 Marc Kriege
Marc Kriege René Rissel1
René Rissel1- 1Department of Anesthesiology, University Medical Center of the Johannes Gutenberg-University Mainz, Mainz, Germany
- 2Department of Cardiac and Vascular Surgery, University Medical Center of the Johannes Gutenberg-University Mainz, Mainz, Germany
Background: A laryngeal tube is often used as an alternative to intubation with direct laryngoscopy during cardiopulmonary resuscitation. However, in a study with piglets undergoing simulated cardiac arrest, reduced carotid artery blood flow was associated with the insertion of different supraglottic airway devices, such as a laryngeal tube. Limited by its construction, secondary tracheal intubation through a laryngeal tube was difficult or impossible in contrast to a second generation laryngeal mask. The new disposable intubating laryngeal tube with suction (iLTS-D®) seems to facilitate tracheal intubation. We hypothesized that iLTS-D, when inflated to the recommended air volume, does not reduce cerebral oxygenation in patients with cardiovascular diseases undergoing elective cardiac surgery.
Methods: This single-center prospective, controlled observational study was approved by the local ethics committee (Ethical Committee No. 2018-13716). Forty adult patients undergoing elective cardiac surgery requiring tracheal intubation were included in this study. The exclusion criteria were age <18 years and a high risk of aspiration, inability to consent, height <155 cm, or pregnancy. Prior to insufflation and deflation of the cuffs, we performed cerebral oximetry via near-infrared spectroscopy. The primary outcome was a significant reduction in NIRS in the context of the preinduction baseline value after inflation of the cuffs with the recommended air volume, defined as a ≥25% decrease from baseline or an absolute value ≤ 50%. The secondary endpoints were differences in time points, insertion success rates, and complications.
Results: There was no significant reduction in cerebral oximetry after inflation with the recommended cuff volume and an initially measured cuff pressure of >120 cmH2O. Overall, tracheal intubation was achieved in a median of 20 s [interquartile range 15-23 s] and enabled sufficient ventilation and tracheal intubation through the iLTS-D in all patients. Traces of blood on the cuffs (after removing the iLTS-D) and a sore throat (evaluated 2 h after removing the tracheal tube) were observed in one patient.
Conclusion: Our results showed no association between the insertion of the iLTS-D and reduced cerebral oxygenation in patients undergoing elective cardiac surgery.
Trial registration: ClinicalTrials.gov, NCT03942809.
Introduction
The laryngeal tube is a standard supraglottic airway device routinely used during cardiopulmonary resuscitation or difficult airway management during in-hospital and out-of-hospital emergencies [1–3]. In a cluster-crossover trial of 3,004 adults with out-of-hospital cardiac arrest, an initial laryngeal tube insertion was associated with a significantly higher 72 h survival compared to tracheal intubation by emergency medical services [1]. The advantage of the laryngeal tube is easier handling (blindly placed) than tracheal intubation with direct laryngoscopy, without the need to stop chest compressions during cardiac arrest [3–5]. Therefore, several guidelines recommend the use of laryngeal tubes as a rescue technique in the event of failed tracheal intubation [6–8].
Despite this recent shift in airway management practice, little is known about the potential effects of laryngeal tubes on cervical vessels and any associated cerebral hemodynamic effects. The proximal (oropharyngeal) balloon is designed to seal the pharynx above the ventilation port, and the distal (esophageal) balloon is designed to seal the airway distally. The clinical effects of cuff insufflation on the cervical vessels were first studied by Colbert et al. [9]. This study concluded that the cross-sectional area of both carotid arteries significantly decreased after inflation of the laryngeal mask cuff, which was compensated by an increase in flow velocity and carotid blood flow [9]. Reduction in the carotid artery diameters was more marked in patients older than 60 years, where the cross-sectional area dropped after inflation by more than 60% when compared with the area measured during cuff deflation [9]. Segal et al. showed in a study with young pigs (32 kg) under experimental cardiac arrest an association between three supraglottic airway devices (laryngeal tube, laryngeal mask and Combi tube) and a significant reduction in carotid blood flow [10]. Eismann et al. observed no difference in flow velocity during cuff inflation of the laryngeal tube and a second-generation laryngeal mask in older patients without a diagnosed carotid stenosis of > 50% [11]. This study excluded patients with carotid artery stenosis >50% of internal diameter and American Society of Anesthesiologists status (ASA) 4.
