
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Built Environ., 14 June 2021
Sec. Indoor Environment
Volume 7 - 2021 | https://doi.org/10.3389/fbuil.2021.688836
This article is part of the Research TopicAcoustics in the Built Environment: a Challenge for Improving the Quality of LifeView all 14 articles
 Kerstin Persson Waye*
Kerstin Persson Waye* Jonas Karlberg
Jonas KarlbergIn Sweden preschool-age children spend most of their waking hours at preschool. At this age children undergo substantial physical and mental development and their hearing sensations may not be comparable to those of an adult. The preschool sound environment is loud and highly intermittent, and the acoustic may not be supportive for young children’s hearing, and wellbeing. This article describes an acoustic intervention among seven preschools, and comparisons with three reference preschools. The intervention included changing floor mats to plastic mats designed to reduce impact sounds, adding damping cushions under chairs, change of ceiling absorbers and, in some rooms, addition of wall absorbers. The effect of the intervention was studied using a previously developed interview protocol, “Inventory of Noise and Children’s Health,” in combination with sound level and room acoustic measurements. A total of 61 children aged 4–6 years were interviewed before the intervention, and 56 after. A reduction of the sound levels in a range of LAeq 1.2–3.8 dB for meal/craft rooms and play rooms were found for the intervention preschools using stationary noise level meters, while this was not found for the reference preschools. The reverberation time (T20) decreased slightly after the interventions. The average room frequency response for the two room types tended to be more flat after the interventions. Further investigations are needed to see its importance for the perceived acoustic quality. The results linking children’s perception and response to the measured reduction in sound levels, confirmed an association between reduced sound levels after the acoustic intervention and a 30% reduction in stomach ache, as well as in children’s perceptions of scraping, screeching sounds. Children’s perceptions of these sounds were further associated with important oral communication outcomes. Children’s bodily sensations of sounds were also associated with psychoacoustic symptoms and wellbeing. Despite the seemingly modest reduction in sound level, the acoustic intervention was indeed perceived and reported on by the children. Future studies should pay more attention to how a supportive preschool acoustic environment should be optimised and acoustically described to take preschool-age hearing and perception into account.
Preschool-age children are in a phase of life which involves substantial physical and mental development. This is also the age period where most of the neural development takes place (Tamburlini et al., 2002). In Sweden, a great majority of children aged 1–5 years spend most of their waking hours at preschool, hence this environment is of prominent importance for their health and wellbeing. Given that the critical period for optimal formation of linguistic skills is also within this early age period, ranging from about 12 to 36 months (Kuhl, 2010), the acoustic environment in which language is communicated and understood is highly relevant. However, preschool premises are often not acoustically optimized for specific preschool requirements supporting children’s perception of sounds, learning, and communication. The preschool sound environment is intermittent and unpredictable, with one Swedish study showing more than 80 one-second logged events exceeding 85 A-weighted decibel (dBA) during hours of preschool activity (Sjodin et al., 2012). Other stationary measurements of noise levels in Turkey found that the sound levels during the meal period was slightly higher than the period of play (Gokdogan and Gokdogan 2016). Five minutes A-weighted equivalent noise levels (LAeq) during the meal times ranged from 60 to 81 dB for the group of 3 years old, 67–82 dB for the 4 years old and 69–85 dB for the group of 5 years old children. Similar noise levels were recorded in public preschools on Iceland where 89% of the samples were above 70 dB LAeq and 43% above 75 dB LAeq (Jonsdottir et al., 2015). High sound levels were also recorded in a preschool in Germany, showing 8 h equivalent noise levels from stationary measurements of 71 dB LAeq, and average dosimeter levels on teachers of 80 dB LAeq (Eysel -Gosepath et al., 2010). Dosimeter measurements on children show that children tend to be exposed to even higher sound levels. An average of 154 measurements on children show levels of 84 dB LAeq during their time spent indoors, with maximum A-weighted noise levels, Fast time weighting (LAFmax) up to 118 dB (Persson Waye et al., 2011); the latter exceeds the permissible maximum levels for the occupational environment in Sweden (AFS 2005:16, 2005).
Preschool children’s hearing and auditory perception differs from that of adults (Fels, 2008). Using anthropometric data from children and subsequent simulation, Fels (2008) was able to show that the diffraction and reflection properties of the head, pinna, and torso (the head-related transfer functions; HRTF) in children are not comparable to those in adults. The HRTFs play a major role when it comes to localizing sounds, as understanding speech in a room under noisy conditions is tightly dependent on the directivity pattern of the head. The HRTF of a child up to the age of seven amplifies the frequencies around 6 kHz, and the ear canal of a child further adds to this frequency amplification, which may be compared to an adult whose HRTF and ear canal leads to amplification around 3 kHz. It has further been found using an auditory oddball paradigm and event-related brain potentials (ERPs) that changes of pitch, but not loudness, evoked ERPs among 6–9-year-olds when the sound was irrelevant to their current task (Sussman and Steinschneider, 2011). For slightly older children (10–12 years), both pitch and loudness evoked a response in similar task situations. This may indicate that neural processing of sound frequency and sound intensity develop during different phases of a child’s development, and that neural processing of frequency precedes that of intensity. Initial support for certain sounds and characteristics playing a key role for small children was also found in a qualitative study of 36 preschool children aged 4–5 (Persson Waye et al., 2013), where uncontrollable sounds and distressing sounds (i.e., angry yelling and scraping, screeching sounds) were experienced as both physically and emotionally painful.
Surprisingly little attention has been paid to the differences between adults and small children in hearing and hearing function, and the possible consequences for attention, learning, and wellbeing. The large body of research in this field has focused on the impact of transportation noise on children’s cognitive functions, with the most consistent results found for exposure to aircraft noise and impaired reading comprehension and long-term memory (Clark and Paunovic, 2018). Fewer studies have been targeted at noise created by the inhabitants of classrooms or preschools, even though this so-called “babble noise” usually contributes to a higher indoor noise level than transportation noise, and has been found to negatively affect primary school children’s performance on verbal tasks (Dockrell and Shield, 2006). A high babble noise and or poor reverberation would be particularly destructive for young children’s word recognition up to the age of 12–15 years as they require better acoustics than adults (Neuman et al., 2010). Apart from its effect on cognition, noise may affect young children’s emotional wellbeing, although there have been very few studies on this topic. One exception is a study by Klatte et al. (2010) which found an association between higher reverberation time in the class room (indicative of poor acoustics) and young children’s reporting of a greater disturbance from indoor noise (“My classmates often behave noisily” “Our teachers often reprove us for silence”) as well as reporting poorer relationships with their teachers and classmates, less motivation and less social integration. Another exception is a recent study by Astolfi et al. (2019). Interviews with 6–7 years old pupils were compared to a wide range of room acoustic measures and noise level measurements. They found that children rated themselves as less happy in classrooms characterised as having bad acoustics. Interestingly, it was also found that reported wellbeing and noise disturbance seemed to depend on the pupils being happy or not, calling for the need of a longitudinal study design. Some further guidance on how noise may affect children emotionally and behaviourly can be derived using preschool teachers’ perspectives. As part of a large survey on preschool teachers’ occupational environment and their health, we included one question asking if teachers judged preschool noise to affect children’s behaviour and if so, how. The analysis showed that 82% of them considered noise to affect children’s behaviour (Persson Waye et al., 2019). A content analysis of the free text provided by the nearly 4,000 preschool teachers that answered yes on the posed question showed that the most common observations were children vocalizing to be heard, followed by children being distracted, unfocussed, angry, sad, exhausted, and withdrawn.
