 Ellen Andries1,2*
Ellen Andries1,2* Artur Lorens3
Artur Lorens3 Piotr Henryk Skarżyński3
Piotr Henryk Skarżyński3 Henryk Skarżyński3
Henryk Skarżyński3 Miryam Calvino4,5
Miryam Calvino4,5 Javier Gavilán4
Javier Gavilán4 Luis Lassaletta4,5
Luis Lassaletta4,5 Dayse Tavora-Vieira6,7,8
Dayse Tavora-Vieira6,7,8 Aanand Acharya6,7,8
Aanand Acharya6,7,8 Anja Kurz9
Anja Kurz9 Rudolf Hagen9
Rudolf Hagen9 Ilona Anderson10Edda Amann10
Ilona Anderson10Edda Amann10 Paul Van de Heyning1,2
Paul Van de Heyning1,2 Vincent Van Rompaey1,2
Vincent Van Rompaey1,2 Griet Mertens1,2
Griet Mertens1,2- 1Department of Otorhinolaryngology, Head and Neck Surgery, Antwerp University Hospital (UZA), Antwerp, Belgium
- 2Experimental Laboratory of Translational Neurosciences and Dento-Otolaryngology, Faculty of Medicine and Health Sciences, University of Antwerp (UA), Antwerp, Belgium
- 3World Hearing Center, Institute of Physiology and Pathology of Hearing, Warsaw, Poland
- 4Department of Otolaryngology, IdiPAZ Institute for Health Research, La Paz University Hospital, Madrid, Spain
- 5Biomedical Research Networking Centre on Rare Diseases (CIBERER-U761), Institute of Health Carlos III, Madrid, Spain
- 6Fiona Stanley Fremantle Hospitals Group, Perth, WA, Australia
- 7Division of Surgery, Medical School, The University of Western Australia, Perth, WA, Australia
- 8School of Occupational Therapy, Social Work and Speech Pathology Faculty of Health Sciences, Curtin University, Perth, WA, Australia
- 9Department of Otolaryngology, University Clinic of Würzburg, Würzburg, Germany
- 10Clinical Research Department, MED-EL GmbH, Innsbruck, Austria
Introduction: No standard protocol based on a multidisciplinary framework currently exists for the evaluation, follow-up and interpretation of Cochlear Implant (CI) outcomes in clinical routine. Therefore, this study aimed to develop and clinically implement a multidimensional Cochlear Implant (CI) outcome assessment protocol for adult CI users based on the International Classification of Functioning, Disability and Health (ICF).
Methods: An international multidisciplinary core group of CI experts selected the most relevant ICF categories and codes for adult CI users out of the existing ICF core set for hearing loss. A well-known, commonly used instrument or method was identified and assigned to each ICF category along with quantified ICF qualifiers. These qualifiers facilitate the interpretation of CI outcomes by categorizing the outcome on a rating scale between 0 and 4, based on the severity of participants' impairment/restriction/limitation/barrier. The ICF-based CI outcome assessment protocol was applied in clinical routine in a prospective longitudinal multicenter study assessing a consecutive sample of 72 adult CI candidates before and 6 months after implantation. For each relevant ICF category, the participants' improvement, stability or deterioration was specified in a descriptive approach using ICF qualifiers.
Results: Participants either showed improved or stable ICF qualifiers after cochlear implantation across all ICF domains (e.g., Body Functions and Structures, Activities, and Participation and Environmental factors). The ICF qualifiers for environmental sound tolerance (n = 30 [45%]) and vestibular functions (n = 21 [33%]) deteriorated most frequently after implantation. ICF qualifiers for falling (n = 53 [83%]) and dizziness (n = 40 [62%]) remained stable in most participants. Auditory perception-related and communication-related categories generally improved in most participants after cochlear implantation, with 46 to 73% (n = 34 to n = 48) of CI users perceiving an improvement postoperatively.
Conclusion: This study is the first to propose and apply a ready-to-use CI outcome assessment protocol based on the ICF model, which provides a common language and comprehensive assessment protocol for the description and measurement of CI outcomes worldwide. Its straightforward outcome description and rating enables CI outcome interpretation by non-experts, enhancing multidisciplinary communication and knowledge on individual healthcare needs in CI users.
1. Introduction
Hearing loss is a major global public health issue. The World Health Organization (WHO) estimated that 1.56 billion people worldwide currently have hearing loss, representing approximately 20 percent of the world population (World Health Organization, 2021). In 2019, the Global Burden of Disease study ranked hearing loss as the third most common cause of global years lived with disability, only standing behind low back pain and migraine (Global Burden of Disease, 2021). Hearing loss is the leading cause for global years lived with disability among individuals older than 70 years, affecting quality of life, social participation, mental health, communication, and cognition (Ciorba et al., 2012; Lin et al., 2013; Cosh et al., 2019; Global Burden of Disease, 2021; Tordrup et al., 2022). Therefore, the WHO proposed a comprehensive package of evidence-based key interventions for hearing loss, including cochlear implantation, to partially restore the sensation of hearing in individuals with severe-to-profound hearing loss (World Health Organization, 2021).
Auditory rehabilitation in cochlear implant (CI) users is a complex multidimensional process involving audio processor fittings, speech therapy sessions, psychological counseling, etc. that goes beyond addressing sensory impairment alone (Boothroyd, 2007; British Society of Audiology, 2012; Grenness et al., 2014). Results from psychophysical measures, such as pure tone and speech audiometry, cannot accurately predict CI users' quality of life nor the effect of the implant on their societal participation and daily life activities (Helvik et al., 2006; Hannula et al., 2011; Gopinath et al., 2012; Hornsby and Kipp, 2016). Hence, a patient-centered multidisciplinary approach to identifying individual health care needs is required in the rehabilitation process of CI users (Boothroyd, 1968; British Society of Audiology, 2012; Grenness et al., 2014; Meyer et al., 2016). No standard protocol currently exists for the evaluation and follow-up of CI outcomes in clinical routine and there is lack of consensus on which outcome measures and methods are the most appropriate to use (Meyer et al., 2016; Vila et al., 2016; Schaefer et al., 2017; McRackan et al., 2018a,b, 2019; Andries et al., 2020). Most CI outcome measures also require specific background knowledge in their interpretation, which complicates multidisciplinary collaboration and communication in the rehabilitation process. The International Classification of Functioning, Disability and Health (ICF) model could be a valuable tool to overcome these challenges.
The ICF model is a biopsychosocial framework endorsed by the WHO in 2001 as the international standard for measuring and describing health and disability (World Health Organization, 2001). It provides a common language to define different perspectives of health (biological, psychological, and social) on an individual level, focusing on consequences of health conditions rather than the cause. Its universal language enhances inter-and multidisciplinary communication in both clinical and research settings and enables the comparison of health states across countries and disciplines. The parts and components of the ICF model are depicted in Figure 1. The negative consequences of a health condition are described using the following terms: impairment (e.g., hearing loss) for Body Functions and Structures, activity limitations (e.g., communication issues) for Activities, participation restrictions (e.g., difficulties engaging in community social life) for Participation and environmental barriers (e.g., aversiveness to sounds) for Environmental factors. The ICF parts and its components include nearly 1,400 coded categories serving as units of classification to define individuals' health and health-related states. To specify the extent or magnitude of functioning or disability in a category, a number or “qualifier” can be added, ranging from “0 NO Impairments/Limitations/Restrictions/Barriers” to “4 COMPLETE Impairments/Limitations/Restrictions/Barriers”. The ICF model suggests a qualifier categorization as shown in Table 1. Applying the entire ICF model to each individual patient in clinical routine would be challenging and time consuming due to the elaborate amount of ICF categories. Therefore, ICF core-sets have been developed comprising only the most relevant categories for particular health conditions (World Health Organization, 2001).
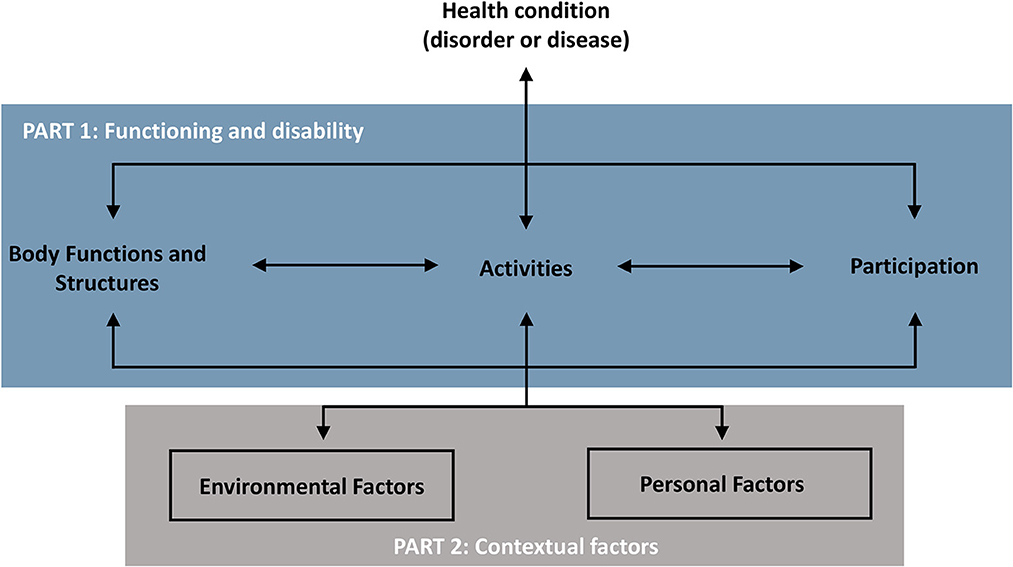
Figure 1. Parts and components of the ICF and their interactions adapted from World Health Organization (2001).
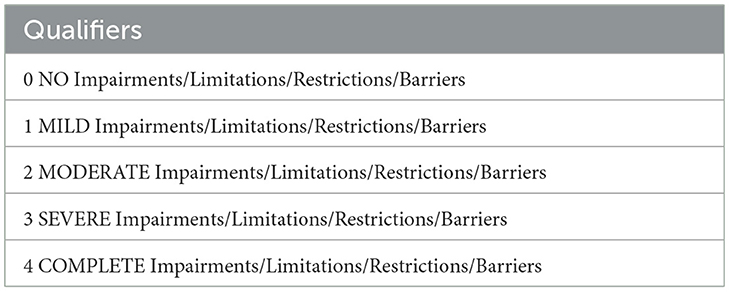
Table 1. General qualifier categorization of the ICF model.
Danermark et al. (2013), Granberg et al. (2014a,b,c,d), and Granberg (2015) developed the ICF core set for hearing loss in 2010, but no patient-centered CI outcome assessment protocol based on the ICF currently exists. Hence, in the first part of the study we aimed to define a CI outcome assessment protocol, based on the ICF core set for hearing loss. This protocol should include all relevant ICF categories to describe the impact of cochlear implantation on different aspects of health. The selected ICF categories for cochlear implantation itself would only provide an overview of which domains of functioning that should be measured and do not include measurement tools. Therefore, we assigned a valid assessment tool to each ICF category relevant to cochlear implantation and aligned all methods across the different centers cooperating in this study. In addition, ICF qualifiers were developed based on the distribution of the applied test outcomes and overworked by clinical experts involved in this study. In the second part of the study, the newly developed ICF-based assessment protocol was applied in clinical practice by using it to assess adult CI users before and 6 months after implantation in all participating centers. Participants were categorized into one of five ICF qualifiers based on the severity of their impairment, restriction, limitation or barrier to improve quality standards, and to develop holistic clinical strategies in the rehabilitation process of CI users.
2. Materials and methods
Part 1: Defining a CI outcome assessment protocol based on the ICF.
An international multidisciplinary core group of ten experts in the field of cochlear implantation, including several experienced healthcare professionals with different backgrounds (e.g., audiology, engineering, pharmacy, psychology, statistics, and speech-language pathology) from different countries (Australia, Austria, Belgium, Germany, Poland, and Spain), reviewed the ICF core set for hearing loss during four pre-study workshops to develop an ICF-based outcome assessment protocol for cochlear implantation. All participating centers are members of the HEARRING group, an international organization including 30 expert clinics dealing with all aspects of hearing restoration with implantable devices. The experts' opinions were collected in structured brainstorming sessions, with each expert contributing opinions and suggestions that were discussed until a unanimous consensus was reached among all experts in the core group.