However, secondary intubation (blind or with a bougie) through a placed laryngeal tube is either difficult or impossible. The novel disposable intubating laryngeal tube with suction (iLTS-D; VBM® Medizintechnik GmbH, Sulz, Germany) was used to study intubation performance in patients undergoing elective surgery [12–15] and a simulated airway [16–20]. The manufacturer recommends endoscopic-guided tracheal intubation, although several studies have reported successful blind tracheal intubation through the iLTS-D [12–15]. The new version presents a different localization of the proximal cuff and a softer material. We hypothesized that iLTS-D after inflated to the recommended air volume does not reduce cerebral oxygenation in patients with cardiovascular diseases undergoing elective cardiac surgery.
The aim of this study was to evaluate whether the new iLTS-D is associated with a significant reduction in cerebral oxygenation in patients with cardiovascular disease undergoing cardiac surgery under general anesthesia.
Methods
Ethics
Data were collected between May 2019 and April 2020 at the University Medical Center, Mainz, Germany. Ethics approval for this study (Ethical Committee No. 2018-13716) was provided by the Ethical Committee of the Medical Association of the Rhineland Palatine State, Germany (Chairperson Dr. A. Wagner) on 18 May. Written informed consent was obtained from all of the patients.
Study design
We designed a prospective, observational study of surgical patients (Department of Cardiac and Vascular Surgery) undergoing general anesthesia at a tertiary university hospital (Clinical Trial Register number NCT03942809).
Participants
The inclusion criteria were adult patients scheduled for elective cardiac surgery under general anesthesia requiring mechanical ventilation via an tracheal tube. We excluded patients if they had an increased risk of pulmonary aspiration, inability to consent, height <155 cm, or were pregnant (Figure 1).
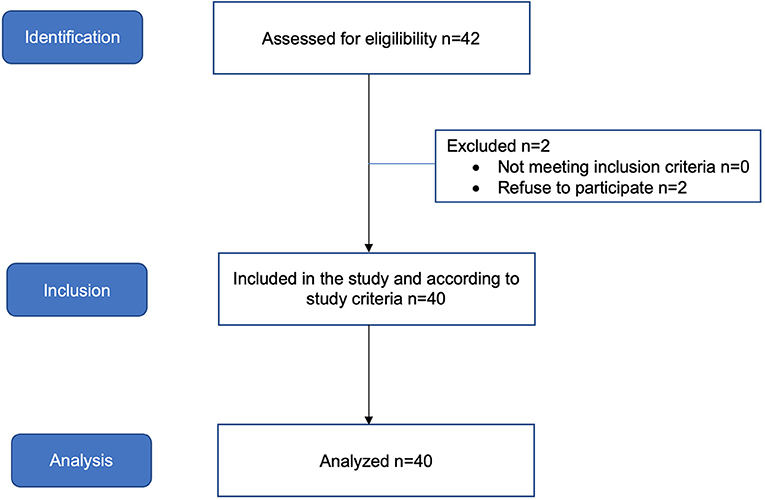
Figure 1. Patient flow chart.
Study settings and measurements
The iLTS-D has been recently modified and is an improved version of the laryngeal tube. The insertion technique is similar to the laryngeal tube. The ventilation orifice is shaped like a “ramp” within the canal to guide the tracheal tube at a steep angle in the direction of the glottis.
The novel iLTS-D is currently available in an adult size, which fits classical laryngeal tube sizes 4 and 5 simultaneously, with two separate marks positioned at the upper front teeth level to define the optimal depth of insertion. The cuffs are inflated with a syringe using the air volume recommended by the manufacturer (the syringe is color-coded by the manufacturer). After placement, the cuff pressure is controlled with a cuff pressure manometer (VBM® Cuff pressure gauge; VBM Medizintechnik, Sulz, Germany). In this trial, we used the aScope™ 4 Regular (Ambu®, Ballerup, Denmark) for endoscopically guided tracheal intubation. The proximal end of the gastric tube is shaped like a small cone for ease of insertion. The manufacturer provides a rigid plastic “pusher” to allow for the removal of the iLTS-D while the tracheal tube is kept in place (Figure 2).
