 Natalie M. Gil
Natalie M. Gil Samuel W. D. Merriel2†
Samuel W. D. Merriel2† Gerard Cummins
Gerard Cummins Robert S. Kerrison
Robert S. Kerrison
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cancer Control Soc., 14 April 2025
Sec. Behavioural Aspects in Cancer Screening and Diagnosis
Volume 3 - 2025 | https://doi.org/10.3389/fcacs.2025.1568786
This article is part of the Research TopicBehavioral Research into Acceptability of Cancer Early DiagnosisView all 6 articles
Introduction: Lynch syndrome affects an estimated 1 in 279 people in the United Kingdom and presents a high lifetime risk of colorectal cancer. Current strategies to support early diagnosis among Lynch Syndrome patients include surveillance colonoscopy. Capsule endoscopy (CE), which enables visualization of the colon and rectum, is an ingestible imaging device, which could provide a potential means of enabling early detection between colonoscopies. However, current CEs are limited only to visual inspection and are unable to obtain samples from the colon, requiring follow-up colonoscopy for biopsy. To this end, we have been developing a novel ingestible device, which (1) can collect samples from the colon and (2) utilizes artificial intelligence to interpret images obtained (using images collected from colonoscopy and CE conducted with the same cohort). As with any new technology, perceived ease of use and usefulness will be key determinants of implementing ingestible devices within patient care. For this reason, we conducted a focus group study in which people living with Lynch Syndrome were invited to discuss their views on the device.
Methods: Online focus groups were conducted with adults (aged 18+ years) living with Lynch Syndrome. The focus groups aimed to explore their attitudes toward the use of a novel ingestible sampling and imaging device, for use within the surveillance pathway.
Results: Three focus groups, comprising 14 participants, were conducted. The majority of participants were of White British ethnicity (n = 13, 92.9%), female (n = 13, 92.9%) and aged 35 years or older (n = 10, 71.4%). We identified 11 barriers and five facilitators to the use of a novel ingestible device. Further, we identified six advantages, one disadvantage, and four potential indications for use. Attitudes were generally positive toward the device. However, participants were clearly opposed to the idea of this replacing colonoscopy entirely. The novel device was seen as something that could be implemented into the surveillance pathway to augment traditional methods and provide additional reassurance during long intervals between procedures.
Discussion: Results were broadly consistent with previous findings that ingestible devices are perceived to be less invasive, less risky, and represent an alternative for people who fear the discomfort and embarrassment of colonoscopy. Previous studies have identified the need for further research with specific high-risk population groups, such as Lynch Syndrome patients. Our findings add to the literature by identifying several findings unique to these patients. Firstly, the recognition that a major barrier to ingestible device use is their inability to remove polyps, an important aspect of colonoscopy for Lynch Syndrome patients. Second, ingestible devices may also fail to recognize certain polyps common in Lynch Syndrome, such as those that are less pedunculated. Assurance around these issues will be required if implemented in the future.
In the United Kingdom, colorectal cancer (CRC, also referred to as “bowel cancer”) is the fourth most common cancer and the second leading cause of cancer death (1). Chances for survival are improved when CRC is diagnosed early, with over 90% of patients diagnosed at stage I surviving five or more years (2). Unfortunately, due to the non-specific symptom profile of early stage CRC and the frequent lack of “red flag symptoms” associated with early-stage disease (3), <40% of CRCs are diagnosed at stage I or II (4).
People with Lynch Syndrome are at elevated risk of CRC (5). An estimated 1 in 279 people in the U.K. have the syndrome (6), and between 10 and 47% of them will be diagnosed with CRC in their lifetime, depending on age and the underlying mismatched repair gene affected (7). The cancer prevalence in the Lynch syndrome patient population undergoing 2-yearly colonoscopy is observed at 4–5%, with an annual incidence rate of 1–4% (5).
The British Society of Gastroenterology (BSG) advise that people with Lynch syndrome who have a change in the MLH1, MLH2 or EPCAM gene should be invited for colonoscopy screening every 2 years, between the ages of 25 to 75, while people are offered screening every 2 years from age 35 to 75 if they have a variant in the MSH6 or PMS2 gene. Capsule endoscopy (CE), an ingestible electronic imaging system that allows visualization of the colon and rectum, may aid in earlier diagnosis by detecting issues between colonoscopies or by decreasing the need for frequent colonoscopy procedures. However, current CEs cannot obtain samples from the colon and require follow-up colonoscopy for biopsy (8). Further, few clinicians are trained to interpret the images obtained (8). To this end, we have been developing a novel ingestible device, which (1) can collect samples from the colon and (2) utilizes artificial intelligence to interpret images obtained (using images collected from colonoscopy and CE conducted with the same cohort).
As with any new technology, perceived ease of use and usefulness will be key determinants of implementing CE within patient care (9). For this reason, we conducted a focus group study in which patients, living with Lynch Syndrome, were invited to discuss their views on the novel device. As the technology is not yet finalized, the focus groups presented an opportunity for us to not only identify potential barriers to using the test, but also to design it in a way that minimized them.
Online focus groups were conducted with adults, aged 18 years or older, who had Lynch Syndrome. Discussions were facilitated by RK (male) and NG (female), two experienced qualitative researchers holding a PhD and MSc in Psychology and Health Psychology, respectively. The aim of the focus groups was to explore attitudes toward the use of a novel ingestible sampling and imaging device within the surveillance pathway.
