 Sharon J. Feng
Sharon J. Feng François Voruz
François Voruz Michelle Yu
Michelle Yu Anil K. Lalwani
Anil K. Lalwani- 1Columbia University Vagelos College of Physicians and Surgeons, New York, NY, United States
- 2Department of Otolaryngology—Head and Neck Surgery, New York-Presbyterian/Columbia University Irving Medical Center, New York, NY, United States
- 3Department of Mechanical Engineering, Columbia University, New York, NY, United States
Interest in hearing loss associated with COVID-19 has increased since the pandemic started. Early on during the spread of SARS-CoV-2 across the globe, reports of smell and taste disorders secondary to COVID-19 emerged, and to a lesser extent, reports of sensorineural hearing loss also surfaced. This raised questions regarding changes in the epidemiology of hearing loss and modifications to otologic practice that have evolved in response to the COVID-19 pandemic. To elucidate these questions, we performed a comprehensive literature search, including articles up to November 2022, using “COVID hearing loss” in MEDLINE. A total of 153 articles were included for full-text review and data extraction. There are several proposed mechanisms through which COVID-19 may contribute to hearing loss—direct viral infection, microthrombi, or hemorrhage. There is a growing repository of case reports and series on SARS-CoV-2-associated sensorineural hearing loss, with variable quality. Most patients who experienced hearing loss did so within a month of infection, with most patients' symptoms resolving within 2 weeks. The growing body of literature discussing SARS-CoV-2-associated hearing loss does not suggest a significant rise in the occurrence of sensorineural or overall hearing loss. In this ongoing COVID-19 era, hearing loss should be approached in the same state-of-the-art manner as before the pandemic.
1. Introduction
COVID-19 is an emerging viral disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Figure 1), which first emerged in Wuhan, China, in December 2019. It has since spread to the rest of the world, reaching pandemic status in March 2020. According to the World Health Organization, as of May 28th, 2023, over 767 million confirmed cases and over 6.9 million deaths have been reported globally (WHO, 2023). From the beginning, COVID-19 has changed the practice of medicine. Although the absolute number of otolaryngological emergencies drastically decreased during the pandemic (Gelardi et al., 2020; Pontillo et al., 2020; Chari et al., 2021; Riemann et al., 2021; Pereira et al., 2023), the virus and its sequelae have brought otolaryngologic expertise to the forefront of medical care (Pandian and Brodsky, 2021). Perhaps the most far-reaching effects on the public were bringing to light the actual depth of the nasal cavity when undergoing a nasopharyngeal swab test. In addition, over time, the world began to recognize smell and taste disorders—an underrepresented aspect of rhinology—and expanded the relevance of these disorders to the general population and not just patients with olfaction-reliant professions. Finally, patients with severe acute respiratory failure requiring prolonged mechanical ventilation often relied on longitudinal and interdisciplinary care facilitated by otolaryngologists for both tracheostomy placement and subsequent encounters; this was especially true in cases involving long-term sequelae such as airway stenosis, dysphagia, and dysphonia. Among other symptoms and signs, hearing loss attributed to COVID-19 has been the subject of increasing medical attention within the literature.
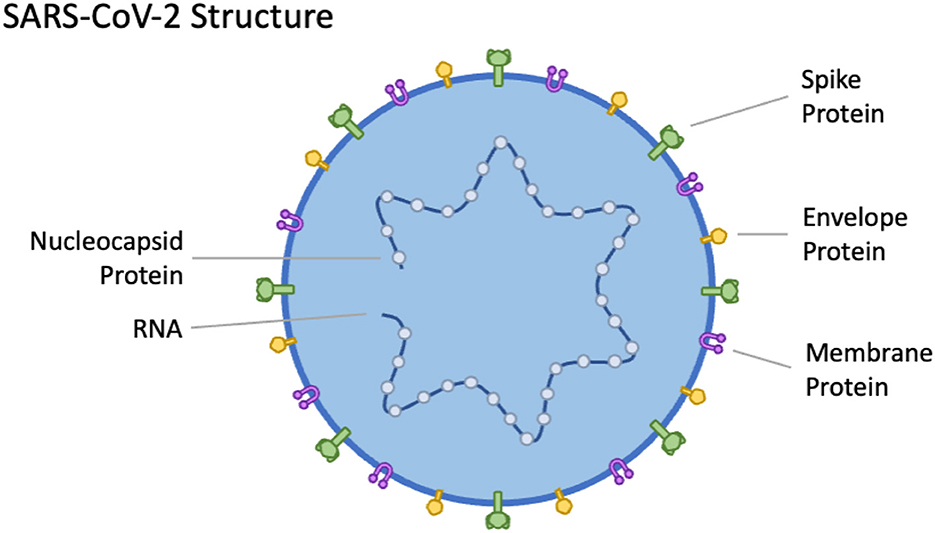
Figure 1. Simplified structure of the SARS-CoV-2, which is comprised of an RNA genome and several key membrane proteins.
This narrative review will focus on COVID-19 and its effect on hearing, as, even 3 years after the beginning of the pandemic, specialists and general clinicians still struggle to answer when a patient or a colleague asks if SARS-CoV-2 may be responsible for hearing loss. Using our clinical experience and a comprehensive literature review, we aim to address the following questions: Has COVID-19 changed the epidemiology of hearing loss, and has the otologic practice changed in response to the pandemic?
2. Materials and methods
The terms “COVID hearing loss” were searched in MEDLINE using PubMed in June 2022. Two hundred ninety-eight abstracts were screened; criteria for inclusion were English language manuscripts that discussed possible hearing loss after SARS-CoV-2 infection, vaccination, or treatment for the disease. Manuscripts that discussed broader, non-hearing loss related issues during the pandemic were excluded. 10 additional manuscripts, encompassing articles published up until November 2022, were identified after the initial screening processes and included in this review. Overall, 153 articles underwent full text review and data extraction (Figure 2).