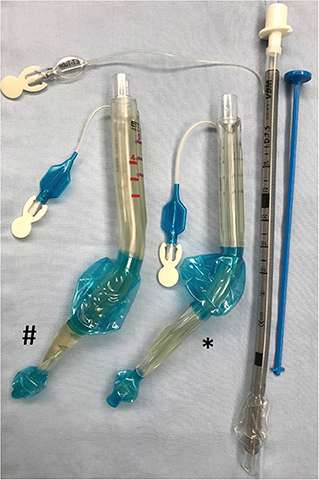
Figure 2. *Novel iLTS-D compared to the #predecessor version and tracheal tube with the rigid plastic pusher.
All patients underwent standard invasive anesthesia monitoring, bispectral analysis monitoring, and near-infrared spectroscopy (NIRS). NIRS cerebral profiles were collected during the procedure using a 2-wavelength (730–810 nm) cerebral oximeter (monitor INVOS 5100C®, Covidien, Medtronic's, USA) to record the regional cerebral oxygen saturation (rScO2). The NIRS optodes were placed on the left frontoparietal side of the patient's head. NIRS is an indirect indicator of perfusion adequacy. Therefore, it provides continuous information on the oxygen supply vs. demand balance. NIRS utilizes the transparency of the scalp and skull to infrared light and the differences in the absorption spectra between oxyhemoglobin and deoxyhemoglobin to quantify the local oxygen saturation of hemoglobin in the brain. Several of the influencing factors include the perfusion pressure, arterial oxygen content, partial pressure of carbon dioxide, hemoglobin, cardiac output, and cerebral metabolic rate of oxygen [21]. Normal values for the NIRS are between 60-75%, but physiological values of 55-60% have been reported in cardiac patients [21]. Therefore, trends in the values are considered more important in clinical practice than the absolute values of rScO2.
Before induction of general anesthesia, the baseline value for each patient was recorded while the patient was still awake, and this baseline was considered the individual reference value. After sufficient preoxygenation (etO2 > 90%), general anesthesia was induced with sufentanil (0.5 μg.kg−1) and propofol (1–2 mg.kg−1), and anesthesia was maintained using either propofol infusion (3-4 mg.kg−1) or volatile anesthetics at a minimal alveolar concentration between 0.8 and 1.0. All patients were pressure-controlled ventilated with a tight-fitting face mask to reach normocapnia (expiratory carbon dioxide between 35 and 45 mmHg), as displayed by the anesthesia respirator (Draeger® Pallas, Luebeck, Germany). Once deep anesthesia (bispectral index <60) and administration of a sufficient dose of a neuromuscular blocking agent (Rocuronium 1 mg.kg−1) were confirmed, the iLTS-D was inserted according to the manufacturer's recommendations. All patients were anesthetized by an experienced cardiac anesthesiologist with prior experience with iLTS-D or laryngeal tubes.
The primary outcome was a significant reduction in NIRS in the context of the preinduction baseline value after inflation of the cuffs with the recommended air volume, defined as a ≥25% decrease from baseline or an absolute value ≤ 50%. NIRS was measured at three time points: (i) baseline, (ii) after anesthesia induction, and (iii) after the initial inflation of the cuffs. NIRS was measured at each time point after three cardiac cycles. The time to insertion, time to ventilation with the iLTS-D, time to tracheal intubation (both times were stopped after inflection of the capnography wave), time to removal of the iLTS-D, success rate of the iLTS-D insertion and tracheal intubation (defined as within <60 s), glottis visualization, and complications were defined as secondary endpoints. For endoscopic-guided tracheal intubation, the best endoscopic views were graded from 1 to 4: 1 = vocal cords entirely visible; 2 = vocal cords or arytenoid cartilages partially visible; 3 = epiglottis only visible; and 4 = no laryngeal structures visible [22]. Capnography confirmed successful iLTS-D insertion and tracheal tube placement. After correct tracheal tube placement, the iLTS-D was removed using the rigid “pusher”. An additional study nurse not involved in patient care was present during the induction of anesthesia to record study parameters.
Statistical analyses
Sample size calculation was performed using G*Power 3.1 [23]. A sample size of 40 was calculated assuming an alpha error of 5% and a power of 90%. All collected data were processed using GraphPad Prism 9.0 h (GraphPad® Software Inc., USA). Data were tested for a normal distribution (Shapiro–Wilk normality test) and are presented as the mean and standard deviation (SD) for a normal distribution or as median and interquartile range [IQR] for a nonnormal distribution. Differences in NIRS and the time intervals were calculated using the Wilcoxon signed-rank test. Statistical significance was set at a P-value < 0.05.