A total of three focus groups were conducted on the basis that this is sufficient to discover 90% of all themes (10). All focus groups were conducted online. Online focus groups were selected over face-to-face focus groups to reduce geographical barriers to participation, enabling a more representative sample of participants to be obtained. Focus groups were selected over one-to-one interviews on the basis that focus groups are more conducive when discussing topics people have no direct experience with (11).
The size of the focus groups varied from three to six participants. Previous studies suggest that between four and six participants per focus group is optimal, with a lower and upper limit of two to 14 participants being the minimum and maximum that can be managed effectively (12). Smaller groups are considered more conducive, as they ensure a balance of opinions, while allowing ample time for everyone to contribute meaningfully (13).
Participants were presented with an explanatory video detailing the design and usage of a classic CE, followed by a verbal explanation of the development of the novel sampling and imaging device. A series of open questions were asked using a topic guide (Appendix 1), to generate discussion about different aspects of the device and its potential implementation into the surveillance pathway.
Participants were recruited through social media (i.e., convenience sampling). Specifically, a study advert (Appendix 2) was posted in a special interest group (relating to Lynch Syndrome) on Facebook. The advert contained the email address of the Principal Investigator (RK), a Senior Lecturer in Cancer Care. Individuals interested in participating in the study were instructed to contact the Principal Investigator, who subsequently forwarded the participant information sheet (Appendix 3) and consent form (Appendix 4) to interested parties. Individuals who signed and returned the consent form were then sent a Doodle poll to confirm their availability for one of five focus group dates. They were sent a calendar invite, and a Teams link to a convenient focus group. Participants who attended a focus group (in part or in full) were remunerated with a £50 financial incentive for their contribution.
With participants' consent, focus groups were recorded using the record feature in Teams and lasted between 1 and 2 h. The video recording was then downloaded to an encrypted University of Surrey laptop and converted into MP3 format. The principal investigator then permanently deleted the video recordings, and the audio recordings were transferred to Devon Transcription for anonymisation and transcription (14). Upon receipt of the transcripts, the audio recordings held by Surrey and Devon Transcription were deleted.
Informed consent was obtained from participants in writing prior to the focus groups. At the beginning of the focus groups, participants were reminded of their right to withdraw from the study at any time, without giving a reason. Participants were also informed of their right to withdraw their data from the study up until the publication of the results (at which time, it would no longer be possible to remove their quotes from the published manuscript).
Transcripts were analyzed using small q thematic analysis (codebook analysis) (15). The study adopted an interpretivist approach, well-suited to generating knowledge relevant to health and clinical practice (16). This approach situates the researcher in the context of that which is being studied so that they may offer an interpretive understanding of the meaning that participants attribute to their own experiences. A detailed overview of the analysis process is provided below:
Stage 1: Transcription. Transcription of the interviews was carried out (verbatim) by Devon Transcription.
Stage 2: Familiarization with the interview data. Transcripts were read and re-read, and typed reflections of initial thoughts and observations were captured in the page margins by two researchers (RK and NG).
Stage 3: Coding. Codes were developed to help describe and classify the data in relation to the research question (i.e., segments of text were assigned codes that reflected the issues discussed within those segments; e.g., “Concerns around choking/swallowing”). Two researchers (RK and NG) initially independently developed ideas for codes using the same sample of transcripts (n = 2). Codes were generated inductively (i.e., from the data; audit trail available from: https://osf.io/8v9dg/).
Stage 4: Development of a working analytical framework. Researchers (RK and NG) met to compare their independently generated ideas for codes and, through discussion, consensually agreed on a working analytical framework that could be applied to further transcripts (i.e., an initial set of codes and the meaning of each).
Stage 5: Applying the analytical framework. One researcher (NG) then coded the remaining transcript using the initial codes. The remaining transcript was judged to contain text that could not be satisfactorily coded using the existing codes, new codes were created, or existing codes updated to reflect the data they represented more accurately. Any new codes were discussed and agreed with RK, before NG subsequently revisited previously coded transcripts to apply the new codes if and where relevant.
Stage 6: Interpreting the data. Themes were developed to delineate key messages in the data, relevant to the research aims. Theme development was iterative and involved three researchers (RK, NG and SM), who reached a consensus by discussing the final content and organization of themes.
This study has been reported in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines (Appendix 5). A database of the coded text, along with an audit trail, is available from Open Science Framework; for full transparency, see: https://osf.io/8v9dg/.
Ethical approval. The study was approved by the University of Surrey's Research Innovation and Governance Office on 14th of August 2023 (reference: FHMS 22-23 218 EGA).
In total, three focus groups, comprising 14 participants, were conducted. The majority of participants were of White British ethnicity (n = 13, 92.9%), female (n = 13, 92.9%) and aged 35 years or older (n = 10, 71.4%; see Table 1). Analysis identified 11 barriers and five facilitators to use of a novel ingestible device. Further, six advantages, one disadvantage, and four potential indications for use were identified and discussed below.
