 Mathieu Hotton
Mathieu Hotton Loonan Chauvette1
Loonan Chauvette1 Jean-Pierre Gagné
Jean-Pierre Gagné- 1School of Rehabilitation Sciences, Laval University, Québec, QC, Canada
- 2Centre interdisciplinaire de recherche en réadaptation et intégration sociale, Québec, QC, Canada
- 3School of Speech-Language Pathology and Audiology, University of Montréal, Montréal, QC, Canada
- 4Centre de recherche de l'Institut universitaire de gériatrie de Montréal, Montréal, QC, Canada
Introduction: Few clinical protocols are presently available to guide hearing healthcare professionals who are responsible for conducting comprehensive audiological needs assessments with their clients. The Québec Audiological Assessment Protocol for Younger and Older Adults (QAAP-YOA) was recently developed for this purpose. This pilot study is the third phase in the development of the QAAP-YOA. Its objective was to assess the implementation of the QAAP-YOA in clinical settings.
Methods: Audiologists (n = 5) and adults with hearing loss (n = 29) participated in the study. Audiologists were trained to use the QAAP-YOA. Then, they administered the QAAP-YOA to clients. Needs assessment reports and QAAP-YOA clinical tools written by audiologists following these assessments were analyzed. Data related to the audiologists' workflow were collected. Individual semi-structured interviews were also conducted with participants to explore their experience.
Results: Audiologists judged the QAAP-YOA relevant and useful. It allowed them to perform more comprehensive and consistent needs assessments, and to formulate more adequate recommendations. Compliance ratings for assessment reports were higher after training (p < 0.001), particularly when the clinical tool was used. Participants were satisfied with the QAAP-YOA, but longer appointments and additional time for record keeping was required to implement it.
Conclusions: Audiologists can benefit from using the QAAP-YOA. Digitalizing the clinical tool may help reduce the time required to administer the procedure, facilitate its use and allow for possibility of adapting the protocol to specific clientele and work settings.
1 Introduction
Hearing loss often results in functional challenges in the daily life of individuals. The environment in which they navigate, and their personal characteristics may influence the nature and extent of the difficulties they experience. As is often seen in the clinic, two clients with similar hearing impairments may seek the help of a hearing healthcare (HHC) professional for completely distinct hearing related difficulties. HHC professionals are thus required to assess the needs of their clients to elaborate a treatment or intervention plan that is appropriately tailored to each person. That plan must consider the order in which the altered life habits or activities will be addressed, based on the client's needs and expressed priorities. Improved outcomes are achieved when the treatment or intervention plan takes into account the clients' individual needs (Grenness et al., 2014; Hickson et al., 2014).
Even though the needs assessment is an important component of the audiological evaluation, few clinical protocols or tools are available to guide HHC professionals who are responsible for conducting a comprehensive needs assessment with clients. Some professional organizations such as the British Society of Audiology (BSA) and the American Academy of Audiology (AAA) discussed the needs assessment in the context of hearing rehabilitation or hearing aid fitting (Ferguson et al., 2016; Valente et al., 2006). Other authors proposed practical tools to facilitate the needs assessment with hearing-impaired individuals (Atcherson et al., 2015; IDA Institute, 2009; van Leeuwen et al., 2020). However, those guidelines and tools are generally limited in the scope of their recommendations, and they do not propose a way to assess audiological needs that is personalized, standardized and clinically validated.
Recently, Hotton and Gagné (2022) developed the Québec Audiological Assessment Protocol for Younger and Older Adults (QAAP-YOA). This protocol implements a structured approach to conduct a comprehensive needs assessment with adults of all ages, within a perspective of setting rehabilitation goals and developing an appropriate intervention program. It integrates the International Classification of Functioning, Disability and Health (ICF) framework (World Health Organization, 2001) and it is compatible with the principles of a client-centered approach (Grenness et al., 2014) and of goal setting (Mckenna, 1987). Its administration, using a semi-structured interview approach, is conceived to be flexible and adapted to everyone regardless of the person's age, personal characteristics, and specific environment in which hearing difficulties are experienced. The five domains covered in the protocol are: (1) Audiological needs (activity limitations, participation restrictions, and environmental factors), (2) Living conditions (social networks and living environment), (3) Personal factors (motivation, dexterity, cognition, etc.), (4) Discussion with the client concerning the goals of the treatment program and the intervention strategies retained, and (5) Formulation of recommendations (Hotton and Gagné, 2022).
The QAAP-YOA protocol can be used with an accompanying clinical tool, which consists of a form that contains open and closed-set questions as well as checklists. It follows the structure, sections and items of the needs assessment protocol. It is intended to be used by the professional to guide the interview with the client and to serve as a checklist of the issues that should be discussed. The completed form may be used to summarize the results of the assessment and be placed in the client's file. The use of the clinical tool is optional. Depending on the clinical setting, type of practice, other clinical tools used, and the client's individual profile, the audiologist may choose not to use it. In those circumstances, the results of the needs assessment protocol are summarized in the audiological report. Because they are not standardized test procedures, no score is computed when the QAAP-YOA and its accompanying clinical tool are administered. The approach proposed by the QAAP-YOA is descriptive and personalized. For more information about the development of the QAAP-YOA, its accompanying clinical tool, and how to use them, the reader is referred to Hotton and Gagné (2022).
A pilot study was undertaken to measure the efficacy of the QAAP-YOA for assessing the needs of individuals with hearing loss in a simulated clinical context (Hotton et al., 2024). A related goal was to examine the added value procured by using the accompanying clinical tool in relation to the appropriateness of the conclusions reached by participants. Eleven audiology students and four early-career audiologists (n = 15) completed two needs assessments with simulated clients and wrote audiological reports, while applying the QAAP-YOA with and without the use of its clinical tool. The audiological assessments were filmed, and the written reports collected. Results revealed that the protocol was easily applicable during the needs assessment interview following a brief 2 h training session. The use of the clinical tool did not influence the interview process since participants complied to the protocol similarly in both experimental conditions. However, in the written reports the compliance to the protocol was higher, and the information provided was more elaborate and coherent with the client's needs when participants used the clinical tool during the needs assessment. The authors concluded that the use of the QAAP-YOA can lead to a greater standardization of needs assessments and to more comprehensive reports, which in turn may lead to intervention programs that are more closely aligned with clients' needs.