Results
Forty patients were enrolled in this study (Figure 1). Patient characteristics are described in Table 1.
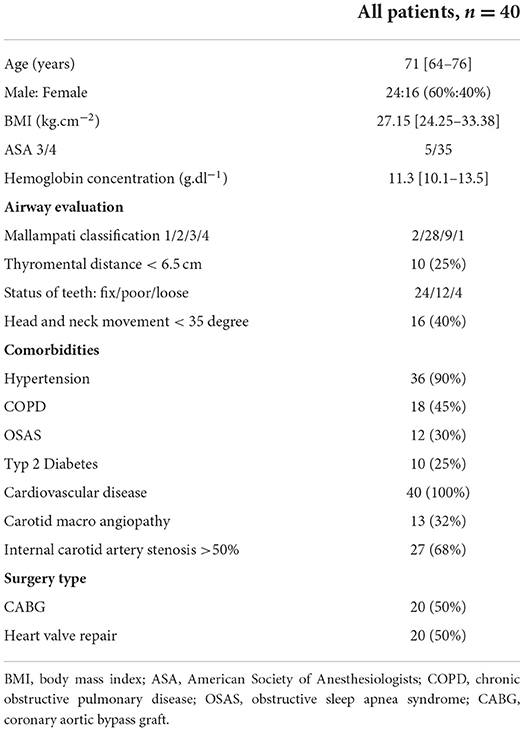
Table 1. Baseline patient characteristics presented as numbers (proportion) or median [IQR].
The first attempt to insert the iLTS-D was successful in all patients. After inflation with the recommended cuff volume, a cuff pressure of 110 [90–120] cmH2O was measured. The oropharyngeal leak pressure was 25 [24–28] cmH2O with a cuff pressure of 50 [50–60] cmH2O. Therefore, we evacuated a cuff volume of 12 ml [8–15] to decrease the initial measured cuff pressure to 60 cmH2O. The NIRS data are presented in Figure 3. NIRS median values before (T0) 72% [70–73], after anesthesia induction (T1) 74% [70–72] and after insertion of the iLTS-D (T2) with inflation of the cuffs at 70% [70–74] were similar (P = 0.31). The perioperative characteristics are shown in Table 2.
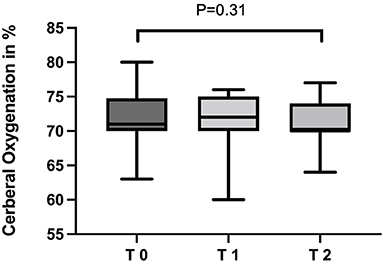
Figure 3. Tukey boxplot of different NIRS in % at the indicated time-points. The line in middle of the box represents the median; the top and bottom of the boxes are the 25 and 75th percentiles [IQR]; the whiskers represent the range. T0: baseline NIRS; T1: after anesthesia induction; T2: after iLTS-D insertion.
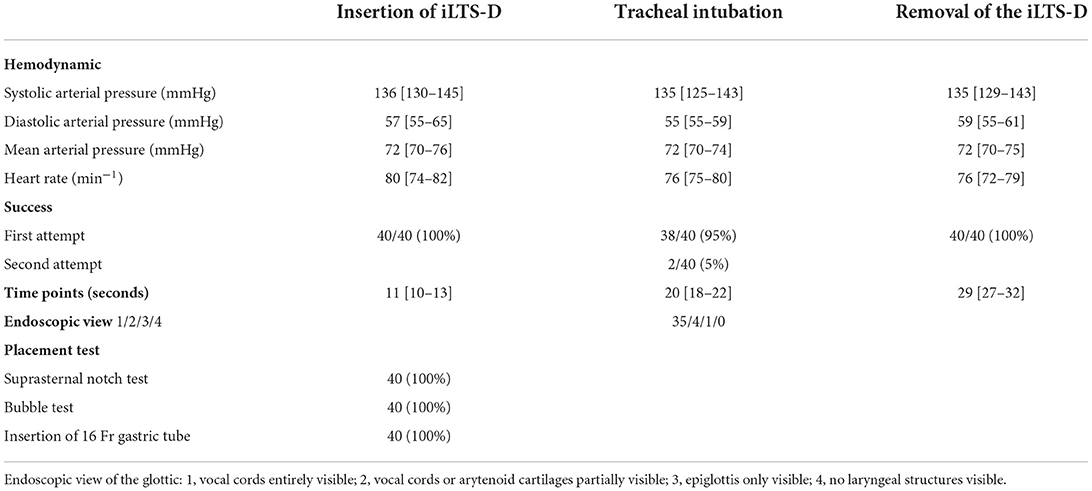
Table 2. Peri-operative characteristics presented as numbers (proportion) or median [IQR].