As a primary step, the most relevant ICF categories and codes for CI users were selected out of the existing core set for hearing loss. During the selection process, the guidelines of Selb et al. (2015) on ICF core set modification and application in specific settings, and previous literature and clinical experience on the possible effects of a CI on different aspects of health were taken into account. In a second step, the appropriate assessment tools that could be assigned to the selected ICF categories and codes were considered. A well-known, commonly used and validated instrument or method, available in all languages of the participating centers and with a limited administration time, was identified and assigned to each ICF category according to the standardized ICF linking rules (Cieza et al., 2019). In total, the administration time of the ICF outcome assessment protocol is approximately one h (30 min psychophysical measures, 30 min questionnaires). Questionnaires can be sent to participants by mail or e-mail, reducing administration time at the clinic because only the psychophysical measures would have to be performed at the clinic. Therefore, the administration time at the clinic can be limited to 30 min in total.
The quantifications for the selected questionnaires, pure tone audiometry and speech audiometry were developed based on the ICF qualifier categorization suggested by the WHO and on the clinical experience of the involved experts in this study. These ICF qualifiers facilitate the interpretation of CI outcomes because they categorize the outcome on a scale between 0 and 4, eliminating the need for background knowledge on the scoring of the various outcome measures for interpretation. For the speech materials and assessment methods, descriptive results such as the mean, the median and the percentiles were used as an additional approach to obtain comparable quantification results for the different language versions. Test methods and ICF qualifiers for speech perception testing were aligned across the different centers based on the normative data for these tests in each language. As different localization set-ups are used in the clinics for objective localization testing, the ICF qualifier quantification was calculated separately per particular localization set-up based on norm level and chance level using the HEARRING_LOC_ICF scale (Mertens et al., 2022). The formula for this calculation is reported in Mertens et al. (2022). The selected ICF categories and codes per ICF component, their assigned test or method and the associated ICF qualifiers are presented in Tables 2–6.
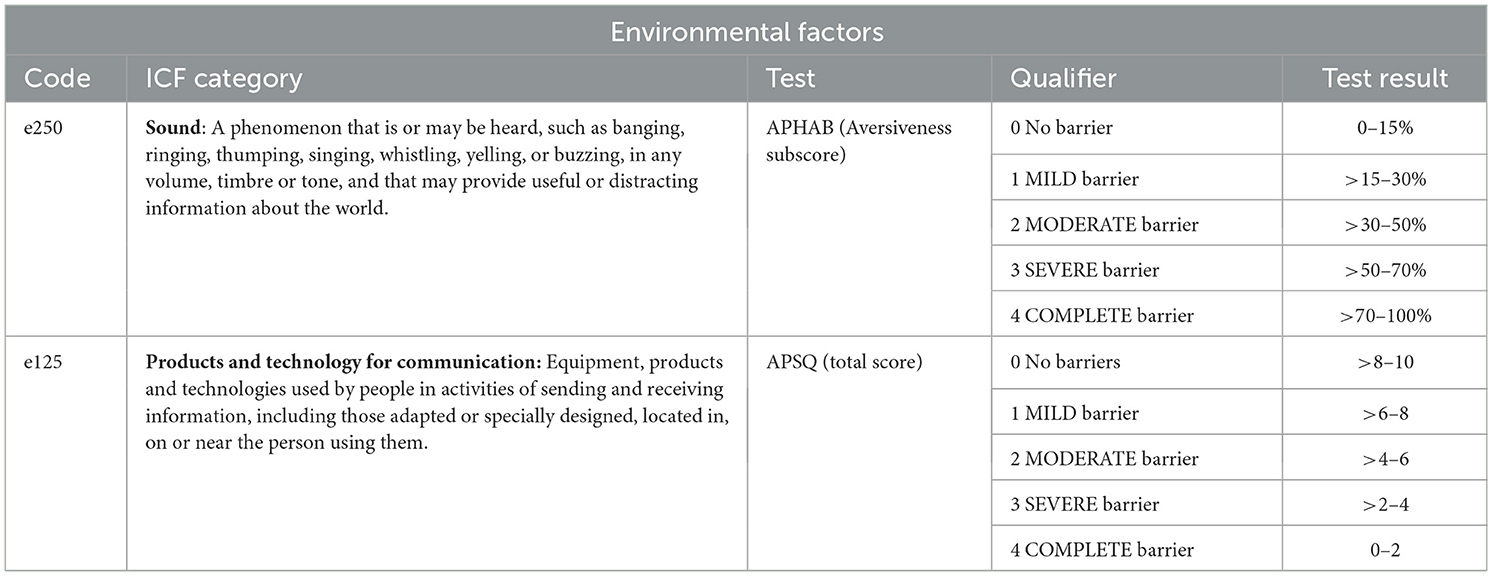
Table 2. Overview of the Environmental factors ICF codes and categories included in the ICF-based outcome assessment protocol and their assigned tests and test results per qualifier.
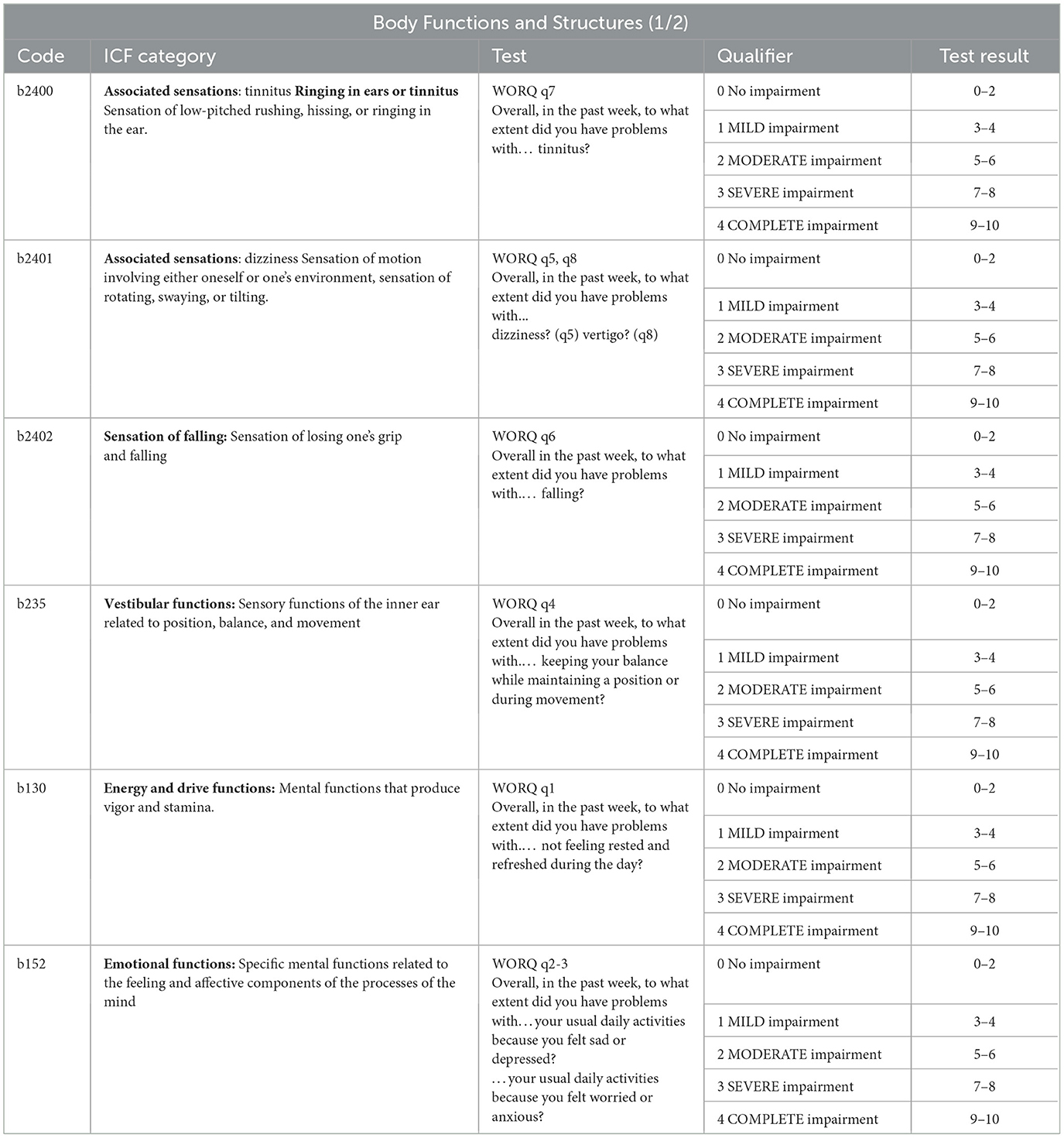
Table 3. Overview of the Body Functions and Structures ICF codes and categories included in the ICF-based outcome assessment protocol and their assigned tests and test results per qualifier, part 1.
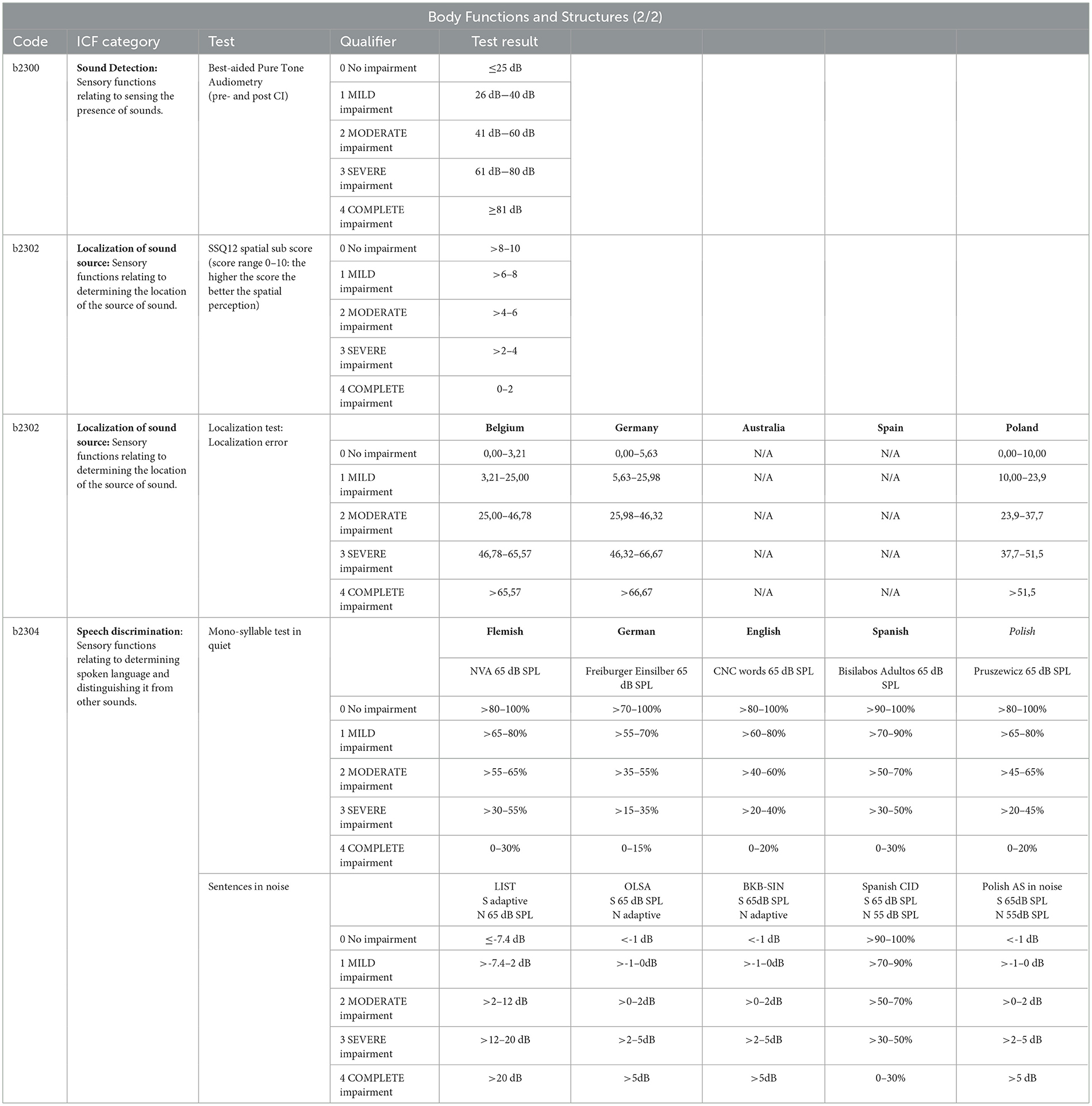
Table 4. Overview of the Body Functions and Structures ICF codes and categories included in the ICF-based outcome assessment protocol and their assigned tests and test results per qualifier, part 2.