Acoustic interventions performed in preschools are typically aimed at reducing the reverberation time, reducing speech interference, or improving clarity. The reverberation time (T or T60) measures the time it takes for a sound to decay by 60 dB (ISO 3382-2, 2008), and is hence a measure of how quickly a sound in the room is attenuated. A longer reverberation time would increase the background noise level and possibly the levels from the children. The length of the reverberation time depends on scattering objects and how absorbent the surfaces are in the room. The Swedish standard (SS 25268:2007+T1, 2017) suggests that the reverberation time (T20) in preschools should be 0.5–0.6 s depending on the room function. Clarity (C50) and Deutlichkeit (D50) describe the ratio of early (before 50 ms) and late reverberation energy, with more early energy meaning less alteration of the direct sound. High values of clarity are typically considered to make the spoken sound more easily perceived, but scientific evidence is ambiguous and especially lacking for children. Less influence of secondary reflexes may also have the beneficiary effect of reducing irrelevant noise. As children and adults tend to increase their voice when speaking in high background noise, referred to as the Lombard effect (Lane and Tranel 1971), a reduction of the secondary reflexes should in principle reduce the need for children to raise their voices. This is important as it is commonly reported that small children raise their voice to be heard in noisy environment (Lindström et al., 2010; Persson Waye et al., 2019). The so-called inverse Lombard effect is though still not well understood and evidence on the mechanism remains inconclusive. Speech transmission index (STI) is also frequently used as a measure of speech intelligibility (IEC 60268-16, 2011). In brief, a test signal is emitted that resembles speech including modulated frequencies, and the signal in the receiver position is compared to the original and analysed with reference to the modulation depth.
Few studies have investigated the effects of acoustic interventions and their possible benefits for children’s learning or wellbeing. Acoustic interventions in schools and preschools typically include fitting absorbents, changing floor carpets, and fitting chairs with noise-reducing cushions. One study evaluated whether the fitting of sound absorbent panels in the ceilings of four classrooms with poor acoustical design in two preschools/kindergarten would affect 3–5 years old children’s cognitive performance, linguistic skills and measure of helplessness. Measurements were done before and one year after the fitting and showed an improvement in letter and number recognition, language skills as rated by the teacher, and a reduced susceptibility to induced helplessness using un unsolvable jigsaw puzzle (Maxwell and Evans, 2000). Another study evaluated the combined effect of reducing the external noise from the train and fitting the classrooms facing the rail by absorbent panels in the ceilings (Bronzaft 1981). Comparisons were made before and after the interventions with pupils in classrooms facing a quiet side. Before the intervention the reading scores were significantly lower for the pupils in the noisy classrooms as compared to the quieter classrooms, but 1 year after the interventions this difference had disappeared.
The study presented here evaluated the effectiveness of an intervention aimed at improving the acoustical qualities in preschools in terms of reduced noise levels, and examined the effects of the intervention on children’s perceptions and reactions assessed before and after the intervention. The study originate from a framework derived on the basis of focus group discussions with children (Dellve et al., 2013). During 11 focus groups, children recruited from five preschools were interviewed about their perception of sound in the preschool situation, their understanding of the source of this sound, and their perceived reactions at both the emotional and the physiological level. The results formed the basis for the development and validation of a questionnaire known as Inventory of Noise and Children’s Health (INCH) (Persson Waye et al., 2013). The present study used INCH to measure the children’s perceptions and reactions.
The aim of this study was to study the association between an acoustic intervention and children’s perceptions of and reactions to sounds in their preschool environment. Specifically, we aimed to study the association between perceptions, reactions, and symptoms in relation to the sound environment both in terms of objective measurements and as perceived by the children.
In the period from October 2006 to October 2009, children aged four to five and their parents were recruited from seven preschools in Mölndal, Sweden, where interventions were undertaken with the purpose of improving the acoustical qualities in the preschools. In total, 63 children and 59 parents filled out the questionnaire before and after the intervention. The response rates ranged from 80% in the parents to 98% in the children. This article reports on the data from the children and the acoustic measurements; parental data will be reported elsewhere. Two of the children fell outside the age range of 4–5 years and were excluded from further analysis, resulting in a study population of 61 children. Data from both the pre- and post-measurements were available for 56 of them.
The study was carried out in accordance with the Declaration of Helsinki on Biomedical Research Involving Human Subjects, and was approved by the ethics committee in Gothenburg (ref: 670-06). Parental consent was obtained in advance for the children’s participation, but regardless of parental consent, no child was made to take part against their own will.
Acoustic interventions included changing floor mats from traditional plastic to plastic mats designed to reduce impact sounds, adding damping cushions under chairs, and installing sound-absorbing tiles on the ceilings and some of the walls. Table tops had already been changed to acoustically soft material before the intervention. All of the mentioned acoustic interventions were in accordance with SS 25268:2007 T1 (2017). The expected effect of the absorbers was a moderate reduction of the A-weighted equivalent sound level in the range of 3 dB, while the changes in table tops and floor mats and the addition of damping cushions were expected to mainly lead to a decrease in the level of contact sounds resulting from, for example, plates and glasses being put down on the table or chairs being pulled over the floor. These latter types of sounds would normally not be of large importance for the overall A-weighted sound level in a preschool, but could still be of importance for high-frequency contact sounds in the acoustic environment.
The room acoustic parameters reverberation time (T20), Clarity (C50), Deutlichkeit (D50), Centre time (Ts) and speech transmission index (STI) were evaluated in three random preschools before and after acoustic interventions (ISO 3382-1, 2009). Two room types were studied; “meal/craft room” and “play room.”
Noise levels were measured during the course of 1 week, 1 month before the intervention and again 3 months after the intervention, using stationary measurements and personal dosimeters. The purpose of measurements using the stationary sound level meters was to gain an overall estimate of the sound levels in the room from the activities, and to see how the acoustic interventions possibly affected the sound levels. Sound levels in the room used for crafts and eating meals (meal/craft room) and the room for organised activity or play (play room) were measured for 1–2 days per room using a stationary sound level meter type I (Bruel and Kjaer 2260) equipped with a ½ inch microphone. The system was calibrated before and after the measurement week and before and after every movement between measurement positions using an acoustic calibrator (Bruel and Kjaer 2231). The microphone was placed 0.5 m from the ceiling at a position where the activity noise would be representative for that room. Figure 1 shows a typical example of a measured sound environment in one of the preschool play rooms.
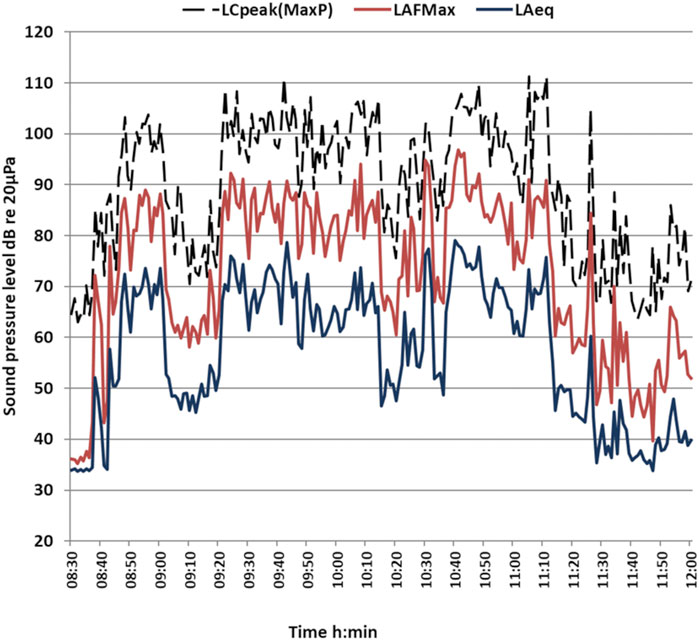
FIGURE 1. Typical example of the distribution of sound pressure levels dB (C-weighted peak levels LCpeak, LAFMax, LAeq) in a play room in the morning, measured as 30-s equivalent noise levels.
The measured 30-s equivalent sound level varied greatly over time during the course of a day, depending on the activities and presence of children and staff in these rooms. In order to cope with this highly variable condition, we adopted a method of analysing the periods when the rooms were occupied. Periods when the rooms were occupied were first identified by asking the staff about the time periods for meals, craft, and play, and then including these periods for each respective room while excluding periods spent elsewhere, for example doing outdoor activities. Using these definitions, the occupied periods were 08:30–11:30 for the play room and 11:30–12:30 and 14:00–15:15 for the meal/craft room; in the analyses, the two meal/craft room periods were combined. We then analysed minute by minute the length of a measurement period for respective room for the levels to become stable, this means that the cumulative period analysed was not deviating significantly from the proceeding period established using a t-distribution based 95% CI. The logarithmic mean values were calculated using the formula stated in Nordtest Method NT ACOU 115 (2003) section 10.4. The theoretical approach was that these periods would be long enough to not show deviation if longer measurement periods would be made at any random interval. The hence derived sound levels would in other words not have been significantly different if we have included a longer time period. In our case, stable periods were derived after an average of 17–22 min depending on the room. The stable periods were determined when the deviation between the different periods were less than 0.5 dB. Using these time periods, we calculated percentiles of time for sound levels in the room. In this study, we judged that sound periods exceeding the 50% level (LAeq50%) would reflect levels when the room is inhabited. For more details of the method, see Nordtest Method NT ACOU 115 (2003). The sound levels for these time periods were averaged for the room types and used as a base for the statistical analyses of the effect of the intervention.
