 Silvia González Santos1*
Silvia González Santos1* Laura Martí Gelonch2
Laura Martí Gelonch2 Nuria González Jorrín1Mireia González Osinalde3Núria Rosell Romero3
Nuria González Jorrín1Mireia González Osinalde3Núria Rosell Romero3
- 1Department of Anesthesiology, Postoperative Care and Pain Management, Donostia University Hospital, San Sebastián, Spain
- 2Department of General Surgery, Donostia University Hospital, San Sebastián, Spain
- 3Department of Physical Medicine and Rehabilitation, Donostia University Hospital, San Sebastián, Spain
Esophagectomy remains being a surgical procedure with a high morbidity and mortality rate. Therefore, prehabilitation, defined as the group of interventions performed on the patient in the preoperative period to improve their functional capacity and clinical condition, becomes highly important to ensure that the patient faces the stress that surgery entails under the best possible clinical situation. Hereby, we describe our prehabilitation protocol that has been implementedsince 2017 and we present the clinical results achieved so far. Preoperative risk assessment and various modalities of prehabilitation protocols are discussed to enhance the patient´s preoperative physiological condition and to reduce the impact of the neuroendocrine and inflammatory response induced by an esophagectomy. Finally, we describe the protocol we intend to implement to improve our clinical practice and reduce complications.
1 Introduction
Esophageal cancer ranks as the eighth most common neoplasm and the sixth leading cause of death due to cancer worldwide, with about 604,127 new cases per year and approximately 544,000 deaths (1). Due to its natural history, esophageal cancer is often diagnosed in advanced stages, leading to high mortality, with a 5-year overall survival (OS) rate of 20%. The estimated average survival after 5 years in localized tumors is 45%, 24% in tumors with lymph node involvement, and 5% in disseminated tumors (1). The two most common histological types worldwide are squamous cell carcinoma and adenocarcinoma. Despite being a disease with a poor prognosis, improvements have been made in the management of esophageal cancer in recent decades. The cornerstone of curative treatment is surgical resection with lymphadenectomy, sometimes combined with neoadjuvant treatment with chemotherapy (CT) or chemoradiotherapy (CRT) with the intention of improving oncological outcomes (2). The choice of the most appropriate surgical technique should be individualized and it is mainly determined by the location of the tumor (3–5). In recent years, the development of minimally invasive surgery has succeeded in reducing complications related to laparotomy and thoracotomy, hospital stay, and respiratory complications, while presenting comparable oncological outcomes and similar rates of anastomotic leak or number of resected lymph nodes (6–9).
The preoperative risk assessment becomes of great importance (modifiable and non-modifiable risks), evaluating comorbidities of the patient, as well as cardiopulmonary function, functional capacity, and nutritional status in order to optimize all possible aspects to ensure that the patient undergoes surgery in the best possible clinical condition, thereby improving outcomes (10, 11). Enhanced recovery after surgery protocols (ERAS programs) aim to improve postoperative outcomes by accelerating the patient's recovery and reducing hospital stay and the associated costs (12). While intra- and postoperative measures have been maximized in these protocols, the preoperative period has been the most neglected one.
Prehabilitation, defined as the combination of interventions performed on the patient in the preoperative period, aims to accompany and prepare patients to face surgery under the best possible clinical conditions (13, 14). Initially based on a three-pillar conception: improvement of the patient's physical condition, nutritional optimization and cognitive intervention to reduce stress and anxiety; it has evolved into a multimodal strategy including smoking cessation, correction of anemia and pharmacological adjustment (15–17). It is worth noting that we are increasingly operating on older patients with a higher rate of associated comorbidities, meeting “frailty” criteria, and with diminished physiological and functional capacity. In these patients, the implementation of different measures from the ERAS program brings benefits, but we need better preoperative optimization of their baseline state, by improving their functional status (physical, nutritional, and psychological capacity), as it is one of the modifiable factors related to poor postoperative outcomes (18). It can be stated that patients who most clearly benefit from these programs are those at high risk (ASA III and IV), as well as those with preoperative studies showing a deteriorated functional status (19).
Regarding prehabilitation, particularly in patients undergoing esophagogastric surgery, the evidence seems to confirm its beneficial effects despite the heterogeneous design of the studies (20).
The main objective of this article is to present our preoperative management protocol for patients undergoing these surgeries and the results obtained with it from January 2017 to November 2023, and, furthermore, to compare it with the results published in the literature.
We also aim to perform a review of the existing evidence regarding specific prehabilitation programs for esophagectomies (within the context of ERAS programs) and their relationship with improving the patients’ functional status and their postoperative outcomes. Additionally, it aims to describe and convey the most important components within these programs.
In addition, we want to present the new prehabilitation protocol of our center, incorporating new measures not previously implemented and aiming to compare, in the future, the results obtained in patients undergoing it with those who underwent surgery before implementing the new protocol, in order to determine if postoperative complications (especially respiratory ones) and mortality are reduced by implementing a more comprehensive (multimodal) prehabilitation approach.
2 Material and methods
A descriptive, retrospective and single-center study has been designed. This study has been reviewed and approved by the Ethics Committee for Scientific Research of the Donostia University Hospital. Our center is a third-level hospital, serving as the provincial reference center for esophageal surgery. Since January 2017 until November 2023, patients undergoing neoadjuvant CRT prior to an esophagectomy participate in the prehabilitation program designed for this purpose.
Variables such as demographic data, associated comorbidities, toxic habits, clinical data at the time of the diagnosis of the desease, analytical and endoscopic data, imaging tests, anatomopathological data, clinical staging, treatment received, treatment-associated complications, surgical aspects, post-intervention complications, definitive anatomopathological results, and survival data were collected.
To review the existing literature related to the topic, a research in Medline, PubMed, Embase, Cinahl, and Cochrane was carried out, including the references that we considered more relevant.
In Tables 1, 2 we show the most relevant publications.