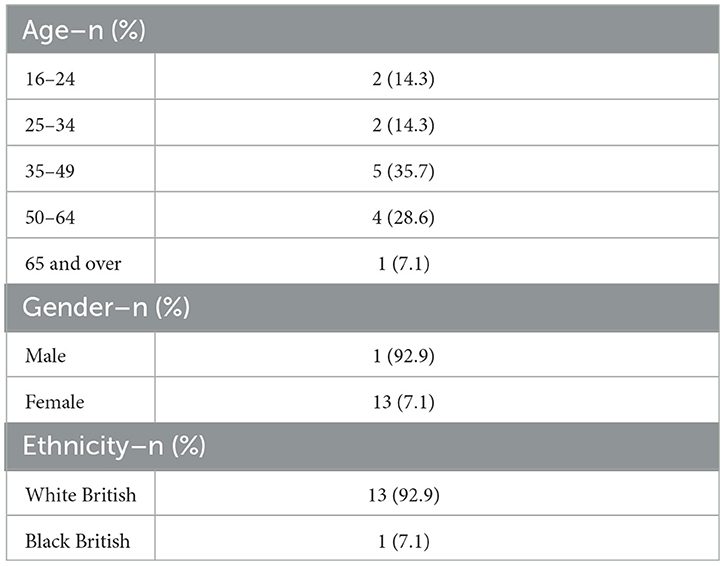
Table 1. Sample characteristics.
An important aspect of this research was to understand the potential barriers to the ingestible device. Eleven barriers were identified during analysis and are discussed below. An overview of the themes, with example quotes, and the number of focus groups they were attributed to, is presented in Table 2.
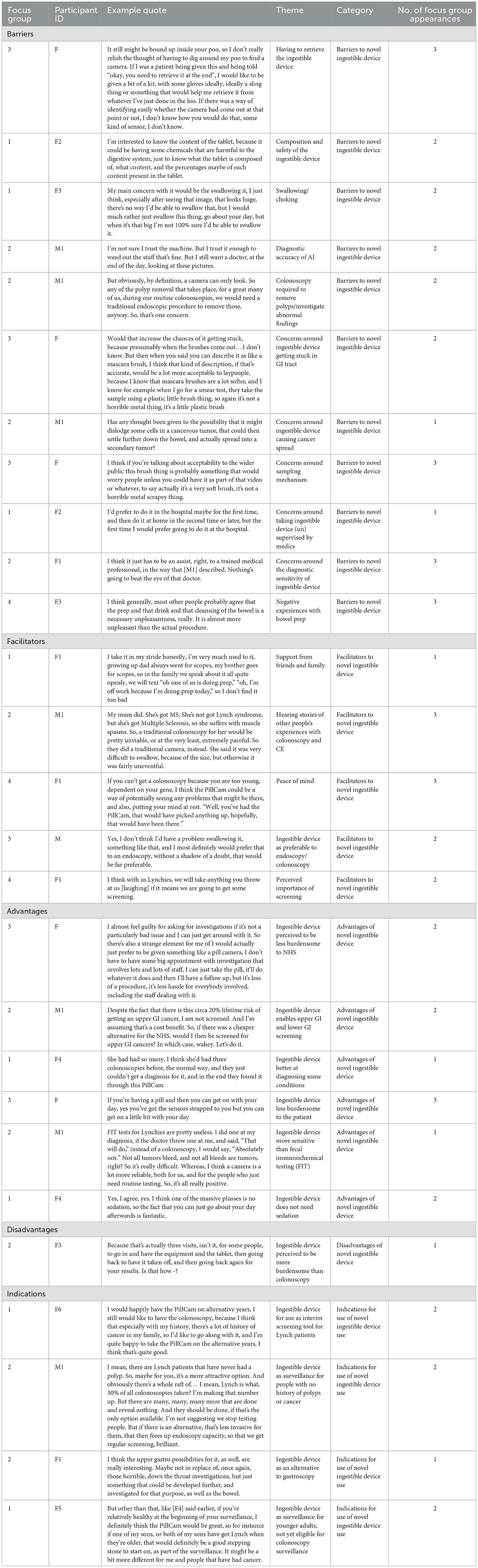
Table 2. Table of themes and example quotations.
The device must be retrieved following excretion in order to collect the physical sample, which was a major theme and discussion point for most participants. The need for retrieval differentiates this device from CE, which wirelessly transmits image data to an external recorder, and the device is flushed away in waste after excretion. Concerns raised were a perceived lack of guidance around how to do this, a lack of clarity around transit time, and difficulty determining whether the capsule had been excreted. Also discussed was the general unpleasantness of “having to look through stool” and the “thought of having to defecate into a pot.” The perception that equipment supplied to capture the device on excretion would be ineffective was also a major theme, as well as the perception that it may not be viable to transport this to places outside of the home, for example, the workplace. Many participants felt that retrieving the device while outside of their own home would be difficult. Potential loss of the device was also discussed at length, with concerns ranging from accidentally flushing the ingestible device resulting in “being charged a lot of money,” the potential loss of images, and “the idea of losing £25,000 of NHS equipment.” Suggestions for improvement on this aspect of the device included the supply of guidance, gloves, a disposable container to aid device collection, and an accurate timescale of when the device would be likely to be excreted.
Several participants raised concerns about the safety and composition of the ingestible device, including worries about ingesting a battery, “chemicals that may be harmful to the digestive system” and subsequent side-effects. The newness of the ingestible device in comparison to colonoscopy, and the idea of ingesting a “foreign object” were also discussed as potential barriers. Some participants described the process of swallowing a camera as “unnatural” and felt that more information would be needed about safety before they would feel comfortable swallowing the device.
