 Vitória Sanches Lemes Soares
Vitória Sanches Lemes Soares Sheila Walbe Ornstein
Sheila Walbe Ornstein Ana Judite Galbiatti Limongi França
Ana Judite Galbiatti Limongi França- Quality and Performance in the Built Environment Research Group, Architecture Technology Department, Faculty of Architecture and Urbanism, University of São Paulo, São Paulo, Brazil
To optimize the emergency room environment, this article puts forward comprehensive diagnoses and recommendations to minimize healthcare-associated infections. Emergency rooms are usually the initial point of entry into the healthcare system for individuals with different illnesses and needs. These environments frequently operate at maximum capacity, which result in challenges related to spatial organization. Therefore, a Post-Occupancy Evaluation was conducted within such an environment during the COVID-19 pandemic, utilizing a combination of qualitative and quantitative data collection methods. The following methodologies were employed to achieve the research objectives and scope: semi-structured interviews with staff members and a specialized architect; walkthrough accompanied by key individuals; behavior observation for flow mapping and quantification; visual records and physical surveys; measurements of environmental conditions; and computational fluid dynamics simulations. The obtained results show the significance of maintaining and monitoring environmental conditions in specific environments; ensuring the appropriate allocation of hospital sectors; leveraging technology to reduce the exchange of paper among professionals; employing video calls to receive patients with flu symptoms; and implementing segregated patient-staff flow. Conclusively, these diagnoses and recommendations hold the potential to not only enhance the built environment of the case study but also to benefit other facilities with similar typologies.
1 Introduction
The research objective was to identify the relevant aspects of the built environment, and those related to Healthcare-Associated Infections (HAI), to develop consistent diagnoses and recommendations for Emergency Room (ER) environments, associated with activity flows and Indoor Air Quality (IAQ), using a case study, taking into consideration the situation and the experience gained in the COVID-19 (Coronavirus Disease 2019) pandemic.
Conducting assessments of in-use built environments facilitates the formulation of diagnoses and recommendations, not only for the subject under evaluation (the case study), but also for spaces sharing similar typology. This serves the purpose of providing valuable feedback for the design process (Preiser et al., 2018). In terms of healthcare environments, the evaluation is even more critical, as these buildings accommodate individuals with varying health conditions. Additionally, these environments rarely interrupt their activities for renovations or interventions, situations that require advanced programming, usually organized by sector and executed with quality to avoid new interventions in the near future. Moreover, decision makers and designers must consider the expenses associated with the equipment and systems in such locations, along with the recommendations outlined in the standards. These factors emphasize the need for heightened caution in both projects and interventions.
In situations such as the COVID-19 pandemic, for example, the existing facilities had to adapt or construct buildings to receive patients with this disease. In Brazil, the Brazilian National Health Regulatory Agency (ANVISA—Agência Nacional de Vigilância Sanitária) recommended that patients with symptoms related to COVID-19 that could indicate severity should be taken to an ER (ANVISA, 2021). This environment comprises facilities designed to provide assistance to patients, whether or not their conditions pose a risk to life, whose injuries necessitate immediate care, with or without hospitalization (Brasil, 2001). However, these units were frequently ill-equipped to receive such patients, especially given the high transmissibility of the disease.
Among the recommendations to prevent the occurrence of HAI, greater care is taken in screening, testing, separating, and isolating those infected. In addition, effective actions include handwashing, wearing a mask, avoiding sharing objects, adhering to social distancing measures, maintaining well-ventilated and clean environments, organizing activity flows, and covering one’s nose and mouth with an elbow or a scarf when coughing (WHO - World Health Organization, 2020; Waroonkun and Prugsiganont, 2022; Salonen et al., 2023). The following are some of the aspects of the built environment that can interfere with the occurrence of contamination by respiratory diseases: Heating, Ventilating and Air Conditioning (HVAC) systems; disinfection and hygiene; layout and spatial organization; air curtain and air purification; natural ventilation; door opening and surface material (Soares et al., 2022). Also, greater use of natural lighting in hospitals is recommended (Emmanuel, Osondu, Kalu, 2020). When possibilities for increasing ventilation and filtering room air are limited, the alternative is using Ultraviolet Germicidal Irradiation systems, according to the Centers for Disease Control and Prevention (CDC) (2023). These systems use ultraviolet C radiation to kill viruses, bacteria, and fungi and this wavelength poses fewer risks to humans (Emmanuel, Osondu, Kalu, 2020; Gola et al., 2021; CDC, 2023). For the research in question, the focus was on the importance of organizing activity flows and controlling IAQ in ERs.
The literature suggests that organizing flows of users, materials, corpses, and equipment contributes to the legibility, humanization, and safety of the environment, as well as to the discipline of employees while performing their tasks (Thomazoni et al., 2016; Dariva and Marconsini, 2020). In addition, the organization of flows allows for the alleviation of undersized circulations and passages (Fiorentini et al., 1995) and to avoid crowding, medical, medication, and protocol errors, aspects that help to control HAI. It is noteworthy that, based on an understanding of activity flows, it is possible to establish proximity relationships between complementary sectors, to define the positioning of barriers, washbasins, and gel alcohol dispensers, and to define the appropriate location of the triage sector, the areas of cohorts (separation of patients by similar symptoms or illnesses), and isolation rooms for patients with aerosol, contact, or droplet transmitted infections (Capolongo et al., 2020; ANVISA, 2021; Lesan et al., 2021).
Technologies, such as telemedicine, help reduce the number of trips healthcare service providers must take to the establishment, since when remote monitoring can be used, it avoids excessive displacements (Pilosof et al., 2021a; Pilosof et al., 2021b). The aspect of employee visibility based on the positioning of nursing and medical prescription stations also contributes to a reduction in the flow of healthcare service providers (Pilosof et al., 2021a; Pilosof et al., 2021b). In terms of employee displacements, it is recommended to segregate them into separate groups, ensuring that employees assigned to a specific sector do not enter other sectors, thereby mitigating the risk of cross-contamination.
Furthermore, there are studies illustrating a direct correlation between the rates of HAI and IAQ. Acceptable IAQ is defined as the “air in which there are no known contaminants at harmful concentrations, as determined by cognizant authorities, and with which a substantial majority (80% or more) of people exposed do not express dissatisfaction” (ASHRAE - American Society of Heating, Refrigerating and Air-Conditioning Engineers, 2022). In the management of IAQ, mechanical systems must regulate physical, chemical, and biological parameters. This includes implementing systems such as air filtration, differential pressure control, temperature and relative humidity control, air conditioning, air renewal, and exhaust systems, among other systems. Specific standards govern air treatment in healthcare facilities, defining the designated environments within the unit and the corresponding parameters that they must adhere to (ASHRAE, 2021; ABNT - Associação Brasileira de Normas Técnicas, 2022).
2 Materials and methods
This study used a combination of quantitative and qualitative methods to assess the performance of the environment in full operation. This involved diversifying data sources, utilizing various data collection techniques, and validating findings through methods such as interviews. These measures enhanced the credibility of the research (Groat and Wang, 2013). Moreover, the qualitative research allow for an efficient understanding of the context and processes that complement the quantitative research data (Federal Facilities Council, 2001). A case study was used in order to understand, interpret, and describe the complexity of a real case, considering its real contexts and incorporating highly complex phenomena (Yin, 2014).
Thereby, a comprehensive Post-Occupancy Evaluation (POE) was conducted within the ER of the University Hospital at the University of São Paulo (USP). This POE employs a multimethod approach that considers perspectives from both experts and users to thoroughly assess performance during the use of a given environment (Ono et al., 2018). Considering the design process as something cyclical and iterative (Bechtel and Churchman, 2002; Zeisel, 2006), the diagnoses obtained allow for an elaboration of recommendations and information that can be incorporated into new interventions and projects. As an initial stage of the POE, authorizations were obtained from the person legally responsible for the case study and from the Research Ethics Committee, as it involved the participation of human beings. The research was approved by the Research Ethics Committee of the University Hospital at USP, on 18 June 2021, with the following Certificate of Presentation for Ethical Appreciation number: 47467921.0.0000.0076. Subsequently, projects, technical documents, and as-builts related to the case study were requested and a search was made for standards, legal definitions, and best practices related to the researched subject (Figure 1).
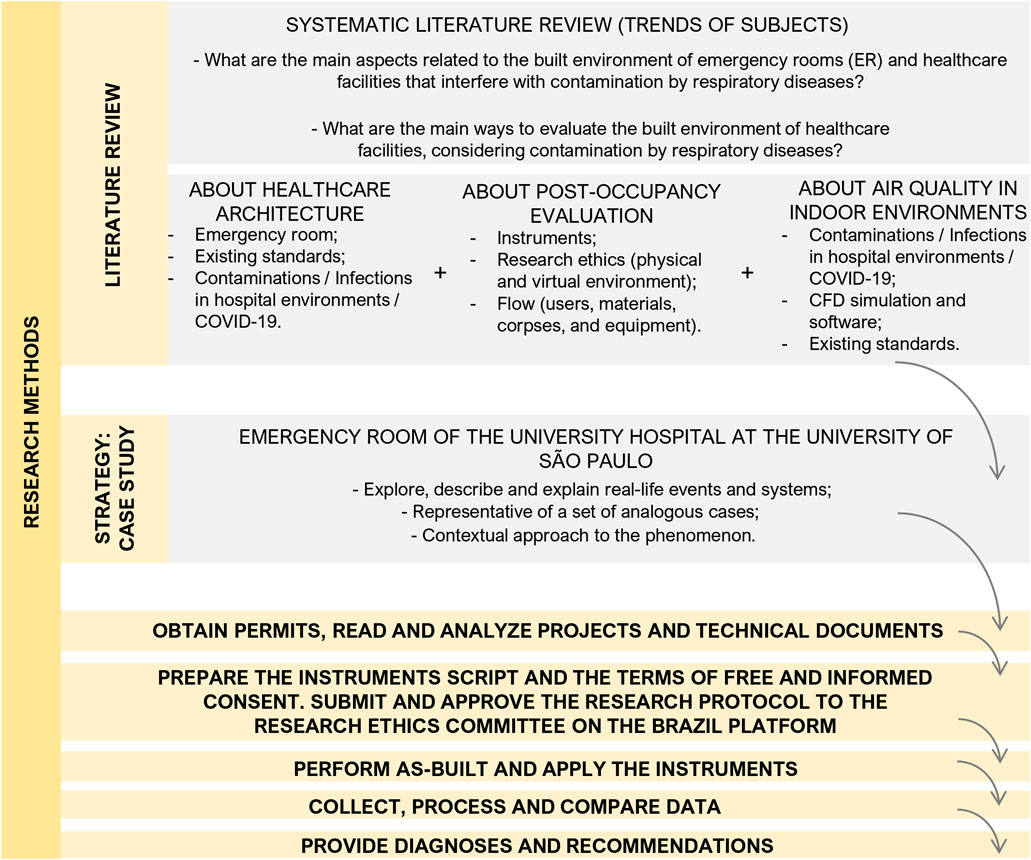
FIGURE 1. Flowchart of research methods SOURCE: elaborated by the authors.