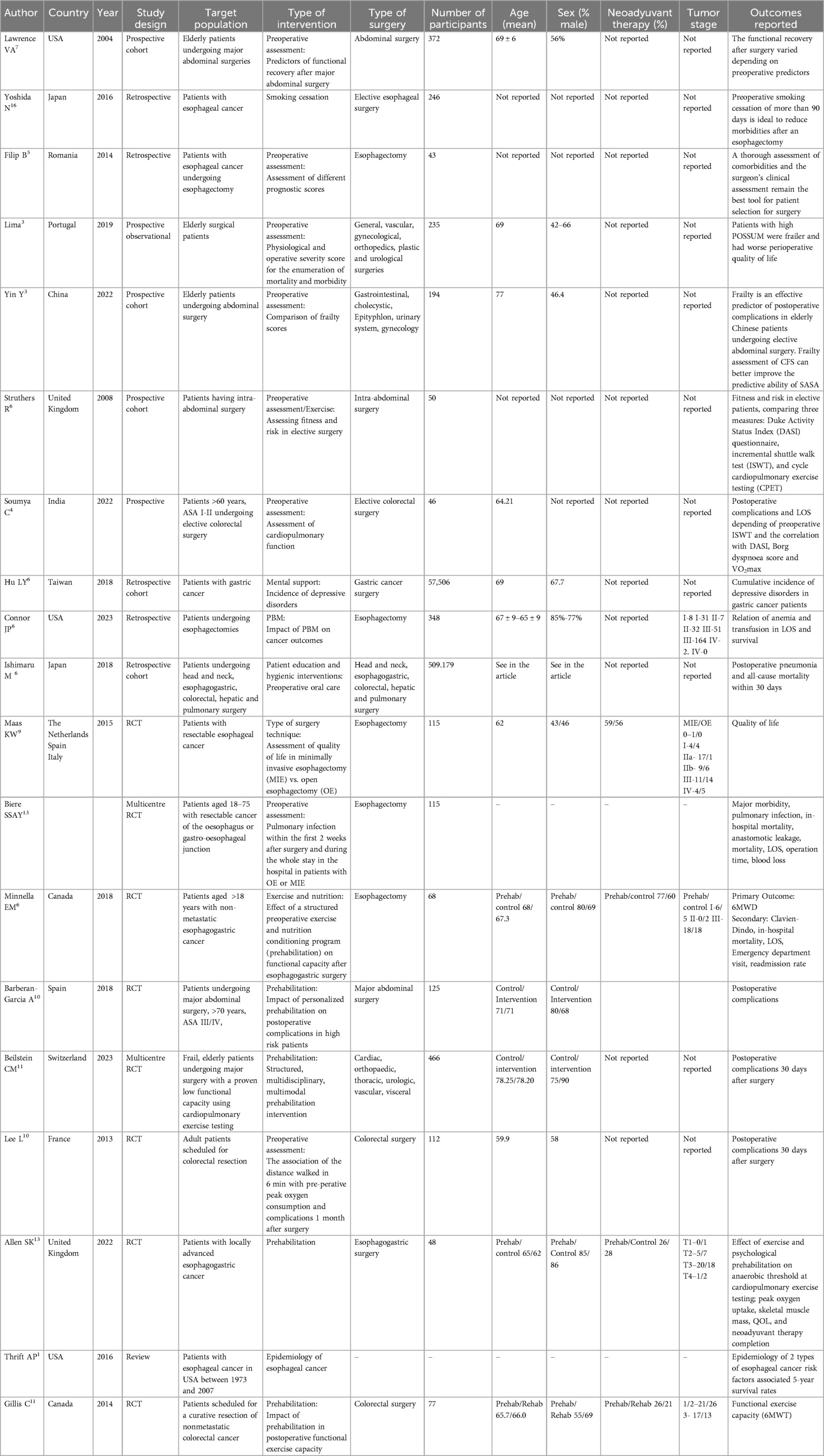
Table 1. Included studies.
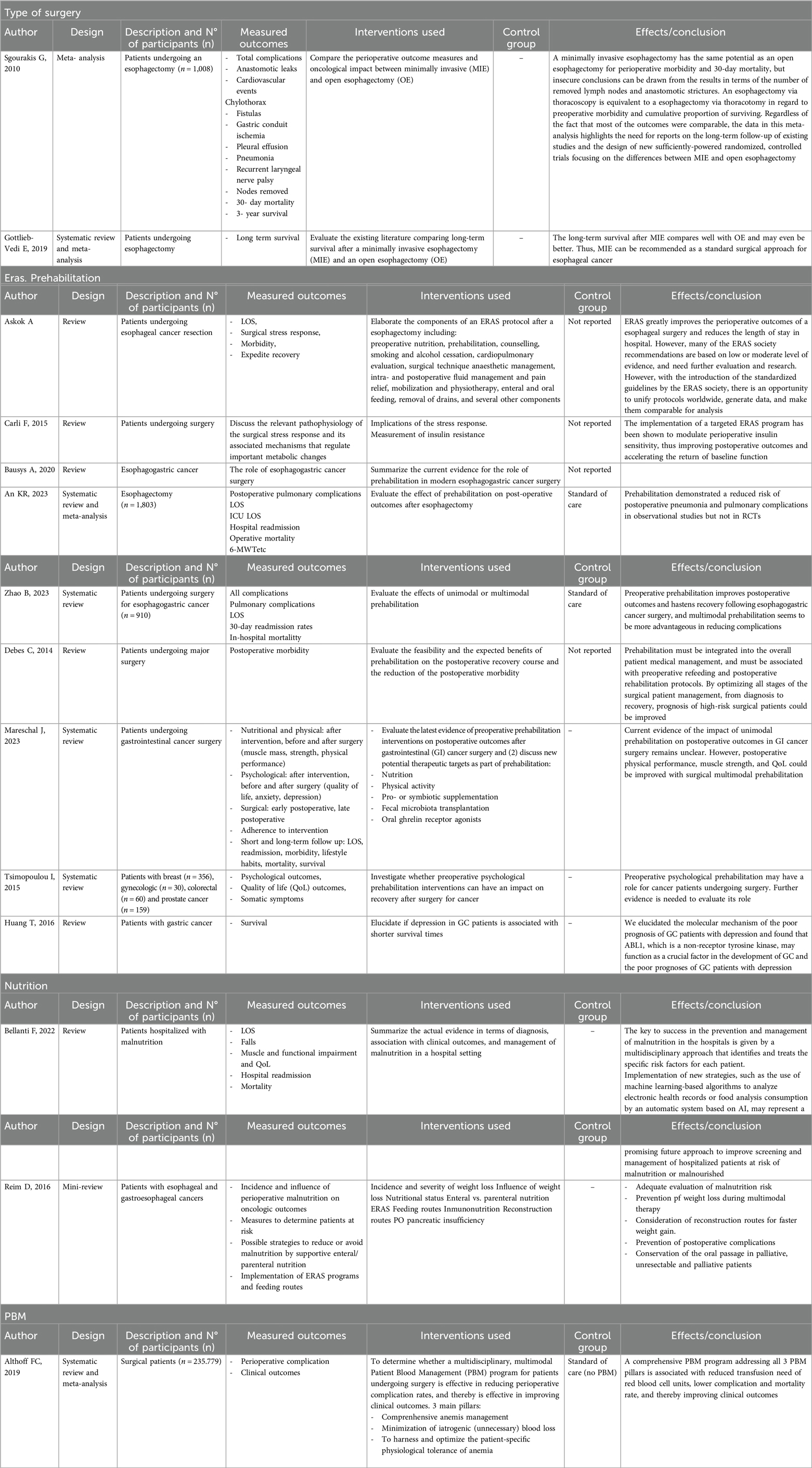
Table 2. Reviews and meta-analysis.
3 Statistical analysis
This is a descriptive analysis where quantitative variables are expressed as mean (minimum and maximum), and categorical variables are expressed as absolute frequencies and relative percentages.
4 Results
Below, we present the preoperative protocol that we applied to patients undergoing esophagectomies between January 2017 and November 2023:
After completing the preoperative study, patients were evaluated in the multidisciplinary tumor committee of the esophagogastric area, where the optimal therapeutic modality was decided based on tumor staging, location, and associated comorbidities. The therapeutic algorithm of our center is attached (21) (Figure 1).