As the pilot assessment of the QAAP-YOA completed by Hotton et al. (2024) was conducted in a simulated clinical context, the next step in its development was to assess the use of the QAAP-YOA and its clinical tool in clinical settings, with real clients and practicing professionals. Therefore, the study presented in this article had the following research objectives: (1) to measure the audiologists' compliance to the QAAP-YOA during the needs assessment process, (2) to describe the impacts of the QAAP-YOA implementation on the audiologists' workflow in a real clinical setting, (3) to describe the experience of audiologists and clients during the QAAP-YOA implementation in terms of satisfaction, benefits, and drawbacks, and (4) to identify possible modifications that could improve the protocol and clinical tool.
2 Materials and methods
2.1 Research design
A mixed-methods research design combining quantitative and qualitative data sources was used (Creswell, 2009). Quantitative data were gathered concerning the audiologists' workflow and samples of written reports were collected from each audiologist before and after the implementation of the QAAP-YOA. Quantitative data were analyzed descriptively, and statistical analyses were completed when appropriate. In addition, qualitative data were gathered after the trial by interviewing participating audiologists and clients who underwent an audiological evaluation with the QAAP-YOA. Data from the interviews were analyzed following a qualitative content analysis methodology.
2.2 Participants
Initially, 15 practicing audiologists agreed to take part in the investigation. This number of participants was considered appropriate based on previous research on the QAAP-YOA during which the same measurement tools were used (Hotton et al., 2024). However, due to reasons associated with the COVID-19 pandemic, 10 participant-audiologists withdrew from the study. Thus, a complete data set is available for five audiologists (two males and three females). The mean age of the audiologists was 37.0 ± 7.8 years, and they had an average of 11.4 ± 8.0 years of clinical experience. Two audiologists worked in a public hospital, and three worked in private clinics, all located in the Province of Québec, Canada. In the context of the public health system in place in Québec, those workplaces represent the most common clinical setting where a majority of the audiologists work, and are considered as first-line audiology clinics, where most people generally go for hearing assessments, hearing loss diagnosis, follow-up and first-line hearing rehabilitation (in comparison with second-line, specialized hearing rehabilitation clinics offering multidisciplinary, more comprehensive services to people with a diagnosed hearing loss who experience more severe functional limitations). Participating audiologists were all registered members of the Ordre des orthophonistes et audiologistes du Québec (OOAQ).
A total of 29 clients (19 men and 10 women) participated in the study. The recruitment target for participating clients was 10 per participating audiologist to allow these latter to gain sufficient experience with the protocol during the trial. However, it was not possible to reach those numbers, again, because of restrictions related to the COVID-19 pandemic. Participating clients had a mean age of 69.2 ± 14.4 years and lived in 7 different regions of the Province of Québec. Most clients (n = 21) had undergone one or more previous audiologic evaluations, and seven of the participants were undergoing their first audiological assessment during the study (the previous experience with audiology consultation was not available for one participant). Most participating clients mentioned having a diagnosed hearing loss for more than 5 years (n = 18). The mean pure tone average (500, 1,000, 2,000 Hz) of the clients' group was 47.4 ± 20.0 dB HL in the left ear and 52.3 ± 22.0 dB HL in the right ear. The main reported causes of hearing impairment were work-related noise exposure (n = 9) and age-related hearing loss (n = 6). Most client-participants were retired (n = 17) while some had a paid employment (n = 11). One client-participant reported being unemployed. Most were already fitted with hearing aids (n = 20), while some had no prior hearing aid experience (n = 9). The primary reason for consultation was most often hearing monitoring (n = 22). Most participating clients live autonomously in their house (n = 17) or an apartment (n = 7). All participants (audiologists and clients) used French as their main language of communication. Therefore, all needs assessments were conducted in French during the project.
2.3 Procedures
Participating audiologists first provided to the research team deidentified copies of three needs assessment reports from past clients that they had written within the 6 months preceding their involvement in the study. These reports presented the needs assessment they typically conducted before they were exposed to the QAAP-YOA and trained on how to apply it. The compliance of these reports to the protocol requirements was then assessed by two independent examinators with an evaluation grid specifically designed for this purpose (Hotton et al., 2024). In addition, a short 5 min questionnaire was administered to each participating audiologist. This questionnaire was designed to provide a description of their typical work routine.
Then, the audiologists were trained on the application of the protocol and clinical tool. The training consisted of three online self-learning modules for a total duration of ~2 h. The training program addressed the issue of how to apply the protocol and how to use the accompanying clinical tool. After completing the training program, the audiologists were instructed to apply the protocol using the clinical tool with clients willing to participate in the study, over a 1 month period. Participating audiologists therefore recruited clients and conducted the needs assessment using the new protocol and its accompanying tool in their usual clinical setting as part of their usual audiologic evaluation. At the end of the trial period, for five typical workdays, the audiologist had to fill-in the same short questionnaire requesting information about their practice, as mentioned above. Additionally, they were asked to provide an estimate of the additional amount of time required to administer the protocol and complete the clinical tool (in comparison to their usual needs assessments and report writing). Finally, audiologists had to submit de-identified copies of all the needs assessment reports written during the trial, including the filled-in clinical tools. Three of these reports from each audiologist were randomly selected for further evaluation of protocol compliance using the same evaluation grid previously described.
Once the field study was completed individual semi-structured interviews were conducted with all five participating audiologists. Some of the participating clients were also contacted to participate in an individual semi-structured interview. A minimum of one client was interviewed by participating audiologist. Due to the unexpected circumstances of the COVID-19 pandemic, leading to a high level of withdrawal on the part of the participant audiologists, and because interviews with clients had to be completed within 1 week after the audiology appointment (to reduce the possibility of a memory bias), it was possible to reach a total of six clients to complete the interview process. All interviews with participating audiologists and clients were conducted by phone or videoconference, by the same researcher to reduce variability and social-desirability bias. All the interviews were recorded for a posteriori analysis and lasted between 30 and 60 min.