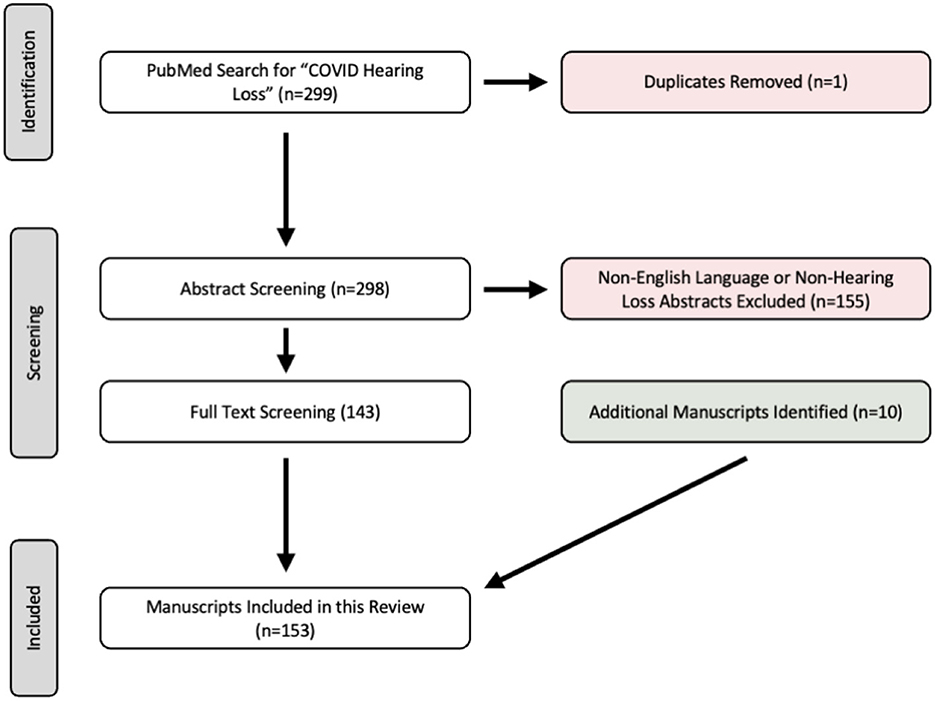
Figure 2. Flow chart of literature search and screening process.
3. Results
3.1. Viruses and hearing loss
Hearing loss is considered the fifth leading cause of disability in the world, and its prevalence constantly increases with the aging population (WHO, 2019). Hearing loss is associated with lower professional achievements (Chadha et al., 2017), impairment of social interactions, and cognitive decline (Cherko et al., 2016). Hearing loss is divided into three categories: (1) conductive hearing loss, where there is mechanical impairment of the external soundwave transmission to the inner ear, (2) sensorineural hearing loss (SNHL), where there is a neurological inability to transduce a soundwave into an electrical signal that is then interpreted by the brain, and (3) mixed hearing loss, where conductive and SNHL are combined. Conductive hearing loss has many etiologies, among which the most common is the transient middle ear effusion during an upper respiratory tract infection. Conductive hearing loss is frequently reversible as the etiology is mechanical in nature, and either self-resolves or may be surgically correctable. On the other hand, SNHL is usually permanent, as the mechanosensory inner ear hair cells do not regenerate. In particular, sudden sensorineural hearing loss (SSNHL) is a well-recognized type of SNHL, with many possible etiologies (infectious, neoplastic, immunological, circulatory, and neurologic), although primarily idiopathic (Hughes et al., 1996). To date, treatment of SNHL is limited to conventional hearing aids and cochlear implants, which only partially alleviate the symptoms.
The inner ear is vulnerable to certain viruses which may induce SNHL, such as herpes simplex (HSV), varicella-zoster virus, cytomegalovirus (CMV), Epstein-Barr virus, mumps, measles, rubella, hepatitis, human immunodeficiency virus (HIV), Lassa, Zika, Ebola, enterovirus, West Nile virus, or lymphocytic choriomeningitis virus (LCMV) (Cohen et al., 2014; Ficenec et al., 2019; Jeong et al., 2021). The mechanisms may include viral-mediated auditory neuritis, cochleitis, cross-reaction of antigens in the inner ear (Kilic et al., 2020), microvascular involvement, and, less likely, temporal lobe involvement. Coronaviruses can also cause otitis media (Liaw et al., 2021; Marom et al., 2021); however, no literature links hearing loss or vestibular symptoms with the two previously encountered types of severe acute respiratory syndrome coronaviruses [severe acute respiratory syndrome (SARS) and middle east respiratory syndrome (MERS)] (Almufarrij et al., 2020).
3.2. Pathophysiology of COVID-19 infection
SARS-CoV-2 infects cells through the angiotensin-converting enzyme 2 (ACE2) receptor and can infect central and peripheral nervous systems (Wan et al., 2021). Given the virus' affinity for mucosal surfaces, the ear is vulnerable to the virus through the mucosal path from the nasopharynx provided by the Eustachian tube. Of note, goblet cells lining the Eustachian tube and middle ear mucosa express ACE2 receptors; the presence of these receptors supports the theory that the Eustachian tube may play an important role as an entry route for SARS-CoV-2 into the middle ear (Jeong et al., 2021). The cochlea itself, while housed mainly in bone, still possesses semi-permeable openings, namely the round window membrane and stapedial annular ligament and footplate (Salt and Plontke, 2009). Thus, the inner ear may be infected by the virus not only through nervous system infection but also through continuity with infection-vulnerable mucosal surfaces in the middle ear. In several studies conducted on intra-operative ears and on cadaveric specimens, SARS-CoV-2 has been detected in the mastoid and middle ear (Frazier, 2020; Jeican et al., 2021; Raad et al., 2021; Kurabi et al., 2022).
SARS-CoV-2 may also be implicated in hearing loss through other indirect mechanisms. For example, with its propensity for increasing the incidence of microthrombi and microhemorrhage (Wan et al., 2021), SARS-CoV-2 could theoretically induce SNHL, given that the inner ear is a sensitive organ with terminal vascularity and, therefore, vulnerable to ischemia (Figure 3) (Tabuchi et al., 2002; Mom et al., 2005; Gyo, 2013). Additionally, ischemic stroke and hemorrhagic transformation—both seen in severe COVID-19—along some portions of the auditory pathway could theoretically induce SNHL, although rare (Bamiou, 2015). In the following sections, we review published studies that contribute to our understanding of COVID-19's place in the landscape of viral hearing loss.