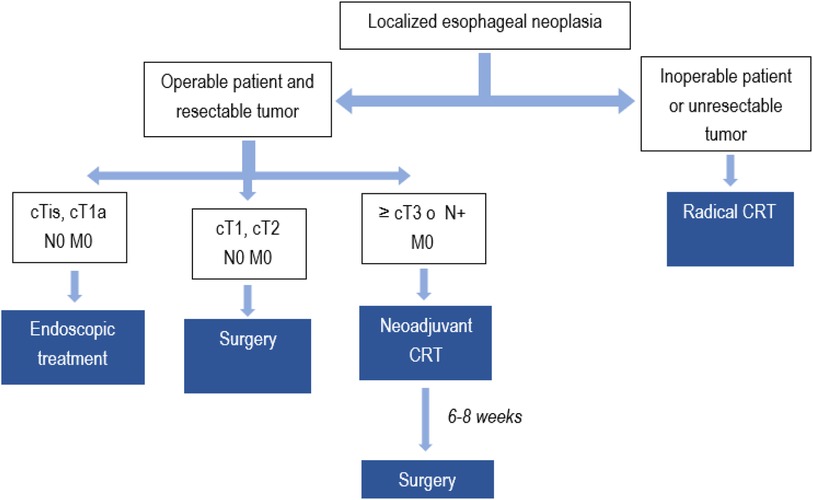
Figure 1. Therapeutic management of patients with esophageal cancer at the Donostia University Hospital. Scheme based on the therapeutic management of esophageal cancer at the Donostia University Hospital.
Patients were considered operable or non-operable based on age and comorbidities. Tumors were considered unresectable if they were staged cT4b or located in the cervical or upper high thoracic region. In all patients eligible for a radical treatment, an initial assessment of nutritional and physical status was conducted. Nutritional status was analyzed using the MUST tool and if there was a risk of malnutrition, a Patient-Generated Subjective Global Assessment (PG-SGA) test was performed. Functional capacity was not assessed. Based on the result of this latter test, corresponding nutritional recommendations were provided as depicted in Figure 2. Following the completion of neoadjuvant CRT, patients eligible for surgery were referred to the Rehabilitation Service to improve their physical condition before the intervention. For this purpose, patients attended 1-h hospital supervised sessions three times per week until the day of the surgery (approximately for 6–8 weeks), during which the following exercises were performed:
• Aerobic exercise (cycling or treadmill, 20–30 min, Borg 11–13).
• Strength training (10–12 repetitions of quadriceps, biceps, latissimus dorsi, Borg 11–13).
• Inspiratory muscle training starting at 30% of MIP (maximum inspiratory pressure), 10–12 repetitions twice a day, progressing 10% every 2 weeks until reaching 50%–60% of MIP).
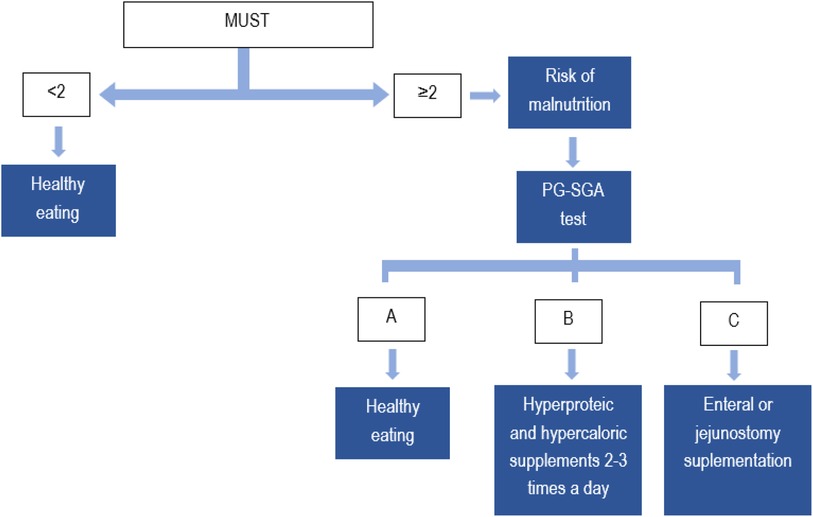
Figure 2. Assessment of nutritional Status in patients with esophageal cancer eligible for curative intent treatment at Donostia University Hospital.
After reviewing the patients during this period, these was the data obtained:
Since the implementation of this protocol in January 2017 until now, 46 patients have undergone neoadjuvant CRT and surgery. The mean age was of 63.7 years (ranging from 46 to 76 years), 37 (80.4%) of them being male patients and 9 (19.5%) female. According to the protocol, patients underwent surgery 6–8 weeks after completing the treatment, during which they were referred to the Rehabilitation Service. They were all patients that had completed the physical training program and had undergone nutritional assessment. Demographic data are collected in Table 3.
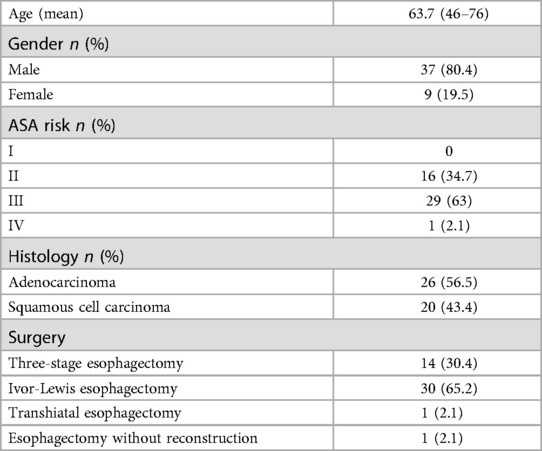
Table 3. Demographic data.
13 patients (28.2%) did not experience any complications, 23 (50%) had complications classified as Clavien-Dindo I or II (minor), and 11 (23.9%) had Clavien-Dindo III or IV (major) complications. Postoperative mortality was 8.7% at 30 days. The postoperative results are collected in Table 4.
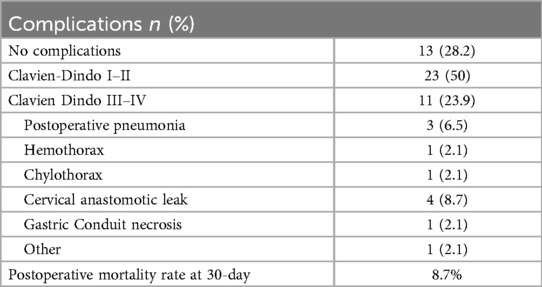
Table 4. Postoperative results.
