
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Built Environ. , 28 January 2022
Sec. Construction Management
Volume 7 - 2021 | https://doi.org/10.3389/fbuil.2021.644104
This article is part of the Research Topic Managerial Responses against COVID-19 View all 7 articles
 Hadi Sarvari1,2*
Hadi Sarvari1,2* Zhen Chen3
Zhen Chen3 Daniel W. M. Chan2
Daniel W. M. Chan2 Ellyn A. Lester4
Ellyn A. Lester4 Nordin Yahaya5
Nordin Yahaya5 Hala Nassereddine6
Hala Nassereddine6 Aynaz Lotfata7
Aynaz Lotfata7Facilities management along with health care are two important aspects in controlling the spread of infectious diseases with regard to controlling the outbreak of global COVID-19 pandemic. Hence, with the increasing outbreak of COVID-19 pandemic, the importance of examining the relationship between the built environment and the outbreak of infectious diseases has become more significant. The aim of the research described in this article is to develop effective infection control and mitigation measures to prevent the transmission of COVID-19 pandemic in the built environment. This study seeks to answer the question of how the facilities management industry can help reduce the transmission of coronavirus. For this purpose, an online survey questionnaire was distributed internationally from 8 April to 25 July, 2020 to collect data from various key stakeholders. The collected data were analyzed by SPSS software. Various methods for the prevention and control of infectious diseases transmission are evaluated through this questionnaire-based survey with regard to their effectiveness for the healthy and safe built environment. These methods were categorized into three groups, including training protocols, operation and maintenance, and design and construction. The results show that all suggested methods have a positive effect on all types of buildings. These methods have an equal effect on low-risk buildings, while for high and very high-risk buildings, training protocols and design and construction measures have the greatest impact. In addition, training protocols and the measures in operation and maintenance will have the greatest effect on medium-risk buildings. The results can help in more rational decision making in relation to controlling the outbreak of COVID-19 pandemic in all types of buildings.
Sustainable development is a new emerging concept and process in major governments’ policies which plays a key role in the human social development (Rahdari et al., 2016; Sarvari et al., 2019; Pirouz et al., 2020). In general, Sustainable development often combines social, economic, and environmental goals in political decision-making (Sarvari et al., 2020). The main aim of sustainable development is the improvement of all aspects of life for the current generation without sacrificing the quality of life of future generations. While creating sustainability might appear simple in theory, of the actual sustainable development process includes numerous unforeseen problems and barriers which slow its progress (Pirouz et al., 2020). Emergence of epidemic diseases is one such unforeseen problem with a negative impact not only on the economy but also on social problems; which are both fundamental parts of sustainable development. Although such problems can be temporary and transient, they can potentially disrupt the ongoing processes, resulting in adverse effects for many years (Filho et al., 2020; Shen et al., 2020; Yu et al., 2020).
One of the most serious challenges faced by governments in the current world if the COVID-19 pandemic and lack of sufficient research regarding this problem (Pirouz et al., 2020). Same other industries, COVID-19 is having a huge impact on the construction industry. It is expected as the COVID-19 situation evolves, other problems also are appearing. While COVID-19 does not generally prevents the completion of projects, it can slow the process, resulting in delays and disruption, due to severe disruption of supply chains among other reasons. It has resulted in temporary halt in many projects, often with the intention of restarting the work at a later date. The situation is evolving, with specific orders to close construction sites or authorize contractors to suspend works and extend deadlines until the end of the state of emergency in some countries.
Health and safety risks of COVID-19 can vary for each project. For instance, people who work outdoors without physical proximity to others may be able to comply with the new health and safety guidelines while those working in an enclosed environment might face various difficulties. However, in all cases, health and safety risk assessments must be performed based on medical and scientific guidelines when the work continues, as part of contractors’ duty of providing a safe working environment. Given the restrictions of comfort requirements in the interior of a building, it is obvious that the problem of safety is a multidimensional one (Dounis and Caraiscos, 2009).
With the importance of healthcare information for controlling COVID-19 pandemic and protecting vulnerable populations, one identified area with a key role in this matter is that of property/facilities management. The interdependent relation between health and the built environment has become increasingly evident with the spread of COVID-19 (Pinheiro and Luís, 2020). Buildings which use procedures and administrative controls for safe and proper building to reduce the duration, frequency, or intensity of exposure to a hazard are known as safe building environments. Safe work practices in this case include provision of resources and work environment in order to promote hygiene (Gwenzi, 2020), or posting signs in buildings (OSHA, 2020). Although much is still unknown when it comes to this new pandemic, there are immediate preventive steps that can be taken across the property management industry to reduce the risk of infection.
From the above and as initially stated, the present study aims to discover effective control and mitigation measures to prevent the transmission of COVID-19 in the built environment. For this purpose, an international survey questionnaire was conducted between the months of April July 2020 to collect data. The data collection questionnaire was created using library and field methods based on the literature review as well as expert interviews for the identification stage of effective control and mitigation measures. In fact, this study seeks to answer the question of how the property management industry can help reduce the transmission of coronavirus. The statistical population of the study included a wide range of Architecture, Engineering, Construction and Operation (AECO) experts. The collected data were analyzed by SPSS software. Various methods for the prevention and control of infectious diseases transmission are evaluated. The results show that all methods have a positive effect in all types of buildings. Findings from the described research can make a useful contribution to fill the knowledge gap in the context of technical responses against infections at workplaces. These results will help decision-makers to make more rational decisions in relation to controlling the outbreak of COVID-19 in all types of buildings.