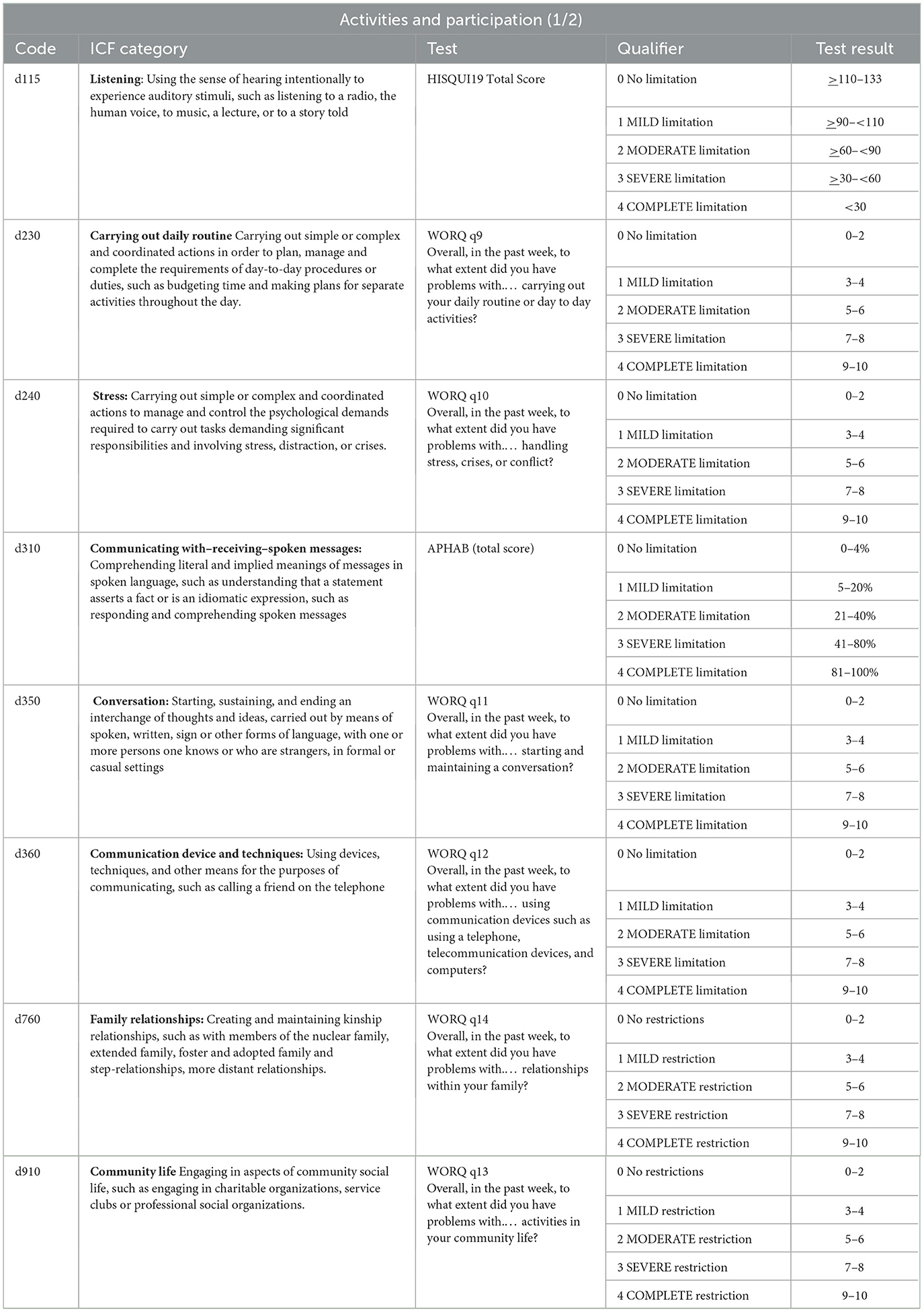
Table 5. Overview of the activities and participation ICF codes and categories included in the ICF-based outcome assessment protocol and their assigned tests and test results per qualifier, part 1.
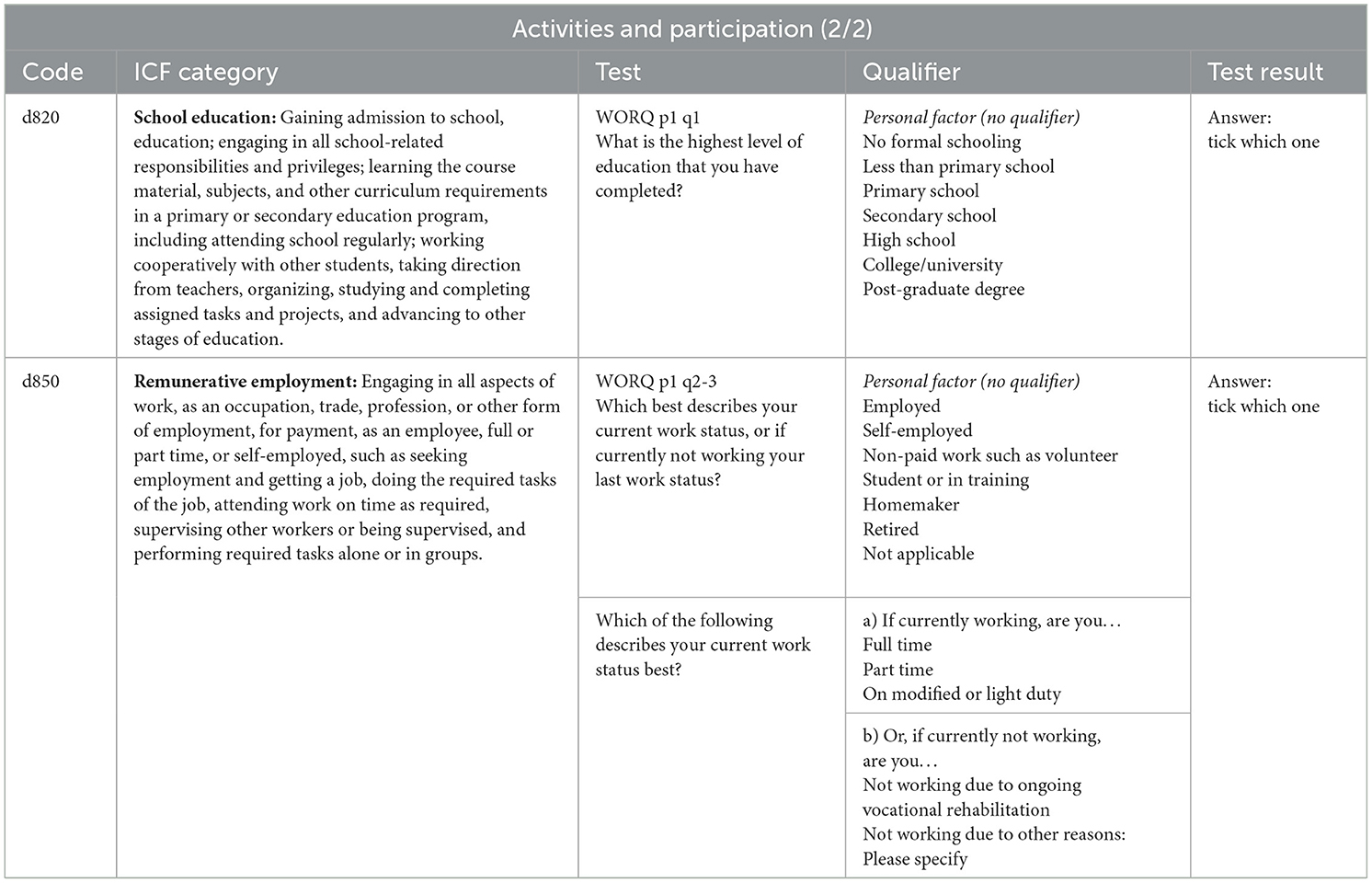
Table 6. Overview of the activities and participation ICF codes and categories included in the ICF-based outcome assessment protocol and their assigned tests and test results per qualifier, part 2.
Part 2: Implementing the ICF-based assessment tool in clinical practice.
2.1. Ethics
The study was carried out in conformity with the recommendations of the local ethics committees and competing authorities (Antwerp 20/27/357; Madrid PI-4359; Perth RGS0000004350; Warsaw KB/3/2021; Würzburg 199/20). All participants gave their written informed consent in accordance with the Declaration of Helsinki prior to participation. All patient data was anonymized prior to the respective analysis.
2.2. Design
This prospective observational longitudinal multicenter study was conducted over a 2-year period (August 2020–August 2022) in five participating centers: La Paz University Hospital (Madrid, Spain), the Antwerp University Hospital (Antwerp, Belgium), the Fiona Stanley Fremantle Hospital Group (Perth, Australia), the University of Würzburg (Würzburg, Germany), and the World Hearing Center (Warsaw, Poland). The study protocol was retrospectively registered at Clinical Trials (Clinicaltrials.gov) on November 2, 2020 (identifier: NCT04611555).
2.3. Participants
A consecutive sample of CI candidates with unilateral or bilateral post-lingual severe-to-profound hearing loss aged ≥18 years who were qualified and scheduled for cochlear implantation according to the candidate selection criteria of their local implanting center were enrolled in this study. All possible CI fitting types were included (e.g., bimodal, unilateral CI, bilateral CI, single-sided deafness, electroacoustic). Participants were assessed 1 month before implantation and 6 months post activation of the audio processor. They had to be fluent in the language of the implanting center and receive their first CI. The audio processor was activated approximately 4 weeks postoperatively and its settings were optimized during regular clinical programming sessions. Participants were excluded in case of reimplantation of the CI, presence of contra-indications for surgery in general and cochlear implantation in particular.
2.4. CI outcome assessment
2.4.1. Questionnaires
Based on the consensus achieved among our expert group during our pre-study workshops, five questionnaires were identified, namely: the Work Rehabilitation Questionnaire (WORQ), the Abbreviated Profile of Hearing Aid Benefit (APHAB), the Audio Processor Satisfaction Questionnaire (APSQ), the Speech, Spatial, and Qualities of Hearing Questionnaire with 12 items (SSQ12), and the Hearing Implant Sound Quality Index 19 (HISQUI19). All of these questionnaires are available in Dutch, English, German, Polish, and Spanish and were completed by each participant. Participants completed the questionnaires at a routine visit to the clinic, via e-mail or via mail. Detailed information can be found in the Supplementary material.
2.4.1.1. The work rehabilitation questionnaire
The 59-item WORQ (Finger et al., 2014; Vermeulen et al., 2019) is a questionnaire based on the ICF core set for vocational rehabilitation, assessing work related functioning. The original WORQ has been revised to match the core needs of the ICF categories and codes for CI users (Andries et al., 2022). The revised version includes two parts addressing demographics and relevant background information (Part 1) and work functioning (Part 2). Each item in the WORQ represents an ICF category. Part 1 consists of 4 items and part 2 includes 14 items. In part 2, participants have to rate to what extent they had problems with a certain activity or task in the last week using a numerical scale ranging from 0 (no problem) to 10 (complete problem). The WORQ takes < 5 min to complete.
2.4.1.2. The abbreviated profile of hearing aid benefit
The APHAB (Cox and Alexander, 1995) is a 24-item questionnaire derived from the original 66-item Profile of Hearing Aid Benefit. The self-assessment instrument evaluates consequences of hearing impairment for functioning in real-life situations with and without hearing aids. Participants must rate how often a given statement is true in their daily life. More detailed information on response alternatives, subscales, etc can be found in Table 7. Participants were instructed to complete the APHAB with their current hearing situation in mind (e.g., preoperatively with hearing aid(s) if aided and after implantation with the combination of a hearing aid and a CI or with CI only). The APHAB typically requires 10 min or less to complete.
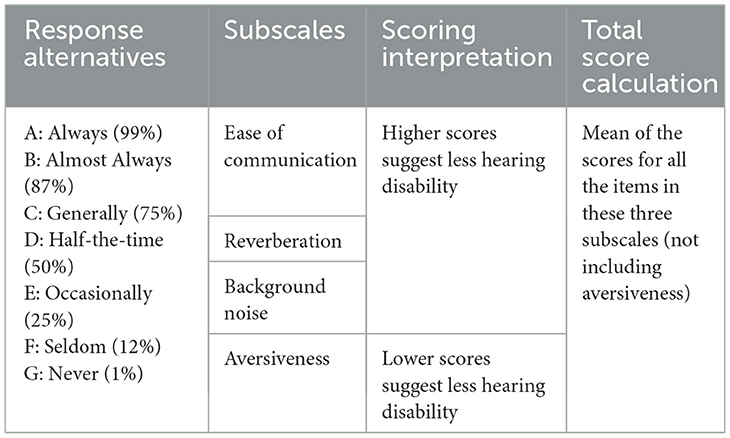
Table 7. APHAB response alternatives, subscales, scoring interpretation and total score calculation.
2.4.1.3. The audio processor satisfaction questionnaire
The APSQ (Billinger-Finke et al., 2020) is a questionnaire which is designed to assess the handling of hearing devices, taking 5 min to complete. It assesses the wearing comfort, sound quality, and other device-specific factors related to the audio processor with 15 items on a VAS scale from 0 (does not agree at all) to 10 (fully agrees). Participants had to complete the APSQ 6 months post activation.