Based on the goals, the object and the time of research, the instruments made available by the POE were selected (Figure 2). The following were the instruments for measuring the users’ environmental perception: walkthroughs accompanied by key individuals; semi-structured interviews with employees; and behavior observations (related to existing flows). Instruments employed for the specialist’s evaluation included: physical surveys and visual records; semi-structured interviews with an expert architect; measurements of environmental conditions; and computational simulation focused on indoor air flow dynamics. This article presents and discusses the results of the walkthroughs accompanied by key individuals; semi-structured interviews with employees; behavior observations (related to existing flows); physical surveys and visual records; and measurements of environmental conditions (related to CO₂ concentration).
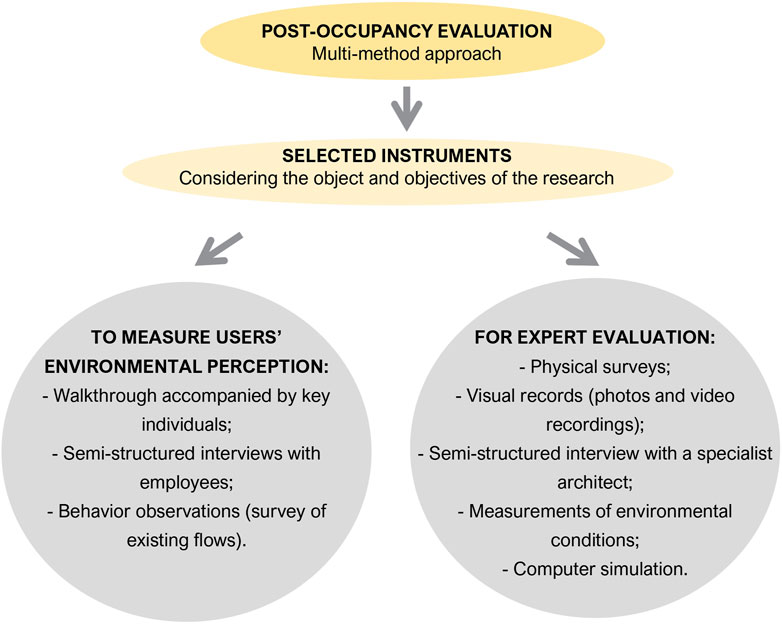
FIGURE 2. Selected instruments, considering the research object and objectives SOURCE: elaborated by the authors.
The instruments were applied between October 2021 and July 2022. After applying and analyzing each of the results obtained, the data were crossed in chart and map format. These are known as summary chart of diagnoses and recommendations and summary map of diagnoses and recommendations, which display the diagnosed situation (with photo), the sector in which it is located, the instruments applied that allowed its identification, the recommendation, the degree of intervention priority and the infection risk. Organizing the information in these formats allows the decision makers to better visualize and understand the information (Ono et al., 2018).
In this study, the research limitations refer to the fact that only one case study was examined and used. Furthermore, the study started in March 2021 and on-site surveys were conducted only in November 2021, according to the recommendation of the head of the hospital’s research board, during the period deemed “between waves” and after the researcher had received complete vaccination. Another issue was that the initial analysis of the project indicated the presence of a central air conditioning system in the ER. However, over time, this system, which was old and malfunctioning, was deactivated and replaced by high wall split air conditioning units. In terms of data collection, a limitation was that staff and technicians advised against leaving instruments in rooms for extended periods of time due to the high foot traffic, posing the devices’ risk of damage. Consequently, it was recommended that the researcher be aware of the instruments during the CO₂ measurements.
The case study and its main aspects related to the context of the COVID-19 pandemic are presented below. In sequence, there is a summary of the normative references and best practices related to ER, activity flows, and IAQ. Afterwards, there is the description of the preparation of the instruments covered in this article. The results section explains the application mode and the main results, which is followed by the data cross-referencing and the diagnoses and recommendations.
2.1 The ER of the University Hospital at USP
The University Hospital, in addition to promoting teaching and research, must provide assistance to the USP community and to the Butantã health district. It was opened in 1981 and is located at the University City Armando Salles de Oliveira, USP campus. The architectural project was carried out by the architect Osmar Antônio Mammini, through the USP Construction Fund. The construction used reinforced concrete (Universidade de São Paulo, 2005) with solid brick masonry for sealing, and lightweight panels in specific areas. The building has 36,000 m2 of total constructed area, spread over six floors. The three highest floors (fourth, fifth, and sixth) housed the inpatient structure and the third floor accommodated administrative activities.
Figure 3 shows the ER on the hospital’s second floor, which was partially below ground level. This floor housed the surgical center, ambulatory services, and the imaging examination area. The first floor, also partially below ground level, accommodated service departments such as nutrition, linen room, and the sterilized material center, among others. Over time, the division of the first and the second floors was noticed, with the inclusion of services and day-to-day demands.
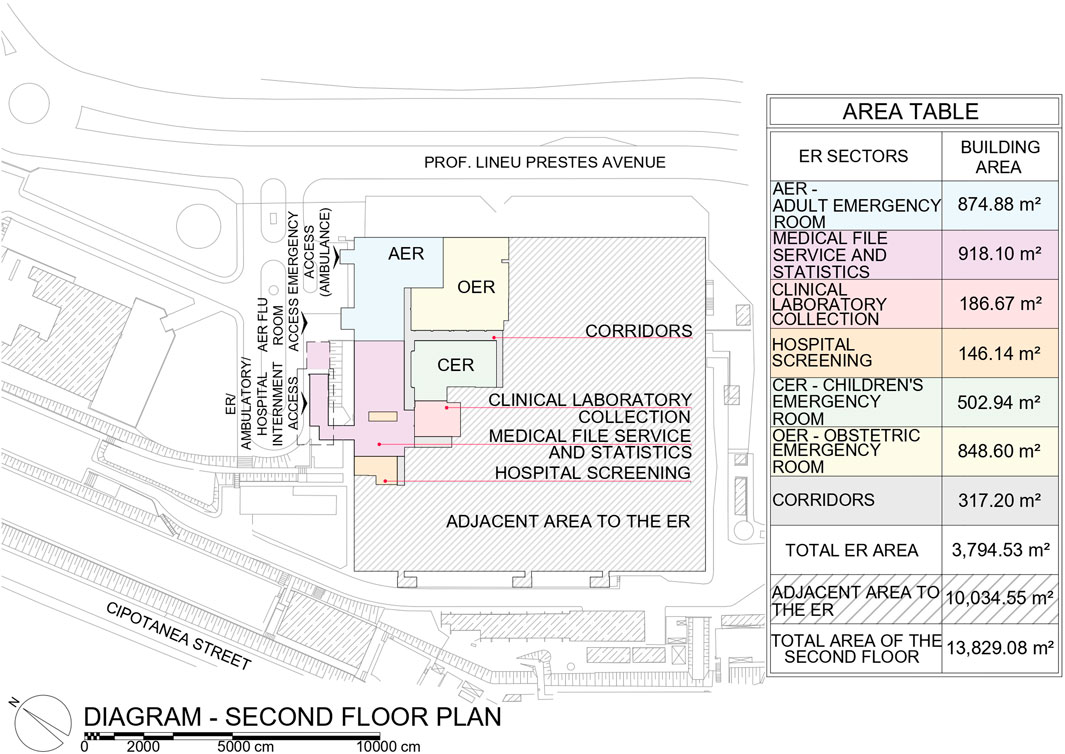
FIGURE 3. Diagram of the 2nd floor plan of the hospital with the ER area delimited SOURCE: USP Physical Space Superintendence Collection. Based on Soares (2023) and adapted by the authors.
The ER comprised: Adult Emergency Room (AER); Children’s Emergency Room (CER); Obstetric Emergency Room (OER); Clinical Laboratory Collection Sector; Hospital Screening Sector; and Medical File Service and Statistics Sector, covering an area of 3,794.53 m2 (Figure 3). In 2017, the ER started to operate in a referenced way, based on referrals from other health units in the Butantã health district, mainly due to the lack of employees. In 2020, the ER environment underwent adaptations due to the COVID-19 scenario, according to data obtained from the application of the instruments, presented in the results item.
2.2 Normative references and best practices
In Brazil, the main standard for elaborating the healthcare facilities’ projects is the Resolution of the Collegiate Board No. 50, of 21 February 2002. This document specifies the technical regulation for planning, programming, elaborating, and evaluating the physical projects of healthcare environments. It is organized into 08 functional units or assignments, with number 02 corresponding to immediate service (Figure 4). For each of these units there are tables of minimum design conditions, such as the mandatory existence of the environment, dimensions, facilities, and others (ANVISA, 2002).

FIGURE 4. Assignments of healthcare facilities SOURCE: ANVISA (2002). Adapted by the authors.
This standard includes criteria pertaining to environmental conditions for the control of HAI. The key aspects addressed include the location of the healthcare facility, zoning of environments (critical, semi-critical, and non-critical areas), circulation areas, physical barriers, workflow, water distribution, placement of lavatories/sinks/surgical lavatories, drains (sewers), location of purge rooms, biosafety in laboratories, finishing materials, elevators/freight elevators/tubes, bidets/bathtubs, synanthropic animals, and air renewal in critical areas. The document underscores the importance of exercising care, confinement, and appropriate packaging of materials during transportation. It cautions against the creation of “clean and dirty” circulations, as this may lead to counterproductive duplication of cleaning and security routines, infrastructure, among other factors (ANVISA, 2002).