Since the outbreak of COVID-19, many studies have been conducted to control and respond to the epidemic. In one study, the researcher demonstrated ten steps all workplaces can take to reduce risk of exposure to coronavirus (OSHA, 2020). Methods used for isolating individuals from possible work-related hazards are known Engineering controls. These controls, when used appropriately, reduce exposure to hazards regardless of individual behavior and are often the most cost-effective solution. Engineering controls suitable for SARS-CoV-2 pandemic can include installation of high-efficiency air filters, higher ventilation rates for indoor areas, installation of physical barriers such as clear plastic guards, using drive-through windows for customer service, and use of specialized negative-pressure ventilation for areas with high aerosol generation (e.g., airborne infection isolation rooms in healthcare settings and specialized autopsy suites in mortuary settings) (OSHA, 2020). In another study, Li et al. (2020) estimated the trend of the COVID-19 outbreak in China. The results of their study show that rapid and dynamic strategies in the area of facilities management can be useful in diminishing and constraining the current crisis.
The risk of exposure to SARS-CoV-2, and COVID-19 disease, during an outbreak varies from very high to high, medium, or lower (caution) risks (OSHA, 2020). Furthermore, the effect of temperature on virus spread and survival varies in different studies. Some studies have investigated the effects of environmental parameters on spread of epidemic diseases. In some cases, cold and dry environments were introduced as important factors for the spread of the virus (Mecenas et al., 2020). Wang et al. (2020) suggested the adoption of strictest social control measures in colder regions of the world due to significant effect of low temperatures on viability, transmission rate and survival rates of coronaviruses. In addition, many of recent researches show the effect of temperature on the Coronavirose transmission rate (Lowen et al., 2007; Price et al., 2019). Researchers believe that COVID-19 is less likely to spread in warmer climates (Mecenas et al., 2020). However, the epidemic of the coronavirus known as MERS-CoV, was between April and August, indicating quick spread of the virus in warm temperature, low wind speeds, low relative humidity, and high ultraviolet index (Altamimi and Ahmed, 2020).
In their review, Luongo et al. (2016) assessed epidemiologic studies published after 2000 found at least one HVAC-related parameter affecting infectious disease outcomes in buildings. Their results indicated that HVAC system might play a role in airborne pathogen transmission, but that more robust, interventional studies are needed.
Guo et al. (2020) used real-time PCR to test surface and air (including air outlets) samples from an ICU and general COVID-19 ward at Huoshenshan Hospital in Wuhan, China for SARS-CoV-2 presence [d]. In total, thirty-five percent of samples (14 out of 40 samples) from the ICU and 12.5% (2 out of 16) of samples obtained from the general ward were tested positive. Swab samples obtained from air outlets also tested positive with the rates of 66.7% (8 out of 12) for ICUs and 8.3% (1 out of 12) for general ward samples. The positive rate differed based on the sampling site with 44.4% (8 out of 18) positive results in samples obtained from patients’ rooms, 35.7% (5 out of 14) in samples obtained near air outlets and 12.5% (1 out of 8) for samples from doctors’ office area. These results indicated that aerosols containing virus samples were mainly found near and downstream from the patients; with maximum transmission distance of 4 m. Air sampling in the general ward was carried out in different areas around patients, in the corridor leading to patients’ rooms and under air inlets. Only air samples obtained from around the patients were tested positive. These results lead to the conclusion that SARS-CoV-2 can be widely distributed in the air and on surfaces but not through HVAC systems (Alberta Health Services, 2020; Guo et al., 2020). Both this and the study by Liu et al. (2020) were limited due to lack of viable virus testing. Furthermore, the relation between environmental contamination with viral RNA and clinical infection is still unclear (Alberta Health Services, 2020; Liu et al., 2020).
In the study by Ong et al. (2020), samples were collected from surfaces at 26 different sites in three airborne infection isolation rooms (12 air exchanges per hour) which included anterooms and bathrooms used for SARS-CoV-2 patients in outbreak center in Singapore between January 24 and February 4, 2020. The results indicated extensive environmental contamination originating from SARS-CoV-2 patient with mild upper respiratory tract involvement. Samples obtained from toilet bowl and sink were also tested positive. These results suggested that viral shedding in stool can be considered as a possible transmission route. The results of samples obtained after cleaning samples were negative which indicated the adequacy of current decontamination measures. Despite the extent of environmental contamination, the test results for air samples were negative. On the other hand, two out of the three air exhaust outlet samples were positive. This indicated that small droplets contaminated with virus may be displaced by airflows and deposited on equipment such as vents. The final conclusion indicated that environment is a potential medium for transmission indicating the need for strict environmental and hand hygiene procedures. However, this study used no viral culture in order to demonstrate viability, while also using inconsistent methodology and small sample size which could be among its limitations (Alberta Health Services, 2020; Ong et al., 2020).