2.4 Outcome measures
An evaluation grid was used to measure the audiologists' compliance to the protocol. The grid used was the same as the one employed in a previous study (see Hotton et al., 2024). The scoring grid for the written report incorporated 10 key elements of the protocol that were expected to be addressed in the written report. Each of the 10 items was scored on a scale from 1 to 5 points (1 indicating total disagreement and 5 indicating total agreement). A total score was obtained by adding the total number of points obtained for one report. That score represented the degree of conformity of the participating audiologist's performance regarding the QAAP-YOA recommendations (refer to Hotton et al., 2024 for more details on the content of the grid and scoring procedure). For each report, the evaluation grid was scored by two independent experienced audiologists who had over 10 years of clinical experience and a good knowledge of the QAAP-YOA. The final score was calculated by averaging the total scores attributed by each assessor then converted in a percentage of adherence to the QAAP-YOA. In the context of this study, compliance was defined as the participants' ability to adhere to the QAAP-YOA while writing its reports. Therefore, a 100% compliance rating for reports corresponded to a total adherence to the QAAP-YOA requirements. Compliance ratings for the written reports were obtained for the two experimental conditions: (1) pre-experimental condition (control, usual condition), and (2) post-experimental condition (with the use of the protocol and clinical tool). In the post-experimental condition, for each participating-audiologist, three different report ratings were computed: (a) the written report by itself, (b) the filled-in clinical tool by itself, and (c) the score obtained when the information contained in the written report and the clinical tool were amalgamated together.
The quantitative data that addressed the office workflow were collected using a questionnaire that each audiologist had to fill-in before and after the trial. This questionnaire was completed on five different workdays prior completing the training session on the QAAP-YOA and on five different workdays during which the audiologists applied the QAAP-YOA. The questionnaire addressed: the number of clients seen in the day, the total time spent in direct interaction with clients, the total time spent managing clinical files (i.e., interventions in the absence of the client such as searching for information, consulting the client record, consulting with a partner, etc.), and the total time spent writing audiologic reports or filling clinical forms. The questionnaire used for the post-experimentation inquiry contained an additional question about the additional time required to administer the protocol and complete the clinical tool (in comparison with their usual needs assessments and report writing).
Two interview grids were also prepared to guide semi-structured interviews with participating audiologists and clients. The interview grid for participating audiologists covered the following topics: the relevance, the usefulness, the benefits and disadvantages of using the QAAP-YOA and accompanying clinical tool; any modifications suggested to improve the implementation of the protocol; the overall satisfaction of audiologists regarding this new assessment protocol; perceived facilitators and barriers to the implementation of the protocol and clinical tool; and audiologists' perceived needs for further support to adapt their practice according to the new protocol. The interview grid for participating clients also included the relevance, the usefulness, the benefits and disadvantages of the use of the QAAP-YOA and accompanying clinical tool; the modifications suggested to improve the implementation of the protocol; and the overall satisfaction of clients regarding this new assessment protocol. It also included specific questions to establish if the clinician's assessment of their needs appeared to be consistent with the protocol. All materials used in the present study were in Canadian French. The English versions of the two interview grids for participating audiologists and clients are provided in Appendices 1 and 2, respectively.
2.5 Data analysis
A descriptive analysis of quantitative data collected (including socio-demographic and workflow data) before and after the trial was conducted. Non-parametric Friedman tests followed by Conover post-hoc analyses with Holm-Bonferroni corrections (alpha = 0.05), using JASP software version 0.19.0 (JASP Team, 2024) were used to determine if changes occurred in the content of the information reported by the audiologists under the four experimental conditions (pre, post report only, post tool only, and post report plus tool).
This analysis was supported by a secondary statistical analysis to compare the scores obtained in the four conditions for each item of the scoring grid for written reports and tools. This analysis was performed to explore if the observed changes in total scores among conditions may be attributed to only some items of the scoring grid or if those changes are reflected in most items. Considering that an ordinal measurement scale was used in the scoring grid, a non-parametric approach was used for this analysis. Friedman and Conover tests were computed and p-values were corrected for multiple comparisons using the Holm-Bonferroni adjustment (alpha = 0.05).
Results obtained by the participating audiologists to individual items of the scoring grid were also analyzed using a visual approach. Mean compliance ratings and 95% confidence intervals for each item of the grid for all four conditions are illustrated on a forest plot, which also shows the total mean scores for each condition. This visual analysis facilitated the identification of items for which the audiologists obtained lower scores. Items that fell consistently at or under the total mean scores of all four conditions were identified.
A qualitative content analysis was also performed on the data collected during the semi-structured interviews. The recordings from interviews were first transcribed and the verbatim were fully read by two members of the research team. Then, the answers provided by participants during the interviews were classified in subthemes and themes according to the corresponding topics in the interview guides. Finally, a summary of the most salient points mentioned by participants was prepared in relation to each theme. The methodology followed for this qualitative content analysis was based on well-established methods (Graneheim and Lundman, 2004; Knudsen et al., 2012), but because of the pilot nature of the study and the small number of participants, the analysis was done more informally; no formal coding process was followed, and no qualitative analysis software was used.
2.6 Ethics
This research project has been approved by the Vieillissement-Neuroimagerie ethics board of the Centre intégré universitaire de santé et de services sociaux du Centre-Sud-de-l'Île-de-Montréal (study #CER-VN-18-19-15-MP). Participants had to sign a consent form before the beginning of data collection. Participating audiologists received a financial compensation of 50 CAD. Clients received no financial compensation except those who participated in the interview (10 CAD).
3 Results
3.1 Compliance to the QAAP-YOA requirements
Mean overall compliance ratings of the completed audiological reports and clinical tools regarding the protocol requirements (in percentage) are displayed in Figure 1. Results from the Friedman analysis of variance suggest that there is a significant difference between conditions [χ2(3) = 11.327, p = 0.010]. Post-hoc tests results show that the mean compliance rating of the post-experimentation report accompanied by the clinical tool is significantly different from the pre-experimentation report (94.7% vs. 46.9%; T = 6.037, p < 0.001, p-adjusted < 0.001), the post-experimentation report alone (94.7% vs. 73.0%; T = 3.578, p = 0.004, p-adjusted = 0.019), and the post-experimentation clinical tool alone (94.7% vs. 88.7%; T = 2.907, p = 0.013, p-adjusted = 0.039) conditions. The post-experimentation clinical tool, when used alone, also had a significantly higher mean compliance rating than the pre-experimentation report (88.7% vs. 46.9%; T = 3.130, p = 0.009, p-adjusted = 0.035). No other statistically significant difference was observed between conditions.