The Department of Health (2013) also developed design strategies to manage HAI, they are: rapid assessment before a patient enters the ER; natural light in patient and staff rooms; touch-free doors; a lavatory in front of each room; separation of the staff corridor from the patient corridor; and 100% single rooms (Department of Health, 2013). The importance of individual rooms and cohort areas is related to the existing types of precaution and isolation. Based on the precaution or isolation of the patient who has a disease transmissible by contact, private rooms are recommended. Patients with diseases transmissible by aerosol should be in rooms with the door closed, negative pressure, filtration system, and adequate air renewal (ANVISA, 2021).
Figure 5 presents an example of an isolation room with negative pressure control, that is, the air must not leave the room and flow into the hospital corridors. There is an air extractor and an air return 20 cm from the floor, as required by Brazilian Standard 7256:2022. Part of this air is removed from the environment and part is treated, filtered and returned to the environment. In this case, temperatures must be between 20°C and 24°C and humidity at a maximum of 60%, according to Brazilian Standard 7256:2022 parameters. This standard is based on ASHRAE Standard 170-2021 which addresses ventilation of healthcare facilities. There are also other standards and laws, such as the law number 13,589, of 4 January 2018, which requires the periodic implementation of the Maintenance, Operation and Control Plan for air conditioning systems in buildings for public and collective use (Brasil, 2018). There are also standards and resolutions with IAQ reference standards.

FIGURE 5. Example of cascade pressure control in Airborne Infection Isolation Room, with recirculation SOURCE: ABNT (2022). Adapted by the authors.
To exemplify, there is the Carbon Dioxide (CO₂) concentration, which is the main product of human respiratory activity, and its emission is accompanied by other biological effluents. Consequently, this measurement can indicate whether the environment has good ventilation or air renewal at different occupancy levels (CDC, 2023). The CDC recommends maximum levels of 800 ppm for good ventilation (CDC, 2023). However, an environment can have different concentrations of CO₂, due to pockets of stagnant air. Two environments can also present the same level of CO₂ concentration and there may be a patient with COVID-19 in only one of them, so it is not possible to accurately identify the increased risk of transmission (CDC, 2023).
In Brazil, this concentration is determined at 700 ppm above what is measured in the external environment (approximately 400 ppm) (ABNT, 2023). Regarding the reference standard of CO₂ concentration, there is an interesting observation in Spain. For hospital buildings, the admissible concentration is 350 ppm above the concentration of external air (IDAE - Instituto para la Diversificación y Ahorro de la Energía, 2007). This concentration by type of building may be a relevant implementation, since hospitals tend to have a greater number of airborne pathogens.
2.3 Preparing the instruments
The walkthrough comprised a guided exploration and dialogue with an experienced employee in the relevant sector (Ono et al., 2018), which in this research identified environments, explained the case study, and described the interrelationships between sectors. The script was prepared to include the possible environments in the case study, considering the first technical drawings obtained and the areas provided in the immediate care section of ANVISA (2002). Questions were designed to guide and feed the discussion. This instrument was applied using various recording techniques, such as videos, audio recording, photos, and notes, with prior consent given by the institution and individuals involved, according to the Research Ethics Committee. The activity lasted about an hour.
The decision was made to use semi-structured interviews in order to prepare a script to be followed with a certain amount of flexibility (Rheingantz et al., 2009). Five scripts addressing healthcare, administration, reception, maintenance, and cleaning professionals were prepared. This activity aimed to obtain information about the work routine and the users’ perception of the flows and the IAQ. In this activity, the script and the number of questions were devised to last about 30 min. The first questions were about the employee’s role and work routine within the hospital. Then, the interviewees were asked about flows (routes) and QAI and, finally, there were questions about points of positive trend, points of negative trend, and what should be changed in the ER.
Through observation, the researcher can understand how user activities are supported or inhibited by the built environment that houses them (Bechtel and Churchman, 2002). According to Zeisel (2006), this instrument can be recorded through verbal descriptions, diagrams, pre-coded checklists for counting, plans, maps, photographs, and filming. When the researcher wants to know in detail how often an activity takes place, qualitative observation data can be used to develop a counting checklist, for example,. In addition, recording activities for plans or maps are convenient for situations that require an observation and analysis of how many people are in an area at the same time (Zeisel, 2006).
For the observational survey of the flow of users in the ER (staff, patients, companions, and visitors), materials (medicines, food, clean linen, waste/expurgation, and storeroom), corpses, and equipment, a script was prepared to be applied on different days, considering both weekdays and weekends, during all periods (morning, afternoon, night, and dawn). A legend was drawn up to distinguish, whenever possible, the user’s role and the type of equipment or material being transported. Eight observation points were set up so that, from each one, the researcher could quantify the flow of two to four imaginary lines of passage over 20 min. The imaginary lines and observation points were placed in strategic positions, considering the researchers’ experience in the ER. In addition, there were spaces to register atypical and/or important situations in the script.
Physical surveys allow checking and updating existing projects and technical documents, as well as obtaining information on the materials and measurements of building elements, furniture, and equipment. These surveys are related to visual records, since at this stage the video recordings and photos help to analyze the situation found on a given day and time, as well as to verify and obtain additional and complementary information.
Finally, measurements of environmental conditions provide quantitative data that can be compared with existing parameters in standards and with the users’ opinion. Based on the walkthrough and interviews, the most critical sectors of the ER were identified for carrying out CO₂ concentration measurements. They were: ER reception, AER observation room, CER observation room, AER isolation room, and external environment (for comparison purposes). These measurements were carried out in accordance with the guidelines of Resolution No. 9, of 16 January 2003 (ANVISA, 2003).
3 Results
This article presents the application method and outcomes of five of the seven instruments employed in the research. These instruments include walkthroughs conducted with key individuals, semi-structured interviews with employees, behavior observations (focused on existing flows), physical surveys and visual records, as well as measurements of environmental conditions (specifically related to CO₂ concentration).
3.1 Application and results of instruments for measuring users’ environmental perception
3.1.1 Walkthrough accompanied by key individuals
This instrument was implemented on 29 November 2021, with the participation of two key individuals. The first was an AER nurse, and this dialogued route included the AER, lasting 22 min. The second was a doctor from the Division of Pediatric Clinic, performing the dialogued route through the CER, lasting 25 min, and the OER, lasting 9 min. At the obstetric sector, it was explained that because of the rooms used to perform cesarean sections, the OER should function similarly to the surgical center, taking the necessary care required for such environments, due to the risk of contamination. Thus, on account of the difficulty in accessing this area during the surveys, it was decided to limit the research to the other ER sectors.
Due to the COVID-19 pandemic, significant functional and physical alterations were implemented within the ER of the University Hospital at USP. Throughout this period, both the AER and CER were partitioned into separate sections—an observation area and a flu area. Moreover, temporary structures were erected outside the ER, synchronized with peak COVID-19 case occurrences. The access to the ER was renovated, operating via three designated entrances. Figure 3 specifies each door: door 3 remained assigned for emergency cases transported by ambulances, door 2 was modified to serve adult patients with flu-like symptoms, and door 1 was allocated for all other cases.
In the case of door 2, the initial assistance was provided through a digital environment, using telemedicine. Consequently, a healthcare professional conducted the triage, provided instructions to the patient, and, subsequently, there was a waiting room and a collection room where the COVID-19 diagnostic test was administered. Within the flu area, additional facilities included dressing and undressing rooms for employees, a nursing team room, a restroom, a room to prepare medication, a room for emergency procedures, and four isolation rooms. In the case of the hospital area adapted for adult flu, three of the four isolation rooms had a high wall split air conditioning system and one had windows for natural ventilation (Figure 6).
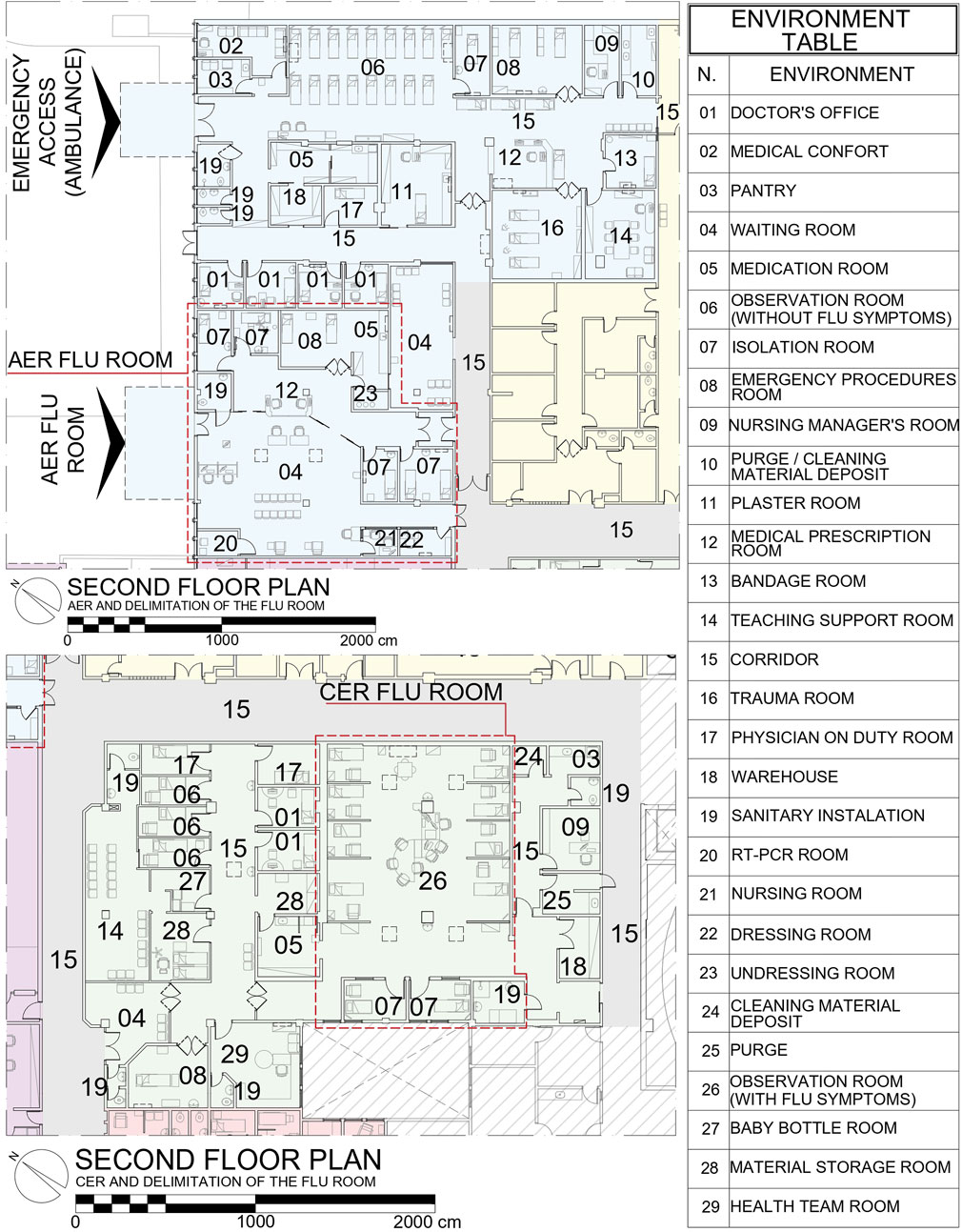
FIGURE 6. AER and CER, with the flu area delimitation SOURCE: based on Soares (2023) and adapted by the authors.