Santarpia et al. (2020) in their study, monitored and cared for 13 confirmed cases of SARS-CoV-2 infections in the care of University of Nebraska Medical Center and its clinical partner Nebraska Medicine, [g]. The patients requiring hospital care were monitored in the Nebraska Biocontainment Unit (NBU) while National Quarantine Unit (NQU) was used for isolation of asymptomatic or mildly ill patients. All rooms included private bathrooms and used negative pressure setting. Samples were obtained from high volume air samples and low volume personal air samples in two NBU and nine NQU rooms with positive SARS-CoV-2 infection patients. Sampled surfaces included ventilation grates, tabletops and window ledges. Air samples were also collected from patients’ rooms. RT-PCR method was used to analyze surface and aerosol samples. The results indicated that from 163 collected samples, 77.3% tested positive for SARS-CoV-2. Viral gene copy concentrations recovered from samples were generally low and highly variable, in the range of 0–1.75 copies/µL. The highest viral concentration was observed in air handling grate of the NBU. Air samples tested positive RT-PCR demonstrated no viral propagation or viral replication during relevant tests. One matter of note was the presence of viral RNA on the floor under the bed and on the window ledges which suggests the role of airflow. In the NBU suite, airflow inlet is located at the top center of the room while the outlets are on either side of the room in grates near the head of the patient’s bed. The results of airflow modelling indicated turbulent eddies forming under the patient’s bed causing contamination under the bed, while particles are carried away from the patient and toward the edges of the room through the dominant airflow, which is the possible cause for particles deposited by the windows. However, this study lacked aerodynamic or computational modeling necessary for supporting this hypothesis (Alberta Health Services, 2020; Santarpia et al., 2020).
Building services maintenance solely based on individual experiences of engineers often leads to unsatisfactory results. This approach can pose a high risk in building services availability while also leading to poor maintenance. This means that risk assessment and management must be carried out before full implementation of a design. Despite this fact, the use of prediction theories and tools (e.g., reliability evaluation of engineering systems) is not prevalent in the building services industry (Lam, 2006).
The preliminary literature review indicated that there was a lack of systemic study on the methodology of active COVID-19 response in the built environment. It was therefore the reason to conduct a worldwide questionnaire based survey, which is described in this paper, so as to make a contribution to building capability, which has been being led by professional bodies such as IFMA (2020), against the COVID-19 attack at workplaces. The research described in this paper aims to identify major prevention and mitigation measures that can be adopted in facilities management to effectively combat against the transmission of COVID-19 in buildings. It is expected that this paper can be useful to inform professional practice on facilities management with an international perspective derived in 2020.
Facilities management along with health care are very important in controlling the spread and outbreak of COVID-19. With the increasing outbreak of COVID-19, the importance of examining the relationship between the built environment and the outbreak of this disease has also increased. There are immediate preventive measures in the real estate industry that can be taken to control the risk of infection, although the behavior of the virus has changed over time. The aim of this study was to discover effective control and mitigation measures to prevent the transmission of COVID-19 in the built environment. For this purpose, the online survey questionnaire was reviewed internationally from 8 April to 25 July, 2020 to collect data (Sarvari et al., 2020). This method of data collection, in addition to allowing the comparison of prevention and control methods at the international level, can be helpful in classifying ideas for built environments and presenting new ideas. In fact, this study seeks to answer the question of how the property management industry can help reduce the transmission of coronavirus. Therefore, this review is internationally designed.
According to Appendix1, the questionnaire consists of two sections. The first section is about the personal particulars. The second section of the questionnaire consists of three main sub-sections with each sub-sections divided into three parts. These three parts are asked about 20 major prevention or mitigation measures for buildings at risk of exposure. The first part was consist of four training protocols, including (i) Identifying the sources of COVID-19 that people might be exposed in buildings: where, how, and to what; (ii) Establishing building specific hygiene and cleanliness protocols for design, construction and, operation; (iii) Providing effective guidance and/or trainings against the risk of coronavirus; (iv) Installation of post educational hygiene signage in buildings (handwashing signage, etc.). In addition, the second part was consist of four measures in operation and maintenance, including (i) Maintaining the optimum temperatures inside the building; (ii) Maintaining the optimum levels of humidity inside the building; (iii) Maintaining the optimum levels of natural and artificial lighting inside the building; (iv) Maintaining the optimum natural and mechanical ventilations inside buildings. Moreover, the third part was consist of 12 Measures in design and construction, including (i) Maintaining flexible policies that permit people to work from home (Establishing the policy on flexible working to reinforce business continuity, and workforce productivity). (ii) Adopting social distancing principles in process reengineering and workplace design; (iii) Announcing dynamic data and information about environmental situations for building occupancy; (iv) Providing relevant personal protective equipment (PPE) and cabinets according to scenario based calculations in building operation; (v) Proving separated rooms for pets; and (vi) Incorporating regular sterilization in design considerations and Service Level Agreement (SLA). (vii) Providing special access and spaces for vulnerable people; (viii) Adopting advanced techniques, materials and equipment for cleaning, gardening and wastes collection; (ix) Using antimicrobial materials for surfaces design and maintenance; (x) Adopting compulsory body temperature check at the entrance of buildings; (xi) Using smart sterilizer sensors at the entrance of buildings; (xii) Using automatic doors for buildings. Each sub-section of the second section of the questionnaire was dedicated to a specific type of buildings. The first sub-section was about low-risk buildings (i.e. Hotels and boarding houses, and Residential apartments), the second sub-section was about medium-risk buildings (i.e. Leisure centers, Shopping centers, Mosques and Churches and other religious centers, Office buildings, Restaurants, Transport facilities (Stations and Terminals), Universities and colleges, Schools, Workplaces and Community Locations, Urban public buildings (Libraries, Museums and Cinemas, etc.), and Low traffic workplaces), and the third sub-section was about high and very high-risk buildings (i.e. Business centers (Conference and Exhibition centers), Hospitals, Laboratories and Healthcare Facilities, and Industrial centers and large factories).