Endoscopic guided intubation at the first attempt was successful in 38/40 (95%) patients. In two (5%) patients with difficult visualization of the laryngeal structures (one patient with only the epiglottis visible and one patient with no visible laryngeal structures), intubation was possible after correcting the position of the iLTS-D, guided by visualization with the video endoscope. After removal of the iLTS-D over the tracheal tube, no traces of blood at the iLTS-D cuff or dental/lip lesions were observed. Desaturation did not occur during or after any step in this study. One female patient complained of a sore throat 2 h after tracheal extubation in the intensive care unit.
Discussion
This study showed no significant differences in regional cerebral oxygen saturation measured by NIRS as an indirect indicator of cerebral perfusion using the novel iLTS-D in patients with cardiovascular disease undergoing elective cardiac surgery. To the best of our knowledge, this is the first study evaluating the potential for impaired cerebral oxygenation during use of the iLTS-D as a supraglottic airway device in patients undergoing cardiac surgery.
The patient characteristics in this study were consistent with those of previous studies evaluating iLTS-D in a clinical setting [12–15]. Different from other studies, we included ASA 4 patients with changes in their cervical vessels (e.g., carotid artery stenosis). Our findings are in contrast to one study suggesting a significant reduction in carotid artery blood flow when using a laryngeal tube [10]. However, the authors investigated piglets with a weight of 32 kg and limited transferability to human conditions. Furthermore, their measurements were obtained during cardiac arrest and not during hemodynamic stability. A study in humans investigating different supraglottic airway devices yielded heterogeneous results, as the laryngeal tube was not associated with impaired internal carotid artery blood flow during general anesthesia in adult patients with an ASA ≤ 3 and without diagnosed carotid stenosis >50% [11].
Otherwise, one study demonstrated that inflation with a fixed cuff volume (without a cuff pressure measurement) of a laryngeal mask resulted in a decrease in the cross-sectional area and a decrease in blood flow in the common carotid bulb in adult patients <55 years with an ASA ≤ 3 [9]. Sulzgruber et al. showed a poor 30-day survival rate (8.9 vs. 15.8%) in patients with out-of-hospital cardiac arrest and the use of laryngeal tubes compared to tracheal intubation [23]. Interestingly, Whang et al. showed a higher 72 h survival rate (18.3 vs. 15.4%), successful initial airway insertion (44.1 vs. 11.8%), and faster return of spontaneous circulation (27.9 vs. 24.3%) in the laryngeal tube group than in the tracheal intubation group [24]. The authors explained the different survival rates by provider experience (paramedics vs. emergency physicians), adequate chest compressions or sufficient ventilation and aspiration, or crossover timings.
First-pass success for the iLTS-D insertion was comparable with existing studies that investigated iLTS-D in humans or manikins (98–100% [12–19]). Noticeable in clinical settings, more correction maneuvers (2–4 maneuvers) are necessary to improve ventilation after iLTS-D insertion [12, 13]. Manikin-based studies are not directly transferable to humans because of the simulated airway anatomy. Additionally, a possibly harmful overestimation of the clinical capability of inexperienced participants after simulator training was reported [4]. In this current trial, 95% of video endoscope-guided tracheal intubations were successful on the first attempt. In 5% of patients, the reason for failed intubation was the tracheal tube being hindered from moving forward in the device due to impingement of the tracheal tube against the laryngeal structure (e.g., arytenoid cartilages). In accordance with other studies, we observed two patients with limited visualization of the glottic structures graded III–IV with the need for a second attempt [12–14]. Blind intubation in humans at the first attempt has inconsistent success, ranging from 13 to 65% [12–14]. One study reported a success rate of blind intubation through an iLTS-D of 65% and a high leak pressure (mean 39.6 cmH2O) in extremely obese patients [14]. Correct alignment of the cuffs and ventilation orifice of the iLTS-D has been reported as essential, hence resulting in a strong recommendation to use endoscopic assistance for guided tracheal intubation via a supraglottic airway device [12, 13, 25–28]. The specific time measurements were comparable to the existing data in clinical or simulated-based studies [12–19]. Interestingly, the definition of “intubation time” varies among studies. Either the time was stopped after the chest rose [16, 17] or inflection on the expired waveform capnography [12–14]. In contrast to the study by Reviriego-Agudo et al. [13], we observed no bloodstains after removal of the iLTS-D and a lower frequency of sore throat [12, 14, 15]. A possible reason might be the dispensation of blind attempts in combination with a high first-pass success rate.