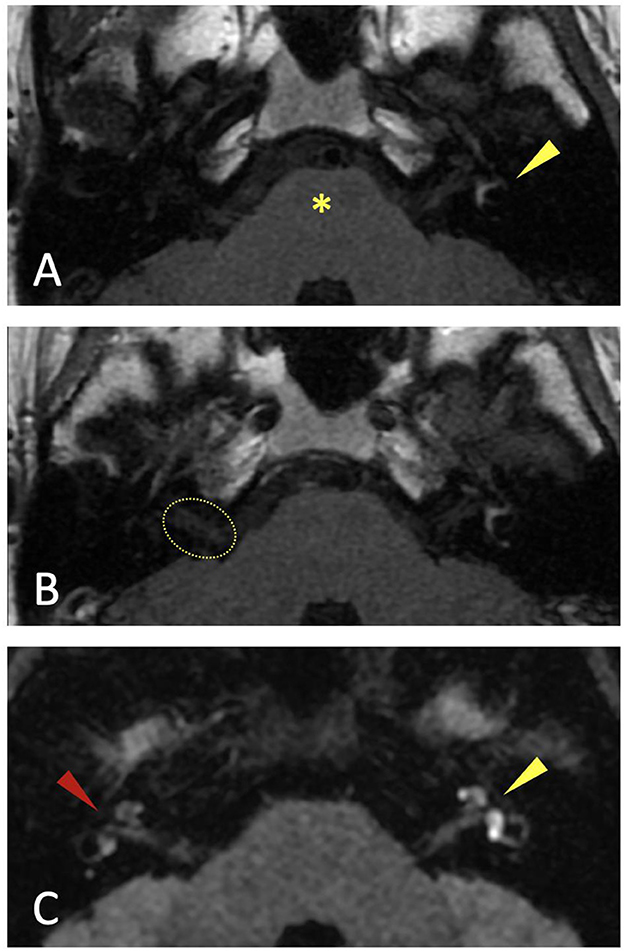
Figure 3. MRI of the internal auditory canals of an 18-year-old woman COVID-19 positive with bilateral sudden sensorineural hearing loss, consistent with bilateral intralabyrinthine hemorrhage greater on the left. (A) Axial T1 pre-contrast. Increased signal in the left labyrinth (arrowhead), consistent with the presence of methemoglobin from blood. The pons is indicated by the star. (B) Axial T1 post-contrast (gadolinium). No abnormal enhancement indicating an underlying inflammatory or tumoral process in the labyrinths or in the internal auditory canals. The dotted ellipse indicates the right internal auditory canal. (C) Axial 3D-FLAIR demonstrating signal abnormality suggestive of intralabyrinthine hemorrhage on the left side (yellow arrowhead), and possibly on the right (red arrowhead).
3.3. Direct effects of COVID-19 on hearing
3.3.1. Otitis media
SARS-CoV-2 can induce acute otitis media (Raad et al., 2021), and a multicentered prospective study comparing audiometry and symptoms in 331 patients with and 80 without COVID-19 did not find a difference in the hearing status of the infected patients, even at 3 months follow-up, although they may present with aural symptoms (Bhatta et al., 2022).
3.3.2. Sudden sensorineural hearing loss
Most of the articles about COVID-19 and SSNHL are case reports, which by their nature have limited generalizability and can only be used to establish associative, not causal, relationships. No definitive conclusions could be drawn from systematic reviews and meta-analyses conducted at various time points (Almufarrij and Munro, 2021; Fancello et al., 2022; Jafari et al., 2022; Maleki et al., 2022). One systematic review and meta-analysis suggested that SARS-CoV-2 may impair hearing, but most available literature relies on case reports (Fancello et al., 2022). It is well known in the research community that association does not equate with causality; as such, the temporal association between SNHL and an active SARS-CoV-2 infection does not necessarily imply a causal relationship. That said, rare potential COVID-19-induced SSNHL cases with more robust causality were also reported, describing—in addition to concomitant SARS-CoV-2 infection—unusual clinical and radiological features, suggesting unusual SSNHL etiology. The main features noted by these case reports included bilateral involvement and magnetic resonance imaging (MRI) changes compatible with labyrinthitis or intra-labyrinthine hemorrhage (Figure 3) (Chern et al., 2021; Edwards et al., 2021; Ozer and Alkan, 2021; Perret et al., 2021; Da Silva et al., 2022). Importantly, when hearing loss was correlated with MRI abnormalities, the severity increased, bilateral in half of the cases, without recovery (Fancello et al., 2022).
In a survey of more than 200 American otorhinolaryngologists in March 2021, most did not notice any rise in SSNHL incidence during the pandemic (Pool et al., 2022). Most studies exploring the incidence of SSNHL during the pandemic compared to before the pandemic found no difference (Aslan and Cicek, 2021; Chari et al., 2021; Chao and Young, 2022; Parrino et al., 2022). Some found a decreased incidence of SSNHL (Doweck et al., 2022), some an increased incidence, without clear explanation (Wichova et al., 2021). In one study, no SARS-CoV-2 infection was found in 25 consecutive SSNHL patients during the pandemic (van Rijssen et al., 2022). A systematic review from 2022 found inconsistent and contradictory results, unable to determine whether SARS-CoV-2 has contributed to the increased incidence of SSNHL worldwide (Meng et al., 2022a).
Overall, studies agreed that hearing loss during the pandemic or active SARS-CoV-2 infection should not sway the clinician from following the standardized audiological workup (Guigou et al., 2021; Malesci et al., 2022). These patients should still be managed according to clinical practice guidelines, for instance, guidelines published by the American Academy of Otolaryngology-Head and Neck Surgery (Chandrasekhar, 2019).
3.3.3. Congenital hearing loss
SARS-CoV-2 has the potency to be vertically transmitted from the infected—even asymptomatic—mother (Sevilla-Montoya et al., 2021; Vigil-Vázquez et al., 2022), and therefore could affect the hearing of newborns in a similar manner as other hearing-nociceptive congenital viruses (CMV, rubella, LCMV, HIV, HSV, Zika). Although the follow-up is relatively short, a recent systematic review found some publications demonstrating that maternal COVID-19 does not affect newborn hearing, whereas some found an effect, especially in mid- and late-stage pregnancy (Meng et al., 2022b). Putative pathophysiological mechanisms include systemic hypoxia in the mother, intrauterine hypoxia secondary to placental dysfunction, and vertical transmission through the placenta. The authors conclude that whether SARS-CoV-2 infection in mothers will affect the hearing of newborns remains unclear.
Adjacent to the potential direct vertical effect of SARS-CoV-2 on newborn hearing, the pandemic has affected congenital hearing loss through delayed diagnosis. Congenital hearing loss affects 1–2 per 1000 births, impairing speech development, especially if late diagnosed (Lieu et al., 2020). Early detection and intervention are paramount for cognitive and social development. For this reason, within the last 25 years, several countries implemented systematic neonatal hearing screening in the maternity ward (Grandori, 1999), with effective results (Nelson et al., 2008; Edmond et al., 2022). Depending on the waning and waxing phases of the pandemic, the usual course of medical care was compromised, including access to universal neonatal hearing screening. Additionally, an increase in births out of the hospitals has been described. A study estimated that up to 50% of infants born with hearing loss in Maryland (USA) in 2021 may be delayed in diagnosis due to the pandemic (Jenks et al., 2022).