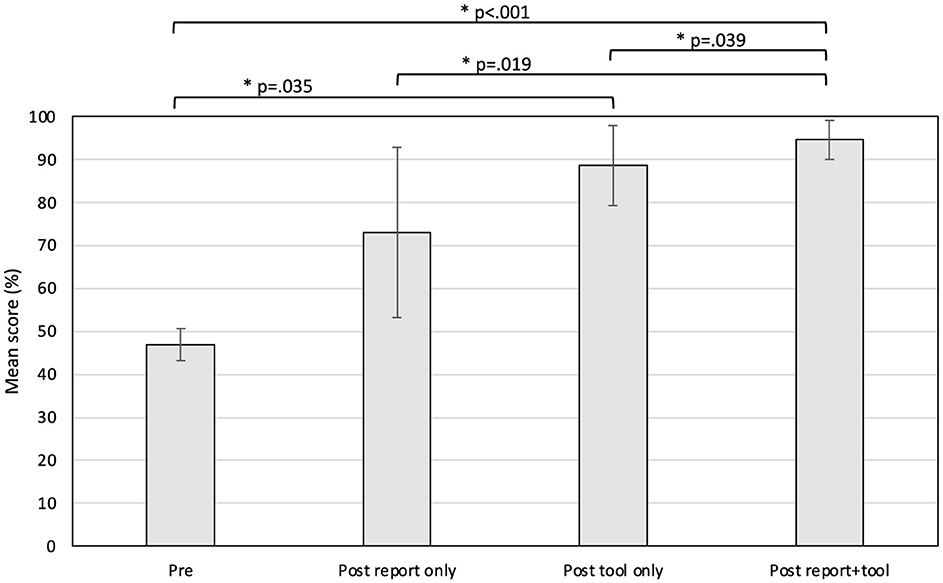
Figure 1. Mean compliance scores in each condition. *Statistically significant result (alpha < 0.05).
Results of the statistical analysis done on each item of the scoring grid are presented in Table 1 (Friedman analyses of variance) and Table 2 (Conover post-hoc tests). Analyses of variance show that the score differences observed are statistically significant on all items individually (p < 0.05). Post-hoc test results indicate that the score differences between pre- and post-intervention in the report plus tool condition are also statistically significant for all items (p < 0.05). There are significant differences between other conditions for some items as well (i.e., item 7, pre vs. post report only conditions, p = 0.002; see Table 2), but this result is less common and systematic among items.
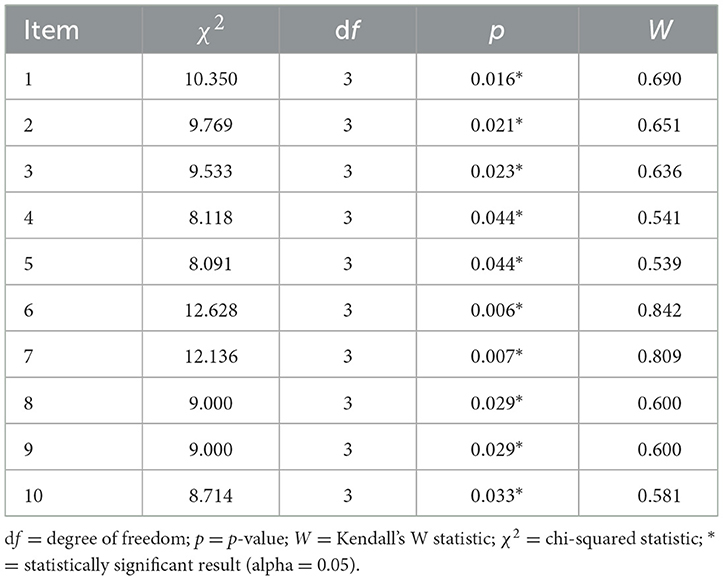
Table 1. Results of the Friedman tests completed to compare scores obtained to each item of the report scoring grid.
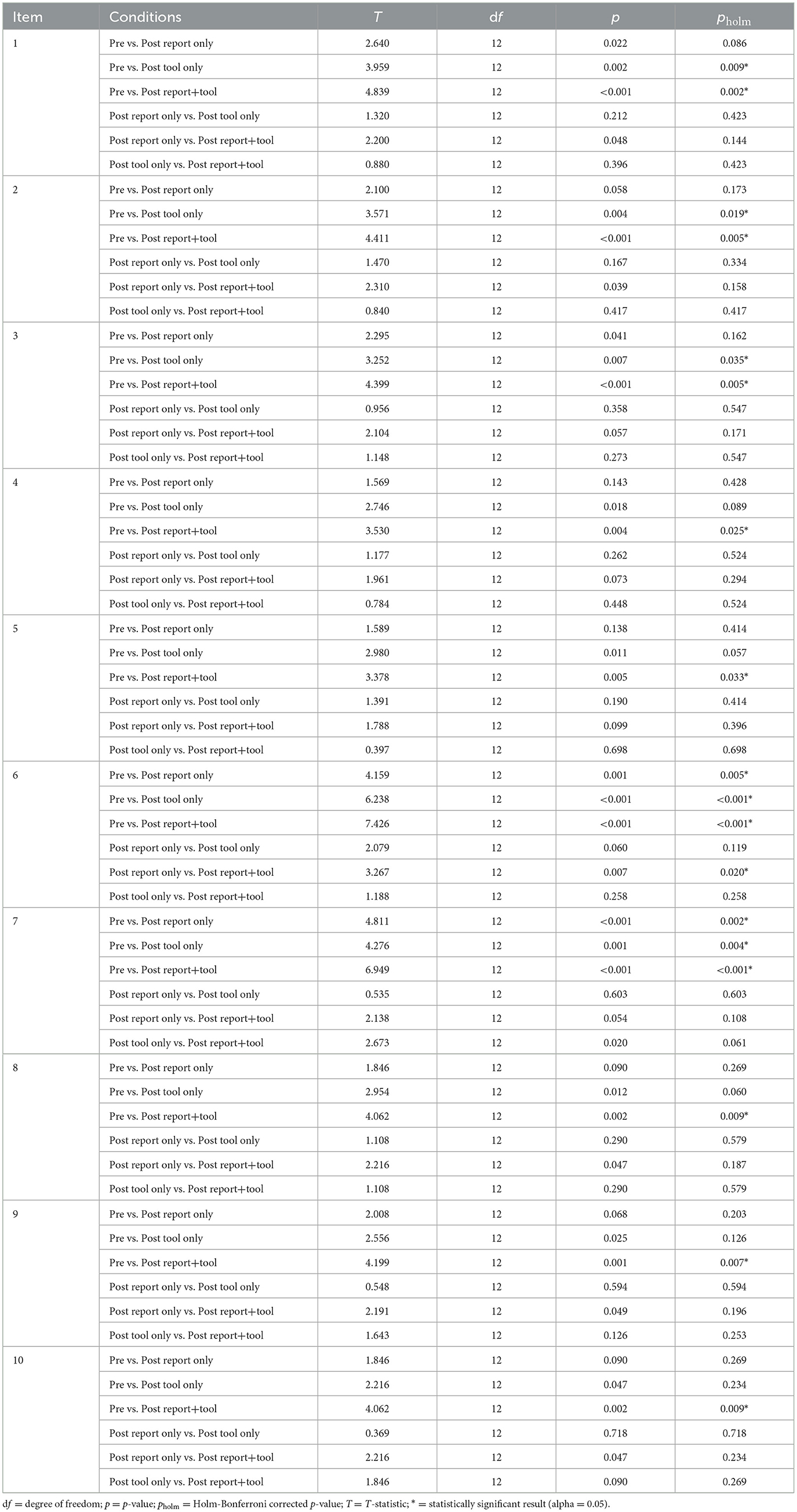
Table 2. Results of the Conover tests completed to compare scores obtained to each item of the report scoring grid.