In relation to the CER, due to a greater demand of patients with flu-like symptoms, the existing observation area started to function as a flu room (Figure 6). This environment had the capacity to accommodate 10 patients, 02 that could be allocated in 02 isolation rooms. These rooms had a window to the external environment and did not have air conditioners or other systems to control environmental conditions. Children without flu-like symptoms were accommodated in adapted offices, in an independent corridor inside the CER.
3.1.2 Semi-structured interviews with employees
There were 16 employees selected to be interviewed face-to-face or in virtual format, throughout the second half of 2021 and the first half of 2022 (Table 1).
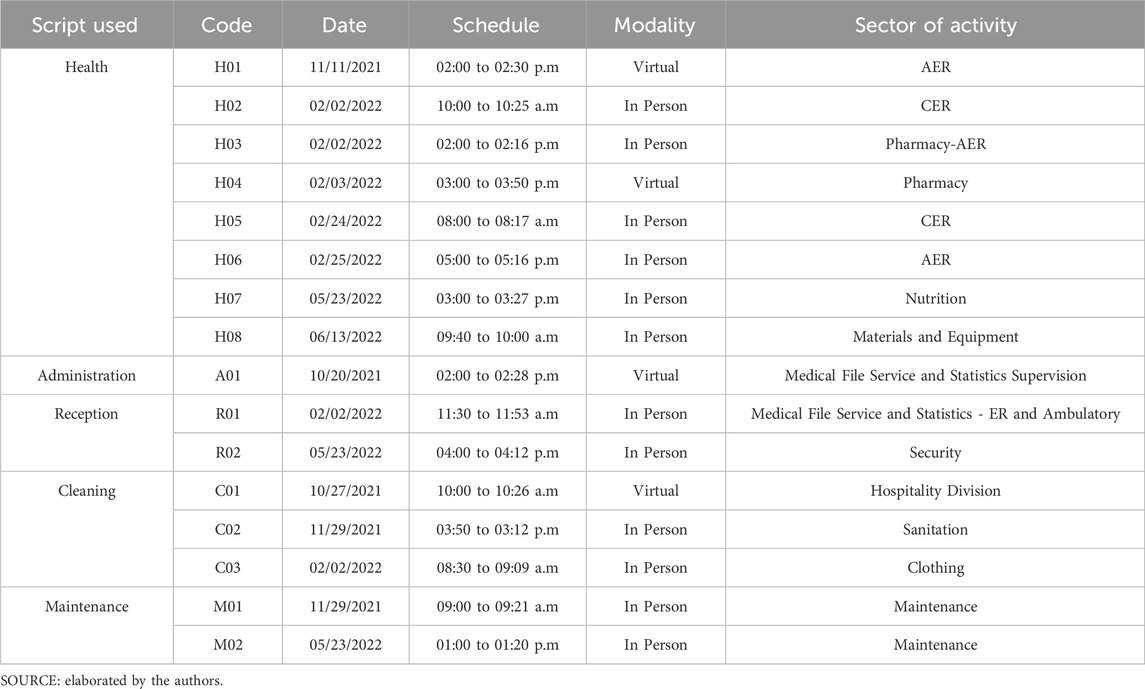
TABLE 1. List of employees interviewed.
During the interviews, the distances from the ambulance arrival door to the emergency procedures room and between complementary sectors, such as AER and the area to carry out imaging tests, were discussed. The information flow faced challenges due to the absence of an electronic medical record system, thus having to rely on paper records in that environment. Additionally, issues with vertical transportation via elevators were reported, especially during maintenance of the clean or dirty freight elevator. It was identified that there was a lack of properly designed isolation environments that were equipped with pressure monitoring, dressing and undressing spaces, and private bathrooms. On a positive note, the flu sector and the implementation of remote registration for individuals exhibiting flu-like symptoms were highlighted.
Concerning ventilation and IAQ, there were widespread reports of malfunctioning air conditioning units, largely the older units of high wall split or cassette types. The central air-conditioning system was only present in the surgical center and x-ray environment. There was maintenance, operation, and control plan, incorporated in periodic maintenance activities at the hospital.
3.1.3 Behavior observation for flow mappings and quantifications
The observations for surveying and quantifying the flows showed the flows of users and materials. Thus, observation points correlated to imaginary counting lines were determined based on the researchers’ experience in the case study, as well as what had been stated in the interviews. Figure 7 displays all observation points and all imaginary counting lines. When one of the classifications crossed the line, it would be counted. This instrument enabled the design of the flow map and the elaboration of graphs, which allowed for the identification of situations that could be improved. Such observations occurred in the morning, afternoon, night, and dawn of the following days: 06/28/2022; 06/29/2022; 07/01/2022; 07/02/2022; 07/03/2022 (dawn); 07/05/2022; 07/06/2022 (dawn); 07/07/2022; 07/09/2022.
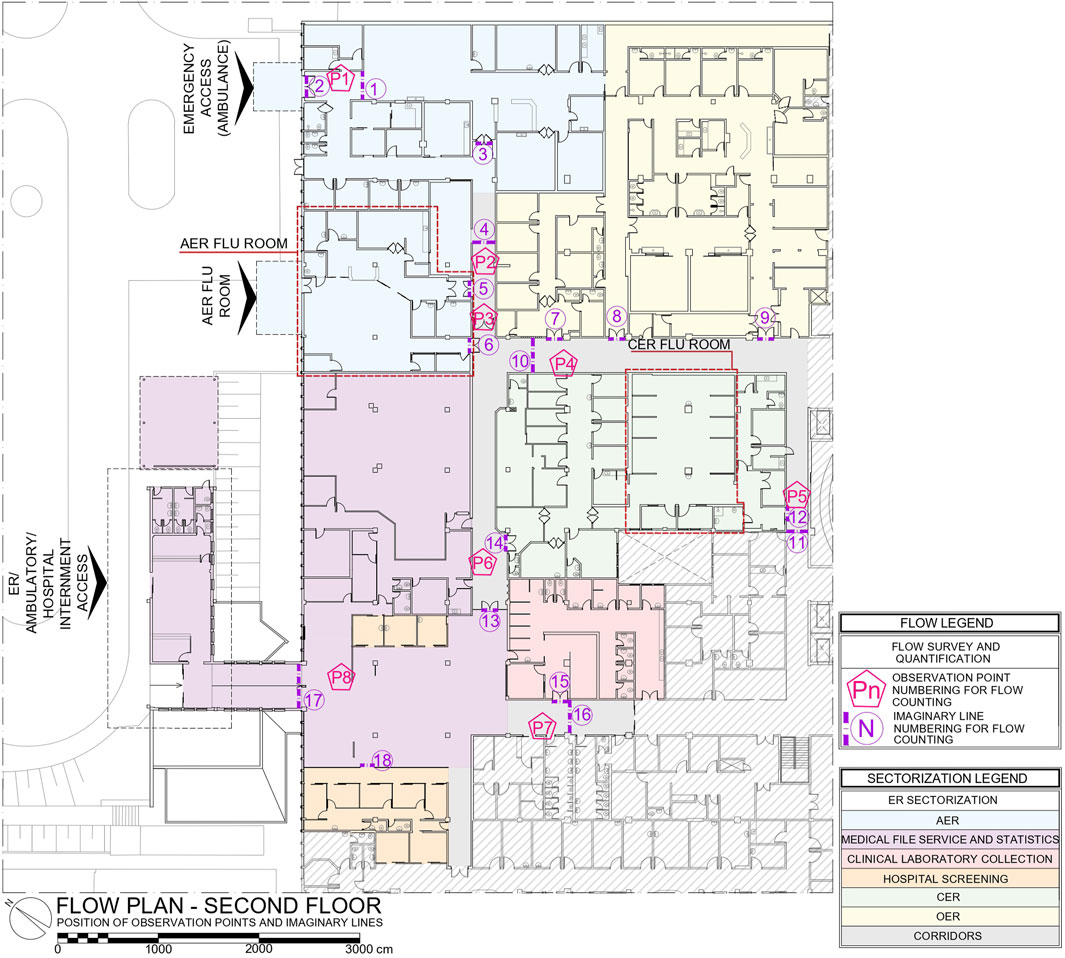
FIGURE 7. Position of observation points and imaginary crossing lines SOURCE: based on Soares (2023) and adapted by the authors.
With the quantification and classification of passers-by, graphs associated with imaginary counting lines were created (Figure 8). Thus, the circulations most used for services (less exposed circulations), by visitors and companions, by healthcare service providers (doctors, nurses, and healthcare students) changing shifts, and others, were identified. The imaginary counting line number 3 was selected to be commented (Figure 8), as it was an access door to the AER sector, not a general circulation area, which presented profiles of passers-by and quantities similar to the hospital’s general circulation areas. This door was located next to the AER waiting room and waste trolleys, nutrition trolleys, patients who needed to undergo imaging tests, companions, cleaning staff, and others passed through it. The door was a swing door, commonly used. Its automation would be relevant, together with the insertion of a washbasin in its proximity and the use of another access for services, not considered dirty circulation, but for the humanization, organization, and discipline of the environment flows.