Swallowing the ingestible device was raised as an issue among participants who had previously struggled to swallow medications, with several participants raising concerns about size of the capsule or the device “getting stuck” as it moved through the digestive system. Participants requested the measurements, and said their “main concern” would be swallowing the pill as it looked “huge.” The suggestion that swallowing something of that size may induce vomiting was also expressed as a concern.
“I think the feeling of that going down your throat might just automatically make you want to bring it back up, I don't know.”-Focus Group 1, F6
Participants expressed interest in using AI in diagnostics and recognized the benefits of this alongside human input. However, this seemed to be a new area of knowledge, with several comments expressing concern about the diagnostic accuracy of AI and many noting that something “could be missed” during interpretation and that they “still want a doctor, at the end of the day, looking at these pictures.”
Several participants expressed concerns that, as Lynch Syndrome patients, colonoscopy is an important part of treating pathology arising from their condition (i.e., removal of polyps). Therefore, colonoscopy would still be required, should a pathology be reported in the ingestible device results. Many participants had previously had polyps removed during colonoscopy, some during every investigation. Therefore, this “whizzy new camera,” as described by one participant, would not make colonoscopy unnecessary, rather it would delay the process of removing polyps, which would cause anxiety/distress.
“No it won't. Because you're going to find polyps, and you ain't leaving them. I won't sleep until you get them out.” – Focus Group 2, M1
Furthermore, participants suggested that the skill to safely and successfully remove polyps requires a specially trained endoscopist to perform their colonoscopies.
“There's always going to be a barrier for us, I think, when we talk about these cameras. Until they're effectively manned by tiny little shrunk-down doctors, like little submarines, it's going to be really tough.” Focus Group 2, M1
Another questioned whether it would be possible to feel the ingestible device as it moved through the system.
“Will you feel it? That probably sounds really daft, but will you feel it?” Focus Group 2, F2
Several participants discussed the perceived risk of the device becoming stuck in the GI tract, noting that, as Lynch Syndrome patients, with potential “problems in that area,” lower motility could present a problem for the device to successfully move through the digestive system. While a patency capsule is commonly used to ascertain individual risk in this area, retention in people with strictures is higher and participants suggested that providing more information around this, and what the procedure to remove the device would be, should it become stuck, could be beneficial for managing these concerns.
One participant raised concerns around the possibility of the ingestible device causing cancer spread by transporting malignant cells throughout the GI tract.
“Has any thought been given to the possibility that it might dislodge some cells in a cancerous tumor, that could then settle further down the bowel, and actually spread into a secondary tumor?” – Focus Group 3, M1
Several concerns were raised regarding the sampling mechanism of the device, including the design of the brush being “intrusive,” its potential size, the perception that the mechanism may “scrape” or “snap” inside the digestive tract. Participants suggested that people may find the brush “worrying” or may picture it as “scissor like” or a “horrible metal scrapey thing.”
Some participants liked the idea of being able to ingest the device at home, saying it was “less pressure” and “more relaxing.” However, there was a sense that initially it would be preferable to have one administered in a healthcare setting to ensure it was “safe and successful.”
The concept of preferring to have a medical professional conducting screening and examining diagnostic images was prevalent among participants. There were concerns that the ingestible device “might miss something,” as well as worries that a camera “facing one way” would be inferior to a “trained medical professional.” Participants wanted to know the efficacy of the device in relation to “traditional methods,” as well as the success rates as well as expressing concerns that the camera may “flip round” or fail to focus on areas of suspicious tissue. One participant mentioned the fact that both cancers and polyps related to Lynch Syndrome are flatter and less noticeable, often requiring a specific method of colonoscopy involving blue dye to illuminate any potential pathology. Another noted that while colonoscopy is “more invasive,” the risk of waiting 2 years between screening appointments to then have a “tablet miss something” would be unacceptable to Lynch Syndrome patients.
An overarching barrier to both colonoscopy and ingestible devices was negative experience of bowel prep, which participants describe as an “unfortunate reality.” Many felt that it was the “worst part of any bowel screening experience overall” and that they “often wondered why a better alternative” has not yet been developed. Others discussed “developing techniques” to “protect themselves” from the unpleasantness and mentioned the inconvenience of having to stop eating 12 h prior to the procedure as well as both the volume and the “disgusting” taste of the drink. The suggestion that one may have to do this twice if using an ingestible device, followed by further investigations with colonoscopy was also discussed as a major barrier among Lynch Syndrome patients.
“Doing bowel prep twice, in quite close succession, is not only really tough on just you, but also on your exterior. It takes a few weeks to recover.” – Focus Group 2, M1
Understanding potential facilitators to ingestible device usage is also key to successful development and implementation within the surveillance and management of Lynch Syndrome. Five facilitators were identified during the analysis and are discussed below.
During discussions, participants highlighted the importance of family support and shared experiences of screening. One participant shared how she was “very much used to it, as growing up Dad always went for scopes.” The ability to “speak openly about it”, led them to feel that they could “take it in their stride.”
Several participants described how hearing other people's negative experiences of colonoscopy could act as a facilitator to an ingestible device for surveillance, particularly in relation to how difficult the procedure can be for people with co-morbidities, such as Multiple Sclerosis, or those recovering from recent surgeries, such as hysterectomy. This led to the perception that an ingestible device would be “preferable.” One participant shared their mother's previous experience of CE as “uneventful” in comparison to colonoscopy, which was “extremely painful due to muscle spasms.”