Mean compliance ratings and 95% confidence intervals for each item of the grid on all four conditions along with the total mean scores for each condition that were used for the visual analysis are presented in Figure 2. Despite a great amount of variability in the scores obtained by the participants for most items of the grid, it is possible to observe some trends in the results. First, the score differences between conditions, as confirmed by statistical analyses, are clearly visible for all items, particularly between pre- and post-intervention in the report plus tool condition. The mean scores of the conditions are always ranked in the same order: the lowest score is always obtained in the pre-intervention condition, followed by the post-intervention report alone condition, the post-intervention tool alone condition, and finally the post-intervention report and tool condition, which always obtained the strongest score. Additionally, four items with a mean score that fell consistently at or under the total mean scores of all four conditions were identified as those for which the participants performed generally more poorly during the experiment, regardless of the condition. Those items are:
• “The participant ranked the difficulties identified in order of priority” (item 2);
• “For each prioritized difficulty, the participant formulated a rehabilitation objective coherent with the clinical data collected during the evaluation of needs” (item 7);
• “The participant recommended a realistic rehabilitation schedule based on the prioritized difficulties” (item 9);
• “The participant mentioned the method that would be used to verify if each objective was achieved” (item 10).
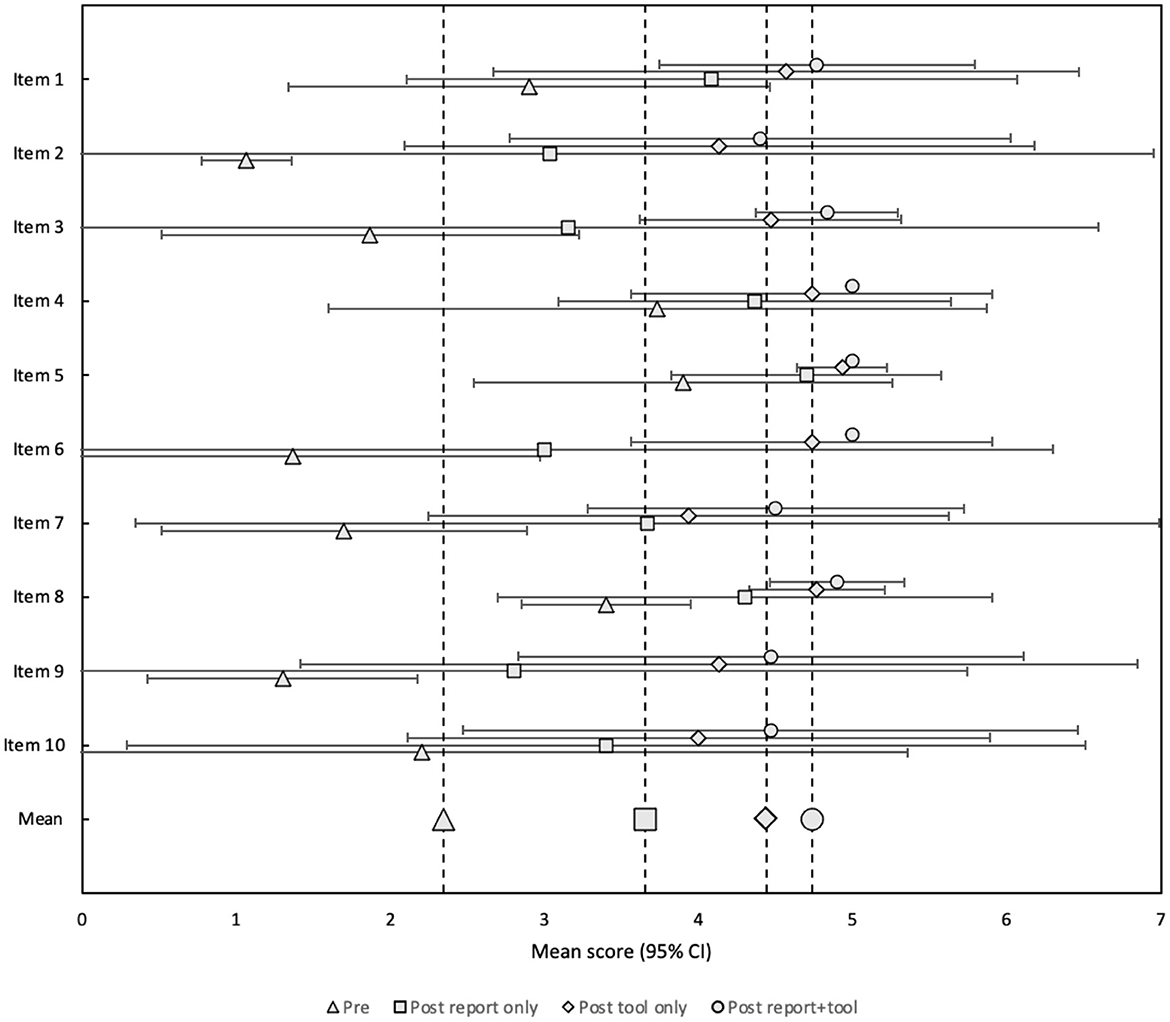
Figure 2. Mean scores and 95% confidence intervals obtained by audiologists to each item of the evaluation grid in each condition.