Individual noise exposures were obtained from two children at a time, using dosimeters (SPARK 705 +), and analysed using BLAZE 5.06 software, type II. The purpose was to gain an estimate of the children’s and personnel’s noise exposure when being indoors. The settings used were 30-s averaging intervals, a gain of 30 dB, and a range of 43–113 dB. Only time periods when the staff and children were participating in their usual indoor preschool activities were used for these personal measurements (referred to in the following as time indoors, Ti). The same procedure was undertaken in the reference schools where no interventions took place. The total numbers of dosimeter measurements at times I (pre-intervention) and II (post-intervention) were 61 and 55 for the study group children, 66 for the study group staff on both occasions. For the reference groups there were 18 children and 18 staff at time I and 20 children and 23 for staff at time II.
Perception of sounds was measured by means of a questionnaire (INCH) developed through focus group interviews with 3–5-year-old preschoolers (Dellve et al., 2013) and subsequently validated and presented in Persson Waye et al., (2013). The interviews were performed by one research assistant within our research group A Agge. She was trained in interviewing children by a special care pedagogue that carried out the focus group interviews in the preceding study (Dellve et al., 2013). After parental consent and in agreement with the preschool teachers, one child at a time was interviewed in a room at the preschool premises. The child was initially asked general questions on what colours he/she would like at the preschool, and if he/she liked the dining room and the play room and what sounds he/she normally heard at the preschool. After this introductory conversation the child was asked how frequently he or she heard sounds from the three sound sources found to be most relevant from the analyses of focus groups (Dellve et al., 2013): yelling and angry children, strong and loud sounds, and scraping and screeching sounds. Answers were indicated on a five-point Likert scale (ranging from “almost never” to “very often”) presented as five circles increasing in size and including 1–5 dots.
Using the same scale of circles, the children were asked how often they experienced the teachers yelling or shouting when talking. For the analyses, a bipolar scale was created with scores ≤3 recorded as 0 and scores >3 as 1.
Bodily perception of sounds was indicated by pointing at various parts of the body of a child-like figure with neutral bodily and facial expression, shown in isolation but similar to the middle figure on the scale in Figure 2. The answer was recorded for all three sounds separately, but to increase the robustness of the analysis, any physical perception of any sound was used; this was scored as 1 and 0, with the latter indicating no bodily perception of any sound.
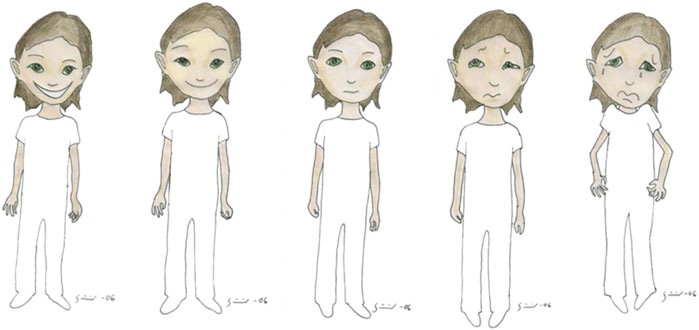
FIGURE 2. Visual representation of the scale measuring sad reaction, with the furthest left position labelled happy/safe and the furthest right position labelled sad/afraid. The neutral position was used in a separate figure for children to score the bodily reaction.
Aspects of reaction were measured using the following wording: “How do you feel when you hear (the sounds of angry, yelling children) (loud and strong sounds) (scraping and screeching sounds)?” Answers were indicated on a bipolar visual scale representing figures drawn with different facial and bodily expressions ranging from glad/safe to sad/afraid (sad reaction) and from kind/friendly to angry/irritated (angry reaction), respectively. The scale of the sad reaction is given in Figure 2.
The reaction was recoded to neutral position (code 3) for those children who indicated on the previous question on perception that they “almost never” heard the sound. In the analyses, scores ≤3 were coded as 0 and scores >3 as 1.
Psychosomatic symptoms that may be related to noise among children were elicited using the question: “During the last few days at preschool have you had a (tummy ache) (headache)?” The prevalence of hoarse throat was measured using the same question. Answers were given on a 5-graded scale with circles increasing in size from “never” to “often.” Finally, a question was asked about general wellbeing, using figures similar to those used for sad/happy reaction (Figure 2). As above, a bipolar scale was created with scores ≤3 recorded as 0 and scores >3 as 1.
An overview of the design and procedure is given in Table 1. Children in the intervention preschools were interviewed 1 month before (time I) and 3 months after the intervention (time II). Times I and II were chosen to include spring and autumn, which are similar with regard to daylight and time spent outdoors. The periods therefore did not include December and January, which are the darkest and coldest period, and the summer months of May and August. In order to diminish the risk of inter-rater variance as much as possible, the interviews were performed by two trained persons. The children were asked questions in a structured way, and presented with visual representations of scales on show cards. When the child was not able to answer the question, they were not prompted to do so. In the reference preschool, children were not interviewed; only sound levels were measured.
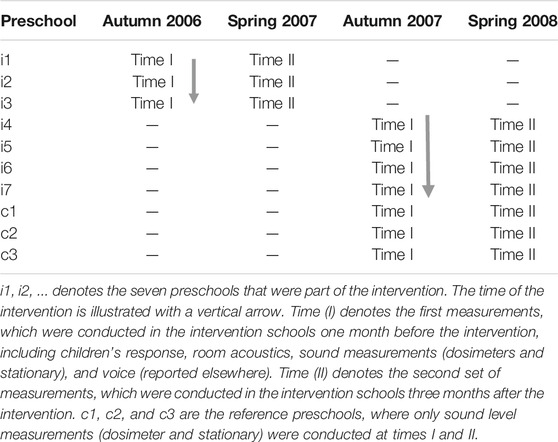
TABLE 1. Study design and the time measurements in relation to the intervention, in the intervention preschools and the reference preschools.
The children in the studied preschools typically arrived before breakfast, which was at 08.00, and were collected by their parents or similar between 16.00 and 18.00. Table 2 shows the distribution of age and gender of the children included in the analysis of the interviews. There was a high participation rate among the children both before and after and there was no difference in response rate between preschools. The children included in the before and after study were fairly well distributed over gender and age groups. All children aged 4–6 years were asked to participate in the interviews; the number who participated ranged from 4 to 15 per preschool. Only children who took part in both the before and after study were included in the analyses.
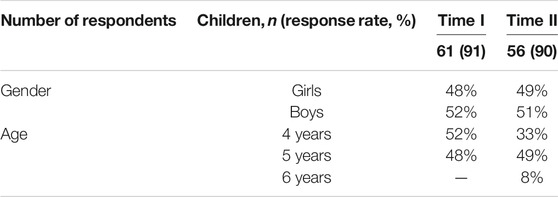
TABLE 2. Study population before (Time I) and after (Time II) the intervention.
Supplementary Table S1 gives the numbers of children attending the preschools every day during the study periods; as shown, the average numbers of children were fairly similar across periods.
Equivalent noise levels from the stationary measurements in the two room categories in each preschool before and after the intervention, as well as the dosimeter measures, are presented using descriptive statistics. The dosimeter levels will have been most strongly influenced by the direct sounds from the child’s own voice, the voices of others, and activities, and to a lesser degree by indirect sounds from the room; they will therefore mainly be used to describe the child’s sound exposure. The noise levels from the stationary microphones, on the other hand, include both direct and indirect (reflected) sound signals from activities in the meal/craft room and play room, and could be hypothesised to be affected by the interventions. In the statistical analyses of whether the intervention affected the noise in the rooms, we compared sound levels occurring more than 50% of the time (LAeq50%) as this would reflect levels when the room is inhabited.
