 Zhengdong Li
Zhengdong Li Ming Pei
Ming Pei Jianhua Zhang1
Jianhua Zhang1 Ningguo Liu
Ningguo Liu Donghua Zou
Donghua Zou
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Bioeng. Biotechnol. , 14 June 2023
Sec. Biomechanics
Volume 11 - 2023 | https://doi.org/10.3389/fbioe.2023.1178199
The mechanical properties and material constitution of the aorta are important in forensic science and clinical medicine. Existing studies on the material constitution of the aorta do not satisfy the practical requirements of forensic and clinical medicine, as the reported failure stress and failure strain values for human aortic materials have a high dispersion. In this study, descending thoracic aortas were obtained from 50 cadavers (dead within 24 h) free of thoracic aortic disease, aged from 27 to 86 years old, which were divided into six age groups. The descending thoracic aorta was divided into proximal and distal segments. A customized 4-mm cutter was used to punch a circumferential and an axial dog-bone-shaped specimen from each segment; the aortic ostia and calcification were avoided. Instron 8,874 and digital image correlation were used to perform a uniaxial tensile test on each sample. Four samples from each descending thoracic aorta produced ideal stress-strain curves. All parameter-fitting regressions from the selected mathematical model converged, and the best-fit parameters of each sample were obtained. The elastic modulus of collagen fiber, failure stress, and the strain showed a decreasing trend with age, while the elastic modulus of elastic fiber showed an increasing trend with age. The elastic modulus of collagen fiber, failure stress, and strain of circumferential tensile were all greater than those for axial tensile. There was no statistical difference in model parameters and physiological moduli between the proximal and distal segments. The failure stress and strain in the proximal circumferential, distal circumferential, and distal axial tensile were all greater for the male group than for the female group. Finally, the Fung-type hyperelastic constitutive equations were fitted for the different segments in different age groups.
The aorta, the largest blood vessel in the body, is the primary artery in the systemic circulation. It is very important for maintaining the function of the human body. Aorta rupture causes up to 80%–94.4% mortality and is an important cause of in forensic practice (Hiller et al., 2010; Teixeira et al., 2011; Kent, 2014). Aortic ruptures can be caused by trauma, disease, or medical practice. Distinguishing pathologic and traumatic aortic ruptures from one another is one of the difficulties in forensic identifications, especially with regard to the identification of the degree of participation of trauma when multiple trauma exist or trauma and disease coexist. However, the causative mechanism of aorta ruptures, such as deceleration, osseous pinch, torsion, longitudinal stretch, and water-hammer effects, etc. (Neschis et al., 2008), are difficult neither to reproduce experimentally on cadavers, nor to observe the dynamic aortic response in situ (Bass et al., 2001). The finite element (FE) simulation can be used to study the mechanism of aortic injuries, while mechanical properties and material constitution of the aorta are an important basis of FE simulation, which directly affects the accuracy of simulation results. Clinically, surgical indications of aortic aneurysm mainly depend on the diameter and growth rate (Lederle et al., 2002; Hans et al., 2005; Grootenboer et al., 2009), which ignores the more important relationship between rupture and mechanical properties of the aorta, especially the tensile strength of the aortic wall. In addition, the mechanical properties of the prosthesis for aortic aneurysm surgery should be as consistent as possible with the mechanical properties of the aorta. During interventional surgery, the protection of blood vessels should also take into consideration the material constitution of the walls of the blood vessels. Therefore, the mechanical properties and material constitution of the aorta are very important in forensic and clinical medicine.
At present, the most common methods for studying the mechanical properties of the aorta are uniaxial tensile, biaxial tensile, peeling test, residual strain/stress test. Uniaxial tensile is the main method because it is relatively simple and can be performed on a variety of materials (Raghavan et al., 1996; Sherebrin et al., 1989; Vorp et al., 2003; Vallabhaneni et al., 2004; Guinea et al., 2010; Sokolis et al., 2012; García-Herrera et al., 2012; Ninomiya et al., 2015; Ferrara et al., 2016; Ferrara et al., 2018). We have reviewed the common literature on human aortic stretching experiments and list the results in Table 1. It was found that there are some differences among different studies in the source of inspection materials, geometric shape and size of inspection materials, experimental methods (preloading, pre-stretching, strain rate, clamping, test temperature and environment), strain measurement methods, etc. These differences lead to large data discrepancies in different studies, and the material properties of aortas from different parts or even the same part are often inconsistent, and some are even contradictory. In 1982, Mohan and Melvin (Mohan and Melvin, 1982) used a dog-bone-shaped sample with a width of 6.35 mm or 4.57 mm to measure the circumferential and axial failure stress and strain under quasi-static and dynamic conditions. The circumferential and longitudinal tensile failure stresses under quasi-static conditions are 1.72 ± 0.89 MPa and 1.47 ± 0.91 MPa, respectively. Vallabhaneni et al. (Vallabhaneni et al., 2004) reported lower values of 610 ± 70 kPa and 1,300 ± 110 KPa for circumferential and longitudinal failure stresses, respectively, using rectangular samples of healthy thoracic aorta with a width of 4 mm. However, Garcı'a-Herrera et al. (García-Herrera et al., 2012) reported higher values, where the circumferential and longitudinal values can reach 2,180 ± 240 kPa and 1,140 ± 100 kPa. It can be seen from Table 1 that most studies believe that the circumferential stress is greater than the longitudianl stress (Mohan and Melvin, 1982; Raghavan et al., 1996; Sokolis et al., 2012; Pichamuthu et al., 2013), but a small number of studies have the opposite result (Raghavan et al., 2011), especially Vorp et al. (Vorp et al., 2003) considered no difference in material properties in the two directions. The material properties of different segments of the aorta may also be different. Sokolis (Sokolis, 2007) based on the uniaxial tensile test of the porcine aorta, found that under physiological pressure, the material properties and structure of the aorta have segmental changes with different aortic pressures. Haskett et al. (Haskett et al., 2010) found for the first time that the circumferential and axial tangential moduli of the aorta harden with age based on biaxial stretching experiments of the human aorta, and that the abdominal aorta was stiffer than other parts. Furthermore, Sokolis (Sokolis, 2023) studied the failure parameters of nine consecutive segments of the aorta and the intima, media, and adventitia in the circumferential and axial directions. It was found that the strength of the intima and media remained unchanged along the aorta, but its longitudinal stretching ability decreased, and the strength of the adventitia was significantly higher than that of the intima and media. Females rarely have different failure parameters than males. Sokolis has also conducted extensive research on regional delamination strength (Sokolis and Papadodima, 2022), layer-specific residual deformation (Sokolis et al., 2021) in different parts of the aorta, and aortic circumferential residual strains (Sokolis et al., 2017) that vary with sex and age. These studies have helped to advance our understanding of aortic physiology and explain the biomechanism of aortic dissection.
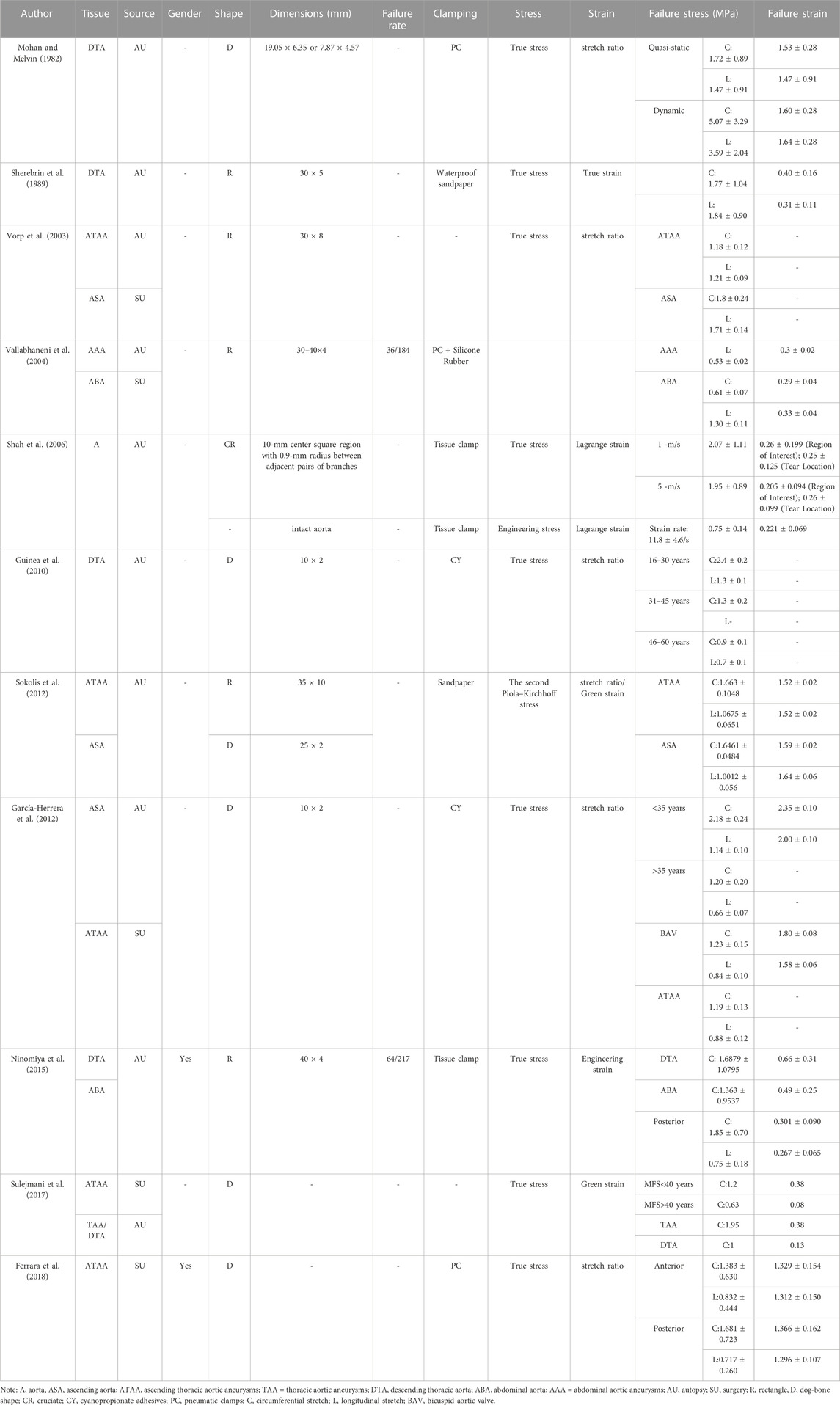
TABLE 1. Overview of tensile test results on aorta full-thickness tests performed until failure.