It is important to note that the post-experimentation report alone condition (without the use of the clinical tool) showed a lot of variability in the results. As a matter of fact, the 95% confidence interval for this condition often included the minimum and maximum of the 5-point rating scale used in the evaluation grid.
3.2 Workflow data
Many participating audiologists did not record the workflow information in the format that had been requested. Moreover, most of the workflow data for the post-trial timepoint were lacking. Therefore, it was not possible to compute indicators and draw conclusions about the impact of QAAP-YOA implementation on the number of clients seen, the total time spent in direct interaction with clients, the total time spent managing clinical files, and the total time spent writing audiologic reports or filling clinical forms. To compensate for this lack of data, we relied on the estimates of the time and number of clients information reported by participants during the interviews.
Regarding the QAAP-YOA time requirements, data reported by participating audiologists during the interviews are presented in Table 3. Audiologists required more time to implement the new needs assessment protocol in the clinic (between 5 and 45 min per client), including the administration of the QAAP-YOA during the appointment and the time required to write the audiological report according to the guidelines of the protocol. Additional time was also required to fill in the clinical tool after the appointment (between 5 and 60 min per client). Audiologists mentioned that the time required to administer the QAAP-YOA and to fill in the clinical tool was more important at the beginning of the trial. The time required to administer the protocol and fill-in the clinical tool was shorter as the audiologists became more familiar with the procedures involved. Audiologists also reported that the use of the protocol and clinical tool did not affect the number of clients seen in a day.
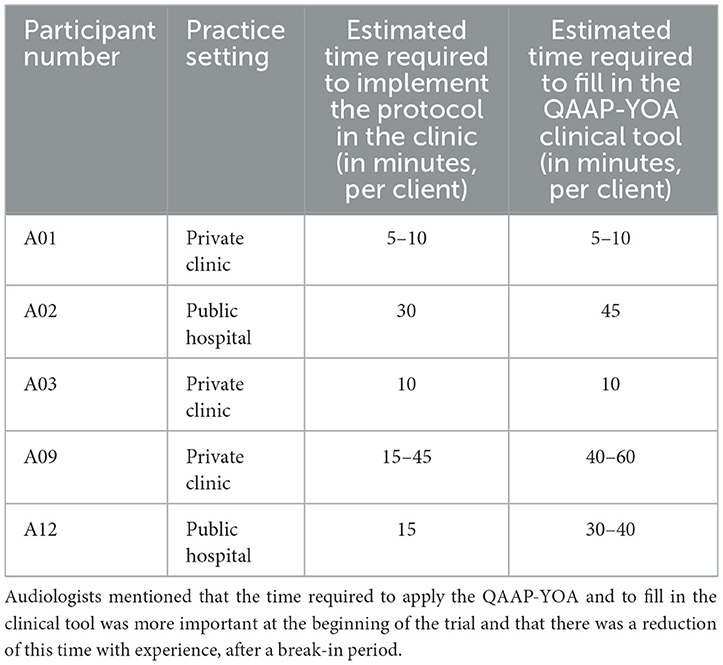
Table 3. Time required to administer the QAAP-YOA as reported by participating audiologists.
3.3 Interviews with participating audiologists
Participating audiologists noted multiple benefits of using the QAAP-YOA and clinical tool. They found that it allowed them to conduct a more thorough needs assessment. They believed that the protocol enabled them to better personalize the recommendations to the specific needs and life situation of the client, which would lead to better client care assuming a proper follow-up to review the progress of the rehabilitation objectives. The clinicians commented that no systematic procedure for needs assessment was previously available to them and that the new protocol addresses this clinical need in a novel and applicable way. Concerning the clinical tool, audiologists thought it eased the application of the protocol by guiding the intervention.
Some drawbacks of the protocol were reported by participating audiologists. They found that the protocol was sometimes hard to apply in a first-line audiology setting and felt it was more applicable to secondary care settings (e.g., specialized rehabilitation services). The protocol also seemed to increase the amount of time required to complete the needs assessment with the client as well as for archiving the documents cumulated during an appointment. Clinicians raised concerns that the implementation of the QAAP-YOA in their practice would require a significant overhaul in the scheduling of appointments and meetings. They reported that it would be difficult to introduce the use of the protocol in their current work schedule. Doing so would require a review of other practices as well as developing new strategies that would save time in the provision of other clinical activities. Further, some participating audiologists were concerned that applying the protocol may result in overwhelming some clients with information (e.g., when the protocol is administered to a client who is undergoing an audiological assessment for the first time). Some limitations were also noted by audiologists concerning the clinical tool. Notably, clinicians who used a standardized protocol to conduct a case history were apprehensive about using a second clinical tool to conduct a needs assessment.
Participating audiologists suggested modifications to the QAAP-YOA. More specifically, their comments were directed toward the accompanying clinical tool: how to improve its efficacy and reduce the time required to administer it. They suggested the creation of a digital version of the tool which could ease its completion and shorten record keeping. The general feeling of the audiologists was that it would save them time if they could complete the clinical tool on their computers, as most of their other tools are computer-based (i.e., intake forms, reports). They also suggested the clinical tool could be given to clients as a summary of their audiological needs and be a helpful reminder of the conclusions reached during the appointment. Additionally, audiologists suggested that the integration of a case history section to the protocol and tool would be helpful in streamlining the workflow in the clinic.
3.4 Interviews with participating clients
The six clients who were interviewed unanimously claimed their satisfaction about the way their needs were assessed by the participating audiologists. The clients recalled that the appointment was a positive experience that met their needs and expectations. They found that the topics covered, and the duration of the appointment were appropriate. Interestingly, no client reported having felt uncomfortable during the needs assessment. They all felt the questions asked by the audiologists were reasonable. Clients didn't suggest any modification to the protocol or the clinical tool.