2.4.1.4. The speech, spatial, and qualities of hearing questionnaire with 12 items
The SSQ12 (Noble et al., 2013) is designed to measure self-reported auditory disability across a wide variety of domains, reflecting the reality of hearing in the everyday world. It takes approximately 5 min to complete. It covers hearing speech in a variety of competing contexts; the directional, distance, and movement components of spatial hearing; segregation of sounds and attending to simultaneous speech streams; ease of listening; the naturalness, clarity, and identifiability of different speakers; different musical pieces and instruments; and different everyday sounds. The SSQ12 consists of 12 questions divided across three subscales (Speech, Spatial and Qualities of Hearing) that subjects score on a scale from 0 (not at all) to 10 (perfectly). The total score is the mean of all items, subscale scores are the mean of all items in that subscale.
2.4.1.5. The hearing implant sound quality index 19
The HISQUI19 is a self-administered questionnaire to quantify the individual perceived sound quality of hearing implanted patients in daily life (Amann and Anderson, 2014). The questionnaire consists of 19 seven-level Likert items ranging from “always (99%)” to “never (1%)”, taking approximately 10 min to complete. Added percentage values support the answering. The total score is the sum of all items and ranges from 19 to 133 points.
2.4.2. Audiological examinations
2.4.2.1. Pure tone audiometry
Pure tone audiometry was performed according to current clinical standards (ISO 8253-1, 2010) by an experienced Good Clinical Practice certificated audiologist. Pre- and post-operatively, best-aided pure tone audiometry was measured at 500, 1,000, 2,000, 4,000, and 8,000 Hz using warble tones in sound field in a sound treated booth. The loudspeaker was placed in front of the participant (0 degrees) at ear level at 1-meter distance. The best-aided pure tone average (PTA4) was calculated by averaging participants' hearing thresholds at 500, 1,000, 2,000, and 4,000 Hz in best-aided condition.
2.4.2.2. Speech recognition
Speech recognition was evaluated in quiet, using disyllables in Spanish and monosyllables in the other languages, and in noise, using sentences. These tests were performed pre- and postoperatively in best-aided condition according to current clinical standards (ISO 8253-1, 2010). Participants sat in front of the loudspeaker (0 degrees), positioned at ear level, at a one-meter distance. They were instructed to repeat the speech stimuli they heard. Speech materials and assessment methods were aligned across the different centers cooperating in this study to obtain comparable results. Detailed information about the used speech tests per center can be found in the Supplementary material.
2.4.2.3. Sound localization testing
Each center used its own localization set-up, all meeting the localization testing standards published by Van de Heyning et al. (2017). Norm values were based on the current set-up in each participating center. Two centers did not have an appropriate set-up at the start of this study and therefore only used the SSQ12 spatial subscale.
2.4.3. Subject demographics
Subject demographics were retrieved from the participants' medical file or by asking them if the information is not available. The following information was retrieved: age, sex, ear to be implanted, etiology, date, type and onset of hearing loss, preoperative hearing aid use, previous ear surgery and otological condition. The 11th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-11) classification was used to code subjects' hearing loss etiology (WHO, 2018).
2.5. Statistics
Firstly, audiometry results and questionnaire total scores (APSQ, HISQUI19), subscale scores (APHAB aversiveness subscale; SSQ12 spatial subscore) or single questions (WORQ) were assigned according to the quantified ICF qualifiers as suggested in Part 1 of the methods section. In a second step, IBM SPSS Statistics 24 (IBM, Armonik, New York) was used to calculate the percentage values of the ICF qualifiers for the ICF categories before and 6 months after implantation. Thus, for each ICF category the improvement, stability or deterioriation could be specified in a descriptive approach. Absolute and relative frequencies were used to describe patient characteristics (e.g., age, sex, etiology). Localization test results and their assigned qualifiers were calculated using the HEARRING_LOC_ICF scale.
3. Results
In total, 72 CI candidates were enrolled in this study. More details of their characteristics are presented in Table 8.
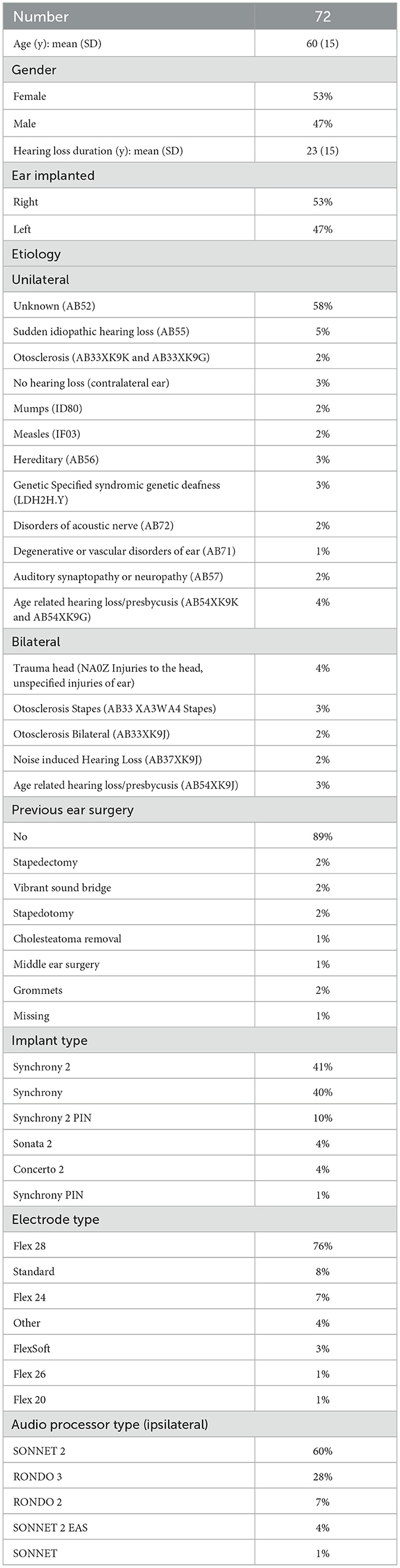
Table 8. Overview of the participants' characteristics.
Overall, the participants in our study either showed improved or stable ICF qualifiers after cochlear implantation. Participants most commonly showed ICF qualifier improvement for sound detection, with n = 48 participants (73%) showing improved ICF qualifiers 6 m postoperatively compared to preoperatively. Most participants also demonstrated ICF qualifier improvement for speech discrimination (speech in quiet) (n = 48 [69%]); self-reported localization (n = 40 [59%]); and communicating with—receiving—spoken messages (n = 34 [52%]) after implantation. The ICF qualifiers for sound (APHAB aversiveness) (n = 30 [45%]) and vestibular functions (n = 21 [33%]) deteriorated most frequently among the participants after implantation. ICF qualifiers for falling (n = 53 [83%]); dizziness (n = 40 [62%]); emotional functions (n = 39 [62%]); and family relationships (n = 39 [62%]) remained stable in most participants preoperatively compared to postoperatively. If there was any change in ICF qualifiers, the majority generally changed from mild to no impairments/limitations/restrictions/barriers or from severe to moderate impairments/limitations/restrictions/barriers. More details on the change in ICF qualifiers over time can be found in Table 9.
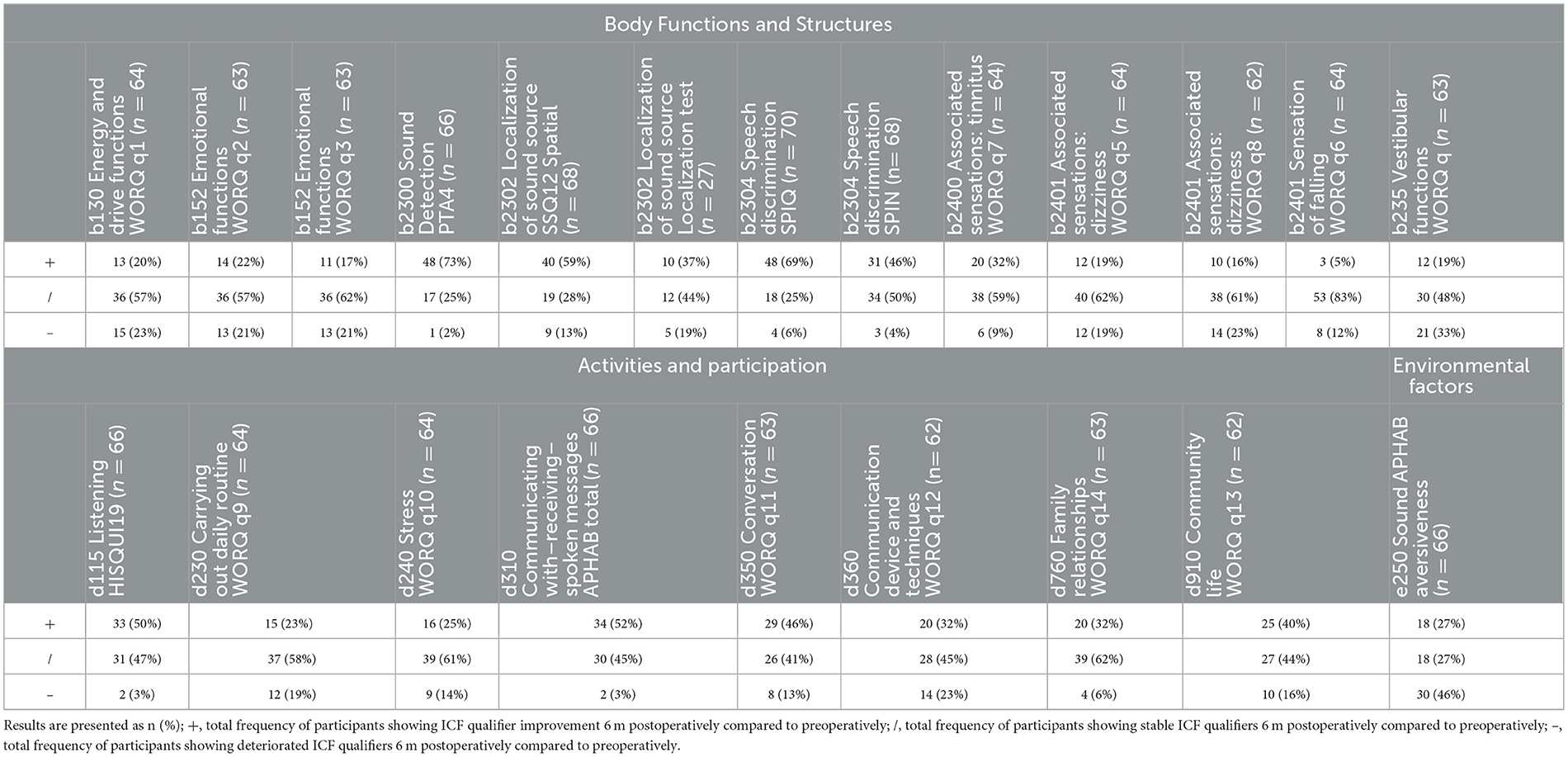
Table 9. Overview total frequency of improvement, stability, and deterioration after cochlear implantation indicated by the ICF qualifiers over time per ICF category.
The ICF qualifiers per ICF category preoperatively and postoperatively are presented in Figures 2, 3. For “Body Functions and Structures”, most participants reported a complete impairment preoperatively for speech discrimination in noise (n = 37 [54%]), followed by self-reported localization (n = 32 [47%]) (measured by SSQ12). Postoperatively, both categories still frequently pose a complete impairment for the participants, but the frequency decreased to n = 25 (37%) and n = 12 (18%), respectively. Most of the participants perceived no impairment preoperatively for falling (n = 59 [92%]), emotional functions (n = 46 [73%]), and dizziness (n = 45 [70%]). Postoperatively, falling remained the category for which most participants perceived no impairment (n = 54 [84%]), followed by dizziness (n = 44 [69%]), and tinnitus (n = 44 [69%]) in the “Body Functions and Structures” domain.