It should be noted that the validity of the questionnaire was confirmed through content validity. In addition, the reliability of the questionnaire was assessed using Cronbach’s α which is a criterion used to confirm the internal reliability of observed variables in each construct that must exceed 0.7 for suitable reliability (Cronbach and Meehl, 1955). The reliability of the questionnaire in selecting 10% of the total sample size to be collected was 0.967, which is greater than 0.7. The questionnaire shows strong reliability and as a result it will be possible to repeat this research and compare the results in the coming years. Reliability results of different sections of the questionnaire which obtained using the SPSS software are given in Table 1.

TABLE 1. Reliability table by different sections of the questionnaire.
Based on Table 1, it can be seen that the reliability value is higher than 0.7 and is therefore acceptable, although the reliability of the building specific workplace flexibilities, protections, and controls sub-section is higher than the business-oriented basic infection prevention measures sub-section in all building conditions.
It looks the statistical population of the study included a wide range of AECO experts. Sampling method in this study is random sampling selection from a list of people who were known around the world and worked in this field academically or practically. Due to the difficulty of collecting information, reminder messages and calls were made during the regular collection period. Due to the uncertainty of the population size of the study and Zarif Sagheb et al. (2020) suggestion, Krejcie and Morgan’s table was applied to determine sample size. Krejcie & Morgan (1970) introduced a table to determine sample size. According to this table, the sample size was estimated to be 384, and data collection was stopped when the sample size approached this amount.
In fact, this study examines the hypothesis that the effect of the method of coping with this disease will be different in different types of buildings. In order to test this hypothesis, repeated measures analysis method and SPSS software were used. As shown in Figure 1, for this purpose, three types of coping methods which have been extracted from the research questions using exploratory factor analysis method were selected which included training protocols (group 1), measures in operation and maintenance (group 2) and measures in design and construction (group 3). According to the OSHA (2020), buildings are also classified into three categories: low-risk (type 1), medium-risk (type 2) and high and very high-risk (type 3). In this research, methods are considered as intra-subject factors because they can be used in all three types of buildings and buildings are considered as inter-subject factors because they are different in nature.
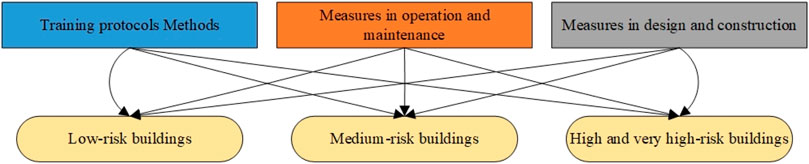
FIGURE 1. The hypothetical model for consideration in this study.
As can be seen in Figure 1, it must first be determined whether these methods are effective in each type of building, and then it must be determined which method is the most effective in which building in order to make the necessary planning.
In the next section, first the descriptive analysis of the data is performed during the first two steps and then the extraction of inferential results and comparison between buildings in the final two steps is carried out. In fact, the present analysis of this research includes four steps, which are described below.
The results of this research, as it is clear from the research steps, will be in four steps. The first two steps are descriptive, with the first step examining demographic factors and the second step examining research questions. For the other two steps, one examines the results of the hypothesis being tested and the other presents the final conclusion of the work. The research steps are followed by a case study.
This step is used to evaluate the participants in the sample and to examine the similarity of its demographic factors with the community. Table 2 shows the Details of the people participating in the sample. As can be seen in Table 2, the number of academic, engineers, and project managers in this sample have higher frequency than other items. Furthermore, most participants have a doctorate and a master’s degree, which seems quite logical considering the profession of the participants.
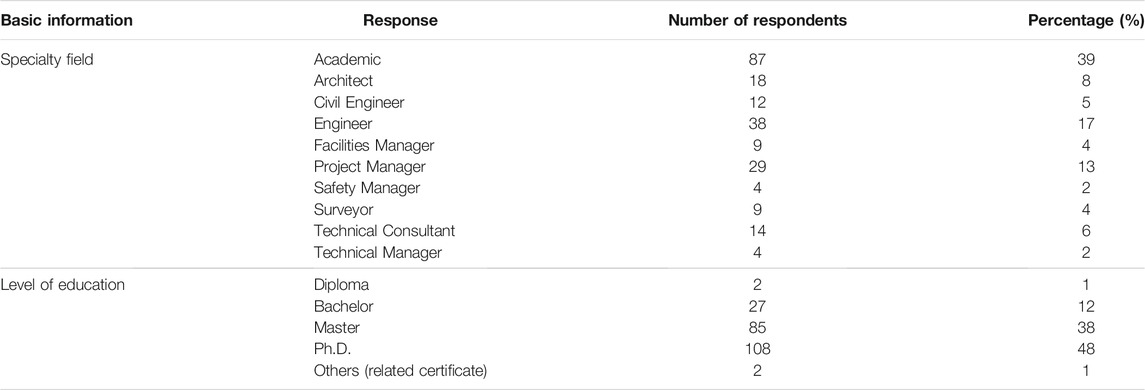
TABLE 2. Details of the survey participants.
In addition, Figure 2 shows the relationship between the numbers of participants from each profession relative to the continent of residence. As can be seen in Figure 2, each profession is represented by specific colours on the continents. In addition, the proportion of participants in continental Europe is higher, followed by Europe and the United States. These ratios are significantly higher than in other academic professions, engineering, project manager and technology consultants.