4 Discussion
The goal of the present study was to assess the QAAP-YOA performance in real clinical settings. Following a training session, audiologists applied the protocol using the clinical tool with clients over a period of 1 month. Data about audiologists' workflow and audiological reports written by them were collected before the training and after the trial period. Semi-structured interviews were also conducted at the end of the trial with audiologists and clients.
Results revealed that after a short 2 h training session, audiologists produced audiological reports that were significantly more in compliance with the QAAP-YOA requirements, particularly when the clinical tool was used in addition to applying the protocol. Results also showed that better ratings were obtained even when the participating audiologists used the clinical tool alone. This suggests that the clinical tool is helpful for driving improvement and a systematic application of a needs assessment protocol. Furthermore, the fact that the statistical and visual analyses performed on individual items of the scoring grid showed significant and consistent improvements on each of the 10 items of the evaluation grid across all experimental conditions suggests that the effect of applying the protocol and/or the accompanying tool was not caused by an improvement on just some of the evaluation criteria. Rather results show that an overall improvement effect was obtained.
The study also aimed to measure how the application of the protocol and clinical tool impacted the workflow of audiologists in a real clinical setting. Participating audiologists indicated that more time was required to apply the protocol and use the clinical tool in comparison with their usual needs assessment practices. Nevertheless, audiologists did not mention that the number of clients seen per day was affected during the trial period, which may appear contradictory. Those results should be interpreted with caution because the experimentation took place during exceptional circumstances, due to the COVID-19 pandemic, which might have influenced the results. For example, two audiologists reported that the number of clients seen per day was generally lower than usual during the period in which the study was conducted due to the pandemic and the sanitary restrictions in place in their clinics. Moreover, during this study, participating audiologists had to take time from their regular work schedule to recruit participating clients. This task most certainly contributed to the additional time the audiologists needed to perform their daily work routine. Unfortunately, we were not able to obtain quantitative data concerning the professional activities conducted during the post-training phase of the study. That information would have allowed us to validate those observations. Therefore, results about the impacts of the QAAP-YOA implementation on the audiologists' workflow may not be representative of the reality. Still, it is reasonable to surmise that the implementation of the QAAP-YOA influenced the duration of appointments and time required for record keeping. As audiologists reported that the amount of time required to conduct the needs assessment when they used the new protocol tended to decrease as they gained experience with it, it would be expected that the application of the protocol and the accompanying tool would be more time efficient as they mastered its use.
Despite the reported impact of the QAAP-YOA implementation on the audiologists' workflow, the overall satisfaction with the QAAP-YOA and its accompanying clinical tool was generally positive amongst participants. They were deemed valuable, helpful, and appropriate from the perspective of audiologists and clients. Nevertheless, some suggestions for improvement were given by the participating audiologists. As many clinical tools are now available online or can be filled in on a computer, it was no surprise that most audiologists would have preferred to work with a digital format of the clinical tool rather than a paper-and-pencil version. Converting the QAAP-YOA clinical tool in a digital tool would facilitate its application in the clinic, but it would also allow for a better customization to different client profiles. It could be possible to create multiple versions of the tool, or an adaptive tool, with different layers of detail or questions specific to the client's characteristics (i.e., hearing aid user or not). The conversion of the QAAP-YOA clinical tool in a digital tool will be part of our future work on the improvement of the protocol.
Participating audiologists also stated that the protocol appeared less suitable for some clients, such as experienced hearing aid users or first-time audiology clients not ready for intervention. This illustrates the fact that the QAAP-YOA is not intended to be used the same way with all clients. The QAAP-YOA and its administration are conceived to be flexible, to be adapted to each client regardless of the person's age, personal characteristics, and the environments in which they experience hearing difficulties. Audiologists are encouraged to customize the QAAP-YOA and clinical tool so that it meets the specific needs of their clientele and clinic reality.
As shown by the detailed analysis of compliance ratings obtained by participating audiologists to each item of the scoring grid, some items generally had lower scores in comparison to others, regardless of whether the clinical tool was used or not. Those items were related to setting the rehabilitation objectives, determining the treatment plan and establishing a follow-up schedule. This suggests that the participants may have experienced some difficulty applying those elements of the QAAP-YOA. This was also observed in our previous pilot study on the QAAP-YOA (Hotton et al., 2024). In that study, graduate audiology students and recently graduated professionals participated in a research project designed to assess how the QAAP-YOA was applied and the benefits its use procured. That study was conducted in a university clinic and recruited actors as simulated clients. At the conclusion of that study, it was hypothesized that (1) the 2 h training provided to the participant-professionals at the beginning of the study might not have been sufficient, and (2) The performance of the participants might have been due (at least in part) to their limited clinical experience. In the present study, the same trend was observed even though the professionals were experienced audiologists. The present results reinforce the idea that the training offered to participants prior to the implementation of the QAAP-YOA should be reviewed. The components of the program that address the setting of audiological objectives, selection of an appropriate intervention program, and the establishment of follow-up schedule could be modified and more clearly explained.
4.1 Study limitations
Unfortunately, only a small number of audiologists completed the trial (n = 5). Initially, 15 audiologists were recruited, but 10 withdrew due to reasons associated with the COVID-19 pandemic. Most of those 10 audiologists were working in public hospitals. In the Province of Québec, in Canada, many audiology clinics located in public hospitals closed for several months during the pandemic. During those periods of time, audiologists were reassigned by the government to other tasks that were judged more critical for the population, such as COVID-19 screening and vaccination campaigns, and basic physical care in nursing homes for seniors. Of course, it was not possible for reassigned audiologists to pursue their participation in the investigation, so they had to withdraw from the study. Clearly, the COVID-19 pandemic affected the course of the study by reducing the number of enrolled audiologists, but also by modifying the clinical workflow of remaining participants. The limited number of participating audiologists likely contributed to increased variability in the collected data, as some participants showed very different performance under the same conditions. This variability was especially evident in the post-experimentation report alone condition (without the use of the clinical tool). Future studies on the QAAP-YOA should aim to include a larger sample size to reduce such variability.
Moreover, the present study was conducted in first-line audiology clinics, in the Province of Québec, Canada. The participants reflected on their experience using the protocol and clinical tool in this context, considering the specific healthcare structures and services in the province. Audiologists or hearing care professionals working in other parts of the world may have faced different issues due to regional specificities of health and hearing care settings in their country, which might have led potentially to the identification of different shortcomings.