3.4. Indirect effects of COVID-19 on hearing
3.4.1. Ototoxicity
Apart from SARS-CoV-2 itself, many medications used to treat patients with COVID-19 are considered potentially ototoxic. These medications include quinine-derivatives (Altulea et al., 2021; Singh et al., 2021), which were ineffective in treating COVID-19 infection, loop diuretics, and antiviral drugs (Monteiro, 2020; Prayuenyong et al., 2020; Coffin et al., 2021; De Luca et al., 2021; Little and Cosetti, 2021). Admission to the intensive care unit (ICU) also confounds the incidence of SNHL in COVID-19 patients, given that these patients are more likely to be treated with ototoxic loop diuretics and may require dialysis for renal insufficiency or suffer from septic shock. Therefore, unusual SNHL during and after ICU could be incorrectly (Gerstacker et al., 2021) attributed to SARS-CoV-2. A systematic review found that, although uncommon, the likelihood of bilateral SSNHL was significantly higher in COVID-19 patients than in the general population, which may represent the bilateral nature of ototoxicity-driven SNHL (Meng et al., 2022a).
3.4.2. Vaccination
Cases of SSNHL after COVID-19 vaccination have been reported, though the causality remains unclear. Several pathophysiological mechanisms of immunization-induced SNHL have been proposed, such as immunocomplex-mediated autoimmune response directed toward the cochlea (Okhovat et al., 2015), or reactivation of latent virus resulting in cochlear inflammation. As side effects of newly developed COVID-19 vaccines were subject to public and scientific scrutiny, proper studies specifically assessed the risk of SNHL, with comforting conclusions (Pisani et al., 2022). No association between vaccination and an increased rate of SSNHL compared to the expected incidence in the general population was noted in a large analysis (Formeister, 2022). Another study concluded that an increased risk of SSNHL might be associated with Pfizer vaccine, however with a minimal effect size (Yanir et al., 2022). The most frequent otolaryngological side-effects of COVID-19 vaccines are audio-vestibular symptoms, but none severe or life-threatening, and the underlying mechanisms are still mostly unknown (Colizza et al., 2022). Thus, COVID-19 vaccine-related SSNHL is considered rare, and the benefit of vaccination far outweighs the risks (Pisani et al., 2022; Ulrich et al., 2022).
3.4.3. Communication impairments with masks
The hearing-impaired population indirectly encountered negative consequences on their hearing during the pandemic for two main reasons. First, face masks hide lip movements and decrease speech recognition, especially in higher frequencies; this becomes more apparent in levels of high background noise (Magee et al., 2020; Rahne et al., 2021; Toscano and Toscano, 2021; Seol et al., 2023). Second, social distancing led to increased physical distance between people, which reduces the signal-to-noise ratio of sound. Consequently, there was more anxiety and stress during the pandemic in the hearing-impaired population than in the standard population (Maleki et al., 2022).
4. Discussion
In April 2020, the first article reporting a case of SNHL attributed to COVID-19 was published in Thailand, the second country touched by the pandemic after China (Sriwijitalai and Wiwanitkit, 2020). Unfortunately, no quantification nor qualification of the hearing loss was described, and apart from the presence of concomitant SARS-CoV-2 infection, no evidence of causality could be drawn. Case reports with similar observations appeared progressively during the pandemic, describing the occurrence of SNHL in patients infected with SARS-CoV-2. Since the world medical corps and the public had no experience with COVID-19, any symptoms during active infection could be attributed to the emergent disease. As such, the literature was flooded with case reports and series that appeared to be lower in quality, in attempt to quickly disseminate information on this novel virus. Given the uncertainty surrounding the disease, the pandemic opened the door to a suboptimal review process and allowed for less rigorous research methods during the publishing frenzy, leading to a substantial number of retracted articles (Bramstedt, 2020; Shimray, 2022).
Self-reported hearing loss and other ear symptoms—such as discomfort, fullness, and tinnitus—are nonspecific and frequently occur in many systemic and upper respiratory viral illnesses. Conductive hearing loss resulting from middle ear effusion is expected and will resolve spontaneously without impairing long-term cochlear function. Conversely, SNHL can potentially impair long-term hearing and should be addressed differently. Additionally, a mild sensorineural hearing loss associated with middle ear effusion is more compatible with an otitis media (Malesci et al., 2022) than with an unusual SNHL supposedly attributed to COVID-19 (Gunay et al., 2021), having in mind that the accuracy of the—inherently subjective—audiometry depends on the physical and psychological state of the patient. Hearing symptoms are frequent and likely due to transient middle ear involvement and Eustachian tube dysfunction, without abnormal hearing threshold shift (Gallus et al., 2021; Bhatta et al., 2022). One must therefore be especially careful when reporting “hearing loss” in the context of a viral disease.
That said, a substantial amount of COVID-19-related hearing loss literature deals with symptoms only, self-reported by a variable proportion of infected patients (up to 50%) (Elibol, 2021; AlJasser et al., 2022; Almishaal and Alrushaidan, 2022; Deva et al., 2022; Savtale et al., 2022; Vielsmeier et al., 2022). These reports often did not quantify or qualify the hearing (Wagatsuma et al., 2022), and therefore were limited in their contributions to the literature (Almufarrij and Munro, 2021; Trott et al., 2022). It is also important to consider that hearing loss may have been underreported by patients during the pandemic, as many patients avoided hospitals (by choice or not). Moreover, a large survey examining auditory symptoms from individuals with confirmed or suspected SARS-CoV-2 infection found inconsistent reporting and recall bias, as well as possible nocebo effects (Saunders et al., 2022). A scoping review concluded that the majority of patients who experienced hearing symptoms during COVID-19 did so within a month, most experiencing complete resolution within 2 weeks. The pattern was consistent with the natural history of a systemic viral infection (Ong and Cruz, 2022).
5. Conclusion
Since the onset of the pandemic, case reports regarding COVID-19 and hearing loss have been published, and pathophysiological mechanisms have been proposed. However, the quality of published literature is highly variable, reflecting the need for rapid dissemination of information during the worldwide pandemic. Although some reports of hearing loss attributed to SARS-CoV-2 are well documented, the literature does not support a significant rise in the occurrence of SSNHL or hearing loss in general. Therefore, in this ongoing COVID-19 era, hearing loss should be approached in the same state-of-the-art manner as before the pandemic, balancing the risks and benefits of therapeutic interventions.