The concept of peace of mind was particularly important among Lynch Syndrome patients, and many discussed the feeling of “reassurance” they had from “just being looked at.” They described the worry of “every little ache and pain” and how an ingestible device could be used as an adjunct to colonoscopy to offer additional screening and reassurance, particularly during years where colonoscopy was not offered.
“We're Lynchies, we want everything you can throw at us” – Focus Group 3, F3
Reasons for preferring an ingestible device to endoscopy included the perception that “swallowing something” is less invasive, less painful and an “easier medical investigation” than colonoscopy. Most participants had positive attitudes toward the development of new technologies to improve screening and surveillance. Many described ingestible devices as “by far and away the favourite” option “without a shadow of a doubt” preferable to the “dreaded endoscopy.”
“If somebody said to me, ‘You can swallow something, or you can have a colonoscopy, and the results in terms of accuracy and success rate are the same,' then swallowing something would probably be a preference.” -Focus Group 3, F3
Throughout conversations, the perceived importance of screening was evident. Participants described themselves as “realists” that know that despite the sometimes-difficult aspects of surveillence, “it is better to screen than not.” The perception that increased surveillance could reduce cancer risk and improve early diagnosis was also discussed.
“I'm quite a realist, and my thinking behind it is, I need to take this drink to be able to get the colonoscopy, to be able to detect cancer.” Focus Group 2, F2
Understanding the perceived advantages of ingestible devices will be key to successful implementation and uptake. Six clear advantages were identified in the findings and are discussed below.
During discussions, several participants with Lynch Syndrome raised the issue of surveillence as being costly to the NHS. Despite the fact that NHS tariff for CE is in some cases higher than that for endoscopy, participants perceived ingestible devices as a more cost-effective method of surveillance, and felt that this would require less staffing. Another participant discussed the possibility of using an ingestible device as a screening tool for those high-risk individuals prior to standard screening, or to screen for other cancers for which certain patients may be at risk without adding much additional burden to the NHS.
“I almost feel guilty for asking for investigations. So there's also a strange element for me of I would actually just prefer to be given something like a pill camera, I don't have to have some big appointment, I can just take the pill, it's less hassle for everybody involved, including the staff dealing with it”- Focus Group 3, F2
Some participants discussed the benefit of an ingestible device potentially enabling both upper and lower GI screening, also without additional cost. There was a perception that the device could “get into certain parts of the intestine that you can't get into with traditional methods” as well as reducing anxieties, as it offers a “more comprehensive” examination “from the mouth through to the anus.” There was a sense that this could provide greater reassurance to patients, particularly those at a higher risk of cancer.
One participant noted that, despite three colonoscopies, a family member had struggled to receive a colitis diagnosis until they received a CE. This led to the perception that ingestible devices may be better at diagnosing certain conditions than colonoscopy.
During discussions, it was clear that many participants perceived ingestible devices to be less burdensome to patients, as it would be less invasive, less painful, they would be in their own home and be able to drive themselves to and from appointments. The idea that participants could “get on with their day” with “minimal impact,” while at the same time being in the comfort of their own environment, in case they did feel unwell, was also raised as a positive aspect of this method. One participant noted that feeling unwell during the colonoscopy procedure can pose a real risk to the results, whereas the possibility of this would be significantly reduced by the use of an ingestible device.
“If you're feeling a bit ill then that's doable, the thing is still working inside you, whereas if you're having the procedure with the camera up and you start to feel really poorly and you think ‘I really need to go and go to the loo'…I would actually prefer to have a pill, and then if I need to go and just lie down for a while, then I can just go and do that without it affecting the result.” – Focus Group 3, F1
For one participant with Lynch Syndrome, there was a perception that FIT was an unsuitable surveillance method as “not all tumors bleed.” The idea that “a camera is a lot more reliable” was a key factor, which indicates the use of ingestible devices may be regarded as advantageous for bowel surveillance among Lynch Syndrome patients.
Finally, participants described not needing sedation as a “real plus,” since they could “go about their day” afterwards, while procedures requiring sedation mean that effectively a “day is lost” with the added inconvenience that sedation can also require more time off from work.
Despite recognition of the advantages, some participants perceived the procedure of an ingestible device to be more burdensome, as it required several visits to receive the equipment and ingest the device, followed by returning the equipment and, later, receiving the results. It would be important to clarify how this process could be streamlined in order to address the negative perceptions surrounding this aspect of the procedure.
There were four potential indications for use identified during analysis. These are outlined and discussed below.
Many participants liked the idea that an ingestible device could complement colonoscopy and provide additional assurance for Lynch Syndrome patients on alternate years. This was particularly welcome for participants with a family history of cancer, who felt it could go hand in hand with colonoscopy. Despite expressing confidence in an ingestible device as an interim screening tool, there was still some uncertainty in relying on this entirely as perhaps “they can't take extra pictures of suspicious sites” or “they won't be aware if there is anything suspicious.”