However, the specimen extraction methods and experimental methods used in the above-mentioned studies are not uniform, which has resulted in large differences in the experimental results and a lack of direct comparability. To address this issue, our research group has developed a series of sampling molds and experimental methods suitable for aortic uniaxial tension experiments using porcine aorta. Specifically, the specimens are expanded into a dog-bone shape with a region of interest of 24 mm × 4 mm. Strain is measured using digital image correlation (DIC) (Pei et al., 2021). Due to the small area of the ascending aorta and aortic arch, we were unable to extract enough specimens from these regions, which could have affected the systematicness of the data. Additionally, among patients with blunt chest trauma, the most common site of aortic rupture is the isthmus, followed by the distal descending aorta, ascending aorta, and aortic arch (Watanabe et al., 2013). For these reasons, we performed material sampling and tensile testing on the part below the aortic isthmus.
The reported failure stress and failure strain values for human aortic materials have a high dispersion. This, along with the lack of systematic and large-sample Chinese experimental data, means that the current state of knowledge is not sufficient to satisfy the needs of forensic science and clinical medicine in China. Therefore, it is necessary to conduct systematic material property testing on Chinese human aorta. In this study, 50 adult descending thoracic aortas were divided into six age groups, and the descending thoracic aorta was divided into proximal and distal segments. A customized cutter was used to punch a circumferential and an axial dog-bone-shaped specimen in each segment, while avoiding the aortic ostia and calcification. Instron 8,874 and DIC were used to perform a uniaxial tensile test on each sample. The mechanical properties and hyperelastic material constituents of different parts of the descending thoracic aorta from each age group were characterized. Finally, the differences between age groups, sex, tensile direction, and segments were compared and analyzed.
This study was approved by the Ethics Committee of the Academy of Forensic Science (Ministry of Justice, China), including the acquisition of specimens and informed consent of close relatives of the deceased. Fresh corpses in 50 forensic cases (dead within 24 h and without thoracic aortic aneurysm, aortic dissection and other serious diseases) were recruited ranging in age from 27 to 86 years. The average age was 51.14 years, and the median age was 51.5 years old. There were 34 men and 16 women, divided into six age groups (The group 1 consisted of 13 corpses, aged 27–35 years old. Of these, 11 were male and 2 were female. The group 2 consisted of 9 corpses, aged 36–45 years old. Of these, 7 were male and 2 were female. The group 3 consisted of 7 corpses, aged 46–55 years old. Of these, 3 were male and 4 were female. The group 4 consisted of 11 corpses, aged 56–65 years old. Of these, 6 were male and 5 were female. The group 5 consisted of 5 corpses, aged 66–75 years old. Of these, 3 were male and 2 were female. The group 6 consisted of 5 corpses, aged 76–86 years old. Of these, 4 were male and 1 was female.). The descending thoracic aorta was extracted from cadavers.
After dissections, the samples were stored at −80°C, and the tests were completed within 1 week. Before the experiment, the sample was taken from the −80°C refrigerator and soaked overnight in a normal saline solution without Ca2+. After equilibrium at room temperature, the loose connective tissue attached to the adventitia of the aorta was dissected. The human descending thoracic aorta was divided into proximal and distal segments at the level of the seventh-eighth intercostal posterior artery. Circumferential and axial are defined according to the direction of aortic curvature. A customized 4-mm cutter (Pei et al., 2021) (see in Supplementary Figure S1) was used to systematically punch out two circumferential (upper part) and two axial (lower part) dog-bone-shaped samples from each segment (see in Supplementary Figure S2). The dimensions of the narrow middle part were 24 mm × 4 mm [optimal dimensions identified in our previous study (Pei et al., 2021)]; moreover, the calcification and aortic ostia were avoided.
The original thickness and width of the test area were photographed under the unloaded state with a customized profile measurement system (see in Supplementary Figure S3). The VisionMaster3 software (Hikrobot Co., Ltd., China) was used for measurements. After the profile was measured, black speckles were sprayed on the endothelial surface of the test area. The convex plates of the customized clamps were placed in the fixture groove, and the middle part of the specimen was placed in the specimen groove of the customized mold. Subsequently, the two ends of the specimen were quickly squeezed between the clamps and using cyanoacrylate to avoid slippage (Pei et al., 2021) (the photo of sample in the grips of customized apparatus is shown in Supplementary Figure S4).
The samples were subjected to uniaxial tensile tests using an Instron 8,874 (Illinois Tool Works Inc., USA) coupled to a DIC system at room temperature. The clamps and samples were mounted in the jaws of the pneumatic grips of the Instron 8,874. The distance between the grips was adjusted, starting from a slightly curved configuration. The sample was then slowly extended until the load cell recorded the minimum tensile force, which was assumed to be the load-free configuration (initial point). The distance between the grips at this initial point was denoted as the original length L). Each specimen was preconditioned at a speed of 0.2 L per minute and a stretching amplitude of 0.04 L for five cycles to eliminate the hysteresis effect and obtain a repeatable stress-strain curve. The specimen was then stretched at the same speed until it failed. The applied force was continuously measured and stored by Instron 8,874 (maximum load of 25 kN with an accuracy of 0.5% of full scale), and the DIC system (with resulotion of 5 million pixels) synchronously collected surface strain photos of the specimens at a sampling rate of 1 Hz to record the strain in the tensile direction. Physiological saline was sprayed on the specimens to keep them moist before and during the experiment.
According to the width and thickness measured for the initial state of the specimens, combined with the incompressible nature of the aorta (Chuong and Fung, 1983) (the volume of the specimen is constant during the stretching process), engineering strain and stress, stretch ratio, true strain, and true stress can be calculated and converted.
The engineering strain (
The true stress (
In order to simplify the analysis and facilitate comparison between different groups of specimens, this study adopted the mathematical model proposed by Raghavan et al. (Raghavan et al., 1996):
In this model,
In the first phase, the tensile stress is low and only elastic fibers bear the tensile stress. At this time,
In phase 2, collagen fibers begin to bear the tensile load, and the slope of the stress-strain curve increases, indicating hyperelasticity.
In phase 3, all the collagen fibers have become taut and the stiffness of the tissue reaches its maximum. Here, the slope of the stress-strain curve corresponds to the sum of the total stiffness of the elastic and collagen fibers. As B
According to the above formula, K is the inverse of (EE + EC). A is the strain intercept of the maximum slope (EE + EC) of the stress-strain curve during the third phase. A is related to the recruitment speed of collagen fibers. The smaller the A value, the faster the collagen fibers bear the load. B is the stress value at the intersection of the slope of phase 1 and the maximum slope of phase 3. σu and εu are failure stress (the true stress) and failure strain (the engineering strain), respectively. In summary, the stress-strain curve is simplified as a function of three parameters: K, A, and B. EE and EC can be derived from those parameters.
On the basis of the above analysis, the Fung-type strain-energy function (Chuong and Fung, 1983) was used to fit the average stress-strain curve for the original data from each age group to characterize the mechanical properties of the descending thoracic aorta. This strain-energy function is the most commonly used two-dimensional exponential model in biomechanics literature regarding soft tissue (Sacks and Sun, 2003; Vito and Dixon, 2003; Sokolis et al., 2012). In this model, the aorta is regarded as incompressible, homogeneous, nonlinear, and anisotropic, and the function is expressed as:
where Ei is Green strain, which is calculated as:
λ is the stretch ratio; i = θ, z which represent the circumferential and axial tensile directions, respectively. The material constant K is a scale factor, and Cθθ, Czz, and Cθz represent the circumferential stiffness, axial stiffness, and the interaction between circumferential and axial stiffness, respectively.
The formula to derive Cauchy stress (the true stress) is:
The boundary condition of circumferential stretching is:
The boundary condition of axial stretching is:
The SPSS software (version 20) was used for parameter fitting and statistical analyses. According to the data collected and calculated by the material testing and DIC systems, as well as the original cross-sectional area of specimens, the stress-strain curve, failure stress, and failure strain were obtained for each specimen. The nonlinear regression Levenberg–Marquardt algorithm was used to fit Raghavan’s mathematical model with the stress-strain data from each sample, and the best-fitting parameters K, A, and B were obtained for each sample. The elastic modulus of the elastic fiber EE and the elastic modulus of the collagen fiber EC were then calculated. The Levenberg–Marquardt minimization algorithm was also used to fit the average stress-strain curves for the original data from each age group, and the Fung-type strain-energy function was fitted. The average stress-strain curves for circumferentially and axially oriented tissue were fitted concurrently using the Fung-type model.
The root mean square difference ε) and correlation coefficient (R2) were used to evaluate the fitting degree of the experimental data and the model. Calculation methods for this are presented below:
Where exp and mod represent experimental and model data; θ and z represent circumferential and axial tensile directions, respectively, and m and n are the number of data points tested in the two directions respectively (Iliopoulos et al., 2013). ε ≤ 0.1 means good fitting to the experimental data.
According to the previous grouping, the values of each parameter are expressed as the mean ± standard deviation of each group. ANOVA was used for comparison between the groups, and LSD (least significant difference) was used for multiple comparison tests if the overall comparison was different. Comparison between the different segments (in all individuals), genders (in the third, fourth, and fifth groups, with a relatively appropriate sex ratio and quantity) and two directions was performed by a two-tailed independent t-test. A significant difference was assumed if a p-value was less than 0.05.