Author contributions
SF and FV: substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of data for the work. MY and AL: drafting the work or revising it critically for important intellectual content. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author AL declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
AlJasser, A., Alkeridy, W., Munro, K. J, Plack, C. J. (2022). Is COVID-19 associated with self-reported audio-vestibular symptoms? Int. J. Audiol. 61, 832–840. doi: 10.1080/14992027.2021.1957161
Almishaal, A. A., and Alrushaidan, A. A. (2022). Short- and long-term self-reported audiovestibular symptoms of SARS-CoV-2 infection in hospitalized and nonhospitalized patients. Audiol. Neurootol. 27, 297–311. doi: 10.1159/000521963
Almufarrij, I., and Munro, K. J. (2021). One year on: an updated systematic review of SARS-CoV-2, COVID-19 and audio-vestibular symptoms. Int. J. Audiol. 60, 935–945. doi: 10.1080/14992027.2021.1896793
Almufarrij, I., Uus, K., and Munro, K. J. (2020). Does coronavirus affect the audio-vestibular system? a rapid systematic review. Int. J. Audiol. 59, 487–491. doi: 10.1080/14992027.2020.1776406
Altulea, D., Maassen, S., Baranov, M. V., and van den Bogaart, G. (2021). What makes (hydroxy)chloroquine ineffective against COVID-19: insights from cell biology. J. Mol. Cell Biol. 13, 175–184. doi: 10.1093/jmcb/mjab016
Aslan, M., and Cicek, M. T. (2021). Can isolated sudden sensorineural hearing loss (SSNHL) and idiopathic acute facial paralysis (Bell's palsy) be symptoms of COVID-19? Am. J. Otolaryngol. 42, 103129. doi: 10.1016/j.amjoto.2021.103129
Bamiou, D. E. (2015). Hearing disorders in stroke. Handb. Clin. Neurol. 129, 633–647. doi: 10.1016/B978-0-444-62630-1.00035-4
Bhatta, S., Sharma, S., Sharma, D., Maharjan, L., Bhattachan, S., Sah, M. K, et al. (2022). Study of hearing status in COVID-19 Patients: a multicentered review. Indian J. Otolaryngol. Head Neck. Surg. 74, 3036–3042. doi: 10.1007/s12070-021-02710-w
Bramstedt, K. A. (2020). The carnage of substandard research during the COVID-19 pandemic: a call for quality. J. Med. Ethics. 46, 803–807. doi: 10.1136/medethics-2020-106494
Chadha, S. L., Lucero agarwal, Paraz, Ambett, and Ranjeeta. (2017). Global costs of unaddressed hearing loss and costs-effectiveness of interventions. A WHO report.
Chandrasekhar, S. S, Do, B. S. T, Schwartz, S. R, Bontempo, L. J, Faucett, E. A, and Finestone, S. A. (2019). Clinical practice guideline: sudden hearing loss (Update). Otolaryngol. Head Neck Surg. 161(1_suppl):S1–S45. doi: 10.1177/0194599819859885
Chao, C. H., and Young, Y.H. (2022). Evolution of incidence of audiovestibular disorders during the pandemic COVID-19 period. Eur. Arch. Otorhinolaryngol. 279, 3341–3345. doi: 10.1007/s00405-021-07037-4
Chari, D. A, Parikh, A., Kozin, E. D, Reed, M., and Jung, D. H. (2021). Impact of COVID-19 on presentation of sudden sensorineural hearing loss at a single institution. Otolaryngol. Head Neck. Surg. 165, 163–165. doi: 10.1177/0194599820974685
Cherko, M., Hickson, L., and Bhutta, M. (2016). Auditory deprivation and health in the elderly. Maturitas 88, 52–57. doi: 10.1016/j.maturitas.2016.03.008
Chern, A., Famuyide, A. O, Moonis, G., and Lalwani, A. K. (2021). Bilateral sudden sensorineural hearing loss and intralabyrinthine hemorrhage in a patient with COVID-19. Otol. Neurotol. 42, e10–e14. doi: 10.1097/MAO.0000000000003233
Coffin, A. B, Boney, R., Hill, J., Tian, C., and Steyger, P. S. (2021). Detecting novel ototoxins and potentiation of ototoxicity by disease settings. Front. Neurol. 12, 725566. doi: 10.3389/fneur.2021.725566
Cohen, B. E., Durstenfeld, A., and Roehm, P. C. (2014). Viral causes of hearing loss: a review for hearing health professionals. Trends Hear. 18, 2331216514541361. doi: 10.1177/2331216514541361
Colizza, A., Ralli, M., Turchetta, R., Minni, A., Greco, A., and de Vincentiis, M. (2022). Otolaryngology adverse events following COVID-19 vaccines. Eur. Rev. Med. Pharmacol. Sci. 26, 4113–4116. doi: 10.26355/eurrev_202206_28981
Da Silva, V. A. R., Villarim, A. P., Bem, M. C. F., Filho, M. C. M., Castilho, A. M., Bezerra, T. F. P., et al. (2022). SARS-CoV-2 infection with bilateral intralabyrinthine hemorrhage. Clin. Case Rep. 10, e6177. doi: 10.1002/ccr3.6177
De Luca, P., Scarpa, A., De Bonis, E., Cavaliere, M., Viola, P., Gioacchini, F. M, et al. (2021). Chloroquine and hydroxychloroquine ototoxicity; potential implications for SARS-CoV-2 treatment. A brief review of the literature. Am. J. Otolaryngol. 42, 102640. doi: 10.1016/j.amjoto.2020.102640
Deva, F. A. L, Gupta, A., Manhas, M., and Kalsotra, P. (2022). Neuro-otological Symptoms: An Atypical Aspect of COVID-19 Disease. Indian J. Otolaryngol. Head Neck Surg. 74, 3273–3282. doi: 10.1007/s12070-022-03088-z
Doweck, I., Yanir, Y., Najjar-Debbiny, R., Shibli, R., and Saliba, W. (2022). Sudden sensorineural hearing loss during the COVID-19 pandemic. JAMA Otolaryngol. Head Neck Surg. 148, 373–375. doi: 10.1001/jamaoto.2021.4105
Edmond, K., Chadha, S., Hunnicutt, C., Strobel, N., Manchaiah, V., Yoshinga-Itano, C., et al. (2022). Effectiveness of universal newborn hearing screening: a systematic review and meta-analysis. J. Glob. Health. 12, 12006. doi: 10.7189/jogh.12.12006