Generalised estimating equation (GEE) logistic regression models were applied to analyse the associations between different outcomes and relevant explanatory variables while accounting for potential confounders and the repeated measures due to the intervention (before-after design) Compound symmetry structure was used for the working correlation matrix (structure: exchangeable). Three models were built. Model I included equivalent stationary noise levels (before and after) as primary explanatory variable, and children’s sound perception, perception of teachers’ vocal behaviour, bodily sensations, sound source reactions, and symptoms as dependent variables. As only one of the sound sources (scraping and screeching sound) was found to be significantly associated with the change of sound level, only this source was included in further analyses. Model II adopted children’s perceptions of sounds as an indicator of perceived noise, and perceptions of teacher’s vocal behaviour, sound source reactions, and symptoms as outcomes. Finally, Model III adopted bodily sensations as an explanatory or independent variable for reported symptoms. Dependent variables were recalculated into binary variables by giving scale values 1, 2, and 3 a score of 0, 4, and 5 a score of 1. Scale values of 4 and 5 are interpreted as “often” and “very often” (perception and symptoms) or as “much” and “very much” (for reaction and wellbeing). For bodily reaction, any bodily reaction to any sound was given a value of 1, and no reaction to any sound a value of 0.
Potential confounding variables such as age and gender were included in all models. The results of regression analyses are given as odds ratios (OR) with 95% confidence intervals (CI). The OR in the presented models denotes an increased or decreased odds of the binary outcomes in relation to a change of the independent variable. If the odds is below 1 and the 95% confidence intervals do not include 1, it shows a significantly reduced perception, reaction or symptom at time II as compared to time I. All statistical analyses were performed using version 20.0 of IBM SPSS Statistics for Windows (IBM Corp, Armonk, NY, United States), applying two-tailed tests and a 5% level of significance.
The mean equivalent A-weighted noise levels measured in the meal/craft room and play room are given in Table 3.

TABLE 3. Mean equivalent A-weighted noise levels, exceeded 50% of the time (LAeq 50%)* dB measured in the meal/craft room and play room at the intervention i) and reference (c) preschools.
For the intervention preschools the mean point estimate of the difference in LAeq 50% in the meal/craft room at time II was rather modest or 1.2 dB, but statistically significant from time I. In the play room the mean point estimate for the intervention preschools was greater, but did not fully reach statistical significance (p = 0.059, t-test), as also indicated by the 95% CI (Table 3). Importantly, there were no statistical differences of mean point estimates the LAeq 50% levels between times I and II in the reference preschools. In Figures 3A,B the equivalent A-weighted noise levels for each averaged time interval of between 17 and 22 min, used to calculate equivalent levels exceeding 50% of the time, are shown for each room type.
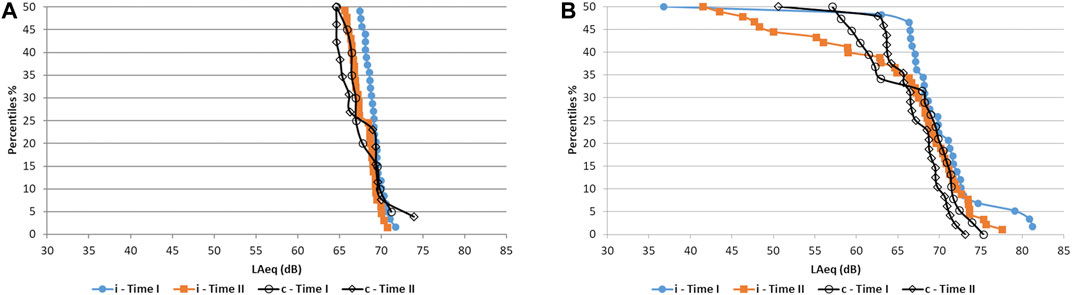
FIGURE 3. LAeq values from stationary measurements before (time I) and after (time II) interventions. Each point represent an equivalent value calculated for a time interval of 17–22 min, depending on the room. Sound levels exceeding the 50% level, LAeq50% are shown. Intervention, “i,” and reference, “c,” for meal/craft room (A) and play room (B).
The average dosimeter levels for children in the intervention group were 85 dB LAeq (95% CI 83.0–86.0) before and 83 dB LAeq (95% CI 82.2–84.6) after the intervention; the corresponding figures for children in the reference group were 84 dB LAeq (95% CI 82.8–85.2) and 84 dB LAeq (95% CI 82.3–86.5) at times I and II, respectively. There was no difference in dosimeter levels between the intervention and the reference groups. Neither did we see any clear differences between weekdays. Table 4 shows the 5, 25 and 50% percentile dosimeter sound levels for the intervention and reference group combined. Dosimeter levels for the staff were on average 6–8 dB LAeq lower than those for the children in both groups (data not shown), and their exposure was significantly different from the children’s exposure (Student’s t-test p < 0.001). In Figures 4A,B the measured dosimeter values for children are shown, each dot or square represent one daily measurement. The obtained values for LAeq and LAFmax are shown together with the limit value for equivalent levels 8 h (LAeq 85 dB) and limit value for maximum levels (LAFmax 115 dB), respectively. As can be seen in Figure 3A, there is some variation of the equivalent sound level between children’s exposure, but a clear majority are exposed to sound levels above LAeq 80 dB during their time spent indoors. For the maximum levels most children are at some time during the day exposed to events exceeding LAFmax 115 dB. According to the work environment statue (AFS 2005:16, 2005) noises above the lower action limit (80 LAeq 8h) dB) require attention while levels above the limit (85LAeq 8h dB or 115 LAFmax dB) require actions such as a requirement for hearing protection.

TABLE 4. Percentiles of dosimeter sound levels LAeqi corresponding to time spent indoors from all intervention 1) and reference (c) preschools at time I and II.
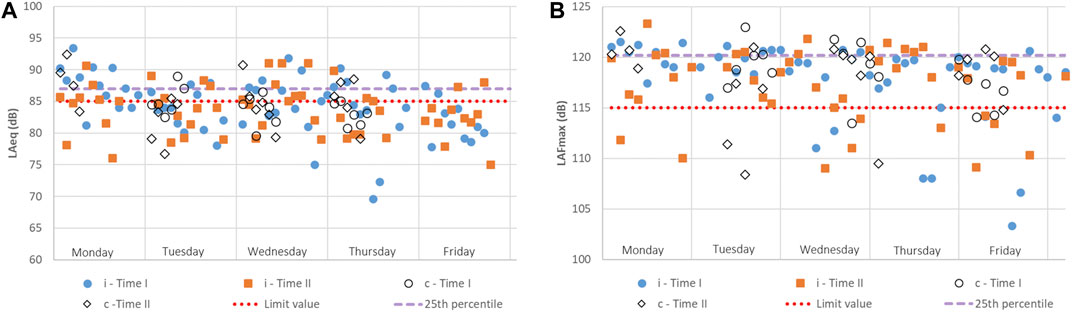
FIGURE 4. Measured dosimeter values per weekday for time I and time II together with 25th percentile, which is based on the whole data-set. In (A) the values for LAeq are shown together with the Limit value (85 dB). In (B) the values for LAFmax are shown together with the Limit value (115 dB). Intervention marked with “i” and reference schools “c.”
Prevalence of children’s perception of angry, yelling sounds, loud sounds, scraping screeching sounds, teachers yelling, and feeling a bodily sensation of any sound “often” and “very often” at time I and II are given in Figure 5.