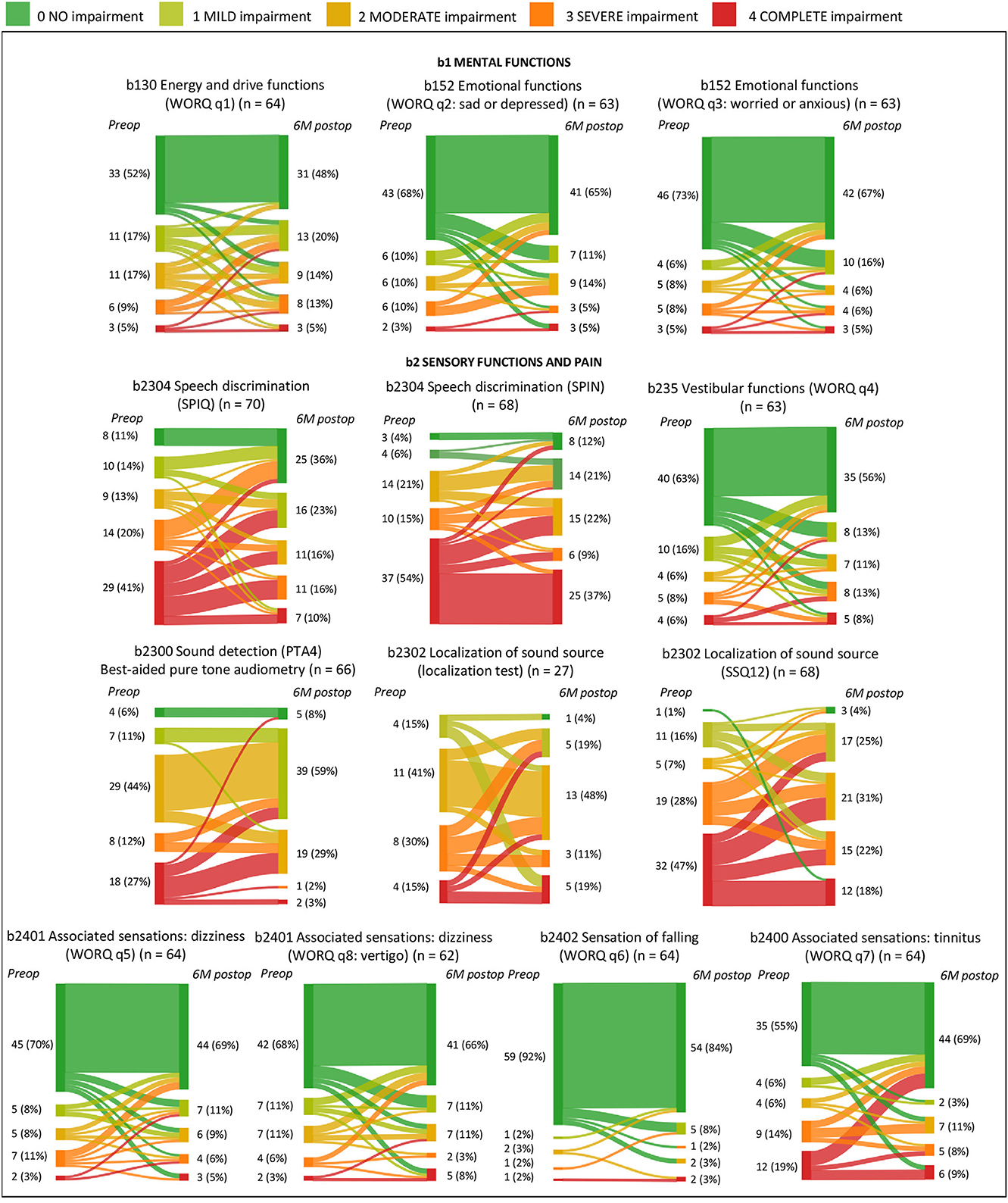
Figure 2. Overview of the change in ICF qualifiers preoperatively compared to postoperatively per ICF code and category for Body Functions and Structures (b). Numbers are presented as n (%); WORQ, work rehabilitation questionnaire; SPIQ, speech in quiet; SPIN, speech in noise; PTA4, pure tone average; SSQ12, speech spatial and qualities of hearing scale with 12 questions.
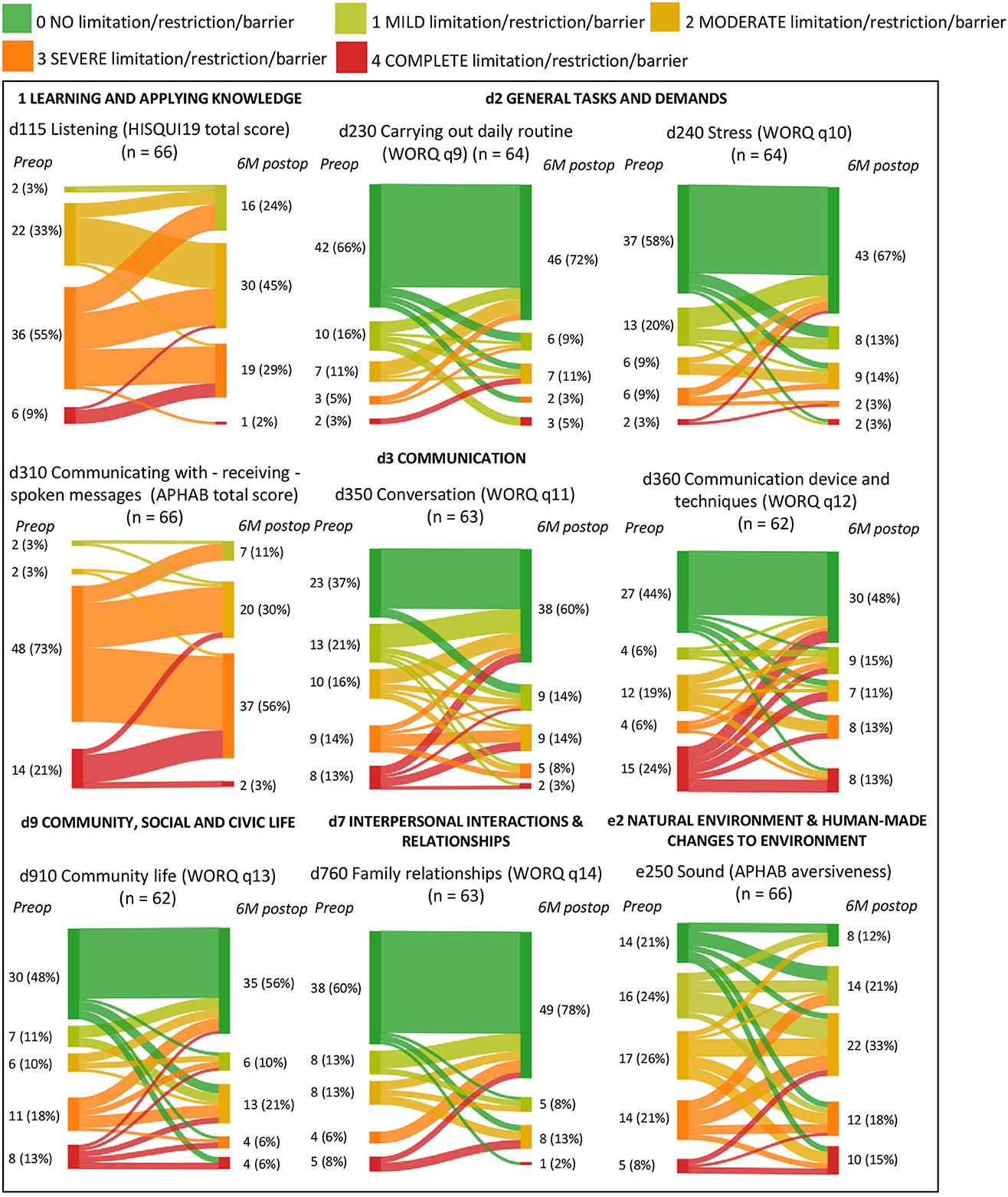
Figure 3. Overview of the change in ICF qualifiers preoperatively compared to postoperatively per ICF code and category for Activities and Participation (b) and Environmental factors (e). Numbers are presented as n (%); HISQUI19, hearing implant sound quality index 19; WORQ, work rehabilitation questionnaire; APHAB, abbreviated profile of hearing aid benefit.
In the “Activities and Participation” domain, most participants reported a complete limitation preoperatively for communication devices and techniques (n = 15 [24%]) and communicating with receiving—spoken messages (n = 14 [21%]). Postoperatively, many participants showed improvement for communicating with receiving—spoken messages (n = 34 [52%]), leading to only n = 2 of the CI users (3%) perceiving a complete limitation for this category after implantation. Many participants also perceived an improvement regarding communication devices and techniques (n = 20 [32%]), but it remained the category for which most participants experienced a complete limitation (n = 8 [13%]) after implantation in the “Activities and Participation” domain. No limitation or restriction was most frequently perceived for carrying out daily routine (n = 42 [66%] preop vs. n = 46 [72%] postop), family relationships (n = 38 [60%] preop vs. n = 49 [78%] postop), and stress (n = 37 [58%] preop vs. n = 43 [67%] postop), preoperatively as well as postoperatively. Overall, the ICF categories listening, and communicating with- receiving—spoken messages showed the least number of participants perceiving no limitation (n = 0 [0%]), both preoperatively and postoperatively. Most CI users finished secondary school (n = 39 [54%]) or college/university (n = 25 [35%]), were retired (n = 30 [42%]) or employed (n = 26 [36%]), and were working full-time (n = 20 [28%]) or not working due to other reasons such as retirement (n = 16 [22%]). More details are presented in Figure 4.
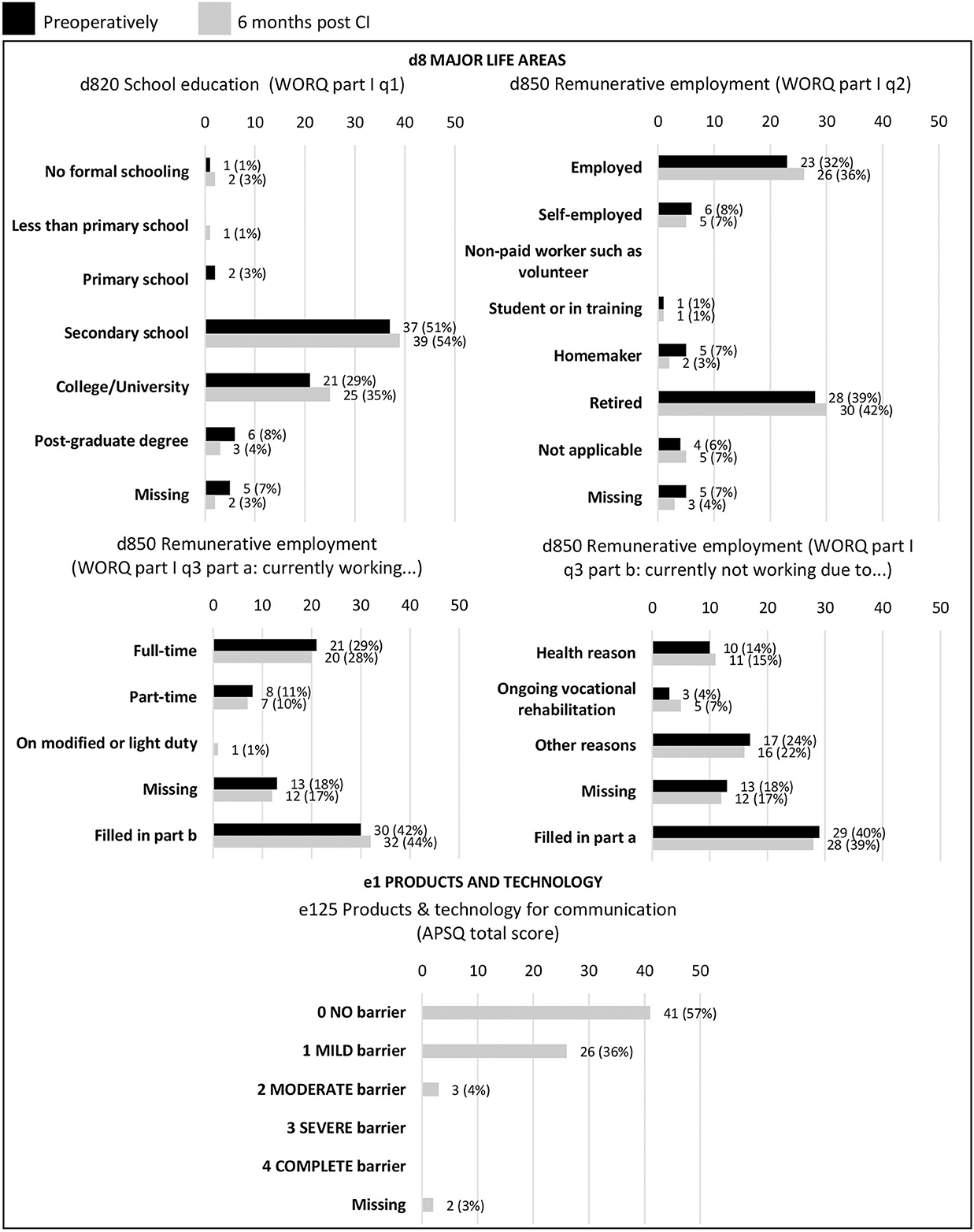
Figure 4. Overview of the ICF qualifiers per ICF category and code preoperatively and postoperatively for Activities and Participation (d) and Environmental factors (e). Numbers are presented as n (%); WORQ, work rehabilitation questionnaire; APSQ, audio processor satisfaction questionnaire.