Ideal stress-strain curves were obtained from four specimens of each descending thoracic aorta. Figure 1 shows the stress-strain curves of four samples from each representative aorta from the different age groups, including proximal and distal circumferential and axial stretching. Rapidly increasing elastic modulus in the stress-strain curves indicates a significant hyperelastic characteristic of the human aorta, and the increase in the elastic modulus of circumferential specimens is more obvious than that of the axial specimens. The failure stress and strain of circumferential specimens are larger than that of axial specimens. With increasing age, the failure stress and strain tend to decrease.
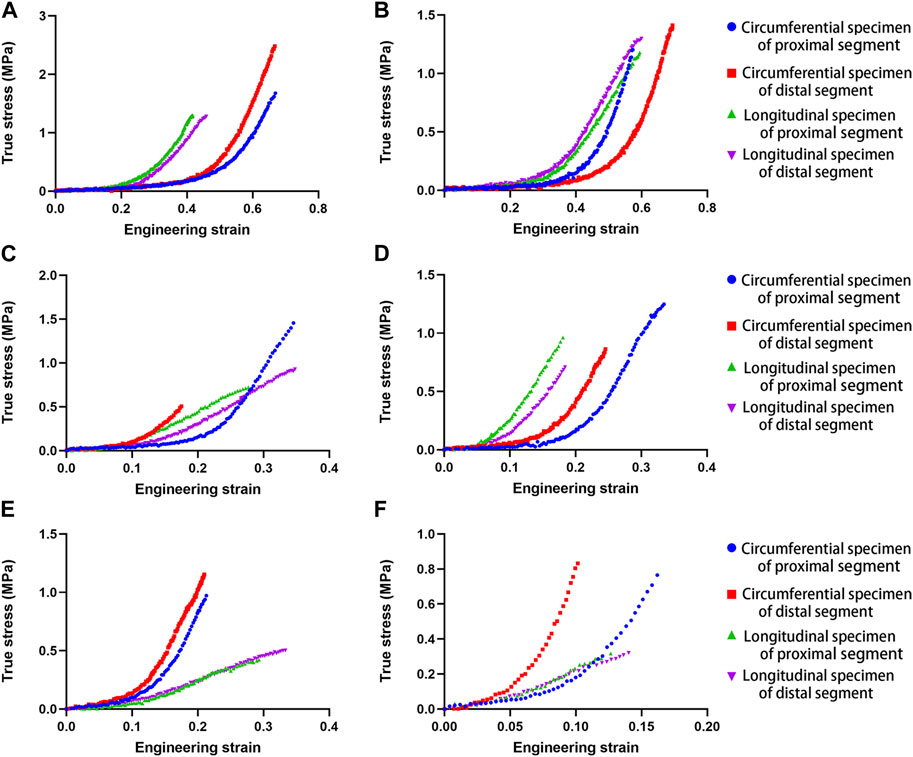
FIGURE 1. Uniaxial tensile stress-strain curves in human aortas at different ages (A). 28 years; (B). 37 years; (C). 54 years; (D). 64 years; (E). 75 years; (F). 81 years.
All parameter-fitting regressions of the selected mathematical model in this study converge to obtain the best-fitting parameters for each sample. The stress-strain curves of all specimens indicate a satisfactory fit with the mathematical model. Figure 2 shows the original experimental data for the four specimens of one aorta and the mathematical model curves with the best-fitting parameters. The mean values of parameters for the different parts and different age groups are shown in Table 2, and the mean values of the physiological moduli are shown in Table 3. The average stress-strain curves for the different tensile directions of the different parts and different age groups are plotted in Figure 3 using the average values of model parameters (Table 2).
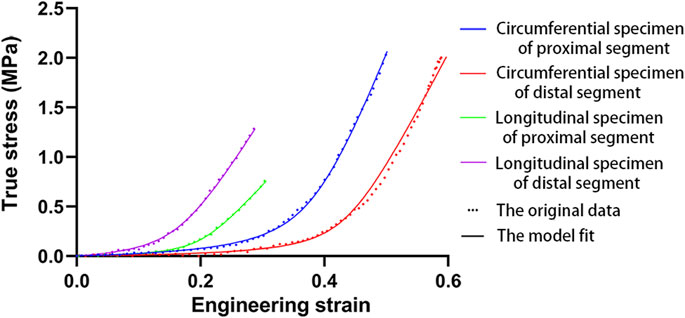
FIGURE 2. The original data and model fitting (35 years).
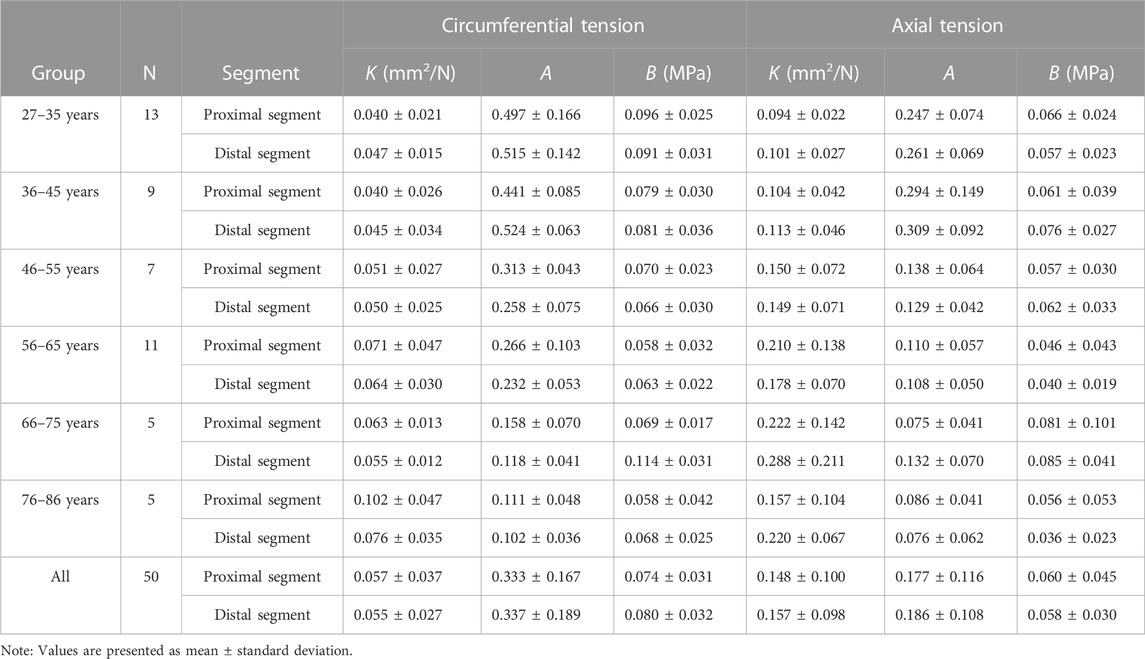
TABLE 2. The mean model parameters for the different aortic parts for the different age groups.
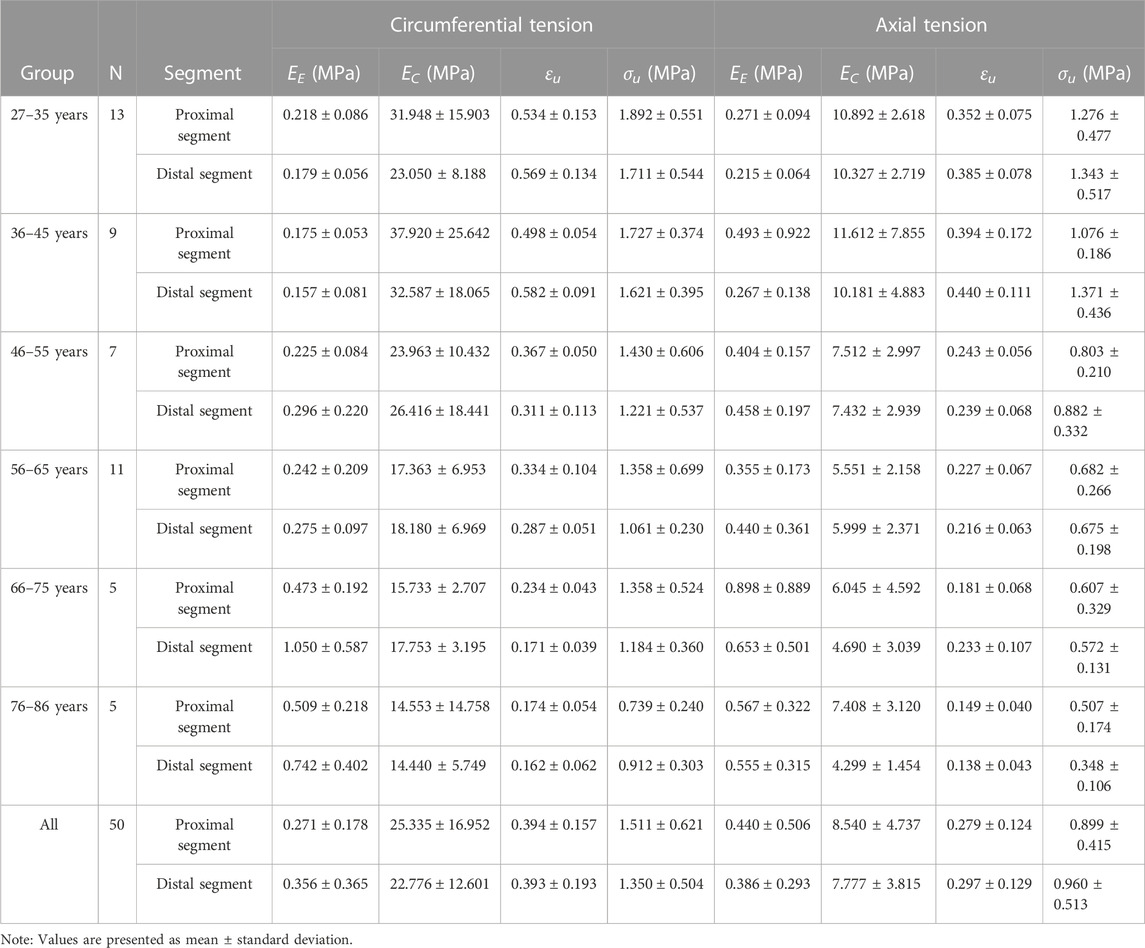
TABLE 3. Mean physiological modulus of the different parts for the different age groups.