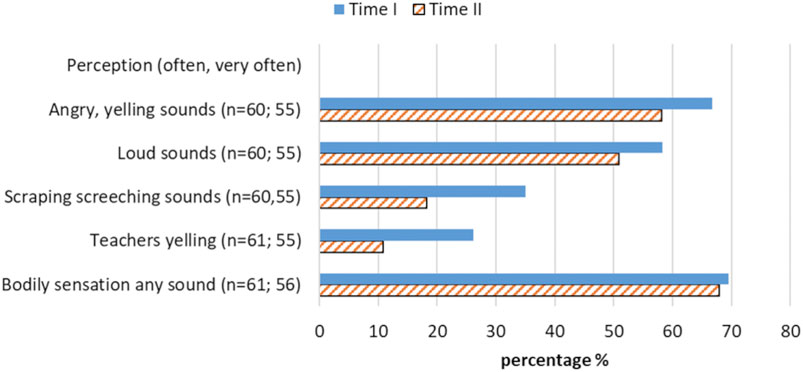
FIGURE 5. Prevalence of children’s perception of angry, yelling sounds, loud sounds, scraping screeching sounds, teachers yelling, and feeling a bodily sensation of any sound “often” and “very often.” Blue bars denote before (time I) and orange bars with diagonal lines denote after (time II), the intervention.
As shown in Figure 5, the proportion of children hearing various sounds tended to be higher before the intervention, with more than 65% of the children reporting hearing angry, yelling sounds often or very often, around 55% hearing loud sounds, and about a third hearing scraping, screeching sounds and the teacher yelling often or very often. Remarkably, close to 70% reported feeling some sounds in various parts of their body, with very similar prevalences in the before and after conditions.
Prevalence of children’s angry or sad reactions to loud strong sounds, scraping screeching sounds and angry, yelling sounds, given a value of four or five on the scale as well as symptoms being reported to occur “often” at time I and II are given in Figure 6.
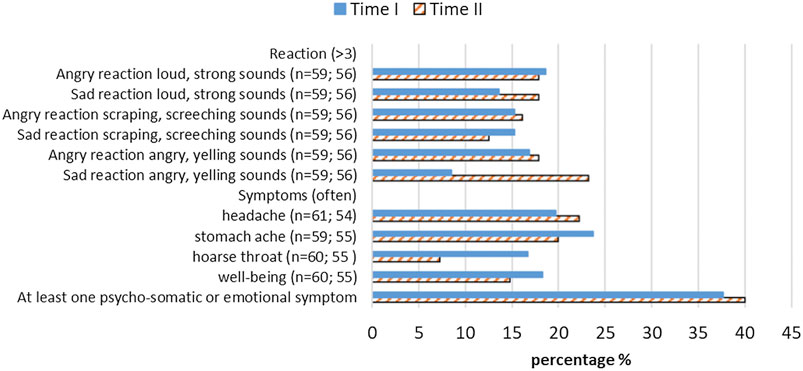
FIGURE 6. Prevalence of children’s angry or sad reactions of four or five on the scale and symptoms reported often. Blue bars denote before (time I) and orange bars with diagonal lines denote after (time II), the intervention.
The pattern of reactions to sounds seemed more ambiguous, with most reactions tending to be higher after the intervention (Figure 6). Conversely, most symptoms seemed to be slightly lower after the intervention, with hoarse voice having the largest prevalence reduction.
Results from the GEE logistic regression for all three models are given in Table 5. Model I included the change of stationary noise levels before and after measured in the meal/craft room, as levels in the play room were not found to be statistically significantly explanatory factors between time I and time II. Age and gender were not found to have a significant impact on any outcome.
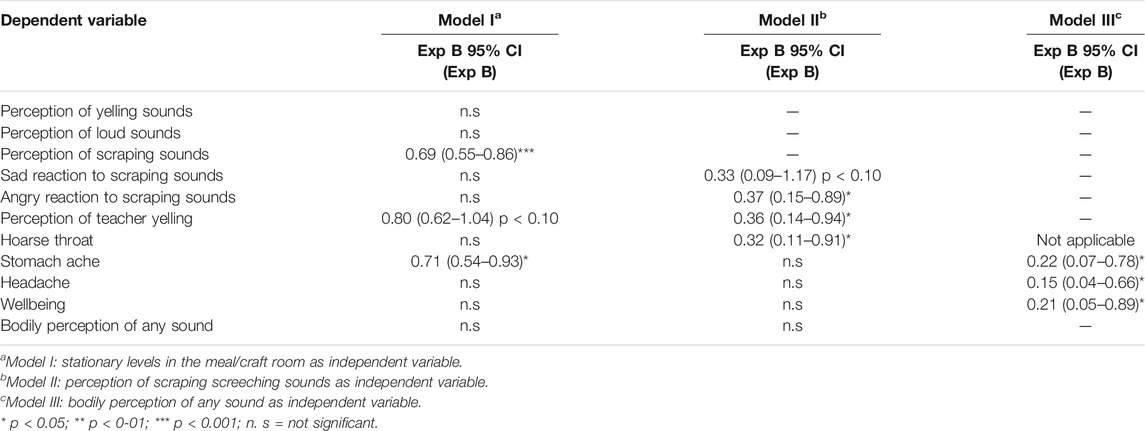
TABLE 5. Associations between the explanatory variables of measured or perceived noise exposure, provided by the three analytical models, and children’s perceptions, reactions, and bodily symptoms.
Model I showed that a change in noise levels in the meal/craft room was associated with a 31% reduction in children’s perception of scraping and screeching sounds with the odds being 0.69, and a near 30% reduction in the frequency of reported stomach ache (odds of 0.71). There was also a tendency toward a 20% reduction in children reporting occurrences of the teacher yelling or calling out with a raised voice, but this did not reach statistical significance (p = 0.093). The perceptions of the other sound characteristics were not significantly affected by the change of sound level. Model II showed that a reduction of the perception of scraping and screeching sounds per se was associated with a 63% reduction of reporting of anger in reaction to these sounds with the odds being 0.37, while differences in sad reactions did not reach statistical significance (p = 0.086). A reduced perception of scraping and screeching sounds was associated with a 64% reduction in children’s reporting teachers yelling or calling out with a raised voice, and a reduced perception of scraping and screeching sounds was associated with a 68% reduction in reporting a hoarse throat. Finally, Model III showed that a reduction in bodily perception of any sounds was associated with a large and significant reduction in the symptoms of stomach ache, headache, and increase in wellbeing, all in the range of 81–85%.
All measured rooms in the preschools had reverberation times in the order of 0.3–0.5 s before the intervention, and after the intervention the average reduction was in the order of 0.1 s. These measures are considered very low also before the intervention. The measurements showed the greatest reduction in the frequency range of 250–500 Hz for meal/craft room and in 250–500 and 2,000–4,000 Hz for play room, as seen in Supplementary Figures S3A, S4. The reduction in the frequency range 250–500 Hz was expected due to the configuration of suspended acoustic tiles with bass reinforcement. In one preschool the reverberation time increased after the intervention which is most likely due to how T20 is evaluated. The rooms in this preschool had broken decay curves which can occur when there are an uneven distribution of absorptive surfaces in one dimension. In this case it was most probably in the vertical plane due to the acoustic tiles in the ceiling (ISO 3382-2, 2008). The estimated standard deviation for T20 ranged from 0.001 to 0.009 s before the intervention for meal/craft room and from 0.001 to 0.008 s after. Values were in a similar range for play room. These values were obtained by using the described method in ISO 3382-1 on the averaged T20 results for each room type. The STI also improved slightly, increasing by around four to five percentage points, but as with the reverberation time the STI was already very good (more than 75%) before the interventions. (Larsson, 2011).
In addition to the reverberation time, an analysis of the rooms’ frequency responses were performed. The measured impulse responses were averaged for each room and compared before and after the intervention. The general observation was that the room responses became more flat after the intervention. Hence the signal was less affected (coloured) by the room. The frequency responses in the frequency range 250–4,000 Hz were averaged by room type and the results are shown in Supplementary Figures S5, S6. The area under each curve was calculated using the “trapz” function in matlab in order to compare the dynamic of the responses. The integral was computed with equal spacing with steps of 1 Hz. The frequency responses were normalised to the minimum sound pressure level within the chosen frequency range for each room type. For further clarification see Supplementary Material S2—Calculations of area under the curve.
The average ratio of the areas under the curves between time I and time II for the two rooms are seen in Table 6. The area decreased at time II for both meal/craft room and play room.
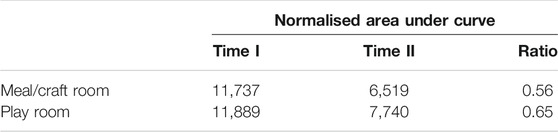
TABLE 6. Calculated ratio of area under the curve for averaged room frequency responses per room type.