5 Prehabilitation measures
A review of the current evidence on prehabilitation in esophageal cancer has been conducted, aiming to identify measures of particular interest and have an impact on outcomes, thus enabling future protocols to be tailored and evidence to be published. These measures are described below:
5.1 Proper preoperative assessment and pharmacological adjustment
Carrying out a proper preoperative assessment is extremely important due to the high obesity rate, respiratory and cardiovascular pathologies, and the increasing age of the patients. Approximately 30% of surgery candidates are ASA III or IV. There is not a complete consensus on this matter yet, and predicting which patients will develop complications is not an easy task (22). However, risk factors that increase morbidity and mortality after an esophagectomy have been established: poor cardiopulmonary reserve, advanced age, tumor stage, diabetes mellitus, liver dysfunction and overall a poor clinical condition (11).
There is no consensus either regarding the mortality scale to be used in the assessment of these patients. Some of the scales described in the literature are the POSSUM and the P-POSSUM, which seem to be directly related to worse perioperative quality of life in patients with high scores (23). One of the most commonly used is the American Society of Anesthesiologists (ASA) scale, which relates the anesthesia risk to the patient's various comorbidities, not the anesthesia risk itself (24). This scale on its own does not predict perioperative risks. Associated with other factors, such as the type of surgery and frailty, it can be more accurate in determining perioperative risks. The Clinical Frailty Scale (CFS) has been shown to be reliable predicting complications in patients undergoing major abdominal surgery (25).
Several tools have been described for determining the patient's functional capacity, such as the Duke Activity Status Index (DASI), the Shuttle Walk Test (SWT), and the Cardiopulmonary Exercise Testing (CPET) (26, 27).
In a review of different tools to identify patients at risk of malnutrition, the Malnutrition Universal Screening Tool (MUST) was found to be the most sensitive, specific, and accurate identifying malnourished patients (28).
The adjustment of the patient's pharmacological treatment for surgery should be done since the pre-anesthesia consultation.
5.2 Preoperative anemia
Anemia in cancer patients is quite common. The causes are varied: losses caused by the tumor itself, anemia due to chronic illnesses, marrow suppression induced by chemotherapy and radiotherapy, deficiencies due to nutritional deficiencies, or acute losses during surgery, among others. Additionally, both anemia and transfusions have been established as independent risk factors for increased mortality in esophageal cancer patients. Therefore, diagnosing it becomes essential to establish a treatment targeted at the cause to correct it before surgery, thus minimizing the number of transfusions (29, 30). Patient Blood Management (PBM) programs are evidence-based guidelines, implemented in hospitals progressively, aiming to detect anemia in the preoperative period to treat it in time before surgery, thereby minimizing the use of blood products in the perioperative period (intravenous iron, erythropoietin). They also promote other measures with the same objective, such as reducing intraoperative bleeding with the use of antifibrinolytic drugs like tranexamic acid and employing more restrictive transfusion thresholds (Hb 7 g/dl) (30, 31).
5.3 Exercise training
Exercise has beneficial effects on individual health, including those patients with cancer. Physical activity improves patients’ functional capacity, reduces cancer-related fatigue, and enhances quality of life (32, 33). The postoperative period is associated with a decrease of 20%–40% in functional capacity. Traditionally, the postoperative period has been used for the recovery of this functional capacity (rehabilitation). However, it has been demonstrated that this is not the ideal time to do so, due to the clinical and personal situation experienced by the patient after surgery. The preoperative period is the optimal time to intervene and improve the patient's physical and functional capacity (prehabilitation) (19), as demonstrated by Gillis et al. in a clinical trial with patients undergoing colorectal surgery. They showed a significant increase in functional capacity measured with the 6MWT in patients undergoing a prehabilitation program between 3 and 4 weeks before surgery, within the context of an enhanced recovery program (34). Previously, a low preoperative 6MWT had been associated with an increased risk of respiratory complications in patients (35). Therefore, exercise is one of the pillars of prehabilitation programs.
Nevertheless, there is no agreement on which exercise regimen is best, resulting in a wide variety of interventions. These programs should include at least 4 weeks of a combination of aerobic training, resistance training, and inspiratory muscle training to ensure endurance. The frequency, intensity, and duration of each exercise should differ depending on each patient's initial fitness and their health status and should be managed by skilled individuals. Unsupervised or tele-exercise with remote supervision exercises may also be possible in selected patients. Exercise and physical activity programs should also include the promotion of daily physical activity, reducing sitting or sedentary time, and promoting long-term behavior changes to embrace a more active lifestyle.
5.4 Nutritional status
There is evidence that malnutrition is an independent predictor of poor postoperative outcomes (36). This is particularly important considering that the prevalence of malnutrition in patients with this type of cancer can reach up to 80% (37, 38).
Therefore, detecting patients at risk of malnutrition is a fundamental task during the preoperative period, establishing the specific situation of each patient to initiate an individualized nutritional treatment (15, 39, 40).
In those with a MUST ≥2, a nutritional treatment should be initiated to improve their state before surgery and maintain it throughout the perioperative period. Evidence supports starting treatments at least 2 weeks before surgery (41). Depending on the severity of the patients’ malnutrition, patients will receive counseling from a nutritionist, who will assess the appropriate treatment for the patient, instructing them on nutrition and healthy habits. Diet enrichment, either with natural ingredients or with hyperproteic and caloric supplements, is recommended. Micronutrient intake will be recommended in particular cases (42). According to the ESPEN guidelines, supplements should provide at least 400 Kcal with ≥30 g of protein per day (43). Enteral and parenteral nutrition will be considered in cases where oral intake is not possible (28).
Regarding new nutritional therapies, the evidence is limited at the moment. The benefits of probiotic and symbiotic interventions in patients with gastrointestinal cancer are controversial. There is a phase II study investigating the possible beneficial action of fecal microbiota transplantation from obese patients to cachectic patients with esophagogastric cancer (44).
5.5 Mental support
We must not forget the psychological effect that a cancer diagnosis has on patients. Although there is not much evidence, partly due to the limited availability of these resources in hospitals, it does seem that therapies aimed at reducing stress and anxiety in the preoperative period would have a beneficial effect on the patient (45, 46). Depression and anxiety generated by the process can influence a lower treatment compliance, thereby worsening the prognosis, and it also seems to favor a disease progression (47–49). There is not much evidence regarding the type of psychological treatment to employ (45).
5.6 Patient educational and hygienic interventions
5.6.1 Smoking cessation
Smoking has also been linked to a higher rate of postoperative complications and increased costs. It has been established that a reduction of respiratory complications is noticeable after 4 weeks. The responsible physician should advise the patient and provide all available therapeutic tools to facilitate smoking cessation before surgery (50).
5.6.2 Alcohol consumption
Harmful alcohol consumption is associated with increased postoperative complications, such as increased bleeding, infections, pulmonary complications, interference with anesthetic drugs, and delayed recovery, leading to increased admissions to critical care units and hospital stays.
In a review of RCTs evaluating the effects of preoperative alcohol cessation on postoperative complications, the primary objectives were postoperative complications and 30-day mortality. Secondary objectives included the length of the hospital stay and alcohol use in the postoperative period.
A significant reduction in the rate of postoperative complications was observed, but not in the 30-day mortality rate or the length of stay (51).
The ideal therapy to implement for alcohol abuse cessation (counselling sessions and/or pharmacologic therapies) and the optimal cessation period before surgery is yet to be determined. Cessation between 6 and 8 weeks before surgery is recommended, but it appears that cessation of 2–4 weeks could already be associated with a decrease in the risk of postoperative complications.