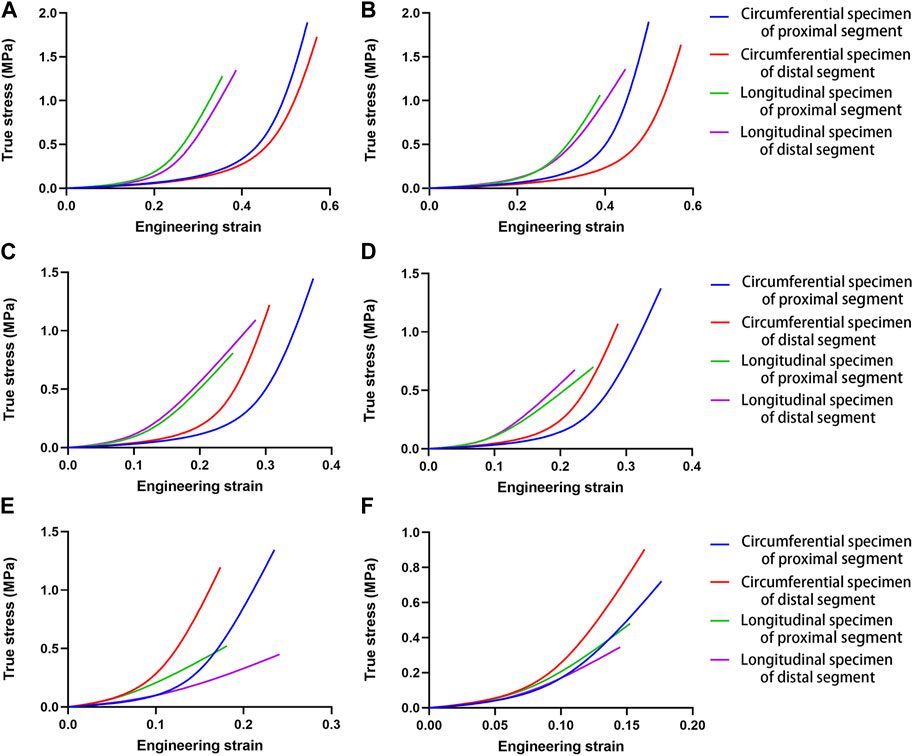
FIGURE 3. Mean stress-strain curves for the different tensile directions in different aortic segments for the different age groups. (A). Group 1, 27–35 years; (B). Group 2, 36–45 years; (C). Group 3, 46–55 years; (D). Group 4, 56–65 years; (E). Group 5, 66–75 years; (F). Group 6, 76–86 years.
K, A, B, EE, EC, the failure stress and the failure strain were different among the proximal circumferential tensile groups. The pairwise comparison results are listed below. K: there was a statistical difference between groups 1, 2 and 4, 6, and a statistical difference between groups 3 and 6. A: there was a statistical difference between groups 1, 2 and 3, 4, 5, 6. B: there was a statistical difference between groups 1 and 4, 6. EE increased with age, and there was a statistical difference between groups 1, 2, 3, 4, and 5, 6. EC decreased with age, and there was a statistical difference between groups 1, 2 and 4, 6 (Figure 4A). The failure stress decreased with age, and there was a statistical difference between groups 1 and 4, 6, and a statistical difference between groups 2, 3, 4, and 6. The failure strain decreased with age, and there were statistical differences between groups 1, 2 and 3, 4, 5, 6, and between 3 and 5, 6, and between 4 and 6 (Figure 5A). Figures 6A,B show the scatter plots of failure stress and the failure strain with age. The linear fitting equations were σu = 2.536–0.02 × Age, R2 = 0.296, and εu = 0.774–0.007 × age, R2 = 0.629.
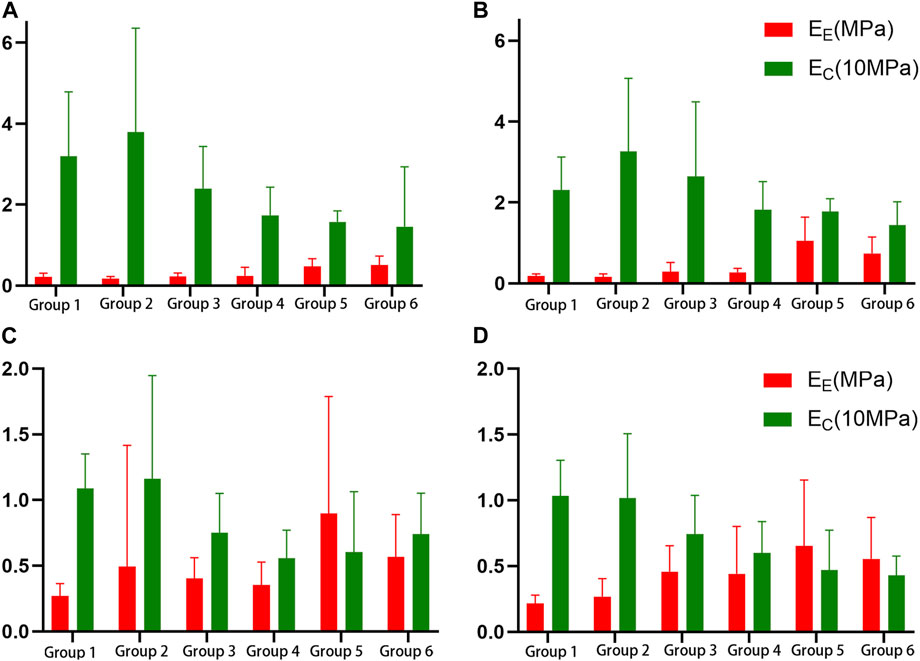
FIGURE 4. Histogram of the elastic fiber modulus (EE) and the collagen fiber modulus (EC). (A). Proximal circumferential tensile; (B). Distal circumferential tensile; (C). Proximal axial tensile; (D). Distal axial tensile.
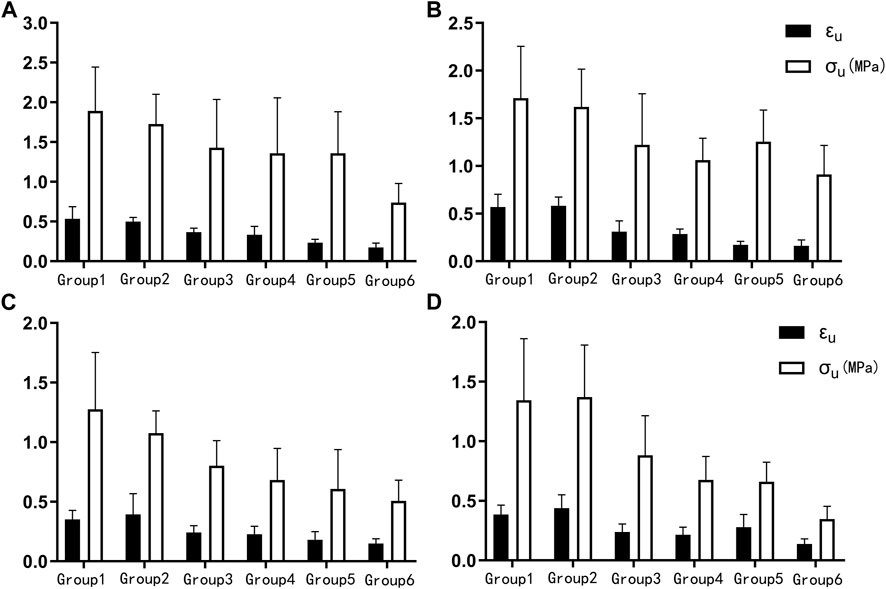
FIGURE 5. Histogram of the failure stress (σu) and failure strain (εu). (A). Proximal circumferential tensile; (B). Distal circumferential tensile; (C). Proximal axial tensile; (D). Distal axial tensile.
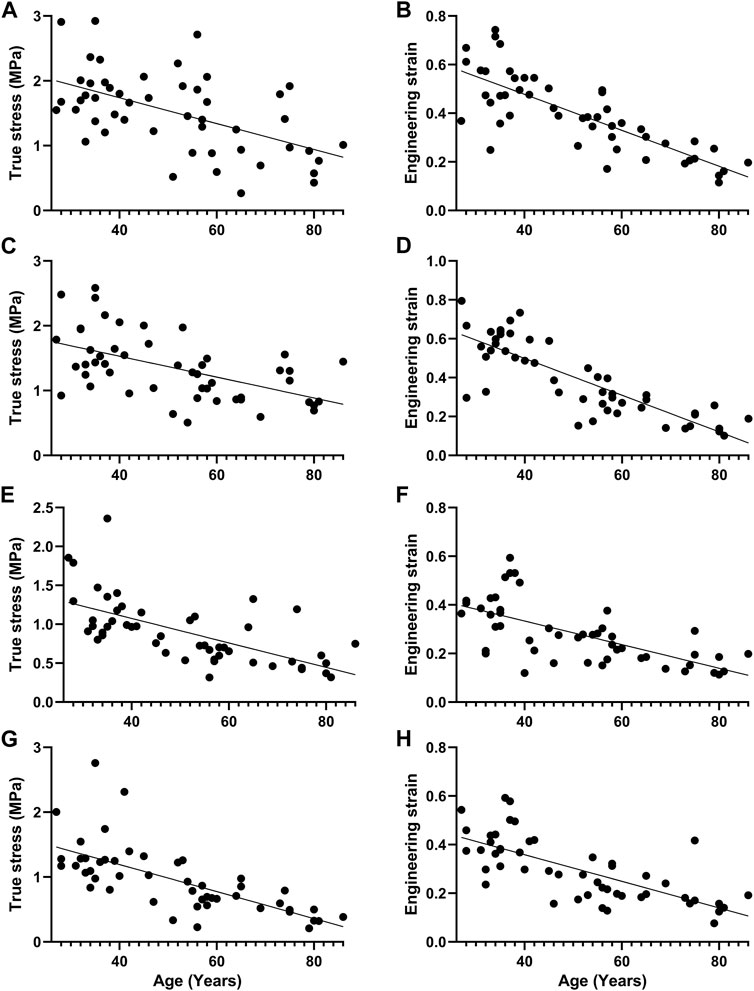
FIGURE 6. Scatter plot of failure stress and failure strain with age and straight line fitting. (A, B). Proximal circumferential tensile; (C,D). Distal circumferential tensile; (E,F). Proximal axial tensile; (G,H). Distal axial tensile.