“I can see it being an interim option, or something. Like myself, I've never had a polyp, knock on wood. So, maybe in the intervening time of when my surveillance cycle was, I would be open to it. But, I think I would still want the full kit and caboodle every other time, or something like that..” Focus Group 2, F1
Many participants felt that an ingestible device would be a welcome first-line check to begin surveillance of otherwise healthy individuals with Lynch Syndrome as a stepping stone, particularly for individuals who have not had polyps removed or a previous cancer diagnosis. The less invasive option of an ingestible device was an attractive prospect under these circumstances. There was a heightened awareness among participants of the pressures on endoscopy services, and recognition that while Lynch Syndrome patients definitely needed regular surveillance, the majority of investigations reveal no pathology. The introduction of an ingestible device to the surveillance pathway for people with no history of pathology could reduce risk and “free up endoscopy capacity.”
Several participants discussed whether an ingestible device could potentially be used as a rule-out tool for gastroscopy. Despite the fact this is not currently feasible due to the size of the stomach, participants expressed that upper GI investigations were particularly unpleasant, and something they had struggled with previously, and that an ingestible device would be preferable.
“I don't know what's worse, having one of those and knowing it wasn't worth it, because there's nothing there? Or it was worth it, because there's something horrible found. No, well obviously that's worse. But yes, knowing if there's a good reason to go through a gastroscopy again, before I have to go through it, I think is valuable.” Focus Group 2, M1
Finally, the possibility of an ingestible device as an early introduction to surveillance for Lynch Syndrome patients was discussed, with one participant noting that while current guidelines do not recommend screening for patients until over the age of 25, earlier surveillance could be advantageous.
“..with Lynch the screening doesn't start until they're 25, I think there's an argument for starting younger than that, this sort of thing would be fantastic and a good introduction to the whole screening process.”
To our knowledge, this study is the first to explore patient acceptability of a novel ingestible sampling and imaging device for the early detection of bowel cancer, among people with Lynch Syndrome. We identified 11 barriers and five facilitators to the ingestible device. Further, we identified six advantages, as well as one disadvantage and four potential indications for use.
Overall, attitudes were generally positive toward the ingestible device. However, participants were clearly opposed to the idea of this replacing colonoscopy entirely. Rather, it was seen as something that could be implemented into the surveillance pathway to augment traditional methods (colonoscopy) and provide additional reassurance during long intervals between procedures. There was a sense that this could be a useful tool among populations for whom colonoscopy would not be appropriate, for example, those who are outside of the recommended age of surveillance, people with pre-existing conditions (who may find colonoscopy more painful), or where there may be a higher risk associated with colonoscopy.
Major barriers to use of an ingestible device for bowel surveillance were negative perceptions around safe and manageable usage, including composition and safety, swallowing the capsule, the likelihood of the device becoming stuck during transit, concerns around the safety and discomfort of the sampling mechanism and ease of retrieval following excretion. Concerns were also raised regarding the efficacy of the device itself, in terms of its ability to recognize pathology, capture accurate images and the diagnostic sensitivity of AI.
Facilitators included support from family and friends, namely hearing other people's experiences of CE, the peace of mind that additional surveillance would offer to high-risk patients, and the perceived importance of screening. Advantages of an ingestible device included the perception that it is less burdensome to the NHS, that it may be better at diagnosing certain conditions, has potential to screen upper and lower GI tract, and that it does not require sedation.
Indications for use include the option of an ingestible device as an alternative or rule-out investigation for gastroscopy, as an interim screening tool for additional reassurance between scopes, as a surveillance tool for patients with no history of polyps or cancer and as a potential introduction to surveillance for patients with Lynch Syndrome, who are below the current recommended age for surveillance.
The results of this study are broadly consistent with previous findings that CE is perceived to be less invasive (17), less risky (18), and represents an alternative for people who fear the discomfort and embarrassment of colonoscopy (19). Our findings are also in line with previous literature that identified the potential for ingestible devices to address limitations of other diagnostic modalities and visualize additional areas of the GI tract (20), as well as patient preference to complete procedures at home rather than hospital (21), and without requiring sedation (22). Also in line with previous literature was the perception that ingestible devices reduce the workload of overburdened screening practitioners (23). Additionally, the results of this study support previous findings highlighting concerns about the size and safety of swallowing ingestible devices (24), accuracy and sensitivity compared to colonoscopy (25), and the risk of technical failure (20).
Previous studies have identified the need for further research with specific high-risk population groups, such as Lynch Syndrome patients (17). Our findings add to the literature by identifying several findings unique to these patients. Firstly, the recognition that a major barrier to ingestible devices is the inability to remove polyps (an important aspect of colonoscopy for Lynch Syndrome patients). Such devices may also fail to recognize certain polyps common in Lynch Syndrome (e.g., those which are less pedunculated). However, they were thought to be better at identifying certain conditions (e.g. colitis) and were also considered a more suitable surveillance method than FIT, for example, as not all tumors bleed.
This study has a number of strengths. First, following each stage of data analysis, two reviewers (RK and NG), plus a third reviewer (SM), discussed the thematic findings and resolved disagreements through discussion to help maintain theoretical validity (reliability of data interpretation) (26). Second, pragmatic validity (efficacy and transferability of findings) was improved by inclusion of participant characteristic tables, providing context around the individuals, allowing readers to judge the usefulness of the findings (27). Finally, an audit trail for the generation of codes and themes is provided, and the results reported in-line with COREQ guidelines, enhancing the transparency and reproducibility of the study.