Table 7 shows the C50 and D50 before and after the intervention. C50 and D50 showed an overall increase in the order of 3 dB and 5% which corresponds to 3 and 1 units of just noticeable difference (JND), respectively. However, the values before the interventions were C50 > 6 dB and D50 > 80% and it is not clear that a further increase of C50 and D50 in these rooms are beneficial or even perceivable. Centre time (Ts) was also evaluated and showed the same tendency as previously mentioned parameters. The measured Ts were in the range of 21–25 ms before and 15–17 ms after the interventions, hence the differences were then below JND and thereby most probably not perceivable. It can be noted that the values for Ts were considered to be very low also before the intervention meaning that the late energy in the impulse responses was attenuated.
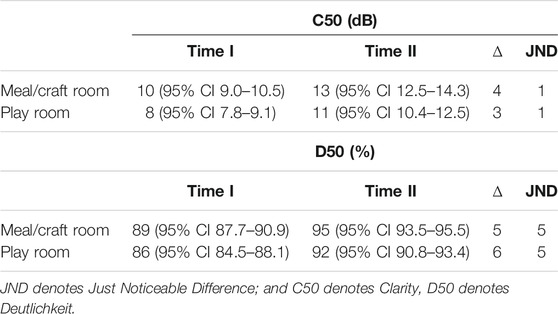
TABLE 7. Averaged values and 95%CI for C50 and D50 per room type.
The main finding of this study was a confirmed association between reduction of stationary noise levels after an acoustic intervention and a 30% reduction in children’s perceptions of scraping and screeching sounds along with a similar reduction in self-reported stomach ache. In addition, when using children’s perceptions of scraping and screeching sounds as predictor of the sound environmental change after the intervention, the change was associated with important oral communication outcomes, perception of teachers yelling and hoarse throat. Finally, when using the children’s bodily sensation of any sound as a predictor of the sound environment change after the intervention, the change was associated with psychosomatic symptoms and wellbeing. The reduction of the sound levels seen in the intervention preschools was not found in the reference schools. As we unfortunately could not interview the children in the reference preschools, our conclusions are hampered by the lack of control for factors other than the acoustic interventions that may have affected the children’s responses.
Given the very high sound equivalent and maximum levels that children were exposed to, as shown by the ample dosimeter measurements and stationary microphone measurements in the rooms, reductions of the indoor sound levels are highly needed. A reduction of the A-weighted equivalent noise level of 1–3 dB is not enough from a health perspective, but as it refers to a change of equivalent sound levels over one to 2 days per measurement point, it is clearly indicative. A change of up to 3 dB A-weighted equivalent level is also what can be expected with the fitting of absorbents to the ceiling.
The perceptual analyses, indicate that the interventions may to a lesser degree have affected perceived strength, but had a larger impact on perceptual qualities of the sound environment, that may be well less captured by the A-weighted equivalent sound level. The change in perceptual qualities could partly be explained by data showing that human neural processing of frequency develops at an earlier age than that of intensity (Sussman and Steinschneider, 2011), meaning that young children may be more attentive to changes in frequency characteristics than changes in intensity. It is also plausible that children more strongly direct their awareness toward (and hence are more likely to report on) sound characteristics that they perceived as most unpleasant. Scraping and screeching sounds were one unpleasant sound characteristics reported by children interviewed during the development of the INCH instrument (Dellve et al., 2013). Children typically described unease and bodily discomfort from sources such as the screeching sound of a swing or the scraping sounds of cutlery on plates. This observation was also confirmed in data obtained in German schools, where a relationship between binaural sharpness measured using a child’s artificial head and children’s reporting of sad reactions using INCH was indicated (Loh and Fels 2018). The amplification of high frequencies by small children’s HRTF (Fels 2008) would enhance the perception of these types of high-frequency sounds, to a level that may be perceived as unpleasant. The intervention, which included fitting dampening cushions on chairs and absorbent tiling on the walls and ceilings, could, in combination with the already fitted acoustically soft table top, be of high importance in reducing the direct high-frequency sounds that reach the child’s eardrum, however more studies are clearly needed to elucidate these matters.
The room acoustic interventions had the expected effect when studying the evaluated room acoustic parameters by room type. The measures were however considered to be good also before the interventions and thus the relative difference was small. The difference of C50 and D50 were close to or below JND in four out of six evaluated rooms and therefore, we cannot be certain that a change in acoustic quality was perceivable. Parameters such as C50 and D50 are greatly affected by the volume of the room due to more early reflections occurring because of the surfaces being closer to one another compared to a bigger room. It is not clear if these measures describe the perceived acoustic quality of small rooms from a child’s perspective and further investigations are needed. Finally, when comparing the evaluated parameters per room, one of the preschools showed the opposite behaviour with increasing T20 and decreasing C50 and D50. This can be explained by an uneven distribution of absorptive surfaces as well as less diffusive elements in the horizontal plane.
Unexpectedly, the reduction in A-weighted noise levels after the intervention were not found to be associated to a lower rating of the perception of loud, strong sounds. One explanation for this could be that the loudness curves on which the A-weighting is based were derived from adults (ISO 226:2003, 2003) and as the HRTFs and ear canal of small children amplify higher frequencies differently compared to an adult (Fels, 2008), the loudness relation to frequency may not be similar for children and adults. If this is confirmed in future studies it would mean that that the A-weighted levels may not fully represent how young children perceive loudness.
A reduced perception of yelling sounds from other children would also have been plausible. However, children’s yelling would mainly reach other children as direct sounds not well attenuated by the absorbent tiling placed on the ceiling or high up on the walls, where its main function would be to absorb reflected sounds. The lack of reduction of direct sounds was also shown by the lack of change in the dosimeter levels obtained for the staff and children before and after the intervention. An interesting finding was the tendency for the children to perceive the teacher as yelling or calling out less often after the intervention, a result also confirmed by a significant association in Model II. This suggests that the teachers experienced a higher acoustic speech comfort or were more aware of their noise-generating behaviour as a side-effect of the intervention, this could be of interest for future studies. The lack of an association between children’s yelling and the intervention may also be interpreted as a non-confirmation of a reverse Lombard effect, as the acoustic interventions would be expected to make children less prone to raise their voices. It is possible that children’s vocal effort would have benefited more if the absorbing tiles had been placed at child height, but this can currently only be speculated on, and needs to be furthered studied. Other studies investigating the effect of an acoustic intervention on vocal symptoms have focused on the teacher. For example alleviation of some vocal symptoms was reported among participating teachers and an improved perceived clarity and audibility of the teacher’s voice was reported by school aged children after an acoustic interventions in a classroom (Pirilä et al., 2020).
Although the change of the traditional room acoustic parameters was small, the shape of the room response curves showed a tendency of being flatter after the interventions. The implication of frequency balance of low and high frequencies has previously been studied in other contexts e.g. “spectral balance” with emphasis on the perceptual qualities of low frequency noise from ventilation systems (Beranek 1989) and in music studios (International Telecommunication Union 2015), but not in this context. It is plausible however, that the frequency balance of the room response may be of importance for the perceived acoustic quality in preschools rooms, as small children seem to be more susceptible to high frequency contents in the sounds. On the other hand, a low frequency dominance may also impair children’s language achievement as low frequency noise may mask frequencies important for speech communication (Pickett 1959). Though these studies have to the authors knowledge, not been performed within a child population. Taken together it seems as if a balanced or flattening of the room response curve would be advantageous also in a preschool environment, however this needs to be further studied.
The association between a lower perception of scraping, screeching sounds and a 70% reduction in children reporting a hoarse throat, as well as a similar reduction in being angry when hearing scraping and screeching sounds was seen in Model II. These findings could indicate an improved acoustic environment, where children have less need to raise their voice in order to be heard. This would be a very significant achievement, as using vocal behaviour to “be heard” was the main category reported by preschool teachers when describing how preschool noise affected children (Persson Waye et al., 2019). This category included more than 7,000 occurrences of words with the same meaning as “to be heard.” The category in second place, which described children being distracted, included only 2,600 word counts.