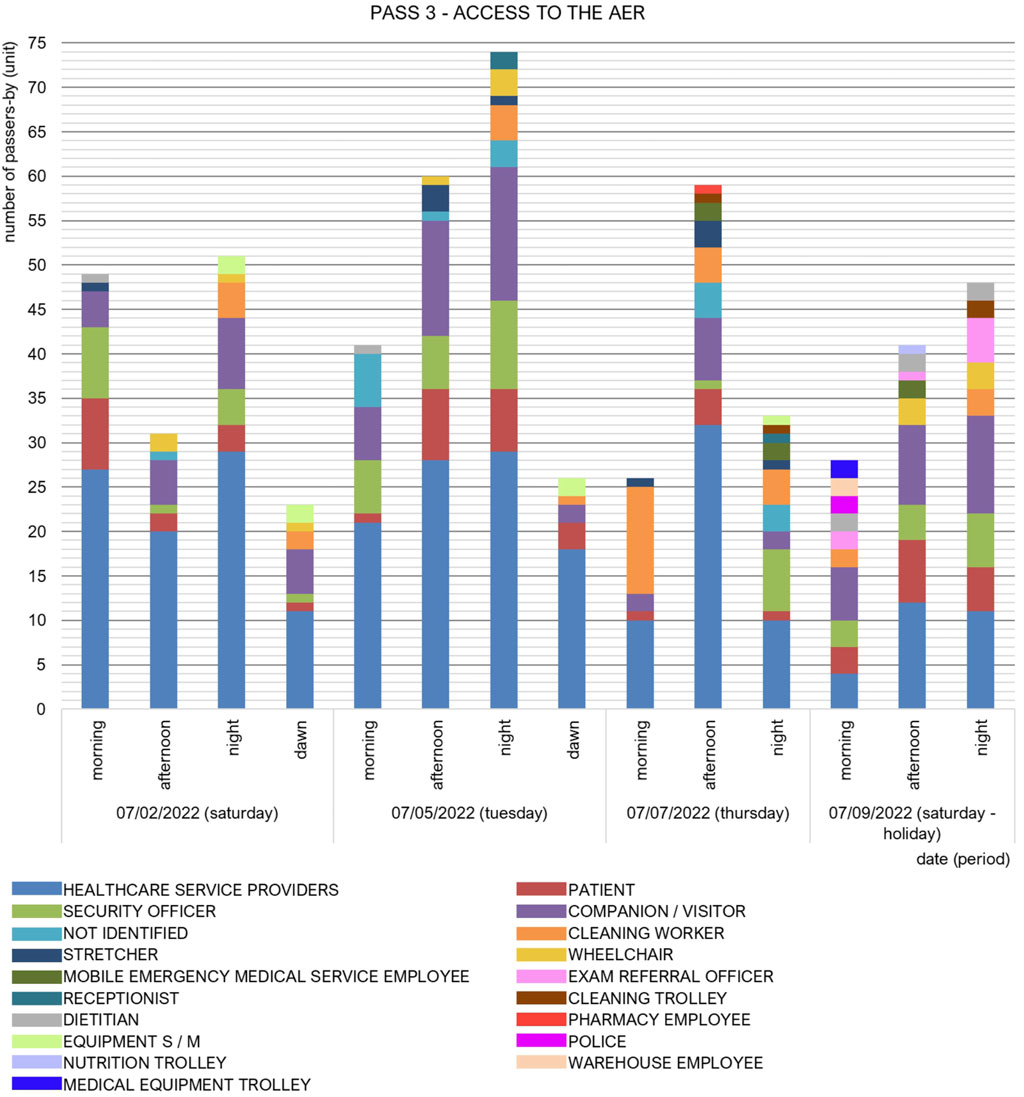
FIGURE 8. Number of passers-by through passage 3 during the dates and periods of observation SOURCE: based on Soares (2023) and adapted by the authors.
The generation of user and material flow maps was made possible through meticulous observation and classification of individuals passing through. As a result, certain discrepancies emerged that contradicted the information obtained from walkthroughs and interviews. For instance, it was noted that the patient elevator was being utilized to transport deceased individuals, contrary to the designated soiled freight elevator. Moreover, waste materials were being disposed of, and warehouse supplies were delivered through the main access door within the AER (marked by the imaginary counting line number 3).
3.2 Application and results of instruments for the evaluation of the specialist
3.2.1 Visual records and physical surveys
Visual records (video recordings and photos) were made during standard hospital procedures (Figure 9), mainly in the ‘walkthrough accompanied by key individuals’ stage. The objective of these records was to obtain information on the constructive elements and layout of the ER. When it was presented and used throughout the research, the anonymity of hospital users was guaranteed.

FIGURE 9. ER photographic records SOURCE: authors’ collection.
The physical surveys were necessary to verify the technical drawings and the as-built layout of the ER. Therefore, the ER plan was printed in different scales, in order to facilitate the annotations of the measurements obtained, using a laser and a manual tape.
3.2.2 Measurements of environmental conditions related to CO₂ concentration
The CO₂ concentration was measured in the external environment, ER reception, AER observation room (at two different points), CER observation room (at two different points), and AER isolation room (Figure 10). The portable greenhouse gas analyzer, brand - ABB Measurement & Analytics, model—918M-GGA-(918-0011-0000-0000) was positioned intentionally to not disturb the flow of users and materials, and to present a distance of at least 2 m from CO₂ emitting sources. The analyzer hose inlet was secured onto a mobile support and positioned 1.50 m from the floor, as recommended by Resolution No. 9, of 16 January 2003 (ANVISA, 2003), and a protection filter installed to prevent particulate matter.
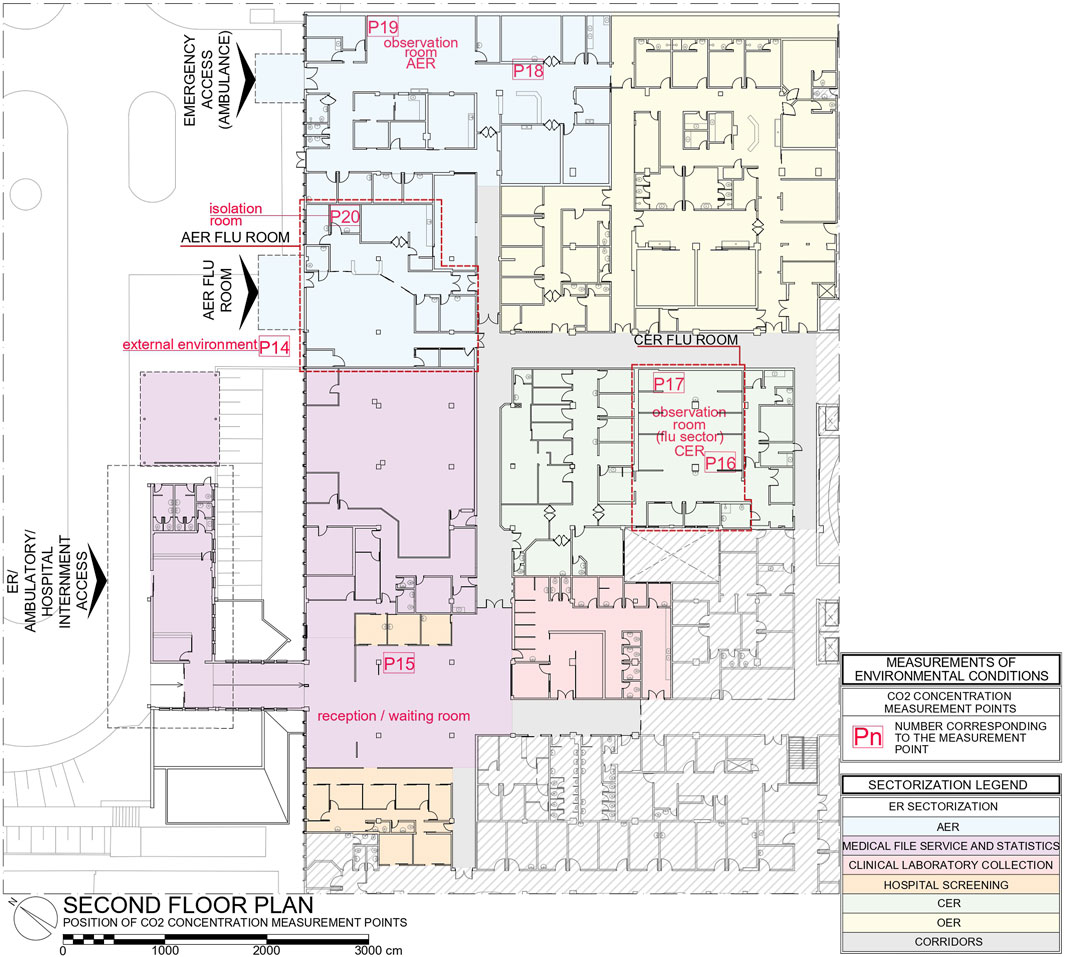
FIGURE 10. Position of CO₂ concentration measurement points SOURCE: based on Soares (2023) and adapted by the authors.
Thus, on 06/29/2022 and 07/01/2022, the set consisting of the analyzer, screen (monitor) and hose with filter was transported to the respective measurement points, generally remaining for 20 min at each point. Below, the measurements are shown from 07/01/2022 for points P14, P15, P17, and P19, and from 06/29/2022 for points P16, P18, and P20.
The external measurement (P14) was around 450 ppm for the two measurement days. At the reception (P15), with around 20 to 30 people, with closed windows, without fan/air conditioning on and with the access door permanently open, the measurement indicated approximately 535 ppm. In the CER, measurements were made at two points. At the most critical point (P17), at the back of the room, a maximum value of 937 ppm was measured, with about 10–15 people in the room, without air conditioning on and windows closed. In the AER, the most critical point, in the background (P19), it was 902 ppm, with no air conditioning on, some windows open, and the ambulance door frequently open. In the isolation room (P20), the researcher stayed in the room for 1 h 30 min, simulating a patient. In 1 h 30 min the concentration reached about 791 ppm, decreasing based on the opening of the room door (Figure 11).