A, B, EE, failure stress, and failure strain were different among the groups under distal circumferential tensile. The pairwise comparison results are listed below. A: there were statistical differences between groups 1, 2 and 3, 4, 5, 6, and between 3, 4 and 5, 6. B: there were statistical differences between groups 1 and 4 and between 2, 3, 4, 6 and 5. EE increased with age, and there were statistical differences between groups 1, 2, 3, 4 and 5, 6, and between 5 and 6 (Figure 4B). The failure stress decreased with age, and there were statistical differences between groups 1 and 3, 4, 5, 6, and between 2, and 4, 6. The failure strain decreased with age, and there were statistical differences between groups 1, 2 and 3, 4, 5, 6, and between 3, 4 and 5, 6 (Figure 5B). Figures 6C,D show the scatter plots of failure stress and the failure strain with age. The linear fitting equation is σu = 2.174–0.016 × age, R2 = 0.294, and εu = 0.876–0.009 × age, R2 = 0.691.
K, A, EC, failure stress, and failure strain were different among the groups under proximal axial tensile. The pairwise comparison results are listed below. K: groups 1, 2 were statistically different from 4, 5. A: groups 1, 2 were statistically different from 3, 4, 5, 6. EC decreased with age, and there was a statistical difference between groups 1, 2 and 4, 5 (Figure 4C). The failure stress decreased with age, and there were statistical differences between groups 1 and 3, 4, 5, 6, and between 2 and 4, 5, 6. The failure strain generally showed a decreasing trend with age, and there was a statistical difference between groups 1, 2 and 3, 4, 5, 6 (Figure 5C). Figures 6E,F show the scatter plots of failure stress and failure strain with age. The linear fitting equation is σu = 1.704–0.016 × age, R2 = 0.413, and εu = 0.528–0.005 × age, R2 = 0.441.
K, A, B, EE, EC, failure stress, and failure strain were different among the groups under distal axial tensile. Pairwise comparison, K: there were statistical differences between groups 1 and 4, 5, 6, between 2 and 5, 6, and between 3, 4 and 5. A: groups 1, 2 were statistically different from 3, 4, 5, 6. B: there were statistically significant differences between groups 1 and 5, between 2 and 4, 6, between 3 and 6, between 4 and 5, and between 5 and 6. EE increased with age, and there was a statistical difference between groups 1, 2 and 4, 5, 6. EC decreased with age, and there was a statistical difference between groups 1, 2 and 4, 5, 6 (Figure 4D). The failure stress showed a decreasing trend with age, and groups 1, 2 were statistically different from the other four groups, and group 3 was statistically different from 6. The failure strain decreased with age, and there were statistical differences between groups 1, 2 and 3, 4, 5, 6, and between 3 and 6 (Figure 5D). Figures 6G,H show the scatter plots of the failure stress and the failure strain with age. The linear fitting equation is σu = 2.025–0.021 × age, R2 = 0.474, and εu = 0.578–0.005 × age, R2 = 0.517.
There were statistical differences between proximal axial stretching and circumferential tensile, except B. EC, failure stress, and failure strain were greater under circumferential stretching than under axial stretching, while EE was smaller. The mean circumferential tensile failure stress and failure strain were 1.511 MPa and 0.394, respectively; the mean EE and EC were 0.271 MPa and 25.335 MPa, respectively. The mean axial tensile failure stress and failure strain were 0.899 MPa and 0.279 MPa, respectively. The mean EE and EC were 0.440 MPa and 8.540 MPa, respectively (Figure 7A).
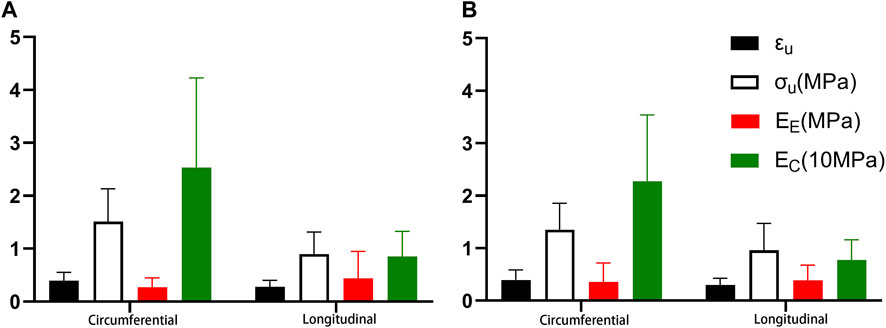
FIGURE 7. Comparison of the different stretching directions. (A). Proximal segment; (B). Distal segment.
While there was no statistical difference in EE between distal circumferential and axial stretching, there were statistical differences in other parameters. Ec, failure stress, and failure strain were greater under circumferential stretching than under axial stretching. The mean circumferential tensile failure stress and failure strains were 1.350 MPa and 0.393 MPa respectively, and the mean EE and EC were 0.356 MPa and 22.776 MPa respectively. The mean axial tensile failure stress and failure strain were 0.960 MPa and 0.297, respectively, and the mean values of EE and EC were 0.386 MPa and 7.777 MPa, respectively (Figure 7B).
There were no statistically significant differences in the fitting parameters and physiological moduli between the proximal and distal segments for both circumferential and axial stretching (Figure 8).
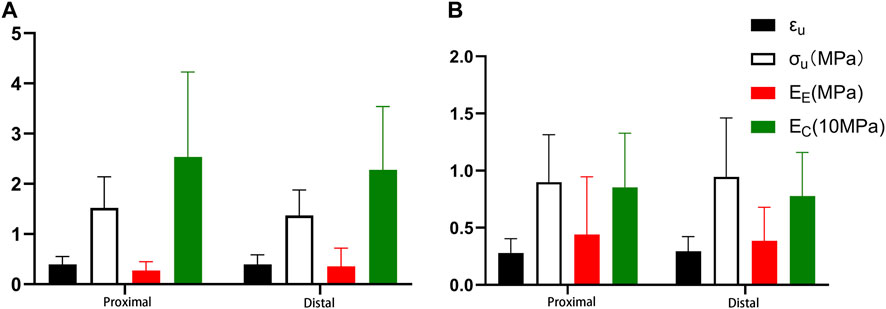
FIGURE 8. Comparison of different segments (A). Circumferential tension; (B). Axial tension.
To investigate the effect of gender on the mechanical properties of the aorta, we enrolled 23 patients (12 male and 11 female, mean age = 60.50 years for men and 59.36 years for women), namely, group 3, group 4, and group 5, aged 46–75 years. The fitting parameters and physiological moduli of the samples are listed in Tables 4 and 5. There was no statistical difference in the fitting parameters among the different gender groups. In proximal circumferential stretching, distal circumferential stretching, and distal axial stretching, the failure stress and the failure strain of the male group were all greater than those of the female group (Figure 9).
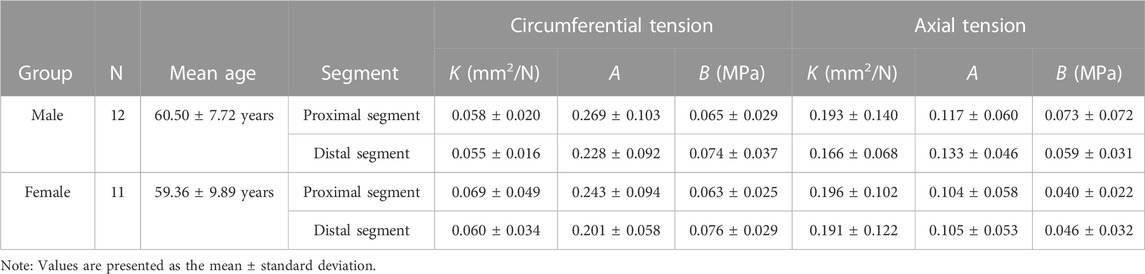
TABLE 4. Mean fitting parameters of different gender groups.
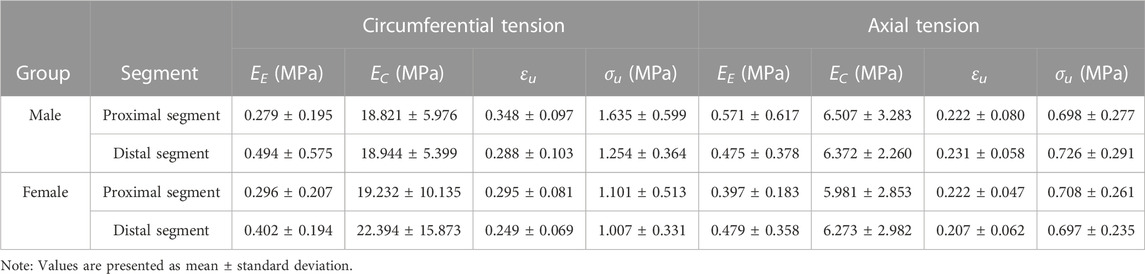
TABLE 5. Mean physiological modulus of the different gender groups.