5.6.3 Other drugs
Patients with drug abuse disorders such as opioids, benzodiazepines, etc., are at higher risk of postoperative complications such as delirium, pneumonia, respiratory failure, mechanical ventilation, prolonged hospital stays, and difficult postoperative pain control.
Ideally, the patient should be provided with a personalized perioperative plan, if possible, combined with an addiction specialist and a pain management expert. It would be necessary to establish an evidence-based protocol to ensure adequate pain control while avoiding the development of withdrawal symptoms. More studies are required (52, 53).
5.6.4 Dental care
Improving the patients’ dental hygiene could reduce the cases of postoperative pneumonia that may arise from the aspiration of oropharyngeal secretions. Ishimaru et al. conducted a retrospective cohort study to evaluate the relationship between preoperative oral care and postoperative complications in patients undergoing major oncological surgery. Between May 2012 and December 2015, they studied patients undergoing head and neck, esophagogastric, colorectal, hepatic, and pulmonary surgery. The primary objectives were postoperative pneumonia and 30-day mortality. Of a total of 509 patients, 179, only 16%, received oral treatments from a dentist. They concluded that preoperative oral care by a dentist significantly reduced the incidence of pneumonia and 30-day mortality (54).
In any case, we must provide personalized attention and try to provide an individualized program for each of our patients (10).
6 Discussion
Firstly, we have compared our results with our current prehabilitation protocol to those published in the literature.
Regarding our series, the most common histological types include squamous cell carcinoma and adenocarcinoma. The mean age at diagnosis in our population has been 63.7 years, which is 5 years lower than the national average (55). The prevalence, as reflected in the literature, has been higher in males for both histological types (56). As recommended by the The National Comprehensive Cancer Network (NCCN) guidelines, optimal treatment should be based on accurate disease staging, tumor location and histology, and therapeutic approach should be discussed by a multidisciplinary team (57). In our center, the creation of the Multidisciplinary Committee for Gastroesophageal Tumors took place in 2005, it consisted of pathologists, medical oncologists, radiation oncologists, surgeons, radiologists, and nursing staff, discussing all the cases of esophageal cancer individually. Surgery-related complications, in addition to increasing the average length of hospital stay, costs, and resource utilization; have a negative impact on postoperative survival and quality of life (58). They act as independent prognostic factors after an esophageal resection, with 5-year survival rates and disease-specific survival rates lower than those of patients who do not present them (59). The most common complications after resective esophageal surgery are pneumonia, atrial fibrillation, and anastomotic leakage, occurring in 14.6%, 14.5%, and 11.4%, respectively, according to the Esophageal Complications Consensus Group (ECCG) benchmark (60). Respiratory complications are the most common major complications, resulting from the impact of surgery on the thoracic wall, diaphragm, and abdominal wall, and are responsible for 50%–65% of surgery-related mortality. In our series, the rate of postoperative pneumonia was 6.5% lower than the one reported by the ECCG, with rates of 14.6%. The rate of anastomotic leakage after a neoadjuvant therapy reached 10.8%, also lower than reported while the 30-day mortality rate was 8.7%, similar to the reported rates in the literature ranging from 6% to 8.9% at 30 days and 13.3–15.8% at 90 days (61, 62).
Therefore, although we have observed lower morbidity rates in our series when compared to the current literature, we believe that we could improve these results by implementing new measures in the prehabilitation protocol, making it more comprehensive.
As we have already mentioned throughout the article, prehabilitation has gained importance as a tool aimed at improving patient recovery and postoperative outcomes, encompassing a set of measures aimed at optimizing, among others, the physical, nutritional, and psychological status of the patient. While there is strong evidence supporting its utility in improving postoperative outcomes following abdominal surgery, in the context of the ERAS programs, specific evidence in esophagectomies remains limited. However, due to, on the one hand, the high rate of postoperative morbidity associated with this type of surgery, and, on the other hand, the impact on functional reserve caused by cachexia and neoadjuvant therapy, as well as the psychological impact of cancer diagnosis, it seems logical to think that these patients would greatly benefit their functional, physiological, and psychological capacity by undergoing these prehabilitation programs to face surgery and recover from it.
In that sense, Bausys et al. conducted a review of the existing evidence, concluding that there is still considerable variability among prehabilitation programs, as well as in the interventions performed and the outcomes collected (21). They also asserted that one of the main problems with these programs is the low adherence to them. However, their beneficial effect can be confirmed.
Minella et al. in 2018, published the results of a clinical trial in which they noted a significant improvement in the functional capacity of patients before and after surgery in those undergoing prehabilitation (18).
Furthermore, in 2023, An et al., in another systematic review and meta-analysis, with studies from 2000 to 2023 (1,803 patients from 584 clinical trials and 1,219 from observational studies), concluded that prehabilitation reduced respiratory complications and pneumonia in observational studies, but not in clinical trials. These results highlight the low quality of existing evidence in esophagectomies. Regarding the stay in the intensive care unit, operative mortality, and severe complications (Clavien-Dindo ≥3), there were no differences between groups (63).
Zhao et al. have recently published a meta-analysis with the purpose of evaluating the effect of uni- or multimodal prehabilitation in esophagogastric cancer. They included 6 clinical trials and another 6 cohort studies in their analysis, and concluded that multimodal prehabilitation was effective in reducing the risk of severe complications, unlike unimodal prehabilitation (64).
Therefore, in summary, the objective of prehabilitation is to prevent the functional consequences that oncological treatment has on patients, acting on modifiable factors such as exercise, nutrition, anemia, or smoking habits. It aims to improve the patient's overall situation (65).
6.1 Future protocol changes
Taking into account the evidence and being critical of our clinical practice, we believe that despite our results being in line with published series, there are still areas that need to be improved in the preoperative period.
Having reduced our prehabilitation protocol to a trimodal program (nutrition, anemia and exercise) so far, our goal is to expand it into a multimodal program with the inclusion of additional measures.
Firstly, we are beginning with the incorporation of anesthesiologists into the Tumor Committee, as their involvement will provide a valuable perspective in the initial decision-making process.
Furthermore, we will expand the screening of physical fitness to include not only patients eligible for preoperative chemotherapy or radiotherapy but also those selected for direct surgery. We will also assess functional capacity (Duke Activity Status Index, DASI). Thus, all patients with a DASI ≤34 or a CFS ≤4 will be referred to the rehabilitation clinic to determine the appropriate physiotherapy program.
Regarding nutritional status, patients with a MUST = 1 and/or albumin <3 g/dl or a MUST ≥2 will be referred to the nutritionist's clinic (a clinical figure we now have in our hospital) to initiate appropriate nutritional treatment.
Additionally, we have updated our PBM program in these patients and thus, all patients will undergo a blood test with an iron profile, so those with an Hb < 13 g/dl will be evaluated to initiate treatment with intravenous iron, erythropoietin, or both (consensus protocol with the Hematology Department) depending on the etiology of the anemia.