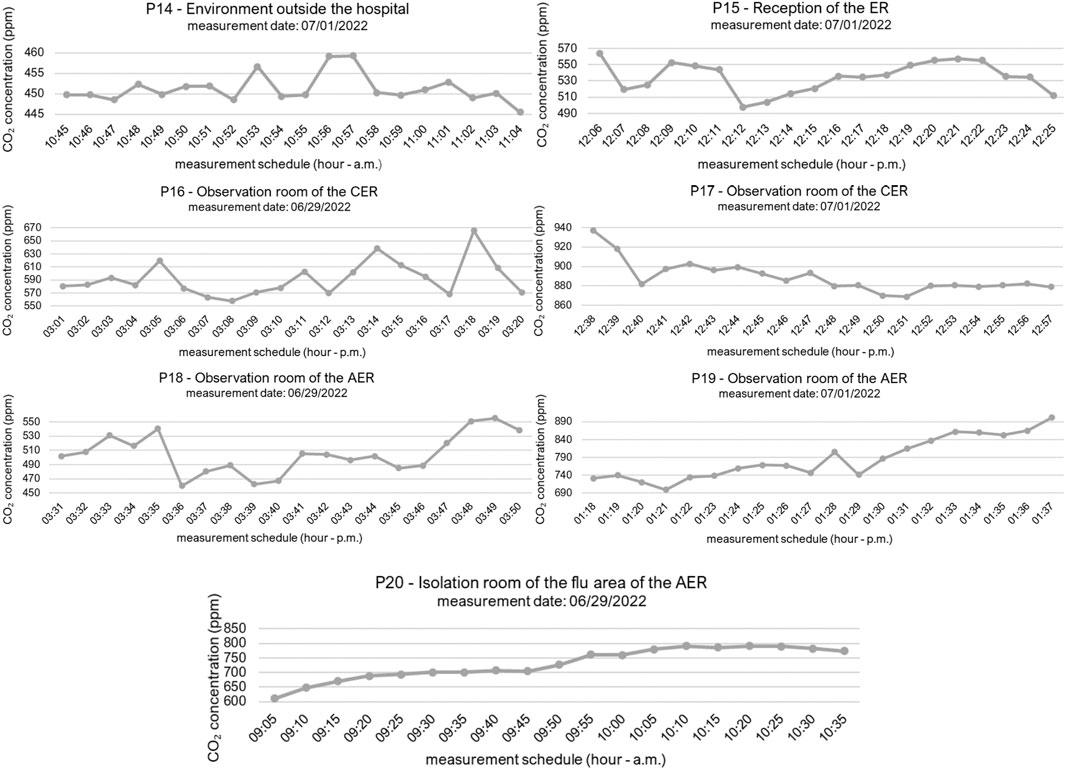
FIGURE 11. Comparison of CO2 concentration measurements SOURCE: based on Soares (2023) and adapted by the authors.
4 Discussion
4.1 Diagnoses and recommendations
Two summary tables were compiled. The first addressed the primary occurrences diagnosed and related to flows, and the second detailed the main occurrences associated with IAQ. The occurrences were systematically listed, and the corresponding sectors were identified. Subsequently, the instruments employed for identifying the situation were outlined, followed by recommendations based on standards, best practices, and references used in the research. An excerpt of these (Table 2) is provided as an illustrative example. Criteria were established for classifying the risk of infection (high, medium, or low) and, consequently, the intervention priority (maximum, medium or minimum).
a) High risk and maximum priority: critical area (ANVISA, 2002) or environment with a risk level of 2–3 (ABNT, 2022) or more than one group of users (employees, patients, companions, and visitors) affected by the occurrence or aspects related to the transport of materials or patients.
b) Medium risk and medium priority: semi-critical area (ANVISA, 2002) or environment with risk level 1 (ABNT, 2022) or a single group of users affected by the occurrence.
c) Low risk and minimum priority: non-critical area (ANVISA, 2002) or environment with risk level 0 (ABNT, 2022).
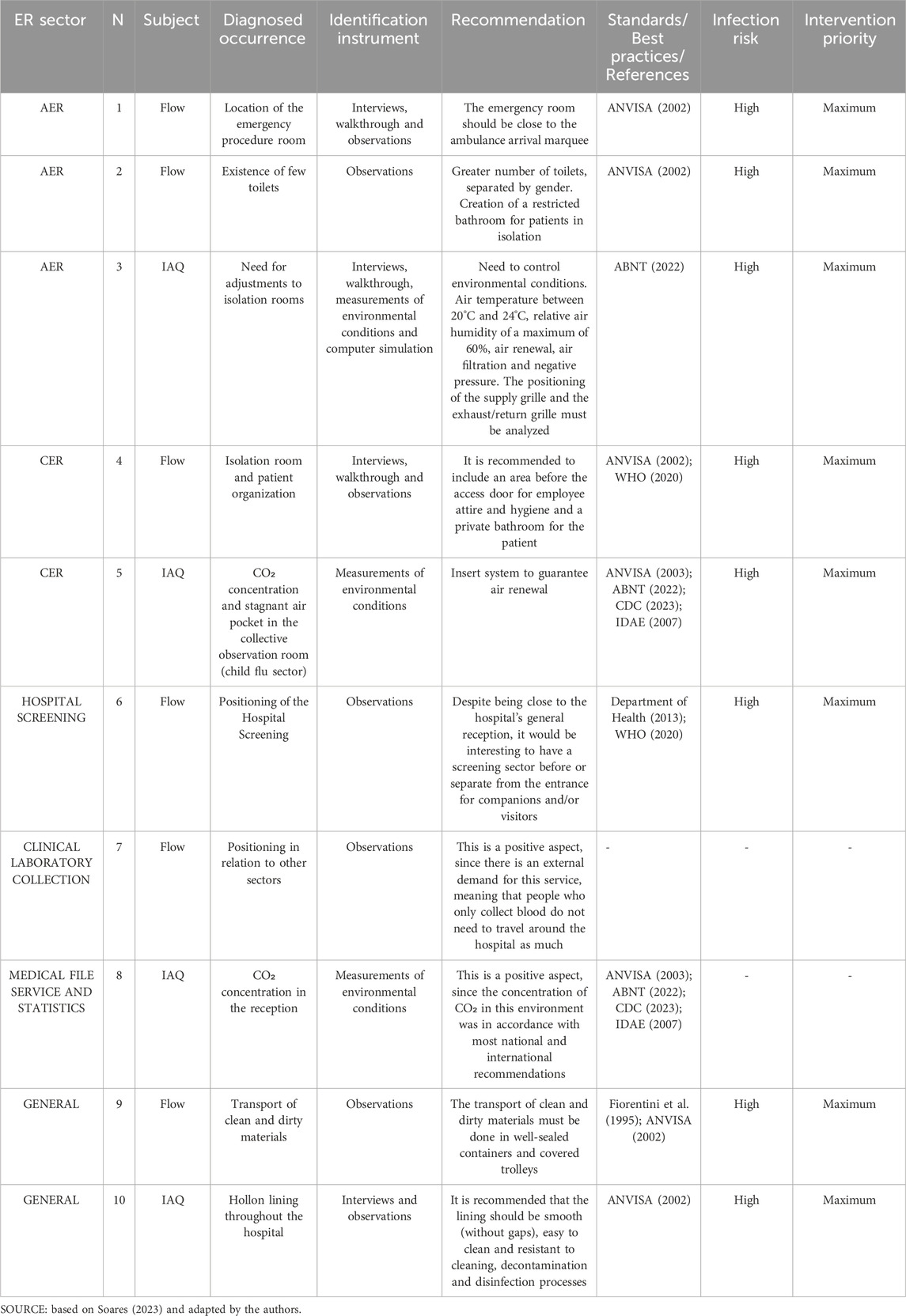
TABLE 2. Example of summary table of diagnoses and recommendations.
The positive aspects identified in the ER were also addressed in the summary table and in the summary map. For these occurrences, risk-level of infections and intervention priority were not determined.
Maps were prepared in order to cover the diagnoses and recommendations presented in the summary table to help visualize and understand the results. Thus, the plan structure of the sectors that comprise the ER and a summary of the information presented in the table were inserted (Supplementary Material). Each map contains a set of cards and each card has the number of that diagnosed occurrence; the sector where it is located; the subject addressed (whether it is related to the flow or the IAQ); the instruments that were used to identify the occurrence; the classification of the risk of infection (high, medium, or low); and the intervention priority (maximum, medium, minimum). In addition, there is a description of the diagnosed occurrence, along with a photo, related standards/best practices/references, and a summary of the recommendations.
An example is shown in the Supplementary Material. In all, 07 boards were prepared with all 50 diagnoses obtained throughout the research related both to the positive aspects identified and to those that could be improved. The photos and information present in the summary table and in the summary map were obtained between the second half of 2021 and the first half of 2022, with the possibility that interventions were carried out at the hospital after the second half of 2022.
Examples of areas for improvement, particularly regarding flows, include the lack of dedicated space for storing equipment such as wheelchairs, currently placed in corridors, posing potential disruptions to flows. Issues were also identified regarding the transport of dirty clothes/waste in improperly sealed trolleys, leading to strain on garbage bags and the risk of ripping. There is a significant need for increased rigor and adherence to the use of vertical circulations. Additionally, there is a shortage of closets to accommodate clean clothes in both the AER and CER. Patient accommodations in the collective AER observation room were identified as being in close proximity without dividers between beds. The absence of a Master Plan to guide organizational aspects, growth, priorities, connections, and circulations within the hospital was noted. Moreover, considerable distances were observed between complementary sectors of the hospital, such as the imaging exams sector and the ER. A single access point for patients, companions, and visitors to the hospital was identified. Recommendations included positioning the emergency procedures room near the ambulance access marquee to enhance faster service. Finally, it was suggested to use and to recognize ER observation rooms as transition areas to other hospital sectors, such as the intensive care unit, surgical centers, hospitalization, or discharge, providing temporary shelter for patients.
Some of the positive aspect mentioned are the flu sector with independent access, which facilitated the organization of patient flows; the visibility of the nursing or medical prescription station to avoid unnecessary distance to patient beds; the use of video calls to receive patients with flu-like symptoms; and the existence of alcohol gel dispensers, information posters, washbasins in the doctor’s offices, and other features.
These aspects are in line with the design strategies proposed by Capolongo et al. (2020). It was observed that these authors highlighted the importance of flexibility and resilience, mainly related to adapting spaces and circulation, which are favored by horizontal hospital configurations (main body connected to support pavilions). The authors also emphasized the existence of independent flows for employees and patients and, in the case of patients with infectious diseases, they must enter the building through another access point (Capolongo et al., 2020; Jovanović, 2022), as in the AER of the case study analyzed in this research. Moreover, a greater supply of single rooms and isolation rooms is essential in these situations (Capolongo et al., 2020), something reported by ER employees in the interviews. The existence of pre-screening tents outside the building was also mentioned by Capolongo et al. (2020) and observed in the case study of this research.