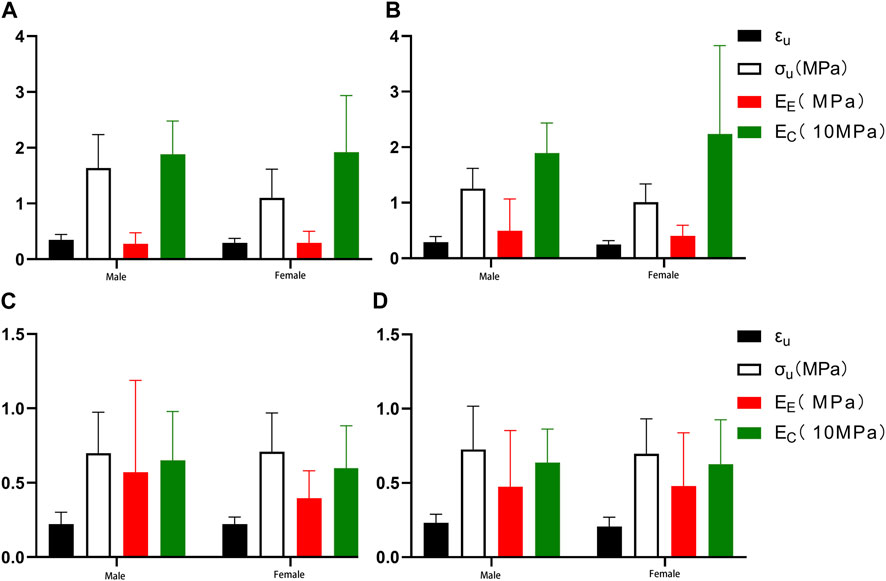
FIGURE 9. Comparing the effects of gender on mechanical parameters. (A) Proximal circumferential tensile; (B). Distal circumferential tensile; (C). Proximal axial tensile; (D). Distal axial tensile.
We used the Levenberg–Marquardt minimization algorithm to fit the mean stress-strain curve for each group in the original data. The Fung-type strain energy function was used to fit the different segments from each age group. Root mean square difference ε) and correlation coefficient (R2) were used to evaluate the fitting degree of the experimental data and the model (Table 6). The fitting degree of the constitutive equation for each segment was satisfactory.
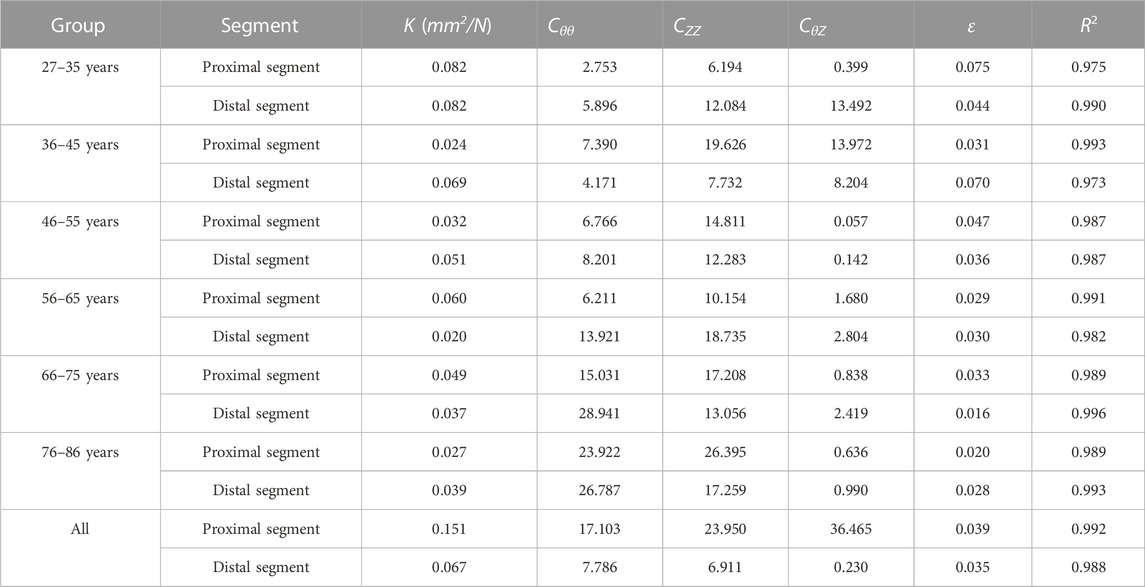
TABLE 6. Constitutive equation parameters of the different segments in the different age groups.
In this study, a total of 50 descending thoracic aortae from Chinese adults in forensic cases were subjected to a uniaxial tensile test. The study found that both model parameters and physiological moduli changed with age, which was consistent with previous studies (Haskett et al., 2010; Sokolis et al., 2017). This is the first systematic study that applies the uniaxial tensile test on the different segments of the Chinese adult descending thoracic aorta of different ages. It also has the largest size of uniaxial tensile samples of the human aorta (non-aortic aneurysm) so far (Mohan and Melvin, 1982; Perejda et al., 1985; Sherebrin et al., 1989; García-Herrera et al., 2012; Ninomiya et al., 2015). We have also worked out the constitutive equations for different ages and segments of the descending thoracic aorta (Table 6), which can be used for biomedical modeling.
In this study, the mean failure stress and failure strain under circumferential tensile of the proximal descending thoracic aorta were 1.511 MPa and 0.394, and those of axial tensile was 0.899 MPa and 0.279 respectively. The mean failure stress and failure strain of circumferential tensile of the distal descending thoracic aorta were 1.350 MPa and 0.393; their values were 0.960 MPa and 0.297 for axial tensile, respectively. Mohan and Melvin (Mohan and Melvin, 1982) reported the mean failure stress and failure strain under quasi-static uniaxial stretching in the middle part of the normal descending thoracic aorta for 19 cases (mean age 54.6 years), where mean values of circumferential stretching were 1.72 MPa and 0.53, and those of axial stretching were 1.47 MPa and 0.47. Both of these sets of values are slightly larger than those measured in this study. Ninomiya et al. (Ninomiya et al., 2015) performed a circumferential uniaxial tensile test on 26 aortas aged 33–89 years old (mean age = 64 years); the mean failure stress and failure strain of descending thoracic aorta were 1.688 MPa and 0.66, respectively. The failure strain was greater than that measured in this study. Sherebrin et al. (Sherebrin et al., 1989) performed a uniaxial tensile test on 23 descending thoracic aortas aged 15–81 years old and reported lower values with mean circumferential and axial failure stresses of 177 kPa and 184 kPa, respectively. Shah et al. (Shah et al., 2006) Performed dynamic biaxial tensile tests on 12 aortas and reported higher values with mean failure stress of 2.07 MPa and failure strain of 0.26 at 1 m/s. These differences may be related to the different ages and sites of samples or different experimental approaches.
This study also found that failure stress and failure strain of both circumferential and axial aortic stretching decreased with age (Figures 5, 6), which is consistent with previous study (Sherebrin et al., 1989). Changes in biomechanical characteristics of tissues are rarely considered in forensic age assessment. As shown in Figure 6, we conducted a linear regression fitting for the failure stress and failure strain in different tensile directions of different segments with age. Age-related changes in the failure stress and failure strain of the descending thoracic aorta might be used as auxiliary methods to evaluate the age of unknown cadavers in forensic practices.
Collagen fibers, elastic fibers, and smooth muscle cells are the main components of the aortic wall, which are directly related to its material properties (Sherebrin et al., 1989). Elastin is an elastic protein with mechanical behavior similar to Hookean material. Collagen fibers, which are stronger than elastic fibers, are arranged in a spiral pattern within the medial membrane of the artery wall. Elastic fibers are responsible for the elastic properties of the aorta, while collagen fibers provide mechanical strength (Sherebrin et al., 1989).
The contents and moduli of elastic and collagen fibers in the aortic wall vary widely in the literature. Ninomiya et al. (Ninomiya et al., 2015) found that the content of collagen fibers in the aortic wall was positively correlated with and increased with age, while the elastic fibers did not. Wuyts et al. (Wuyts et al., 1995) proposed a circumferential stress-strain mathematical model based on the vascular wall structure and fitted the aortic stretching data in the literature by Langewouters et al. (Langewouters et al., 1984). The mean value of the elastic modulus of thoracic aortic elastic fibers calculated by model parameters was 0.532 MPa, and the mean value of the elastic modulus of collagen fiber was 300 MPa. The elastic modulus of elastic fiber decreases with age, while that of collagen fiber increases. By establishing the strain energy function model of the aorta, Zulliger et al. (Zulliger and Stergiopulos, 2007) analyzed the data in the literature of Langewouters et al. (Langewouters et al., 1984). They fixed the elastic modulus of collagen fiber at 200 MPa and found the mean elastic modulus of elastic fiber was 0.06 MPa. It was concluded that the elastic modulus of the aortic elastic fibers is not age-related, and the main reason for the decrease in aortic elasticity is a change in the collagen fiber network with age, which affects the aortic mechanical properties.
This study calculated the elastic modulus of elastic fibers and collagen fibers to be 0.271 MPa and 25.335 MPa in the circumferential direction of the proximal end, and 0.440 MPa and 8.540 MPa in the axial direction. The circumferential and axial stretches of the distal end were 0.356 MPa and 22.776 MPa, and 0.386 MPa and 7.777 MPa, respectively. As shown in Figure 4, the elastic modulus of elastic fibers increases with age, while the elastic modulus of collagen fibers decreases with age. This may be due to the loss of elastic fibers with age, and the earlier involvement of collagen fibers in mechanical bearing, resulting in an increase in the modulus of elastic fibers calculated by the model with age. For collagen fibers, this study calculated the maximum modulus from stretching to fracture. As the age increases, the failure stress and strain also decrease. The final result is that the slope of the stress-strain curve before failure increases with age. Therefore, the calculated collagen fiber modulus is smaller than that in the literature, and it decreases with age.
In this study, the mean failure strain, failure stress, and elastic modulus of collagen fiber of each group in circumferential stretching were larger than that of axial stretching. In addition, as shown in Figure 7, the elastic modulus of the elastic fiber was smaller than that of axial stretching (no significant difference at the distal segment). This is consistent with most studies in the literature (Langewouters et al., 1984).