Limitations
The current study had several limitations. First, the design was observational, single-center, and included only one type of supraglottic airway device. Second, all investigators had sufficient clinical experience with the iLTS-D for both iLTS-D insertions and tracheal intubation, which probably does not reflect daily practice. To the best of our knowledge, there are no data on the learning curve of the iLTS-D. In addition, the number of analyzed patients might have been too small to identify relevant effects in changes in the cerebral oxygenation, hemodynamics or rate of complications with the iLTS-D. Otherwise, we recorded a high insertion and intubation first-pass success rate in this small patient group. Third, we documented cerebral oxygenation using NIRS, which may not have detected previously described reductions in the carotid artery diameter or blood flow. Fourth, the recommended use of a flexible endoscope to guide the intubation changes the configuration of the intubation technique compared to the intubating laryngeal mask (e.g., Fastrach™). Although the latter was not routinely used to guide the intubation, it might have changed the ease and success rate of the intubation. Fifth, we used a standardized assessment after anesthesia induction and one neuromuscular blockade to ensure optimal conditions for iLTS-D insertion. In contrast to our study, many anesthesiologists or paramedics use laryngeal tubes out-of-hospital in patients with cardiac arrest. In these cases, the conditions of the tongue muscle tone and laryngeal airway reflexes are comparable with our study setting, but our findings do not apply to patients with cardiac arrest.
Conclusion
This observational study showed no impairment of cerebral oxygenation by the novel iLTS-D in patients with cardiovascular disease undergoing cardiac surgery. Advantages of this new device include a high first-pass success rate, high oropharyngeal leak pressure, and in combination with video endoscope guidance, facilitated tracheal intubation, both of which demonstrate benefits for clinical practice. Further comparative studies, especially under low-flow perfusion or cardiac arrest, are needed to exclude any detrimental effects of supraglottic airway devices in humans.
Author's note
This manuscript is our original unpublished work and has not been submitted to any other journal. Parts of this study have been presented as a poster presentation at the European Society for Airway Management Congress (EAC) 2018, Valencia, Spain.
Data availability statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession number(s) can be found in the article/Supplementary material.
Ethics statement
Ethical approval for this study (Ethical Committee No. 2018-13716) was provided by the Ethical Committee of the Medical Association of the Rhineland Palatine State, Germany (Chairperson Dr. A. Wagner) on 18 May. Written informed consent was obtained from all the patients. The patients/participants provided their written informed consent to participate in this study.
Author contributions
MK is the guarantor of the paper. All authors meet the criteria for authorship as recommended by the International Committee of Medical Journal Editors. All authors contributed to the production of the final manuscript with revision for important intellectual content.
Funding
This trial was supported by a local grant from the Department of Anesthesiology. No company supported this trial financially or was involved in the study design, data collection, analysis, or interpretation of the results. No other funding or competing interests were declared.