Equally vital is the emphasis on establishing protocols and training for hospital staff (Jovanović, 2022), particularly concerning the proper transportation of materials, food, waste, dirty garments, and clean apparel, all adequately sealed. The organization of flows (physical, at certain times, or by type) also contributes to humanization and to easing the flow in undersized or very busy areas or passages (Fiorentini et al., 1995; ANVISA, 2002). The care for elderly patients also deserves attention. Many patients with dementia, who required specific care from the medical staff, nursing staff, and companions were observed during the visits. It would be interesting if the ER was divided into AER, CER, OER, and a specific area for elderly people.
Concerning IAQ, it is imperative to check water pipes in order to address potential infiltrations and repair plaster partition damages. The application of hollow lining in critical or semi-critical areas of the hospital, such as the AER observation room, is not recommended, and it is stipulated that linings should be gap-free and easily cleanable. The absence of a dedicated room in the ER for inhalation procedures is noteworthy. Attention should be given to enhancing environments intended for employee comfort. Adjustments are required in critical and semi-critical areas, including emergency procedures and isolation rooms, which require systems for temperature, humidity, pressure, air filtration, and renewal control. There is a possibility for air recirculation zones at the farther ends of the observation rooms, attributed to elevated CO₂ concentration values.
Marinelli (2020) and Gola et al. (2021) emphasized the importance of having hospital environments with controlled pressure and other mechanical ventilation systems. Singh and Dewan (2020) reported on the dangers of using air conditioning units that do not blow fresh air into the environment and only recirculate the existing air. This was observed in the case study, as critical and semi-critical environments had this type of device, which only contributes to thermal comfort. Łukasik and Porębska (2022) reported an oversight related to legislation and health unit designers, the lack of anteroom (air chambers) in isolation rooms. This situation was also observed in the ER of the University Hospital at USP.
Regarding CO₂ concentration measurements, the need to include a system that guarantees air renewal in its environment is highlighted, paying attention to the position of the insufflation grille and the exhaust/return air grille. With the split air conditioning on and the airborne infection isolation room closed, a gradual increase in CO₂ concentration was observed in that room occupied by one person (over the course of 1 h 30 min). This can confirm that the air only circulates in the environment, with no significant renewed air flow. Furthermore, it was noticed that, in the same environment with a similar occupancy situation, the CO₂ concentration may be different according to the positioning of the measuring point. This may indicate that the room lacks a good air mix, as mentioned by CDC (2023). Such recirculating air flow, generally in the corners of the room and around furniture, can trap air and infectious aerosol, delaying its evacuation through the exhaust system (Sinha et al., 2022). This situation can be harmful to both the patient and the healthcare service providers.
In the Brazilian Standard 7256:2022 (ABNT, 2022) the multitude of requirements for air treatment in healthcare facilities encompasses international standards, notably ASHRAE standards and recommendations. Nevertheless, a pertinent question arises: within the Brazilian context, to what extent can these air treatment requirements be feasibly implemented? This consideration takes into account integrating systems into pre-existing buildings, heightened maintenance considerations, and the financial resources required for its implementation.
Additionally, the main standard for Brazilian healthcare facilities projects, Resolution of the Collegiate Board No. 50 of 2002 (ANVISA, 2002), is more than 20 years old. This standard defines an airborne infection isolation room, presenting a door with a fixed window, an area before the bedroom for cleaning and dressing (anteroom), and a private patient bathroom, but it does not classify the existence of such an environment as mandatory in ERs. Moreover, considering the technological evolutions related to health buildings, health emergencies, and the greater occurrence of epidemics over this period, it is identified that Resolution of the Collegiate Board No. 50 of 2002 (ANVISA, 2002) should be updated so as to include specific requirements related to the built environment of healthcare facilities, helping them to be expandible, flexible, and resilient.
A positive aspect identified is the concentration of CO₂ at the reception within the parameters established as standard, and the existence of a Maintenance, Operation, and Control Plan followed and carried out periodically by the hospital.
5 Conclusion
This study focused on identifying the relevant aspects to elaborate consistent diagnoses and recommendations directed at ER environments, using a case study. Considering the situation experienced and the experience gained in the COVID-19 pandemic, these diagnoses and recommendations are related to activity flows and IAQ. The results obtained contribute not only to improving the case study environment, but also to providing support for ERs and healthcare facilities related to HAI, pandemics, endemics, epidemics, or outbreaks.
Based on the first analysis of the case study environment, the first interviews, and the walkthrough, it was noticed that the area had problems related to indoor air, due to the lack of an adequate HVAC system and the fact that the sector was semi-underground. As for the activity flows, these were rearranged due to the COVID-19 pandemic scenario. Thus, with the appropriate approval from the Research Ethics Committee, multiple POE methods were used. The research proved to be consistent, especially because multi-methods were used, and also because it was possible to cross reference and combine results in order to prepare diagnoses and recommendations.
It is therefore important to highlight the need for ER environments to present a sector that is physically more independent and delimited to receive cases related, for example, to Severe Acute Respiratory Syndrome, with a triage area and organization of environments so that patients can be separated into cohorts. The greater supply of single rooms or partitions between the patients’ beds contributes not only to reducing HAI rates but also to affording a patient’s privacy. Furthermore, the existence of adequate airborne infection isolation rooms proved to be essential in terms of the case study regarding the COVID-19 pandemic. These environments, as well as others that have requirements established in standards, must have systems to control their environmental conditions, where air temperature is just one of the variables to be controlled and, therefore, air conditioners that only provide thermal comfort are not recommended. In critical and semi-critical areas, control and stability of environmental conditions must be ensured, implementing adequate artificial systems that are constantly kept clean, sanitized, and maintained.
A positive point emphasized was the ER adaptation to receive and allocate patients with flu symptoms, with access to the area outside the building. Access through an independent door, separate from the hospital’s general front desk, contributes to the safety of other users and to greater control of the flow of people with such symptoms. The insertion of telemedicine to open records is also a positive aspect, considering the exposure of the receptionists at the front desk. Consequently, the research underscored the significance of integrating technologies like video call service at the reception area, electronic medical records, and touchless doors (automatic). These implementations mitigate physical contact with surfaces and decrease the need for paper exchange among professionals and departments. The positioning of washbasins and gel alcohol dispensers along the circulation areas and at the entrance to the sectors and the organization of the flows help to set up discipline measures in the employees’ routine.
Recommendations for future surveys also include incorporating other equally important issues in discussions related to HAI, namely: cleaning and surface materials; waste management, separation, and storage; and analysis of air or water samples for the verification and quantification process of biological agents. Future research may discuss aspects related to the visibility and humanization of environments or sectors intended for isolating patients. The aspect of privacy in ER observation rooms, the environments that receive patients in different situations, also deserves attention.
Another relevant aspect to investigate is the issue of the reference standard of CO₂ concentration. In a more recent standard, Brazilian Standard 17037 published in 2023, it assumes a reference value of 700 ppm above that which is measured in the external environment, something around 400 ppm. During the pandemic, the CDC (2023) recommended values of around 800 ppm to indicate good air ventilation. Furthermore, it would be interesting if the resolutions established lower CO₂ concentrations for the classification of healthcare facilities, as is done in IDAE (2007), since the low air renewal in such environments can further contribute to the accumulation of pathogens in the air.
It is important to quantify the benefit-cost ratios to incorporate systems in order to control environmental conditions and technologies that can quicken assistance, avoiding unnecessary trips to access information, and other arrangements. Thus, showing that these systems, when designed and operated correctly, contribute to reducing HAI and, consequently, to lowering costs with such patients, while improving the user’s health condition, it is possible that decision makers will be more open to these ideas.
Hence, it is evident that all identified aspects can and should be integrated into discussions related to renovations or projects for healthcare facilities overall. These environments are fundamental for providing support and instilling a sense of security to patients and their families, especially when in vulnerable states. Additionally, they play a vital role in ensuring the wellbeing of employees who spend a significant amount of their time in such settings.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: University of São Paulo Repository: https://repositorio.uspdigital.usp.br/handle/item/524; https://repositorio.uspdigital.usp.br/handle/item/532; http://repositorio.uspdigital.usp.br/handle/item/549; https://repositorio.uspdigital.usp.br/handle/item/550.
Ethics statement
The studies involving humans were approved by the Research Ethics Committee of the University Hospital at the University of São Paulo, on 18 June 2021. Certificate of Presentation for Ethical Appreciation number: 47467921.0.0000.0076. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
VS: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Methodology, Validation, Visualization, Writing–original draft, Writing–review and editing. SO: Conceptualization, Funding acquisition, Methodology, Project administration, Supervision, Writing–review and editing. AF: Conceptualization, Formal Analysis, Methodology, Supervision, Validation, Visualization, Writing–review and editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by the São Paulo Research Foundation (FAPESP) under process No. 2021/04063-3 and the National Council for Scientific and Technological Development (CNPq) under process No. 304131/2020-2.
Acknowledgments
The author VS thanks the São Paulo Research Foundation (Fapesp—process 2021/04063-3) for the master’s scholarship received. The author SO thanks the National Council for Scientific and Technological Development (CNPq-process 304131/2020-2) for the productivity grant received. The authors thank the University Hospital at USP for authorizing the search, and all its employees who participated and contributed with information about the case study. The authors thank Lucas Melchiori Pereira and Ranieri Carvalho Higa for their assistance in the data collection stage, and Professor Fernando Akira Kurokawa for his assistance in the computational fluid dynamics simulation stage.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fbuil.2023.1331970/full#supplementary-material
Abbreviations
ABNT, Associação Brasileira de Normas Técnicas; AER, Adult Emergency Room; ANVISA, Agência Nacional de Vigilância Sanitária; ASHRAE, American Society of Heating, Refrigerating and Air-Conditioning Engineers; CDC, Centers for Disease Control and Prevention; CER, Children’s Emergency Room; CO₂, Carbon Dioxide; COVID-19, Coronavirus Disease 2019; ER, Emergency Room; HAI, Healthcare-Associated Infections; HVAC, Heating, Ventilating and Air Conditioning; IAQ, Indoor Air Quality; IDAE, Instituto para la Diversificación y Ahorro de la Energía; OER, Obstetric Emergency Room; POE, Post-Occupancy Evaluation; USP, University of São Paulo; WHO, World Health Organization.
References
ABNT – Associação Brasileira de Normas Técnicas (2022). Norma Brasileira 7256: tratamento de ar em estabelecimentos assistenciais de saúde – requisitos para projeto e execução das instalações. Rio de Janeiro.