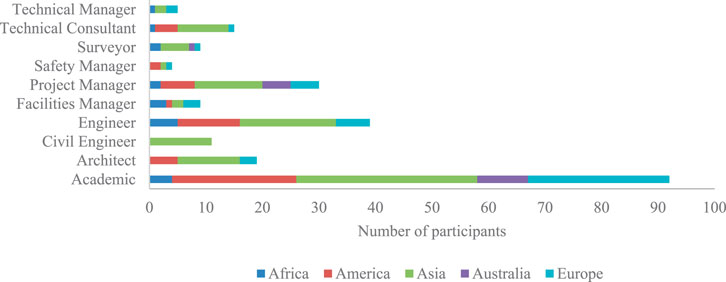
FIGURE 2. The relationship between profession and the continent of residence.
In order to check the initial status of answering the questions, comparison of the effect of methods based on types of buildings is shown in Figure 3. As can be seen in Figure 3, the studied methods seem to have almost the same effect in all types of buildings. The measures in design and construction have the highest score in all three types of buildings and training protocols have the least score in all three types of buildings.
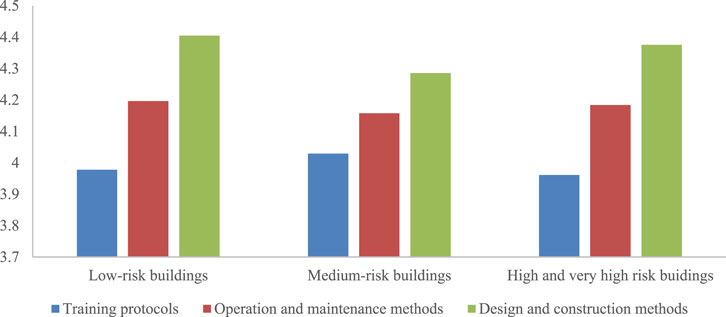
FIGURE 3. Comparing the effect of methods based on all types of buildings.
Radar diagram (Figure 4) shows the effect of the presented methods based on the all types of building. As shown in Figure 4, the studied methods have the highest scores in high and very high-risk buildings. This situation is also noticeable in medium-risk buildings, but has the least effect in buildings at lower risk of exposure. This may be due to the fact that with the change of methods, no significant change is felt in these buildings, which is due to their low-risk nature. For this reason, this hypothesis can be fully examined by inferential analysis.
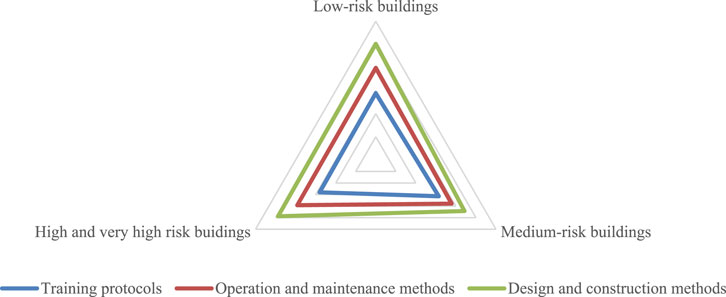
FIGURE 4. Comparing the effect of methods based on the all type of buildings.
In this study, the hypothesis is that the effect of the method of coping with this disease will be different in different types of buildings. In order to test this hypothesis, repeated measures analysis method and SPSS software were used. For this purpose, three types of coping methods extracted from the research questions using exploratory factor analysis method were selected which include training protocols (group 1), measures in operation and maintenance (group 2) and measures in design and construction (group 3). Buildings are also classified into three categories of low-risk (type 1), medium-risk (type 2) and high and very high-risk (type 3). In this research, methods are considered as intra-subject factors because they can be used in all three types of buildings and buildings are considered as inter-subject factors because they are different in nature.
Table 3 shows the results of descriptive analysis by grouping the coping method and the type of building. As can be seen in Table 3, the average of all subjects among the construction groups and method is higher than the value of 3, which means that the respondents have averaged above average values in the impact.
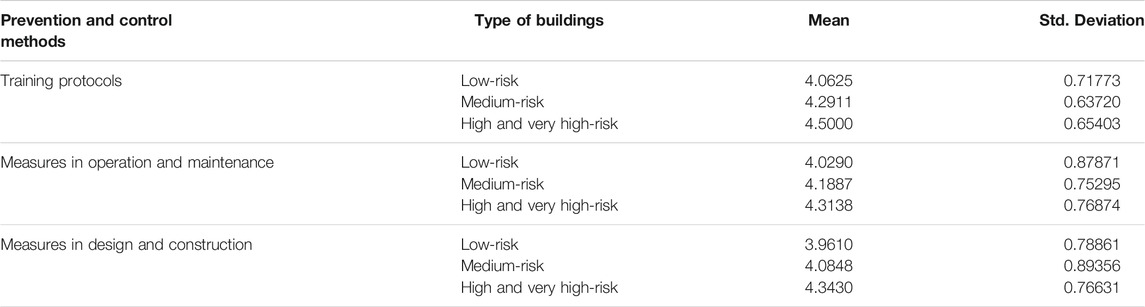
TABLE 3. Comparison of methods classification by type of buildings.
Table 4 is related to the box statistics test. This statistic tests the hypothesis that the observed covariance matrix of dependent variables (methods) is equal between different construction groups. In Table 4, the probability value is less than 0.05, which means that the null hypothesis is rejected. This means that the observed covariance matrices are not equal between different groups. That is, the methods vary between different construction groups.
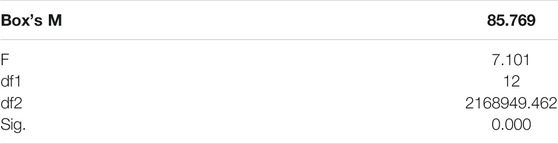
TABLE 4. Box’s test of equality of covariance matrices.