This study also has a number of important limitations. First, focus groups were conducted online, which may have precluded some populations from being able to take part, reducing the generalisability of the results. Second, participants were predominantly of white ethnicity. As such, the findings may not represent the perceptions of other populations, including ethnic minority groups. Thirdly, only one male participated in this study. Previous research has found that mixed-sex health research studies are typically only comprised of 20% male participants (28). This may be due to the subject matter, as reported in previous studies, which describe significant and pervasive difficulty in engaging male research participants in sensitive health-related discussions (29). However, this study falls short of this participation rate and it would be important to consider how to successfully engage male particpants in conversations of this nature. Finally, the study is subject to hypothetical bias, as none of the participants were offered the ingestible device in an ecological setting.
This study has several implications for policy and future research.
Firstly, there is a pressing need for the introduction of alternative methods in the surveillance pathway for high-risk patients, particularly as a rule-out investigation for suspected colorectal cancer. The burden of gastrointestinal diseases has led to increased demand for colonoscopy, which is a scarce and expensive resource, requiring specialist screening practitioners, and one that does carry some risk of complications. While CE has already been implemented within the NHS, this study helps to identify potential barriers to ingestible device use, so that we may better understand how to address patient concerns as we effectively roll out this novel sampling and imaging technology on a larger scale.
In addition, there is a need to validate these findings in an ecological sample, where people have experience of using the sampling and imaging ingestible device, as well as to conduct quantitative research to understand the possible interactions between barriers and facilitators in real-world scenarios, where people have been invited for ingestible device screening and accepted or declined the invitation. Finally, as with the implementation of any new diagnostics, it is important to consider the perspectives of the healthcare practitioners who will recommend them. Future research should focus on the perspectives of healthcare providers throughout the screening pathway, from primary care to specialist screening practitioners.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found at: https://osf.io/8v9dg/.
The studies involving humans were approved by University of Surrey Assurance Team. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
NG: Data curation, Formal analysis, Methodology, Project administration, Writing – original draft, Writing – review & editing. SM: Conceptualization, Formal analysis, Funding acquisition, Methodology, Writing – review & editing. HS: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. GC: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. EF: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. RK: Conceptualization, Data curation, Formal analysis, Funding acquisition, Methodology, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This study was funded by Cancer Research UK (Reference: EDDISA-Jan22/100002). SM was supported by the National Institute for Health and Care Research (NIHR) Manchester Biomedical Research Center (BRC) (NIHR203308).
The authors would like to thank the participants for their involvement in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcacs.2025.1568786/full#supplementary-material
1. Cancer Research UK. Cancer Incidence for Common Cancers. (2020). Available online at: https://www.cancerresearchuk.org/health-professional/cancer-statistics/incidence/common-cancers-compared (accessed May 24, 2024).
2. Cancer Research UK. Survival for Bowel Cancer. (2021). Available online at: https://www.cancerresearchuk.org/about-cancer/bowel-cancer/survival (accessed May 24, 2024).
3. Cardoso R, Guo F, Heisser T, Hackl M, Ihle P, De Schutter H, et al. Colorectal cancer incidence, mortality, and stage distribution in European countries in the colorectal cancer screening era: an international population-based study. Lancet Oncol. (2021) 22:1002–13. doi: 10.1016/S1470-2045(21)00199-6
4. Walter FM, Emery JD, Mendonca S, Hall N, Morris HC, Mills K, et al. Symptoms and patient factors associated with longer time to diagnosis for colorectal cancer: results from a prospective cohort study. Br J Cancer. (2016) 115:533–41. doi: 10.1038/bjc.2016.221
5. Monahan KJ, Lincoln A, East JE, Benton S, Burn J, DeSouza B, et al. Management strategies for the colonoscopic surveillance of people with lynch syndrome during the COVID-19 pandemic. Gut. (2021) 70:624–6. doi: 10.1136/gutjnl-2020-321993
6. Huntley C, Loong L, Mallinson C, Bethell R, Rahman T, Alhaddad N, et al. The comprehensive English national lynch syndrome registry: development and description of a new genomics data resource. E Clinical Medicine. (2024) 69:102465. doi: 10.1016/j.eclinm.2024.102465
7. Møller P, Seppälä T, Bernstein I, Holinski-Feder E, Sala P, Evans DG, et al. Cancer incidence and survival in lynch syndrome patients receiving colonoscopic and gynaecological surveillance: first report from the prospective lynch syndrome database. Gut. (2017) 66:464–72. doi: 10.1136/gutjnl-2015-309675
8. Hosoe N, Limpias Kamiya KJ, Hayashi Y, Sujino T, Ogata H, Kanai T, et al. Current status of colon capsule endoscopy. Dig Endosc. (2021) 33:529–37. doi: 10.1111/den.13769
9. Marangunić N, Granić A. Technology acceptance model: a literature review from 1986 to 2013. Univ Access Inf Soc. (2015) 14:81–95. doi: 10.1007/s10209-014-0348-1
10. Doria N, Condran B, Boulos L, Curtis Maillet DG, Dowling L, Levy A. Sharpening the focus: differentiating between focus groups for patient engagement vs. qualitative research. Res Involv Engagem. (2018) 4:19. doi: 10.1186/s40900-018-0102-6
11. Guest G, Namey E, McKenna K. How many focus groups are enough? Building an evidence base for nonprobability sample sizes. Field Methods. (2017) 29:3–22. doi: 10.1177/1525822X16639015
12. Bloor M, Frankland J, Thomas M, Robson K. Focus Groups in Social Research. London: SAGE Publications Ltd (2001). doi: 10.4135/9781849209175
13. Sim J, Waterfield J. Focus group methodology: some ethical challenges. Qual Quant. (2019) 53:3003–22. doi: 10.1007/s11135-019-00914-5
14. Devon Transcription. About us (2024). Available online at: https://www.devontranscription.co.uk/about-us.html (accessed May 24, 2024).
