Glycemic Outcomes of People With Type 1 Diabetes. Conf. Proc. IEEE Eng. Med. Biol. Soc. (2021) 2021:1472–5. doi: 10.1109/EMBC46164.2021.9629487
32. Palmer W, Greeley SAW, Letourneau-Freiberg LR, Naylor RN. Using a Do-It-Yourself Artificial Pancreas: Perspectives From Patients and Diabetes Providers. J. Diabetes Sci. Technol. (2020) 14:860–7. doi: 10.1177/1932296820942258
33. Barnard KD, Ziegler R, Klonoff DC, Braune K, Petersen B, Rendschmidt T, et al. Open Source Closed-Loop Insulin Delivery Systems: A Clash of Cultures or Merging of Diverse Approaches? J. Diabetes Sci. Technol. (2018) 12:1223–6. doi: 10.1177/1932296818792577
34. Burnside M, Crocket H, Mayo M, Pickering J, Tappe A, de Bock M. Do-It-Yourself Automated Insulin Delivery: A Leading Example of the Democratization of Medicine. J. Diabetes Sci. Technol. (2020) 14:878–82. doi: 10.1177/1932296819890623
35. O’Donnell S, Lewis D, Marchante Fernández M, Wäldchen M, Cleal B, Skinner T, et al. Evidence on User-Led Innovation in Diabetes Technology (The OPEN Project): Protocol for a Mixed Methods Study. JMIR Res. Protoc. (2019) 8:e15368. doi: 10.2196/15368
36. Gajewska KA, Biesma R, Bennett K, Sreenan S. Barriers and Facilitators to Accessing Insulin Pump Therapy by Adults With Type 1 Diabetes Mellitus: A Qualitative Study. Acta Diabetol. (2021) 58:93–105. doi: 10.1007/s00592-020-01595-5
37. Ahmed SH, Ewins DL, Bridges J, Timmis A, Payne N, Mooney C, et al. Do-It-Yourself (DIY) Artificial Pancreas Systems for Type 1 Diabetes: Perspectives of Two Adult Users, Parent of a User and Healthcare Professionals. Adv. Ther. (2020) 37:3929–41. doi: 10.1007/s12325-020-01431-w
38. de Bock M. The “Do it Yourself” Type 1 Diabetes Dilemma for Medical Practitioners. Intern. Med. J. (2019) 49:559–61. doi: 10.1111/imj.14286
39. Roberts JTF, Moore V, Quigley M. Prescribing Unapproved Medical Devices? The Case of DIY Artificial Pancreas Systems. Med. Law Int. (2021) 21:42–68. doi: 10.1177/0968533221997510
40. Marshall DC, Holloway M, Korer M, Woodman J, Brackenridge A, Hussain S. Do-It-Yourself Artificial Pancreas Systems in Type 1 Diabetes: Perspectives of Two Adult Users, a Caregiver and Three Physicians. Diabetes Ther. (2019) 10:1553–64. doi: 10.1007/s13300-019-00679-y
41. Shaw D, Crabtree TSJ, Hammond P, McLay A, Wilmot EG. The DIY Artificial Pancreas System: An Ethical Dilemma for Doctors. Diabetes Med. (2020). doi: 10.1111/dme.14270
42. Crabtree TSJ, Choudhary P, Lumb A, Hammond P, McLay A, Campbell F, et al. Association of British Clinical Diabetologists, Diabetes Technology Network UK and Association of Children’s Diabetes Clinicians Survey of UK Healthcare Professional Attitudes Towards Open-Source Automated Insulin Delivery Systems. Diabetes Ther. (2022). doi: 10.1007/s13300-022-01203-5
43. Shepard JA, Breton M, Nimri R, Roberts JTF, Street T, Klonoff D, et al. User and Healthcare Professional Perspectives on Do-It-Yourself Artificial Pancreas Systems: A Need for Guidelines. J. Diabetes Sci. Technol. (2020), 1932296820957728. doi: 10.1177/1932296820957728
44. DeSalvo DJ, Noor N, Xie C, Corathers SD, Majidi S, McDonough RJ, et al. Patient Demographics and Clinical Outcomes Among Type 1 Diabetes Patients Using Continuous Glucose Monitors: Data From T1D Exchange Real-World Observational Study. J. Diabetes Sci. Technol. (2021), 19322968211049783. doi: 10.1177/19322968211049783
45. Addala A, Hanes S, Naranjo D, Maahs DM, Hood KK. Provider Implicit Bias Impacts Pediatric Type 1 Diabetes Technology Recommendations in the United States: Findings From The Gatekeeper Study. J. Diabetes Sci. Technol. (2021) 15:1027–33. doi: 10.1177/19322968211006476
46. Lawton J, Kirkham J, Rankin D, White DA, Elliott J, Jaap A, et al. Who Gains Clinical Benefit From Using Insulin Pump Therapy? A Qualitative Study of the Perceptions and Views of Health Professionals Involved in the Relative Effectiveness of Pumps Over MDI and Structured Education (REPOSE) Trial. Diabetes Med. (2016) 33:243–51. doi: 10.1111/dme.12879
47. Puckett C, Wong JC, Daley TC, Cossen K. How Organizations Shape Medical Technology Allocation: Insulin Pumps and Pediatric Patients With Type 1 Diabetes. Soc. Sci. Med. (2020) 249:112825. doi: 10.1016/j.socscimed.2020.112825
48. Wong J, Suttiratana S, Lal RA, Lum J, Lanning MS, Dunlap A, et al. Discontinued Use of the Loop Insulin Dosing System: A Mixed-Methods Investigation. Diabetes Technol. Ther. (2021). doi: 10.1089/dia.2021.0362
49. Braune K, O’donnell S, Cleal B, Lewis DM, Tappe A, Hauck B, et al. 117-LB: DIWHY: Factors Influencing Motivation, Barriers, and Duration of DIY Artificial Pancreas System Use Among Real-World Users. Diabetes (2019) 68. doi: 10.2337/db19-117-LB
Keywords: automated insulin delivery, closed-loop, digital innovation, diabetes technology, barriers, human factors, health inequalities, access
Citation: Huhndt A, Chen Y, O’Donnell S, Cooper D, Ballhausen H, Gajewska KA, Froment T, Wäldchen M, Lewis DM, Raile K, Skinner TC and Braune K (2022) Barriers to Uptake of Open-Source Automated Insulin Delivery Systems: Analysis of Socioeconomic Factors and Perceived Challenges of Caregivers of Children and Adolescents With Type 1 Diabetes From the OPEN Survey. Front. Clin. Diabetes Healthc. 3:876511. doi: 10.3389/fcdhc.2022.876511
Received: 15 February 2022; Accepted: 04 May 2022;
Published: 25 July 2022.
Edited by:
Julia K Mader, Medical University of Graz, AustriaReviewed by:
Sabine Elisabeth Hofer, Innsbruck Medical University, AustriaAndrea Enzo Scaramuzza, Istituti Ospitalieri di Cremona, Italy
Copyright © 2022 Huhndt, Chen, O’Donnell, Cooper, Ballhausen, Gajewska, Froment, Wäldchen, Lewis, Raile, Skinner and Braune. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Katarina Braune, a2F0YXJpbmEuYnJhdW5lQGNoYXJpdGUuZGU=