The aorta is composed of intima, media, and adventitia. The mechanical response of aortic anisotropy is due to the different alignment of elastic fibers and collagen fibers (Sokolis, 2023). Both fiber families are approximately circumferential in the media, longitudinal in the adventitia, and relatively evenly distributed in the intima (Sokolis, 2023). Therefore, its response is orthotropic and can be considered to originate from fiber-reinforced material (Holzapfel et al., 2000; Holzapfel, 2006). The circumferential stretching of the arterial wall has larger values of failure strain and failure stress; the elastic modulus of collagen fibers is also higher. The elastic modulus of elastic fiber in circumferential stretching is smaller than that in axial stretching, which may be related to the involvement of passive loading of collagen fiber in axial stretching. Thus, a circumferential bias of fibers orientation in the media is the basis for the anisotropic behavior of the aorta. Haskett et al. (Haskett et al., 2010)found that the fiber direction of the aorta is mainly circumferential at all positions and ages. With increasing age, both circumferential and axial fiber stiffness will increase, making it easier for the aorta to fail.
Currently, no studies exist on the comparison of different parts of the human descending thoracic aorta using the uniaxial tensile test. In most relevant studies (Mohan and Melvin, 1982; Sherebrin et al., 1989; García-Herrera et al., 2012; Ninomiya et al., 2015), the mechanical properties of different parts of the descending thoracic aorta are presumed to be isotropic. Ninomiya et al. (Ninomiya et al., 2015) conducted a circumferential uniaxial tensile test on the thoracic and abdominal aorta and found that the descending thoracic aorta had higher strength and elasticity than the abdominal aorta. In this study, the descending thoracic aorta was divided into the proximal and the distal segments; circumferential and axial uniaxial tensile tests were performed, respectively, to calculate the model parameters, failure strain, failure stress, as well as the elastic modulus of elastic fiber and collagen fiber. No statistical differences were observed between the proximal and distal descending thoracic aorta (Figure 8).
Gender differences in the occurrence, development, treatment, and prognosis of cardiovascular diseases have attracted more and more attention (Chung et al., 2020). Although women are less likely to develop thoracic aortic aneurysms, they are three times more likely than men to have a dissection or rupture (Davies et al., 2002). The risk of rupture and death in women is 4 times higher than that in men (Dimick et al., 2002; Brown et al., 2003), and the incidence of postoperative complications is nearly 3 times greater than that in men (Wolf et al., 2002). It can be seen that although aortic aneurysm is more common in men, female aortic aneurysm patients have a higher risk of rupture and a worse clinical prognosis. The underlying mechanism of this gender difference is still not fully understood.
Our study showed that the failure stress and failure strain in the male group were greater than in the female group. This was especially true for proximal circumferential stretching, distal circumferential stretching, and distal axial stretching. There were statistically significant differences in the failure stresses of proximal circumferential tensile, while no statistically significant differences were noted for others (Figure 9). This is similar to the results of Ninomiya et al. (Ninomiya et al., 2015), who conducted circumferential uniaxial tensile tests on the descending thoracic aorta and abdominal aorta of 9 males and 9 females. Although dissection is more frequent in males than in females, Sokolis et al. (Sokolis and Papadodima, 2022) found that there is no gender-related effect on the delamination properties of the aorta. In terms of circumferential residual strain, females and males have similar opening angle and residual stretches (Sokolis et al., 2017). Sokolis et al. (Sokolis and Iliopoulos, 2014) provides a molecular explanation for this gender difference. Higher levels of matrix metalloproteinase (MMP)-2 and MMP-9, which can degrade and reconstruct arterial walls, and lower expression of tissue inhibitors of metalloproteinase (TIMP-1) and TIMP-2 in the females than in the male, may lead to increased degradation and decreased strength of the aortic extracellular matrix in females. Gender differences in aortic biomechanics may contribute to the greater risk of aortic aneurysm rupture and worse clinical prognosis in women than in men.
The aortic wall is anisotropic and should ideally stretch in multiple directions simultaneously to mimic physiological conditions rather than with uniaxial tension. However, biaxial tension, for example, puts a higher demand on the specimen and equipment, and it is difficult to detect the failure of the specimen due to the small range of strain measurement. Therefore, uniaxial tension is still the dominant method for performing aortic mechanical tests.
Collecting human aorta is challenging, and obtaining an ideal age and gender distribution is difficult. The six age groups were not matched by gender. Futhermore, there were no samples for infants and adolescents under 26 years old in our study. The material properties of the aorta in infants and adolescents may differ from those of adults. We will thus continue to collect aortic specimens of different age group and perform further tensile tests.
Our study focused on the mechanical behavior of healthy aortas and excluded the arterial plaque and the aortic ostia. In the future, we will compare and study the biomechanical differences between the arterial tissue at the atherosclerotic site, tissue at the ostia, and the healthy aortic tissue, to provide data for abnormal aortic mechanical parameters.
Our study is the first uniaxial tensile test on the adult descending thoracic aorta of different ages and segments. It has the largest sample size of the human aorta (non-aortic aneurysm) subjected to uniaxial tensile tests so far. The model parameters, failure stress, failure strain, elastic modulus of elastic fiber, and elastic modulus of collagen fiber in different thoracic aortic segments of 50 adults were obtained, and the differences between groups and gender were statistically analyzed. Additionally, the Fung hyperelastic constitutive equations of the different segments of the descending thoracic aorta in different age groups were fitted, which can be used by biomedical engineers for modeling.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by Ethics Committee of the Academy of Forensic Science (Ministry of Justice, China). The patients/participants provided their written informed consent to participate in this study.
Conceptualization, ZL and MP; methodology, ZL and MP; formal analysis JZ and NL; writing—original draft preparation, MP; supervision, JW and DZ; project administration, ZL and JW; funding acquisition, DZ and ZL. All authors contributed to the article and approved the submitted version.
The study was financially supported by grants from the National Key Research and Development Plan (Grant No. 2022YFC3302002), National Natural Science Foundation of China (82171872), Natural Science Foundation of Shanghai (21ZR1464600), Shanghai Key Laboratory of Forensic Medicine (21DZ2273200), Shanghai Forensic Service Platform (19DZ2290900), Central Research Institute Public Project (GY2020G-4 and GY2021G-5).
The authors would like to extend special thanks to the editor and reviewers for their constructive comments and suggestions for improving the quality of this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fbioe.2023.1178199/full#supplementary-material
Bass, C. R., Darvish, K., Bush, B., Crandall, J. R., Srinivasan, S. C., Tribble, C., et al. (2001). Material properties for modeling traumatic aortic rupture. Stapp Car Crash J. 45, 143–160. doi:10.4271/2001-22-0006
Brown, P. M., Zelt, D. T., and Sobolev, B. (2003). The risk of rupture in untreated aneurysms: The impact of size, gender, and expansion rate. J. Vasc. Surg. 37 (2), 280–284. doi:10.1067/mva.2003.119
Chung, J., Coutinho, T., Chu, M. W., and Ouzounian, M. (2020). Sex differences in thoracic aortic disease: A review of the literature and a call to action. J. Thorac. Cardiovasc. Surg. 160 (3), 656–660. doi:10.1016/j.jtcvs.2019.09.194
Chuong, C. J., and Fung, Y. C. (1983). Three-dimensional stress distribution in arteries. J. biomechanical Eng. 105 (3), 268–274. doi:10.1115/1.3138417
Davies, R. R., Goldstein, L. J., Coady, M. A., Tittle, S. L., Rizzo, J. A., Kopf, G. S., et al. (2002). Yearly rupture or dissection rates for thoracic aortic aneurysms: Simple prediction based on size. Ann. Thorac. Surg. 73 (1), 17–28. doi:10.1016/s0003-4975(01)03236-2
Dimick, J. B., Stanley, J. C., Axelrod, D. A., Kazmers, A., Henke, P. K., Jacobs, L. A., et al. (2002). Variation in death rate after abdominal aortic aneurysmectomy in the United States: Impact of hospital volume, gender, and age. Ann. Surg. 235 (4), 579–585. doi:10.1097/00000658-200204000-00017
Ferrara, A., Morganti, S., Totaro, P., Mazzola, A., and Auricchio, F. (2016). Human dilated ascending aorta: Mechanical characterization via uniaxial tensile tests. J. Mech. Behav. Biomed. Mater. 53, 257–271. doi:10.1016/j.jmbbm.2015.08.021
Ferrara, A., Totaro, P., Morganti, S., and Auricchio, F. (2018). Effects of clinico-pathological risk factors on in-vitro mechanical properties of human dilated ascending aorta. J. Mech. Behav. Biomed. Mater. 77, 1–11. doi:10.1016/j.jmbbm.2017.08.032