Table 5 shows the results of multivariate tests (Pillay effect test, Landa Wilkes test, hoteling effect, largest zinc root). For significance and non-significance of each test, the probability value can be considered, which is significant at the level of 0.05 if it is less than 0.05. According to the box table (Table 4) in this section, the amount of hoteling effect should be examined. As can be seen in Table 5, the effect of the method is significant, but the interaction effect of the method and the structure with each other is not significant. This means that there is a significant difference between the methods in nature, but a specific method is not necessarily used separately for the building in the sample under study and instead a combination of methods is used.

TABLE 5. Multivariate tests.
Table 6 shows the results of the spherical test. The valence sphericity test investigates the hypothesis that the covariance matrix of the error related to the dependent variables (methods) of a normal matrix is identical and homogenous. In this test, if the significance level is less than 0.05, the null hypothesis is rejected and otherwise the null hypothesis is confirmed. If the null hypothesis is rejected, the spherical power view of the variance-covariance matrix of the dependent variable (methods) is accepted and the other three Greenhouse-Geiser, Hyun-Felt or lower limit tests must be used to correct the degree of freedom. In this example, the sphericity of the covariance matrix of variance is accepted at an error level of 0.05 and no need to use the other three tests.

TABLE 6. Mauchly’s test of sphericity.
Table 7 shows the test results for the effects within the subjects. Because the sphericity was confirmed by the Machley test in the previous section, the Sphericity Assumed tests should be considered. If it was rejected, three more rows were used. As can be seen in Table 7, only the effect of the method is significant in this test, i.e. the effect is differentiated between the methods or the effect of the methods is different.
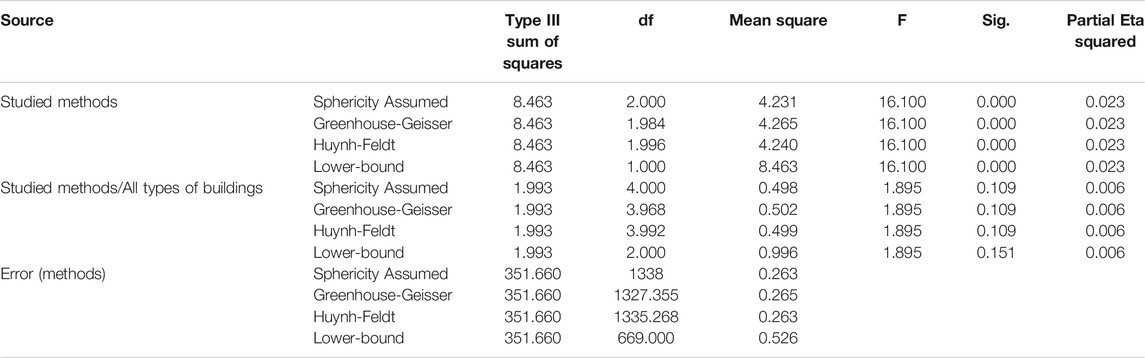
TABLE 7. Tests of within-subjects effects.
In Table 8, it is clear that the effect of the method is significant and linear, i.e. methods that are stronger in nature have a direct effect on the nature of the subject.

TABLE 8. Tests of within-subjects contrasts.
Table 9 shows the results of the Levene’s test. This test shows whether the variances of the method’s variable error in its three dimensions are equal and whether there are noticeable changes due to the nature of the method. As can be seen in Table 8, in the first and third methods, this test is not significant while it is significant in the second method. In other words, the variance of error (changes) between buildings becomes significant when using the second method.
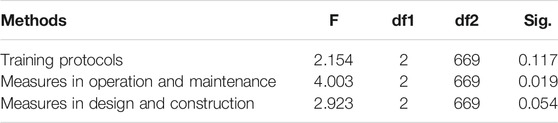
TABLE 9. Levene’s test of equality of error.
Table 10 contains the most important research results. The methods had different effects between different buildings which is confirmed by the opposite result of the BUILDING variable. This means that the effect of the methods varies significantly depending on the type of building.

TABLE 10. Tests of between-subjects effects.
As can be seen in Figure 5, the methods are effective in all types of buildings which is confirmed using the upward trend of the graphs. The blue line shows that type one methods are more effective in all types of buildings, especially in high and very high-risk buildings, than the other two methods. However, all methods have almost the same effect in low-risk buildings. Type 2 methods (measures in operation and maintenance) are also effective in all three types of buildings, but this effectiveness is less than type 3 methods (measures in design and construction) in high and very high-risk buildings. Methods of the third type (measures in design and construction) are also less efficient among low-risk and medium-risk buildings than the methods of the second (measures in operation and maintenance) and the first (training protocols) type.
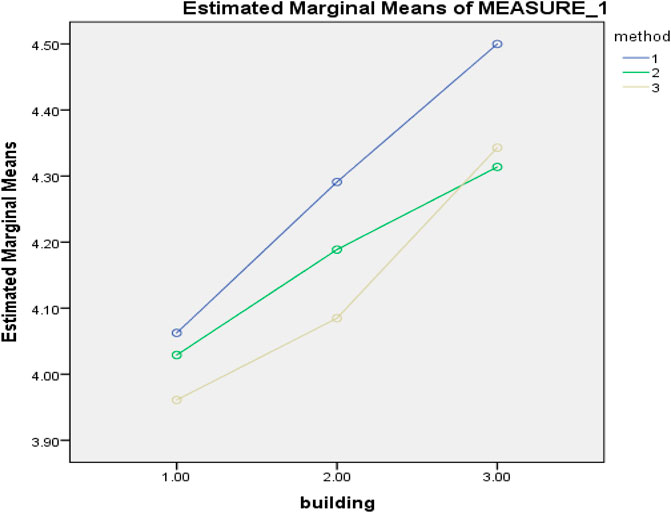
FIGURE 5. Comparing the effects of methods on three types of buildings.