Acknowledgments
The authors would like to thank all anesthesiologists and nurses for their assistance in conducting this clinical trial.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fanes.2022.990391/full#supplementary-material
References
1. Bernhard M, Beres W, Timmermann A, Stepan R, Greim CA, Kaisers UX, et al. Prehospital airway management using the laryngeal tube. An emergency department point of view. Anaesthesist. (2014) 63:589–96. doi: 10.1007/s00101-014-2348-1
2. Schalk R, Auhuber T, Haller O, Latasch L, Wetzel S, Weber CF, et al. Implementation of the laryngeal tube for prehospital airway management: training of 1,069 emergency physicians and paramedics. Anaesthesist. (2012) 61:35–40. doi: 10.1007/s00101-011-1966-0
3. van Tulder R, Schriefl C, Roth D, Stratil P, Thalhammer M, Wieczorek H, et al. Laryngeal tube practice in a metropolitan ambulance service: a five-year retrospective observational study (2009-2013). Prehosp emerg care. (2020) 24:434–40. doi: 10.3109/10903127.2015.1129473
4. Wang HE, Schmicker RH, Daya MR, Stephens SW, Idris AH, Carlson JN, et al. Effect of a strategy of initial laryngeal tube insertion vs endotracheal intubation on 72-hour survival in adults with out-of-hospital cardiac arrest: a randomized clinical trial. JAMA. (2018) 320:769–78. doi: 10.1001/jama.2018.7044
5. Burns JB Jr, Branson R, Barnes SL, Tsuei BJ. Emergency airway placement by EMS providers: comparison between the King LT supralaryngeal airway and endotracheal intubation. Prehosp Disaster Med. (2010) 25:92–5. doi: 10.1017/S1049023X00007743
6. Piepho T, Cavus E, Noppens R, Byhahn C, Dörges V, Zwissler B, et al. S1 guidelines on airway management: Guideline of the German Society of Anesthesiology and Intensive Care Medicine. Anaesthesist. (2015) 64:27–40. doi: 10.1007/s00101-015-0109-4
7. Timmermann A, Böttiger BW, Byhahn C, Dörges V, Eich C, Gräsner JT, et al. S1-Leitlinie: Prähospitales Atemwegsmanagement. Anästh Intensiv Care. (2019) 60:316–36. doi: 10.19224/ai2019.316
8. Law JA, Duggan LV, Asselin M, Baker P, Crosby E, Downey A, et al. Canadian Airway Focus Group updated consensus-based recommendations for management of the difficult airway: part 2. Planning and implementing safe management of the patient with an anticipated difficult airway. Can J Anaesth. (2021) 68:1405–36. doi: 10.1007/s12630-021-02008-z
9. Colbert S, O'Hanlon DM, Page R, Flanagan F, Moriarty D. Haemodynamic changes with the laryngeal mask airway-off the cuff. Euro J Anaesthesiol. (1997) 14:514–7. doi: 10.1097/00003643-199709000-00006
10. Segal N, Yannopoulos D, Mahoney BD, Frascone RJ, Matsuura T, Cowles CG, et al. Impairment of carotid artery blood flow by supraglottic airway use in a swine model of cardiac arrest. Resuscitation. (2012) 83:1025–30. doi: 10.1016/j.resuscitation.2012.03.025
11. Eismann H, Sieg L, Otten O, Leffler A, Palmaers T. Impact of the laryngeal tube as supraglottic airway device on blood flow of the internal carotid artery in patients undergoing general anesthesia. Resuscitation. (2019) 138:141–5. doi: 10.1016/j.resuscitation.2019.03.010
12. Bergold MN, Kahle S, Schultzik T, Bucheler M, Byhahn C. Intubating laryngeal tube suction disposable: Initial clinical experiences with a novel device for endotracheal intubation. Anaesthesist. (2016) 65:30–5. doi: 10.1007/s00101-015-0100-0
13. Reviriego-Agudo L, Charco-Mora P, Greif R, Kleine-Brueggeney M. Blind intubation through the disposable intubating laryngeal tube suction: A prospective observational study. Euro J Anaesthesiol. (2020) 37:508–10. doi: 10.1097/EJA.0000000000001213
14. Gaszynski T. The intubating laryngeal tube (iLTS-D) for blind intubation in superobese patients. J Clin Anesth. (2019) 52:91–2. doi: 10.1016/j.jclinane.2018.09.017
15. Zuercher M, Casso G, Krugel V, Potié A, Barry MP, Schoettker P. Tracheal intubation using intubating laryngeal tube iLTS-D™ and LMA Fastrach™ in 99 adult patients: A prospective multicentric randomised non-inferiority study. J Clin Anesth. (2022) 78:110671. doi: 10.1016/j.jclinane.2022.110671