Furthermore, we will conduct an assessment of the patient's social and family situation. If any social alarm indicators are detected (living alone, lack of self-care capacity, homelessness), we will collaborate with the social worker to implement appropriate measures for home discharge after surgery.
Regarding the need for psychological support, while we currently lack a psychologist for this purpose in the hospital, we are actively working to include psychological well-being optimization as soon as possible. This will involve identifying patients who require psychological intervention (using SF-36, HADS) and providing anxiety-reducing techniques for all patients based on their preference. It is one of the areas we are actively working on as we consider it of vital importance. While we cannot guarantee it in all cases yet, we will strive to provide support to those patients we deem most in need with the current resources available in the hospital (psycho-oncology unit).
We will emphasize smoking cessation, providing patients with all necessary information and tools for quitting.
In addition to expanding our protocol to make it more comprehensive, we are developing a strategy to record patients included in the program and register the implemented measures in a dedicated database. Subsequently, we will conduct a review of patients to assess, on the one hand, the compliance of the measures included in the protocol and, on the other hand, to assess the effect of their implementation in terms of outcomes to determine if we, indeed, have improved these, reducing complications.
Conclusion
Enhanced Recovery After Surgery (ERAS) improves postoperative outcomes of esophageal surgery, although many ERAS society recommendations are based on low or moderate levels of evidence and require further evaluation and research. Considering that esophagectomies remain associated with major surgical trauma and significant morbidity, the preoperative risk assessment gains great importance, playing a crucial role in identifying potential risks and optimizing the patient outcomes. Taking advantage of the preoperative period is crucial to ensure that patients arrive in the best clinical and psychological condition, known as prehabilitation, which includes nutrition optimization, exercise (both physical and cognitive), anxiety/stress reduction, smoking and alcohol cessation, identification and treatment of anemia, and adjustment of medical treatments. We advocate for a multimodal prehabilitation program.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
SG: Data curation, Writing – original draft, Writing – review & editing, Formal Analysis, Investigation. LM: Writing – review & editing. NG: Writing – review & editing. MG: Data curation, Investigation, Writing – review & editing. NR: Data curation, Formal Analysis, Investigation, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2021) 71(3):209–49. doi: 10.3322/caac.2166033538338
2. Chen YJ, Schultheiss TE, Wong JYC, Kernstine KH. Impact of the number of resected and involved lymph nodes on esophageal cancer survival. J Surg Oncol. (2009) 100(2):127–32. doi: 10.1002/jso.2131219544364
3. Orringer MB, Sloan H. Esophagectomy without thoracotomy. J Thorac Cardiovasc Surg. (1978) 76(5):643–54. doi: 10.1016/S0022-5223(19)41012-X703369
4. Reed CE. Technique of open Ivor Lewis esophagectomy. Oper Tech Thorac Cardiovasc Surg. (2009) 14(3):160–75. doi: 10.1053/j.optechstcvs.2009.06.001
5. McKeown KC. Total three-stage oesophagectomy for cancer of the oesophagus. Br J Surg. (1976) 63(4):259–62. doi: 10.1002/bjs.18006304031276657
6. Gottlieb-Vedi E, Kauppila JH, Malietzis G, Nilsson M, Markar SR, Lagergren J. Long-term survival in esophageal cancer after minimally invasive compared to open esophagectomy: a systematic review and meta-analysis. Ann Surg. (2019) 270(6):1005–17. doi: 10.1097/SLA.000000000000325230817355
7. Maas KW, Cuesta MA, van Berge Henegouwen MI, Roig J, Bonavina L, Rosman C, et al. Quality of life and late complications after minimally invasive compared to open esophagectomy: results of a randomized trial. World J Surg. (2015) 39(8):1986–93. doi: 10.1007/s00268-015-3100-y26037024
8. Sgourakis G, Gockel I, Radtke A, Musholt TJ, Timm S, Rink A, et al. Minimally invasive versus open esophagectomy: meta-analysis of outcomes. Dig Dis Sci. (2010) 55(11):3031–40. doi: 10.1007/s10620-010-1153-120186484
9. Biere SSAY, van Berge Henegouwen MI, Maas KW, Bonavina L, Rosman C, Garcia JR, et al. Minimally invasive versus open oesophagectomy for patients with oesophageal cancer: a multicentre, open-label, randomised controlled trial. Lancet Lond Engl. (2012) 379(9829):1887–92. doi: 10.1016/S0140-6736(12)60516-9
10. Fay KA, Hasson RM. Editorial: preoperative frailty risk assessment prior to esophagectomy, where are we? Ann Surg Oncol. (2023) 30(7):3892–3. doi: 10.1245/s10434-023-13210-236917334
11. Carney A, Dickinson M. Anesthesia for esophagectomy. Anesthesiol Clin. (2015) 33(1):143–63. doi: 10.1016/j.anclin.2014.11.00925701933
12. Ashok A, Niyogi D, Ranganathan P, Tandon S, Bhaskar M, Karimundackal G, et al. The enhanced recovery after surgery (ERAS) protocol to promote recovery following esophageal cancer resection. Surg Today. (2020) 50(4):323–34. doi: 10.1007/s00595-020-01956-132048046
13. Wynter-Blyth V, Moorthy K. Prehabilitation: preparing patients for surgery. Br Med J. (2017) 358:j3702. doi: 10.1136/bmj.j3702
14. Minnella EM, Coca-Martinez M, Carli F. Prehabilitation: the anesthesiologist's role and what is the evidence? Curr Opin Anaesthesiol. (2020) 33(3):411–6. doi: 10.1097/ACO.000000000000085432371632
15. Minnella EM, Awasthi R, Loiselle SE, Agnihotram RV, Ferri LE, Carli F. Effect of exercise and nutrition prehabilitation on functional capacity in esophagogastric cancer surgery: a randomized clinical trial. JAMA Surg. (2018) 153(12):1081–9. doi: 10.1001/jamasurg.2018.164530193337
16. Yoshida N, Baba Y, Hiyoshi Y, Shigaki H, Kurashige J, Sakamoto Y, et al. Duration of smoking cessation and postoperative morbidity after esophagectomy for esophageal cancer: how long should patients stop smoking before surgery? World J Surg. (2015) 40(1):142–7. doi: 10.1007/s00268-015-3236-9
17. Carli F. Physiologic considerations of enhanced recovery after surgery (ERAS) programs: implications of the stress response. Can J Anesth Can Anesth. (2015) 62(2):110–9. doi: 10.1007/s12630-014-0264-0
18. Lawrence VA, Hazuda HP, Cornell JE, Pederson T, Bradshaw PT, Mulrow CD, et al. Functional independence after major abdominal surgery in the elderly. J Am Coll Surg. (2004) 199(5):762–72. doi: 10.1016/j.jamcollsurg.2004.05.28015501119
19. Barberan-Garcia A, Ubré M, Roca J, Lacy AM, Burgos F, Risco R, et al. Personalised prehabilitation in high-risk patients undergoing elective major abdominal surgery: a randomized blinded controlled trial. Ann Surg. (2018) 267(1):50–6. doi: 10.1097/SLA.000000000000229328489682
20. Bausys A, Mazeikaite M, Bickaite K, Bausys B, Bausys R, Strupas K. The role of prehabilitation in modern esophagogastric cancer surgery: a comprehensive review. Cancers (Basel). (2022) 14(9):2096. doi: 10.3390/cancers1409209635565226
21. Protocolo54_Cancer_Gastrico.pdf. Available online at: https://www.osakidetza.euskadi.eus/contenidos/informacion/hd_publicaciones/es_hdon/adjuntos/Protocolo54_Cancer_Gastrico.pdf (cited February 6, 2024).