One way to control covid-19 disease is to use prevention techniques in the construction and design of buildings. In this study, in order to investigate the effect of prevention methods in design and buildings, information was collected in the field. For this purpose, a questionnaire designed online was distributed internationally from April 8 to July 25, 2020. Individuals were randomly selected from the available list. The selected people have been active in this field scientifically or practically. 384 Individuals were randomly selected from the available list as the statistical samples. These people were contacted via email and message. This questionnaire had good content validity and the total reliability of the questionnaire was 0.967 which is a very good value. Primary methods of infectious prevention and control and flexible methods were evaluated in the questionnaire according to their impact on the building. To reach the correct conclusion, the research was divided into four main steps: first, demographic factors were examined, in the second stage, the questions were considered descriptively, in the third stage, the hypothesis was examined that the effect of each method was based on the type of building. The final conclusion was reached with a comparison chart.
In this study, the most of the participants in the sample were selected from academics and those who worked as project managers. Naturally, the number of people at the doctoral, master’s and bachelor’s levels was the highest. The highest abundance is in Asia, followed by Europe and the United States. In the initial review of the graphs and descriptive tables related to the questions, the score of the questions showed that the methods are useful, but these methods have the greatest impact on high and very high-risk buildings from the point of view of the participants in the sample.
In examining the hypothesis tested (the methods are effective in terms of the type of building), it was observed that the hypothesis tested was significant. In fact, these methods have different effects depending on the type of building and as it was observed, they have a direct impact on each other. That is, with the improvement of methods, their impact on buildings increases. The repetitive measurement method was used to obtain the answer to this question. Given that each method was used in each building, the methods were dependent on the type of building, so analysis of covariance by analysing repetitive measurements could answer this question.
In the end, it was observed that all methods have a positive effect in all types of buildings. However, while these methods have an equal effect in low-risk buildings, in high and very high-risk buildings, training protocols and design and construction measures have the greatest impact, but training protocols and the measures in operation and maintenance will have the greatest effect, in medium-risk buildings, respectively.
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found below: http://dx.doi.org/10.17632/jtf9d9dyt3.3.
The studies involving human participants were reviewed and approved by Yes. This study was approved by a research ethics committee at the University of Strathclyde in United Kingdom. All survey participants were well informed about the study and have given their permissions on data collection and usage. The patients/participants provided their written informed consent to participate in this study.
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We sincerely thank Professor Kerry London for engaging with us in the data collection process and her contribution to the questionnaire-based survey.
Alberta Health Services (2020). COVID-19 Scientific Advisory Group Rapid Evidence Report. Available at: https://www.albertahealthservices.ca/assets/info/ppih/if-ppih-covid-19-sag-risk-prediction-tools-rapid-review.pdf (Accessed June, , 2020).
Altamimi, A., and Ahmed, A. E. (2020). Climate Factors and Incidence of Middle East Respiratory Syndrome Coronavirus. J. Infect. Public Health 13 (5), 704–708. doi:10.1016/j.jiph.2019.11.011
Cronbach, L. J., Meehl, P. E., and Lange Salvia, A. (1955). Construct Validity in Psychological Tests Psychol. Bull. 52 (4), 281–302. doi:10.1037/h0040957
Dounis, A. I., and Caraiscos, C. (2009). Advanced Control Systems Engineering for Energy and comfort Management in a Building Environment-A Review. Renew. Sust. Energ. Rev. 13 (6-7), 1246–1261. doi:10.1016/j.rser.2008.09.015
Filho, W. L., Brandli, L. L., Lange Salvia, A., Rayman-Bacchus, L., and Platje, J. (2020). COVID-19 and the UN Sustainable Development Goals: Threat to Solidarity or an Opportunity? Sustainability 12 (13), 5343. doi:10.3390/su12135343
Guo, Z.-D., Wang, Z.-Y., Zhang, S.-F., Li, X., Li, L., Li, C., et al. (2020). Aerosol and Surface Distribution of Severe Acute Respiratory Syndrome Coronavirus 2 in Hospital Wards, Wuhan, China, 2020. Emerg. Infect. Dis. 26 (7), 1583–1591. doi:10.3201/eid2607.200885
Gwenzi, W. (2021). Leaving No Stone Unturned in Light of the COVID-19 Faecal-Oral Hypothesis? A Water, Sanitation and hygiene (WASH) Perspective Targeting Low-Income Countries. Sci. Total Environ. 753, 141751. doi:10.1016/j.scitotenv.2020.141751
IFMA (2020). Coronavirus (COVID-19) Resource Center: Webinars. Houston, USA: International Facility Management Association.
Krejcie, R. V., and Morgan, D. W. (1970). Determining Sample Size for Research Activities. Educ. Psychol. Meas. 30 (3), 607–610. doi:10.1177/001316447003000308
Lam, K. C. (2006). “Managing Building Services Maintenance Risk with Prediction Theories,” in CIBSE National Conference 2006, London, UK, March 21-22, 2006.