16. Bruceta MA, Priti DG, McAllister P, Prozesky J, Vaida SJ, Budde AO. Ambu AuraGain versus intubating laryngeal tube suction as a conduit for endotracheal intubation. J Anaesthesiol. (2019) 35:348–52. doi: 10.4103/joacp.JOACP_214_17
17. Ott T, Fischer M, Limbach T, Schmidtmann I, Piepho T, Noppens RR. The novel intubating laryngeal tube (iLTS-D) is comparable to the intubating laryngeal mask (Fastrach)—a prospective randomised manikin study. Scand J Trauma. (2015) 23:44. doi: 10.1186/s13049-015-0126-y
18. Ott T, Tschöpe K, Toenges G, Buggenhagen H, Engelhard K, Kriege M. Does the revised intubating laryngeal tube (ILTS-D2) perform better than the intubating laryngeal mask (Fastrach)?—A randomised simulation research study. BMC Anesthesiol. (2020) 20:111. doi: 10.1186/s12871-020-01029-3
19. Somri M, Matter I, Gaitini LA, Safadi A, Hawash N, Gómez-Ríos M. Fiberoptic-guided and blind tracheal intubation through iLTS-D, Ambu® Auragain™, and I-Gel® supraglottic airway devices: a randomized crossover manikin trial. J Emerg Med. (2019) 16:S0736–4679. doi: 10.1016/j.jemermed.2019.09.045
20. Aleksandrowicz D, Gaszynski T. Intubation through 2 supraglottic airway device in cervical spine immobilization: a randomized trial of residents' use of the intubating laryngeal mask airway and the intubating laryngeal tube in manikins. Emergencias. (2018) 30:186–9.
21. Denault A, Deschamps A, Murkin JM. A proposed algorithm for the intraoperative use of cerebral near-infrared spectroscopy. Semin Cardiothorac Vasc Anesth. (2007) 11:274–81. doi: 10.1177/1089253207311685
22. Verghese C, Berlet J, Kapila A, Pollard R. Clinical assessment of the single use laryngeal mask airway-the LMA-unique. Brit J Anaesth. (1998) 80:677–9. doi: 10.1093/bja/80.5.677
23. Faul F, Erdfelder E, Lang A-G, Buchner A. G* Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. (2007) 39:175–91. doi: 10.3758/BF03193146
24. Sulzgruber P, Datler P, Sterz F, Poppe M, Lobmeyr E, Keferböck M, et al. The impact of airway strategy on the patient outcome after out-of-hospital cardiac arrest: A propensity score matched analysis. Eur Heart J Acute Cardiovasc Care. (2018) 7:423–31. doi: 10.1177/2048872617731894
25. Wenk M, Waurick R, Schotes D, Wenk M, Gerdes C, Van Aken HK, et al. Simulation-based medical education is no better than problem-based discussions and induces misjudgment in self-assessment. Adv Health Sci Educ Theory Pract. (2009) 14:159–71. doi: 10.1007/s10459-008-9098-2
26. Theiler L, Gutzmann M, Kleine-Brueggeney M, Urwyler N, Kaempfen B, Greif R. i-gel supraglottic airway in clinical practice: a prospective observational multicentre study. Brit J Anaesth. (2012) 109:990–5. doi: 10.1093/bja/aes309
27. Lee J-H, Park S, Jang Y-E, Kim E-H, Kim H-S, Kim J-T. The distance between the glottis and the cuff of a tracheal tube placed through three supraglottic airway devices in children: a randomised controlled trial. Eur J Anesthesiol. (2019) 36:721–7. doi: 10.1097/EJA.0000000000001070
Keywords: oxygen saturation, endotracheal intubation, airway management, hemodynamic monitoring, anesthesia, cardiac procedures
Citation: Kriege M, Rissel R, Heid F, Ott T, Beyrouti HE and Hotz E (2022) Airway management with novel intubating laryngeal tubes has no influence on cerebral oxygenation in cardiac surgery patients: A prospective observational study. Front. Anesthesiol. 1:990391. doi: 10.3389/fanes.2022.990391
Received: 09 July 2022; Accepted: 05 October 2022;
Published: 22 November 2022.
Edited by:
Giovanni Landoni, San Raffaele Hospital (IRCCS), ItalyReviewed by:
Wael Saasouh, Detroit Medical Center, United StatesSilvia Delrio, University of Udine, Italy
Copyright © 2022 Kriege, Rissel, Heid, Ott, Beyrouti and Hotz. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marc Kriege, bWFrcmllZ2VAdW5pLW1haW56LmRl