Edwards, M., Muzaffar, J., Naik, P., and Coulson, C. (2021). Catastrophic bilateral sudden sensorineural hearing loss following COVID-19. BMJ Case Rep. 14, e243157. doi: 10.1136/bcr-2021-243157
Elibol, E. (2021). Otolaryngological symptoms in COVID-19. Eur. Arch. Otorhinolaryngol. 278, 1233–1236. doi: 10.1007/s00405-020-06319-7
Fancello, V., Fancello, G., Hatzopoulos, S., Bianchini, C., Stomeo, F., Pelucchi, S., et al. (2022). Sensorineural hearing loss post-COVID-19 infection: an update. Audiol. Res. 12, 307–315. doi: 10.3390/audiolres12030032
Ficenec, S. C., Schieffelin, J. S., and Emmett, S. D. (2019). A review of hearing loss associated with Zika, Ebola, and Lassa Fever. Am. J. Trop. Med. Hyg. 101, 484–490. doi: 10.4269/ajtmh.18-0934
Formeister, E. J, Wu, M. J, Chari, D. A 3rd R. M, Rauch, S. D, and Remenschneider, A. K. (2022). Assessment of sudden sensorineural hearing loss after COVID-19 vaccination. JAMA Otolaryngol. Head Neck Surg. 148, 307–315. doi: 10.1001/jamaoto.2021.4414
Frazier, K. M, Hooper, J. E, Mostafa, H. H, and Stewart, C. M. (2020). SARS-CoV-2 virus isolated from the mastoid and middle ear: implications for COVID-19 precautions during ear surgery. JAMA Otolaryngol. Head Neck Surg. 146, 964–966. doi: 10.1001/jamaoto.2020.1922
Gallus, R., Melis, A., Rizzo, D., Piras, A., De Luca, L. M, Tramaloni, P., et al. (2021). Audiovestibular symptoms and sequelae in COVID-19 patients. J. Vestib. Res. 31, 381–387. doi: 10.3233/VES-201505
Gelardi, M., Iannuzzi, L., Trecca, E. M. C, Kim, B., Quaranta, N. A. A, and Cassano, M. (2020). COVID-19: what happened to all of the otolaryngology emergencies? Eur. Arch. Otorhinolaryngol. 277, 3231–3232. doi: 10.1007/s00405-020-06046-z
Gerstacker, K., Speck, I., Riemann, S., Aschendorff, A., Knopf, A., and Arndt, S. (2021). Deafness after COVID-19? HNO. 69, 92–95. doi: 10.1007/s00106-021-01041-0
Grandori, F. (1999). The european consensus development conference on neonatal hearing screening (Milan, May 15-16, 1998). Arch. Otolaryngol. Head Neck Surg. 125, 118. doi: 10.1001/archotol.125.1.118
Guigou, C., Schein, A.-D., Blanchard, C., and Folia, M. (2021). Sudden sensorineural hearing loss and SARS-CoV-2: donaeurot forget the standard work-up! Eur. Ann. Otorhinolaryngol. Head Neck Dis. 138, 219–220. doi: 10.1016/j.anorl.2021.02.010
Gunay, E., Kozan, G., Yuksel, E., Mizrakli, A., Aslan, O., Kavak, S., et al. (2021). A case of peritoneal dialysis in which SARS-CoV-2 was diagnosed by sudden hearing loss. Ren. Fail. 43, 325–326. doi: 10.1080/0886022X.2021.1882493
Gyo, K. (2013). Experimental study of transient cochlear ischemia as a cause of sudden deafness. World J. Otorhinolaryngol. 3, 1–15. doi: 10.5319/wjo.v3.i1.1
Hughes, G. B., Freedman, M. A., Haberkamp, and Guay, M. E. (1996). Sudden sensorineural hearing loss. Otolaryngol. Clin. North Am. 29, 393–405. doi: 10.1016/S0030-6665(20)30362-5
Jafari, Z., Kolb, B. E., and Mohajerani, M. H. (2022). Hearing loss, tinnitus, and dizziness in COVID-19: a systematic review and meta-analysis. Can. J. Neurol. Sci. 49, 184–195. doi: 10.1017/cjn.2021.63
Jeican, I. I., Aluaş, M., Lazăr, M., Barbu-Tudoran, L., Gheban, D., Inişca, P., et al. (2021). Evidence of SARS-CoV-2 virus in the middle ear of deceased COVID-19 patients. Diagnostics. 11, 1535. doi: 10.3390/diagnostics11091535
Jenks, C. M., DeSell, M., and Walsh, J. (2022). Delays in infant hearing detection and intervention during the COVID-19 pandemic: commentary. Otolaryngol. Head Neck Surg. 166, 603–604. doi: 10.1177/01945998211067728
Jeong, M., Ocwieja, K. E, Han, D., Wackym, P. A, Zhang, Y., Brown, A., et al. (2021). Direct SARS-CoV-2 infection of the human inner ear may underlie COVID-19-associated audiovestibular dysfunction. Commun. Med. 1, 44. doi: 10.1038/s43856-021-00044-w
Kilic, O., Kalcioglu, M. T., Cag, Y., Tuysuz, O., Pektas, E., Caskurlu, H., and Cetin, F. (2020). Could sudden sensorineural hearing loss be the sole manifestation of COVID-19? An investigation into SARS-CoV-2 in the etiology of sudden sensorineural hearing loss. Int. J. Infect. Dis. 97, 208–211. doi: 10.1016/j.ijid.2020.06.023
Kurabi, A., Pak, K., DeConde, A. S, Ryan, A. F, and Yan, C. H. (2022). Immunohistochemical and qPCR detection of SARS-CoV-2 in the human middle ear versus the nasal cavity: case series. Head Neck Pathol. 16, 607–611. doi: 10.1007/s12105-021-01378-6
Liaw, J., Saadi, R., Patel, V. A, and Isildak, H. (2021). Middle ear viral load considerations in the COVID-19 era: a systematic review. Otol. Neurotol. 42, 217–226. doi: 10.1097/MAO.0000000000002986
Lieu, J. E. C., Kenna, M., Anne, S., and Davidson, L. (2020). Hearing loss in children: a review. JAMA. 324, 2195–2205. doi: 10.1001/jama.2020.17647
Little, C., and Cosetti, M. K. (2021). A narrative review of pharmacologic treatments for COVID-19: safety considerations and ototoxicity. Laryngoscope. 131, 1626–1632. doi: 10.1002/lary.29424
Magee, M., Lewis, C., Noffs, G., Reece, H., Chan, J. C. S, Zaga, C. J, et al. (2020). Effects of face masks on acoustic analysis and speech perception: Implications for peri-pandemic protocols. J. Acoust. Soc. Am. 148, 3562. doi: 10.1121/10.0002873
Maleki, M., Maarefvand, M., Nazeri, A. R, Baghban, A. R. A, and Borna, A. (2022). Audio-vestibular profile of COVID-19; systematic review and meta-analysis. Iran J. Otorhinolaryngol. 34, 145–155.