4. Discussion
This longitudinal prospective multicenter cohort study aimed (1) to define a CI outcome assessment protocol based on the ICF model, (2) apply it in clinical routine by using it to assess adult CI users before and 6 months after implantation in all participating centers. The need and relevance for applying the ICF model to audiological rehabilitation has been reported in several studies but, to our knowledge, measures have only been suggested for the ICF core set for hearing loss with no assigned qualifiers and there is no protocol yet for the application in clinical routine (Boothroyd, 2007; Danermark et al., 2013; Granberg et al., 2014a,b,c,d; Meyer et al., 2016; Psarros and Love, 2016; Van Leeuwen et al., 2017; Glade et al., 2020; Lorens et al., 2020). Our study is the first to propose and apply a ready-to-use CI outcome assessment protocol based on the ICF model. A post-study forum was organized to discuss clinical applications, which showed that the protocol was positively received in all participating centers and the involved healthcare professionals. Particularly its comprehensive patient-centered approach, common language in outcome reporting and short administration time was appreciated. Our study shows that CI outcomes can be described similarly across the globe, facilitating national and international comparisons at the individual level as well as at group level. By adding ICF qualifiers to the ICF codes and categories, the outcomes can be interpreted by individuals with no or limited knowledge of the outcome measures and their scores (e.g., healthcare professionals without ENT-background, stakeholders, and policy makers), enhancing multidisciplinary communication and increasing the focus and knowledge on individual healthcare needs in CI users. The ICF-based CI outcome assessment protocol enables a comprehensive assessment of the most relevant CI outcomes in multiple domains, using a new standardized combination of well-known and commonly used measures in the field of cochlear implantation.
Global calculations of the prevalence of health conditions are based on classification systems such as the ICD-11, which was used in our study to code hearing loss etiology (World Health Organization, 2018). Applying a classification system such as the ICF model would enable prevalence calculations of the functional aspects of these health conditions. Hence, using the ICF-based CI outcome assessment protocol would allow for a standardized prevalence calculation of the effects of cochlear implantation in adults using the general ICD-11 code for presence of otological or audiological implants (QB51.3). Linking the ICD-11 coded hearing loss etiology to its functional consequences coded in the ICF protocol would enable the prevalence calculation of the functional and disabling aspects of different hearing loss etiologies in CI users instead of only calculating the prevalence of these etiologies without considering their impact (Granberg et al., 2014d). Nevertheless, the hearing loss etiology of most of the CI users in our study (59%) was “unknown”, which could partly be due to e.g., unknown genetic contributions, late-onset cytomegalovirus infections. Therefore, linking these two classification systems based on hearing loss etiology was not reliable in our study and future research should focus more closely on a method for (early) identification of post-lingual severe-to-profound hearing loss etiology in clinical routine.
The CI outcome results showed that auditory perception-related and communication-related categories generally improved the most after cochlear implantation, which is in line with previous studies showing large positive effects of cochlear implantation on these domains (Carlson, 2020; Kay-Rivest et al., 2022; Rasmussen et al., 2022). The mono- or disyllable words test demonstrated more improvement after cochlear implantation compared to the sentences in noise test for speech discrimination. This could be attributed to the higher level of complexity of the sentences in noise test, including background noise and the combination of multiple words in a sentence, compared to the mono- or disyllable words test including isolated words in quiet (Pichora-Fuller et al., 2016). Having a conversation was also found to be easier after cochlear implantation by most of the participants. The WORQ question assigned to this ICF category was worded as: “to what extent did you have problems last week with starting and maintaining a conversation”, not explicitly mentioning oral conversations so participants may also have considered written or typed conversations when completing this question. CI users frequently reported difficulties with using communication devices and techniques such as computers or smartphones before and after cochlear implantation. This could partly be due to the fact that CI users generally continue to have difficulties with communicating over the phone after implantation, caused by a reduced signal transmission bandwidth, lack of contextual cues and lip-reading and potentially unfamiliar topics and speakers (Anderson et al., 2006; Castro et al., 2008). Along with the more advancing technology of both CIs and general communication devices, these issues might diminish in the future. In addition, our study sample consisted of mainly older participants (mean age 61 years, median 63 years) who tend to have more issues with using technical devices compared to younger adults given that they generally struggle with for example compressed keys, hierarchical menus and mild vision impairments (Arning and Ziefle, 2007; Zhou et al., 2014). Listening and communicating with and receiving spoken messages was still difficult after receiving a CI for most of our participants, but these categories also showed improvement for approximately half of them. These results highlight that a CI does not completely restore hearing function but does generally improve overall communication and auditory perception. We also should bear in mind the short 6 months follow-up time; therefore further improvement can be anticipated. Stability in the results for these domains could be due to ceiling effects, because in certain fitting types (e.g., EAS or SSD) individuals either have low frequency residual hearing or a normal-hearing contralateral ear which might limit the effects of a CI on auditory perception (Adunka et al., 2010; Hoth et al., 2016; Doge et al., 2017). Therefore, in a next study we will investigate the influence of best-aided fitting type on the variables included in the ICF-based CI outcome protocol.
ICF categories related to vestibular function mostly remained stable, but generally showed more decrease than improvement in our sample of CI users. Vestibular loss is a possible complication of CI surgery and there is a significant association between severe-to-profound hearing loss and vestibular loss, which might explain the changes in qualifiers indicating deterioration for part of the CI users (Sun et al., 2014; Batuecas-Caletrio et al., 2015; Meli et al., 2016; Ibrahim et al., 2017; Agrawal et al., 2018). Balance issues also increase with age and therefore our population may have skewed the results. In addition, cochlear implantation partially restores hearing function but is not a treatment for vestibular disorders. Therefore, the follow-up of vestibular function in CI users is important to monitor and, where possible, to treat vestibular problems and CI candidates should be informed about the potential effect of CI surgery on the vestibular system. No objective vestibular measures such as electronystagmography were included in our ICF-based protocol, but if patients report vestibular problems it is recommended to do additional objective vestibular assessments. Next to vestibular loss, tinnitus is also a known complication of CI surgery (Amoodi et al., 2011; Arts et al., 2012, 2015a,b). However, most CI users' tinnitus perception either remained stable or improved after implantation in our study, which is more in line with studies indicating that tinnitus perception might improve after cochlear implantation (Kim et al., 2013, 2016; Blasco and Redleaf, 2014; Holder et al., 2017). Still, approximately 25% of the CI users in our sample experienced troublesome tinnitus after implantation, which concurs with previous literature (Baguley, 2010; Andries et al., 2022). Self-reported localization was one of the most improving categories after implantation, while objective localization remained stable in most of the CI users. This could be attributed to the fact that most CI users in our sample were bilaterally severely-to-profoundly hearing impaired but had a unilateral CI or bimodal fitting. A CI improves auditory perception and might therefore give the impression of enhanced localization skills, as after CI the sounds to be localized are (better) perceived but, particularly in unilateral CI fitting, sounds are only perceived in one ear making objective localization difficult (Buhagiar et al., 2004; Kerber and Seeber, 2012). In the SSD group, consisting of participants with normal hearing in one ear and a CI in the other ear, we would expect an improvement of localization skills as they are able to receive binaural acoustic information postoperatively.
The ICF category “Sound” in Environmental factors, measured by APHAB aversiveness, worsened in most CI users, indicating that they have a greater negative reaction to environmental sounds after implantation. This finding corroborates with those of Cox and Alexander (1995), Palmer et al. (2006), and Johnson et al. (2010) demonstrating that aversion to sounds increases with amplification as it is influenced by the audibility of noise (Cox and Alexander, 1995; Palmer et al., 2006; Johnson et al., 2010). These results seem to suggest that aversiveness to sounds is a negative by-product of amplification. However, Palmer et al. (2006) showed that appropriate amplification returns a normal perception of aversive sounds when compared to the performance of normal hearing individuals on aversiveness measures (Palmer et al., 2006). Hence, CI candidates should be counseled that increased auditory perception after implantation leads to a more normalized perception of annoying environmental sounds, which might require an adjustment period. Products and technology for communication generally posed little barriers for the CI users, indicating that most of them can handle the implant and are satisfied with it. This category was not assessed before implantation as a lot of CI candidates did not wear hearing aids before implantation and because the APSQ is a questionnaire specifically developed for hearing implant users which makes some questions less applicable for conventional hearing aid users (Billinger-Finke et al., 2020).
Personal factors such as school education and remunerative employment remained stable after implantation, as expected, given the short 6 months follow-up time in our study. Nevertheless, the ICF can be used continuously to follow up these factors to ensure (re)integration in school education and/or professional life if desired after implantation. Question 3 of Part 1 of the revised WORQ for CI users was revisited as mentioned in Andries et al. (2022) because of the large number of missing values for this question (Andries et al., 2022). These missing values could partly be due to question 3 including two parts: part one “currently working”, and part two “currently not working due to”. Participants only have to fill in the part that is most applicable to them, which could have been confusing for the participants causing them to skip the question entirely. Additionally, no explicit response alternative is provided for retired participants for this question. The following response alternative must be ticked and completed if retired: “Not working due to other reasons. Please specify:…”, which could have been unclear for some participants. Therefore, the response alternative “retirement” will be added to the final version of the revised WORQ for CI users. Mental functions already posed limited problems preoperatively in most of the CI users and generally remained stable postoperatively, confirming the results of previous studies on these topics (Claes et al., 2018; Ketterer et al., 2018; Mertens et al., 2020; Calvino et al., 2022). General tasks and demands, community life and family relationships generally improved or remained stable after implantation in most of the CI users. The improvement in communication abilities of the CI users could partly explain these improvements and several studies demonstrated a positive effect of cochlear implantation on the daily lives of both CI users and their relatives (Mo et al., 2005; Ng et al., 2016).
The Nijmegen Cochlear Implant Questionnaire (NCIQ), a commonly used, well-known CI-specific quality of life assessment tool, was not included in our ICF-based CI outcome assessment tool because of its length (60 questions) and because other measures were a better fit for measuring the ICF categories relevant for CI users (Hinderink et al., 2000). In addition, the recently developed Cochlear Implant Quality of Life questionnaire could not be included in the protocol because it is not available nor translated in all languages of the participating centers. Multiple studies proved the benefits of cochlear implantation in severely-to-profoundly hearing-impaired individuals on multiple domains, but a CI is generally unable to address all disabling aspects of severe-to-profound hearing loss (Berrettini et al., 2011; McRackan et al., 2018b; Boisvert et al., 2020; Carlyon and Goehring, 2021). This underlines the importance of implementing the ICF-based CI outcome protocol in the rehabilitation process of CI users as it would allow for the identification of individual healthcare needs of CI users across multiple domains, using a patient-centered approach. The ICF model is a universal classification system aiming to describe functioning and disability in a standardized way using codes, categories and qualifiers (World Health Organization, 2001). The ICF model itself is not a measurement instrument and is therefore not meant for statistical test comparisons. Hence, we used descriptive statistics in this study to describe the overall change and improvement of the participants across the ICF categories relevant for cochlear implantation. In another paper we will statistically compare the raw data of the used measurement instruments in this study. Furthermore, the influence of participants' characteristics (e.g., duration of deafness, etiology) and fitting type (e.g., EAS, bilateral CI) on the CI outcomes will also be studied. Since the ICF Core set for hearing loss was already developed according to the guidelines of Selb et al. (2015) and since cochlear implantation can be considered as a subdomain of hearing loss management, we modified the ICF Core set for hearing loss to create the ICF-based CI outcome assessment protocol and applied it in adult CI candidates (Selb et al., 2015). In future research, it would be interesting to assign measurement tools appropriate for pediatric CI users to the ICF core set for hearing loss to be able to implement it in their rehabilitation process. Additionally, a comparative analysis between participants with and without prior hearing surgical interventions would have been valuable. Since participants who had prior hearing surgical interventions might have different expectations and psychosocial experiences compared to those without any such history, it might affect CI outcomes, particularly in terms of aversiveness results. However, in our study we only have a small sample size (n = 8) of participants who had previous hearing restoration surgeries compared to participants without previous surgeries (n = 64). Comparing these groups could therefore lead to unreliable conclusions, which is why we did not add it in our study. Nevertheless, it would be interesting to explore this in future studies.
5. Conclusion
The selected ICF categories for cochlear implantation and their assigned measurement tools provide a common language and comprehensive assessment protocol for the description and measurement of CI outcomes worldwide, facilitating national and international comparisons on group and individual level in both research and clinical settings. The straightforward outcome description and rating of the ICF-based CI outcome assessment protocol enables CI outcome interpretation by non-experts, which enhances multidisciplinary communication and knowledge on individual healthcare needs in CI users. It can and should be adopted in the rehabilitation process of CI users to allow for a patient-centered approach, addressing a unique combination of not only Body Functions and Structure impairments but also relevant activity limitations, participation restrictions and environmental barriers, which would ultimately benefit CI outcomes.