5 Conclusion
Based on the results of two previous studies related to (1) the development of the QAAP-YOA (protocol and tool) and (2) its implementation in a simulated setting, the present study was designed to assess the performance of this new needs assessment protocol and clinical tool in a real clinical environment. Results revealed that audiologists can benefit from using the QAAP-YOA, particularly when accompanied by the clinical tool. Feedback from the participating audiologists and clients was generally positive, but some drawbacks and suggestions were also reported. For instance, the implementation of the QAAP-YOA requires time and may impact the needs assessment duration during the audiology appointment, and the time allocated for record keeping. One promising possibility to reduce the QAAP-YOA time burden would be to convert the clinical tool into a digital format, which would facilitate its use in the clinic as well as allow for the customization of the tool to different client profiles. Future work on the improvement of the QAAP-YOA should aim at converting the clinical tool in a digital tool and improve its customization possibilities. Following that modification, another trial with the digital version of the QAAP-YOA tool, using a larger sample size, in a more usual clinical context (e.g., no pandemic), would allow for a better description of the impacts of the QAAP-YOA implementation on the audiologist's professional practices and quality of service at short and long terms.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Vieillissement-Neuroimagerie Ethics Board of the Centre intégré universitaire de santé et de services sociaux du Centre-Sud-de-l'Île-de-Montréal (study #CER-VN-18-19-15-MP). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
MH: Conceptualization, Formal analysis, Funding acquisition, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. LC: Writing – original draft, Writing – review & editing. SP: Writing – original draft, Writing – review & editing. J-PG: Conceptualization, Formal analysis, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by the Québec Ministry of Health and Social Services. MH received a postdoctoral fellowship award from the Fonds de recherche du Québec en santé and from the Centre intégré universitaire de santé et de services sociaux du Centre-Sud-del'Île-de-Montréal. Additional funds were provided by the Endowed research Chair of the Fondation Caroline Durand en audition et vieillissement de l'Université de Montréal, held by J-PG, and by the Centre interdisciplinaire de recherche en réadaptation et intégration sociale.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fauot.2024.1520014/full#supplementary-material
Abbreviations
AAA, American Academy of Audiology; BSA, British Society of Audiology; COVID-19, Coronavirus disease; HHC, Hearing healthcare; ICF, International Classification of Functioning, Disability and Health; OOAQ, Ordre des orthophonistes et audiologistes du Québec; QAAP-YOA, Québec Audiological Assessment Protocol for Younger and Older Adults; WHO, World Health Organization.
References
Atcherson, S. R., Franklin, C. A., and Smith-Olinde, L. (2015). Needs Assessment. Hearing Assistive and Access Technology. San Diego, CA: Plural Publishing.
Creswell, J. W. (2009). Research Design: Qualitative, Quantitative, and Mixed Methods Approaches. Thousand Oaks, CA: Sage Publications.
Ferguson, M., Handscomb, L., and Pryce, H. (2016). Common Principles of Rehabilitation for Adults in Audiology Services. Bathgate: British Society of Audiology.
Graneheim, U. H., and Lundman, B. (2004). Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ. Today 24, 105–112. doi: 10.1016/j.nedt.2003.10.001
Grenness, C., Hickson, L., Laplante-Lévesque, A., and Davidson, B. (2014). Patient-centred care: a review for rehabilitative audiologists. Int. J. Audiol. 53, S60–S67. doi: 10.3109/14992027.2013.847286
Hickson, L., Meyer, C., Lovelock, K., Lampert, M., and Khan, A. (2014). Factors associated with success with hearing aids in older adults. Int. J. Audiol. 53, S18–S27. doi: 10.3109/14992027.2013.860488
Hotton, M., Chauvette, L., and Gagné, J. P. (2024). Pilot evaluation of a protocol and a clinical tool developed to assess the audiological needs of adults with hearing loss. Int. J. Audiol. 63, 827–835. doi: 10.1080/14992027.2023.2211737
Hotton, M., and Gagné, J. P. (2022). Development of a protocol and a clinical tool to assess the audiological needs of younger and older adults with hearing loss. Int. J. Audiol. 61, 453–462. doi: 10.1080/14992027.2021.1947532
IDA Institute (2009). Motivation Tools. The Line, Box and Circle. Denmark: IDA Institute. Available: https://idainstitute.com/fileadmin/user_upload/documents/Motivational_Tools_final_nov13.pdf (accessed online at February 28, 2020).
Knudsen, L. V., Laplante-Levesque, A., Jones, L., Preminger, J. E., Nielsen, C., Lunner, T., et al. (2012). Conducting qualitative research in audiology: a tutorial. Int. J. Audiol. 51, 83–92. doi: 10.3109/14992027.2011.606283
Mckenna, L. (1987). Goal planning in audiological rehabilitation. Br. J. Audiol. 21, 5–11. doi: 10.3109/03005368709077768
Valente, M., Abrams, H., Benson, D., Chisolm, T., Citron, D., Hampton, D., et al. (2006). Guidelines for the audiologic management of adult hearing impairment. Audiol. Today 18, 1–44.
van Leeuwen, L. M., Pronk, M., Merkus, P., Goverts, S. T., Terwee, C. B., Kramer, S. E., et al. (2020). Operationalization of the brief ICF core set for hearing loss: an ICF-based e-intake tool in clinical otology and audiology practice. Ear Hear. 41, 1533–1544. doi: 10.1097/AUD.0000000000000867
Keywords: audiology, needs assessment, persons with hearing impairment, client-centered approach, international classification of functioning, disability and health
Citation: Hotton M, Chauvette L, Poulin S and Gagné J-P (2025) Investigating the implementation of a new protocol and clinical tool designed to assess the audiological needs of individuals with hearing loss in clinical settings. Front. Audiol. Otol. 2:1520014. doi: 10.3389/fauot.2024.1520014
Received: 30 October 2024; Accepted: 16 December 2024;
Published: 08 January 2025.
Edited by:
Ilona Anderson, MED-EL, AustriaReviewed by:
Sten Olof Martin Hellström, Karolinska Institutet (KI), SwedenRobert Eikelboom, Ear Science Institute Australia, Australia
Copyright © 2025 Hotton, Chauvette, Poulin and Gagné. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mathieu Hotton, bWF0aGlldS5ob3R0b25AZm1lZC51bGF2YWwuY2E=