22. Filip B, Hutanu I, Radu I, Anitei MG, Scripcariu V. Assessment of different prognostic scores for early postoperative outcomes after esophagectomy. Chir Buchar Rom. (2014) 109(4):480–5. PMID: 25149610
23. Lima MM, Cristelo DM, Mourão J. Physiological and operative severity score for the enumeration of mortality and morbidity, frailty, and perioperative quality of life in the elderly. Saudi J Anaesth. (2019) 13(1):3. doi: 10.4103/sja.SJA_275_1830692881
24. Daabiss M. American society of anaesthesiologists physical status classification. Indian J Anaesth. (2011) 55(2):111–5. doi: 10.4103/0019-5049.7987921712864
25. Yin Y, Jiang L, Xue L. Which frailty evaluation method can better improve the predictive ability of the SASA for postoperative complications of patients undergoing elective abdominal surgery? Ther Clin Risk Manag. (2022) 18:541–50. doi: 10.2147/TCRM.S35728535548665
26. Soumya C, Thomas M, Ravindran S, Jagathnath Krishna K. Preoperative incremental shuttle walk test for morbidity and mortality prediction in elective major colorectal surgery. Indian J Anaesth. (2022) 66(17):250. doi: 10.4103/ija.ija_739_21
27. Struthers R, Erasmus P, Holmes K, Warman P, Collingwood A, Sneyd JR. Assessing fitness for surgery: a comparison of questionnaire, incremental shuttle walk, and cardiopulmonary exercise testing in general surgical patients. Br J Anaesth. (2008) 101(6):774–80. doi: 10.1093/bja/aen31018953057
28. Bellanti F, lo Buglio A, Quiete S, Vendemiale G. Malnutrition in hospitalized old patients: screening and diagnosis, clinical outcomes, and management. Nutrients. (2022) 14(4):910. doi: 10.3390/nu1404091035215559
29. Abdel-Razeq H, Hashem H. Recent update in the pathogenesis and treatment of chemotherapy and cancer induced anemia. Crit Rev Oncol Hematol. (2020) 145:102837. doi: 10.1016/j.critrevonc.2019.10283731830663
30. Connor JP, Destrampe E, Robbins D, Hess AS, McCarthy D, Maloney J. Pre-operative anemia and peri-operative transfusion are associated with poor oncologic outcomes in cancers of the esophagus: potential impact of patient blood management on cancer outcomes. BMC Cancer. (2023) 23:99. doi: 10.1186/s12885-023-10579-x36709278
31. Althoff FC, Neb H, Herrmann E, Trentino KM, Vernich L, Füllenbach C, et al. Multimodal patient blood management program based on a three-pillar strategy: a systematic review and meta-analysis. Ann Surg. (2019) 269(5):794–804. doi: 10.1097/SLA.000000000000309530418206
32. Debes C, Aissou M, Beaussier M. La préhabilitation. Préparer les patients à la chirurgie pour améliorer la récupération fonctionnelle et réduire la morbidité postopératoire. Ann Fr Anesth Réanimation. (2014) 33(1):33–40. doi: 10.1016/j.annfar.2013.12.012
33. Takahashi C, Shridhar R, Huston J, Meredith K. Esophagectomy from then to now. J Gastrointest Oncol. (2018) 9(5):903–9. doi: 10.21037/jgo.2018.08.1530505593
34. Gillis C, Li C, Lee L, Awasthi R, Augustin B, Gamsa A, et al. Prehabilitation versus rehabilitation: a randomized control trial in patients undergoing colorectal resection for cancer. Anesthesiology. (2014) 121(5):937–47. doi: 10.1097/ALN.000000000000039325076007
35. Lee L, Schwartzman K, Carli F, Zavorsky GS, Li C, Charlebois P, et al. The association of the distance walked in 6 min with pre-operative peak oxygen consumption and complications 1 month after colorectal resection. Anaesthesia. (2013) 68(8):811–6. doi: 10.1111/anae.1232923789780
36. Lee DU, Fan GH, Hastie DJ, Addonizio EA, Han J, Prakasam VN, et al. The clinical impact of malnutrition on the postoperative outcomes of patients undergoing gastrectomy for gastric cancer: propensity score matched analysis of 2011–2017 hospital database. Clin Nutr ESPEN. (2021) 46:484–90. doi: 10.1016/j.clnesp.2021.09.00534857239
37. Reim D, Friess H. Feeding challenges in patients with esophageal and gastroesophageal cancers. Gastrointest Tumors. (2016) 2(4):166–77. doi: 10.1159/00044290727403411
38. Son YG, Kwon IG, Ryu SW. Assessment of nutritional status in laparoscopic gastrectomy for gastric cancer. Transl Gastroenterol Hepatol. (2017) 2:85. doi: 10.21037/tgh.2017.09.0829167832
39. Weimann A, Braga M, Carli F, Higashiguchi T, Hübner M, Klek S, et al. ESPEN practical guideline: clinical nutrition in surgery. Clin Nutr. (2021) 40(7):4745–61. doi: 10.1016/j.clnu.2021.03.03134242915
40. Zhang Y, Tan S, Wu G. ESPEN practical guideline: clinical nutrition in surgery. Clin Nutr. (2021) 40(9):5071. doi: 10.1016/j.clnu.2021.07.01234455265
41. Mareschal J, Hemmer A, Douissard J, Dupertuis YM, Collet TH, Koessler T, et al. Surgical prehabilitation in patients with gastrointestinal cancers: impact of unimodal and multimodal programs on postoperative outcomes and prospects for new therapeutic strategies—a systematic review. Cancers (Basel). (2023) 15(6):1881. doi: 10.3390/cancers1506188136980767
42. Thibault R, Abbasoglu O, Ioannou E, Meija L, Ottens-Oussoren K, Pichard C, et al. ESPEN guideline on hospital nutrition. Clin Nutr. (2021) 40(12):5684–709. doi: 10.1016/j.clnu.2021.09.03934742138
43. Volkert D, Beck AM, Cederholm T, Cereda E, Cruz-Jentoft A, Goisser S, et al. Management of malnutrition in older patients—current approaches, evidence and open questions. J Clin Med. (2019) 8(7):974. doi: 10.3390/jcm807097431277488
44. Zhao M, Jiang G, Zhou H, Li J, Xiang W, Li S, et al. Gut microbiota: a potential target for improved cancer therapy. J Cancer Res Clin Oncol. (2022) 149(1):541–52. doi: 10.1007/s00432-022-04546-536550389
45. Tsimopoulou I, Pasquali S, Howard R, Desai A, Gourevitch D, Tolosa I, et al. Psychological prehabilitation before cancer surgery: a systematic review. Ann Surg Oncol. (2015) 22(13):4117–23. doi: 10.1245/s10434-015-4550-z25869228