Malesci, R., Rizzo, D., Vecchio, V. D, Serra, N., Tarallo, G., D'Errico, D., et al. (2022). The absence of permanent sensorineural hearing loss in a cohort of children with SARS-CoV-2 infection and the importance of performing the audiological “work-up”. Children. 9, 1681. doi: 10.3390/children9111681
Marom, T., Pitaro, J., Shah, U. K, Torretta, S., Marchisio, P., Kumar, A. T, et al. (2021). Otitis media practice during the COVID-19 pandemic. Front. Cell Infect. Microbiol. 11, 749911. doi: 10.3389/fcimb.2021.749911
Meng, X., Wang, J., Sun, J., and Zhu, K. (2022a). COVID-19 and sudden sensorineural hearing loss: a systematic review. Front. Neurol. 13, 883749. doi: 10.3389/fneur.2022.883749
Meng, X., Zhu, K., Wang, J., and Liu, P. (2022b). Can SARS-CoV-2 positive pregnant women affect the hearing of their newborns: a systematic review. Am. J. Otolaryngol. 43, 103523. doi: 10.1016/j.amjoto.2022.103523
Mom, T., Chazal, J., Gabrillargues, J., Gilain, L., and Avan, L. (2005). Cochlear blood supply: an update on anatomy and function. Fr ORL. 88, 81–88.
Monteiro, E. M. R, Nascimento, M. F. L, Brito, T. R. C, Lima, M. C, Sefair, L. R, and Pedrosa, M. M. (2020). Chloroquine and COVID-19: should we care about ototoxicity? Int. Arch. Otorhinolaryngol. 24, e359–e363. doi: 10.1055/s-0040-1714142
Nelson, H. D, Bougatsos, C., Nygren, P., and 2001 US Preventive Services Task Force. (2008). Universal newborn hearing screening: systematic review to update the 2001 US preventive services task force recommendation. Pediatrics. 122, e266–e276. doi: 10.1542/peds.2007-1422
Okhovat, S., Fox, R., Magill, J., and Narula, A. (2015). Sudden onset unilateral sensorineural hearing loss after rabies vaccination. BMJ Case Rep. doi: 10.1136/bcr-2015-211977
Ong, K. M. C., and Cruz, T. L. G. (2022). Otologic and vestibular symptoms in COVID-19: a scoping review. World J. Otorhinolaryngol. Head Neck. Surg. 8, 287–96. doi: 10.1002/wjo2.57
Ozer, F., and Alkan, O. (2021). Simultaneous sudden hearing loss and peripheral facial paralysis in a patient with COVID-19. Ear Nose Throat J. 2021, 1455613211028094. doi: 10.1177/01455613211028094
Pandian, V., Brodsky, M. B, Brigham, E. P, Parker, A. M, Hillel, A. T, Levy, J. M, et al. (2021). COVID-19 survivorship: how otolaryngologist-head and neck surgeons can restore quality of life after critical illness. Am. J. Otolaryngol. 42, 102917. doi: 10.1016/j.amjoto.2021.102917
Parrino, D., Frosolini, A., Toninato, D., Matarazzo, A., Marioni, G., and de Filippis, C. (2022). Sudden hearing loss and vestibular disorders during and before COVID-19 pandemic: an audiology tertiary referral centre experience. Am. J. Otolaryngol. 43, 103241. doi: 10.1016/j.amjoto.2021.103241
Pereira, M. C. P, Fernandes, J. C. H, Fernandes, G. V. O, Nor, F., Marques, T., and Couto, P. (2023). Impact of the COVID-19 pandemic period on patients with head and neck carcinoma: a systematic review. Diseases. 11, 61. doi: 10.3390/diseases11020061
Perret, M., Bernard, A., Rahmani, A., Manckoundia, P., and Putot, A. (2021). Acute labyrinthitis revealing COVID-19. Diagnostics. 11, 482. doi: 10.3390/diagnostics11030482
Pisani, D., Gioacchini, F. M, Viola, P., Scarpa, A., Astorina, A., Re, M., et al. (2022). Audiovestibular disorders after COVID-19 vaccine: is there an association? Audiol. Res. 12, 212–223. doi: 10.3390/audiolres12030024
Pontillo, V., Iannuzzi, L., Petrone, P., Sciancalepore, P. I., D'Auria, C., Rinaldi, M., et al. (2020). ENT surgical emergencies during the COVID-19 outbreak. Acta Otorhinolaryngol. Ital. 40, 399–404. doi: 10.14639/0392-100X-N1036
Pool, C., King, T. S, Pradhan, S., and Isildak, H. (2022). Sudden sensorineural hearing loss and coronavirus disease 2019. J. Laryngol. Otol. 136, 823–826. doi: 10.1017/S0022215122000068
Prayuenyong, P., Kasbekar, A. V., and Baguley, D. M. (2020). Clinical implications of chloroquine and hydroxychloroquine ototoxicity for COVID-19 treatment: a mini-review. Front. Public Health. 8, 252. doi: 10.3389/fpubh.2020.00252
Raad, N., Ghorbani, J., Mikaniki, N., Haseli, S., and Karimi-Galougahi, M. (2021). Otitis media in coronavirus disease 2019: a case series. J. Laryngol. Otol. 135, 10–13. doi: 10.1017/S0022215120002741
Rahne, T., Fröhlich, L., Plontke, S., and Wagner, L. (2021). Influence of surgical and N95 face masks on speech perception and listening effort in noise. PLoS ONE. 16, e0253874. doi: 10.1371/journal.pone.0253874
Riemann, S., Speck, I., Gerstacker, K., Becker, C., and Knopf, A. (2021). Collateral damage of the COVID-19 pandemic: an alarming decline in critical procedures in otorhinolaryngology in a German university hospital. Eur. Arch. Otorhinolaryngol. 278, 3417–3423. doi: 10.1007/s00405-020-06519-1
Salt, A. N., and Plontke, S. K. (2009). Principles of local drug delivery to the inner ear. Audiol. Neurootol. 14, 350–360. doi: 10.1159/000241892