The hypothesis of a reduction of scraping and screeching sounds being indicative of improved acoustic comfort is in line with the reduced occurrence of stomach ache found with the reduction of sound levels after the intervention. It is known from other areas of research that gastrointestinal organs are particularly sensitive to stress, especially in children (Ricour, 1989). Stomach ache, headache, and tiredness are reported as frequent causes of psychosomatic complaints in children (Silber and Pao, 2003), and a large study indicated that childhood stress may trigger psychosomatic and emotional symptoms (Vanaelst et al., 2012). The latter study collected parental reports on more than 4,000 children from eight European countries on headaches, stomach aches, sickness, and low emotional wellbeing, and related this to childhood adversity in a broad sense. The prevalence of frequent occurrence of at least one such psychosomatic and emotional symptom was broken down by age group, and it is interesting to note that the prevalence for 4-year-olds and 5-year-olds were 38.4 and 39.3%, respectively; remarkably similar to the percentages of 38 and 40% at times I and II in our study. It should be noted that our sample size was very small and hence prone to random errors, and that “sickness” was not included in our study. This again raises the need for further studies.
The findings from Model III showed a strong association between bodily perception and the psychosomatic symptoms of headache, stomach ache, and effects on wellbeing; a reduction of bodily perception was associated with around 80% reduction of symptoms. A previous qualitative study (Dellve et al., 2013) found that children perceive sounds and noise physically and within their body, and so it was important to include bodily perception in this study as a complement to auditory perception. Reducing psychosomatic symptoms would be a substantial achievement, as the prevalence of psychosomatic symptoms is greatly increasing among young children and adolescents (Luntamo et al., 2012; Vanaelst et al., 2012). Although noise is only one factor that may contribute to psychosomatic symptoms, it is a highly prevalent stressor for a large population of preschool-age children, both in Sweden and in other countries, and may therefore warrant concern.
Achieving an acoustic environment that reduces auditory and bodily discomfort is important not just from a wellbeing and health perspective but also for language acquisition and learning, as children tend to cope with aversive noise by ignoring or disregarding auditory inputs (Evans, 2006; Evans and Hygge, 2007). An unfortunate consequence of this is that important speech signals are also tuned out, which may result in impaired writing and reading abilities. Non-native language speaking children and children with language disorder and hearing impairments are at particular risk in such settings.
Achieving an acoustic environment that reduces auditory and bodily discomfort as well as supports language acquisition and learning is of major importance for children in the preschool environment. To reach this goal we need to know more on how small children perceive and react to sounds and noise in their environment. This study provided for the first time data on how children perceptually may perceive and react to a change of the sound environment and acoustic qualities resulting from an acoustic intervention. Furthermore, we were able to gather children’s response using a questionnaire derived from children’s own wording. It points to the importance of acoustical qualities that may not be included in today’s standards of room acoustics and suggests that a revision of standards for preschools need to take as a point of departure small children’s hearing, perception and reaction, paying attention to factors such as direct sounds from, i.e., friction between surfaces. Future studies should aim to include a larger sample of children, use a child perspective approach and perform a systematic evaluation of which room acoustics and sound qualities that are supportive of children’s health and wellbeing.
An important limitation is the lack of interviews with the children from the reference preschools, where only measurements of noise levels were carried out. This makes our conclusions open to the influence of factors other than the acoustic interventions that may have affected the children’s responses to the intervention at the preschools. The room acoustic measurements were only performed in three preschools to control that the intervention had the expected effect and we can therefore not make direct analyses of possible associations between the change of room acoustics and children response. A possible limitation for generalisability to today’s situation could be that the study was performed between 2006 and 2009, and hence it is possible that the preschool environment has changed to the better. Unfortunately, there are little indications of a positive change of the sound environment as the Swedish National Agency for Education report that the number of children per group and the number of children per personnel is largely the same today, while the proportion of preschool teachers with a university degree has even decreased with about 3 percentage units. Furthermore, the follow up study performed among the preschool teachers in 2013–2014 indicated large problems with noise and similar reactions among the children (Persson Waye et al., 2019).
Another limitation is that Models II and III used self-report for the dependent and independent variables, hence including the possibility of information bias. However, this is currently unavoidable when investigating perceptual qualities from a child’s perspective. Using only the measured values (A-weighted sound pressure levels) as independent variable may bias the results as the weighting is based on loudness estimations and derived from adult perceptions. However, as Model I, with the objective measures as independent variable, showed a relationship with children’s perceptions of scraping screeching sounds, it gave a basis for the use of children’s perceptions of these sound qualities as an independent variable in Model II. The INCH questionnaire has been validated and the similar reporting of prevalence of perceptions, reactions, symptoms, and wellbeing on the two occasions gives credibility to the instrument. A strength is that the questionnaire was constructed from focus group interviews and so the questions posed to the children were worded in their own “language.”
The datasets presented in this article are not readily available because ethics do not allow redistribution of data of the children, however acoustic data can be shared. Requests to access the datasets should be directed to kerstin.persson.waye@amm.gu.se.
The studies involving human participants were reviewed and approved by Gothenburg (ref: 670-06). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
KPW aquired the funding, designed the study and supervised the work and carried out the main analyses of the intervention study. She drafted the article and revised. She also carried out part of the field work. JK reanalysed the room acoustic data and took part in the revision of the article.
The study was funded by Swedish national research funds FAS/Forte (Swedish research council for health working life and welfare), and 2008-0901 and FORMAS (Swedish Research Council for sustainable development) 2005-1153.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author would like to thank Agneta Agge for valuable help in performing the field studies; the Mölndal city employees who collaborated in this work; the children, parents, and staff at the preschools; and Assistant Professor Jeong Lim Kim and Assistant Professor Laith Hussain-Alkhateeb for their statistical guidance. The study was funded by FAS 2008-0901 and FORMAS 2005-1153.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fbuil.2021.688836/full#supplementary-material
AFS 2005: 16 (2005). Noise (In Swedish) the Swedish Work Environment Authority - Code of Statue. Solna. Available at: https://www.av.se/globalassets/filer/publikationer/foreskrifter/buller-foreskrifter-afs2005-16.pdf (Accessed February 12, 2020).
Astolfi, A., Puglisi, G. E., Murgia, S., Minelli, G., Pellerey, F., Prato, A., et al. (2019). Influence of Classroom Acoustics on Noise Disturbance and Well-Being for First Graders. Front. Psychol. 10, 2736. doi:10.3389/fpsyg.2019.02736
Beranek, L. L. (1989). Balanced Noise‐criterion (NCB) Curves. The J. Acoust. Soc. America 86, 650–664. doi:10.1121/1.398243
Clark, C., and Paunovic, K. (2018). WHO Environmental Noise Guidelines for the European Region: a Systematic Review on Environmental Noise and Quality of Life, Wellbeing and Mental Health. Ijerph 15, 2400. doi:10.3390/ijerph15112400
Dellve, L., Samuelsson, L., and Persson Waye, K. (2013). Preschool Children's Experience and Understanding of Their Soundscape. Qual. Res. Psychol. 10, 1–13. doi:10.1080/14780887.2011.586099
Dockrell, J. E., and Shield, B. M. (2006). Acoustical Barriers in Classrooms: the Impact of Noise on Performance in the Classroom. Br. Educ. Res. J. 32, 509–525. doi:10.1080/01411920600635494
Evans, G., and Hygge, S. (2007). in Noise and Cognitive Performance in Children and Adults. Editors Luxon, L. M., and Prasher, D. (Chichester: Hoboken, NJ: Wiley).
Evans, G. W. (2006). Child Development and the Physical Environment. Annu. Rev. Psychol. 57, 423–451. doi:10.1146/annurev.psych.57.102904.190057
Eysel-Gosepath, K., Pape, H. G., Erren, T., Thinschmidt, M., Lehmacher, W., and Piekarski, C. (2010). Lärm in Kindertagesstätten. HNO 58, 1013–1020. doi:10.1007/s00106-010-2121-y
Fels, J. (2008). From Children to Adults: How Binaural Cues and Ear Canal Impedances Grow. Phd dissertation. Logos Verlag Berlin GmbH: RWTH Aache. doi:10.1145/1400468.1400522
Gokdogan, O., and Gokdogan, C. (2016). Determination of the Level of Noise in Nurseries and Pre-schools and the Teachers′ Level of Annoyance. Noise Health 18, 256–259. doi:10.4103/1463-1741.192475
IEC 60268-16 (2011). Sound System Equipment – Part 16: Objective Rating of Speech Intelligibility by Speech Transmission index. Geneva, Switzerland: International Electrotechnical Commission.