Data availability statement
The datasets presented in this article are not readily available because to protect study participant privacy, data cannot be shared openly. The public availability of data was not included in the ethics approval of this study. The data management part of the study protocol states that raw participant data can only be accessed by the principal investigators and cannot be shared or given to anyone outside the study team. Requests to access the datasets should be directed to ZWxsZW4uYW5kcmllc0B1emEuYmU=.
Ethics statement
The study was carried out in conformity with the recommendations of the local Ethics Committees and competing authorities (Antwerp 20/27/357; Madrid PI-4359; Perth RGS0000004350; Warsaw KB/3/2021; Würzburg 199/20). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
Conceptualization and writing—review and editing: EAn, AL, PS, HS, MC, JG, LL, DT-V, AA, AK, RH, IA, EAm, PV, VV, and GM. Methodology: EAn, AL, MC, DT-V, AK, IA, EAm, and GM. Formal analysis: EAn and EAm. Writing—original draft preparation and visualization: EAn. All authors have read and agreed to the published version of the manuscript.
Funding
The authors declare financial support was received for the research, authorship, and/or publication of this article. The Antwerp University Hospital receives a research grant from the company MED-EL GmbH, Innsbruck (Austria). MED-EL GmbH, Innsbruck (Austria) was not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
Conflict of interest
IA and EAm are employees of MED-EL GmbH. All participating centers are members of the HEARRING network, which was supported by MED-EL GmbH.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fauot.2023.1257504/full#supplementary-material
References
Adunka, O. F., Pillsbury, H. C., Adunka, M. C., and Buchman, C. A. (2010). Is electric acoustic stimulation better than conventional cochlear implantation for speech perception in quiet? Otol. Neurotol. 31, 1049–1054. doi: 10.1097/MAO.0b013e3181d8d6fe
Agrawal, Y., Pineault, K. G., and Semenov, Y. R. (2018). Health-related quality of life and economic burden of vestibular loss in older adults. Laryng. Invest. Otolaryngol. 3, 8–15. doi: 10.1002/lio2.129
Amann, E., and Anderson, I. (2014). Development and validation of a questionnaire for hearing implant users to self-assess their auditory abilities in everyday communication situations: the Hearing Implant Sound Quality Index (HISQUI19). Acta Otolaryngol. 134, 915–923. doi: 10.3109/00016489.2014.909604
Amoodi, H. A., Mick, P. T., Shipp, D. B., Friesen, L. M., Nedzelski, J. M., Chen, J. M., et al. (2011). The effects of unilateral cochlear implantation on the tinnitus handicap inventory and the influence on quality of life. Laryngoscope 121, 1536–1540. doi: 10.1002/lary.21851
Anderson, I., Baumgartner, W.-D., Böheim, K., Nahler, A., Arnolder, C., and D'Haese, P. (2006). Telephone use: What benefit do cochlear implant users receive? Int. J. Audiol. 45, 446–453. doi: 10.1080/14992020600690969
Andries, E., Gilles, A., Topsakal, V., Vanderveken, O.livier M., Van de Heyning, P., Van Rompaey, V., et al. (2020). Systematic review of quality of life assessments after cochlear implantation in older adults. Audiol. Neurotol. 26, 61–75. doi: 10.1159/000508433
Andries, E., Lorens, A., Skarzyński, P. H., SkarZynski, H., Calvino, M., Gavilan, J., et al. (2022). Evaluating the revised work rehabilitation questionnaire in cochlear implant users cochlear implant outcome assessment based on the international classification of functioning, disability, and health (ICF). Otol. Neurotol. 43, e571–e577. doi: 10.1097/MAO.0000000000003524
Arning, K., and Ziefle, M. (2007). Understanding age differences in PDA acceptance and performance. Computers in human behavior 23, 2904–2927. doi: 10.1016/j.chb.2006.06.005
Arts, R. A., George, E. L., Griessner, A., Zierhofer, C., and Stokroos, R. J. (2015a). Tinnitus suppression by intracochlear electrical stimulation in single-sided deafness: a prospective clinical trial - Part I. Audiol. Neurootol. 20, 294–313. doi: 10.1159/000381936
Arts, R. A., George, E. L., Stokroos, R. J., and Vermeire, K. (2012). Review: cochlear implants as a treatment of tinnitus in single-sided deafness. Curr. Opin. Otolaryngol. Head Neck. Surg. 20, 398–403. doi: 10.1097/MOO.0b013e3283577b66
Arts, R. A., Netz, T., Janssen, A. M., George, E. L., and Stokroos, R. J. (2015b). The occurrence of tinnitus after CI surgery in patients with severe hearing loss: A retrospective study. Int. J. Audiol. 54, 910–917. doi: 10.3109/14992027.2015.1079930
Baguley, D. M. (2010). New insights into tinnitus in cochlear implant recipients. Cochlear. Implants Int. 11, 31–36. doi: 10.1179/146701010X12726366068616
Batuecas-Caletrio, A., Klumpp, M., Santacruz-Ruiz, S., Benito Gonzalez, F., Gonzalez Sanchez, E., and Arriaga, M. (2015). Vestibular function in cochlear implantation: Correlating objectiveness and subjectiveness. Laryngoscope 125, 2371–2375. doi: 10.1002/lary.25299
Berrettini, S., Baggiani, A., Bruschini, L., Cassandro, E., Cuda, D., Filipo, R., et al. (2011). Systematic review of the literature on the clinical effectiveness of the cochlear implant procedure in adult patients. Acta Otorhinolaryngol. Ital. 31, 299–310.
Billinger-Finke, M., Bracker, T., Weber, A., Amann, E., Anderson, I., and Batsoulis, C. (2020). Development and validation of the audio processor satisfaction questionnaire (APSQ) for hearing implant users. Int. J. Audiol. 16, 830. doi: 10.1080/14992027.2019.1697830
Blasco, M. A., and Redleaf, M. I. (2014). Cochlear implantation in unilateral sudden deafness improves tinnitus and speech comprehension: meta-analysis and systematic review. Otol. Neurotol. 35, 1426–1432. doi: 10.1097/MAO.0000000000000431
Boisvert, I., Reis, M., Au, A., Cowan, R., and Dowell, R. C. (2020). Cochlear implantation outcomes in adults: A scoping review. PLoS ONE 15, e0232421. doi: 10.1371/journal.pone.0232421
Boothroyd, A. (1968). Developments in Speech Audiometry. Br. J. Audiol. 2, 3–10. doi: 10.3109/00381796809075436
Boothroyd, A. (2007). Adult aural rehabilitation: what is it and does it work? Trends Amplif. 11, 63–71. doi: 10.1177/1084713807301073
British Society of Audiology (2012). Common principles of rehabilitation for adults with hearing- and/or balance-related problems in routine audiology services. Practice guidance. Available online at: http://www.thebsa.org.uk/wp-content/uploads/2016/10/Practice-Guidance-Common-Principles-of-Rehabilitation-for-Adults-in-Audiology-Services-2016.pdf (accessed July 11, 2023).
Buhagiar, R., Lutman, M. E., Brinton, J. E., and Eyles, J. (2004). Localization performance of unilateral cochlear implant users for speech, tones and noise. Cochlear. Implant. Int. 5, 96–104. doi: 10.1179/cim.2004.5.3.96
Calvino, M., Sánchez-Cuadrado, I., Gavilán, J., Gutiérrez-Revilla, M. A., Polo, R., and Lassaletta, L. (2022). Effect of cochlear implantation on cognitive decline and quality of life in younger and older adults with severe-to-profound hearing loss. Eur. Arch. Otorhinolaryngol. 279, 4745–4759. doi: 10.1007/s00405-022-07253-6
Carlson, M. L. (2020). Cochlear implantation in adults. N. Engl. J. Med. 382, 1531–1542. doi: 10.1056/NEJMra1904407
Carlyon, R. P., and Goehring, T. (2021). Cochlear implant research and development in the twenty-first century: a critical update. J. Assoc. Res. Otolaryngol. 22, 481–508. doi: 10.1007/s10162-021-00811-5
Castro, A., Lassaletta, L., Bastarrica, M., Perez-Mora, R., Josefa De Sarri,á, M., and Gavilán, J. (2008). Benefits from a mobile telephone adapter in Combi40+ cochlear implant users. Acta Otolaryngol. 128, 661–665. doi: 10.1080/00016480701675650
Cieza, A., Fayed, N., Bickenbach, J., and Prodinger, B. (2019). Refinements of the ICF Linking Rules to strengthen their potential for establishing comparability of health information. Disabil. Rehabilit. 41, 574–583. doi: 10.3109/09638288.2016.1145258
Ciorba, A., Bianchini, C., Pelucchi, S., and Pastore, A. (2012). The impact of hearing loss on the quality of life of elderly adults. Clin. Interv. Aging 7, 159. doi: 10.2147/CIA.S26059
Claes, A. J., Van de Heyning, P., Gilles, A., Van Rompaey, V., and Mertens, G. (2018). Cognitive performance of severely hearing-impaired older adults before and after cochlear implantation: preliminary results of a prospective, longitudinal cohort study using the RBANS-H. Otol. Neurotol. 39, e765–e773. doi: 10.1097/MAO.0000000000001936
Cosh, S., Helmer, C., Delcourt, C., Robins, T. G., and Tully, P. J. (2019). Depression in elderly patients with hearing loss: current perspectives. Clin. Interv. Aging 14, 1471–1480. doi: 10.2147/CIA.S195824
Cox, M. R., and Alexander, C. G. (1995). The abbreviated profile of hearing aid benefit. Ear. Hear. 16, 176–186. doi: 10.1097/00003446-199504000-00005
Danermark, B., Granberg, S., Kramer, S. E., Selb, M., and Moller, C. (2013). The creation of a comprehensive and a brief core set for hearing loss using the international classification of functioning, disability and health. Am. J. Audiol. 22, 323–328. doi: 10.1044/1059-0889(2013/12-0052)
Doge, J., Baumann, U., Weissgerber, T., and Rader, T. (2017). Single-sided deafness: impact of cochlear implantation on speech perception in complex noise and on auditory localization accuracy. Otol. Neurotol. 38, e563–e569. doi: 10.1097/MAO.0000000000001520
Finger, M., Escorpizo, R., Bostan, C., and Bie, R. (2014). Work rehabilitation questionnaire (WORQ): development and preliminary psychometric evidence of an ICF-Based Questionnaire for Vocational Rehabilitation. J. Occupat. Rehabilit. 24, 498–510. doi: 10.1007/s10926-013-9485-2
Glade, R., Taylor, E., Culbertson, D. S., and Ray, C. (2020). Overview of current approaches to aural rehabilitation for adults with cochlear implants. Perspect. ASHA Special Interest Groups 5, 1175–1187. doi: 10.1044/2020_PERSP-20-00078
Global Burden of Disease (2021). Hearing loss prevalence and years lived with disability, 1990-2019: findings from the Global Burden of Disease Study 2019. Lancet 397, 996–1009. doi: 10.1016/S0140-6736(21)00516-X
Gopinath, B., Schneider, J., Hickson, L., McMahon, C. M., Burlutsky, G., Leeder, S. R., et al. (2012). Hearing handicap, rather than measured hearing impairment, predicts poorer quality of life over 10 years in older adults. Maturitas 72, 146–151. doi: 10.1016/j.maturitas.2012.03.010
Granberg, S. (2015). Functioning and disability in adults with hearing loss: the preparatory studies in the ICF Core sets for hearing loss project. (Doctoral dissertation, Örebro university).