Saunders, G. H, Beukes, E., Uus, K., Armitage, C. J, Kelly, J., and Munro, K. J. (2022). Shedding light on SARS-CoV-2, COVID-19, COVID-19 vaccination, and auditory symptoms: causality or spurious conjunction? Front. Public Health. 10, 837513. doi: 10.3389/fpubh.2022.837513
Savtale, S., Hippargekar, P., Bhise, S., and Kothule, S. (2022). Prevalence of otorhinolaryngological symptoms in COVID 19 patients. Indian J. Otolaryngol. Head Neck Surg. 74, 3378–3384. doi: 10.1007/s12070-021-02410-5
Seol, H. Y, Jo, M., Yun, H., Park, J. G, Byun, H. M, and Moon, I. J. (2023). Comparison of speech recognition performance with and without a face mask between a basic and a premium hearing aid in hearing-impaired listeners. Am. J. Otolaryngol. 44, 103929. doi: 10.1016/j.amjoto.2023.103929
Sevilla-Montoya, R., Hidalgo-Bravo, A., Estrada-Gutiérrez, G., Villavicencio-Carrisoza, O., Leon-Juarez, M., Villegas-Mota, I., et al. (2021). Evidence of possible SARS-CoV-2 vertical transmission according to World Health Organization criteria in asymptomatic pregnant women. Ultrasound Obstet. Gynecol. 58, 900–908. doi: 10.1002/uog.24787
Shimray, S. R. (2022). Research done wrong: a comprehensive investigation of retracted publications in COVID-19. Account Res. 2022, 1–14. doi: 10.1080/08989621.2021.2014327
Singh, B., Ryan, H., Kredo, T., Chaplin, M., and Fletcher, T. (2021). Chloroquine or hydroxychloroquine for prevention and treatment of COVID-19. Cochrane Database Syst. Rev. 2, CD013587. doi: 10.1002/14651858.CD013587.pub2
Sriwijitalai, W., and Wiwanitkit, V. (2020). Hearing loss and COVID-19: a note. Am. J. Otolaryngol. 41, 102473. doi: 10.1016/j.amjoto.2020.102473
Tabuchi, K., Tsuji, S., Fujihira, K., Oikawa, K., Hara, A., and Kusakari, J. (2002). Outer hair cells functionally and structurally deteriorate during reperfusion. Hear Res. 173, 153–163. doi: 10.1016/S0378-5955(02)00349-0
Toscano, J. C., and Toscano, C. M. (2021). Effects of face masks on speech recognition in multi-talker babble noise. PLoS ONE. 16, e0246842. doi: 10.1371/journal.pone.0246842
Trott, M., Driscoll, R., and Pardhan, S. (2022). The prevalence of sensory changes in post-COVID syndrome: a systematic review and meta-analysis. Front. Med. 9, 980253. doi: 10.3389/fmed.2022.980253
Ulrich, A. K., Sundaram, M. E., and Osterholm, M. T. (2022). Rare sudden sensorineural hearing loss potentially associated with COVID-19 vaccination does not outweigh the benefit of COVID-19 vaccines. JAMA Otolaryngol. Head Neck Surg. 148, 315–316. doi: 10.1001/jamaoto.2021.4279
van Rijssen, L. B, Derks, W., Hoffmans, R., van Looij, M. A, van Maanen, J. P, van Monsjou, H. S, et al. (2022). No COVID-19 in patients with sudden sensorineural hearing loss (SSNHL). Otol. Neurotol. 43, 170–173. doi: 10.1097/MAO.0000000000003438
Vielsmeier, V., Marcrum, S. C, Weber, F. C, Langguth, B., and Hintschich, C. (2022). Audiological effects of COVID-19 infection: results of a standardized interview. Can. J. Neurol. Sci. 49, 623–624. doi: 10.1017/cjn.2021.179
Vigil-Vázquez, S., Carrasco-García, I., Hernanz-Lobo, A., Manzanares, Á., Pérez-Pérez, A., Toledano-Revenga, J., et al. (2022). Impact of gestational COVID-19 on neonatal outcomes: is vertical infection possible? Pediatr. Infect Dis. J. 41, 466–472. doi: 10.1097/INF.0000000000003518
Wagatsuma, Y., Daimaru, K., Deng, S., Chen, J. Y., et al. (2022). Hearing loss and the COVID-19 pandemic. BMC Res. Notes. 15, 228. doi: 10.1186/s13104-022-06120-1
Wan, D., Du, T., Hong, W., Chen, L., Que, H., Lu, S., et al. (2021). Neurological complications and infection mechanism of SARS-CoV-2. Signal Transduct. Target Ther. 6, 406. doi: 10.1038/s41392-021-00818-7
WHO (2019). WHO fact sheets-Deafness and hearing loss. Available online at: http://www.who.int/mediacentre/factsheets/fs300/en/ (accessed March 20, 2019).
WHO (2023). Weekly epidemiological update on COVID-19. Available online at: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19-−1-june-2023 (accessed June 1, 2023).
Wichova, H., Miller, M. E., and Derebery, M. J. (2021). Otologic manifestations after COVID-19 vaccination: the house ear clinic experience. Otol. Neurotol. 42, e1213–e1218. doi: 10.1097/MAO.0000000000003275
Keywords: COVID, COVID-19, SARS-CoV-2, hearing loss, sudden sensorineural hearing loss (SSNHL), ototoxicity, inner ear, pandemic
Citation: Feng SJ, Voruz F, Yu M and Lalwani AK (2023) COVID-19 and hearing loss—A narrative review. Front. Audiol. Otol. 1:1233793. doi: 10.3389/fauot.2023.1233793
Received: 02 June 2023; Accepted: 27 July 2023;
Published: 11 August 2023.
Edited by:
Katrin Reimann, University Hospital Giessen and Marburg, GermanyReviewed by:
Iva Speck, University of Freiburg, GermanyKruthika Thangavelu, University Medical Center Giessen, Germany
Copyright © 2023 Feng, Voruz, Yu and Lalwani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anil K. Lalwani, YWtsMjE0NEBjdW1jLmNvbHVtYmlhLmVkdQ==
†These authors share first authorship