García-Herrera, C. M., Atienza, J. M., Rojo, F. J., Claes, E., Guinea, G. V., Celentano, D. J., et al. (2012). Mechanical behaviour and rupture of normal and pathological human ascending aortic wall. Med. Biol. Eng. Comput. 50 (6), 559–566. doi:10.1007/s11517-012-0876-x
Grootenboer, N., Bosch, J., Hendriks, J., and van Sambeek, M. (2009). Epidemiology, aetiology, risk of rupture and treatment of abdominal aortic aneurysms: Does sex matter? Eur. J. Vasc. Endovascular Surg. 38 (3), 278–284. doi:10.1016/j.ejvs.2009.05.004
Guinea, G. V., Atienza, J. M., Rojo, F. J., García-Herrera, C. M., Yiqun, L., Claes, E., et al. (2010). Factors influencing the mechanical behaviour of healthy human descending thoracic aorta. Physiol. Meas. 31 (12), 1553–1565. doi:10.1088/0967-3334/31/12/001
Hans, S. S., Jareunpoon, O., Balasubramaniam, M., and Zelenock, G. B. (2005). Size and location of thrombus in intact and ruptured abdominal aortic aneurysms. J. Vasc. Surg. 41 (4), 584–588. doi:10.1016/j.jvs.2005.01.004
Haskett, D., Johnson, G., Zhou, A., Utzinger, U., and Vande Geest, J. (2010). Microstructural and biomechanical alterations of the human aorta as a function of age and location. Biomechanics Model. Mechanobiol. 9 (6), 725–736. doi:10.1007/s10237-010-0209-7
Hiller, R. J., Mikocka-Walus, A. A., and Cameron, P. A. (2010). Aortic transection: Demographics, treatment and outcomes in victoria, Australia. Emerg. Med. J. 27 (5), 368–371. doi:10.1136/emj.2009.075978
Holzapfel, G. A. (2006). Determination of material models for arterial walls from uniaxial extension tests and histological structure. J. Theor. Biol. 238 (2), 290–302. doi:10.1016/j.jtbi.2005.05.006
Holzapfel, G. A., Gasser, T. C., and Ogden, R. W. (2000). A new constitutive framework for arterial wall mechanics and a comparative study of material models. J. Elast. Phys. Sci. solids 61 (1), 1–48. doi:10.1023/a:1010835316564
Iliopoulos, D. C., Kritharis, E. P., Boussias, S., Demis, A., Iliopoulos, C. D., and Sokolis, D. P. (2013). Biomechanical properties and histological structure of sinus of Valsalva aneurysms in relation to age and region. J. biomechanics 46 (5), 931–940. doi:10.1016/j.jbiomech.2012.12.004
Kent, K. C. (2014). Abdominal aortic aneurysms. N. Engl. J. Med. 371 (22), 2101–2108. doi:10.1056/nejmcp1401430
Langewouters, G. J., Wesseling, K. H., and Goedhard, W. (1984). The static elastic properties of 45 human thoracic and 20 abdominal aortas in vitro and the parameters of a new model. J. biomechanics 17 (6), 425–435. doi:10.1016/0021-9290(84)90034-4
Lederle, F. A., Wilson, S. E., Johnson, G. R., Reinke, D. B., Littooy, F. N., Acher, C. W., et al. (2002). Immediate repair compared with surveillance of small abdominal aortic aneurysms. N. Engl. J. Med. 346 (19), 1437–1444. doi:10.1056/nejmoa012573
Mohan, D., and Melvin, J. W. (1982). Failure properties of passive human aortic tissue. I—uniaxial tension tests. J. biomechanics 15 (11), 887–902. doi:10.1016/0021-9290(82)90055-0
Neschis, D. G., Scalea, T. M., Flinn, W. R., and Griffith, B. P. (2008). Blunt aortic injury. N. Engl. J. Med. 359 (16), 1708–1716. doi:10.1056/nejmra0706159
Ninomiya, O. H., Tavares Monteiro, J. A., Higuchi, M. d. L., Puech-Leão, P., de Luccia, N., Raghavan, M. L., et al. (2015). Biomechanical properties and microstructural analysis of the human nonaneurysmal aorta as a function of age, gender and location: An autopsy study. J. Vasc. Res. 52 (4), 257–264. doi:10.1159/000442979
Pei, M., Zou, D., Gao, Y., Zhang, J., Huang, P., Wang, J., et al. (2021). The influence of sample geometry and size on porcine aortic material properties from uniaxial tensile tests using custom-designed tissue cutters, clamps and molds. PLoS One 16 (2), e0244390. doi:10.1371/journal.pone.0244390
Perejda, A. J., Abraham, P. A., Carnes, W. H., Coulson, W. F., and Uitto, J. (1985). Marfan's syndrome: Structural, biochemical, and mechanical studies of the aortic media. J. laboratory Clin. Med. 106 (4), 376–383.
Pichamuthu, J. E., Phillippi, J. A., Cleary, D. A., Chew, D. W., Hempel, J., Vorp, D. A., et al. (2013). Differential tensile strength and collagen composition in ascending aortic aneurysms by aortic valve phenotype. Ann. Thorac. Surg. 96 (6), 2147–2154. doi:10.1016/j.athoracsur.2013.07.001
Raghavan, M. L., Hanaoka, M. M., Kratzberg, J. A., Higuchi, M. d. L., and da Silva, E. S. (2011). Biomechanical failure properties and microstructural content of ruptured and unruptured abdominal aortic aneurysms. J. biomechanics 44 (13), 2501–2507. doi:10.1016/j.jbiomech.2011.06.004
Raghavan, M. L., Webster, M. W., and Vorp, D. A. (1996). Ex vivo biomechanical behavior of abdominal aortic aneurysm: Assessment using a new mathematical model. Ann. Biomed. Eng. 24 (5), 573–582. doi:10.1007/bf02684226
Sacks, M. S., and Sun, W. (2003). Multiaxial mechanical behavior of biological materials. Annu. Rev. Biomed. Eng. 5 (1), 251–284. doi:10.1146/annurev.bioeng.5.011303.120714
Shah, C. S., Hardy, W. N., Mason, M. J., Yang, K. H., Van Ee, C. A., Morgan, R., et al. (2006). Dynamic biaxial tissue properties of the human cadaver aorta. Stapp Car Crash J. 50, 217–246. doi:10.4271/2006-22-0010
Sherebrin, M. H., Hegney, J. E., and Roach, M. R. (1989). Effects of age on the anisotropy of the descending human thoracic aorta determined by uniaxial tensile testing and digestion by NaOH under load. Can. J. physiology Pharmacol. 67 (8), 871–878. doi:10.1139/y89-136
Sokolis, D. P., Gouskou, N., Papadodima, S. A., and Kourkoulis, S. K. (2021). Layer-specific residual deformations and their variation along the human aorta. J. Biomechanical Eng. 143 (9), 094504. doi:10.1115/1.4050913
Sokolis, D. P., and Iliopoulos, D. C. (2014). Impaired mechanics and matrix metalloproteinases/inhibitors expression in female ascending thoracic aortic aneurysms. J. Mech. Behav. Biomed. Mater. 34, 154–164. doi:10.1016/j.jmbbm.2014.02.015
Sokolis, D. P., Kritharis, E. P., Giagini, A. T., Lampropoulos, K. M., Papadodima, S. A., and Iliopoulos, D. C. (2012). Biomechanical response of ascending thoracic aortic aneurysms: Association with structural remodelling. Comput. methods biomechanics Biomed. Eng. 15 (3), 231–248. doi:10.1080/10255842.2010.522186
Sokolis, D. P. (2023). Layer-specific tensile strength of the human aorta: Segmental variations. J. Biomechanical Eng. 145 (6), 064502. doi:10.1115/1.4056748
Sokolis, D. P., and Papadodima, S. A. (2022). Regional delamination strength in the human aorta underlies the anatomical localization of the dissection channel. J. Biomechanics 141, 111174. doi:10.1016/j.jbiomech.2022.111174
Sokolis, D. P. (2007). Passive mechanical properties and structure of the aorta: Segmental analysis. Acta physiol. 190 (4), 277–289. doi:10.1111/j.1748-1716.2006.01661.x
Sokolis, D. P., Savva, G. D., Papadodima, S. A., and Kourkoulis, S. K. (2017). Regional distribution of circumferential residual strains in the human aorta according to age and gender. J. Mech. Behav. Biomed. Mater. 67, 87–100. doi:10.1016/j.jmbbm.2016.12.003
Sulejmani, F., Pokutta-Paskaleva, A., Ziganshin, B., Leshnower, B., Iannucci, G., Elefteriades, J., et al. (2017). Biomechanical properties of the thoracic aorta in Marfan patients. Ann. Cardiothorac. Surg. 6 (6), 610–624. doi:10.21037/acs.2017.09.12
Teixeira, P. G., Inaba, K., and Barmparas, G. (2011). Blunt thoracic aortic injuries: An autopsy study. J. Trauma 70 (1), 581–202. doi:10.1016/j.jvs.2011.06.087
Vallabhaneni, S. R., Gilling-Smith, G. L., How, T. V., Carter, S. D., Brennan, J. A., and Harris, P. L. (2004). Heterogeneity of tensile strength and matrix metalloproteinase activity in the wall of abdominal aortic aneurysms. J. Endovascular Ther. 11 (4), 494–502. doi:10.1583/04-1239.1
Vito, R. P., and Dixon, S. A. (2003). Blood vessel constitutive models—1995–2002. Annu. Rev. Biomed. Eng. 5 (1), 413–439. doi:10.1146/annurev.bioeng.5.011303.120719
Vorp, D. A., Schiro, B. J., Ehrlich, M. P., Juvonen, T. S., Ergin, M., and Griffith, B. P. (2003). Effect of aneurysm on the tensile strength and biomechanical behavior of the ascending thoracic aorta. Ann. Thorac. Surg. 75 (4), 1210–1214. doi:10.1016/s0003-4975(02)04711-2
Watanabe, K., Fukuda, I., and Asari, Y. (2013). Management of traumatic aortic rupture. Surg. today 43, 1339–1346. doi:10.1007/s00595-012-0471-7
Wolf, Y. G., Arko, F. R., Hill, B. B., Olcott, C., Harris, E., Fogarty, T. J., et al. (2002). Gender differences in endovascular abdominal aortic aneurysm repair with the AneuRx stent graft. J. Vasc. Surg. 35 (5), 882–886. doi:10.1067/mva.2002.123754
Wuyts, F. L., Vanhuyse, V. J., Langewouters, G. J., Decraemer, W. F., Raman, E. R., and Buyle, S. (1995). Elastic properties of human aortas in relation to age and atherosclerosis: A structural model. Phys. Med. Biol. 40 (10), 1577–1597. doi:10.1088/0031-9155/40/10/002
Keywords: human aorta, uniaxial tensile test, digital image correlation, material properties, material constitutive model
Citation: Li Z, Pei M, Zhang J, Liu N, Wang J and Zou D (2023) A study to characterize the mechanical properties and material constitution of adult descending thoracic aorta based on uniaxial tensile test and digital image correlation. Front. Bioeng. Biotechnol. 11:1178199. doi: 10.3389/fbioe.2023.1178199
Received: 02 March 2023; Accepted: 05 June 2023;
Published: 14 June 2023.
Edited by:
Yang Liu, Hong Kong Polytechnic University, Hong Kong SAR, ChinaReviewed by:
Dimitrios Sokolis, Biomedical Research Foundation of the Academy of Athens (BRFAA), GreeceCopyright © 2023 Li, Pei, Zhang, Liu, Wang and Zou. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhengdong Li, bGl6ZEBzc2ZqZC5jbg==; Jinming Wang, d2FuZ2ptQHNzZmpkLmNu; Donghua Zou, em91ZGhAc3NmamQuY24=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.