15. Braun V, Clarke V. Conceptual and design thinking for thematic analysis. Qual Psychol. (2022) 9:3–26. doi: 10.1037/qup0000196
16. Gil N, Fisher A, Beeken RJ, Pini S, Miller N, Buck C, et al. The role of partner support for health behaviours in people living with and beyond cancer: a qualitative study. Psychooncology. (2022) 31:1997–2006. doi: 10.1002/pon.6032
17. Deding U, Cortegoso Valdivia P, Koulaouzidis A, Baatrup G, Toth E, Spada C, et al. Patient-reported outcomes and preferences for colon capsule endoscopy and colonoscopy: a systematic review with meta-analysis. Diagnostics. (2021) 11:1730. doi: 10.3390/diagnostics11091730
18. Ali O, Gupta S, Brain K, Lifford KJ, Paranjothy S, Dolwani S. Acceptability of alternative technologies compared with faecal immunochemical test and/or colonoscopy in colorectal cancer screening: a systematic review. J Med Screen. (2023) 30:14–27. doi: 10.1177/09691413221109999
19. Sijben J, Peters Y, van der Velden K, Rainey L, Siersema PD, Broeders MJM. Public acceptance and uptake of oesophageal adenocarcinoma screening strategies: a mixed-methods systematic review. EClinicalMedicine. (2022) 46:101367. doi: 10.1016/j.eclinm.2022.101367
20. Carretero C, Carbonnel F, Ferrante M, Knudsen T, Van Lent N, Lobo AJ, et al. Monitoring established crohn's disease with pan-intestinal video capsule endoscopy in Europe: clinician consultation using the nominal group technique. Curr Med Res Opin. (2021) 37:1547–54. doi: 10.1080/03007995.2021.1940910
21. Thygesen MK, Baatrup G, Petersen C, Qvist N, Kroijer R, Kobaek-Larsen M. Screening individuals' experiences of colonoscopy and colon capsule endoscopy; a mixed methods study. Acta Oncol. (2019) 58:S71–6. doi: 10.1080/0284186X.2019.1581372
22. Ferrari A, Neefs I, Hoeck S, Peeters M, Van Hal G. Towards novel non-invasive colorectal cancer screening methods: a comprehensive review. Cancers. (2021) 13:1820. doi: 10.3390/cancers13081820
23. Okabayashi S, Kobayashi T, Nakano M, Toyonaga T, Ozaki R, Tablante MC, et al. A simple 1-day colon capsule endoscopy procedure demonstrated to be a highly acceptable monitoring tool for ulcerative colitis. Inflamm Bowel Dis. (2018) 24:2404–12. doi: 10.1093/ibd/izy125
24. Bond S, Kyfonidis C, Jamieson M, Maguire R, McCann L, Watson A, et al. Evaluation of an innovative colon capsule endoscopy service in Scotland from the perspective of patients: mixed methods study. J Med Internet Res. (2023) 25:e45181. doi: 10.2196/45181
25. Tran TN, Ferrari A, Hoeck S, Peeters M, Van Hal G. Colorectal cancer screening: have we addressed concerns and needs of the target population? Gastrointest Disord. (2021) 3:173–203. doi: 10.3390/gidisord3040018
26. Roberts P, Priest H. Reliability and validity in research. Nurs Stand. (2006) 20:41–6. doi: 10.7748/ns2006.02.20.23.41.c4069
27. Worren NA, Moore K, Elliott R. When theories become tools: toward a framework for pragmatic validity. Hum Relat. (2002) 55:1227–50. doi: 10.1177/a028082
28. Borg DJ, Haritopoulou-Sinanidou M, Gabrovska P, Tseng HW, Honeyman D, Schweitzer D, et al. Barriers and facilitators for recruiting and retaining male participants into longitudinal health research: a systematic review. BMC Med Res Methodol. (2024) 24:46. doi: 10.1186/s12874-024-02163-z
Keywords: cancer, Lynch Syndrome, surveillance, early detection, screening
Citation: Gil NM, Merriel SWD, Sailem H, Cummins G, Finn E and Kerrison RS (2025) Patient acceptability of an ingestible sampling and imaging capsule (Samplecam) for bowel surveillance and early detection of colorectal cancer among Lynch Syndrome patients: a focus group study. Front. Cancer Control Soc. 3:1568786. doi: 10.3389/fcacs.2025.1568786
Received: 30 January 2025; Accepted: 10 March 2025;
Published: 14 April 2025.
Edited by:
Edvīns Miklaševičs, Riga Stradiņš University, LatviaReviewed by:
Giulia Martina Cavestro, Vita-Salute San Raffaele University, ItalyCopyright © 2025 Gil, Merriel, Sailem, Cummins, Finn and Kerrison. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Natalie M. Gil, bi5naWxAc3VycmV5LmFjLnVr
†ORCID: Samuel W. D. Merriel orcid.org/0000-0003-2919-9087
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.