ABNT – Associação Brasileira de Normas Técnicas (2023). Norma Brasileira 17037: qualidade do ar interior em ambientes não residenciais climatizados artificialmente – padrões referenciais. Rio de Janeiro.
ANVISA—Agência Nacional de Vigilância Sanitária (2002). Resolução n° 50, de 21 de fevereiro de 2002. Dispõe sobre o regulamento técnico para planejamento, programação, elaboração e avaliação de projetos físicos de estabelecimentos assistenciais de saúde. Brasília: Ministério da Saúde.
ANVISA—Agência Nacional de Vigilância Sanitária (2003). Resolução n° 9, de 16 de janeiro de 2003. Referenciais de qualidade do ar interior em ambientes climatizados artificialmente de uso público e coletivo. Brasília: Ministério da Saúde.
ANVISA—Agência Nacional de Vigilância Sanitária (2021). Nota Técnica GVIMS/GGTES/ANVISA Nº 04/2020 - orientações para serviços de saúde: medidas de prevenção e controle que devem ser adotadas durante a assistência aos casos suspeitos ou confirmados de infecção pelo novo coronavírus (SARS-CoV-2). Brasília: Ministério da Saúde.
ASHRAE—American Society of Heating, Refrigerating and Air-Conditioning Engineers (2021). Ventilation of health care facilities: ANSI/ASHRAE/ASHE Standard 170-2021. Available at: https://www.ashrae.org/technical-resources/standards-and-guidelines (Accessed October 19, 2023).
ASHRAE—American Society of Heating, Refrigerating and Air-Conditioning Engineers (2022). Vent. Accept. Indoor Air Qual. ANSI/ASHRAE Stand. 62, 1–2022.
Bechtel, R. B., and Churchman, A. (2002). Handbook of environmental psychology. New York: John Wiley & Sons.
Brasil (2001). “Portaria n°511, de 29 de dezembro de 2000,” in Diário Oficial da União: seção 1 (Brasília: DF).
Brasil (2018). Lei nº 13.589, de 4 de janeiro de 2018. Dispõe sobre a manutenção de instalações e equipamentos de sistemas de climatização de ambientes. Diário Oficial da União: seção 1. Brasília: DF.
Capolongo, S., Gola, M., Brambilla, A., Morganti, A., Mosca, E. I., and Barach, P. (2020). COVID-19 and healthcare facilities: a Decalogue of design strategies for resilient hospitals. Acta Bio Medica Atenei Parm. 91 (9-S), 50–60. doi:10.23750/abm.v91i9-S.10117
CDC – Centers for Disease Control and Prevention. (2023). COVID-19 -ventilation in buildings. Centers for disease control and prevention. Available at: https://www.cdc.gov/coronavirus/2019-ncov/community/ventilation.html (Accessed October 19, 2023).
Dariva, L. C. T. L., and Marconsini, C. (2020). O estudo dos fluxos no projeto hospitalar: inter-relações entre sistemas de circulação, organização espacial e forma. Rev. Ambiente Hosp. 13, 41–50.
Department of Health (2013). Health Building Note 15-01: accident & emergency departments – planning and design guidance. London: The National Health Service (NHS). Available at: https://www.england.nhs.uk/wp-content/uploads/2021/05/15_01final3_v3.pdf (Accessed October 19, 2023).
Emmanuel, U., Osondu, E. D., and Kalu, K. C. (2020). Architectural design strategies for infection prevention and control (IPC) in health-care facilities: towards curbing the spread of Covid-19. J. Environ. Health Sci. Eng. 18, 1699–1707. doi:10.1007/s40201-020-00580-y
Federal Facilities Council (2001). Learning from our buildings: a state-of-the-practice summary of Post-Occupancy Evaluation. Washington, D.C.: National Academy Press. Federal Facilities Council Technical Report No. 145.
Fiorentini, D. M. F., Lima, V. H. de A., and Karman, J. B. (1995). Arquitetura na prevenção de infecção hospitalar. Brasília Ministério Saúde.
Gola, M., Caggiano, G., De Giglio, O., Napoli, C., Diella, G., Carlucci, M., et al. (2021). SARS-CoV-2 indoor contamination: considerations on anti-COVID-19 management of ventilation systems, and finishing materials in healthcare facilities. Ann. Ig. Med. preventiva comunita 33 (4), 381–392. doi:10.7416/ai.2020.2396
IDAE – Instituto para la Diversificación y Ahorro de la Energía (2007). Comentarios RITE-2007: reglamento de instalaciones térmicas em los edifícios. Madrid, Spain. Available at: https://www.idae.es/sites/default/files/documentos/publicaciones_idae/documentos_10540_comentarios_rite_gt7_07_2200d691.pdf (Accessed October 19, 2023).
Jovanović, N. (2022). Hospital architecture in times of crisis. Int. Rev. Psychiatry 34 (7-8), 861–867. doi:10.1080/09540261.2022.2154642
Lesan, M., Khozaei, F., Kim, M. J., and Nejad, S. M. (2021). Identifying health care environment contradictions in terms of infection control during a pandemic with a focus on health workers’ experience. Sustainability 13 (17), 9964–9980. doi:10.3390/su13179964
Łukasik, M., and Porębska, A. (2022). Responsiveness and adaptability of healthcare facilities in emergency scenarios: COVID-19 experience. Int. J. Environ. Res. public health 19 (2), 675. doi:10.3390/ijerph19020675
Marinelli, M. (2020). Emergency healthcare facilities: managing design in a Post covid-19 World. IEEE Eng. Manag. Rev. 48 (4), 65–71. doi:10.1109/EMR.2020.3029850
Ono, R., Ornstein, S. W., Villa, S. B., and França, A. J. G. L. (2018). Avaliação Pós-Ocupação: na arquitetura, no urbanismo e no design - da teoria à prática. São Paulo: Oficina de Textos.
Pilosof, N. P., Barrett, M., Oborn, E., Barkai, G., Pessach, I. M., and Zimlichman, E. (2021a). Telemedicine implementation in COVID-19 ICU: balancing physical and virtual forms of visibility. HERD Health Environ. Res. Des. J. 14 (3), 34–48. doi:10.1177/19375867211009225
Pilosof, N. P., Barrett, M., Oborn, E., Barkai, G., Pessach, I. M., and Zimlichman, E. (2021b). Inpatient telemedicine and new models of care during COVID-19: hospital design strategies to enhance patient and staff safety. Int. J. Environ. Res. Public Health 18 (16), 8391–8405. doi:10.3390/ijerph18168391
Preiser, W. F. E., Hardy, A. E., and Schramm, U. (2018). Building performance evaluation: from delivery process to life cycle phases. 2. Switzerland: Springer International Publishing AG.
Rheingantz, P. A., Azevedo, G. A. N., Brasileiro, A., Alcantra, D., and Queiroz, M. (2009). Observando a qualidade do lugar: procedimentos para a avaliação pós-ocupação. Rio de Janeiro: Programa de Pós-Graduação em Arquitetura da Faculdade de Arquitetura e Urbanismo da Universidade Federal do Rio de Janeiro.
Salonen, N., Ahonen, M., Sirén, K., Mäkinen, R., Anttila, V. J., Kivisaari, M., et al. (2023). Methods for infection prevention in the built environment – a mini-review. Front. Built Environ. 9, 1–13. doi:10.3389/fbuil.2023.1212920
Singh, R., and Dewan, A. (2020). Rethinking use of individual room air-conditioners in view of COVID-19. Creat. Space 1, 15–20. doi:10.15415/cs.2020.81002
Sinha, K., Yadav, M. S., Jayakrishnan, R., Kumaraswamy, G., Murallidharan, J. S., and Kumar, V. (2022). Field experiments to identify and eliminate recirculation zones to improve indoor ventilation: comparison with CFD. Trans. Indian Natl. Acad. Eng. 7, 911–926. doi:10.1007/s41403-022-00335-1
Soares, V. S. L. (2023). Ambiente de pronto-socorro hospitalar e infecções: avaliação pós-ocupação realizada no contexto da pandemia de COVID-19. Dissertation (Master's Degree in Architectural Technology). São Paulo (SP): Faculdade de Arquitetura e Urbanismo da Universidade de São Paulo.
Soares, V. S. L., Ornstein, S. W., and França, A. J. G. L. (2022). Current approaches for preventing environment-associated contamination in healthcare facilities: a systematic literature review by open access database. Archit. Struct. Constr. 2, 439–453. doi:10.1007/s44150-022-00063-8
Thomazoni, A. D. L., Ornstein, S. W., and Ono, R. (2016). “Post-occupancy evaluation applied to the design of a complex hospital by means of flow analysis,” in Revisiting the Role of Architectural Science in Design and Practice: 50th International Conference of the Architectural Science Association. The Architectural Science Association and The University of Adelaide. 1, Adelaide, South Australia, 7-9 December 2016, 537–546.
Universidade de São Paulo. Centro de Preservação Cultural (2005). Cidades Universitárias: patrimônio Urbanístico e Arquitetônico da USP/Centro de Preservação Cultural. São Paulo: Editora da Universidade de São Paulo: Imprensa Oficial do Estado de São Paulo.
Waroonkun, T., and Prugsiganont, S. (2022). Preventing the spread of COVID-19 through environmental design in Thai community hospitals. Front. Built Environ. 8, 1–17. doi:10.3389/fbuil.2022.947211
WHO - World Health Organization (2020). Severe Acute respiratory infections treatment centre. World health organization. Available at: https://www.who.int/publications/i/item/10665-331603 (Accessed October 19, 2023).
Keywords: COVID-19, emergency room, emergency department, healthcare environment, indoor air quality, healthcare-associated infection, post-occupancy evaluation, activity flow
Citation: Soares VSL, Ornstein SW and França AJGL (2024) Evaluation of an emergency room in operation during the COVID-19 pandemic: diagnoses and recommendations concerning environmental factors. Front. Built Environ. 9:1331970. doi: 10.3389/fbuil.2023.1331970
Received: 02 November 2023; Accepted: 22 December 2023;
Published: 25 January 2024.
Edited by:
Hasim Altan, Prince Mohammad bin Fahd University, Saudi ArabiaReviewed by:
Nishant Raj Kapoor, Academy of Scientific and Innovative Research (AcSIR), IndiaTanut Waroonkun, Chiang Mai University, Thailand
Copyright © 2024 Soares, Ornstein and França. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Vitória Sanches Lemes Soares, dml0b3JpYXNsc29hcmVzQGdtYWlsLmNvbQ==