Li, Q., Feng, W., and Quan, Y.-H. (2020). Trend and Forecasting of the COVID-19 Outbreak in China. J. Infect. 80 (4), 469–496. doi:10.1016/j.jinf.2020.02.014
Liu, Y., Ning, Z., Chen, Y., Guo, M., Liu, Y., Gali, N. K., et al. (2020). Aerodynamic Analysis of SARS-CoV-2 in Two Wuhan Hospitals. Nature 582 (7813), 557–560. doi:10.1038/s41586-020-2271-3
Lowen, A. C., Mubareka, S., Steel, J., and Palese, P. (2007). Influenza Virus Transmission Is Dependent on Relative Humidity and Temperature. Plos Pathog. 3 (10), e151. doi:10.1371/journal.ppat.0030151
Luongo, J. C., Fennelly, K. P., Keen, J. A., Zhai, Z. J., Jones, B. W., and Miller, S. L. (2016). Role of Mechanical Ventilation in the Airborne Transmission of Infectious Agents in Buildings. Indoor Air 26 (5), 666–678. doi:10.1111/ina.12267
Mecenas, P., Bastos, R. T. d. R. M., Vallinoto, A. C. R., and Normando, D. (2020). Effects of Temperature and Humidity on the Spread of COVID-19: A Systematic Review. PLoS ONE 15 (9), e0238339. doi:10.1371/journal.pone.0238339
Ong, S. W. X., Tan, Y. K., Chia, P. Y., Lee, T. H., Ng, O. T., Wong, M. S. Y., et al. (2020). Air, Surface Environmental, and Personal Protective Equipment Contamination by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) from a Symptomatic Patient. Jama 323 (16), 1610–1612. doi:10.1001/jama.2020.3227
OSHA (2020). Guidance on Preparing Workplaces for COVID-19, 35. Washington, DC: Occupational Safety and Health Administration.
Pinheiro, M. D., and Luís, N. C. (2020). COVID-19 Could Leverage a Sustainable Built Environment. Sustainability 12 (14), 5863. doi:10.3390/su12145863
Pirouz, B., Shaffiee Haghshenas, S., Shaffiee Haghshenas, S., and Piro, P. (2020). Investigating a Serious challenge in the Sustainable Development Process: Analysis of Confirmed Cases of COVID-19 (New Type of Coronavirus) through a Binary Classification Using Artificial Intelligence and Regression Analysis. Sustainability 12 (6), 2427. doi:10.3390/su12062427
Price, R. H. M., Graham, C., and Ramalingam, S. (2019). Association between Viral Seasonality and Meteorological Factors. Sci. Rep. 9 (1), 1–11. doi:10.1038/s41598-018-37481-y
Rahdari, A., Sepasi, S., and Moradi, M. (2016). Achieving Sustainability through Schumpeterian Social Entrepreneurship: The Role of Social Enterprises. J. Clean. Prod. 137, 347–360. doi:10.1016/j.jclepro.2016.06.159
Sagheb, M. Z., Ghasemi, B., and Nourbakhsh, S. K. (2020). Factors Affecting purchase Intention of Foreign Food Products: An Empirical Study in the Iranian Context. Bfj 122 (5), 1485–1504. doi:10.1108/BFJ-05-2019-0318
Santarpia, J. L., Rivera, D. N., Herrera, V. L., Morwitzer, M. J., Creager, H. M., Santarpia, G. W., et al. (2020). Aerosol and Surface Contamination of SARS-CoV-2 Observed in Quarantine and Isolation Care. Sci. Rep. 10 (1), 1–8. doi:10.1038/s41598-020-69286-3
Sarvari, H., Chen, Z., Chan, D. W. M., Lester, E. A., Yahaya, N., and London, K. (2020). Data from: The Dataset of an International Survey on COVID-19 Response in Facilities Management in 2020. Mendeley Data, V1. doi:10.17632/jtf9d9dyt3.3
Sarvari, H., Rakhshanifar, M., Tamošaitienė, J., Chan, D. W. M., and Beer, M. (2019). A Risk Based Approach to Evaluating the Impacts of Zayanderood Drought on Sustainable Development Indicators of Riverside Urban in Isfahan-Iran. Sustainability 11 (23), 6797. doi:10.3390/su11236797
Shen, M., Peng, Z., Guo, Y., Rong, L., Li, Y., Xiao, Y., et al. (2020). Assessing the Effects of Metropolitan-wide Quarantine on the Spread of COVID-19 in Public Space and Households. Int. J. Infect. Dis. 96, 503–505. doi:10.1016/j.ijid.2020.05.019
Wang, M., Jiang, A., Gong, L., Lu, L., Guo, W., Li, C., et al. (2020). Temperature Significantly Change COVID-19 Transmission in 429 Cities. medRxiv. doi:10.1101/2020.02.22.20025791
Keywords: COVID-19 response, built environment, facilities management, buildings, international survey
Citation: Sarvari H, Chen Z, Chan DWM, Lester EA, Yahaya N, Nassereddine H and Lotfata A (2022) A Global Survey of Infection Control and Mitigation Measures for Combating the Transmission of COVID-19 Pandemic in Buildings Under Facilities Management Services. Front. Built Environ. 7:644104. doi: 10.3389/fbuil.2021.644104
Received: 19 December 2020; Accepted: 20 December 2021;
Published: 28 January 2022.
Edited by:
Jiro Yoshida, The Pennsylvania State University (PSU), United StatesReviewed by:
Susy Fatena Rostiyanti, Podomoro University, IndonesiaCopyright © 2022 Sarvari, Chen, Chan, Lester, Yahaya, Nassereddine and Lotfata. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hadi Sarvari, aC5zYXJ2YXJpQGtodWlzZi5hYy5pcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.