Granberg, S., Dahlstrom, J., Moller, C., Kahari, K., and Danermark, B. (2014a). The ICF Core Sets for hearing loss–researcher perspective. Part I: Systematic review of outcome measures identified in audiological research. Int. J. Audiol. 53, 65–76. doi: 10.3109/14992027.2013.851799
Granberg, S., Möller, K., Skagerstrand, Å., Möller, C., and Danermark, B. (2014b). The ICF Core Sets for hearing loss: researcher perspective, Part II: Linking outcome measures to the International Classification of Functioning, Disability and Health (ICF). 53, 77–87. doi: 10.3109/14992027.2013.858279
Granberg, S., Pronk, M., Swanepoel, D. W., Kramer, S. E., Hagsten, H., Hjaldahl, J., et al. (2014c). The ICF core sets for hearing loss project: Functioning and disability from the patient perspective. Int. J. Audiol. 53, 777–786. doi: 10.3109/14992027.2014.938370
Granberg, S., Swanepoel, D. W., Englund, U., Möller, C., and Danermark, B. (2014d). The ICF core sets for hearing loss project: International expert survey on functioning and disability of adults with hearing loss using the international classification of functioning, disability, and health (ICF). Int. J. Audiol. 53, 497–506. doi: 10.3109/14992027.2014.900196
Grenness, C., Hickson, L., Laplante-Lévesque, A., and Davidson, B. (2014). Patient-centred care: a review for rehabilitative audiologists. Int. J. Audiol. 53, S60–67. doi: 10.3109/14992027.2013.847286
Hannula, S., Bloigu, R., Majamaa, K., Sorri, M., and Mäki-Torkko, E. (2011). Self-reported hearing problems among older adults: prevalence and comparison to measured hearing impairment. J. Am. Acad. Audiol. 22, 550–559. doi: 10.3766/jaaa.22.8.7
Helvik, A. S., Jacobsen, G., and Hallberg, L. R. (2006). Psychological well-being of adults with acquired hearing impairment. Disabil. Rehabil. 28, 535–545. doi: 10.1080/09638280500215891
Hinderink, J. B., Krabbe, P. F., and Van Den Broek, P. (2000). Development and application of a health-related quality-of-life instrument for adults with cochlear implants: the Nijmegen cochlear implant questionnaire. Otolaryngol. Head Neck. Surg. 123, 756–765. doi: 10.1067/mhn.2000.108203
Holder, J. T., O'Connell, B., Hedley-Williams, A., and Wanna, G. (2017). Cochlear implantation for single-sided deafness and tinnitus suppression. Am. J. Otolaryngol. 38, 226–229. doi: 10.1016/j.amjoto.2017.01.020
Hornsby, B. W., and Kipp, A. M. (2016). Subjective ratings of fatigue and vigor in adults with hearing loss are driven by perceived hearing difficulties not degree of hearing loss. Ear. Hear. 37, e1–10. doi: 10.1097/AUD.0000000000000203
Hoth, S., Rosli-Khabas, M., Herisanu, I., Plinkert, P. K., and Praetorius, M. (2016). Cochlear implantation in recipients with single-sided deafness: Audiological performance. Cochlear. Implant. Int. 17, 190–199. doi: 10.1080/14670100.2016.1176778
Ibrahim, I., da Silva, S. D., Segal, B., and Zeitouni, A. (2017). Effect of cochlear implant surgery on vestibular function: meta-analysis study. J. Otolaryngol. Head Neck Surg. 46, 1–10. doi: 10.1186/s40463-017-0224-0
Johnson, J. A., Cox, R. M., and Alexander, G. C. (2010). Development of APHAB Norms for WDRC hearing aids and comparisons with original norms. Ear. Hear. 31, 47–55. doi: 10.1097/AUD.0b013e3181b8397c
Kay-Rivest, E., Schlacter, J., and Waltzman, S. B. (2022). Cochlear implantation outcomes in the older adult: a scoping review. Cochlear. Implant. Int. 23, 280–290. doi: 10.1080/14670100.2022.2091723
Kerber, S., and Seeber, B. U. (2012). Sound localization in noise by normal-hearing listeners and cochlear implant users. Ear. Hear. 33, 445–457. doi: 10.1097/AUD.0b013e318257607b
Ketterer, M. C., Knopke, S., Häußler, S. M., Hildenbrand, T., Becker, C., Gräbel, S., et al. (2018). Asymmetric hearing loss and the benefit of cochlear implantation regarding speech perception, tinnitus burden and psychological comorbidities: a prospective follow-up study. Eur. Arch. Oto-Rhino-Laryngol. 275, 2683–2693. doi: 10.1007/s00405-018-5135-9
Kim, D. K., Bae, S. C., Park, K. H., Jun, B. C., Lee, D. H., Yeo, S. W., et al. (2013). Tinnitus in patients with profound hearing loss and the effect of cochlear implantation. Eur. Arch. Otorhinolaryngol. 270, 1803–1808. doi: 10.1007/s00405-012-2193-2
Kim, D. K., Moon, I. S., Lim, H. J., Yoo, S. Y., Heo, K. W., Bae, S. C., et al. (2016). Prospective, Multicenter Study on Tinnitus Changes after Cochlear Implantation. Audiol. Neurootol. 21, 165–171. doi: 10.1159/000445164
Lin, F. R., Yaffe, K., Xia, J., Xue, Q.-L., Harris, T. B., Purchase-Helzner, E., et al. (2013). Hearing loss and cognitive decline in older adults (Report). JAMA Internal Med. 173, 293. doi: 10.1001/jamainternmed.2013.1868
Lorens, A., Mertens, G., and Kurz, A. (2020). “Audiological Rehabilitation After Cochlear Implantation: A New Model Developed Based on the International Classification of Functioning, Disability and Health (ICF),” in BMC Medical Informatics and Decision Making. doi: 10.21203/rs.3.rs-74876/v1
McRackan, T. R., Bauschard, L. M., Hatch, R. J., Franko-Tobin, A. E., Droghini, A. H., Velozo, R. C., et al. (2018a). Meta-analysis of cochlear implantation outcomes evaluated with general health-related patient-reported outcome measures. Otol. Neurotol. 39, 29–36. doi: 10.1097/MAO.0000000000001620
McRackan, T. R., Bauschard, M., Hatch, J. L., Franko-Tobin, E., Droghini, H. R., Nguyen, S. A., et al. (2018b). Meta-analysis of quality-of-life improvement after cochlear implantation and associations with speech recognition abilities. Laryngoscope 128, 982–990. doi: 10.1002/lary.26738
McRackan, T. R., Fabie, J. E., Bhenswala, P. N., Nguyen, S. A., and Dubno, J. R. (2019). General health quality of life instruments underestimate the impact of bilateral cochlear implantation. Otol. Neurotol. 40, 745–753. doi: 10.1097/MAO.0000000000002225
Meli, A., Aud, B. M., Aud, S. T., Aud, R. G., and Cristofari, E. (2016). Vestibular function after cochlear implant surgery. Cochlear. Implant. Int. 17, 151–157. doi: 10.1179/1754762815Y.0000000014
Mertens, G., Andries, E., Claes, A. J., Topsakal, V., Van de Heyning, P., Van Rompaey, V., et al. (2020). Cognitive improvement after cochlear implantation in older adults with severe or profound hearing impairment: a prospective, longitudinal, controlled, multicenter study. Ear. Hear. 42, 606–614. doi: 10.1097/AUD.0000000000000962
Mertens, G., Andries, E., Kurz, A., Tȧvora-Vieira, D., Calvino, M., Amann, E., et al. (2022). Towards a consensus on an ICF-based classification system for horizontal sound-source localization. J. Personal. Med. 12, 1971. doi: 10.3390/jpm12121971
Meyer, C., Grenness, C., Scarinci, N., and Hickson, L. (2016). What is the international classification of functioning, disability and health and why is it relevant to audiology? Semin. Hear. 37, 163–186. doi: 10.1055/s-0036-1584412
Mo, B., Lindbæk, M., and Harris, S. (2005). Cochlear implants and quality of life: a prospective study. Ear. Hear. 26, 186–194. doi: 10.1097/00003446-200504000-00006
Ng, Z. Y., Lamb, B., Harrigan, S., Archbold, S., Athalye, S., and Allen, S. (2016). Perspectives of adults with cochlear implants on current CI services and daily life. Cochlear. Implant. Int. 17, 89–93. doi: 10.1080/14670100.2016.1157314
Noble, W., Jensen, N. S., Naylor, G., Bhullar, N., and Akeroyd, M. A. (2013). A short form of the Speech, Spatial and Qualities of Hearing scale suitable for clinical use: the SSQ12. Int. J. Audiol. 52, 409–412. doi: 10.3109/14992027.2013.781278
Palmer, C. V., Bentler, R., and Mueller, H. G. (2006). Amplification with digital noise reduction and the perception of annoying and aversive sounds. Trends Amplif. 10, 95–104. doi: 10.1177/1084713806289554
Pichora-Fuller, M. K., Kramer, S. E., Eckert, M. A., Edwards, B., Hornsby, B. W. Y., Humes, L. E., et al. (2016). Hearing impairment and cognitive energy: the framework for understanding effortful listening (FUEL). Ear. Hear. 37, 5S−27S. doi: 10.1097/AUD.0000000000000312
Psarros, C., and Love, S. (2016). The role of the world health organization's international classification of functioning, health and disability in models of infant cochlear implant management. Semin. Hear. 37, 272–290. doi: 10.1055/s-0036-1584414
Rasmussen, K. M. B., West, N. C., Bille, M., Sandvej, M. G., and Cayé-Thomasen, P. (2022). Cochlear implantation improves both speech perception and patient-reported outcomes: a prospective follow-up study of treatment benefits among adult cochlear implant recipients. J. Clin. Med. 11, 2257. doi: 10.3390/jcm11082257
Schaefer, S., Henderson, L., Graham, J., Broomfield, S., Cullington, H., Schramm, D., et al. (2017). Review of outcomes and measurement instruments in cochlear implantation studies. Cochlear. Implant. Int. 18, 237–239. doi: 10.1080/14670100.2017.1353761
Selb, M., Escorpizo, R., Kostanjsek, N., Stucki, G., Ustun, B., and Cieza, A. (2015). A guide on how to develop an international classification of functioning, disability and health core set. Eur. J. Phys. Rehabil. Med. 51, 105–117.
Sun, D. Q., Ward, B. K., and Semenov, Y. R. (2014). Bilateral vestibular deficiency: quality of life and economic implications (Report). JAMA Otolaryngol. Head Neck Surg. 140, 527. doi: 10.1001/jamaoto.2014.490
Tordrup, D., Smith, R., Kamenov, K., Bertram, M. Y., Green, N., and Chadha, S. (2022). Global return on investment and cost-effectiveness of WHO's HEAR interventions for hearing loss: a modelling study. Lancet Glob Health 10, e52–e62. doi: 10.1016/S2214-109X(21)00447-2
Van de Heyning, P., Távora-Vieira, D., Mertens, G., Van Rompaey, V., Rajan, G. P., Müller, J., et al. (2017). Towards a unified testing framework for single-sided deafness studies: a consensus paper. Audiol. Neurotol. 21, 391–398. doi: 10.1159/000455058
Van Leeuwen, M. L., Merkus, T. P., Pronk, E. M., Van Der Torn, E. M., Maré, E. M., Goverts, E. S., et al. (2017). Overlap and nonoverlap between the ICF core sets for hearing loss and otology and audiology intake documentation. Ear. Hear. 38, 103–116. doi: 10.1097/AUD.0000000000000358
Vermeulen, K., Woestyn, M., Oostra, K., Geers, S., Ryngaert, K., Van de Velde, K., et al. (2019). Cross-Cultural adaptation and psychometric evaluation of the dutch version of the work rehabilitation questionnaire (WORQ-VL). J. Occup. Rehabilit. 29, 514–525. doi: 10.1007/s10926-018-9812-8
Vila, P. M., Hullar, T. E., Buchman, C. A., and Lieu, J. E. (2016). Analysis of outcome domains in adult cochlear implantation: a systematic review. Otolaryngol. Head Neck. Surg. 155, 238–245. doi: 10.1177/0194599816641382
WHO (2018). International classification of diseases for mortality and morbidity statistics (11th Revision). Available online at: https://icd.who.int/browse11/l-m/en (accessed July 11, 2023).
World Health Organization (2001). International classification of functioning, disability and health. Geneva: WHO.
World Health Organization (2018). International classification of diseases for mortality and morbidity statistics (11th Revision).
World Health Organization (2021). World report on hearing. Geneva: World Health Organization. Licence: CC BY-NC-SA 3.0 IGO.
Keywords: ICF, cochlear implantation, outcome assessment, cochlear implant outcomes, ICF qualifiers
Citation: Andries E, Lorens A, Skarżyński PH, Skarżyński H, Calvino M, Gavilán J, Lassaletta L, Tavora-Vieira D, Acharya A, Kurz A, Hagen R, Anderson I, Amann E, Van de Heyning P, Van Rompaey V and Mertens G (2023) Implementation of the International Classification of Functioning, Disability and Health model in cochlear implant recipients: a multi-center prospective follow-up cohort study. Front. Audiol. Otol. 1:1257504. doi: 10.3389/fauot.2023.1257504
Received: 12 July 2023; Accepted: 15 August 2023;
Published: 05 September 2023.
Edited by:
Mehdi Abouzari, University of California, Irvine, United StatesReviewed by:
Karen Tawk, University of California, Irvine, United StatesSasan Dabiri, Tehran University of Medical Sciences, Iran
Copyright © 2023 Andries, Lorens, Skarżyński, Skarżyński, Calvino, Gavilán, Lassaletta, Tavora-Vieira, Acharya, Kurz, Hagen, Anderson, Amann, Van de Heyning, Van Rompaey and Mertens. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ellen Andries, ZWxsZW4uYW5kcmllc0B1emEuYmU=