ISO 226 2003 (2003). Acoustics — normal Equal-Loudness-Level Contours. Stockholm, Sweden: ISO (The International Organization for Standardization.
ISO 3382-1 (2009). Acoustics – Measurement of Room Acoustic Parameters – Part 1: Performance Spaces. Stockholm, Sweden: ISO (The International Organization for Standardization).
ISO 3382-2 (2008). Acoustics — Measurement of Room Acoustic Parameters — Part 2: Reverberation Time in Ordinary Rooms. Stockholm, Sweden: ISO (The International Organization for Standardization.
International Telecommunication Union (2015). Recommendation ITU-R BS. 1116-3: Methods for the Subjective Assessment of Small Impairments in Audio Systems. Geneva, Switzerland: International Telecommunication Union.
Jonsdottir, V., Rantala, L., Oskarsson, G., and Sala, E. (2015). Effects of Pedagogical Ideology on the Perceived Loudness and Noise Levels in Preschools. Noise Health 17, 282–293. doi:10.4103/1463-1741.165044
Klatte, M., Hellbrück, J., Seidel, J., and Leistner, P. (2010). Effects of Classroom Acoustics on Performance and Well-Being in Elementary School Children: a Field Study. Environ. Behav. 42, 659–692. doi:10.1177/0013916509336813
Kuhl, P. K. (2010). Brain Mechanisms in Early Language Acquisition. Neuron 67, 713–727. doi:10.1016/j.neuron.2010.08.038
Lane, H., and Tranel, B. (1971). The Lombard Sign and the Role of Hearing in Speech. J. Speech Hearing Res. 14, 677–709. doi:10.1044/jshr.1404.677
Larsson, P. (2011). God Ljudmiljö I Förskola - Beskrivning Av Rumsakustik Före Och Efter Åtgärdsprogram. Gothenburg: Enheten för Arbet-soch miljömedicin, Avdelningen för Samhällsmedicin och Folkhälsa, Sahlgrenska Akademin vid Göteborgs universitet. Available at: http://hdl.handle.net/2077/35768 (Accessed February 12, 2020)
Lindstrom, F., Ohlsson, A.-C., Sjöholm, J., and Persson Waye, K. (20102010). Mean F0 Values Obtained through Standard Phrase Pronunciation Compared with Values Obtained from the normal Work Environment: a Study on Teacher and Child Voices Performed in a Preschool Environment. J. Voice 24 (3), 319–323. doi:10.1016/j.jvoice.2008.10.006
Loh, K., and Fels, J. (2018). Binaural Psychoacoustic Parameters Describing Noise Perception of Children in Comparison to Adults. Hersonissos, Crete, Greece: Euronoise
Luntamo, T., Sourander, A., Santalahti, P., Aromaa, M., and Helenius, H. (2012). Prevalence Changes of Pain, Sleep Problems and Fatigue Among 8-Year-Old Children: Years 1989, 1999, and 2005*. J. Pediatr. Psychol. 37, 307–318. doi:10.1093/jpepsy/jsr091
Maxwell, L. E., and Evans, G. W. (2000). The Effects of Noise on Pre-school Children's Pre-reading Skills. J. Environ. Psychol. 20, 91–97. doi:10.1006/jevp.1999.0144
Neuman, A. C., Wroblewski, M., Hajicek, J., and Rubinstein, A. (2010). Combined Effects of Noise and Reverberation on Speech Recognition Performance of Normal-Hearing Children and Adults. Ear & Hearing 31, 336–344. doi:10.1097/AUD.0b013e3181d3d514
Nordtest Method NT ACOU 115 (2003). Measurement of Occupational Noise Exposure of Workers: Part II: Engineering Method, 19.
Persson Waye, K., Agge, A., Lindström, F., and Hult, M. (2011). God Ljudmiljö I Förskola - Samband Mellan Ljudmiljö, Hälsa Och Välbefinnande Före Och Efter Åtgärdsprogram. Gothenburg: Enheten för Arbetsoch miljömedicin, Avdelningen för Samhällsmedicin och Folkhälsa, Sahlgrenska Akademin vid Göteborgs universitet. Available at: http://hdl.handle.net/2077/35765 (Accessed February 12, 2020).
Persson Waye, K., Fredriksson, S., Hussain-Alkhateeb, L., Gustafsson, J., and van Kamp, I. (2019). Preschool Teachers' Perspective on How High Noise Levels at Preschool Affect Children's Behavior. PLoS ONE 14, e0214464. doi:10.1371/journal.pone.0214464
Persson Waye, K., Van Kamp, I., and Dellve, L. (2013). Validation of a Questionnaire Measuring Preschool Children's Reactions to and Coping with Noise in a Repeated Measurement Design. BMJ Open 3, e002408. doi:10.1136/bmjopen-2012-002408
Pickett, J. M. (1959). Low‐Frequency Noise and Methods for Calculating Speech Intelligibility. J. Acoust. Soc. America 31 (9), 1259–1263. doi:10.1121/1.1907855
Pirilä, S., Jokitulppo, J., Niemitalo-Haapola, E., Yliherva, A., and Rantala, L. (2020). Teachers' and Children's Experiences after an Acoustic Intervention and a Noise-Controlling Workshop in Two Elementary Classrooms. Folia Phoniatr Logop 72, 454–463. doi:10.1159/000503231
Ricour, C. (1989). Stress-induced Disturbances of the Gastro-Intestinal Tract in Children. Intensive Care Med. 15, S32–S36. doi:10.1007/BF00260881
Silber, T. J., and Pao, M. (2003). Somatization Disorders in Children and Adolescents. Pediatr. Rev. 24, 255–264. doi:10.1542/pir.24-8-255
Sjödin, F., Kjellberg, A., Knutsson, A., Landström, U., and Lindberg, L. (2012). Noise Exposure and Auditory Effects on Preschool Personnel. Noise Health 14, 72. doi:10.4103/1463-1741.95135
SS 25268 2007+T1 (2017). Acoustics – Sound Classification of Spaces in Buildings – Institutional Premises, Rooms for Education, Preschools and Leisure-Time Centres, Rooms for Office Work and Hotels. Stockholm, Sweden: SIS – Swedish Standards Institute. Available at: www.sis.se (Accessed January 15, 2020).
Sussman, E. S., and Steinschneider, M. (2011). Attention Modifies Sound Level Detection in Young Children. Dev. Cogn. Neurosci. 1, 351–360. doi:10.1016/j.dcn.2011.01.003
Tamburlini, G., Ehrenstein, O. S. V., and Bertollini, R. (2002). Children’s Health and Environment: A Review of Evidence. Copenhagen/Rome: European Environment Agency.
Vanaelst, B., De Vriendt, T., Ahrens, W., Bammann, K., Hadjigeorgiou, C., Konstabel, K., et al. (2012). Prevalence of Psychosomatic and Emotional Symptoms in European School-Aged Children and its Relationship with Childhood Adversities: Results from the IDEFICS Study. Eur. Child. Adolesc. Psychiatry 21, 253–265. doi:10.1007/s00787-012-0258-9
Keywords: acoustic intervention, child, perception, reaction, psychosomatic symptoms, INCH questionnaire, noise, high frequency sounds
Citation: Persson Waye K and Karlberg J (2021) Sound Quality Characteristics of Importance for Preschool Children’s Perception and Wellbeing After an Acoustic Intervention. Front. Built Environ. 7:688836. doi: 10.3389/fbuil.2021.688836
Received: 31 March 2021; Accepted: 26 May 2021;
Published: 14 June 2021.
Edited by:
Jian Kang, University College London, United KingdomCopyright © 2021 Persson Waye and Karlberg. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kerstin Persson Waye, S2Vyc3Rpbi5wZXJzc29uLndheWVAYW1tLmd1LnNl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.