46. Allen SK, Brown V, White D, King D, Hunt J, Wainwright J, et al. Multimodal prehabilitation during neoadjuvant therapy prior to esophagogastric cancer resection: effect on cardiopulmonary exercise test performance, muscle mass and quality of life-a pilot randomized clinical trial. Ann Surg Oncol. (2022) 29(3):1839–50. doi: 10.1245/s10434-021-11002-034725764
47. Huang T, Zhou F, Wang-Johanning F, Nan K, Wei Y. Depression accelerates the development of gastric cancer through reactive oxygen species-activated ABL1 (review). Oncol Rep. (2016) 36(5):2435–43. doi: 10.3892/or.2016.512727666407
48. Housman B, Flores R, Lee DS. Narrative review of anxiety and depression in patients with esophageal cancer: underappreciated and undertreated. J Thorac Dis. (2021) 13(5):3160–70. doi: 10.21037/jtd-20-352934164206
49. Hu LY, Liu CJ, Yeh CM, Lu T, Hu YW, Chen TJ, et al. Depressive disorders among patients with gastric cancer in Taiwan: a nationwide population-based study. BMC Psychiatry. (2018) 18(1):272. doi: 10.1186/s12888-018-1859-830176847
50. Wong J, An D, Urman RD, Warner DO, Tønnesen H, Raveendran R, et al. Society for perioperative assessment and quality improvement (SPAQI) consensus statement on perioperative smoking cessation. Anesth Analg. (2020) 131(3):955. doi: 10.1213/ANE.000000000000450831764157
51. Egholm JW, Pedersen B, Møller AM, Adami J, Juhl CB, Tønnesen H. Perioperative alcohol cessation intervention for postoperative complications. Cochrane Database Syst Rev. (2018) 11(11):CD008343. doi: 10.1002/14651858.CD008343.pub330408162
52. Pfander V. Substance use disorder and the surgical patient. J Perianesth Nurs. (2023) 38(2):371–2. doi: 10.1016/j.jopan.2023.01.00236965925
53. Song Y, Tang R, Roses RE, Fraker DL, DeMatteo RP, Kelz RR, et al. Opioid use disorder is associated with complications and increased length of stay after major abdominal surgery. Ann Surg. (2021) 274(6):992–1000. doi: 10.1097/SLA.000000000000369731800489
54. Ishimaru M, Matsui H, Ono S, Hagiwara Y, Morita K, Yasunaga H. Preoperative oral care and effect on postoperative complications after major cancer surgery. Br J Surg. (2018) 105(12):1688–96. doi: 10.1002/bjs.1091530088267
55. Las_Cifras_del_cancer_en_Espana2018.pdf. Available online at: https://seom.org/seomcms/images/stories/recursos/Las_Cifras_del_cancer_en_Espana2018.pdf (cited April 8, 2024).
56. Thrumurthy SG, Chaudry MA, Thrumurthy SSD, Mughal M. Oesophageal cancer: risks, prevention, and diagnosis. BMJ. (2019) 366:l4373. doi: 10.1136/bmj.l437331289038
57. Ajani JA, D’Amico TA, Bentrem DJ, Cooke D, Corvera C, Das P, et al. Esophageal and esophagogastric junction cancers, version 2.2023, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. (2023) 21(4):393–422. doi: 10.6004/jnccn.2023.001937015332
58. Low DE, Bodnar A. Update on clinical impact, documentation, and management of complications associated with esophagectomy. Thorac Surg Clin. (2013) 23(4):535–50. doi: 10.1016/j.thorsurg.2013.07.00324199703
59. Saeki H, Tsutsumi S, Tajiri H, Yukaya T, Tsutsumi R, Nishimura S, et al. Prognostic significance of postoperative complications after curative resection for patients with esophageal squamous cell carcinoma. Ann Surg. (2017) 265(3):527–33. doi: 10.1097/SLA.000000000000169228169928
60. Low DE, Kuppusamy MK, Alderson D, Cecconello I, Chang AC, Darling G, et al. Benchmarking complications associated with esophagectomy. Ann Surg. (2019) 269(2):291–8. doi: 10.1097/SLA.000000000000261129206677
61. Low DE, Alderson D, Cecconello I, Chang AC, Darling GE, D'Journo XB, et al. International consensus on standardization of data collection for complications associated with esophagectomy: esophagectomy complications consensus group (ECCG). Ann Surg. (2015) 262(2):286–94. doi: 10.1097/SLA.000000000000109825607756
62. Walters DM, McMurry TL, Isbell JM, Stukenborg GJ, Kozower BD. Understanding mortality as a quality indicator after esophagectomy. Ann Thorac Surg. (2014) 98(2):506–11; discussion 511–512. doi: 10.1016/j.athoracsur.2014.03.04124841544
63. An KR, Seijas V, Xu MS, Grüßer L, Humar S, Moreno AA, et al. Does prehabilitation before esophagectomy improve postoperative outcomes? A systematic review and meta-analysis. Dis Esophagus. (2024) 37(3):doad066. doi: 10.1093/dote/doad06638018252
64. Zhao B, Zhang T, Chen Y, Zhang C. Effects of unimodal or multimodal prehabilitation on patients undergoing surgery for esophagogastric cancer: a systematic review and meta-analysis. Support Care Cancer. (2023) 32(1):15. doi: 10.1007/s00520-023-08229-w38060053
65. Beilstein CM, Krutkyte G, Vetsch T, Eser P, Wilhelm M, Stanga Z, et al. Multimodal prehabilitation for major surgery in elderly patients to lower complications: protocol of a randomised, prospective, multicentre, multidisciplinary trial (PREHABIL trial). BMJ Open. (2023) 13(1):e070253. doi: 10.1136/bmjopen-2022-07025336596634
Keywords: esophageal surgery, ERAS, prehabilitation program, preoperative risk assessment, exercise
Citation: González Santos S, Martí Gelonch L, González Jorrín N, González Osinalde M and Rosell Romero N (2024) Preoperative risk assessment and prehabilitation strategies in patients undergoing an esophagectomy for cancer resections: a single center retrospective analysis and a review of the literature. Front. Anesthesiol. 3:1358847. doi: 10.3389/fanes.2024.1358847
Received: 20 December 2023; Accepted: 12 August 2024;
Published: 29 August 2024.
Edited by:
Hong Liu, UC Davis Health, United StatesReviewed by:
Marc Licker, University of Geneva, SwitzerlandChristian Bohringer, UC Davis Medical Center, United States
Copyright: © 2024 González Santos, Martí Gelonch, González Jorrín, González Osinalde and Rosell Romero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Silvia González Santos, ZHJhX3Nnc2FudG9zQHlhaG9vLmVz